Embed Size (px)
Citation preview

Int. J. Oral Maxillofac. Surg. 1986: 15: 93-97
(Key words: C)'SI. latent bone; mandible; C)'SI. stafne)
Idiopathic lingual mandibular bone"depression"
M. A. POGREL, K. SANDERS AND L. S. HANSEN
Divisions ofOral and Maxillofacial Surgery and Oral Pathology. University ofCalifornia, Sail Francisco.USA, Department of Oral and Maxillofacial Surgery. Peterborough District Hospital. Peterborough.England
ABSTRACT - A case of Stafne's idiopathic lingual bone depression is described. This occurred in the classical position below the mandibularmolars. On surgical exploration, the defect was found to contain a lymphnode rather than the more usual salivary tissue. This may throw somelight on the possible etiology of this condition.
(Accepted for publication 4 January 1985)
The idiopathic lingual mandibular bone depression was first described by Stafne in19423°, who reported 35 cases, and since thattime there have been many reports of singlecases and also small series of cases. Reviewof the literature reveals some confusion because of the many different names appliedto this lesion, resulting partly from the uncertainty of its etiology. Terms which havebeen used include: mandibular embryonicdefect", latent bone cyst":", static bone defeet', static bone cavity', aberrant salivargland defect', mandibular salivary gland inelusion", developmental lingual mandibularsalivary gland depression", lingual corticalmandibular defect", developmental mandibular bone defect", and idiopathic bonecavity28-30, which was the term originallyusedby Stafne.
The lesion is always asymptomatic and is
usually a chance radiographic finding. Theappearance on the radiograph is of a welldefined cystic lesion normally below themandibular molars and lying below the inferior alveolar canal. There is no obviousconnection with other dental structures andassociated teeth are not involved. It isknown from cases that have been investigated surgically that although lesions appear cystic on radiographs, the lesion in factrepresents a defect on the lingual side ofthe mandible in that the lingual plate isdisplaced buccally in this region and thatthere is no actual cyst. There is no connection between these lesions and the traumatic, hemorrhagic or solitary bone cyst.
The incidence of these lesions is in somedoubt, but LILLY et al.J6 found 2 casesamong 1,287 dentists given a panoramicradiograph at a meeting of The American

94 POGREL, SANDERS AND HANSEN
Dental Association. A similar study of4,963panoramic radiographs on adult males attending a Veteran Administration Dental
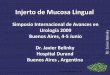
Fig. 1. Radiograph showing well-circumscribedradiolucent lesion beneath lower right molars.
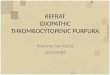
Fig. 2. Soft tissue mass (t) reflected from lingualbone depression.
Clinic", showed 18 of these lesions, suggesting an instance of 1 in 276 in adultmales. A more recent Veterans Administration Study?showed 13lesions in 2,693 panoral radiographs. In studies on cadaver mandibles, HARVEY & NOBLE II , found 7 cavitiesin 950 mandibles, whilst KAy14 noted 11idiopathic bone cavities in 1,385 mandibles,which again shows a similar level of incidence.
Males appear to be affected more frequently than females though there seems tobe no reason for this. The peak ages ofdiscovery appear to be in the 3rd and 4thdecades. To date, it has not been describedin young children.
Case reportAn otherwise fit and healthy 35-year-old malewas referred to hospital because his general dentist had noted a radiolucent lesion towards thelower border of the right mandible on routinepanoramic radiography (Fig. 1). The lesion wascompletely asymptomatic. There was no associated pathologic findings, and the nearest teethwere vital and asymptomatic. The lesion was situated below the inferior alveolar canal.
A provisional diagnosis ofa Stafne's idiopathicbone cavity was made, but it was not possible toobtain a diagnostic sialogram of the area, andbecause of the wish for a definitive diagnosis onboth the patient's and the surgeon's behalf, thearea was explored via an extra-oral approachunder general anesthesia.
At operation, the buccal side of the mandiblein this area was explored first. The buccal platewas found to be slightly expanded in this areaand thinned with a blue undertone to it. Attention was then turned to the lingual aspect of themandible in the affected region, and here a defect3 m long by 1 em in height was found; it wasfound to be filled with soft tissue (Fig. 2). Thesoft tissue was gently retracted from the areaand dissected from the rest of the submandibulartissues and submitted for histologic microscopicexamination. The cavity was then seen to besmooth walled and rather than a perforation ofthe Iigual plate; it was seen that the defect represented a buccal movement of the lingual plate,

