Embed Size (px)
Citation preview
1
第6回認定医集中教育セミナー
「抗HLA抗体のモニタリング」
広島大学大学院医歯薬保健学研究院応用生命科学部門消化器・移植外科学
大段 秀樹
Anti-HLA Abs9 非自己HLA抗原の移入により産生
輸血、妊娠、移植歴など、
9 抗体関連型拒絶反応のハイリスク群
9 グラフト廃絶の主要な原因
日本臨床腎移植学会 第6回集中セミナー 2014年3月14日「抗HLA抗体のモニタリング」
2
Cell-Based Assays•Complement-dependent cytotoxicity (CDC)
Methods for HLA-specific Ab screening and donor cross-matching testing
•Complement-dependent cytotoxicity (CDC)
=Lymphocyte cytotoxicity test (LCT)
→Anti-human immunoblobulin-LCT (AHG-LCT)
•Flow cytometry crossmatch (FCXM)
Solid-Phase ImmunoassaysSolid Phase Immunoassays•Enzyme-linked immunosorbent assay (ELISA)
•Bead-based array assays
(Flow cytometry or Luminex)
Complement-dependent cytotoxicity (CDC)=Lymphocyte cytotoxicity test (LCT)
日本臨床腎移植学会 第6回集中セミナー 2014年3月14日「抗HLA抗体のモニタリング」
2014/3/4
3
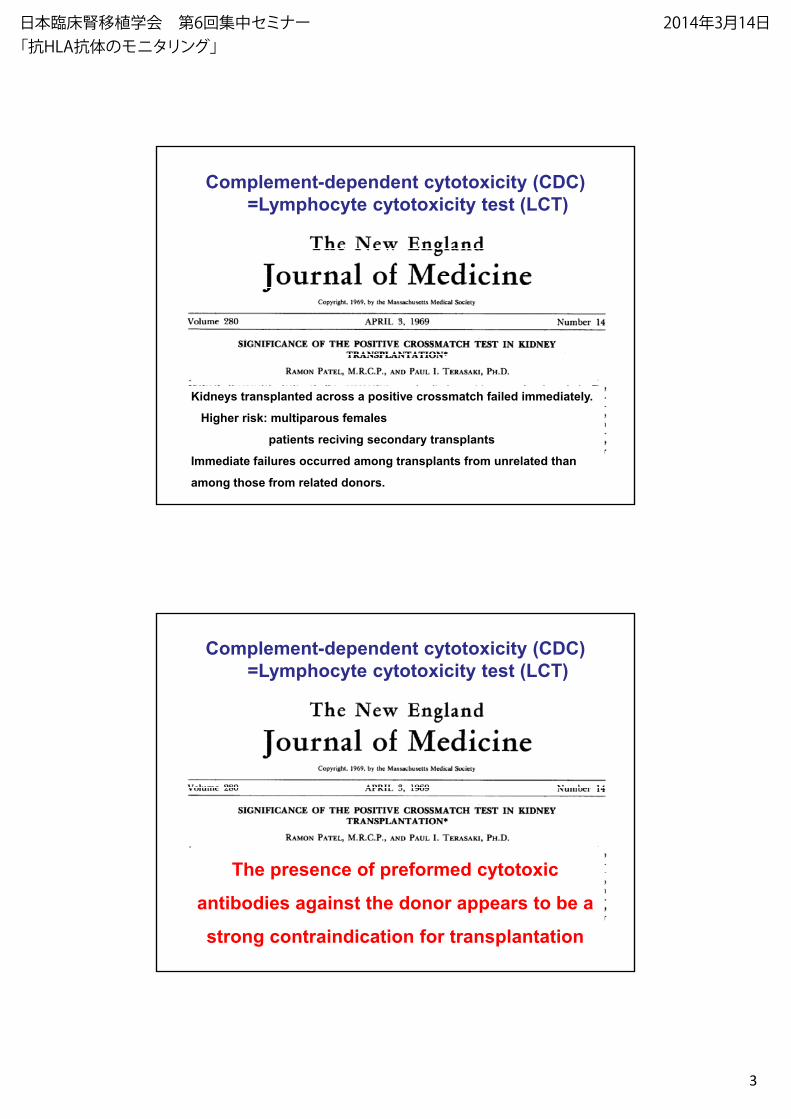
Complement-dependent cytotoxicity (CDC)=Lymphocyte cytotoxicity test (LCT)
Kidneys transplanted across a positive crossmatch failed immediately.
Higher risk: multiparous females
patients reciving secondary transplants
Immediate failures occurred among transplants from unrelated than
among those from related donors.
Complement-dependent cytotoxicity (CDC)=Lymphocyte cytotoxicity test (LCT)
The presence of preformed cytotoxic
antibodies against the donor appears to be a
strong contraindication for transplantation
日本臨床腎移植学会 第6回集中セミナー「抗HLA抗体のモニタリング」
2014年3月14日
2014/3/4
4
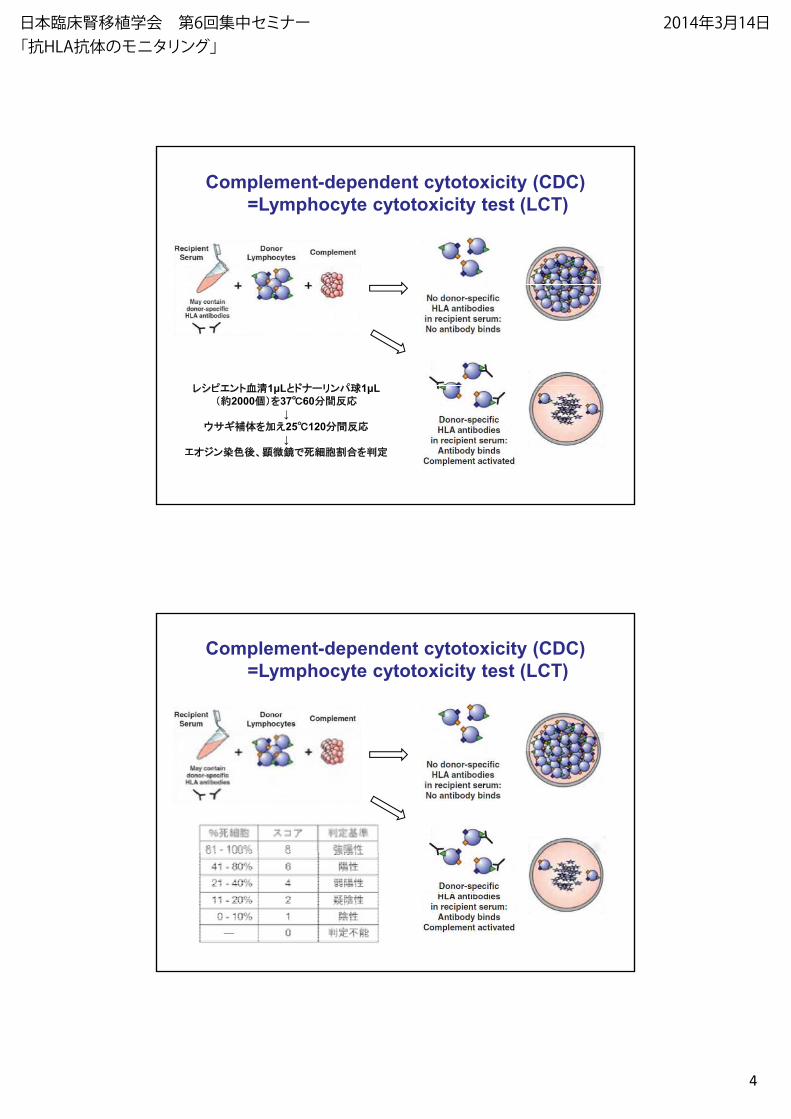
Complement-dependent cytotoxicity (CDC)=Lymphocyte cytotoxicity test (LCT)
ント血 1 L ナ リン 1 Lント血 1 L ナーリン 1 L2000 37℃60 反応
体 25℃120 反応
ン 、 定
Complement-dependent cytotoxicity (CDC)=Lymphocyte cytotoxicity test (LCT)
日本臨床腎移植学会 第6回集中セミナー「抗HLA抗体のモニタリング」
