-
A Case Report of Syndrome of Inappropriate Secretion
ofAntidiuretic Hormone With Marked Edema Due to
Administration of Hypertonic Saline
Hiroto Maeda, Kazuhiko Tsuruya, Hideki Yotsueda, Masatomo
Taniguchi,Masanori Tokumoto, Hideki Hirakata, and Mitsuo Iida
Department of Medicine and Clinical Science, Graduate School of
Medical Sciences, Kyushu University,Fukuoka, Japan
Abstract: A 61-year-old man had hyponatremia (serumNa112
mmol/L), which was associated with disturbance ofconsciousness.
Therefore, administration of hypertonicsaline was commenced.
Eventually he was diagnosed withthe syndrome of inappropriate
secretion of antidiuretichormone (SIADH). Hypertonic saline was
continued for45 days, and plasma Na concentration rose to 138
mmol/L.At that time we were consulted regarding further
adminis-tration of hypertonic saline.At the time of the
consultationmarked edema had developed affecting the whole body.The
cardiothoracic ratio was increased and pleural effusionwas evident
on the chest X-ray. Administration of hyper-tonic saline was
discontinued to prevent further worseningof the edema. Furthermore,
water restriction (500 mL/day)
was started. Body weight decreased by 4.3 kg in 7 days andthe
edema was diminished. However, plasma Na concen-tration decreased
to 117 mmol/L.At that stage, we neededto balance the treatment of
hyponatremia to the increasedextracellular fluid volume (ECF).To
normalize the ECF,wecarried out ultrafiltration (UF) three times.
Resolution ofedema by using an extracorporeal UF method allowed
thecontrol of plasma Na concentration. In this case increasedECF
volume hindered the adjustment of plasma Na con-centration. The
infusion of hypertonic saline is now usedcommonly by physicians. It
is necessary to consider thepotential risks of such treatment.
KeyWords:Hyponatre-mia, Olfactory neuroblastoma, Syndrome of
inappropriatesecretion of antidiuretic hormone,
Ultrafiltration.
Under normal conditions, antidiuretic hormone(ADH) provides fine
adjustment of plasma Na con-centration based on plasma osmotic
pressure. Thesyndrome of inappropriate secretion of ADH(SIADH) is
characterized by non-physiologic releaseof ADH with resultant
impairment of water excre-tion. Since the excretion of Na is normal
in SIADH,the extracellular fluid (ECF) volume is normal oronly
slightly increased. Therefore, patients withSIADH are typically
euvolemic and free of periph-eral or pulmonary edema. Here, we
report a patientof SIADH who developed marked edema, which
wascaused by continuous administration of hypertonic
saline. Resolution of edema by using an extracorpo-real
ultrafiltration (UF) method allowed the controlof plasma Na
concentration. It is concluded thatincreased ECF volume hinders the
adjustment ofplasma Na concentration.
CASE REPORT
A 61-year-old man noticed swelling of the rightcervical lymph
node in the first 10 days of January2005, but did not seek medical
consultation.However, he later visited the local hospital
afterdeveloping nasal bleeding and nasal congestion on 28January.
Lymph node biopsy was carried out and hewas diagnosed with
malignant lymphoma. Becausethere was no hematologist in the
hospital, he wasreferred to another hospital on 1 March 2005.
Onadmission (2 March), he was noted to havehyponatremia (serum Na:
116 mmol/L), which
Received May 2006.Address correspondence and reprint requests to
Dr Kazuhiko
Tsuruya, Department of Medicine and Clinical Science,
GraduateSchool of Medical Sciences, Kyushu University, Maidashi
3-1-1,Higashi-ku, Fukuoka 812-8582, Japan. Email:
[email protected]
Therapeutic Apheresis and Dialysis 11(4):309313doi:
10.1111/j.1744-9987.2007.00469.x 2007 International Society for
Apheresis
309
-
further deteriorated to 112 mmol/L on 5 March. Thelatter was
associated with disturbance of conscious-ness.Administration of
hypertonic saline (2.5%NaClat 600 mL/day) was commenced on the same
day.Theconsciousness status improved with the rise in plasmaNa
concentration, which was maintained between115 and 126 mmol/L
thereafter. In summary, thepatient showed the following features:
(i) hyponatre-mia and hypo-osmolality (plasma Na: 125 mmol/L,Posm:
258 mOsm/kgH2O); (ii) inappropriately highurinary osmolality (Uosm:
580 mOsm/kgH2O); (iii)high urinary Na concentration (209 mmol/L);
(iv)normovolemia; and (v) normal renal, adrenal, andthyroid
functions. Based on these findings, he wasdiagnosed with
SIADH.Nasal cavity biopsy established the diagnosis as
olfactory neuroblastoma (ONB), not malignant lym-phoma.ONB was
thought to be the cause of SIADH.He was considered not suitable for
surgical treatmentbecause magnetic resonance imaging (MRI)
showedintracranial infiltration of the ONB. Therefore, hewas
transferred to our hospital for radiotherapy bythe otolaryngologist
on 22 March.On admission, he was consciously alert.Height was
156.3 cm, body weight was 53.4 kg and blood pres-sure was 144/86
mm Hg. The right cheek and righteye were swollen and cervical lymph
nodes were pal-pable.Laboratory findings are shown in Table
1.Totalprotein and serum albumin were slightly low; bloodurea
nitrogen was markedly decreased, with persis-tence of hyponatremia.
