Embed Size (px)
Citation preview

………………..……………………………………………………………………………………………………………………………………..
Orthopedic Manual Therapy for the Pediatric Patient
Mitchell Selhorst, DPT, OCSNationwide Children’s Hospital Sports and Orthopedic PT
Columbus, Ohio

………………..……………………………………………………………………………………………………………………………………..
Learning Objectives
The attendee will:• Understand the specific precautions and the
relative risk of performing orthopedic manual therapy on pediatric patients.
• Identify pediatric patients who are appropriate for orthopedic manual therapy.
• Use orthopedic manual physical therapy to minimize pain and maximize function in pediatric orthopedic patients.

………………..……………………………………………………………………………………………………………………………………..
Pediatric Physical Therapy

This is the Pediatric I Mean

Kids Need PT Too!

Pediatric Pain is Not Benign
• Injury in childhood may lead to increased risk of pain in adulthood.23
• Pain does not go away on its own– 2/3 of adolescents with low back pain will
have chronic or recurrent symptoms 6 months later.38
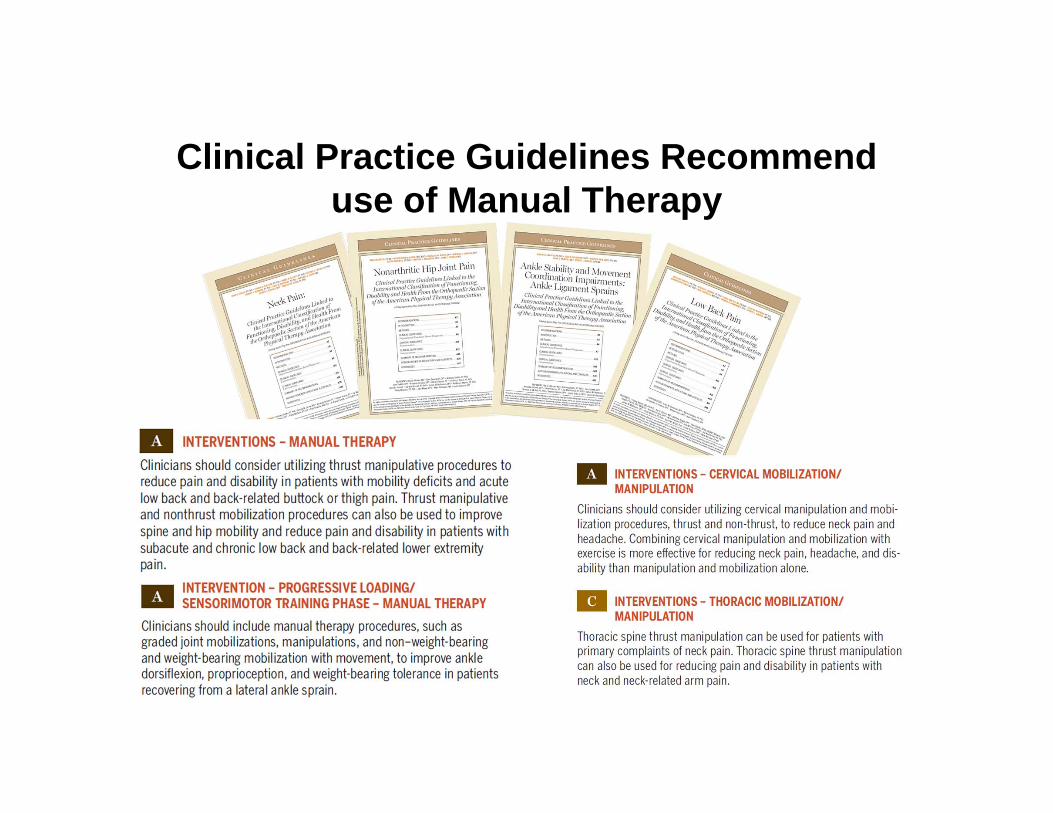
Clinical Practice Guidelines Recommend use of Manual Therapy

………………..……………………………………………………………………………………………………………………………………..
Alright, Let’s Do Manual Therapy!
Growing Children
Wait…

