Embed Size (px)
Citation preview

The Korean Journal of Gastrointestinal Endoscopy ❙Room B❙
152 The Korean Journal of Gastrointestinal Endoscopy
항응고제 및 항혈소판제 복용 환자의 내시경시술을 위한 관리
이 옥 재
경상대학교 의학전문대학원 내과학교실
Anticoagulation and Antiplatelet Therapy for EndoscopyOk-Jae Lee, M.D.
Department of Internal Medicine, Gyeongsang National University School of Medicine, Jinu, Korea
서론
노령인구가 증가함에 따라 심혈관 및 뇌혈관계 혈전색전질
환이나 정맥 혈전색전증과 같이 항응고제를 필요로 하는 질환
이 점점 늘고 있으며, 항응고제 및 항혈소판제의 종류가 다양
해졌을 뿐만 아니라 새로운 약제가 계속 개발 출시되고 있다.
내시경기기 및 기술이 빠르게 발전하면서 진단 및 치료목적의
내시경시술이 많이 시행되면서, 장기적인 항혈전제를 복용하는
중에 내시경시술을 필요로 하는 환자도 점점 증가하고 있다.
이러한 상황에서 항혈전제에 대한 적절한 관리가 임상적으로
매우 중요하다. 그러나 내시경시술 전후의 적절한 항혈전제의
관리는 결코 간단한 문제가 아니며, 이에 대한 근거를 제시할
만한 대규모의 전향적 무작위대조연구가 현실적으로 매우 어렵
기 때문에 근거가 아직 충분하지 않다. 따라서 이에 대한 가이
드라인은 현재까지의 후향적인 연구 결과와 전문가의 의견을 참
고로 하여 수립하는 실정이다.1 결국 항혈전치료를 중단했을 경
우의 혈전색전위험과 내시경 시술에 따른 출혈위험을 비교ㆍ평
가하여 적절한 결정을 해야 한다.
저자는 American Society for Gastrointestinal Endoscopy
(ASGE) 및 British Society of Gastroenterology (BSG)에서 발
표한 가이드라인1-4과 대한소화기내시경학회의 진단5 및 치료6
소화관내시경 길잡이 및 이후의 연구보고들을 검토하여 항혈전
치료제를 복용하는 환자에서 내시경시술을 위한 관리에 대하여
기술하고자 한다.
본론
1. 항혈전제 치료 환자에서 내시경시술 전에 고려할 사항
우선 내시경 시술의 긴급성과 다음의 위험성; (1) 항혈전제
자체로 인한 출혈위험 (2) 항혈전치료 중에 시행할 내시경시술
자체의 출혈위험 (3) 항혈전치료를 중단한 경우의 혈전색전증
의 위험을 고려해야 한다. 내시경을 대신할 다른 검사법(예, 캡
슐내시경이나 방사선 조영술), 경구외 항혈전치료제, 항혈전치
료를 모니터할 검사 등에 대해서도 숙지해야 한다.1
2. 항혈전제의 종류 및 출혈위험
항혈전제는 항응고제와 항혈소판제로 분류하며, 항응고제는
와파린, heparin 및 LMWH (low molecular weight heparin)이
속하고, 항혈소판제에는 아스피린, nonsteroidal anti-inflamma-
tory drugs (NSAIDs), dipyridamole, thienopyridines (eg, clo-
pidrogrel, ticlopidine) 및 glycoprotein IIb/IIIa receptor in-
hibitors 등이 포함된다. 각 항혈전제의 종류와 작용시간 및 항
혈전작용에 대한 역전치료는 Table 1에 요약하였다.1
1) 항응고제
(1) 와파린: 합성 coumarin유도체로 비타민 K epoxide re-
ductase를 억제함으로써 항응고작용을 하며 cytochrome P450
에 의해 대사되는 약제와 약물상호작용을 한다. 반감기는 환자
마다 다르지만 평균 40시간으로 4시간이면 최고혈장농도에 도
달한다. 복용 후 2일부터 항응고효과가 시작되어 5∼7일에 완
전한 항혈전치료 효과에 도달하고, 약제 중단 후 2∼4일이면
정상 응고상태로 회복된다.8 항응고효과는 INR (international
normalized ratio) 2∼3이 적절하고, 1.5 미만이면 출혈위험이
정상인과 유사하다. INR이 4 이상인 환자의 약 81%에서 내시
경 검사로 위장관 출혈병변을 확인할 수 있었으며7 INR 6 이상
은 출혈 위험성이 더욱 높다.8
(2) 헤파린(UFH, unfractionated heparin)과 LMWH: 헤파
린은 가장 흔히 사용하는 경구외 항혈전제로 antithrombin III
의 기능을 활성화시키고 anti-Xa 작용을 증가시켜 항응고효과
를 나타낸다. 즉각적인 항응고효과가 필요할 때 사용하며, 헤파
린의 효과는 APTT (activated partial thromboplastin time)
ratio를 측정하여 모니터하는데 15∼20 U/kg/day 용량으로 시
작하여 APTT가 정상의 2배 가량(1.5∼2.5) 연장되도록 조절한
다.9 헤파린을 사용하는 환자에서 APTT ratio가 3 이상이면 출
혈 위험이 증가한다.4 LMWH은 헤파린과 유사한 항혈전효과를
가지면서 기존의 헤파린에 비해 단백결합이 적어 용량에 따른

항응고제 및 항혈소판제 복용 환자의 내시경시술을 위한 관리이옥재
Vol. 41 (Suppl 2), 2010 (152-165) 153
Table 1. Antithrombotic Drugs: Duration of Action and Routes for Reversal
Drug class Specific agent (s) Duration of action
Test to monitor
Routes for reversal
Elective Urgent
Antiplatelet agents
Anticoagulants
AspirinNSAIDsDipyridamoleThienopyridines (clopidogrel, ticlopidine)GP IIb/IIIa inhibitors (tirofiban, abciximab, eptifibatide)Warfarin
Unfractionated heparinLMWH
10 daysVaries2∼3 days3∼7 days
Varies
3∼5 days
4∼6 h12∼24 h
BT
INR
APTTAPTT
NANA HoldHold
NA
Hold
Hold Hold
Transfuse plateletsTransfuse plateletsTransfuse plateletsTransfuse platelets± desmopressin if overdoseTransfuse platelets; in case of overdose, some agents can be removed with dialysisFFP±vitamin K, consider protamine sulfate*Hold or consider protamine sulfate*Hold or consider protamine sulfate*
BT, bleeding rime; APTT, activated prothrombin time; NA, not applicable; NSAID, nonsteroidal anti-inflammatory drug; GP, glycoprotein; FFP,fresh frozen plasma; LMWH, low molecular weight heparin. *Caution: Can cause severe hypotension and anaphylaxis. Adapted from GastrointestEndosc 2009;70:1060-1070.1
항응고효과를 예측할 수 있으며 헤파린보다 반감기가 길면서
출혈위험이 적다. LMWH는 피하주사가 가능하고, HITT (he-
parin induced thrombocytopenia with thrombosis) 증후군의
발현빈도가 낮으며, 응고시간의 측정 없이 몸무게에 따라 일정
량을 주입하므로 외래에서도 사용할 수 있다.9 헤파린은 중단
후 작용시간이 4∼6시간까지 지속되며, LMWH은 8시간이 경
과하면 항응고작용이 사라진다.10
2) 항혈소판제
(1) 아스피린 및 NSAIDs: 아스피린은 혈소판의 cyclooxyge-
nase (COX)를 비가역적으로 아세틸화하여 혈소판의 thrombo-
xane A2 합성을 억제함으로써 혈소판 응집을 방해한다. 따라서
혈소판의 수명기간인 7∼10일 동안 작용한다.7 건강인에서 아스
피린 복용 후 3일이 경과되면 출혈시간과 혈소판 응집검사가 정
상화된다.11,12 아스피린에 비해 NSAIDs는 가역적으로 COX-1을
억제하며, 내시경시술시 출혈의 위험성을 증가시키지 않는다.13
(2) Adenosine diphosphate (ADP) 수용체 억제제(clo-
pidogrel, ticlopidine): Clopidogrel과 ticlopidine은 thieno-
pyridine 유도체로 ADP가 혈소판막에 존재하는 ADP 수용체에
결합하는 것을 비가역적으로 차단하여 혈소판 응집을 방해한
다.14 투여 3∼5일 후에 항혈소판작용을 나타내며, 투약을 중단
하면 7∼10일 후에 혈소판 기능이 완전히 회복된다. Cytochro-
me P450 체계의 CYP2C19을 통해 활성화되므로 이 효소를 억
제하는 PPI (proton pump inhibitor), 특히 오메프라졸을 병용
하면 clopidogrel의 항혈소판 효과가 감소된다.15,16
Clopidogrel
의 위장관 출혈 위험은 아스피린보다는 낮으며(2.0 vs. 2.7%),17
아스피린과 clopidogrel을 병용할 경우에 출혈위험이 증가한다.7
(3) Adenosine 재흡수 억제제(dipyridamole): Adenosine
의 재흡수를 억제하여 항혈소판작용을 나타내며 아직까지 고위
험 내시경 시술 중의 안전성은 알려지지 않았지만,3 출혈의 위
험성이 아스피린보다 낮으며 아스피린과 병용해도 아스피린의
출혈위험을 증가시키지는 않는 것으로 보이므로,18
표준용량을
사용한다면 내시경 시술을 위해 중단할 필요가 없다.1
(4) Glycoprotein IIb/IIIa 수용체 억제제(abciximab,
eptifibatide, tirofiban): 혈소판 응집의 최종단계인 GP IIb/
IIIa 수용체와 피브리노겐이 결합하는 것을 억제하는 주사제로,
중단 후 약효 지속시간은 abciximab은 24시간, eptifibatide와
tirofiban은 4시간이다. 이 약제들은 중증 출혈의 위험도가 높
아 급성 관상증후군 등의 특수한 경우에만 사용하고 있으며 아
직까지 소개할 만한 연구 결과가 없어 정확한 치료지침이 없
다.3 약제 투여 중 생명을 위협할 정도의 출혈을 보이면 사용을
중단하고 혈소판 혹은 desmopressin를 투여할 것을 권고한다.7
3. 내시경시술의 출혈위험(procedure risks)
내시경시술은 출혈유발 위험도에 따라 고위험시술과 저위험
시술로 분류할 수 있다(Table 2).7 위험도가 낮은 시술은 일반
적으로 출혈위험이 1% 미만인 시술을 지칭하며, 상부 위장관
내시경(0.01∼0.13%),19 소장 내시경(0.1%),19,20 대장내시경(0
∼0.02%),21,22 등의 점막 생검을 포함한 모든 진단 내시경 검사
와, ERCP 및 조임근절개술(sphincterotomy)을 시행하지 않는
담/췌관 스텐트 삽입술(0.26%),23 세침흡인을 시행하지 않는 내
시경초음파와 캡슐내시경을 포함한다.