2014年3月14日
2014/3/4
5
Complement-dependent cytotoxicity (CDC)=Lymphocyte cytotoxicity test (LCT)
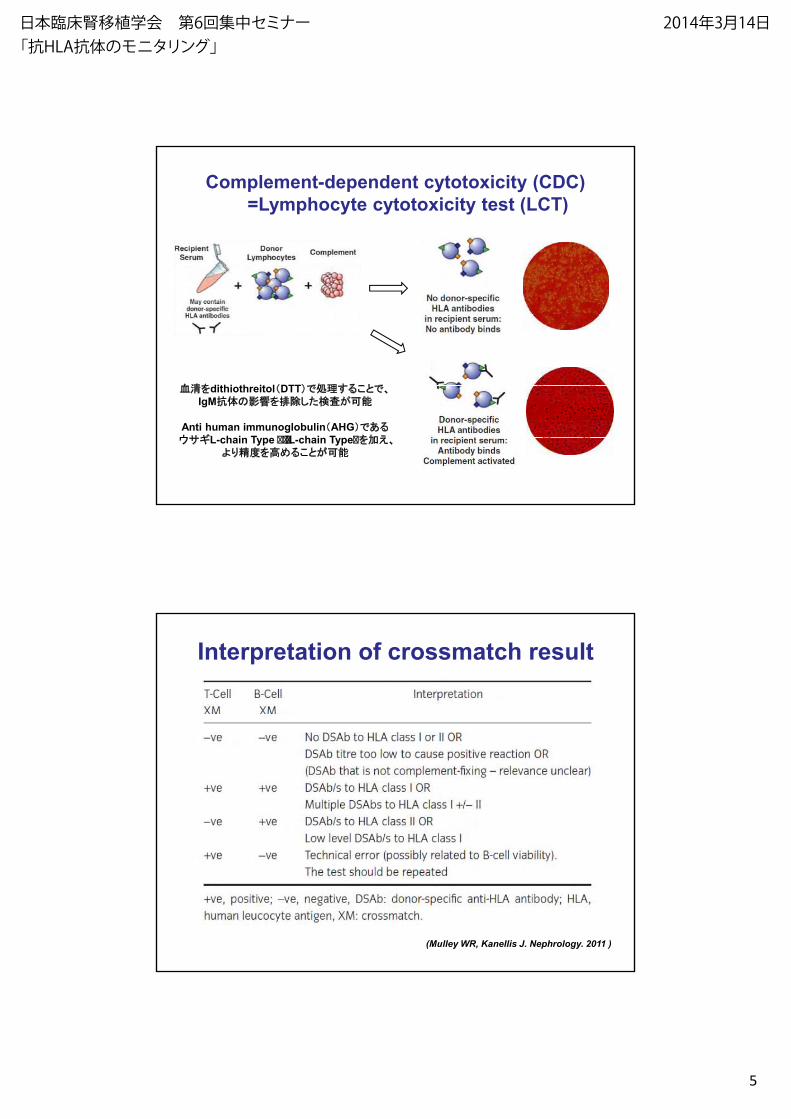
血 dithi th it l DTT血 dithiothreitol DTT 、IgM抗体の
Anti human immunoglobulin AHGL-chain Type ���L-chain Type� 、
より
Interpretation of crossmatch result
(Mulley WR, Kanellis J. Nephrology. 2011 )
日本臨床腎移植学会 第6回集中セミナー「抗HLA抗体のモニタリング」
2014年3月14日
2014/3/4
6
Points at LCT-XM, AHG-LCT-XM
• 定 の主 、 に
• 抗体 な な
• リン のViabilityによ 大
• 非 抗体によ な
• 血 中の抗体 の 、 体 の に
• IgGのisotypeによ 体 な に
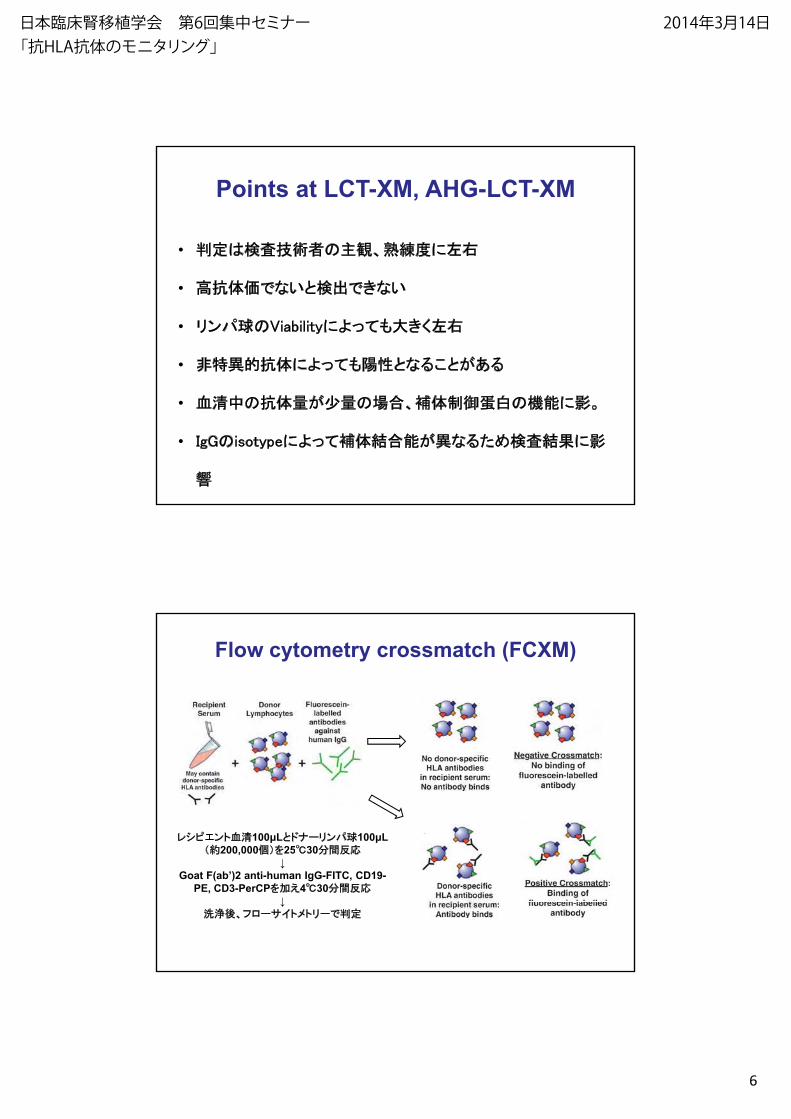
Flow cytometry crossmatch (FCXM)
ント血 100 L ナーリン 100 L200 000 25℃30 反応200,000 25℃30 反応
Goat F(ab’)2 anti-human IgG-FITC, CD19-PE, CD3-PerCP 4℃30 反応
、フ ー イト トリー 定
日本臨床腎移植学会 第6回集中セミナー「抗HLA抗体のモニタリング」
2014年3月14日
2014/3/4
7
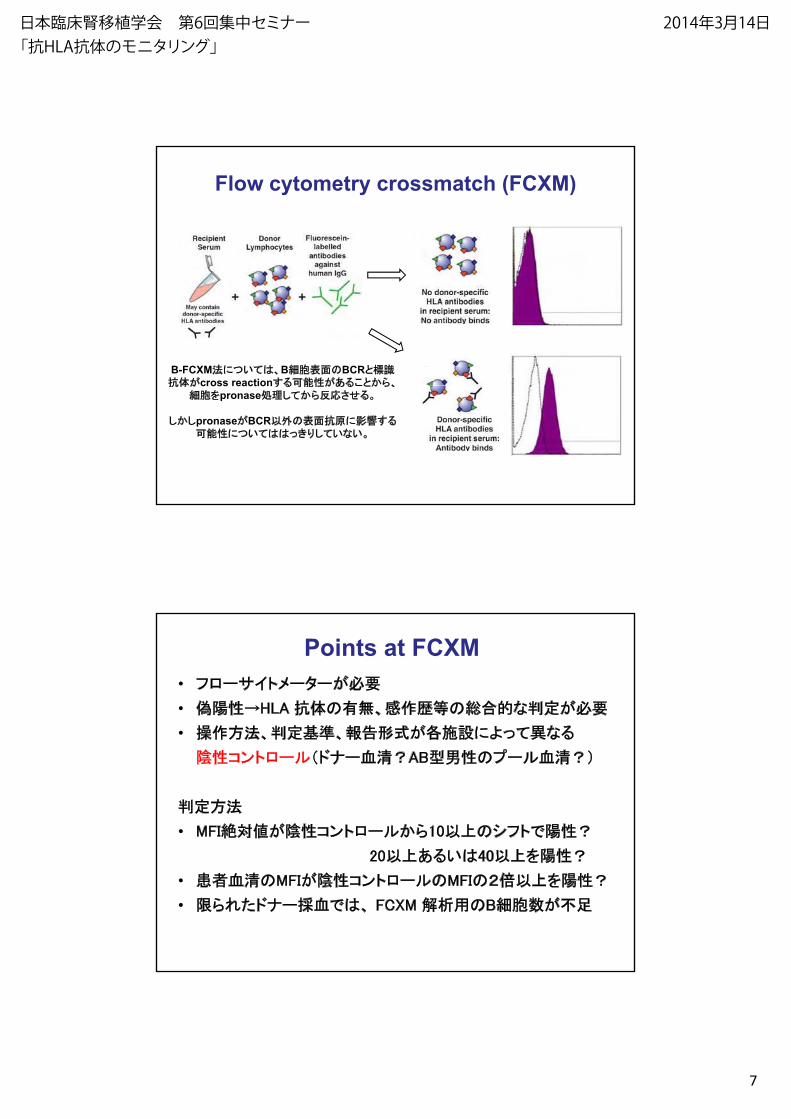
Flow cytometry crossmatch (FCXM)
B-FCXM に 、B のBCR抗体 cross reaction 、抗体 cross reaction 、
pronase 反応
pronase BCR 外の 抗原にに り な
Points at FCXM• フ ー イト ーター 要
• HLA 抗体の 、 歴 の な 定 要
• 定 によ な• 、 定 、 によ な
ント ー ナー血 AB型 の ー 血
定
• MFI絶 ント ー 10 の フト
20 4020 40
• 血 のMFI ント ー のMFIの
• ナー 血 、 FCXM 用のB
日本臨床腎移植学会 第6回集中セミナー「抗HLA抗体のモニタリング」
2014年3月14日
2014/3/4
8
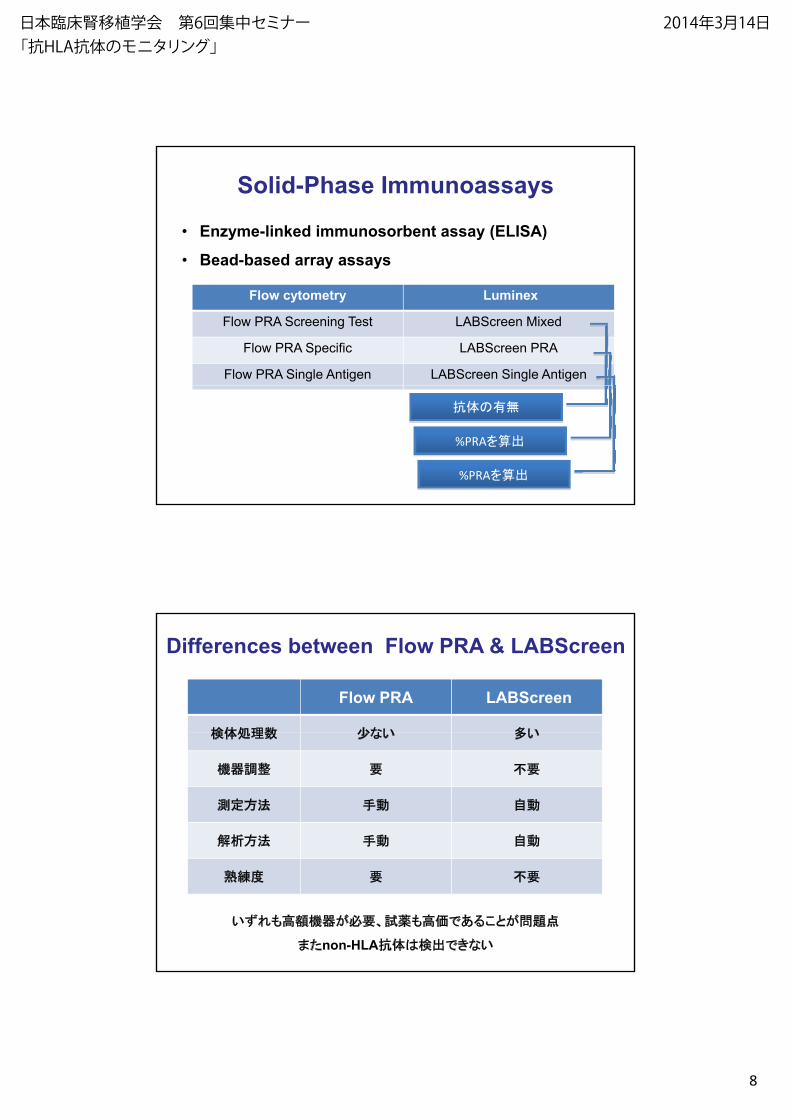
• Enzyme-linked immunosorbent assay (ELISA)
• Bead-based array assays
Solid-Phase Immunoassays
y y
Flow cytometry Luminex
Flow PRA Screening Test LABScreen Mixed
Flow PRA Specific LABScreen PRA
Flow PRA Single Antigen LABScreen Single Antigen
抗体の
%PRA
%PRA
Differences between Flow PRA & LABScreen
Flow PRA LABScreen
体 な体 な
器 要 要
定 自
自
要 要
器 要、 薬
non-HLA抗体 な
日本臨床腎移植学会 第6回集中セミナー「抗HLA抗体のモニタリング」
2014年3月14日
2014/3/4
9
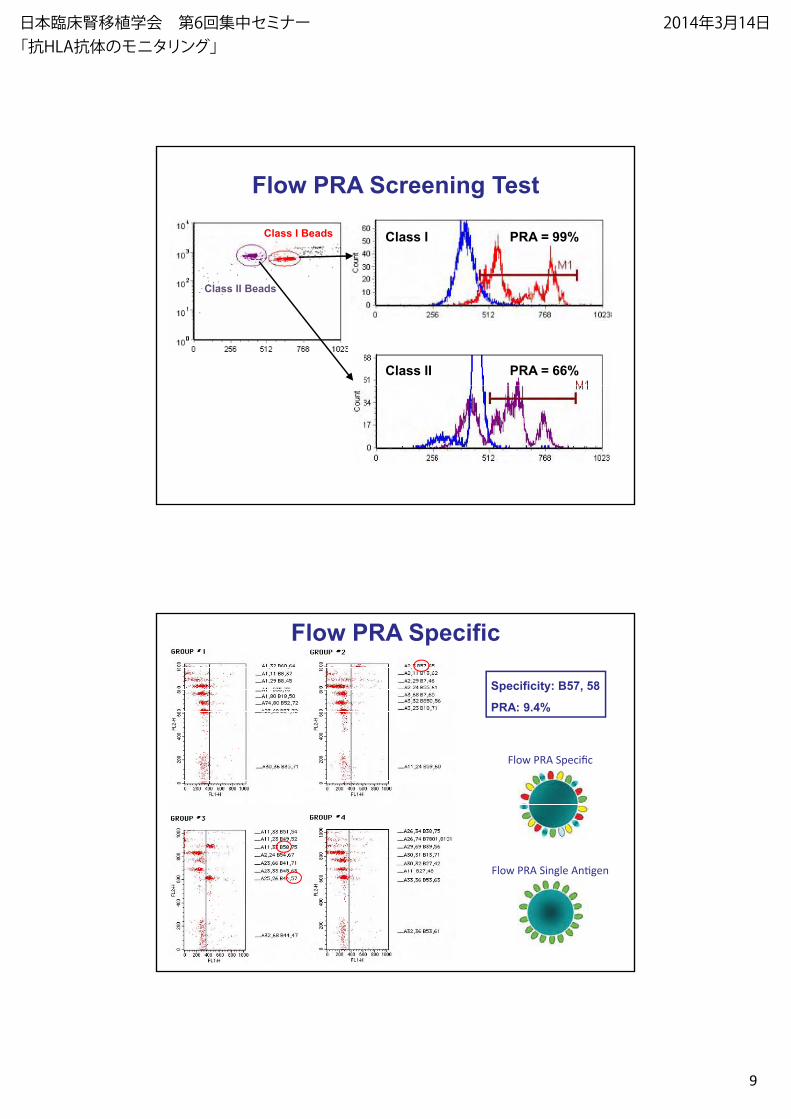
Flow PRA Screening Test