………………..……………………………………………………………………………………………………………………………………..
Contraindications and Precautions• Contraindication: A circumstance which
absolutely rules out the use of a therapeutic method which would otherwise be indicated.
• Precaution: The risks of a treatment have to be carefully assessed before treatment is initiated, and it can only be administered if its benefits to the patient are greater than its risks

………………..……………………………………………………………………………………………………………………………………..
Why are Children a Precaution for Manual Therapy?
Controversial: Not all authors agree that a growing child is a precaution.• Growth plates and cartilage endplates• Ability to give informed consent• Lack of research

Growth and Cartilage End Plates
Growth Plates Age of Ossification
Wrist 17‐19 years
Elbow 15‐18 years
Shoulder 19‐25 years
Hip 18‐25 years
Knee 19‐25years
Foot and Ankle 18‐20 years
Females 1-2 years sooner than males
End Plates Age of Ossification
Cervical 16‐18 years
Thoracic 16‐18 years
Lumbar 16‐18 years
Sacrum 18‐25 years
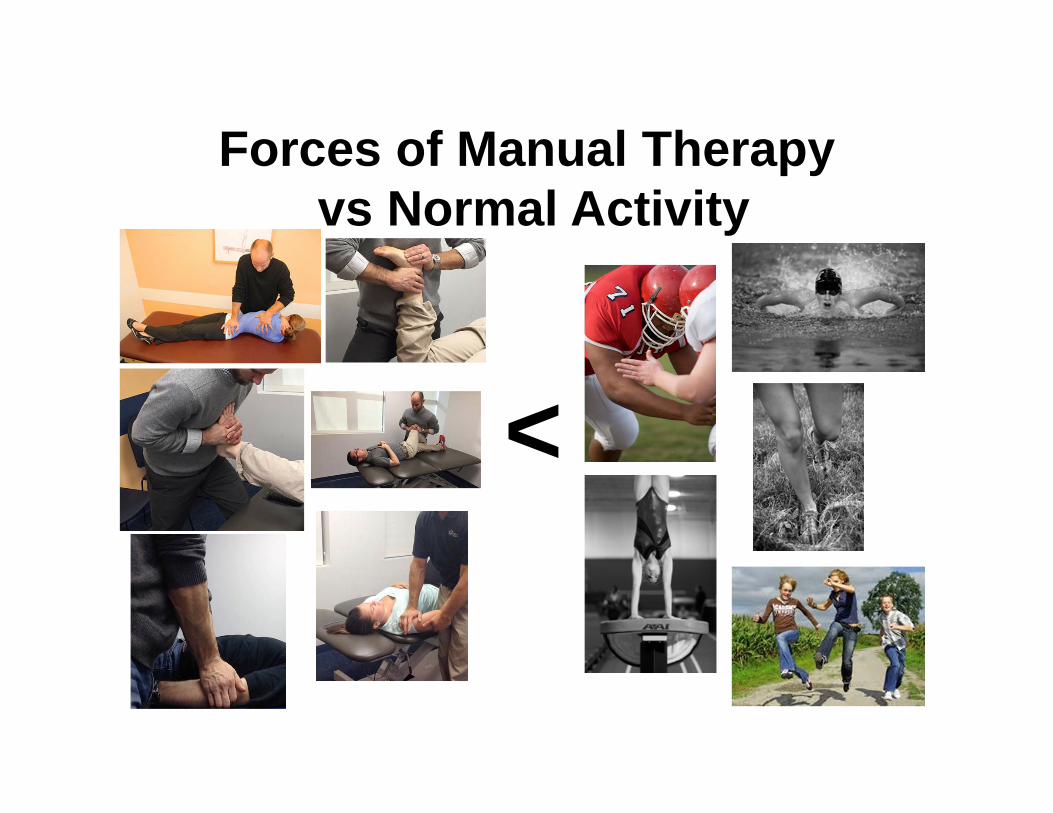
Forces of Manual Therapyvs Normal Activity
<