위험도가 높은 시술은 입원치료, 수혈, 내시경적 지혈술 또
는 수술을 필요로 하는 정도의 출혈을 일으킬 위험이 1% 이상
으로 알려진 시술을 말하며, 폴립절제술(0.7∼10.3%),21,24-27 내
시경점막절제술(22%),28
조임근절개술(2.0∼3.2%),29,30
풍선/부
우지 확장술(1.7%),31 식도 스텐트삽입술(0.5∼5.3%),32-34 PEG

항응고제 및 항혈소판제 복용 환자의 내시경시술을 위한 관리이옥재
154 The Korean Journal of Gastrointestinal Endoscopy
Table 2. Procedure Risk for Bleeding
Procedure Risk of bleeding
Low risk of bleeding (<1%) Diagnostic endoscopy with or without biopsy EGD Double balloon enteroscopy Colonoscopy ERCP, Biliary/pancreatic stent without sphincterotomy Endosonography without FNA Wireless capsule endoscopyHigh risk of bleeding (≥1%) Polypectomy Gastric Duodenal/ampullary 1∼3 cm >3 cm Colonic Endoscopic mucosal resection Biliary sphincterotomy Pneumatic/balloon dilation in achalasia Esophageal stenting PEG placement Endosonography with FNA Laser ablation and coagulation Variceal sclerotherapy Variceal band ligation Thermal ablation and coagulation
0.01∼0.13%19
0.1%19,20
0∼0.02%21,22
0.26%23
−*−*
7.2%24
4.5%25
10.3%25
0.7∼3.3%21,26,27
22%†,28
2.0∼3.2%29,30
1.7%‡,31
0.5∼5.3%32-34
2.5%35
1.3∼6%§,36-38
1.1%39
4∼25.4 %40,41
2.4∼5.7%∥41,42
5%2
EGD, esophagogastroduodenoscopy; FNA, fine-needle aspiration; PEG, percutaneous endoscopic gastrostomy; *Limited data, presumed negligible;†Majority of bleeding in lesions >2 cm; ‡Minor bleeding is reported commonly with balloon and bougie dilators43; §Negligible for solid lesions;∥Less ulceration in band ligation. Adapted from Am J Gastroenterol 2009;104:3085-3097.7
(2.5%),35
내시경 초음파 및 세침흡인술(1.3∼6%)36-38
및 위장
관출혈에 대한 지혈술(1.1∼25.4%)2,39-42 등의 치료목적의 시술
이 속한다.
환자 측의 요인도 시술 후의 출혈에 영향을 줄 수 있으며 연
령,44,45 담관염, 혈액응고장애, 혈액투석 등29,46이 고위험 내시경
시술 후 출혈위험을 높인다. 아직 데이터는 부족하지만 신부전,
간경변증, 선천성/후천성 혈액응고 장애 및 혈소판 감소증도
고위험 내시경시술 중에 출혈 위험을 높일 수 있다.7
기타 시술관련 출혈위험도와 관련하는 요인으로 내시경시술
자의 경험정도와 병변의 크기, 형태 및 폴립의 위치와 같은 병
변 자체관련요인, 그리고 폴립절제술에 사용하는 기술적인 측
면(diathermy 열치료, endoloop 설치, 주입 등)을 들 수 있다.
시술에 따라서 식도확장술이나 스텐트 삽입술과 내시경초음파
하 세침흡인술에 의해 장기밖에 혈종이 생기는 경우와 같이 내
시경이 도달하기 어려운 부위의 출혈을 일으켜 수술을 필요로
함으로써 이환율을 증가시킬 수도 있다.7
4. 혈전색전증의 위험(condition risks)
내시경시술을 위해 항혈전치료를 중단할 경우에 혈전색전증
의 발생 가능성은 환자가 항혈전 치료를 필요로 했던 기저질환
과 관련하며, 혈전색전증의 위험도에 따라서 저위험군과 고위
험군으로 분류한다(Table 3).1,7
저위험군은 심부정맥혈전증(DVT), 판막질환과 무관한 만성
또는 발작성 심방세동, 생체인공판막(bioprosthetic valve), 인
공 대동맥판막치환술을 한 경우가 속하고, 고위험군은 심장판
막질환 환자, 인공판막치환술을 받은 환자, CHADS2 점수가 3
이상인 환자에서 동반된 심방세동 환자, 인공승모판막치환술을
받은 환자, 인공판막치환술의 위치와 무관하게 이전에 혈전색
전증의 병력이 있는 환자, 관상동맥 스텐트(특히 drug-eluting
stent, DES)삽입 환자가 포함되며 특히 최소 권장기간 이전에
dual antiplatelet therapy (DAT)를 중단한 경우에는 스텐트 혈
전의 위험이 높다.1-4,7
American Heart Association (AHA)의 지
침은 DES 삽입 후 12개월간 DAT를 지속할 것을 권장하고 있
다.47 CHADS2 점수는 Congestive heart failure, Hypertension,
Age>75, Diabetes mellitus, history of Stroke or transient
ischemic attack (TIA)의 머리글자에서 유래한 용어로 판막질환
과 무관한 심방세동환자에서 색전위험을 정하는 분류방법으로
가장 널리 사용하는 방법이다.48
심부전증, 고혈압, 나이 75세

항응고제 및 항혈소판제 복용 환자의 내시경시술을 위한 관리이옥재
Vol. 41 (Suppl 2), 2010 (152-165) 155
Table 3. Condition Risk for Thromboembolic Event
Higher-risk condition Low-risk condition
Atrial fibrillation
Mechanical valve
Coronary disease and stents
DVT/PE
Associated valvular heart disease, Prosthetic valves, Active congestive heart failure, Left ventricular ejection fraction<35%, A history of a thromboembolic event, Hypertension, Diabetes mellitus, Age ≥75 yrDiscontinuing antiplatelet/anticoagulant in bioprosthetic valve <3 monthsMechanical valve in mitral positionAny position with previous thromboembolic eventRecent acute coronary event <4∼6 wksRecently (<1 yr) placed coronary stentNonstented percutaneous coronary intervention after myocardial infarctionDiscontinuing dual antiplatelet therapy in: Drug-eluting stent <1 year Bare metal stent <1 monthDiscontinuing anticoagulation in event <3 monthsRecurrent DVT/PESevere hypercoagulable states: active cancer, paroxysmal nocturnal hemoglobinuria, myeloproliferative syndromes
Uncomplicated or paroxysmal nonvalvular atrial fibrillation
Bioprosthetic valveMechanical valve in the aortic position
Deep vein thrombosis
DVT, deep venous thrombosis; PE, pulmonary embolism. Adapted from Gastrointest Endosc 2009;70:1060-10701 and Am J Gastroenterol 2009;104:3085-3097.7
이상, 당뇨의 점수를 각각 1점으로 산정하고, 혈전색전증의 병
력을 2점으로 계산하여 0점에서 6점까지 분류하여 높을수록 혈
전색전증의 발생위험이 높다.