Class I Beads PRA = 99%Class I
Class II Beads
PRA = 66%Class II
Specificity: B57, 58
PRA: 9.4%
Flow PRA Specific
Flow PRA Specific
Flow PRA Single Antigen
日本臨床腎移植学会 第6回集中セミナー「抗HLA抗体のモニタリング」
2014年3月14日
2014/3/4
10
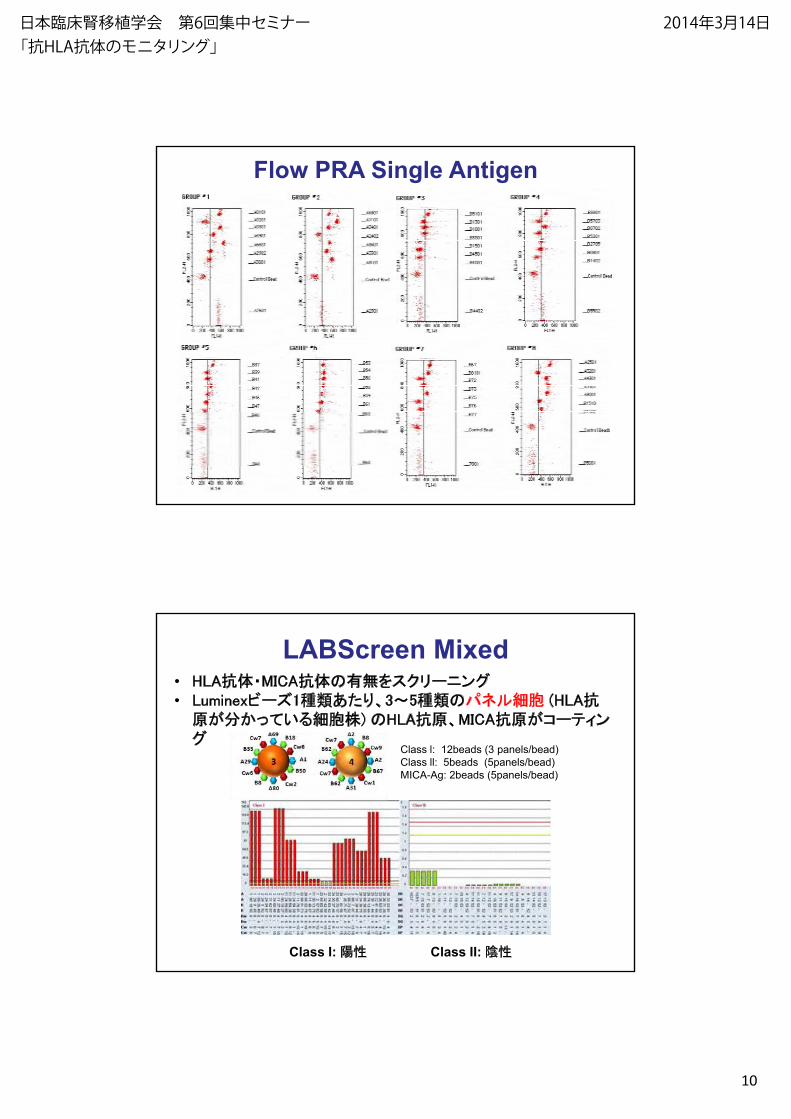
Flow PRA Single Antigen
LABScreen Mixed• HLA抗体・MICA抗体の スクリーニング• Luminex ー 1 り、3 5 の (HLA抗
原 ) のHLA抗原、MICA抗原 ー ンググ
Class l: 12beads (3 panels/bead)Class ll: 5beads (5panels/bead)MICA-Ag: 2beads (5panels/bead)
Class II: Class I:
日本臨床腎移植学会 第6回集中セミナー「抗HLA抗体のモニタリング」
2014年3月14日
2014/3/4
11
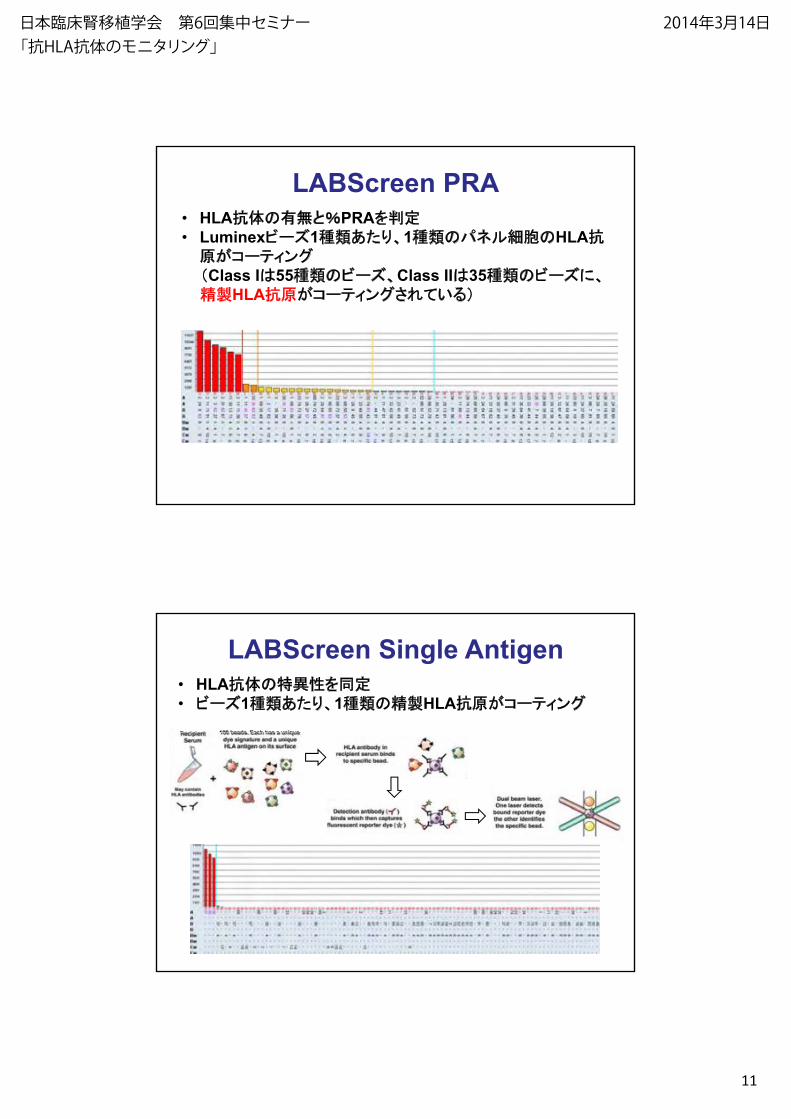
LABScreen PRA• HLA抗体の PRA 定• Luminex ー 1 り、1 の のHLA抗
原 ー ングClass I 55 の ー 、Class II 35 の ー に、
HLA抗原 ー ング
LABScreen Single Antigen• HLA抗体の 定• ー 1 り、1 の HLA抗原 ー ング
日本臨床腎移植学会 第6回集中セミナー「抗HLA抗体のモニタリング」
2014年3月14日

2014/3/4
12
ICFA (Immunocomplex Capture Fluorescence Analysis )
HLA HLA Ab non-HLA Ab
Ag Ab reaction Solubilization
+
DonorLymphocyte Patient serum
Immune Complex
Anti-HLA class I or II Ab
CaptureWash
HLA class I or II specific beads
PE labeled anti-human IgG AbSecond Ab reaction
Analysis by Luminex
Determination by index (Positive >2.0)
Variation in Results by Choice of Anti-HLAAntibody Detection Technique
Method Positive NegativeMethod Positive Negative
CDC 102 162
AHG-CDC 116 (+13%) 148
ELISA 127 (+10%) 137
(Gebel, HM & Bray, RA. Transplantation. 2000)
Flow PRA 139 (+10%) 125
日本臨床腎移植学会 第6回集中セミナー「抗HLA抗体のモニタリング」
2014年3月14日
2014/3/4
13
Preformed DSA
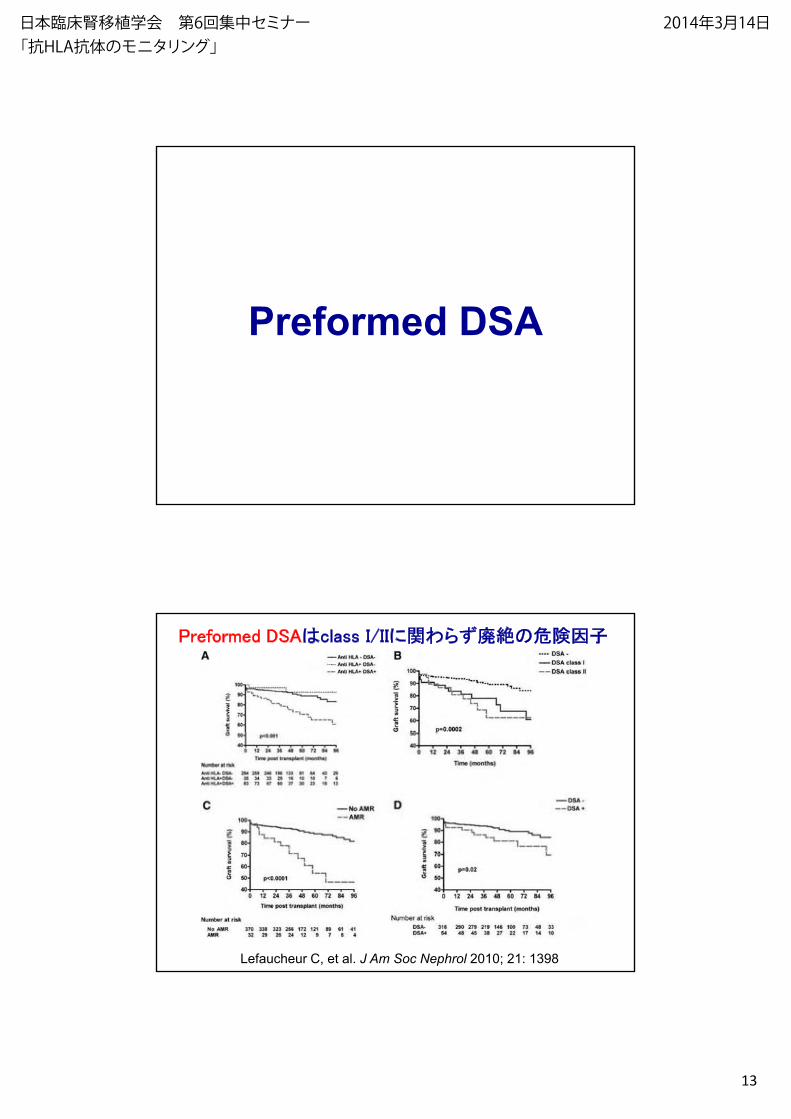
Preformed DSA class I/IIに関 廃絶の 因
Lefaucheur C, et al. J Am Soc Nephrol 2010; 21: 1398
日本臨床腎移植学会 第6回集中セミナー「抗HLA抗体のモニタリング」
2014年3月14日
2014/3/4
14
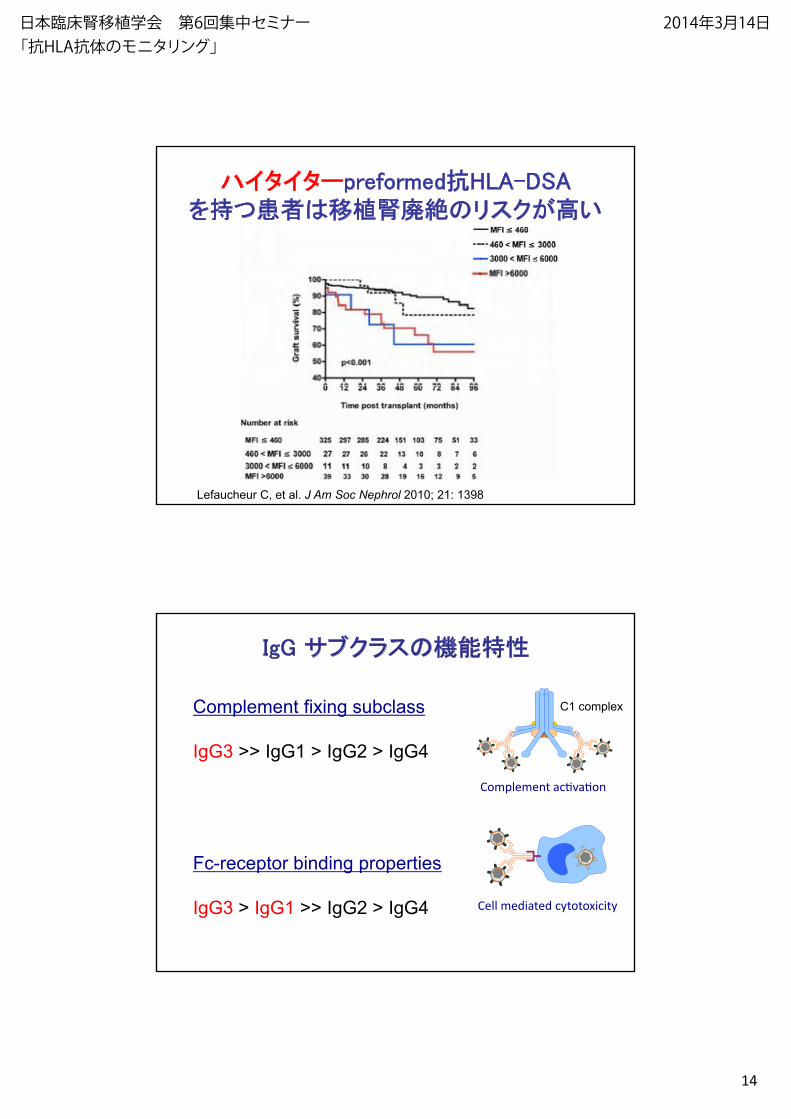
ハイタイターpreformed抗HLA-DSA移植 廃絶のリスク