………………..……………………………………………………………………………………………………………………………………..
What is the Risk MT will damage a growth plate?
• Unknown: No documented case of growth plate injury has occurred due to manual therapy.– 10,000,000 manual therapy interventions
performed on children every year.– 2.3 million performed in the US alone.31

Gaining Informed Consent from a Child
• A minor cannot provide informed consent• Discussion of the risks and benefits of
manual therapy becomes a family discussion

………………..……………………………………………………………………………………………………………………………………..
Risks from Lack of Research
• Children are not tiny adults, many research results are not generalizable.
• We don’t know what we don’t know
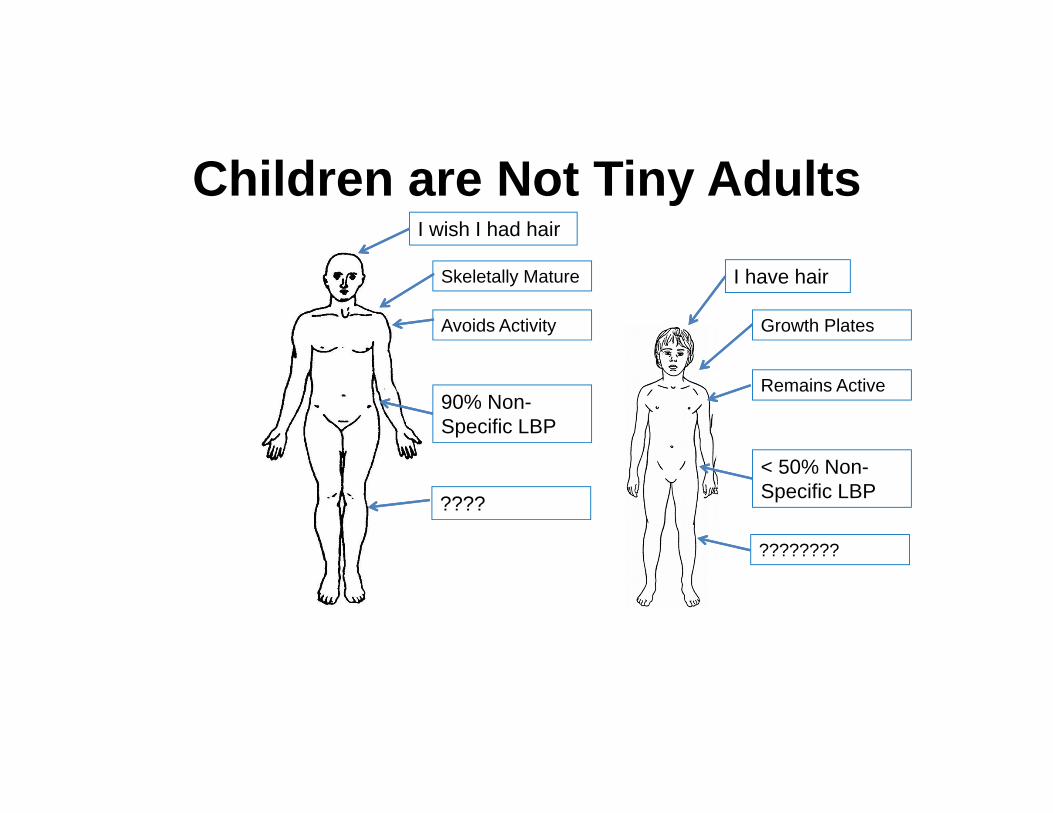
Children are Not Tiny Adults
I have hair
< 50% Non-Specific LBP
90% Non-Specific LBP
Remains Active
Skeletally Mature
Growth PlatesAvoids Activity
????????
????
I wish I had hair

………………..……………………………………………………………………………………………………………………………………..
Ruling out Cancer for Back Pain
• Negative on all 4 of these=100% sensitive– Age >50 years of age– Previous history of cancer– Unexplained weight loss– Failure to improve with conservative
management

………………..……………………………………………………………………………………………………………………………………..
Rely on your Red Flags
• Persistent pain• Increases at rest• Progressive neurological deficits• Associated fever• Night pain• Bowel or bladder incontinence