5. 항혈전치료제 복용 환자의 계획된 내시경시술
1) 항혈전치료 중 내시경시술에 의한 출혈위험
(1) 진단 내시경: 아스피린은 복용 후 48시간까지 출혈시간
(bleeding time, BT)을 연장시키지만,49 아스피린이나 clopidog-
rel 투여 중에 조직생검을 포함한 진단내시경 검사로 인해 출혈
빈도가 증가하였다고 입증한 임상보고는 없었다. 와파린도 출
혈위험이 낮은 시술을 하는 경우에는 내시경시술 전후에 중단
하지 않고 지속해도 출혈위험도가 낮았다.50
대장내시경 선별검사의 경우에는 저위험군이라도 와파린을
일시 중단하고 시행하여 폴립절제술까지 시행하는 것이 가장
비용-효율적이다.51 또는 와파린을 그대로 사용하면서 검사를
시행하고 폴립절제술이 필요한 크기의 폴립이 있는 경우에 나
중에 와파린을 중단하고 시술을 다시 시행해야 한다. 고위험군
도 폴립절제술의 가능성을 염두에 두어 와파린을 중단하고
bridge therapy를 하면서 검사를 시행하며, 폴립크기가 작고,
INR이 <2.5이며 내시경시술자가 폴립절제술후 출혈을 충분히
관리할 수 있으면 절제술을 시행한다.7
(2) 대장 폴립절제술: 아스피린/NSAIDs은 복용하는 중에 폴
립절제술을 해도 출혈의 증가는 없거나 1% 미만이었으며,13,52
와파린은 데이터가 제한적이지만 복용 중에 폴립절제술을 시행
하거나 폴립절제술 후 1주 이내에 와파린이나 헤파린의 투여를
재개한 경우에 출혈위험은 증가하였다.53 항혈전제 복용 환자
31명에서 1 cm 미만의 폴립을 절제한 후 예방적 헤모클립을
시행했을 때 출혈률이 0∼3.3%로 낮았다는 보고54-56
가 있었으
나, 아직 무작위 대조연구가 없어서 확실한 임상 데이터가 부
족하고 비용으로 인해 현재로서는 예방적 헤모클립이나 분리형
올가미의 일괄적인 사용은 권장하지 않는다.1
(3) Sphincterotomy 및 PEG: 아스피린이나 NSAID는 조임
근절개술을 시행하기 7일 전부터 중단해도 출혈 위험을 줄이지
못한다.57
그러나 와파린이나 시술 후 3일 이내 헤파린 정맥투
여는 조임근절개술 후 출혈위험을 증가시켰다.58 항혈전치료 중
인 환자에서 PEG의 출혈위험은 알려진 정보가 없다.
2) 계획된 내시경 시술 전 항혈전제 중단의 위험: DVT와 같
이 항혈전 치료가 일시적인 경우에는 가능하면 항응고치료가
더 이상 필요하지 않을 때까지 계획된 내시경 시술을 연기한
다. 특히 최근에 관상동맥 스텐트 삽입을 받은 환자에서는 스
텐트 폐쇄로 인하여 급성 관상동맥 증후군 및 사망까지 이어질
수 있으므로 시술을 연기해야 한다.59-61 만일 항혈전 치료중인
환자에게 내시경 시술을 하기로 결정했다면 항혈전제의 중단이
나 역전치료 여부를 환자 개개인에 따라 차별화해야 한다. 시
술을 위해 역전치료로써 비타민 K를 투여하는 것은 항응고제
투여를 재개했을 때 치료효과를 지연시키기 때문에 피해야 한
다.626262 2006 AHA/American College of Cardiology (ACC) 가이
드라인은 혈전위험이 낮은 환자(Table 3)에서는 시술 전에 와

항응고제 및 항혈소판제 복용 환자의 내시경시술을 위한 관리이옥재
156 The Korean Journal of Gastrointestinal Endoscopy
Table 4. Periprocedural Management of Warfarin for Patients with Atrial Fibrillation or Valvular Heart Disease Undergoing ElectiveEndoscopy
Condition Associated diagnosis Management
Atrial fibrillation
Valvular heart disease
None
Mechanical valve(s) and/or history of cerebrovascular accident, transient ischemic attack, or systemic embolism
Mechanical bileaflet, aortic valve
Mechanical mitral valve or mechanical aortic valve plus any of the following: atrial fibrillation, previous thromboembolic event, left ventricular dysfunction, hypercoagulable condition, mechanical tricuspid valve or >1 mechanical valve
Hold warfarin 3∼5 days before procedure. Restart warfarin within 24 h.*Hold warfarin and start UFH when INR ≤2.0. Stop UFH 4∼6 h before procedure and restart after procedure. Resume warfarin on the evening of the procedure and continue both agents until INR is therapeutic.* Therapeutic doses of SQ UFH or LMWH may be considered in lieu of IV UFH.Hold warfarin 48∼72 h before procedure for a target INR <1.5. Restart warfarin within 24 h.*Hold warfarin and start UFH when INR ≤2.0. Stop UFH 4∼6 h before procedure and restart after procedure. Resume warfarin on the evening of the procedure and continue both agents until INR is therapeutic.* Therapeutic doses of SQ UFH or LMWH may be considered in lieu of IV UFH.
UFH, unfractionated heparin; INR, international normalized ratio; SQ, subcutaneous; LMWH, low molecular weight heparin; *Continuation or reinitiation of anticoagulation should be adjusted according to the stability of the patient and estimated risks surrounding the specific intervention/procedure performed. This table was adapted from the following guidelines: 2006 Guidelines for the Management of Patients with Atrial Fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the EuropeanSociety of Cardiology Committee for Practice Guidelines66 and American College of Cardiology/American Heart Association 2006 guidelines forthe management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Forceon Practice Guidelines.67
파린을 그냥 중단하고 헤파린 bridge therapy는 일반적으로 필
요하지 않다고 권고하고 있다. 항응고제를 4∼7일간 중단한 환
자에서 색전증의 절대적인 위험은 약 1%이다.63,64 최근에 1,024
명을 대상으로 대장내시경, 안과수술, 구강수술 등의 계획된 시
술을 위하여 와파린을 중단한 1,293건에 대해 조사한 대규모의
전향적 다기관 연구63가 보고되었다. 와파린 중단 기간은 다양
했지만 80% 이상이 응고제를 5일 미만 중단하였고 8.3%에서만
헤파린/LMWH bridge therapy를 받았다. 시술 관련 출혈을 보
인 환자의 61%가 헤파린 bridge therapy를 받았으며, 연구대상
가운데 0.7%인 7명만이 시술 후 30일 이내에 혈전색전증을 경
험했으며 7명 모두 bridge therapy를 받지 않았다고 보고하면서
장기적인 항응고요법을 하고 있는 환자가 가벼운 외래 시술을
시행하는 경우에 5일 이하의 와파린 중단은 혈전색전증의 위험
을 높이지 않는다고 하였다. 따라서 가벼운 시술을 할 경우에는
bridge therapy를 결정하기에 앞서 출혈 위험과 혈전색전의 위
험을 비교 평가하여 환자에 따라 차별화할 필요가 있다.
3) 내시경시술을 위한 bridge therapy의 역할: 와파린을 사
용하는 혈전색전증 고위험 환자는 내시경 시술을 전후하여 작
용시간이 짧은 UFH (unfractionated heparin)나 LMWH으로
bridge therapy를 할 수 있다. Bridge therapy에 대한 증거는
제한적이지만, LMWH으로 bridge therapy를 하면서 내시경 시
술을 받은 98명의 환자에서 혈전색전증은 발생하지 않았으며,
의미있는 출혈도 오직 2예에서만 발생했는데 내시경이나 치료
와는 무관한 출혈이었다.65 심방세동/심장판막질환 환자에서 계
획된 침습적 시술시의 항응고제의 관리에 대한 AHA/ACC 가이
드라인을 Table 4에 요약하였다.66-68
4) 계획된 내시경시술 후 항혈전제의 투여재개: 내시경 시술
을 마친 후 항혈전치료제 투여를 재개하는 적절한 시기에 대한
컨센서스는 아직 없다. 혈전색전증의 예방을 위해 항혈전제 투
여를 즉시 재개함으로써 얻는 이점과 이로 인한 출혈위험을 비
교ㆍ평가해야 하고, 시술에 자체에 의한 출혈위험을 고려하여
결정해야 할 것이다.1
AHA/ACC 가이드라인은 심장판막질환이 있지만 혈전색전증
의 위험이 낮은 환자에서는 시술 24시간 내에 와파린 투여를
재개하고 혈전색전증의 위험이 높은 환자에서는 출혈이 안정되
는대로 최대한 빨리 UFH나 LMWH 투여를 재개하고 INR이 적
절한 치료수준에 도달할 때까지 지속해야 한다고 권고하였다.
치료목적의 시술을 마친 후 UFH는 2∼6시간 후에 재투여하며

항응고제 및 항혈소판제 복용 환자의 내시경시술을 위한 관리이옥재
Vol. 41 (Suppl 2), 2010 (152-165) 157
LMWH의 적절한 투여재개 시기는 알려져 있지 않다.1
6. 항혈전제치료 중에 급성 출혈이 발생한 환자에서의 응급
내시경시술
1) 항혈전치료 환자의 급성 위장관 출혈: 장기간의 항응고제
복용의 부작용으로 발생하는 출혈 가운데 위장관 출혈이 가장
흔해서69 와파린을 복용하는 환자의 약 5%에서 급성 위장관출
혈이 발생한다.70 이와 같은 경우에는 항응고제의 중단에 의한
혈전색전증의 위험과 항응고제 유지로 인한 심각한 출혈위험이
공존하고, 한편으로 항응고치료에 대한 적극적인 역전치료
(reversal)의 여부와 중단 후 투여재개의 시기를 결정해야 하는
문제로 치료는 매우 복잡하고 어려워진다.