Renal function was normalwith a creatinine clearance of 114
mL/min/1.73 m2.
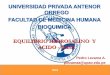
The head MRI showed direct tumor invasion fromthe right nasal
cavity into the mandible, maxillarysinus, ethmoid bone, sphenoidal
sinus, frontal sinusand frontal lobe (Fig. 1). Although hypertonic
saline(2.5% NaCl at 600 mL/day) was continued to beadministered
through the central vein catheter,plasma Na concentration was low
at 116 mmol/L on25 March. Subsequently, a higher concentration
ofsaline solution was infused and plasma Na concentra-tion rose to
138 mmol/L on 18 April (Fig. 2). Basedon the need to withdraw the
central venous catheterdue to infection at the site of the catheter
exit, theotolaryngologist consulted us on 18 April regardingfurther
administration of hypertonic saline.At the time of the
consultation, body weight had
increased by 3.4 kg since admission to our hospitaland marked
edema had developed affecting thewhole body. The cardiothoracic
ratio was increasedand pleural effusion was evident on the chest
X-ray(Fig. 3).Administration of hypertonic saline was dis-continued
to prevent further worsening of theedema. Furthermore, water
restriction (500 mL/day)was started for treatment of hyponatremia
from 19April. On 26 April, body weight decreased by 4.3 kg(from
56.7 to 52.4 kg) and the edema was diminished.However, plasma Na
concentration decreased to117 mmol/L.Accordingly, we carefully
recommencedthe administration of hypertonic saline (2.5% NaClat 600
mL/day) on 26April to prevent any increase inECF. However, plasma
Na concentration did not risebut rather decreased to 115 mmol/L on
28 April, andthe patient developed consciousness disturbance.
TABLE 1. Laboratory data on admission
Peripheral blood Blood chemistry Immunology
WBC (35009000) 7380/uL Total protein (6.78.3) 6.3 g/dL CRP (
-
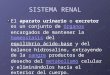
FIG. 2. Clinical course of urinaryNa, serum Na, antidiuretic
hormone(ADH) and body weight. The extra-cellular fluid volume (ECF)
wasincreased due to continuous hyper-tonic saline. We reasoned the
diffi-culty of treatment of hyponatremiawas due to the increased
ECFvolume and carried out ultrafiltra-tion (UF) three times. It
allowed thecontrol of plasma Na concentrationto remain within the
range of 128131 mmol/L.
3.2
Body weight
2.5% 3.8%
ADH4.0 2.8
3.0%UF
UFrosemide 40 mgNaCl 2.5%
Serum Na
Urinary Na
(kg)
(mmol/L) (mmol/L)
(pg/mL)
45
50
55
60
3/23 3/30 4/6 4/13 4/20 4/27 5/4 5/11 5/18 5/25
100
110
120
130
140
0
50
100
150
200
250
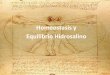
FIG. 3. Chest X-rays taken on (A)admission, and (B) at time of
consul-tation. Note the appearance ofpleural fluid and increased
cardio-thoracic ratio on B.
A B
FIG. 1. Magnetic resonance image(MRI) of the head. The MRI
showstumor infiltration. (A) Note thespread of the tumor into the
maxil-lary sinus, ethmoid bone, sphenoidalsinus and frontal sinus.
(B) Cancerinvasion of the frontal lobe (arrow).
A B
SIADH with Edema Due to Hypertonic Saline 311
2007 International Society for Apheresis Ther Apher Dial, Vol.
11, No. 4, 2007
- The control of hyponatremia was so difficult in thispatient
that the plasma Na concentration haddecreased 24 mmol/L in 9 days.