LINGUAL BONE CAVITY 95
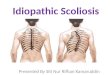
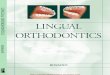
such that buccal and lingual plates were virtuallyin contact (Fig. 3). Following this explorationand excision, the wound was closed and healingwas quite uneventful. Histological examinationof the submitted specimen revealed that it was anessentially normal lymph node. There was noevidence of salivary gland tissue in the sectionsexamined (Fig. 4). The diagnosis was reactivelymphoid hyperplasia, lymph node.
DiscussionIt is evident from a review of cases in theliterature that the Stafne's idiopathic bonecavity is a benign lesion, but its etiology andwhat it represents remain an enigma. Mostreports agree that they do not representtrue cysts, but that they are localized clearly
Fig. 3. Resultant empty lingual bone depression.
Fig. 4. Low power view of lymph node exhibitingmild reactive lymphoid hyperplasia (H & E stain,magnification x 10).
circumscribed depressions in the lingual aspect of the mandible, usually the molar region, though there are isolated reports ofthem occurring in more anterior sites inthe mandibleI.J.4·6.8.1s,I7.18.21-24. Early reports onthese lesions noted a variety of differentcontents, though there are only 2 previousreports of cavities containing lymphoid tissue4.J1 ; however, no photomicrographs wereshown. In other cases the cavity has beenempty', contained fibrous connective tissue' , muscle" and fat, collagen, nerve, striated muscle and vascular anomalies". Mostrecent reports, however, have stressed thatthese lesions virtually always contain a lobule of the submandibular salivary gland andthat sialography can be used in the diagnosis of these lesions' <", Since their benignnature has been confirmed many times,many authorities do not advocate surgicalexploration to confirm the diagnosis'<",
The etiology remains in doubt. Therehave been many differing theories. It hasbeen suggested that they may be congenital,perhaps due to an incorporation of salivarytissue during ossification of the mandible",but this is unlikely since the lesions havenever been found in childhood. That theyare developmental has been further shownfrom cases where earlier X-rays are available , showing that the lesions were not present some years previously, and that therefore they must have developed",
Most authorities appear to agree thatthese lesions are probably caused by a pressure phenomenon on the lingual side of themandible causing pressure resorption ofbone in the affected area. Since most of thelesions investigated contain lobules of thesubmandibular salivary gland, it has beenassumed that the pressure is caused by somehyperplasia of the salivary gland, though itis sometimes difficult to visualize quite howthis could happen. In the handful of casesdescribed in the anterior region of the mandible, these again appear to be filled with

96 POGREL, SANDERS AND HANSEN
salivary tissue. Presumably in the anteriormandible, it is the sublingual salivary glandor an aberrant salivary gland which hasundergone hyperplasia. Though the lesionsthemselves are basically benign, there is, ofcourse, no reason why a salivary gland tumor cannot develop within one of these salivary gland inclusions, and this has in factbeen reported". In the 2 previous cases described containing lymphoid tissue, andpresumably also in this 3rd, present case, itmay be that the pressure was exerted by thesubmandibular salivary gland and that oneof the submandibular lymph nodes, beingclosely associated with the gland, was involved in the pressure-causing phenomenon.KAyl4 strongly agreed with THm,1A3, andWORTH34 noted that virtually all of theselesions occur in the area where the facialartery is in close relation to the mandibleand that resorption may be caused by ananomaly in the artery in a similar way asan aortic aneurysm causing resorbtion ofribs. This hypothesis is supported by a casewhich shows vascular abnormalities associated with the defect", but in fact, the majority of reports have not documented thisfact. Others have postulated that this lesionmay be a "chicken and egg" type phenomenon, in that there may be a primary failureof ossification causing the lesion; then, thenearest soft tissue organ will fill the gap; inmost cases this happens to be the submandibular salivary gland, but in other cases itcan be other structures, such as a lymphnode in our particular case.
SummaryThis paper describes the 3rd reported caseofa Stafne's idiopathic bone cavity containing lymphoid tissue, but it may be the firstcase containing a complete lymph node. Itis assumed that this is one of the submandibular lymph nodes, which could have beenpushed against the mandible by hyperplasia
of the salivary gland causing bony resorption, or it could be that the lymph nodewas incorporated in the development of themandible.
This interesting lesion, which is nowknown to occur between 1 in 150 and 1 in300 persons remains something of anenigma.
ReferencesI. ABRAMSON, A. A.: Ectopic submaxillary
gland in the mandible. Report of a case.J.A.D.A.1966:73: II 14-1 II 6.
2. AMARAL, W. J. & JACOBS, D. S.: Aberrantsalivary gland defect in the mandible. Reportof a case. Oral Surg, 1961: 14: 748-752.
3. ARAICllE, M. & BRODE, H.: Aberrant salivarygland tissue in the mandible. Oral Surg, 1959:12: 727-729.
4. BERGENlIOLTZ, A. & PERSSON, G.: Idiopathicbone cavities: a report of 4 cases. Oral Surg,1963: 16: 703-712.
5. BERNSTEIN, H. E, LAM, R. C. & POMIJE, F.\V.: Static bone cavities of the mandible. Review of the literature and report of case. J.Oral Surg, 1958: 16: 46-52.
6. CAMILLERI, G.: Salivary gland inclusion in themandible. Br. Dent. J. 1963: 114: 515-516.
7. CIIOUKAS, N. C. & TOTO, P. D.: Etiology ofstatic bone defects of the mandible. J. OralSurg, 1960: 18: 16-20.
8. CONNOR, M. S.: Anterior lingual mandibularbone concavity. Oral Surg, 1979: 48: 413--414.
9. CORRELL, R. \V., JENSEN, J. L. & RHYNE, R.R.: Lingual cortical mandibular defects. Oral
. Surg, 1980: 50: 287-291.10. FORDYCE, G. L.: The probable nature of the
so-called latent haemorhagic cysts of themandible. Br. Dent. J. 1956: 101: 40--42.
II. HARVEY, \V. & NOBLE, H. W.: Defects on thelingual surface of the mandible ncar the angle.Br. J. Oral Surg, 1968: 6: 75-83.
12. JACOBS, M. H.: The traumatic bone cyst. OralSurg, 1955: 8: 940-969.
13. KARMIOL, M. & WALSH, R. F.: Incidence ofstatic bone defect of the mandible. Oral Surg,1968: 26: 225-228.
14. KAY, L. \V.: Some anthropologic investigations of interest to oral surgeons. Int. J. OralSurg, 1974: 3: 369-379.
15. LANGLAIS, R. P., COTrONE, J. & KASLE, M.J.: Anterior and posterior lingual depressions

