Embed Size (px)
Citation preview

Precision Medicine and Imaging
Molecular Profiling of Hepatocellular CarcinomaUsing Circulating Cell-Free DNAAhmed O. Kaseb1, Nora S. S�anchez2, Shiraj Sen3, Robin K. Kelley4, Benjamin Tan5,6,Andrea G. Bocobo4, Kian H. Lim5,6, Reham Abdel-Wahab1,7, Marc Uemura3,Roberto Carmagnani Pestana3,Wei Qiao8, Lianchun Xiao8, Jeffrey Morris8,Hesham M. Amin9, Manal M. Hassan10, Asif Rashid11, Kimberly C. Banks12,Richard B. Lanman12, AmirAli Talasaz12, Kenna R. Mills-Shaw2, Bhawana George9,Abedul Haque9, Kanwal P.S. Raghav1, Robert A.Wolff1, James C. Yao1,Funda Meric-Bernstam2,13, Sadakatsu Ikeda14, and Razelle Kurzrock14
Abstract
Purpose: Molecular profiling has been used to selectpatients for targeted therapy and determine prognosis. Non-invasive strategies are critical to hepatocellular carcinoma(HCC) given the challenge of obtaining liver tissue biopsies.
Experimental Design: We analyzed blood samples from206 patients with HCC using comprehensive genomic testing(Guardant Health) of circulating tumor DNA (ctDNA).
Results: A total of 153/206 (74.3%) were men; medianage, 62 years (range, 18–91 years). A total of 181/206patients had �1 alteration. The total number of alterationswas 680 (nonunique); median number of alterations/patient was three (range, 1–13); median mutant allelefrequency (% cfDNA), 0.49% (range, 0.06%–55.03%). TP53was the common altered gene [>120 alterations (non-
unique)] followed by EGFR, MET, ARID1A, MYC, NF1,BRAF, and ERBB2 [20–38 alterations (nonunique)/gene].Of the patients with alterations, 56.9% (103/181) had �1actionable alterations, most commonly in MYC, EGFR,ERBB2, BRAF, CCNE1, MET, PIK3CA, ARID1A, CDK6, andKRAS. In these genes, amplifications occurred more fre-quently than mutations. Hepatitis B (HBV)-positive patientswere more likely to have ERBB2 alterations, 35.7% (5/14)versus 8.8% HBV-negative (P ¼ 0.04).
Conclusions: This study represents the first large-scaleanalysis of blood-derived ctDNA in HCC in United States.The genomic distinction based on HCC risk factors and thehigh percentage of potentially actionable genomic altera-tions suggests potential clinical utility for this technology.
IntroductionRecent technological advances in molecular diagnostics have
allowed for the study of solid malignancies through noninvasiveblood sampling. Importantly, intact circulating tumor cells(CTCs) and cell-free DNA (cfDNA) [leukocyte-derived andtumor-derived (circulating tumor DNA; ctDNA)] can now beinterrogated through advanced sequencing methods in order toidentify somatic mutations that may be druggable targets forfuture therapies (1, 2). Although cfDNA and ctDNA are similar
in that they both derive from cell lysis and apoptosis (3), ctDNA isthe fraction of cfDNA, which can range from <0.1% to >10% (4),specifically derived from primary ormetastatic tumors (5). There-fore, profiling the mutational landscape of ctDNA fromsolid tumors may represent a particularly attractive method foridentifying tumor-associated somatic mutations. Applicationsthat can be envisioned to be of clinical utilityfor hepatocellular carcinoma (HCC) include detection of geno-mic changes, mutational analysis, prognostication, oncogenic
1Department of Gastrointestinal Medical Oncology, The University of Texas MDAnderson Cancer Center, Houston, Texas. 2Sheikh Khalifa Bin Zayed Al NahyanInstitute for Personalized Cancer Therapy, The University of Texas MDAndersonCancer Center, Houston, Texas. 3Division of Cancer Medicine, The University ofTexas MD Anderson Cancer Center, Houston, Texas. 4Helen Diller Family Com-prehensive Cancer Center, University of California, San Francisco, California.5Department of Medicine, Washington University School of Medicine, St. Louis,Missouri. 6Department of Radiology,Washington University School of Medicine,St. Louis, Missouri. 7Arizona Clinical Oncology Department, Assiut UniversityHospital, Assiut, Egypt. 8Department of Biostatistics, The University of Texas MDAnderson Cancer Center, Houston, Texas. 9Department of Hematopathology,The University of Texas MD Anderson Cancer Center, Houston, Texas. 10Depart-ment of Epidemiology, The University of Texas MD Anderson Cancer Center,Houston, Texas. 11Department of Pathology, The University of Texas MDAnderson Cancer Center, Houston, Texas. 12Guardant Health, Inc., RedwoodCity, California. 13Department of Investigational Cancer Therapeutics, TheUniversity of Texas MD Anderson Cancer Center, Houston, Texas. 14Center for
Personalized Cancer Therapy and Division of Hematology and Oncology,University of California San Diego, Moores Cancer Center, La Jolla, California.
Note: Supplementary data for this article are available at Clinical CancerResearch Online (http://clincancerres.aacrjournals.org/).
A.O. Kaseb and N.S. S�anchez contributed to this article.
Corresponding Authors: Ahmed O. Kaseb, University of Texas MD AndersonCancer Center, 1515 Holcombe Blvd., Unit 426, Houston, TX 77030. Phone: 713-792-2828; Fax: 713-745-1163: E-mail: [email protected]; and RazelleKurzrock, University of California San Diego, Moores Cancer Center, La Jolla,CA. E-mail: [email protected]
Clin Cancer Res 2019;25:6107–18
doi: 10.1158/1078-0432.CCR-18-3341
�2019 American Association for Cancer Research.
ClinicalCancerResearch
www.aacrjournals.org 6107
on July 11, 2021. © 2019 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 30, 2019; DOI: 10.1158/1078-0432.CCR-18-3341

pathway determination, prediction/monitoring of treatmentresponse, drug resistance alterations, and identification ofmechanisms of malignant/metastatic transformation based onunderlying risk factor and genetic predisposition.
ctDNA has been found to be inversely correlated with HCCprognosis (6) and shorter overall survival (7). Although severalstudies have investigated the global alterations in cfDNA ofHCC (8–13), the small number of patients and heterogeneity ofdemographics and geographic locations posed a challenge to theapplication of this methodology in the United States (12, 13).
Therefore, the purpose of this study was to examine a largemulti-institutional cohort of HCC tumors with a CLIA-certifiedcfDNA technology that is currently used in practice and to identifythe mutational landscape that may be contributing to HCCtumorigenesis for the purpose of selecting patients for targetedtherapy trials. This investigation represents the largest reportedseries of patients with HCC analyzed to date for the genomicportraits derived from blood-derived cfDNA.