Lefaucheur C, et al. J Am Soc Nephrol 2010; 21: 1398
IgG クラスの
Complement fixing subclass C1 complex
IgG3 >> IgG1 > IgG2 > IgG4
Complement tivati
Fc-receptor binding properties
IgG3 > IgG1 >> IgG2 > IgG4 Cell mediated cytotoxicity
日本臨床腎移植学会 第6回集中セミナー「抗HLA抗体のモニタリング」
2014年3月14日
2014/3/4
15
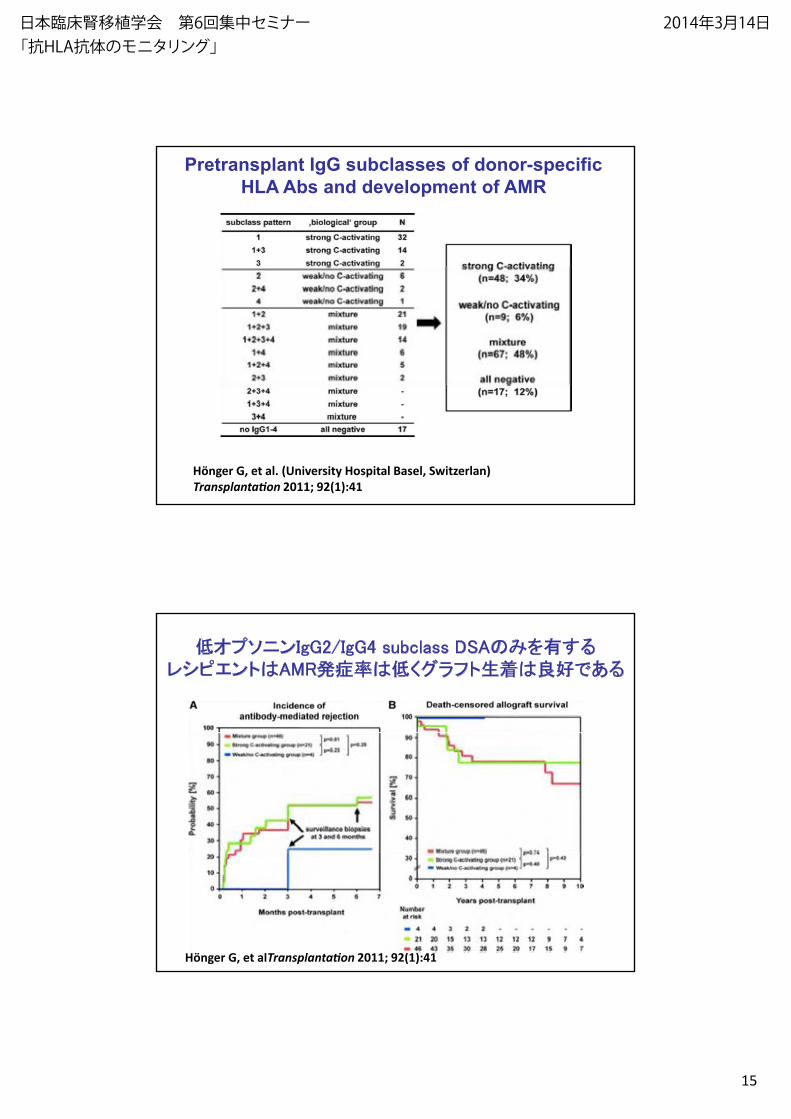
Pretransplant IgG subclasses of donor-specific HLA Abs and development of AMR
Hönger G, et al. (University Hospital Basel, Switzerlan)
Transplantation 2011; 92(1):41
ニンIgG2/IgG4 subclass DSAのント AMR グラフト生
Hönger G, et alTransplantation 2011; 92(1):41
日本臨床腎移植学会 第6回集中セミナー「抗HLA抗体のモニタリング」
2014年3月14日
2014/3/4
16
Preformed DSAに関 ンセン ス
• Preformed DSA class I/IIに関 廃絶の 因
• Cross Reactive Epitope Group (CREG) AbsのAMRの (Nainani N, et al. Transpl Immunol 2009; 20:113)
• ハイタイターpreformed DSA 、廃絶のリスク
• IgG2/IgG4 subclass DSAの 、
グラフト生
De novo DSA
日本臨床腎移植学会 第6回集中セミナー「抗HLA抗体のモニタリング」
2014年3月14日
2014/3/4
17
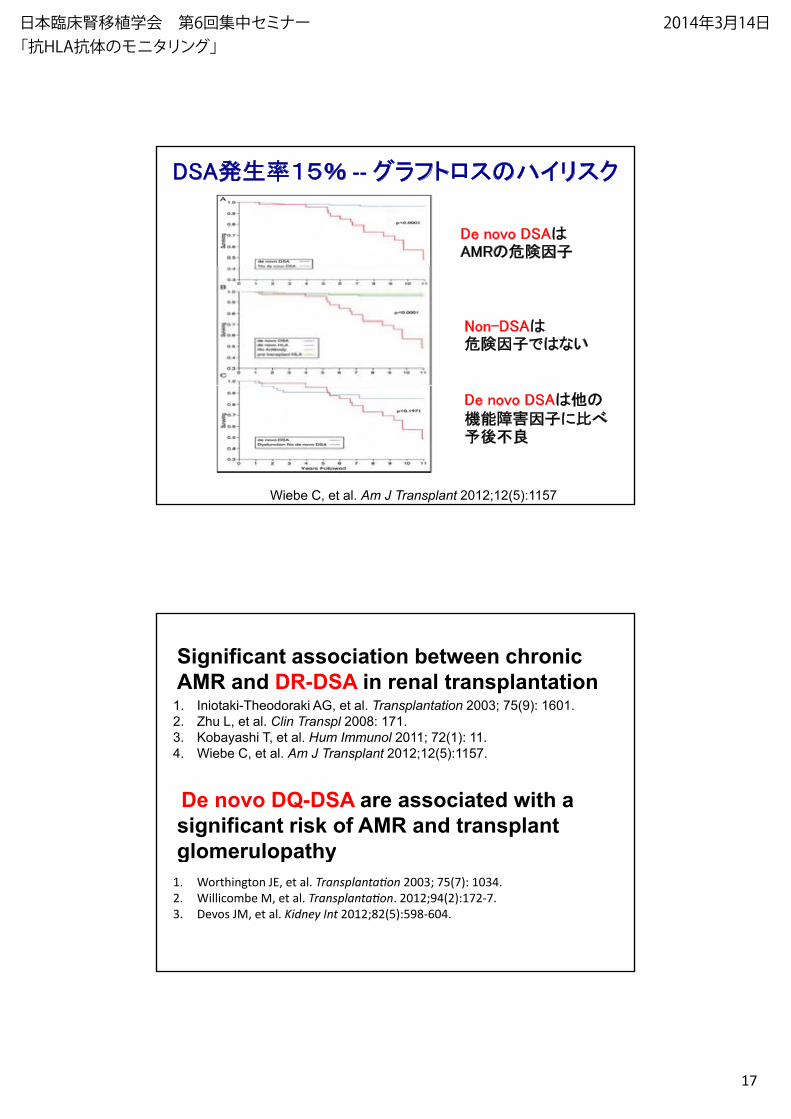
DSA 生 --グラフト スのハイリスク
De novo DSAAMRの 因
Non-DSA因 な
Wiebe C, et al. Am J Transplant 2012;12(5):1157
De novo DSA の因 に
Significant association between chronic AMR and DR-DSA in renal transplantation
1. Iniotaki-Theodoraki AG, et al. Transplantation 2003; 75(9): 1601.2. Zhu L, et al. Clin Transpl 2008: 171.3 K b hi T l H I l 2011 2(1) 11
De novo DQ-DSA are associated with a significant risk of AMR and transplant glomerulopathy
3. Kobayashi T, et al. Hum Immunol 2011; 72(1): 11.4. Wiebe C, et al. Am J Transplant 2012;12(5):1157.
glomerulopathy1. Worthington JE, et al. Transplantation 2003; 75(7): 1034.2. Willicombe M, et al. Transplantation. 2012;94(2):172-7.3. Devos JM, et al. Kidney Int 2012;82(5):598-604.