Ruling out Fractures
• Ottawa Ankle Rules28
• Ottawa Knee Rules37
• Canadian C-Spine Rules
OK!
OK!
STOP!
-Patients >10 years12
-Patient < 10 years12
OK!
Not Sensitive Enough

Can we use CPR’s to guide manual treatment?
• Manipulation for low back pain14
– Pain for <16 days– No pain distal to the knee– 1 Lumbar segment hypomobile– Hip IR >35 degrees– FABQ-work subscale score <19
??? 10-30% more hip IR motion in children

Can we use a Modified CPR for Lumbar Manipulation
Patient meets 3 out of the 4– Pain for <16 days– No pain distal to the knee– 1 Lumbar segment hypomobile– Hip IR >35 degrees
In a RCT assessing lumbar manipulation in adolescents, only 5% met either of these modified rules. Unable to assess the effectiveness of these CPR’s.38OR
Patient have both of the following-Pain for <16 days-No pain distal to the knee
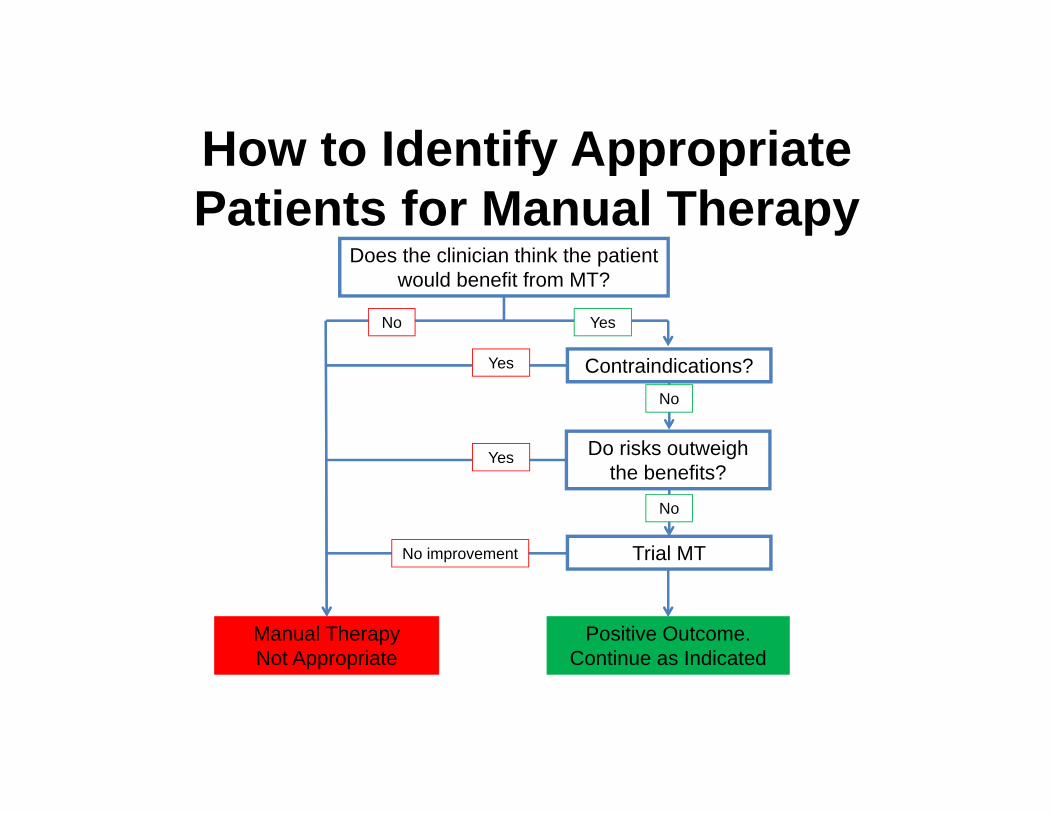
How to Identify Appropriate Patients for Manual Therapy
Does the clinician think the patient would benefit from MT?
Manual Therapy Not Appropriate
Contraindications?
Do risks outweigh the benefits?
Trial MT
Positive Outcome.Continue as Indicated
Yes
Yes
No improvement
No
No
No Yes