Materials and MethodsPatients
During the period extending from November 2014 to July2016, 219 patients with advanced HCC underwent blood-derived cfDNA testing byGuardant Health. The diagnosis of HCCwas established either by histopathologic examination or bycharacteristics imaging findings, following clinical guidelines bythe American Association for the Study of Liver Disease (AASLD;ref. 14). The majority of the patients were from the following 4institutions: MDAnderson Cancer Center (MDACC; 37 patients),University of California San Diego, Moores Cancer Center(UCSD; 36 patients), Washington University School of Medi-cine-Siteman Cancer Center (18 patients), and University ofCalifornia San Francisco-Helen Diller Family ComprehensiveCancer Center (UCSF; 11 patients). The remaining patients werefrom other U.S. institutions. From the 219 patients, 12 had serialtesting. For patients who hadmore than one test, only the first testresult was considered. The analysis and consent of patients in thiscohort followed guidelines of various institutional review boardsand clinical protocols, as follows: MDACC: NCT01772771-Molecular Testing for the MDACC Personalized Cancer TherapyProgram; UCSD: NCT02478931 (PREDICT)-Study of Personal-ized Cancer Therapy to Determine Response and Toxicity;Washington University School of Medicine-Siteman Cancer Cen-ter: WU IRB protocol 201606097, A retrospective analysis of
circulating cell-free DNA in patients with gastrointestinal malig-nancies; UCSF, UCSF IRB No. 12-09576 Hepatobiliary TissueBank and Registry. The latter two institutional IRB approvals werefor nontherapeutic/noninterventional use and hence are notregistered in clinicaltrials.gov. The study was conducted in con-cordance with the Declaration of Helsinki.
Demographic information (i.e., gender, age) and date of bloodcollection were available for all patients. Additional patient infor-mation was requested from the institutions that contributed morethan 10 patients for cfDNA testing (UCSD, MDACC, SitemanCancer Center, and UCSF). The information requested was asfollows: (i) confirmation of HCC diagnosis; (ii) risk factor infor-mation, such as hepatitis A, B, and C status, nonalcoholic steato-hepatitis (NASH), alcoholic liver disease, andmetabolic syndrome;(iii) relevant clinicopathologic information including Child–Pughscore (CPS), Cancer of the Liver Italian Program (CLIP), BarcelonaClinic LiverCancer (BCLC), tumor-node-metastasis (TNM)staging,and treatment status at time of ctDNA testing.Metabolic syndromeas established as a clinical diagnosis as per guidelines by the 2001National Cholesterol Education Program ATP III (15). The diag-nosis ofNASHwas establishedbypathologic diagnosis ofNASH inpatients with available clinical data.
Comprehensive genomic testing in plasmacfDNA was extracted from whole blood collected in 10-mL
Streck tubes. Samples were shipped to a Clinical LaboratoryImprovement Act (CLIA)-certified, College of American Pathol-ogists-accredited laboratory (Guardant Health). After doubleultracentrifugation, 5 ng to 30 ng of cfDNA was isolated fordigital sequencing as described previously (12, 13, 16).
Cell-free DNA fragments, both leukocyte- and tumor-derived,were simultaneously sequenced. The variant allele fraction (VAF)was calculated as the proportion of cfDNA harboring the variantin a background of wild-type cell-free DNA. The analytical sen-sitivity allowed detection of one to two mutant fragments in a10-mL blood sample (0.1% limit of detection) with analyticspecificity >99.9999%. Twelve CNAswere reported as the absolutegene copy number in plasma. Because most cfDNA is leukocyte-derived, the gene copy number is generally 2.0. Tumor-derivedDNA shed into the bloodstream raises this value but, due to therelative proportions of tumor-derived versus leukocyte-derivedcfDNA, it is typically a minor contributor. Gene copy number inplasma is thus a function of both copy number in tissues and thedegree to which tumor DNA is shed into circulation. Plasma copynumber of 2.5 to 4.0 is reported as þþ amplification and >4.0 asþþþ, representing the 50th to 90th and >90th percentile, respec-tively of all CNA calls in the Guardant360 database (12, 13, 16).
Over the course of the study, the panel composition expandedfrom 54 to 68 to 70 genes. The initial 54-gene panel consisted ofcomplete exon coverage or critical exon coverage in 54 cancer-related genes, and amplifications in three genes. In the 68-genepanel, eight genes were retired from the SNV gene set, whereascoverage of gene amplifications expanded from three to 16 genes,and detection of fusions in four genes, and insertions or deletionof bases (indels) in one gene. The 70-gene panel includes allNCCN somatic genomic targets, including complete or criticalexon coverage in 30 and 40 genes, respectively; amplifications in18 genes, fusions in six genes, and indels in three genes (Supple-mentary Table S1). Seven patients were tested on the 54-genepanel was used, 86 on the 68-gene version of the original, and 142on the 70-gene panel version (Supplementary Table S2).
Translational Relevance
Molecular subgrouping of hepatocellular carcinoma (HCC)is challenging due to lack of tissue sampling, and profiling theHCC mutational landscape by cfDNA may be particularlyattractive given the challenge of obtaining liver biopsies. Wereport the largest USA cohort, using a CLIA-certified assayapproved for clinical practice. Our results demonstrate signif-icant trends between alterations and risk factors—metabolicsyndrome and PDGFRA, HBV and ERBB2, HCV and BRCA1. Inaddition, we observed a high percentage of potentially action-able genomic alterations, suggesting clinical utility for thistechnology in HCC.
Kaseb et al.
Clin Cancer Res; 25(20) October 15, 2019 Clinical Cancer Research6108
on July 11, 2021. © 2019 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 30, 2019; DOI: 10.1158/1078-0432.CCR-18-3341

Actionable genes and variants definedTo determine whether an alteration was actionable or not, we
referenced the actionable gene list set in place by the Institute forPersonalized Cancer Therapy-Precision Oncology Decision Sup-port (PODS) team at MD Anderson Cancer Center (17). By thesestandards, a gene is considered actionable if there is supportingevidence that such gene is a driver of tumorigenesis, whereinactionability of the gene can refer to either sensitivity and/orresistance to a drug(s), and sensitivity and/or resistance can beinclusive of all alterations types or specific to alteration classes,that is, applicable to amplifications, but not mutations. Further-more, there must be a clinically available agent targeting suchgene, and for a specific agent, there must be at least preclinicalevidence that supports its role in targeting the specific gene.Although the PODS team aims at maintaining the actionablegene list as comprehensive and up to date as possible, we reliedheavily on the availability of a drug in the context of clinical trial atMDACC. However, we acknowledge that drug availability andtrials varies greatly by institution. Finally, the actionability of agene can be in the context of tumor type(s). For example, incolorectal cancer, the use of the EGFR monoclonal antibodiescetuximab and panitumumab is contraindicated in tumors withactivating KRAS mutations, specifically those in codons G12 andG13 (FDA label; refs. 18–20). Hence, KRAS is deemed actionablefor treatment withMEK inhibitors in all tumor types. However, inthe case of colorectal cancer, it is also deemed actionable forresistance to cetuximab and panitumumab (21). At the moment,there are no HCC-specific actionable gene.
Based on the aforementioned criteria, the following genes wereconsidered actionable based on their sensitivity toward respectivetargeted agents: AKT1, ALK, ARAF, ARID1A, ATM, BRAF, BRCA1,BRCA2, CCND1, CCND2, CDK4, CDK6, CDKN2A, CDKN2B,EGFR, ERBB2, FGFR1, FGFR2, FGFR3, HRAS, IDH1, IDH2, JAK2,JAK3, KIT, MAP2K1, MAP2K2, MET, MPL, MYC, NF1, NOTCH1,NRAS, NTRK1, PDGFRA, PIK3CA, PTEN, PTPN11, RET, ROS1,SMO, STK11, and TSC1.