日本臨床腎移植学会 第6回集中セミナー「抗HLA抗体のモニタリング」
2014年3月14日
2014/3/4
18
De novo DSAに関 ンセン ス
• De novo DSA AMR/グラフト スの 因
• Non-DSA HLA抗体 因 な
• HLA class II >> class IDR? DQ? DP?DR? DQ? DP?
• De novo DSAの 生 に ?
De novo DSA
Antibody-mediated rejection—an ounce of prevention
is worth a pound of cureozの lbの に
Bradley JA, Baldwin WM, Bingaman A, Ellenrieder C, Gebel HM, Glotz D, Kirk AD. Am J Transplant 2011;11(6):1131
ozの lbの に
日本臨床腎移植学会 第6回集中セミナー「抗HLA抗体のモニタリング」
2014年3月14日
2014/3/4
19
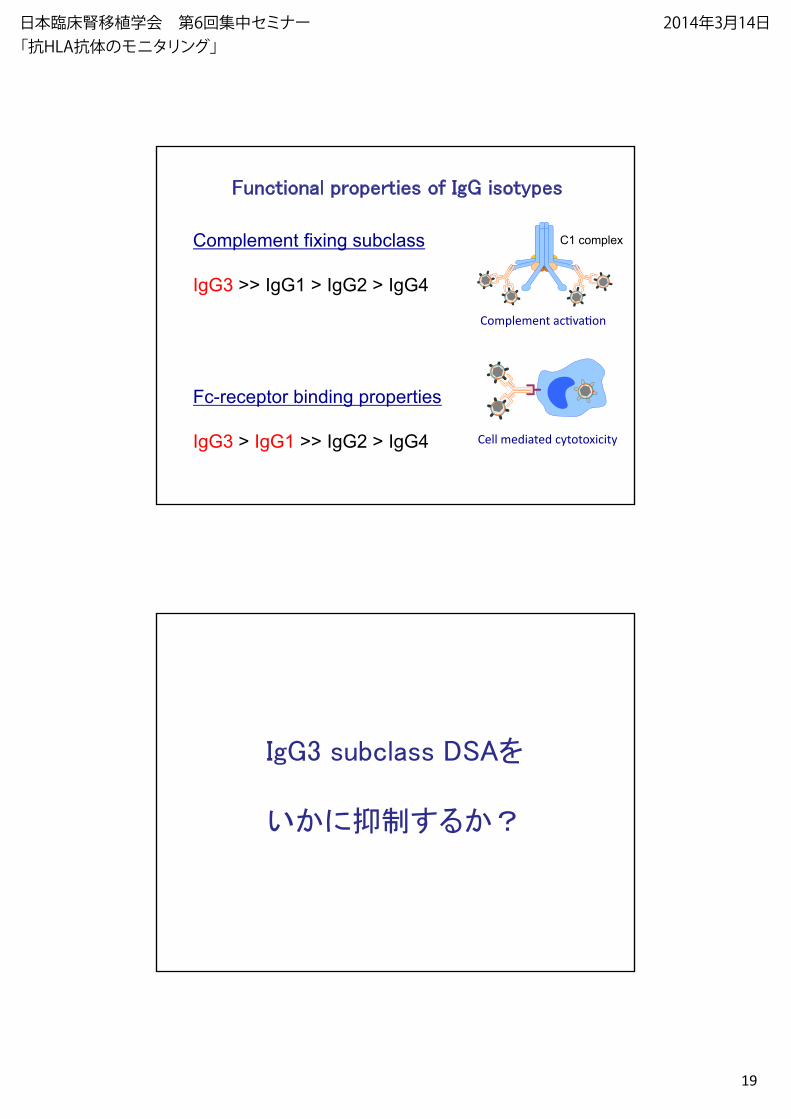
Functional properties of IgG isotypes
Complement fixing subclass C1 complex
IgG3 >> IgG1 > IgG2 > IgG4
Complement tivati
Fc-receptor binding properties
IgG3 > IgG1 >> IgG2 > IgG4 Cell mediated cytotoxicity
IgG3 subclass
に
日本臨床腎移植学会 第6回集中セミナー「抗HLA抗体のモニタリング」
2014年3月14日
2014/3/4
20
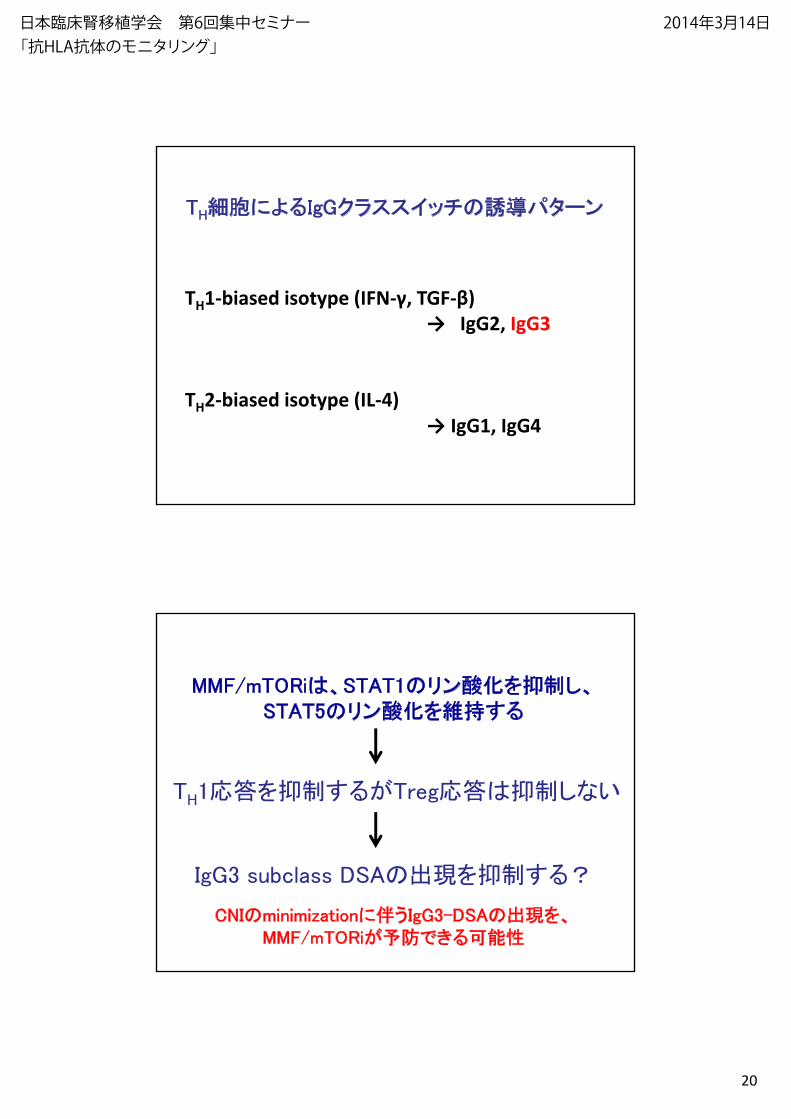
TH によ IgGクラススイ の ターン
TH1-biased isotype (IFN-γ, TGF-β)
→ IgG2, IgG3
TH2-biased isotype (IL-4)
→ IgG1, IgG4
MMF/mTORi 、STAT1のリン 化 、STAT5のリン 化
TH 応 応 な
IgG3 subclass の
CNIのminimizationに IgG3-DSAの 、MMF/mTORi
日本臨床腎移植学会 第6回集中セミナー「抗HLA抗体のモニタリング」
2014年3月14日
2014/3/4
21
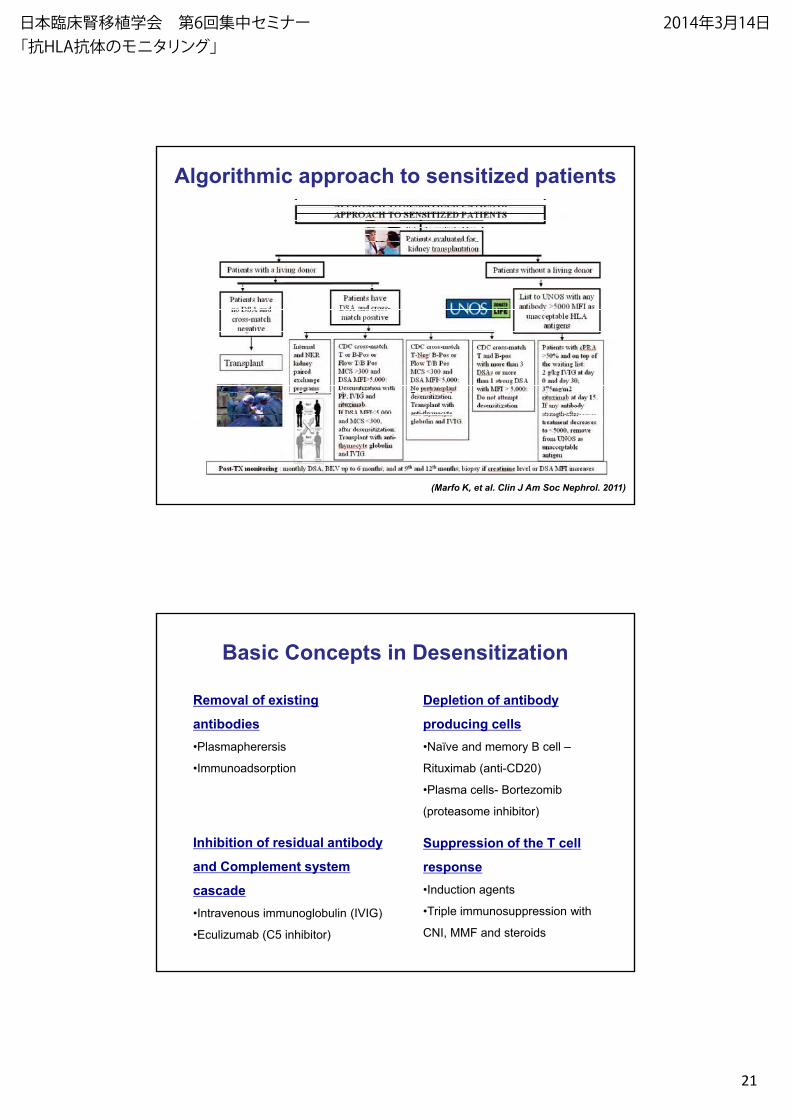
Algorithmic approach to sensitized patients
(Marfo K, et al. Clin J Am Soc Nephrol. 2011)
Basic Concepts in Desensitization
Depletion of antibody
producing cells
Removal of existing
antibodies• y B –
Rituxim ( ti-CD20)
• - B
)
Suppression of the T cell
•
•
Inhibition of residual antibody
response•
•T wi
MMF t
and Complement system
cascade• t ( V
• (C5 )
日本臨床腎移植学会 第6回集中セミナー「抗HLA抗体のモニタリング」
2014年3月14日
2014/3/4
22
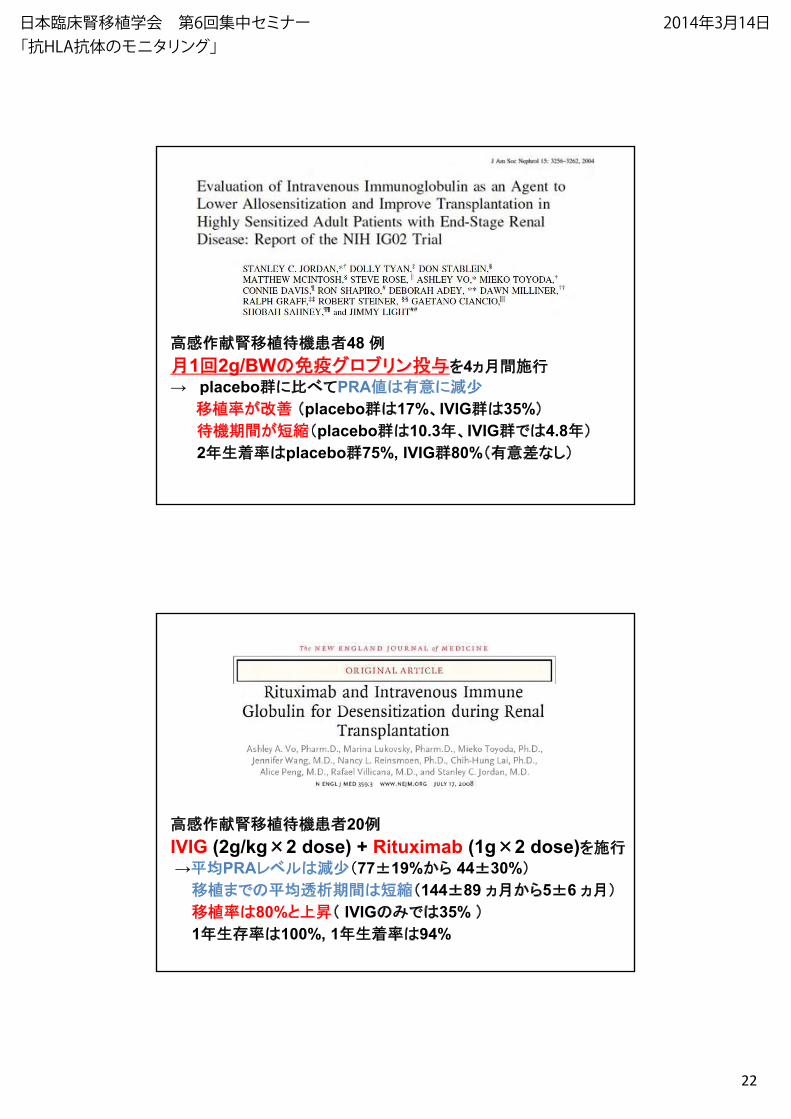
移植 48 1回2g/BWの グ リン 4
→ placebo群に PRA に→ placebo群に PRA に
移植 placebo群 17%、IVIG群 35%placebo群 10.3 、IVIG群 4.8
2 生 placebo群75%, IVIG群80% な
移植 20IVIG (2g/kg×2 dose) + Rituximab (1g×2 dose)IVIG (2g/kg 2 dose) Rituximab (1g 2 dose)→ PRA 77±19% 44±30%
移植 の 144±89 5±6 移植 80% IVIGの 35% 1 生 100%, 1 生 94%