2) 급성 위장관출혈 환자에서 항응고치료 중단의 위험성: 급
성 위장관 출혈상황에서 항응고제 중단의 위험에 대해 알려진
것이 많지 않으며, 급성 위장관출혈로 인하여 와파린을 4∼15
일 중단했을 때 혈전색전증은 없거나 매우 낮았다.71,72
3) 급성 출혈 환자에서 항혈전제를 어떻게 할 것인
가?(Stopping or reversing antithrombotic agents in the
acutely bleeding patient): 항혈전제의 중단, 감량, 역전치
료 여부의 결정은 이로 인한 혈전색전증 발생위험과 항혈전제
를 유지함으로써 계속될 출혈위험을 비교ㆍ평가해서 환자별로
차별화하여 판단해야 한다. 생명을 위협할 정도의 심각한 출혈
의 경우라면 항응고치료의 위험이 혈전색전증의 위험을 능가하
므로 약제의 중단과 함께 즉시 적극적인 역전치료를 해야 하고
(Table 1),7 출혈이 적절하게 조절된 것을 확인할 때까지 투여
를 재개하지 말아야 한다. 그러나 대부분의 경우 위험도를 명
확하게 판단하기가 어려우므로 항응고제를 처방한 심장전문의
나 혈액전문의와의 긴밀한 협진을 통해 환자 개개인의 상황에
맞는 처치를 해야 한다.
American College of Chest Physicians의 지침에 따르면, 생
명을 위협할 정도의 심각한 출혈환자에서는 와파린은 중단하고
비타민 K 10 mg을 천천히 정주하고 FFP, 프로트롬빈 복합농축
제제, 재조합응고인자 VIIa를 투여를 고려하도록 권고하였다.73
그러나 AHA/ACC 지침에서 인공판막을 가진 환자에서는 루틴
으로 고용량 비타민 K (10 mg)을 투여할 경우 과다응고상태를
초래할 위험이 있으므로 피해야 한다고 하였다.74 고용량 비타
민 K보다는 FFP가 더 적절하며 저용량의 비타민 K (1∼2 mg)
을 단독으로 또는 FFP와 함께 투여하는 것이 적절하다.
항혈소판제의 경우는 사용 중인 환자가 심각한 생명을 위협
하는 출혈을 할 경우 약제를 중단하거나 약제 중단과 함께 혈
소판을 수혈할 수 있다.1 그러나 clopidogrel을 복용하는 고위
험 환자에서는 중단하기 전에 심장전문의와 협의하여야한다.
만일 clopidogrel을 중단할 필요가 있는 상황이라면 중단기간
을 최대한 5일로 제한해야 한다. 항혈전제를 지속하거나 최소
기간만 중단하면서 조기에 내시경시술을 시행하여 지혈하는 것
을 최우선 목표로 해야 한다.4
4) 급성 위장관 출혈을 동반한 항혈전제 복용 환자에서 내시
경 치료의 유효성(Efficacy of endoscopic therapy in
patients actively taking antithrombotic agents): INR이
치료범위를 벗어나는(≥4) 환자를 대상으로 위장관 출혈을 조
사하였을 때 약 81%에서 내시경 검사상 병변을 확인할 수 있
으므로75 위장관출혈 증상을 보이는 모든 환자에서 내시경 검
사를 시행해야 한다. 다행히도 항응고치료 환자에서 가장 흔한
출혈부위는 내시경치료가 가능한 범위 내에 있으며 상부위장관
에서는 소화성 궤양이 이러한 환자들의 약 절반정도를 차지하
고,69,70,76,77 하부위장관에서는 게실출혈이다.78,79 따라서 항혈전
제 복용 중에 위장관출혈이 발생한 환자에서 내시경 검사와 치
료는 타당할 뿐만 아니라 안전하다.70
이와 같은 상황에서 안전하고 성공적인 내시경 치료를 위해
어느 정도의 INR 값이 필요한가는 아직 전향적 연구데이터가
없지만, INR을 1.5∼2.5 또는 1.3∼2.7로 교정하면 항응고제
치료를 받지 않는 일반 환자와 마찬가지로 내시경 진단과 여러
가지 지혈술을 성공적으로 시행할 수 있다.69,80 내시경 지혈술
후 즉각적인 항응고제 투여가 필요한 고위험 환자에서는 연구
보고는 없지만 헤모클립과 같은 기계적인 지혈술이 더 유용할
수 있다.1
5) 내시경 지혈술 후 항혈전제 투여의 재개: 대부분의 환자
에서 지혈 후에 항혈전제의 투여재개가 필요하지만, 투여재개
의 시기에 대한 데이터는 부족하다. 항혈전제 투여재개의 여부
도 심장전문의나 혈액전문의와의 긴밀한 협진을 통해 환자 개
인별로 차별화해야 한다. 일반적으로 혈전색전 위험이 재출혈
위험을 능가하는 경우에 투여재개를 고려해야 하며 출혈부위의
적절한 지혈이 이루어진 경우에 고려하게 된다. 항응고제의 시
급한 투여재개가 요구되는 고위험 환자에서는 와파린 투여재개
전에 비교적 작용시간이 짧은 UFH 정주로 bridge therapy를
하면 재출혈 시에 즉시 중단하거나 역전치료가 가능하기 때문
에 LMWH보다 장점이 있다. LMWHs는 UFH보다 반감기가 길
고 protamine sulfate에 의한 역전치료효과가 적다.1,7
아스피린과 관련된 궤양출혈 환자에서는 재출혈을 막기 위
해 clopidogrel으로 전환하는 것보다는 아스피린과 PPI를 병용
하는 것이 더 유용하다.81,82 급성 위장관출혈 환자에서 지혈술
후 아스피린을 30일간 중단한 경우와 3∼5일에 투여를 재개한
경우를 비교하였을 때, 재출혈률은 11% vs. 19%로 낮았으나 2
개월 후 사망률은 14.5% vs. 1.7%로 더 높았다.83 다른 항혈소
판제는 투여재개의 시기에 대한 데이터는 아직 없다.
7. DAT 중인 혈관스텐트/급성 관상동맥증후군 환자의 내시
경시술
1) Elective endoscopy (계획된 내시경시술): 혈관스텐트,
급성관상동맥 증후군, 뇌혈관 질환 환자에서 아스피린과 clo-

항응고제 및 항혈소판제 복용 환자의 내시경시술을 위한 관리이옥재
158 The Korean Journal of Gastrointestinal Endoscopy
pidogrel 병용과 같은 DAT가 임상에서 점점 늘고 있다. ACC/
AHA 지침에 따르면 금속스텐트 삽입 후 최소한 1개월의 DAT
가, DES 삽입 후나 경피 관상동맥중재술을 받은 환자에서는 출
혈위험이 높지 않으면 12개월의 DAT가 이상적이다.60,84
한 종류의 항혈전제 복용에 비해 DAT는 상부 위장관 출혈
위험을 3배 증가시킨다.85 이와 같은 출혈위험에도 불구하고,
특히 DES 환자에서 DAT의 조기중단은 스텐트 혈전의 발생률
을 높이므로 가능하면 이 약제들을 중단하지 말아야 한다.86 따
라서 지금까지의 증거로 볼 때, DAT 치료 환자에서는 모든 계
획된 고위험 시술은 환자가 ACC/AHA 지침에서 권고하는 최소
의 치료기간을 완료할 때까지 연기해야 한다.84 일단 최소 치료
기간이 경과하면 환자 및 관련된 자문의사와 논의하여 위험도
와 얻을 수 있는 이점을 비교평가한 후에 시술의 진행여부를
결정해야 한다. 2가지 항혈전제 중 어느 약제를 중단했을 때
내시경시술로 인한 출혈위험이 낮은지 비교한 연구는 없다. 다
만, clopidogrel과 아스피린의 혈전색전증 위험의 감소효과를
비교한 무작위 전향적연구에서 clopidogrel이 아스피린보다 허
혈성 stroke, 심근경색 및 혈관질환으로 인한 사망의 위험을 줄
이는데 유효했다.17 그러나 현재까지 clopidogrel을 복용 중인
경우보다는 아스피린을 복용하는 중에 폴립절제술의 안전성을
보고한 데이터가 훨씬 많다.13,52,53 따라서, 일반적으로 항혈전제
2가지 중 clopidogrel을 중단하고 aspirin을 유지하면서 내시경
을 시행한다.1-4,7
2) 급성 관상동맥증후군(ACS) 또는 최근에 혈관스텐트를
삽입한 환자에서의 응급 내시경: 많은 ACS 및 최근 혈관 스텐
트 삽입 환자가 혈소판 glycoprotein IIb/IIIa 수용체 길항제를
포함하여 여러 가지 약제를 동시에 사용하고 있으며, ACS 환자
의 1∼3%에서 첫 입원 중에 위장관 출혈이 발생한다.86-89 ACS
상황 중에 위장관 출혈이 발생한 환자는 위장관 출혈이 없는
ACS환자에 비해 입원 중 사망률이 4∼7배 증가한다.87,88 이러
한 상황에서 임상의는 시술로 인한 합병증의 위험이 높은 환자
에게 내시경 검사를 진행해야 하는가 하는 딜레마에 빠지게 된
다.90,91 급성 심장발작이 일어난 당일에 내시경을 받은 환자에
서 시술 합병증은 12%로 높지만,91 심근경색후 상부 위장관내
시경의 전체 합병증 빈도는 약 1∼2%이며90 대장내시경의 합병
증 빈도는 1%이다.91 급성 심근경색증 발작 후 30일 이내에 내
시경 검사를 받은 200명에 대한 후향적 조사에서 위염, 위궤양,
십이지장 궤양, Mallory-Weiss 열상 등의 다양한 병변이 발견되
었다.90 이와 같이 급성 위장관출혈 자체가 급성 심근경색증을
유발할 수도 있으므로, 이러한 환자에서 내시경 검사는 유용하
다. 또 한 위장관출혈 후에 급성 심근경색이 발생한 환자가 급
성심근경색증 치료 후에 위장관출혈을 보인 환자보다 내시경
치료를 더 필요로 하였다고 한다.89
ACS 환자나 최근에 혈관 스텐트를 삽입 환자에서 DAT 및
glycoprotein IIb/IIIa 억제제를 포함한 항혈전제의 복용 중에도
내시경 검사는 안전하지만, 이에 대한 정보는 새로운 경험과
지식이 축적됨에 따라 지속적으로 발전하고 변화하고 있어서,
약제 중단 여부에 대한 강력한 지침을 정하기는 매우 어렵다.