The following genes were deemed actionable based on context-specific criteria:CCNE1 (sensitivity to CDK2 inhibitors; resistanceto CDK4/6 inhibitors); ESR1 (presence is sensitizing to hormonetherapy, mutations cause resistance to anti-hormone therapy);KRAS (sensitivity to MEK inhibitors; resistance to cetuximab andpanitumumab in colorectal and erlotinib, and gefitinib inNSCLC; NRAS (sensitivity to MEK inhibitors, resistance tocetuximab and panitumumab); RAF1 (activating alterationscause sensitivity to MEK inhibitors and resistance to RAFinhibitors; inactivating alterations cause resistance to dasati-nib). Only AR and RB1 were deemed actionable solely becauseof their resistance to antihormone therapy and to CDK4/6inhibitors, respectively.
At the time of analysis, several genes included in the Guardantpanel were denoted as nonactionable including TP53, CTNNB1,APC, GNAS, NFE2L2, MLH1, RIT1, SMAD4, HNF1A, CDH1,GATA3, VHL, FBXW7, and RhoA. To note, some investigators,including coauthors on this manuscript, have considered TP53actionable for Wee-1 or VEGF/VEGFR inhibitors (22–24).Because this remains amatter of debate, TP53was not consideredactionable in this paper. Likewise, because the initial analysis,MLH1 has also become actionable based on FDA-approval ofnivolumab and pembrolizumab in 2017. Finally, variants foundin actionable genes but which lacked any supporting, functionalevidence were designated as "variants of unknown functional
significance" (VUS). A comprehensive list of all genes consideredand their actionability is included in Supplementary Table S1B.
Statistical analysisThe distribution of each continuous variable was summarized
by its mean, SD, and range. The distribution of each categoricalvariable was summarized in terms of its frequencies and percen-tages. Continuous variables were compared between groups byWilcoxon rank sum test, and for categorical data the comparisonwas conductedby Fisher exact test.Heatmapwithdendogramwasgenerated to explore and visualize the gene mutation/amplifica-tion relationship along with the corresponding various risk fac-tors. The relationship between gene types with regard tomutationand amplification as well as synonymous and targetable statuswas evaluated with Spearman rank correlation and displayed inthe correlationmatrix in which the nonsignificant correlations aremarked with "blank" in the graph (Fig. 6). All computations werecarried out in SAS version 9.3 and R version 3.13.
ResultsPatient characteristics
A cohort of 219 patients was enrolled in the study. Themedianage was 62.3 years (range, 18–91; 160 males and 59 females).Irrespective of gene actionability, the median number of altera-tions per patient was three (range, 1–13); the median allelefrequency (AF) of altered cfDNA (%cfDNA) was 0.49% (range,0.06–55.03).
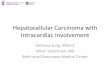
After further evaluation, it was determined that 13 of thesepatients had a diagnosis other than HCC, namely, fibrolamellarHCC, cholangiocarcinoma, or mixed HCC/cholangiocarcinoma.This determination was based on Liver Imaging Reporting andData System (LI-RADS) and tumor markers for HCC, whereasfibrolamellar and mixed HCC/cholangiocarcinoma were mostlyconfirmed by biopsy. These patients were excluded from furtheranalysis. In addition, for the patients who had more than onecfDNA test ordered (n ¼ 12 patients), only the first order wasconsidered for further analysis. After exclusion of these uniquecases, as well as the non-HCC cases, the initial data set wasreduced from219 to206patients, and from777 to680alterations(Fig. 1A–D).
Overall distribution of alteration typesThe majority of patients (87.8% ¼ 181/206) had at least one
alteration; only 12.2% (25/206) had no alterations (Fig. 1A). Atotal of 680 alterations (nonunique) were detected among theformer patient population, of which 10.5% (72/680) were synon-ymous/silent in nature, and 16% were amplifications (109/680).The remaining 73.3% of alterations (499/680) consisted of indels,missense, nonsense, and splice variants. A fraction of these altera-tions (214/499) were classified as "VUS" due to lack of supportingevidence for their functionality. The remaining variants (285/499)were broadly categorized as "mutations," andmade up 42% (285/680) of the total alterations identified (Fig. 1B).
Further analysis of the 42% of alterations that made up the"mutation" category revealed that 53% of these alterationsoccurredwithin actionable genes (actionablemutations) whereasthe remaining 47% occurred within genes not considered action-able (nonactionable mutations) at the time of analysis (Fig. 1C).On the other hand, all of the reported amplifications occurredwithin actionable genes. After accounting for synonymous
Cell-Free DNA in Hepatocellular Carcinoma
www.aacrjournals.org Clin Cancer Res; 25(20) October 15, 2019 6109
on July 11, 2021. © 2019 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 30, 2019; DOI: 10.1158/1078-0432.CCR-18-3341

alterations, VUS, and alterations in nonactionable genes, the totalnumber of actionable alterations was 209 out of the initial 680(nonunique) alterations identified (Fig. 1D).). Of the patientswith alterations, 56.9% (103/181) had�1 actionable alterations.
Most frequently mutated genes identifiedWeassessed the overallmolecular landscape of the 181patients
with HCC with detected alterations, both in terms of number ofalterations reported per gene and number of patients per gene.Additionally, to assess the true utility of cfDNA findings, in termsof their potential for guiding clinical decisions, genes were parsedinto "actionable" and "nonactionable genes," as defined above(see "Materials and Methods" for details). Inclusive of all alter-ation types (i.e., synonymous, VUS), the most frequently alteredgenes (�20 events/gene) were as follows: within actionablegenes—EGFR, MET, ARID1A, MYC, NF1, BRAF, and ERBB2;among non-actionable genes—TP53, followed by CTNNB1 andAPC (Fig. 2A). Overall, TP53 was the most commonly alteredgene, with >120 alterations. By comparison, EGFR had 38 altera-tions. Of note, the gene panel evolved over the course of thisstudy, hence the number of patients evaluated for each of thegenes varied depending on the panel available at that time.Moreover, detection of copy number variations was limited toamplifications in a subset of genes (see Materials and Methodsand Supplementary Tables S1A and S2 for details).
Exclusion of nonactionable alterations, that is, VUS and syn-onymous alterations, further reduced the total number of altera-tions from 680 alterations to 209 alterations. Moreover, thepatient population was also reduced from 181 to 103 patients,as many patients only had alterations detected within nonaction-able genes, or all alterationswere synonymous orVUS.Among the103 patients with actionable alterations, the most commonlyaltered genes (�10 patients/gene) were MYC, EGFR, ERBB2,BRAF, CCNE1, MET, PIK3CA, ARID1A, CDK6, and KRAS. Like-wise, amplifications were more common than mutations amongthe top genes (Fig. 2B).