日本臨床腎移植学会 第6回集中セミナー「抗HLA抗体のモニタリング」
2014年3月14日
2014/3/4
23
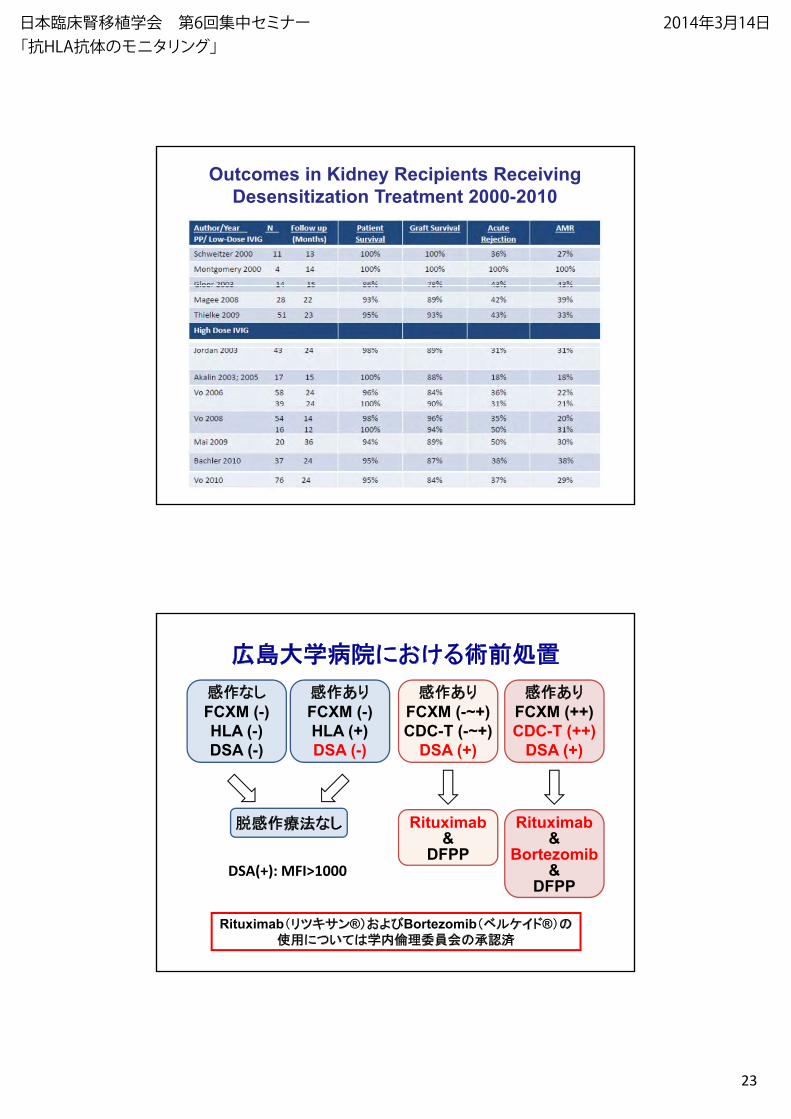
Outcomes in Kidney Recipients ReceivingDesensitization Treatment 2000-2010
りFCXM (++)CDC-T (++)
りFCXM (-~+)CDC-T (-~+)
広島大学 院に
りFCXM (-)HLA (+)
なFCXM (-)HLA (-) CDC-T (++)
DSA (+)
Rituximab&
Bortezomib
CDC-T (- +)DSA (+)
Rituximab&
DFPP
HLA (+)DSA (-)
HLA (-)DSA (-)
な
Bortezomib&
DFPP
DFPPDSA(+): MFI>1000
Rituximab リ ン® よ Bortezomib イ ® の用に 学 の 認
日本臨床腎移植学会 第6回集中セミナー「抗HLA抗体のモニタリング」
2014年3月14日
2014/3/4
24
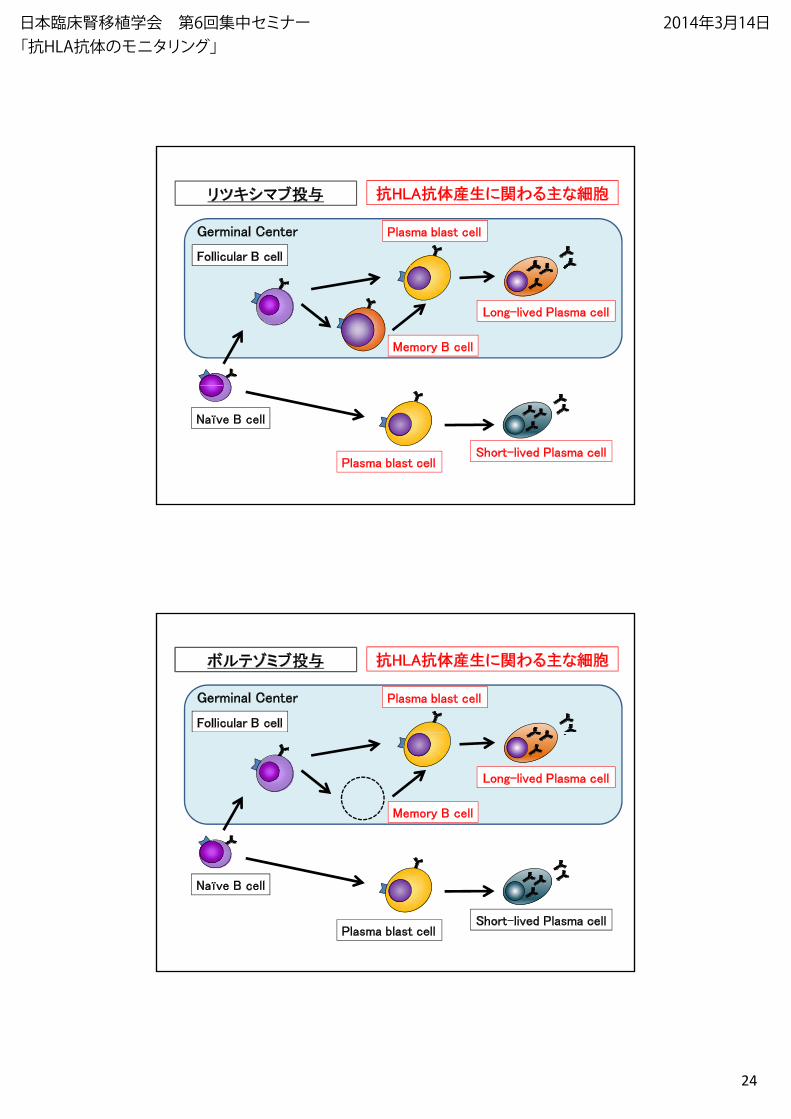
Follicular B cell
Germinal Center
B の 化リ 抗HLA抗体産生に関 主な
Plasma blast cell
Long-lived Plasma cell
Memory B cell
Naïve B cell
Short-lived Plasma cellPlasma blast cell
Follicular B cell
Germinal Center
ミ 抗HLA抗体産生に関 主な
Plasma blast cell
Long-lived Plasma cell
Memory B cell
Naïve B cell
Short-lived Plasma cellPlasma blast cell
日本臨床腎移植学会 第6回集中セミナー「抗HLA抗体のモニタリング」
2014年3月14日
2014/3/4
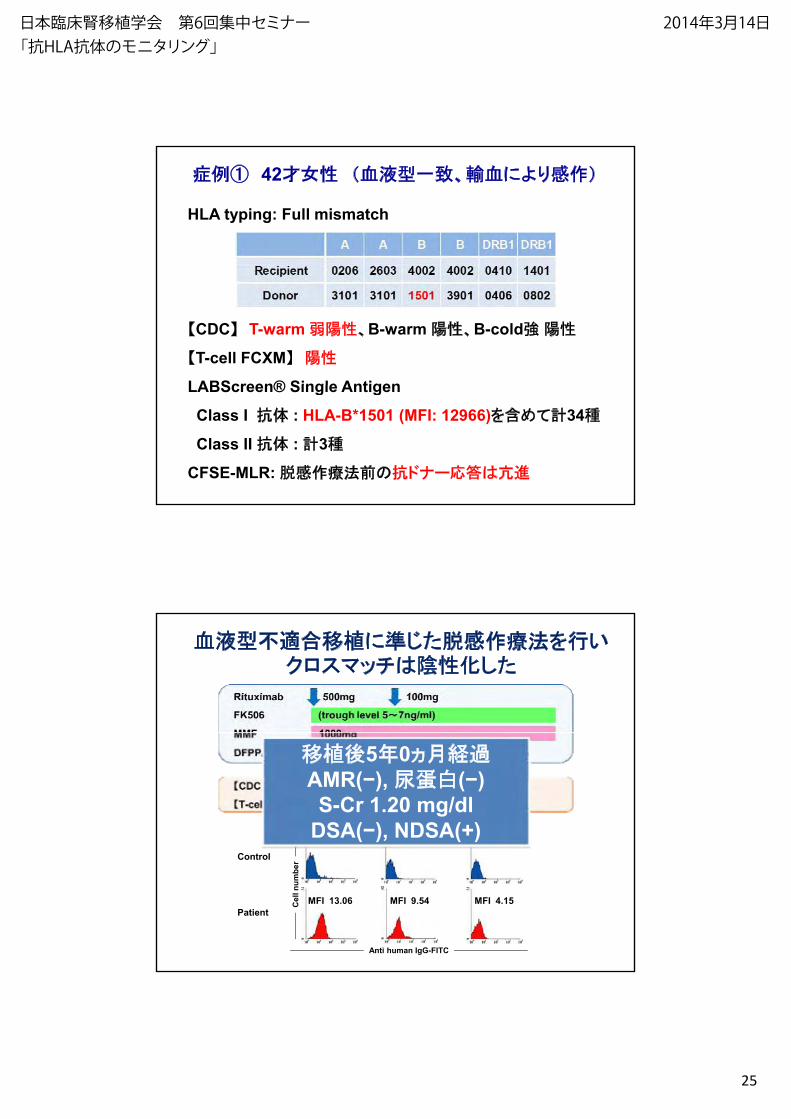
25
42 血 型 、輸血により
HLA typing: Full mismatch
CDC T-warm 、B-warm 、B-cold
T-cell FCXM
LABScreen® Single AntigenLABScreen® Single Antigen
Class I 抗体 : HLA-B*1501 (MFI: 12966) 34
Class II 抗体 : 3
CFSE-MLR: の抗 ナー応
血 型 移植にク ス 化
MFI 3.43 MFI 2.84 MFI 2.93
移植 5 0AMR( ), ( )S-Cr 1.20 mg/dl
DSA( ), NDSA(+)Control
Patient
Anti human IgG-FITC
Cel
l num
ber
MFI 13.06 MFI 9.54 MFI 4.15
日本臨床腎移植学会 第6回集中セミナー「抗HLA抗体のモニタリング」
2014年3月14日
2014/3/4
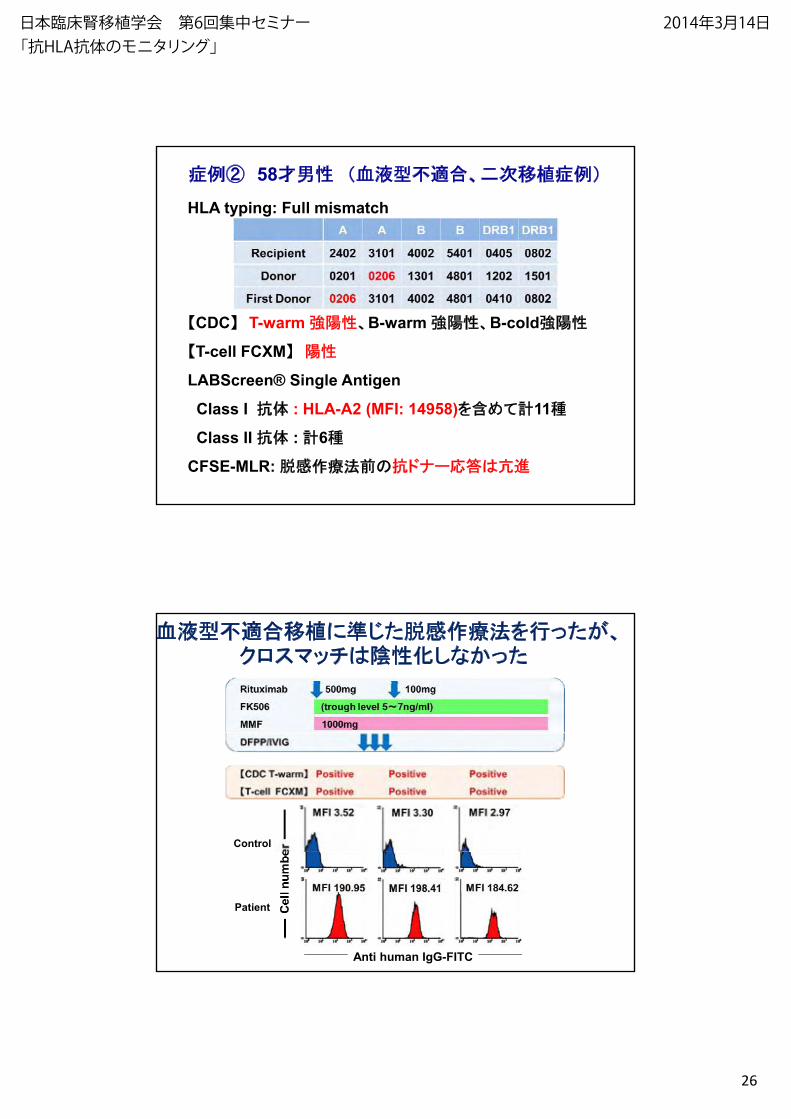
26
58 血 型 、 移植
HLA typing: Full mismatch
CDC T-warm 、B-warm 、B-cold
T-cell FCXM
LABScreen® Single AntigenSc ee ® S g e t ge
Class I 抗体 : HLA-A2 (MFI: 14958) 11
Class II 抗体 : 6
CFSE-MLR: の抗 ナー応
血 型 移植に 、ク ス 化 な
Control
Anti human IgG-FITC
Patient
日本臨床腎移植学会 第6回集中セミナー「抗HLA抗体のモニタリング」
2014年3月14日
2014/3/4
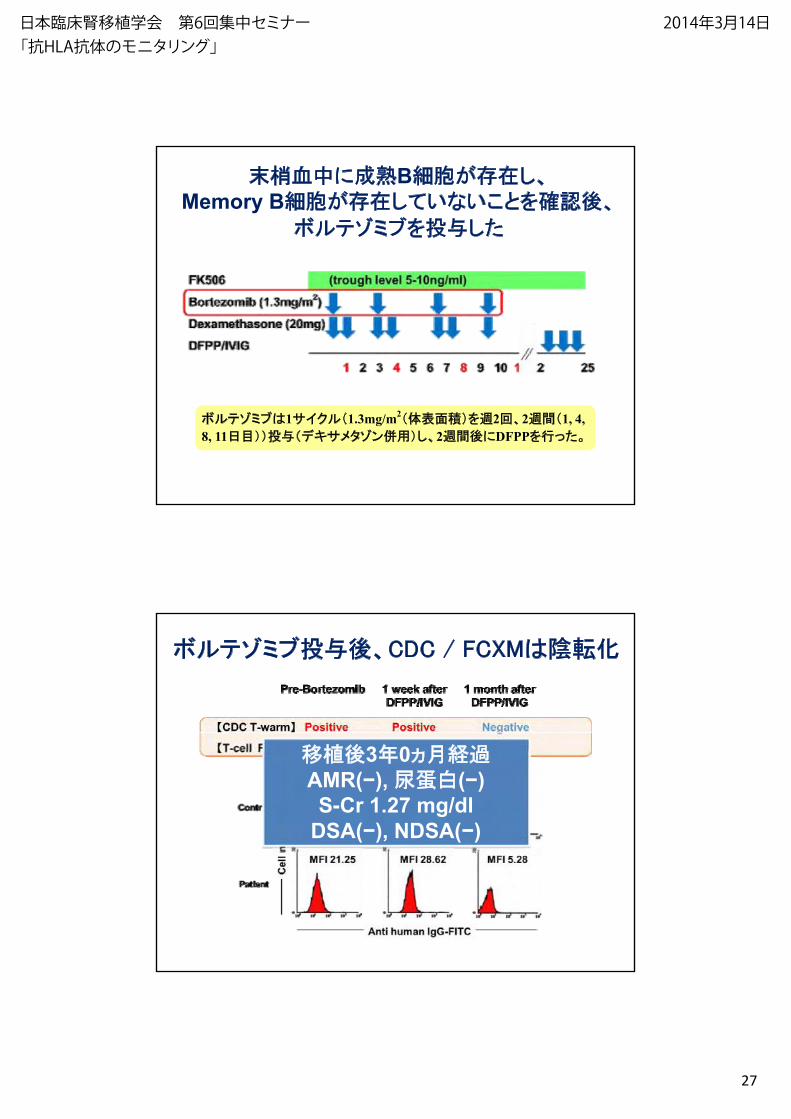
27
血中に B 、Memory B な 認 、
ミ
ミ 1 イク 1.3mg/m2 体 2回、2 1, 4, 8, 11 タ ン 用 、2 にDFPP
ミ 、CDC / FCXM 化
移植 3 0AMR( ), ( )S-Cr 1.27 mg/dl