LINGUAL BONE CAVITY 97
of the mandible. J. Oral Surg, 1976: 34:502-509.
16. LILLY, G. E., SITI!'.'ER, M., IRBY, W B. &TIECKE, R. W: Oral health evaluation: analysis of radiographic findings. J.A.D.A. 1965:71: 635-{j39.
17. MILLER, A. S. & WINNICK, M.: Salivary glandinclusion in the anterior mandible. Oral Surg,1971: 31: 790-797.
18. Mrzoxo, A., KAWABATA, T., NAKA"'O, Y. &MOITGI, K .: Lingual mandibular bone defect- idiopathic bone cavity. Int. J . Oral Surg,1983: 12: 64·-68.
19. OIKARINEN, V.J. & JULKU, M.: An orthopantomographic study of developmental mandibular bone defects. Int. J. Oral Surg, 1974:3: 71-76.
20. OLECH, E. & ARORA, B. K.: Lingual mandibular bone cavity. Oral Surg , 1961: 14:1360-1366.
21. PALLADINO, V. S., ROSE, S. A. & CURREN,T.: Salivary gland tissue in the mandible andStafne's mandibular 'cyst' , J.A .D.A. 1966: 70:388-393.
22. PLEZlA, R. A.: Unusual static bone cavity.Oral Surg, 1977: 43: 979.
23. RICHARD, E. L. & ZISKEVAT, J .: Aberrant salivary gland tissue in the mandible. Oral Surg,1957: 10: 1086--1090.
24. SANDY, J. R. & WILLIAMS, D. M.: Anteriorsalivary gland ' inclusion in the mandible.Pathological entity or anatomical variant? Br.J. Oral Surg, 1981: 19: 223-229.
25. SEWARD, G. R.: Salivary gland inclusions inthe mandible. Br. Dent. J. 1960: 108: 321-325.
26. SHAFER, W. G., HINE M. K. & LEVY, B. M.:A textbook of oral pathology, 4th edit ion . W.B. Saunders Company, Philadelphia, 1983:pp.35-37.
27. SIMPSON, W.: Stafne's mandibular bone defectcontaining a pleomorphic adenoma; report ofa case. J. Oral Surg, 1965: 23: 553-556.
28. STAF!'.'E, E. C.: Oral roentgenographic diagnosis, 3rd edition. W. 8. Saunders Co., Philadelphia 1969, pp. 37-40.
29. STAFNE, E. C.: Value of roentgenograms indiagnosis of the jaws. Oral Surg , 1953: 6:82-92.
30. STAFNE, E. C.: Bone cavities situated nearthe angle of the mand ible. J.A.D.A. 1942: 29:1969-1972.
31. THOMA, K. H.: Case report of a so-calledlatent bone cyst. Oral Surg, 1955: 8: 963-966.
32. TOLMAN, D. E. & STAFNE, E. C.: Developmental defects of the mandible. Oral Surg, 1967:24: 488-490.
33. WHI!'.'ERY, J . G.: Progressive bony cavities ofthe mandible, a review of the so-called traumatic bone cyst and a report of three cases.Oral Surg, 1955: 8: 903-916.
34. WORTH, H . M.: Principles andpractice of oralradiographic interpretation, 1st edition. YearBook Publishers Inc., Chicago, 1963, pp.461-462.
Address:
M. A. Pogrel,Division of Oral and Ma xillofacial SurgeryUniversity of California513 Pamasons Al'enueSan FranciscoCalifornia 94143USA