Gene correlationmatrices to visualize coexpression andmutualexclusivity of genes with alterations detected
Twocorrelationmatriceswere generated (asdescribed inFig. 3),independent of the availability of risk factor information: thefirst matrix considered all confirmed patients with HCC withalterations detected, and included all alterations types (synony-mous, VUS, mutations, amplifications) in both actionable andnonactionable genes. This amounted to 181patients and 62 genesanalyzed (Fig. 2C). The premise of this matrix was to allow anoverall appreciation of all alterations identified. Formore hypoth-esis-generating analysis, the secondmatrix,which focusedonlyonmutations and amplifications within actionable genes (Supple-mentary Fig. S1B), and excluded synonymous andVUSalterations
Figure 1.
Overview of findings. A,Number ofHCC confirmed cases with alterationsdetected through cfDNA. B, Totalnumber of alterations identifiedamong the 181 patients withalterations, and the proportion ofalteration types identified. C,Actionability amongmutationsidentified. D, Total number ofactionable alterations, after removingsilent, VUS, and nonactionablemutations.
Kaseb et al.
Clin Cancer Res; 25(20) October 15, 2019 Clinical Cancer Research6110
on July 11, 2021. © 2019 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 30, 2019; DOI: 10.1158/1078-0432.CCR-18-3341

(Fig. 2D) was generated. Application of these exclusion criteriareduced the initial correlation matrix from 181 to 103 patients,and from 62 to 36 actionable genes. Concordance estimates and95% intervals (Cohen's k) for each pair of geneswere generated tobetter understand any association in terms of coexpression ormutual exclusivity of genes analyzed. In this analysis, any value<0indicatedno agreement, 0 to 0.20 slight agreement, 0.21 to0.40 asfair agreement, 0.41 to 0.60 as moderate agreement, 0.61 to 0.80as substantial agreement, and 0.81 to 1 as almost perfect agree-ment (Fig. 2C and D). Firm conclusions were not possible withthese matrices, given the small sample size, but hypothesis-generating observations could be deduced.
Identifying patients with alterations in actionable genes andavailable risk factor data
To understand if molecular findings correlated with any of therisk factors commonly observed among patients diagnosed withHCC, we requested additional patient information from institu-
tions having >10 HCC participants, as detailed under the Materi-als and Methods section. These included University of CaliforniaSan Diego Moores Cancer Center: 36 patients, 48 orders; MDAnderson Cancer Center: 37 patients, 37 orders; Siteman CancerCenter: 18 patients, 19 orders; and University of California SanFrancisco Comprehensive Cancer Center: 11 patients, 11 orders,for a total of 103 patients.
The 13 non-HCC cases previously excluded were identifiedfrom within this population. Hence, the final number of patientsfrom participating institutions was 89 patients, of which 82patients had alterations detectedwhereas seven had none (Fig. 3).We again parsed this subset of alterations into actionable ornonactionable groups; the latter included synonymous altera-tions, VUS, and nonactionable genes. We identified a subset ofpatients (n ¼ 34) who only had alterations detected in nonac-tionable genes or the alteration type was nonactionable, in thecase of synonymous or VUS. Ultimately, this reduced the patientpopulation with alterations from 82 to 48 patients contributing,
Figure 2.
Most frequently altered genes identified in cfDNA among patients with HCC. A,Distribution of all alterations identified, actionable, and nonactionable genes. B,Proportion of patients with alterations in actionable genes only. C,Gene correlation matrix among all patients with alterations detected. All patients withalterations detected, irrespective of the actionability of the alteration (i.e., variant in nonactionable genes, VUS, and/or synonymous) were considered for thismatrix. In all, from 181 patients and 62 genes were evaluated with Spearman rank correlation and displayed in the correlation matrix above. Nonsignificantcorrelations are marked with "blank" in the graph. Values <0 indicate no agreement, 0–0.20 slight agreement, 0.21–0.40 fair agreement, 0.41–0.60 as moderateagreement, 0.61–0.80 as substantial agreement, and 0.81–1 as almost perfect agreement. D, Gene correlation matrix among patients with HCCwith alterations inactionable genes (synonymous and VUS alteration excluded). Exclusion of nonactionable genes, VUS, and synonymous alterations reduced the patientpopulation size considered for this matrix from 181 to 103 patients and from 62 genes to only 36 actionable genes. The correlation between mutated genes wasevaluated with Spearman rank correlation and displayed in the correlation matrix above. Nonsignificant correlations are marked with "blank" in the graph. Values<0 indicate no agreement, 0–0.20 slight agreement, 0.21–0.40 fair agreement, 0.41–0.60 as moderate agreement, 0.61–0.80 as substantial agreement, and 0.81–1 as almost perfect agreement.
Cell-Free DNA in Hepatocellular Carcinoma
www.aacrjournals.org Clin Cancer Res; 25(20) October 15, 2019 6111
on July 11, 2021. © 2019 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 30, 2019; DOI: 10.1158/1078-0432.CCR-18-3341

for a total of 98 alterations (nonunique) in 31 actionable genes.This small subset of patients was statistically evaluated for theircorrelationwith risk factors contributing toHCC, and consisted of14women, 34men,mostly Caucasian patients (n¼ 30) followedbyHispanic (n¼ 8), Asian (n¼ 5), Black (n¼ 2), Native American(n ¼ 1), and other (n ¼ 2). Nineteen patients were reported tohave alcoholic liver disease, eight had confirmed nonalcoholicsteatohepatitits (NASH) and 10hadmetabolic syndrome. Staginginformation as classified byCPS, BCLC staging system, CLIP, and/or TNM stagingwas requested. There were 27 patients with CPS ofA: (5–6, well compensated), 13 with stage B: (7–9, significantfunctional compromise), and one with C: (10–15, decompen-sated). Six patients had an unknown BCLC classification, where-as 1 was classified as stage A, four as stage B, and 37 as stage C.Hepatitis A was reported in 12 patients; hepatitis B in 14patients; and hepatitis C in 17 patients. There were only ahandful of cases with both hepatitis A and B (n ¼ 4), hepatitisB and C (n ¼ 6), or hepatitis A and C (n ¼ 7; SupplementaryTable S3; Supplementary Fig. S1A–S1D).
Although this smaller subset (only patients with available riskfactor information and only actionable genes) included only 48of 206 patients, it maintained the overall molecular landscape ofthe larger subset (Fig. 2A and B). Although in the overall popu-lation the top 10 most frequently altered actionable genes were
MYC, EGFR, ERBB2, BRAF, CCNE1,MET, PIK3CA, ARID1A,CDK6, and KRAS, in this subset of patients (n ¼ 48) the top10 most frequently altered actionable genes were EGFR, ERBB2,MET, CCNE1,MYC, BRAF, CCND1, CDK6, FGFR2, and ARID1A(Fig. 4A and B). Hence, this subgroup should be considered asuitable and representative model of the molecular profile ofcirculating cell-free DNA in patients with HCC.
Correlation of risk factors with alterations identifiedSignificant differences were noted in the molecular profile of
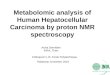
patients based on their underlying hepatic reserve and riskfactors for HCC. Among patients with metabolic syndrome,30% (3/10) had alterations detected in PDGFRA (P ¼ 0.0113),whereas patients without metabolic syndrome (n ¼ 30) had noalterations in this gene. In terms of hepatitis status, 35.7% (5/9)of patients with hepatitis B had alterations in ERBB2 (P ¼0.0365), and 16.7% (3/18) of patients with hepatitis C hadalterations in BRCA1 (P ¼ 0.0472). Hepatitis B and Hepatitis Cnegative patients, did not have any alterations in these respec-tive genes. In addition, 23.1% (3/13) of patients with CPS Bhad alterations in PIK3CA (P ¼ 0.0341) versus 0% (0/27) scoreA (0/27) or C (0/1; P ¼ 0.03). Heat map with dendogram wasgenerated to better visualize and study the gene mutation/amplification relationships along with the corresponding
Figure 3.