Although totalpatient intake had been almost controlled,
urineoutput remained high (Fig. 4). Serum albumin wasgradually
increased and it showed that ECF wasdecreased. It was likely that
the more ECFdecreased, the more Na had decreased.At that stage,we
reasoned the difficulty of treatment of hyponatre-mia was due to
the increased ECF volume. To nor-malize the ECF, we carried out UF
three timesbetween 30 April and 7 May. UF was carried out for10 h
in total until systolic blood pressure decreased to
-
SIADH such as drugs and pulmonary diseases werealso not obvious,
we concluded that ONB causedSIADH.SIADH is characterized by
non-physiologic release
of ADH, resulting in impaired water excretion withnormal sodium
excretion.Renal water reabsorption isenhanced due to persistentADH
activity, resulting indilution (hyponatremia and hypo-osmolality)
andexpansion of body fluids. However, edema does notoccur under
such circumstances because the volumereceptors are activated,
leading to appropriateincrease in urinary Na and water excretion,
which areprobably mediated by the renin-angiotensin system,atrial
natriuretic peptide, and activation of sympa-thetic nerves.The
ensuing volume expansion activatessecondary
natriureticmechanisms,resulting inNa andwater loss (9).Therefore,
water retention and Na lossdonot occur,andplasmaNa concentrations
donot fallwhen water intake is restricted. However, plasma
Naconcentration fell rapidly in spite of the restriction ofwater
intake in our patient. The ECF volume tendedto be normalized and
renal water reabsorption con-tinued to enhance due to persistent
ADH activity.Therefore, even when water intake was
restricted,urinaryNa excretion remained high and the control
ofplasma Na concentration was incomplete.The correc-tion of the
excess ECF volume by UF decreasedurinary Na excretion (Fig. 2), and
it is likely thatplasma Na concentration became easier to
control.Following repeated courses of UF, the plasma
Naconcentration could be controlled only by waterrestriction.Based
on this finding, it is thought that thedifficulty in the treatment
of hyponatremia was due tothe excess of ECF volume.Increased ECF
volume is thought to be solely due
to hypertonic saline for the following reasons: (i)cardiac and
hepatic functions were normal, and (ii)the lack of venous or lymph
duct obstruction by thetumor in radiologic images.In this case we
started water restriction only; as
a result, plasma Na concentration decreased to115 mmol/L. The
patient developed consciousnessdisturbance, and we therefore
carried out UF toeliminate the increased ECF volume in
haste.However, hyponatremia of SIADH is best correctedby giving
loop diuretic and by replacing sodium lost
in the urine by a quantitative replacement in the formof a
hypertonic saline infusion (10).Therefore if furo-semide was used
earlier, it is likely that UF couldhave been avoided. Furthermore
if no hypertonicsaline was administered, the edema would not
occurand plasma Na concentration could be controlled bywater
restriction only.In summary, we report a patient who developed
marked edema in association with SIADH. Thecontrol of plasma Na
concentration was difficult dueto increased ECF volume. Finally, an
adjustment ofECF volume by using UF method allowed easiercontrol of
plasma Na concentration. The infusion ofhypertonic saline only is
now used commonly by phy-sicians. Therefore, it is necessary to
consider thepotential risks of such treatment.
REFERENCES
1. Miura K, Mineta H, Yokota N et al. Olfactory
neuroblastomawith epithelial and endocrine differentiation
transformed intoganglioneuroma after chemoradiotherapy. Pathol Int
2001;51:9427.
2. Myers SL, Hardy DA, Wiebe CB et al. Olfactory neuroblas-toma
invading the oral cavity in a patient with
inappropriateantidiuretic hormone secretion. Oral Surg Oral Med
OralPathol 1994;77:64550.
3. Ahwal MA, Jha N, Nabholtz JM et al. Olfactory neuro-blastoma:
report of a case associated with inappropriate anti-diuretic
hormone secretion. J Otolaryngol 1994;23:4379.
4. Cullen MJ, Cusack DA, OBrian DS et al. Neuroblastoma
ofarginine vasopressin by an olfactory neuroblastoma
causingreversible syndrome of antidiuresis. Am J Med
1986;81:91116.
5. Osterman J, Calhoun A, Dunham M et al. Chronic syndromeof
inappropriate antidiuretic hormone secretion and hyperten-sion in a
patient with olfactory neuroblastoma. Evidence ofectopic production
of arginine vasopressin by the tumor.ArchIntern Med
1986;146:17315.
6. Srigley JR,Dayal VS,Gregor RT et al. Hyponatremia second-ary
to olfactory neuroblastoma. Arch Otolaryngol 1983;109:55962.
7. Singh W,Ramage C, Best P et al. Nasal neuroblastoma
secret-ing vasopressin. A case report. Cancer 1980;45:9616.
8. Pope TL, Morris JL, Cail WS et al.
Esthesioneuroblastomapresenting as an intracranial mass. South Med
J 1980;73:6435.
9. Verbalis JG. Pathogenesis of hyponatremia in an
experimentalmodel of the syndrome of inappropriate antidiuresis. Am
JPhysiol 1994;267:R161725.
10. Decaux G, Waterlot Y, Genette F et al. Treatment of the
syn-drome of inappropriate secretion of antidiuretic hormone
withfurosemide. N Engl J Med 1981;304:32930.
SIADH with Edema Due to Hypertonic Saline 313
2007 International Society for Apheresis Ther Apher Dial, Vol.
11, No. 4, 2007