Embed Size (px)
Citation preview
AIDS RESEARCH AND HUMAN RETROVIRUSESVolume 18, Number 14, 2002, pp. 1089–1090© Mary Ann Liebert, Inc.
Letter to the Editor
Failure to Detect HTLV Type 1 DNA from HTLV Type 1-Seronegative Patients with Chronic Progressive
Spastic Paraparesis in Kagoshima
MASAHIRO NAGAI,1,* TAKANORI UTSUNOMIYA,1,* NORIHIRO TAKENOUCHI,2
SHUJI IZUMO,2 AND MITSUHIRO OSAME1
1089
EDITOR: Human T cell lymphotropic virus type-1 (HTLV-1)is an exogenous human retrovirus responsible for the
chronic progressive neurological disease termed HTLV-1-as-sociated myelopathy/tropical spastic paraparesis (HAM/TSP).In general, HTLV-1 infection is confirmed by the existence ofanti-HTLV-1 antibodies in sera. Although HAM/TSP patientsare essentially seropositive for HTLV-1, it has been reportedthat some patients with chronic progressive spastic paraparesis,which is clinically indistinguishable from HAM/TSP, had nodetectable antibodies to HTLV-1.1 These HTLV-1-seronega-tive, progressive spastic paraparesis patients have been reportedfrom a number of areas in the Caribbean and Latin America,and various etiologies of this disease have been shown.1 It isof interest that HTLV-1 DNA has been detected by polymerasechain reaction (PCR) in peripheral blood mononuclear cells(PBMCs) from some HTLV-1-seronegative progressive spasticparaparesis patients in Chile,2,3 the Caribbean,4 and India.5
Ramirez et al. have demonstrated that a high proportion, thatis, 10 of 15, HTLV-1-seronegative Chilean patients with pro-gressive spastic paraparesis revealed positivity for the HTLV-1 tax gene but not the pol gene.3 They speculated that the pres-ence of defective HTLV-1 provirus was related to thepathomechanism in those patients regardless of their lack of im-mune response. On the other hand, HTLV-1 DNA has not beendetected in PBMCs from HTLV-1-seronegative Brazilian pa-tients with progressive spastic paraparesis.1 Therefore, it is stillcontroversial whether HTLV-1 is associated with progressivespastic paraparesis in HTLV-1-seronegative patients. Kago-shima is an area in Japan where HTLV-1 is highly endemic,and the prevalence of HAM/TSP is also high. In this report, weinvestigated the existence of HTLV-1 DNA in PBMCs fromHTLV-1-seronegative patients with progressive spastic para-paresis in Kagoshima.
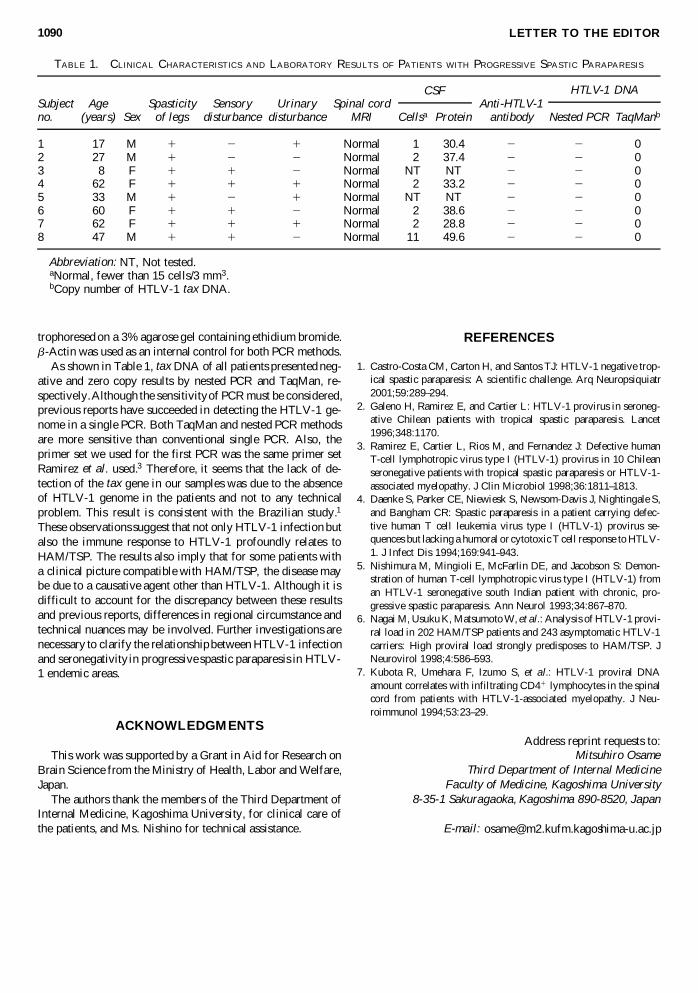
We retrospectively selected all patients who had progressivespastic paraparesis for which the etiology remained unknown.Eight Japanese patients, who were monitored at KagoshimaUniversity, were selected and examined. Clinical history, fam-ily history, neurological findings, laboratory tests, and magneticresonance imaging (MRI) analyses of brain and spinal cordwere examined to exclude the known neurological disorders,such as familial spastic paraplegia, spinal cord tumor, syringo-myelia, spondylosis, and multiple sclerosis. Anti-HTLV-1 an-tibodies were tested in all sera by the particle agglutinationmethod, enzyme-linked immunosorbent assay (ELISA), andWestern