Stratification of patients for analysis over a period of approximately 2 years. A total of 219 patients from various institutions underwent biopsy-free, next-generation sequencing. We collected additional risk factor information for 102 patients, irrespective of alterations detected or not. Two correlation matrices weregenerated, independent of risk factor information. The first considered all patients, and all alteration types (n¼ 181 patients), and the second considered onlypatients with at least one alteration in an actionable gene and excluded VUS and synonymous alterations (n¼ 103 patients).
Kaseb et al.
Clin Cancer Res; 25(20) October 15, 2019 Clinical Cancer Research6112
on July 11, 2021. © 2019 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 30, 2019; DOI: 10.1158/1078-0432.CCR-18-3341

various risk factors. The relationships between gene types, withregard to mutation and amplification as well as synonymousand targetable status, was evaluated with Spearman rank cor-relation and displayed in the correlation matrix in whichthe nonsignificant correlations are marked with "blank" in thegraph. All computations were carried out in SAS version 9.3 andR version 3.13. (Figs. 5 and 6; Supplementary Fig. S2A–S2C).
DiscussionIn the vast majority of patients, HCC comprises a two-disease
state; HCC tumors and concomitant liver disease. Therefore,HCC staging/prognostication systems take into account tumorparameters in addition to hepatic reserve grade, manifested byChild–Pugh classification. While mounting evidence in theliterature suggests different molecular pathogenesis pathwaysbased on the degree of liver fibrosis and underlying HCC risk
factors, this has not been translated into defining molecularsubclasses in HCC. The challenge to defining molecular nosol-ogy is largely due to lack of access to tissue sampling in HCC,given the risk of bleeding due to concomitant coagulopathyand thrombocytopenia in patients with advanced fibrosis andportal hypertension. This bleeding risk led to the developmentand wide acceptance of guidelines to diagnose HCC withouttissue sampling (25). Therefore, despite recent advances in ourunderstanding of HCC molecular profiling based on tissuesampling (26), firm conclusions and biomarker integrationinto HCC staging were not achieved due to major challengesin prospective validation studies that are powered to study riskfactor-specific HCC. Liquid biopsies could bridge this gap,given the practicality of obtaining them in this patient popu-lation, and are expected to help advance the field of molecularprognostication and patient selection in targeted therapy trials.This study represents a step toward achieving this major goal
Figure 4.
Representative molecular landscape among patients with available risk factor data. A, Distribution of all alterations identified, actionable genes only, byalteration. B,Distribution of all alterations identified, actionable genes only, by patient.
Cell-Free DNA in Hepatocellular Carcinoma
www.aacrjournals.org Clin Cancer Res; 25(20) October 15, 2019 6113
on July 11, 2021. © 2019 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 30, 2019; DOI: 10.1158/1078-0432.CCR-18-3341

given our important observations related to specific commonrisk factors in HCC. This study also represents the largest U.S.cohort ever reported. Hence, our correlative findings of molec-ular alterations, as they relate to specific risk factors anddemographics, highlight the importance of cfDNA methodol-ogy in HCC and warrant future validation and exploration onits utility.
Chronic infection with hepatitis B with its incorporation intothe human genome is a common HCC risk factor, particularly
in Asia. The pathogenesis can be due to oncogenic viral proteinsor insertional mutagenesis. The mutational spectrum in HCCarising from hepatitis B infection is known to be enriched withTERT, CCNE1, and MLL4 due to insertional events, whereashepatitis C infection is typically chronic and leads to chronicinflammatory cascade events in the microenvironment andmutations.
Interestingly, our study showed statistically significant asso-ciations between certain alterations and specific risk factors,
Figure 5.
Correlation betweenmolecular landscape and risk factors contributing to HCC. Heat map dendrogramwas generated to explore and visualize the genemutation/amplification relationship along with the corresponding various risk factors. The relationship between gene types with regard to mutation andamplification, synonymous and targetable status was evaluated with Spearman rank correlation and displayed in the correlation matrix in which thenonsignificant correlations are marked with "blank" in the graph.
Kaseb et al.
Clin Cancer Res; 25(20) October 15, 2019 Clinical Cancer Research6114
on July 11, 2021. © 2019 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 30, 2019; DOI: 10.1158/1078-0432.CCR-18-3341

such as metabolic syndrome and PDGFRA (P ¼ 0.0113), HBVand ERBB2 (P ¼ 0.0365), HCV and BRCA1 (P ¼ 0.0472), andCPS B and PIK3CA (P ¼ 0.0341). This relationship betweengene types with regard to alteration type, risk factor, andtargetable status was evaluated with Spearman rank correla-tion and displayed in the correlation matrix. However, giventhe small number of patients in each category, we considerthese findings as hypothesis-generating associations thatshould be studied in future validation studies. However, giventhe small number of patients in each category, we considerthese findings as hypothesis-generating associations thatshould be studied in future validation studies. For example,although ERBB2 dysregulation is not known to be a significantdriver or hallmark of HCC, upregulation, correlation withHCC poor outcome, and cell line data suggest that HBVinteracts with ERBB2 and ERBB3 resulting in protein stabili-zation (20,21). Similarly, dysregulation of BRAF, BRCA1,MET, CDK6, ARID1A, CCNE1, EGFR, FGFR1, MYC, andNOTCH1 correlated with a history of HCV in our study(Supplementary Fig. S4A–S4D). In the case of BRCA1,although there is an exhaustive amount of literature support-ing the role of BRCA1 in breast and ovarian tumor types, less isknown about the role of BRCA1 in HCC, much less in regardsto its role in HCV affected patients with HCC. Nonetheless,
one whole genome-sequencing analysis of 88-matched HCCtumor/normal tissue samples reported that BRCA1 alterationswere identified in 1.1% of patients with HCC (27). By com-parison, our study using cfDNA assay identified BRCA1 altera-tions in four of 212 patients (1.8%) by ctDNA. Although this isnot direct evidence for BRCA1 in HCV in HCC, overall thesefindings are consistent with NGS results in solid tumor testing.Furthermore, increasing evidence supports the role of com-mon molecular signatures across distinct tumor types (28–30).Hence, there is the potential that BRCA1 and/or other genesthat have specifically been implicated in other tumor types,may also be relevant to HCC.
Notably, alterations in TERT promoter and in CTNNB1 genewere reported among the most frequent alterations in HCC (31),and in particular viral hepatitis-related HCC (32). Similarly, ourdata indicated the high prevalence ofCTNNB1mutations but didnot confirm the hepatitis status correlation,most likely because ofthe relatively small sample size of patients with available riskfactors for analysis (33–38).
One of the major strengths of our study is the large numberof patients representing numerous U.S. institutions driven bysamples submitted prospectively to aid in therapeutic decisionmaking using a CLIA-certified assay approved for clinical prac-tice. Moreover, almost half of the patients had risk factors.