따라서 약제를 중단하기 전에 심장전문의, 신경과 전문의 등과
의 협의가 필요하다.
요약
1. Recommendations
다음의 권고안은 the strength of the supporting evidence
(Table 5)92를 기초로 작성한 2009년 ASGE 지침의 권장사항1과
2008년 BSG의 가이드라인4을 요약한 것이다. 약한 권고사항은
‘suggest’로 표기하였고, 강력하게 권고할 내용은 ‘recommend’
로 표기하였다.
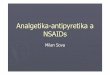
1) Elective procedures (Fig. 1, Table 6)
(1) 일시적인 항응고제 치료를 받는 환자(예, DVT로 와파린
을 복용하는 환자): 계획된 내시경 시술은 항혈전치료를 완료할
때까지 연기한다(suggest). ⊕⊕○○
(2) 아스피린 및/또는 NSAIDs: 모든 내시경 시술에도 지속한
다(recommend). ⊕⊕○○
고위험 시술 예정인 경우에는 환자의 항혈소판제 적응증인
기저질환에 따라서 시술전 5∼7일간 아스피린 &/or NSAIDs의
중지를 고려할 수 있다.
(3) 최근 혈관스텐트 삽입했거나 ACS환자(DAT)
① 계획된 내시경 시술을 적절한 전문기관의 현재 지침에서
권장하는 항혈전제의 최소투여기간(금속스텐트 삽입 후 최소한
1개월, DES 삽입 후나 경피 관상동맥중재술 후 12개월)을 완료
할 때까지 연기한다(recommend).
② 최소투여기간을 경과하면 clopidogrel이나 ticlopidine을
시술 전 약 7∼10일간 중지하고 아스피린은 지속한다(suggest).
③ 아스피린을 복용하지 않는 환자는 내시경 시술 전후에
clopidogrel을 중단하는 동안 아스피린을 복용하면 혈전색전증
의 위험을 감소시킬 수 있다.
④ Clopidogrel이나 ticlopidine은 환자의 상태와 내시경 시
술을 고려하여 시술 후 곧 투여를 재개할 수 있다. 환자의 심
장전문의나 다른 적절한 전문가와 협의하여 적절한 치료를 결
정한다. ⊕⊕⊕○
(4) Clopidogrel과 ticlopidine을 3의 적응증 외에 사용한
경우
① 저위험 내시경시술: 중단하지 않고 유지한다(suggest).
② 고위험 내시경시술: 시술하기 약 7∼10일전에 중단한다
(suggest).
㉠ 환자가 아스피린을 복용하면 아스피린은 지속한다.
㉡ 아스피린을 사용하지 않는 환자는 내시경 시술 전후에
clopidogrel을 중단하는 동안 아스피린을 복용하면 혈

항응고제 및 항혈소판제 복용 환자의 내시경시술을 위한 관리이옥재
Vol. 41 (Suppl 2), 2010 (152-165) 159
Figure 1. Management of antith-rombotic agents in the elective endoscopic se-tting. Adapted from Ga-strointest Endosc 2009; 70:1060-1070.1
Figure 2. Management of antith-rombotic agents in the urgent endoscopic set-ting. Adapted from Ga-strointest Endosc 2009; 70:1060-1070.1
Table 5. GRADE System for Rating the Quality of Evidence for Guidelines
Quality of evidence Definition Symbol
High qualityModerate quality
Low quality
Very low quality
Further research is very unlikely to change our confidence in the estimate of effectFurther research is likely to have an important impact on our confidence in the estimate of effect and may change the estimateFurther research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimateAny estimate of effect is very uncertain
⊕⊕⊕⊕⊕⊕⊕○
⊕⊕○○
⊕○○○
Weaker recommendations are indicated by phrases such as "we suggest", whereas stronger recommendations are typically stated as "we recommend". Adapted from BMJ 2008;336:924-926.92

항응고제 및 항혈소판제 복용 환자의 내시경시술을 위한 관리이옥재
160 The Korean Journal of Gastrointestinal Endoscopy
Table 6. Management of Anticoagulant and Antiplatelet Agents for Endoscopic Procedures
Low-risk condition High-risk condition
Elective endoscopy Postpone endoscopy for patients on temporary anticoagulation therapy (eg, warfarin for DVT)
Low-risk procedure Aspirin/NSAIDs Continue aspirin/NSAIDs Warfarin Continue warfarin
Check INR 1 week before endoscopyIf INR within therapeutic range, continue usual daily doseIf INR above therapeutic range but <5, reduce daily warfarin dose until INR returns to therapeutic range.If INR ≥5, postpone endoscopy & contact reasonable consultant
Clopidogrel Continue clopidogrelHigh-risk procedure Aspirin/NSAIDs Continue or stop for 5∼7 days Continue aspirin/NSAIDs Warfarin Stop warfarin 5 days before endoscopy
Check INR prior to procedure to ensure <1.5Restart warfarin evening of procedure with usual daily doseCheck INR 1 week later to ensure adequate anticoagulation
Stop warfarin 5 days before procedure & Bridge therapyStart LMWH 2 days after stopping warfarinOmit LMWH on day of the procedureRestart warfarin evening of procedure with usual daily doseRestart LMWH 1 day after procedureContinue LMWH until INR adequate
Clopidogrel Stop clopidogrel 7 days before endoscopyContinue aspirin if already prescribed
If not on aspirin, then consider aspirin therapy while clopidogrel discontinued
Discuss with cardiologistStop clopidogrel 7 days before endoscopy if; >12 months after insertion of DES>1 month after insertion of bare metal coronary stentContinue or prescribe aspirinRestart clopidogrel on day following the procedure
Urgent endoscopy;Acute GI bleeding Warfarin Stop warfarin until hemostasis is achieved
FFP, prothrombin complexconcentrate, and/or vitamin K should be individualizedProtamine reserved for life-threatening bleedingon heparin because of anaphylaxis and severe hypotension risk
Consult cardiologist if; recently (<1 year) placed vascular stent &/or ACS before stopping warfarinStop warfarin for life-threatening bleedingCorrect anticoagulation if supratherapeutic INRAfter hemostasis, timing for resumption of anticoagulation individualizedIf high-risk stigmata for rebleeding (eg, visible vessel) then use IV UFH
Clopidogrel/ticlopidine Stop antiplatelet until hemostasis is achievedTransfuse platelets for life-threatening or serious bleeding
Consult cardiologist if; recently (<1 year) placed vascular stent &/or ACS before stopping antiplatelet agent
NSAIDs, nonsteroidal antiinflammatory durgs; INR, international normalized ratio; LMWH, low molecular weight heparin; DES, drug eluting stent;ACS, acute coronary syndrome; UFH, unfractionated heparin. Adapted from Gastrointest Endosc 2009;70:1060-10701 and Gut 2008;57:1322-1329.4
전색전증의 위험을 줄일 수 있다.
㉢ Clopidogrel이나 ticlopidine은 환자의 상태와 내시경
시에 시행하는 치료를 고려하여 시술 후 곧 투여를 재
개할 수 있다. ⊕⊕○○
㉣ Clopidogrel을 중단기간에 계획된 내시경 시술을 시행
하지 못하고 기간을 넘기게 되면 clopidogrel을 다시
투여하고 시술날짜를 다시 잡을 것을 고려해야 한다.
㉤ Clopidogrel: 환자의 주치 심장전문의와 협의한 후에만

항응고제 및 항혈소판제 복용 환자의 내시경시술을 위한 관리이옥재
Vol. 41 (Suppl 2), 2010 (152-165) 161
clopidogrel의 중단을 고려해야 한다. 또한 내시경 시술
담당의는 내시경 수술이 필수적인가를 확인해야 한다.
(5) 항응고제 복용환자
① 저위험 내시경시술: 항응고제를 중단하지 않고 지속한다
(suggest).⊕⊕○○
㉠ 와파린을 사용하는 환자는 INR을 검사하여 치료범위
를 초과하지 않도록 한다.
㉡ 환자가 와파린을 유지하도록 하고 내시경 시술 1주일
전에 INR을 검사한다.