blot. These tests enable detection of antibodies to thestructural proteins of HTLV-1, such as Gag and Env. The char-acteristics of these patients are summarized in Table 1. All pa-tients showed spasticity, hyperreflexia, and weakness of thelower limbs. Five of eight patients showed mild sensory im-pairment without definite spinal cord level. Half of the patientshad neurogenic bladder. No anti-HTLV-1 antibodies were de-tected in any of the patients.
Peripheral blood samples were obtained from the patients af-ter informed consent had been given. PBMCs were isolatedfrom peripheral blood samples by density gradient centrifuga-tion. DNA was extracted from the cells, using a spin columnDNA extraction kit (Qiagen, Valencia, CA). HTLV-1 tax DNAwas measured by real-time quantitative PCR (TaqMan; AppliedBiosystems, Foster City, CA) and conventional nested PCRmethods. The condition for TaqMan PCR were described pre-viously.6 Regarding the nested PCR, we amplified a region of159 bp of the tax gene by 35 cycles of PCR amplification, us-ing SK43 and SK44 primers.7 Two microliters of each of thefirst PCR products was subjected to a second PCR with innerprimers SN443 and SN444 (118-bp product).7 The second PCRwas performed for 35 cycles and the products were elec-
1Third Department of Internal Medicine, Faculty of Medicine, Kagoshima University, 8-35-1 Sakuragaoka, Kagoshima 890-8520, Japan.2Division of Molecular Pathology, Center for Chronic Viral Diseases, Faculty of Medicine, Kagoshima University, 8-35-1 Sakuragaoka,
Kagoshima 890-8520, Japan.*M.N. and T.U. contributed equally to this study.
trophoresed on a 3% agarose gel containing ethidium bromide.b-Actin was used as an internal control for both PCR methods.
As shown in Table 1, tax DNA of all patients presented neg-ative and zero copy results by nested PCR and TaqMan, re-spectively. Although the sensitivity of PCR must be considered,previous reports have succeeded in detecting the HTLV-1 ge-nome in a single PCR. Both TaqMan and nested PCR methodsare more sensitive than conventional single PCR. Also, theprimer set we used for the first PCR was the same primer setRamirez et al. used.3 Therefore, it seems that the lack of de-tection of the tax gene in our samples was due to the absenceof HTLV-1 genome in the patients and not to any technicalproblem. This result is consistent with the Brazilian study.1
These observations suggest that not only HTLV-1 infection butalso the immune response to HTLV-1 profoundly relates toHAM/TSP. The results also imply that for some patients witha clinical picture compatible with HAM/TSP, the disease maybe due to a causative agent other than HTLV-1. Although it isdifficult to account for the discrepancy between these resultsand previous reports, differences in regional circumstance andtechnical nuances may be involved. Further investigations arenecessary to clarify the relationship between HTLV-1 infectionand seronegativity in progressive spastic paraparesis in HTLV-1 endemic areas.