Figure 6.
Correlation betweenmolecular landscape andmetabolic syndrome and/or history of hepatitis. A, Correlationwith metabolic syndrome: a significant number ofpatients with metabolic syndrome, 30% (3/10) had alterations detected in PDGFRA (P¼ 0.0113), whereas patients without metabolic syndrome (n¼ 30) had noalterations in this gene. B, Correlation with hepatitis B status: a significant number of patients with hepatitis B 35.7% (5/9) had alterations in ERBB2 (P¼ 0.0365),whereas HBV-negative patients had none. C, Correlation with hepatitis C status: 16.7% (3/18) of patients with hepatitis C (HCV) had alterations in BRCA1 (P¼0.0472), whereas HCV-negative patients had none. D, Correlation with CPS: 23.1% (3/13) of patients with CPS B had alterations in PIK3CA (P¼ 0.0341), versus0% (0/27) score A or C (0/1; P¼ 0.03).
Cell-Free DNA in Hepatocellular Carcinoma
www.aacrjournals.org Clin Cancer Res; 25(20) October 15, 2019 6115
on July 11, 2021. © 2019 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 30, 2019; DOI: 10.1158/1078-0432.CCR-18-3341

Another major advantage to our study is the critical importanceto assessing ctDNA in patients with HCC, where, obtaininginitial and repeat tissue sampling may be challenging as pre-viously mentioned. However, the study has some limitations.First, firm conclusions of the correlation with risk factors werenot possible given the small number of patients with availablerisk factors from five institutions. However, the pattern of thealterations was similar to the overall cohort. Second, the cfDNApanel is not as comprehensive as some tissue molecular pro-filing panels. However, the panel used is clinically driven inthat it is designed to identify somatic alterations in 73 genes,primarily focused on genomic alterations that are associatedwith (i) FDA-approved targeted therapies, (ii) targeted thera-pies in late stage clinical trials, (iii) known predictive orprognostic value, or (iv) informative of the presence of cfDNA.It is also important to note that the Guardant360 assay reportsout only somatic alterations. Mutant allele fractions (MAFs) arereported quantitatively for somatic SNVs of clinical significanceand distinguished from heterozygous and homozygous germ-line variants by their low concentrations, which are filtered outby the Guardant360 molecular tumor board (16). Anotherstudy limitation was that there was no direct comparison withtumor tissue, in large part because of the difficulty in doingbiopsies in HCC; therefore, our work reflects current clinicalpractice, in which the imaging diagnosis of HCC in the appro-priate setting without tissue diagnosis is widely adopted inboth academic and community centers. However, surgicalresection may be a source of tissue in patients—this procedureis more frequent in South East Asia where HBV patients withHCC may not have cirrhosis. Finally, we acknowledge thedefinition of actionability is dynamic and institution-depen-dent, and data on enrollment on targeted trials based on cfDNAresults was not available. Prospective studies using ctDNAprofiling to guide therapy decisions are warranted.
Notwithstanding the fact that further validation with solidtumor testing results is necessary, we conclude that cfDNAtesting is a valid methodology for HCC molecular profilinggiven the abundance of ctDNA observed in this, the largestcollection of U.S.-based blood samples. Although this directcomparison was not possible within this patient population, asfew patients had solid tumor testing results available, compar-ison to the findings reported recently by the Cancer GenomeAtlas initiative (39) and other prior studies (34, 40) are greatlyencouraging, considering the limitations of the current samplepopulation and the limited comprehensiveness of the cfDNAgene panel. In both the TCGA results and this study, the mostcommonly altered genes were TP53 and CTNNB1, whereasamplifications were most commonly observed in MET andCCND1. Moreover, the interesting molecular alteration find-ings related to specific HCC risk factors, if validated, could alsopave the way for developing a molecularly driven HCC clas-sification, and could aid in stratification for clinical trials.Indeed, genomically driven trials, both ongoing and complet-ed, have begun to allow enrollment based on cfDNA testresults. In HCC specifically, Ikeda and colleagues recentlypublished their findings on the clinical utility of cfDNA testingin HCC, reporting 79% of tested patients having at least oneclinically actionable alteration identified via cfDNA testing,with two patients showing good clinical response to matchedtargeted therapies (41). Nonetheless, future validation studieswith larger numbers of patients with available patient charac-
teristic data are essential for directing HCC translational efforts.Such data are expected to carry critical importance in usingmutational signatures for prognostication and for predictingresponse to targeted therapies. In addition, blood-derivedctDNA analysis is amenable to serial assessment while ontherapy in order to investigate acquired mutations.
Disclosure of Potential Conflicts of InterestR.K. Kelley is a consultant/advisory board member for Genentech/Roche
and TargetPharma Solutions. K.C. Banks holds ownership interest (includ-ing patents) in Guardant Health, Inc. R.B. Lanman is an employee ofGuardant Health, Inc.; holds ownership interest (including patents)in Guardant Health, Blolase, and Forward Medical; and is a consultant/advisory board member for Forward Medical, Inc. A. Talasaz is an employeeof and holds ownership interest (including patents) in Guardant Health,Inc. F. Meric-Bernstam reports receiving commercial research grants fromNovartis, AstraZeneca, Taiho, Genentech, Calithera, Debio, Bayer, Aileron,PUMA, CytoMx, Zymeworks, Curis, Pfizer, eFFECTOR, Abbvie, GuardantHealth, Daiichi Sankyo, and GlaxoSmithKline; reports receiving speakersbureau honoraria from Sumitomo Dainippon Pharma and Dialectica; andis a consultant/advisory board member for Genentech, Inflection Bios-ciences, Pieris, Darwin Health, Samsung Bioepis, Aduro, Spectrum, Origi-Med, Debio, Xencor, Jackson Laboratory, and Mersana. S. Ikeda reportsreceiving speakers bureau honoraria from Guardant Health, Chugai Phar-maceutical, and AstraZeneca. R. Kurzrock is an employee of CureMatch,Inc.; reports receiving other commercial research support to her institutionfrom Incyte, Genentech, Merck Serono, Pfizer, Sequenom, FoundationMedicine, Guardant Health, Grifols, Konica Minolta, DeBipharm, BoehringerIngelheim, and OmniSeq; reports receiving speakers bureau honoraria fromRoche; holds ownership interest (including patents) in IDbyDNA, Cure-Match, and Soluventis; and is an unpaid consultant/advisory board memberfor Gaido, LOXO, X-Biotech, Actuate Therapeutics, Roche, NeoMed, Solu-venits, and Pfizer. No potential conflicts of interest were disclosed by theother authors.