㉢ NR이 치료범위 이내라면 현재 사용용량을 유지한다.
㉣ INR이 치료범위를 넘고 <5이면 치료범위 이내로 회
복하도록 와파린 일일복용량을 감량한다.
㉤ INR ≥5 이상이면 내시경 시술을 연기하고 담당 심장
전문의나 항응고제 처방의와 협의해야 한다.
② 고위험 내시경시술, 저위험 환자; 와파린 등의 항응고제
는 일시 중단한다(suggest).
㉠ 내시경 시술 5일 전에 와파린을 중단한다.
㉡ 내시경 시술 전에 INR을 검사하여 <1.5를 확인한다.
㉢ 내시경 시술 당일 밤에 와파린 평소 용량의 투여를 재
개한다(bridge therapy필요가 없다)
㉣ 시술 1주 후에 INR을 검사하여 적절한 항응고 효과를
유지한다.
③ 고위험 내시경시술, 고위험환자: 와파린은 일시 중단하
고, brdige therapy의 적응이 되면 LMWH이나 UFH으로 brid-
ge therapy로 전환한다(suggest). ⊕⊕○○
㉠ 와파린을 시술 5일 전에 중단해야 한다.
㉡ 와파린 중단 2일 후 LMWH 치료용량을 시작한다.
㉢ 시술 당일에는 LMWH를 생략한다.
㉣ 시술 시행한 당일 밤에 와파린 투여 재개가 권장된다.
㉤ 시술 1일 후에 LMWH 치료용량을 재개한다.
㉥ INR이 치료범위에 도달할 때까지 LMWH를 지속한다.
항응고제를 복용하지 않는 환자와 비슷한 정도로 시술 후 출
혈위험이 있음을 환자에게 고지하여야 한다.
⑥ 항응고제 복용환자에서 폴립절제술 후 기계적 클립의 예
방적 사용에 대한 근거는 아직 충분하지 않다. ⊕⊕○○
⑦ 내시경 중재술 후에 적절한 항응고제 치료의 재개시기:
아직 콘센서스가 없으며, 시술에 따른 상황과 환자의 항응고제
투여적응 기저질환에 따라 결정한다. 혈전색전증의 예방에 있
어서의 즉각적인 항응고제 치료재개의 이점과 출혈위험을 비교
평가하여 환자 개인 별(case-by-case basis)로 결정한다(suggest).
고위험 환자는 UFH나 LMWH bridging therapy를 가능한 즉
시 시행하고, 와파린은 출혈이 없으면 시술 당일 투여를 재개
한다(suggest). UFH는 내시경 치료시술 후 2∼6시간부터 재개
할 수 있다. 내시경 시술 후 LMWH을 재개하는 적절한 시기는
아직 결정된 바가 없다. 저위험 환자(Table 3)는 시술 후 출혈
이 없다면 와파린을 시술 당일 저녁부터 재개하고, bridge
therapy는 필요가 없다(suggest). ⊕⊕○○
⑧ 인공 심장판막을 가진 임산부의 내시경 시술: 계획된 내
시경시술은 가능하면 출산할 때까지 연기하고, 연기가 불가능
하면 LMWH나 UFH bridge therapy를 고려한다(recommend).
환자의 심장전문의 및 산과의와 협진을 해야한다. ⊕⊕○○
2) Urgent and emergent procedures (Fig. 2, Table 6)
(1) 항혈소판제를 복용하는 급성 위장관출혈 환자; 지혈될
때까지 약제를 중단한다(suggest). ⊕⊕○○
생명이 위독한 출혈이나 심각한 출혈환자는 혈소판 투여가
도움이 될 수 있다.
최근 1년 이내에 혈관스텐트를 삽입한 환자나 ASC환자에서
의미있는 출혈이 발생했다면, 항혈소판제를 중단하기 전에 심
장전문의와의 협의가 요구된다(suggest). ⊕⊕○○
(2) 항응고제를 복용하는 급성 위장관출혈 환자; 지혈될 때
까지 약제를 중단한다(recommend). ⊕⊕○○
FFP, 프로트롬빈 복합농축제제, 비타민 K 등의 투여는 환자
개인에 따라 결정해야한다. 프로타민은 아나필락시스 및 심각
한 저혈압의 위험이 있으므로, 생명위급한 출혈환자에게만 제
한해야한다(suggest). ⊕⊕○○
최근 1년 이내에 혈관 스텐트를 삽입한 환자나 ACS 환자가
의미있는 출혈을 보일 경우 항응고제를 중단하기 전에 약제를
처방한 전문가와 협의를 해야 한다(recommend). ⊕⊕○○
(3) 효과적인 내시경 치료에 필요한 적정 수준의 INR이 결정
된 바는 없지만, 와파린 복용 중에 치료 범위의 INR을 벗어난
급성 위장관출혈 환자는 항응고상태를 교정해야 한다(reco-
mmend). ⊕⊕⊕○
(4) 항응고치료를 재개해야만 하는 환자에서 내시경 지혈술
후에 재출혈의 절대적인 위험도는 알려지지 않았으며, 항응고제
의 재개 시기는 환자 개인에 따라 정해야 한다. 혈관노출과 같
은 재출혈의 위험이 높은 징표를 보이는 환자에서는 초기에 작
용시간이 짧은 UFH bridge therapy를 한다(suggest). ⊕⊕○○
결론
항응고제나 항혈소판제를 복용하는 환자에게 내시경 시술이
필요한 경우, 복용중인 약제를 어떻게 관리해야 하는가는 내시
경 시술에 의한 출혈 위험성과 약제를 중단했을 때의 환자의
혈전색전증 위험성, 내시경 시술의 긴박성, 약제의 종류를 고려
하여 결정해야 한다. 일반적으로 출혈위험이 낮은 내시경시술
을 할 때에는 모든 항응고제나 항혈소판제의 조정이나 중단이
필요하지 않다. 출혈위험이 높은 내시경시술의 경우 계획된 시
술을 할 때에는 아스피린과 NSAIDs는 중단할 필요가 없으며,
환자의 혈전색전증의 위험도에 따라서 저위험 환자에서는 환자
의 상태에 따라 지속하거나 시술 전에 중단할 수 있고, 고위험

항응고제 및 항혈소판제 복용 환자의 내시경시술을 위한 관리이옥재
162 The Korean Journal of Gastrointestinal Endoscopy
환자에서는 와파린은 3∼5일 전에 clopidogrel은 7∼10일 전에
중단하고 LMWH나 UFH로 bridge therapy를 시행한다. 응급
내시경이 필요한 급성 출혈 환자에서는 지혈이 될 때까지 항응
고제나 항혈소판제를 중단하고 생명이 위독한 심각한 출혈의
경우 혈소판이나 항응고제의 역전치료를 할 수 있고, 만일 환
자가 최근 1년 이내에 혈관 스텐트를 삽입했거나 급성관상동맥
증후군 환자라면 약제를 중단하기 전에 환자의 심장전문의와
협의를 하여야 한다.
이러한 지침은 현재까지 알려진 정보와 과학적 근거를 기초
로 하여 내시경을 시행하는 임상의가 환자를 적절하게 진료하
는데 도움을 주고자 하는 권장사항으로 절대적인 규칙이라 할
수는 없다. 여러 국가의 관련기관에서 지속적으로 최신 가이드
라인을 새로이 발표해 온 것처럼, 향후의 여러 연구에서 얻는
새로운 정보와 경험이 더욱 축적되면 현재의 지침은 계속 변경
될 것이다. 따라서 이러한 새로운 지침을 잘 숙지하고 환자의
여러 가지 상황을 고려해서 적용해야 한다.
참고문헌
1. ASGE Standards of Practice Committee, Anderson MA, Ben- Menachem T, Gan SI, et al. Management of antithrombotic agents for endoscopic procedures. Gastrointest Endosc 2009; 70:1060-1070.
2. Eisen GM, Baron TH, Dominitz JA, et al. Guideline on the management of anticoagulation and antiplatelet therapy for endoscopic procedures. Gastrointest Endosc 2002;55:775-779.
3. Zuckerman MJ, Hirota WK, Adler DG, et al. Standards of Practice Committee of the American Society for Gastroin-testinal Endoscopy. ASGE guideline: the management of low- molecular-weight heparin and nonaspirin antiplatelet agents for endoscopic procedures. Gastrointest Endosc 2005;61:189- 194.
4. Veitch AM, Baglin TP, Gershlick AH, et al. Guidelines for the management of anticoagulant and antiplatelet therapy in pa-tients undergoing endoscopic procedures. Gut 2008;57:1322- 1329.
5. 대한소화기내시경학회. 진단 소화관 내시경 길잡이. 의학문화사. 2003
6. 대한소화기내시경학회. 치료 소화관 내시경 길잡이. 의학문화사. 2004
7. Kwok A, Faigel DO. Management of anticoagulation before and after gastrointestinal endoscopy. Am J Gastroenterol 2009; 104:3085-3097.
8. Baglin TP, Keeling DM, Watson HG. British Committee for Standards in Haematology. Guidelines on oral anticoagulation (warfarin): third edition-2005 update. Br J Haematol 2006;132: 277-285.