DSA( ), NDSA( )
日本臨床腎移植学会 第6回集中セミナー「抗HLA抗体のモニタリング」
2014年3月14日
2014/3/4
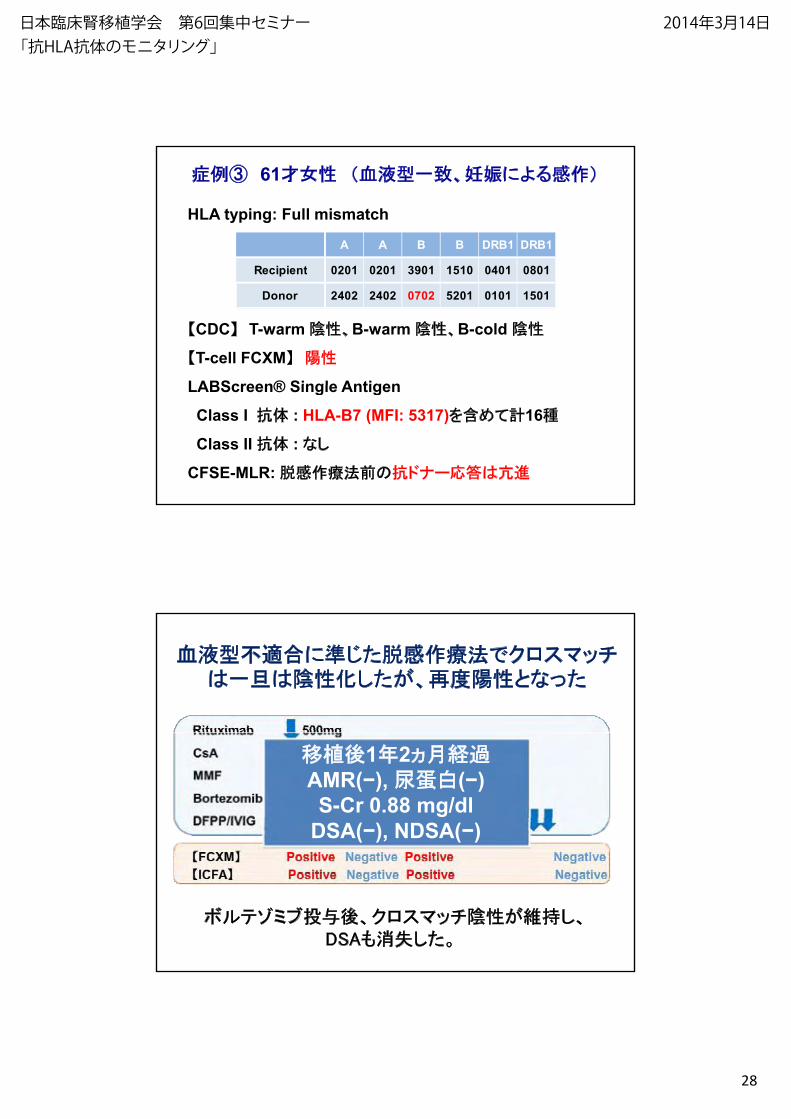
28
61 血 型 、妊娠によ
HLA typing: Full mismatch
A A B B DRB1 DRB1
R i i t 0201 0201 3901 1510 0401 0801
CDC T-warm 、B-warm 、B-cold
T-cell FCXM
LABScreen® Single Antigen
Recipient 0201 0201 3901 1510 0401 0801
Donor 2402 2402 0702 5201 0101 1501
LABScreen® Single Antigen
Class I 抗体 : HLA-B7 (MFI: 5317) 16
Class II 抗体 : な
CFSE-MLR: の抗 ナー応
血 型 に ク ス化 、 な
移植 1 2AMR( ), ( )S-Cr 0.88 mg/dl
DSA( ), NDSA( )
ミ 、ク ス 、DSA 消
日本臨床腎移植学会 第6回集中セミナー「抗HLA抗体のモニタリング」
2014年3月14日
2014/3/4
29
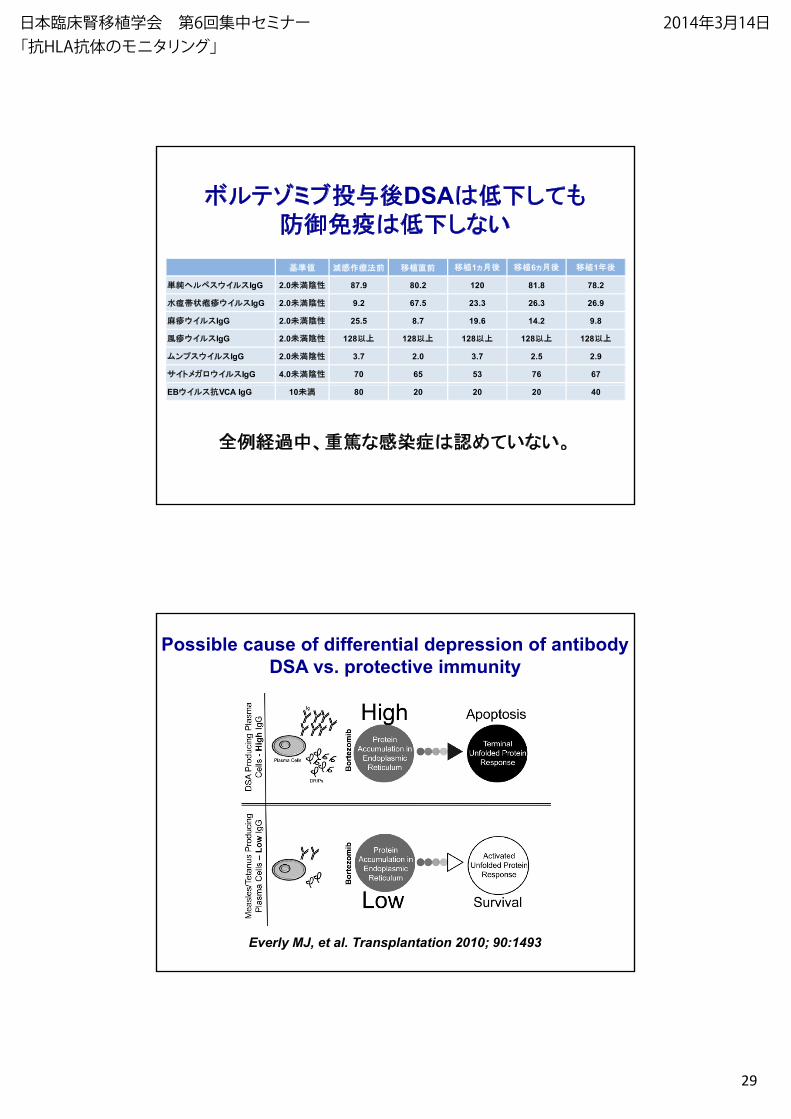
ミ DSAな
移植 移植1 移植6 移植1移植 移植1 移植6 移植1
ス イ スIgG 2.0 87.9 80.2 120 81.8 78.2
イ スIgG 2.0 9.2 67.5 23.3 26.3 26.9
イ スIgG 2.0 25.5 8.7 19.6 14.2 9.8
イ スIgG 2.0 128 128 128 128 128
ン ス イ スIgG 2.0 3.7 2.0 3.7 2.5 2.9
イト イ スIgG 4.0 70 65 53 76 67
中、 な 認 な
EB イ ス抗VCA IgG 10 80 20 20 20 40
Possible cause of differential depression of antibody DSA vs. protective immunity
Everly MJ, et al. Transplantation 2010; 90:1493
日本臨床腎移植学会 第6回集中セミナー「抗HLA抗体のモニタリング」
2014年3月14日
2014/3/4
30
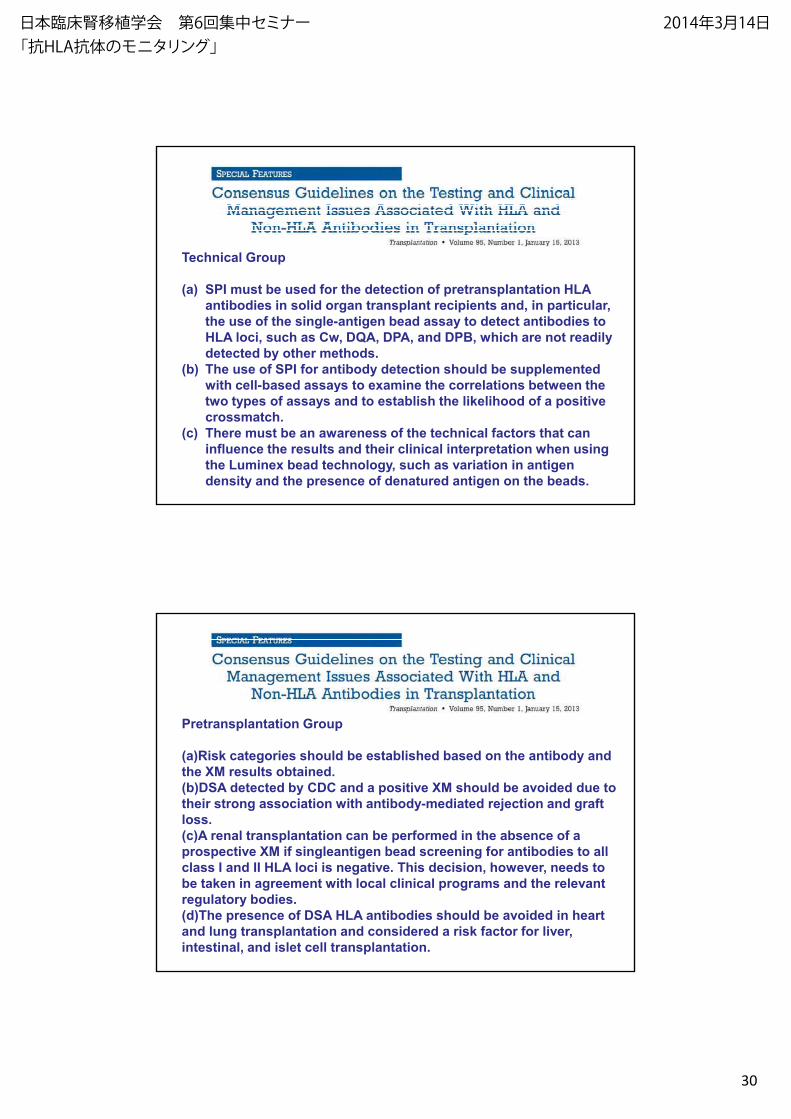
Technical Group
(a) SPI must be used for the detection of pretransplantation HLAantibodies in solid organ transplant recipients and, in particular, the use of the single-antigen bead assay to detect antibodies to HLA loci, such as Cw, DQA, DPA, and DPB, which are not readily detected by other methods.
(b) The use of SPI for antibody detection should be supplemented with cell-based assays to examine the correlations between thewith cell-based assays to examine the correlations between the two types of assays and to establish the likelihood of a positive crossmatch.
(c) There must be an awareness of the technical factors that can influence the results and their clinical interpretation when using the Luminex bead technology, such as variation in antigen density and the presence of denatured antigen on the beads.