Authors' ContributionsConception and design: A.O. Kaseb, N.S. S�anchez, S. Sen, H.M. Amin,M.M. Hassan, K.C. Banks, R.B. Lanman, F. Meric-Bernstam, R. KurzrockDevelopment of methodology: A.O. Kaseb, N.S. S�anchez, M.M. Hassan,R.B. LanmanAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): A.O. Kaseb, N.S. S�anchez, S. Sen, R.K. Kelley,B. Tan, A.G. Bocobo, R. Abdel-Wahab, M. Uemura, R. Carmagnani Pestana,M.M. Hassan, K.C. Banks, R.B. Lanman, B. George, A. Haque, K.P.S. Raghav,F. Meric-Bernstam, S. IkedaAnalysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis): A.O. Kaseb, N.S. S�anchez, S. Sen, R.K. Kelley,R. Abdel-Wahab, R. Carmagnani Pestana, W. Qiao, L. Xiao, J. Morris,H.M. Amin, M.M. Hassan, A. Rashid, R.B. Lanman, K.P.S. Raghav, J.C. Yao,F. Meric-BernstamWriting, review, and/or revision of the manuscript: A.O. Kaseb, N.S. S�anchez,S. Sen, R.K. Kelley, B. Tan, A.G. Bocobo, R. Abdel-Wahab, R. CarmagnaniPestana, J. Morris, H.M. Amin, M.M. Hassan, A. Rashid, K.C. Banks,R.B. Lanman, A.A. Talasaz, K.R. Mills-Shaw, B. George, A. Haque,K.P.S. Raghav, R.A. Wolff, J.C. Yao, F. Meric-Bernstam, S. Ikeda, R. KurzrockAdministrative, technical, or material support (i.e., reporting or organizingdata, constructing databases): A.O. Kaseb, N.S. S�anchez, R.K. Kelley,A.G. Bocobo, K.H. Lim, M.M. Hassan, K.C. Banks, K.R. Mills-Shaw,R.A. Wolff, J.C. YaoStudy supervision: A.O. Kaseb, N.S. S�anchez, M.M. Hassan, A.A. Talasaz,J.C. Yao, F. Meric-Bernstam
AcknowledgmentsBili Project Foundation, Inc.-UCSF Hepatobiliary Tissue Bank and Registry.
This work was supported in part by the NIH through grants CA170035 andCA190945 (to A.O. Kaseb), CA106458 (to M.M. Hassan), and CA178744 (toJ. Morris), The Cancer Prevention and Research Institute of Texas RP150535 (toN.S. S�anchez, F. Meric-Bernstam), the Sheikh Khalifa Bin Zayed Al NahyanInstitute for Personalized Cancer Therapy 1U01 CA180964 (to N.S. S�anchez,
Kaseb et al.
Clin Cancer Res; 25(20) October 15, 2019 Clinical Cancer Research6116
on July 11, 2021. © 2019 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 30, 2019; DOI: 10.1158/1078-0432.CCR-18-3341

K.R. Mills-Shaw, F. Meric-Bernstam), NCATS Grant UL1 TR000371 (Center forClinical and Translational Sciences), and MD Anderson Cancer Center SupportGrant (P30 CA016672).
The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby marked
advertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
ReceivedOctober 12, 2018; revisedFebruary 15, 2019; accepted July 25, 2019;published first July 30, 2019.
References1. HaberDA,VelculescuVE.Blood-based analyses of cancer: circulating tumor
cells and circulating tumor DNA. Cancer Discov 2014;4:650–61.2. KhemlinaG, Ikeda S, Kurzrock R. The biology ofHepatocellular carcinoma:
implications for genomic and immune therapies. Mol Cancer 2017;16:149.
3. StrounM, Lyautey J, LederreyC,Olson-Sand A, Anker P. About the possibleorigin and mechanism of circulating DNA apoptosis and active DNArelease. Clin Chim Acta 2001;313:139–42.
4. Diehl F, Schmidt K, Choti MA, Romans K, Goodman S, Li M, et al.Circulating mutant DNA to assess tumor dynamics. Nat Med 2008;14:985–90.
5. Jen J, Wu L, Sidransky D. An overview on the isolation and analysis ofcirculating tumor DNA in plasma and serum. Ann N Y Acad Sci 2000;906:8–12.
6. RenN,Qin LX, TuH, Liu YK, Zhang BH, Tang ZY, et al. The prognostic valueof circulating plasma DNA level and its allelic imbalance on chromosome8p in patients with hepatocellular carcinoma. J Cancer Res Clin Oncol2006;132:399–407.
7. Tokuhisa Y, Iizuka N, Sakaida I, Moribe T, Fujita N, Miura T, et al.Circulating cell-free DNA as a predictive marker for distant metastasis ofhepatitis C virus-related hepatocellular carcinoma. Br J Cancer 2007;97:1399–403.
8. Tang JC, Feng YL, Guo T, Xie AY, Cai XJ. Circulating tumor DNA inhepatocellular carcinoma: trends and challenges. Cell Biosci 2016;6:32.
9. Schwaederle M, Chattopadhyay R, Kato S, Fanta PT, Banks KC, Choi IS,et al. Genomic alterations in circulating tumor DNA from diverse cancerpatients identified by next-generation sequencing. Cancer Res 2017;77:5419–5427.
10. SchwaederleM,HusainH, Fanta PT, PiccioniDE, Kesari S, SchwabRB, et al.Use of liquid biopsies in clinical oncology: pilot experience in 168patients.Clin Cancer Res 2016;22:5497–5505.
11. OnoA, Fujimoto A, Yamamoto Y, Akamatsu S,HiragaN, ImamuraM, et al.Circulating tumor dna analysis for liver cancers and its usefulness as aliquid biopsy. Cell Mol Gastroenterol Hepatol 2015;1:516–534.
12. Kim ST, Lee WS, Lanman RB, Mortimer S, Zill OA, Kim KM, et al.Prospective blinded study of somatic mutation detection in cell-free DNAutilizing a targeted 54-gene next generation sequencing panel inmetastaticsolid tumor patients. Oncotarget 2015;6:40360–9.
13. Zill OA,GreeneC, SebisanovicD, Siew LM, Leng J, VuM, et al. Cell-free dnanext-generation sequencing inpancreatobiliary carcinomas.CancerDiscov2015;5:1040–8.
14. Marrero JA, Kulik LM, Sirlin CB, Zhu AX, Finn RS, Abecassis MM, et al.Diagnosis, staging, and management of hepatocellular carcinoma: 2018practice guidance by the american association for the study of liverdiseases. Hepatology 2018;68:723–750.
15. Expert Panel on Detection E, Treatment of High Blood Cholesterol in A.Executive summary of the third report of the national cholesterol educa-tion program (NCEP) expert panel on detection, evaluation, and treatmentof high blood cholesterol in adults (adult treatment panel III). JAMA2001;285:2486–2497.
16. Lanman RB, Mortimer SA, Zill OA, Sebisanovic D, Lopez R, Blau S, et al.Analytical and clinical validation of a digital sequencing panel for quan-titative, highly accurate evaluation of cell-free circulating tumor DNA.PLoS One 2015;10:e0140712.
17. Meric-Bernstam F, JohnsonA, Holla V, Bailey AM, Brusco L, Chen K, et al. Adecision support framework for genomically informed investigationalcancer therapy. J Natl Cancer Inst 2015;107.
18. HeinemannV, Stintzing S, Kirchner T, Boeck S, JungA. Clinical relevance ofEGFR- and KRAS-status in colorectal cancer patients treated with mono-clonal antibodies directed against the EGFR. Cancer Treat Rev 2009;35:262–71.