9. Weitz JI. Low-molecular-weight heparins. N Engl J Med 1997; 337:688-698.
10. 박선미. 내시경 시술 관련 예방 항생제, 항응고제 및 항혈소판제의 사용. Korean J Gastrointest Endosc 2010;40:221-228.
11. Komatsu T, Tamai Y, Takami H, Yamagata K, Fukuda S,
Munakata A. Study for determination of the optimal cessation period of therapy with anti-platelet agents prior to invasive endoscopic procedures. J Gastroenterol 2005;40:698-707.
12. Kimchi NA, Broide E, Scapa E, Birkenfeld S. Antiplatelet the-rapy and the risk of bleeding induced by gastrointestinal en-doscopic procedures. A systematic review of the literature and recommendations. Digestion 2007;75:36-45.
13. Shiffman ML, Farrel MT, Yee YS. Risk of bleeding after en-doscopic biopsy or polypectomy in patients taking aspirin of other NSAIDS. Gastrointest Endosc 1994;40:458-462.
14. Sharis PJ, Cannon CP, Loscalzo J. The antiplatelet effects of ticlodipine and clopidogrel. Ann Intern Med 1998;19:394-405.
15. Aubert RE, Epstein RS, Teagarden JR, et al. Proton pump inhibitors effect on clopidogrel effectiveness: the clopidogrel medco outcomes study. Abstract. Circulation 2008;118:S815.
16. Li XQ, Andersson TB, Ahlstrom M, et al. Comparison of in-hibitory effects of the proton pump-inhibiting drugs omepra-zole, esomeprazole, lansoprazole, pantoprazole, and rabepra-zole on human cytochrome P450 activities. Drug Metab Dis-pos 2004;32:821-827.
17. CAPRIE Steering Committee. A randomised, blinded, trial of clopidogrel versus aspirin in patients at risk of ischemic events (CAPRIE). Lancet 1996;348:1329-1339.
18. Diener HC, Cunha L, Forbes C, et al. European Stroke Pre-vention Study. 2. Dipyridamole and acetylsalicylic acid in the secondary prevention of stroke. J Neurol Sci 1996;143:1-13.
19. Cappell MS, Abdullah M. Management of gastrointestinal blee-ding induced by gastrointestinal endoscopy. Gastroenterol Clin North Am 2000;29:125-167.
20. Mensink PB, Haringsma J, Kucharzik T, et al. Complications of double balloon enteroscopy: a multicenter survey. Endos-copy 2007;39:613-615.
21. Waye JD, Lewis BS, Yessayan S. Colonoscopy: a prospective report of complications. J Clin Gastroenterol 1992;15:347-351.
22. MacRae FA, Tank KG, Williams CB. Toward safer colono-scopy: a report on the complications of 5000 diagnostic or therapeutic colonoscopies. Gut 1983;24:376-383.
23. Masci E, Toti G, Mariani A, et al. Complications of diagnostic and therapeutic ERCP: a prospective multicentre study. Am J Gastroenterol 2001;96:417-423.
24. Muehldorfer SM, Stolte M, Martus P, et al. Diagnostic accu-racy of forceps biopsy versus polypectomy for gastric polyps: a prospective multicentre study. Gut 2002;50:465-470.
25. Eswaran SL, Sanders M, Bernadino KP, et al. Success and complications of endoscopic removal of giant duodenal and ampullary polyps: a comparative series. Gastrointest Endosc 2006;64:925-932.
26. Wexner SD, Garbus JE, Singh JJ, et al. A prospective analysis of 13,580 colonoscopies. Reevaluation of credentialing guide-lines. Surg Endosc 2001;15:251-261.
27. Nelson DB, McQuaid KR, Bond JH, et al. Procedural success and complications of large-scale screening colonoscopy. Gas-trointest Endosc 2002;55:307-314.
28. Ahmad NA, Kochman ML, Lon WB, et al. Efficacy, safety, and clinical outcomes of endoscopic mucosal resection: a study of 101 cases. Gastrointest Endosc 2002;55:390-396.
29. Freeman ML, Nelson DB, Sherman S, et al. Complications of

항응고제 및 항혈소판제 복용 환자의 내시경시술을 위한 관리이옥재
Vol. 41 (Suppl 2), 2010 (152-165) 163
endoscopic biliary sphincterotomy. N Engl J Med 1996;335: 909-918.
30. Cotton PB, Lehman G, Vennes JA, et al. Endoscopic sphin-cterotomy complications and their management: an attempt at consensus. Gastrointest Endosc 1991;37:383-393.
31. Metman EH, Lagasse JP, d’Alteroche L, et al. Risk factors for immediate complications after progressive pneumatic dilation for achalasia. Am J Gastroenterol 1999;94:1179-1185.
32. Dormann A, Meisner S, Verin N, et al. Self-expanding metal stents for gastroduodenal malignancies: systematic review of their clinical effectiveness. Endoscopy 2004;36:543-550.
33. Telford JJ, Carr-Locke DL, Baron TH, et al. Palliation of patients with malignant gastric outlet obstruction with the enteral Wallstent: outcomes from a multicenter study. Gastro-intest Endosc 2004;60:916-920.
34. Kozarek RA, Ball TJ, Brandabur JJ, et al. Expandable versus conventional esophageal prostheses: easier insertion may not preclude subsequent stent-related problems. Gastrointest En-dosc 1996;43:204-208.
35. Schapiro GD, Edmundowicz SA. Complications of percuta-neous endoscopic gastrostomy. Gastrointest Endosc Clin N Am 1996;6:409-422.
36. Affi A, Vazquez-Sequeiros E, Norton ID, et al. Acute ex-traluminal hemorrhage associated with EUS-guided fine needle aspiration: frequency and clinical significance. Gastrointest Endosc 2001;53:221-225.
37. Varadarajulu S, Eloubeidi MA. Frequency and significance of acute intracystic hemorrhage during EUS-FNA of cystic lesions of the pancreas. Gastrointest Endosc 2004;60:631-635.
38. Eloubeidi MA, Tamhane A, Varadarajulu S, et al. Frequency of major complications after EUS-guided FNA of solid pancreatic masses: a prospective evaluation. Gastrointest Endosc 2006;63: 622-629.
39. Mathus-Vliegen EM, Tytgat GN. Analysis of failures and com-plications of neodymium: YAG laser photocoagulation in gas-trointestinal tract tumors. A retrospective survey of 18 years’ experience. Endoscopy 1990;22:17-23.
40. Piai G, Cipolletta L, Claar M, et al. Prophylactic sclerotherapy of high risk esophageal varices: results of a multicentric prospective controlled trial. Hepatology 1988;8:1495-1507.
41. Schmitz RJ, Sharma P, Badr AS, et al. Incidence and mana-gement of esophageal stricture formation, ulcer bleeding, perforation, and massive hematoma formation from sclerothe-rapy versus band ligation. Am J Gastroenterol 2001;96:437- 441.
42. de Franchis R, Primignani M. Endoscopic treatments for portal hypertension. Semin Liver Dis 1999;19:439-455.
43. Scolapio JS, Pasha TM, Gostout CJ, et al. A randomized pro-spective study comparing rigid to balloon dilators for benign esophageal strictures and rings. Gastrointest Endosc 1999;50: 13-17.
44. DiPrima RE, Barkin JS, Blinder M, et al. Age as a risk factor in colonoscopy: fact versus fiction. Am J Gastroenterol 1998; 83:123-125.
45. Sorbi D, Norton I, Conio M, et al. Postpolypectomy lower GI bleeding: descriptive analysis. Gastrointest Endosc 2000;51:90- 96.
46. Nelson DB, Freeman ML. Major hemorrhage from endoscopic sphincterotomy: risk factor analysis. J Clin Gastroenterol 1994; 19:283-287.
47. King SB 3rd, Smith SC Jr, Hirshfeld JW Jr, et al. 2007 focused update of the ACC/AHA/SCAI 2005 guideline update for per-cutaneous coronary intervention: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2008;51:172-209.
48. Gage BF, Waterman AD, Shannon W, et al. Validation of clinical classifi cation schemes for predicting stroke: results from the National Registry of Atrial Fibrillation. JAMA 2001; 285:2864-2870.
49. Basson MD, Panzini L, Palmer RH. Effect of nabumetone and aspirin on colonic mucosal bleeding time. Aliment Pharmacol Ther 2001;15:539-542.
50. Gerson LB, Gage BF, Owens DK, et al. Effect and outcomes of the ASGE guidelines on the periendoscopic management of patients who take anticoagulants. Am J Gastroenterol 2000; 95:1717-1724.
51. Gerson LB Triadafi lopoulos G, Gage BF. The management of anticoagulants in the periendoscopic period for patients with atrial fibrillation: a decision analysis. Am J Med 2004;116: 451-459.
52. Hui AJ, Wong RM, Ching JY, et al. Risk of colonoscopic polypectomy bleeding with anticoagulants and antiplatelet agents: analysis of 1657 cases. Gastrointest Endosc 2004;59:44- 48.
53. Sawhney MS, Salfiti N, Nelson DB, et al. Risk factors for severe delayed postpolypectomy bleeding. Endoscopy 2008; 40:115-119.
54. Friedland S, Soetikno R. Colonoscopy with polypectomy in anticoagulated patients. Gastrointest Endosc 2006;64:98-100.
