Embed Size (px)
Citation preview

Mod Rheumatol (2004) 14:331–332 © Japan College of Rheumatology and Springer-Verlag Tokyo 2004DOI 10.1007/s10165-004-0320-7
H. Okamoto (*) · N. KamataniInstitute of Rheumatology, Tokyo Women’s Medical University,10-22 Kawada-cho, Shinjuku-ku, Tokyo 162-0054, JapanTel. �81-3-5269-1725; Fax �81-3-5269-1726e-mail: [email protected]
H. ShindoInstitute of Geriatrics, Tokyo Women’s Medical University, Tokyo,Japan
Key words Behçet’s disease · Colitis · Endoscopic ultra-sonogram (EUS) · Inflammatory bowel diseases (IBD)
To the Editor:Behçet’s disease is a systemic inflammatory disorder of un-known etiology. Although Behçet’s disease has a worldwidedistribution, cases are especially prevalent in Japan, theMiddle East, and some Mediterranean countries. Behçet’sdisease is characterized by recurrent oral aphthous ulcersand genital ulcers, and can be life-threatening.1 Ingastrointestinal Behçet’s disease, the lesions can be distrib-uted along the full length of the gastrointestinal tract fromthe mouth to the anus. However, the ileocecal region ismost frequently affected, although the transverse colon,ascending colon, and rectum may also be involved. Behçet’sdisease with intestinal involvement may exhibit similarclinical manifestations to other inflammatory boweldiseases such as Crohn’s disease and ulcerative colitis.2
Here, we describe the use of a discriminatory endoscopicultrasonogram (EUS) in a male patient with Behçet’scolitis.
A 34-year-old man was admitted with right knee arthral-gia, erythema nodosum on the right leg, oral aphthousulceration, and bloody stools. Blood tests revealed a mildleukocytosis, and an elevated erythrocyte sedimentationrate, CRP, and immunoglobulin D level (21mg/dl).A pathergy test was positive and he was found to beHLA-B51-positive. A diagnosis of Behçet’s disease withgastrointestinal involvement was made according to
international criteria for the diagnosis of Behçet’s disease3
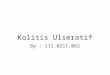
based on the following clinical evidence: (1) recurrent oralulceration; (2) skin lesions (erythema nodosum); (3) posi-tive for pathergy test. Colonoscopy revealed multipleaphthous ulcers in the sigmoid colon (Fig. 1A). An EUS,consisting of an Olympus UM-3R catheter with an operat-ing frequency of 20MHz providing B-mode 360° radial im-aging in a plane perpendicular to the axis of insertion, wasused to examine the same lesions. The EUS revealed thethickened colonic wall and disruption of the normal five-layer wall structure, indicating transmural inflammation(Fig. 1B). The intestinal lesions typical of Crohn’s diseaseare characterized by the presence of longitudinal ulcers witha cobblestone appearance together with noncaseating epi-thelioid granulomas. The intestinal ulceration in our patientlacked the endoscopic characteristics of Crohn’s diseaseulceration. Therefore, in view of the clinical manifestationsand the previously reported histological findings, a diagno-sis of Behcet’s colitis was made.4
EUS is also useful for an assessment of the diseaseseverity. One month after treatment with 5-aminosalicylate(Pentasa 1.5g/day; Nisshin-Kyorin Pharma Co., Tokyo,Japan) was started, the patient’s abdominal symptoms andgenital ulcers improved. A repeat colonoscopy showedresolution of the multiple ulcers (Fig. 1C), and EUS re-vealed an improvement in the swelling and thickness of thecolonic wall, which was almost restored to a normal five-layer structure (Fig. 1D). Since the EUS images demon-strated reduced wall thickness and disruption of the colonicwall structure indicative of an improvement in the underly-ing inflammation, we did not repeat the histological studies.
Gastrointestinal symptoms are common in Behçet’s dis-ease, with ileal ulcers, peritonitis, and gastric ulcers beingthe most common, whilst colitis is rare.5 In contrast to theulcers characteristic of ulcerative colitis, the ulcers inBehçet’s disease are less frequent in the colon and very rarein the rectum (6%).12
Arthritis, uveitis, oral aphthous ulcers, erythemanodosum, and venous thromboembolism are typical clinicalfeatures of Behçet’s disease. However, these symptoms alsooccur in 1%–39% of patients with inflammatory bowel dis-
Letter
Endoscopic ultrasonograms in patients with Behçet’s colitisHiroshi Okamoto · Hironari Shindo · Naoyuki Kamatani
Mod
Rhe
umat
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B W
uerz
burg
on
10/2
9/14
For
pers
onal
use
onl
y.

332
eases such as ulcerative colitis.7 Therefore, it can be difficultto distinguish between Behçet’s disease with ulcerativecolitis-like lesions and ulcerative colitis with BD-likeextraintestinal complications. It has been reported that thecolitis in Behçet’s disease tends to be transmural, whereas itis superficial and mucosal in ulcerative colitis.8 Accordingly,we gave a diagnosis of Behçet’s disease complicated withcolitis.
EUS has evolved into a diagnostic modality that allowsthe visualization of the entire thickness of the bowel wallthrough cross-sectional imaging. As discussed above, EUScan also be used to evaluate the disease activity of thecolitis, thereby limiting the requirement for further histo-logical studies.
In conclusion, EUS is a useful tool for predicting theseverity of histological changes in Behçet’s disease, andcould be used to help distinguish Behçet’s disease fromIBD.
References
1. Kastner DL. Intermittent and periodic arthritic syndromes. In:Koopman WJ, editor. Arthritis and allied conditions. A textbook ofrheumatology. Baltimore: Williams & Wilkins; 1997. p. 1279–306.
2. Yim CW, White RH. Behçet’s syndrome in a family withinflammatory bowel disease. Arch Intern Med 1985;145:1047–50.
3. Criteria for diagnosis of Behçet’s disease. International StudyGroup for Behçet’s Disease. Lancet 1990;335:1078–80.
4. Kobashigawa T, Okamoto H, Kato J, Shindo H, Imamura T, IizukaB, et al. Ulcerative colitis followed by the development of Behçet’sdisease. Intern Med 2004;43:243–7.
5. Sayek I, Aran O, Uzunalimoglu B, Hersek E. Intestinal Behçet’sdisease: surgical experience in seven cases. Hepatogastroenterology1999;165:81–3.
6. Shimizu T, Ehrlich GE, Inaba G, Hayashi K. Behçet’s disease(Behçet’s syndrome). Semin Arthritis Rheum 1979;8:223–60.
7. Kern F Jr. Extraintestinal complications. In: Kirsner JB, ShorterRG, editors. Inflammatory bowel disease. Philadelphia: Lea &Febiger; 1975. p. 127–45.
8. Lew RJ, Ginsberg GG. The role of endoscopic ultrasound ininflammatory bowel disease. Gastrointest Endosc Clin N Am 2002;12:561–71.
A
B
C
D
Fig. 1. Results of colonoscopicstudy and endoscopicultrasonograms of aphthousulcers on the sigmoid colon.A,B Before and C,D aftertreatment
Mod
Rhe
umat
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B W
uerz
burg
on
10/2
9/14
For
pers
onal
use
onl
y.