19. Linardou H, Briasoulis E, Dahabreh IJ, Mountzios G, Papadimitriou C,Papadopoulos S, et al. All about KRAS for clinical oncology practice:gene profile, clinical implications and laboratory recommendations forsomatic mutational testing in colorectal cancer. Cancer Treat Rev 2011;37:221–33.
20. Misale S, Yaeger R, Hobor S, Scala E, Janakiraman M, Liska D, et al.Emergence of KRAS mutations and acquired resistance to anti-EGFRtherapy in colorectal cancer. Nature 2012;486:532–6.
21. Allegra CJ, Jessup JM, Somerfield MR, Hamilton SR, Hammond EH,Hayes DF, et al. American society of clinical oncology provisionalclinical opinion: testing for KRAS gene mutations in patients withmetastatic colorectal carcinoma to predict response to anti-epidermalgrowth factor receptor monoclonal antibody therapy. J Clin Oncol2009;27:2091–6.
22. Koehler K, Liebner D, Chen JL. TP53 mutational status is predictive ofpazopanib response in advanced sarcomas. Ann Oncol 2016;27:539–43.
23. Said R, Hong DS, Warneke CL, Lee JJ, Wheler JJ, Janku F, et al. P53mutations in advanced cancers: clinical characteristics, outcomes, andcorrelation between progression-free survival and bevacizumab-containing therapy. Oncotarget 2013;4:705–14.
24. Schwaederle M, Lazar V, Validire P, Hansson J, Lacroix L, Soria JC, et al.VEGF-A expression correlates with TP53 mutations in non-small cell lungcancer: implications for antiangiogenesis therapy. Cancer Res 2015;75:1187–90.
25. Bruix J, ShermanMPractice guidelines committee AAftSoLD. managementof hepatocellular carcinoma. Hepatology 2005;42:1208–36.
26. Harding JJ, Nandakumar S, Armenia J, Khalil DN, Albano M, Ly M, et al.Prospective genotyping of hepatocellular carcinoma: clinical implicationsof next-generation sequencing for matching patients to targeted andimmune therapies. Clin Cancer Res 2019;25:2116–26.
27. Yoo C, Ryu MH, Ryoo BY, Beck MY, Kang YK. Efficacy, safety, andpharmacokinetics of imatinib dose escalation to 800 mg/day in patientswith advanced gastrointestinal stromal tumors. Investigational NewDrugs2013;31:1367–1374.
28. Damrauer JS, Hoadley KA, ChismDD, FanC, Tiganelli CJ,Wobker SE, et al.Intrinsic subtypes of high-grade bladder cancer reflect the hallmarks ofbreast cancer biology. Proc Natl Acad Sci U S A 2014;111:3110–5.
29. Choi W, Porten S, Kim S, Willis D, Plimack ER, Hoffman-Censits J, et al.Identification of distinct basal and luminal subtypes of muscle-invasivebladder cancer with different sensitivities to frontline chemotherapy.Cancer Cell 2014;25:152–65.
30. Hoadley KA, Yau C, Wolf DM, Cherniack AD, Tamborero D, Ng S, et al.Multiplatform analysis of 12 cancer types reveals molecular classificationwithin and across tissues of origin. Cell 2014;158:929–944.
31. Lee SE, Chang SH, Kim WY, Lim SD, Kim WS, Hwang TS, et al. Frequentsomatic TERT promoter mutations and CTNNB1 mutations in hepatocel-lular carcinoma. Oncotarget 2016;7:69267–69275.
32. Pezzuto F, Izzo F, Buonaguro L, Annunziata C, Tatangelo F, Botti G, et al.Tumor specificmutations in TERTpromoter andCTNNB1 gene in hepatitisB and hepatitis C related hepatocellular carcinoma. Oncotarget 2016;7:54253–54262.
33. Nault JC,De Reynies A, Villanueva A, Calderaro J, Rebouissou S, CouchyG,et al. A hepatocellular carcinoma 5-gene score associated with survival ofpatients after liver resection. Gastroenterology 2013;145:176–87.
34. Schulze K, Imbeaud S, Letouze E, Alexandrov LB, Calderaro J, RebouissouS, et al. Exome sequencing of hepatocellular carcinomas identifies newmutational signatures and potential therapeutic targets. Nat Genet 2015;47:505–511.
35. Nault JC, Bioulac-Sage P, Zucman-Rossi J. Hepatocellular benign tumors-from molecular classification to personalized clinical care. Gastroenterol-ogy 2013;144:888–902.
Cell-Free DNA in Hepatocellular Carcinoma
www.aacrjournals.org Clin Cancer Res; 25(20) October 15, 2019 6117
on July 11, 2021. © 2019 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 30, 2019; DOI: 10.1158/1078-0432.CCR-18-3341

36. Cleary SP, Jeck WR, Zhao X, Chen K, Selitsky SR, Savich GL, et al.Identification of driver genes in hepatocellular carcinoma by exomesequencing. Hepatology 2013;58:1693–702.
37. Guichard C, Amaddeo G, Imbeaud S, Ladeiro Y, Pelletier L, Maad IB, et al.Integrated analysis of somatic mutations and focal copy-number changesidentifies key genes and pathways in hepatocellular carcinoma. Nat Genet2012;44:694–8.
38. Nault JC, Couchy G, Balabaud C, Morcrette G, Caruso S, Blanc JF, et al.Molecular classification of hepatocellular adenoma associates with riskfactors, bleeding, and malignant transformation. Gastroenterology 2017;152:880–894e6.
39. Cancer Genome Atlas Research Network. Electronic address wbe,cancer genome atlas research N. comprehensive and integrative geno-mic characterization of hepatocellular carcinoma. Cell 2017;169:1327–1341.e23.
40. Totoki Y, Tatsuno K, Covington KR, Ueda H, Creighton CJ, Kato M, et al.Trans-ancestry mutational landscape of hepatocellular carcinoma gen-omes. Nat Genet 2014;46:1267–73.
41. Ikeda S, Tsigelny IF, Skjevik AA, Kono Y, Mendler M, Kuo A, et al.Next-generation sequencing of circulating tumor DNA reveals fre-quent alterations in advanced hepatocellular carcinoma. Oncologist2018;23:586–93.
Clin Cancer Res; 25(20) October 15, 2019 Clinical Cancer Research6118
Kaseb et al.
on July 11, 2021. © 2019 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 30, 2019; DOI: 10.1158/1078-0432.CCR-18-3341

2019;25:6107-6118. Published OnlineFirst July 30, 2019.Clin Cancer Res Ahmed O. Kaseb, Nora S. Sánchez, Shiraj Sen, et al. Cell-Free DNAMolecular Profiling of Hepatocellular Carcinoma Using Circulating
Updated version
10.1158/1078-0432.CCR-18-3341doi:
Access the most recent version of this article at:
Material
Supplementary
http://clincancerres.aacrjournals.org/content/suppl/2019/07/30/1078-0432.CCR-18-3341.DC1
Access the most recent supplemental material at:
Cited articles
http://clincancerres.aacrjournals.org/content/25/20/6107.full#ref-list-1
This article cites 40 articles, 9 of which you can access for free at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/25/20/6107To request permission to re-use all or part of this article, use this link
on July 11, 2021. © 2019 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 30, 2019; DOI: 10.1158/1078-0432.CCR-18-3341