55. Howell DA, Eswaran SL, Loew BJ, et al. Use of hemostatic clips in patients undergoing colonoscopy in the setting of Coumadin antithrombotic therapy. Gastrointest Endosc 2006; 63:AB98.
56. Sobrino-Faya M, Martínez S, Gómez Balado M, et al. Clips for the prevention and treatment of postpolypectomy bleeding (hemoclips in polypectomy). Rev Esp Enferm Dig 2002;94: 457-462.
57. Hui CK, Lai KC, Yuen MF, et al. Does withholding aspirin for one week reduce the risk of post-sphincterotomy bleeding? Aliment Pharmacol Ther 2002;16:929-36.
58. Hussain N, Alsulaiman R, Burtin P, et al. The safety of en-doscopic sphincterotomy in patients receiving antiplatelet agents: a case-control study. Aliment Pharmacol Ther 2007; 25:579-584.
59. Williams DO, Abbott JD, Kip KE. DEScover Investigators. Outcomes of 6906 patients undergoing percutaneous coronary intervention in the era of drug-eluting stents: report of the DEScover Registry. Circulation 2006;114:2154-2162.
60. Iakovou I, Schmidt T, Bonizzoni E, et al. Incidence, pre-dictors, and outcome of thrombosis after successful implan-tation of drug-eluting stents. JAMA 2005;293:2126-2130.
61. Mauri L, Hsieh WH, Massaro JM, et al. Stent thrombosis in randomized clinical trials of drug-eluting stents. N Engl J Med 2007;356:1020-1029.

항응고제 및 항혈소판제 복용 환자의 내시경시술을 위한 관리이옥재
164 The Korean Journal of Gastrointestinal Endoscopy
62. Hirsh J, Fuster V, Ansell J, et al. American Heart Association; American College of Cardiology Foundation. Circulation 2003; 107:1692-1711.
63. Garcia DA, Regan S, Henault LE, et al. Risk of thromboem-bolism with short-term interruption of warfarin therapy. Arch Intern Med 2008;168:63-69.
64. Blacker DJ, Wijdicks EF, McClelland RL. Stroke risk in antico-agulated patients with atrial fibrillation undergoing endoscopy. Neurology 2003;61:964-968.
65. Constans M, Santamaria A, Mateo J, et al. Low-molecular- weight heparin as bridging therapy during interruption of oral anticoagulation in patients undergoing colonoscopy or gas-troscopy. Int J Clin Pract 2007;61:212-217.
66. Fuster V, Rydéen LE, Cannom DS, et al. ACC/AHA/ESC 2006 Guidelines for the management of patients with atrial fi-brillation: a report of the American College of Cardiology/ American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to revise the 2001 guidelines for the management of patients with atrial fibri-llation): developed in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society [published erratum appears in Circulation 2007;116:e138]. Circulation 2006;114:e257-e354.
67. Bonow RO, Carabello BA, Chatterjee K, et al. 2006 Writing Committee Members; American College of Cardiology/Ameri-can Heart Association Task Force. 2008 Focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Asso-ciation Task Force on Practice Guidelines (Writing Committee to Revise the 1998 Guidelines for the management of patients with valvular heart disease): endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. Circulation 2008;118:e523-e661.
68. American College of Cardiology/American Heart Association Task Force on Practice Guidelines; Society of Cardiovascular Anesthesiologists; Society for Cardiovascular Angiography and Interventions; Society of Thoracic Surgeons, Bonow RO, Carabello BA, Kanu C, et al. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (writing com-mittee to revise the 1998 Guidelines for the management of patients with valvular heart disease): developed in collabo-ration with the Society of Cardiovascular Anesthesiologists: endorsed by the Society for Cardiovascular Angiography and Interventions and the Society of Thoracic Surgeons [published erratum appears in Circulation 2007;115:e409]. Circulation 2006;114:e84-e231.
69. Choudari CP, Rajgopal C, Palmer KR. Acute gastrointestinal haemorrhage in anticoagulated patients: diagnoses and res-ponse to endoscopic treatment. Gut 1994;35:464-466.
70. Tabibian N. Acute gastrointestinal bleeding in anticoagulated patients: a prospective evaluation. Am J Gastroenterol 1989; 84:10-12.
71. Kuwada SK, Balm R, Gostout CJ. The risk of withdrawing chronic anticoagulation because of acute GI bleeding. Am J Gastroenterol 1996;91:1116-1119.
73. Ansell J, Hirsh J, Poller L, et al. The pharmacology and management of the vitamin K antagonists: the seventh ACCP conference on antithrombotic and thrombolytic therapy [published erratum appears in Chest 2005;127:415-416]. Chest 2004;126:204S-233S.
74. Bonow RO, Carabello BA, Chatterjee K, et al. 2006 Writing Committee Members; American College of Cardiology/Ameri-can Heart Association Task Force. 2008 Focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Asso-ciation Task Force on Practice Guidelines (Writing committee to revise the 1998 guidelines for the management of patients with valvular heart disease): endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. Circulation 2008;118:e523-e661.
75. Rubin TA, Murdoch M, Nelson DB. Acute GI bleeding in the setting of supratherapeutic international normalized ratio in patients taking warfarin: endoscopic diagnosis, clinical mana-gement, and outcomes. Gastrointest Endosc 2003;58:369-373.
76. Wilcox CM, Truss CD. Gastrointestinal bleeding in patients receiving longterm anticoagulant therapy. Am J Med 1988; 84:683-690.
77. Taha AS, Angerson WJ, Knill-Jones RP, et al. Upper gastro-intestinal mucosal abnormalities and blood loss complicating low-dose aspirin and antithrombotic therapy. Aliment Phar-macol Ther 2006;23:489-495.
78. Hashash JG, Shamseddeen W, Skoury A, Aoun N, Barada K. Gross lower gastrointestinal bleeding in patients on antico-agulant and/or antiplatelet therapy: endoscopic findings, ma-nagement, and clinical outcomes. J Clin Gastroenterol 2009; 43:36-42.
79. Rubin TA, Murdoch M, Nelson DB. Acute GI bleeding in the setting of supratherapeutic international normalized ratio in patients taking warfarin: endoscopic diagnosis, clinical ma-nagement, and outcomes. Gastrointest Endosc 2008;58:369- 373.
80. Wolf AT, Wasan SK, Saltzman JR. Impact of anticoagulation on rebleeding following endoscopic therapy for nonvariceal upper gastrointestinal hemorrhage. Am J Gastroenterol 2007; 102:290-296.
81. Chan FK, Ching JY, Hung LC, et al. Clopidogrel versus as-pirin and esomeprazole toprevent recurrent ulcerbleeding. N Engl J Med 2005;352:238-244.
82. Lai KC, Chu KM, Hui WM, et al. Esomeprazole with aspirin versus clopidogrel for prevention of recurrent gastrointestinal ulcer complications. Clin Gastroenterol Hepatol 2006;4:860- 865.
83. Sung J, Lau J, Ching J, et al. Can aspirin be reintroduced with proton pump inhibitor infusion after endoscopic hemostasis? A double blinded randomized controlled trial. Gastroentero-logy 2006;130(suppl 2):A134.
72. Ananthasubramaniam K, Beattie JN, Rosman HS, et al. How

항응고제 및 항혈소판제 복용 환자의 내시경시술을 위한 관리이옥재
Vol. 41 (Suppl 2), 2010 (152-165) 165
safely and for how long can warfarin therapy be withheld in prosthetic heart valve patients hospitalized with a major hemorrhage? Chest 2001;119:478-484.
84. King SB 3rd, Smith SC Jr, Hirshfeld JW Jr, et al. 2007 focused update of the ACC/AHA/SCAI 2005 guideline update for percutaneous coronary intervention: a report of the American College of Cardiology/American Heart Association Task Force on Practice guidelines. J Am Coll Cardiol 2008;51:172-209.
85. Hallas J, Dall M, Andries A, et al. Use of single and com-bined antithrombotic therapy and risk of serious upper gas-trointestinal bleeding: population based case-control study. BMJ 2006;333:726-730.
86. Moscucci M, Fox KA, et al. Predictors of major bleeding in acute coronary syndromes: the Global Registry of Acute Coro-nary Events (GRACE). Eur Heart J 2003;24:1815-823.
87. Al-Mallah M, Bazari RN, Jankowski M, et al. Predictors and outcomes associated with gastrointestinal bleeding in patients with acute coronary syndromes. J Thromb Thrombolysis 2007;23:51-55.
88. Abbas AE, Brodie B, Dixon S, et al. Incidence and prognostic impact of gastrointestinal bleeding after percutaneous coro-nary intervention for acute myocardial infarction. Am J Cardiol 2005;96:173-176.
89. Lin S, Konstance R, Jollis J, et al. The utility of upper endo-scopy in patients with concomitant upper gastrointestinal bleeding and acute myocardial infarction. Dig Dis Sci 2006; 51:2377-2383.
90. Cappell MS, Iacovone FM Jr. Safety and efficacy of esopha-gogastroduodenoscopy after myocardial infarction. Am J Med 1999;106:29-35.
91. Cappell MS. Safety and efficacy of colonoscopy after myo-cardial infarction: an analysis of 100 study patients and 100 control patients at two tertiary cardiac referral hospitals. Gastrointest Endosc 2004;60:901-909.
92. Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008;336:924-926.