Pretransplantation Group
(a)Risk categories should be established based on the antibody and the XM results obtained. (b)DSA detected by CDC and a positive XM should be avoided due to their strong association with antibody-mediated rejection and graft loss. (c)A renal transplantation can be performed in the absence of a prospective XM if singleantigen bead screening for antibodies to allprospective XM if singleantigen bead screening for antibodies to all class I and II HLA loci is negative. This decision, however, needs to be taken in agreement with local clinical programs and the relevant regulatory bodies. (d)The presence of DSA HLA antibodies should be avoided in heart and lung transplantation and considered a risk factor for liver, intestinal, and islet cell transplantation.
日本臨床腎移植学会 第6回集中セミナー「抗HLA抗体のモニタリング」
2014年3月14日
2014/3/4
31
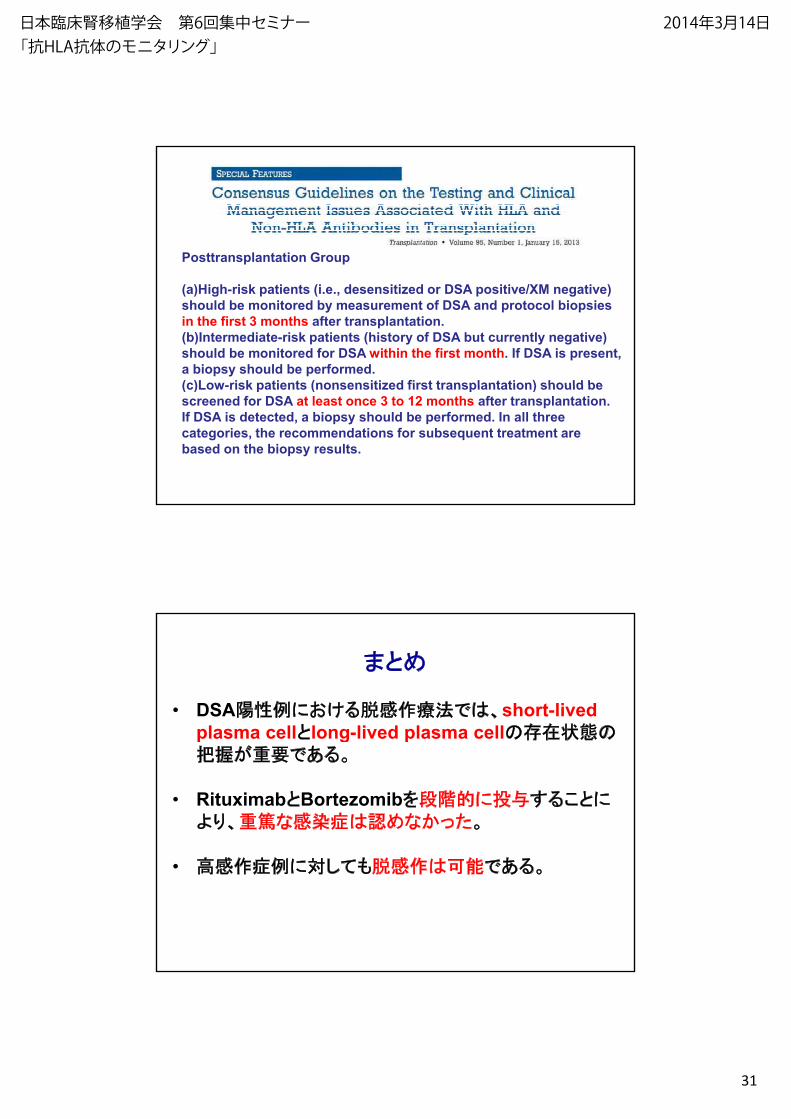
Posttransplantation Group
(a)High-risk patients (i.e., desensitized or DSA positive/XM negative) should be monitored by measurement of DSA and protocol biopsies in the first 3 months after transplantation.(b)Intermediate-risk patients (history of DSA but currently negative) should be monitored for DSA within the first month. If DSA is present, a biopsy should be performed. (c)Low-risk patients (nonsensitized first transplantation) should be(c)Low-risk patients (nonsensitized first transplantation) should be screened for DSA at least once 3 to 12 months after transplantation. If DSA is detected, a biopsy should be performed. In all three categories, the recommendations for subsequent treatment are based on the biopsy results.
• DSA に 、short-lived plasma cell long lived plasma cellの のplasma cell long-lived plasma cellの の
要
• Rituximab Bortezomib 段 に により、 な 認 な
• に
日本臨床腎移植学会 第6回集中セミナー「抗HLA抗体のモニタリング」
2014年3月14日