ACKNOWLEDGMENTS
This work was supported by a Grant in Aid for Research onBrain Science from the Ministry of Health, Labor and Welfare,Japan.
The authors thank the members of the Third Department ofInternal Medicine, Kagoshima University, for clinical care ofthe patients, and Ms. Nishino for technical assistance.
REFERENCES
1. Castro-Costa CM, Carton H, and Santos TJ: HTLV-1 negative trop-ical spastic paraparesis: A scientific challenge. Arq Neuropsiquiatr2001;59:289–294.
2. Galeno H, Ramirez E, and Cartier L: HTLV-1 provirus in seroneg-ative Chilean patients with tropical spastic paraparesis. Lancet1996;348:1170.
3. Ramirez E, Cartier L, Rios M, and Fernandez J: Defective humanT-cell lymphotropic virus type I (HTLV-1) provirus in 10 Chileanseronegative patients with tropical spastic paraparesis or HTLV-1-associated myelopathy. J Clin Microbiol 1998;36:1811–1813.
4. Daenke S, Parker CE, Niewiesk S, Newsom-Davis J, Nightingale S,and Bangham CR: Spastic paraparesis in a patient carrying defec-tive human T cell leukemia virus type I (HTLV-1) provirus se-quences but lacking a humoral or cytotoxic T cell response to HTLV-1. J Infect Dis 1994;169:941–943.
5. Nishimura M, Mingioli E, McFarlin DE, and Jacobson S: Demon-stration of human T-cell lymphotropic virus type I (HTLV-1) froman HTLV-1 seronegative south Indian patient with chronic, pro-gressive spastic paraparesis. Ann Neurol 1993;34:867–870.
6. Nagai M, Usuku K, Matsumoto W, et al.: Analysis of HTLV-1 provi-ral load in 202 HAM/TSP patients and 243 asymptomatic HTLV-1carriers: High proviral load strongly predisposes to HAM/TSP. JNeurovirol 1998;4:586–593.
7. Kubota R, Umehara F, Izumo S, et al.: HTLV-1 proviral DNAamount correlates with infiltrating CD41 lymphocytes in the spinalcord from patients with HTLV-1-associated myelopathy. J Neu-roimmunol 1994;53:23–29.
Address reprint requests to:Mitsuhiro Osame
Third Department of Internal MedicineFaculty of Medicine, Kagoshima University
8-35-1 Sakuragaoka, Kagoshima 890-8520, Japan
E-mail: [email protected]
LETTER TO THE EDITOR1090
TABLE 1. CLINICAL CHARACTERISTICS AND LABORATORY RESULTS OF PATIENTS WITH PROGRESSIVE SPASTIC PARAPARESIS
Subject Age Spasticity Sensory Urinary Spinal cord Anti-HTLV-1no. (years) Sex of legs disturbance disturbance MRI Cellsa Protein antibody Nested PCR TaqManb
1 17 M 1 2 1 Normal 1 30.4 2 2 02 27 M 1 2 2 Normal 2 37.4 2 2 03 8 F 1 1 2 Normal NT NT 2 2 04 62 F 1 1 1 Normal 2 33.2 2 2 05 33 M 1 2 1 Normal NT NT 2 2 06 60 F 1 1 2 Normal 2 38.6 2 2 07 62 F 1 1 1 Normal 2 28.8 2 2 08 47 M 1 1 2 Normal 11 49.6 2 2 0
Abbreviation: NT, Not tested.aNormal, fewer than 15 cells/3 mm3.bCopy number of HTLV-1 tax DNA.
HTLV-1 DNACSF