Case of Low Back Pain
13-year-old female – 2-month hx of LBP– Insidious onset – Has not improved over
past 4 weeks– No report of pain, NT, or
weakness in LE’s– No red flags noted during
evaluation

Case of Low Back Pain 13-year-old female with 2-month hx of LBP
-Recreational dancer (Hip Hop and Ballet) 4 hours of class a week.-Pain is worse with activity(2/10 at rest 6/10 pain during dance)-Pain increases by 2/10 with lumbar extension-Scored a 14/30 on Patient Specific Functional Scale
Dance 4/10Bending backwards 5/10Walking for >20 minutes 5/10

Should We Utilize Manual Therapy with this Patient?

Treatment Consideration for the pediatric lumbar spine
• Much of pediatric back pain has an anatomical cause, some can be precautions or contraindications to manual therapy
• Up to 50% of adolescent athletes with low back pain have a spondylolysis or spondylolisthesis.43

SpondylolysisType Name Pathogenisis
Type I Dysplastic Congenital abnormalities
Type II Isthmic Stress fracture in the pars interarticularis
Type III Degenerative Degeneration of the intervertebraldiscs
Type IV Traumatic Acute fracture in areas other than pars
Type V Pathological Bone disease, tumor, or infection
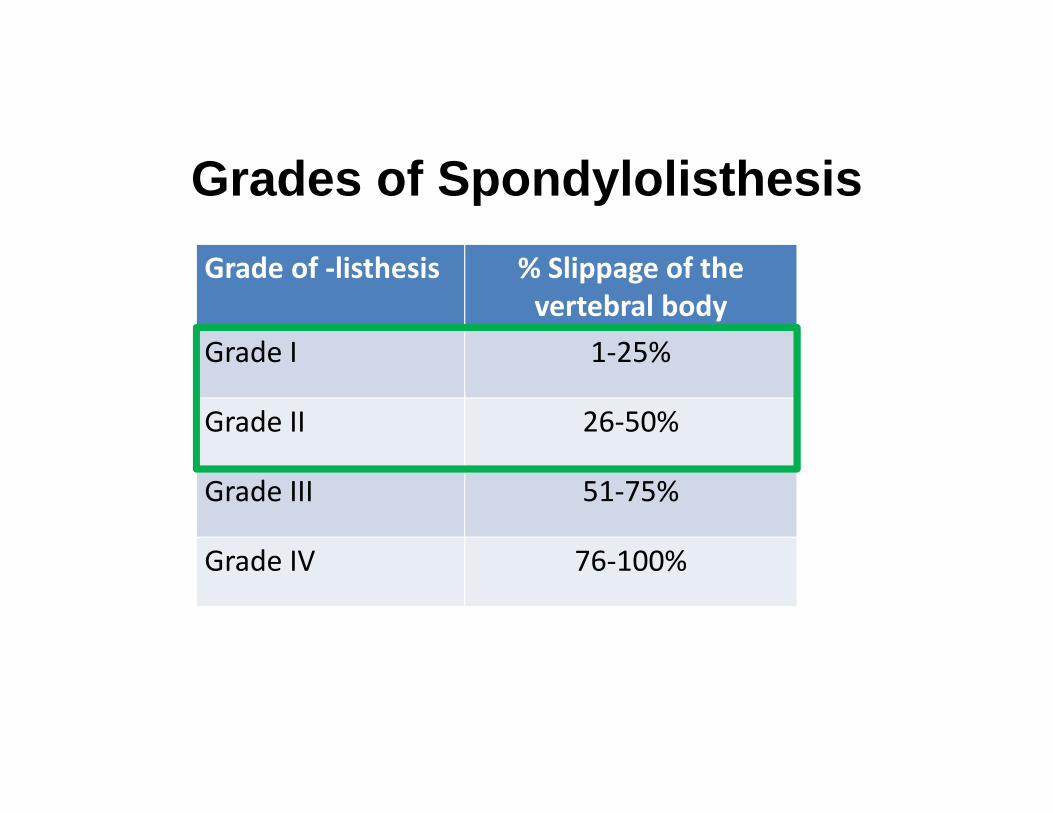
Grades of SpondylolisthesisGrade of ‐listhesis % Slippage of the
vertebral bodyGrade I 1‐25%
Grade II 26‐50%
Grade III 51‐75%
Grade IV 76‐100%
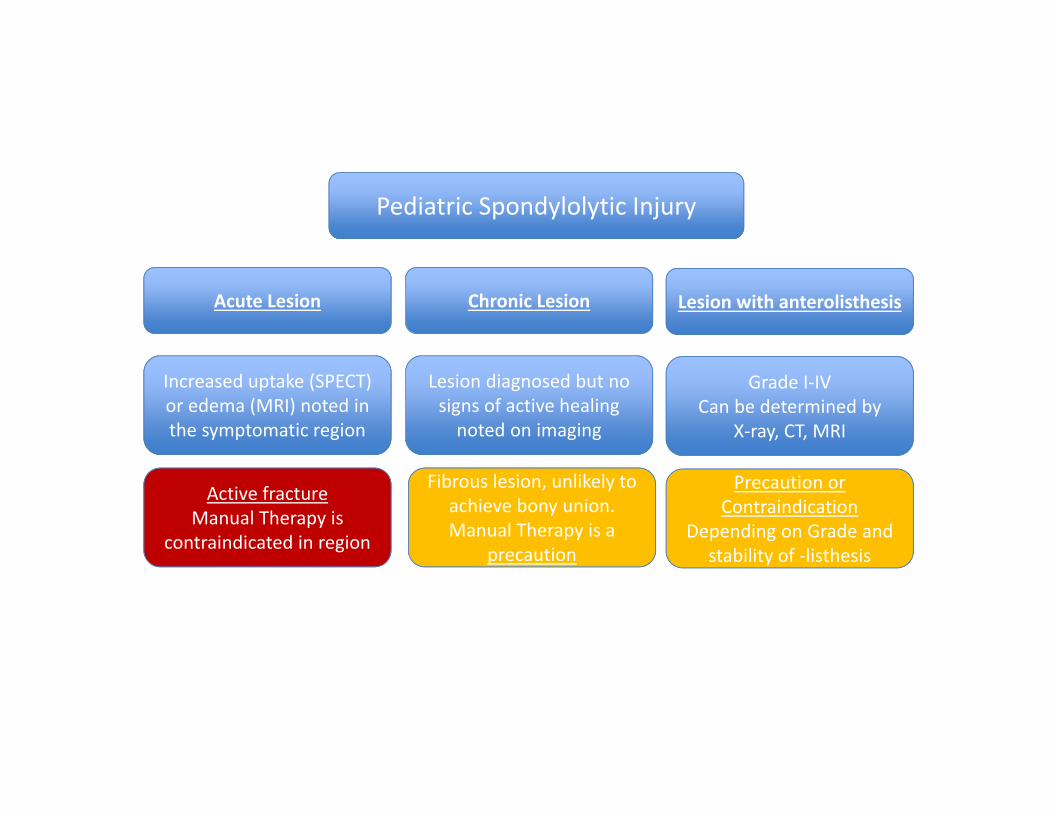
Pediatric Spondylolytic Injury
Acute Lesion Chronic Lesion Lesion with anterolisthesis
Increased uptake (SPECT) or edema (MRI) noted in the symptomatic region
Active fractureManual Therapy is
contraindicated in region
Lesion diagnosed but no signs of active healing noted on imaging
Fibrous lesion, unlikely to achieve bony union. Manual Therapy is a
precaution
Grade I‐IV Can be determined by
X‐ray, CT, MRI
Precaution or Contraindication
Depending on Grade and stability of ‐listhesis

Are there contraindication for manual therapy?
13-year-old female with 2-month hx of LBP
– ImagingX-ray - NegativeMRI - Negative

Risk and Benefits of Manual Therapy with this Patient?
• Physical therapy, including manual treatment, results in significantly better outcomes in children with back pain.1
• Lumbar manipulation does not increase risk of an adverse event in adolescents with non-specific low back pain.38
Trial Manual Therapy!
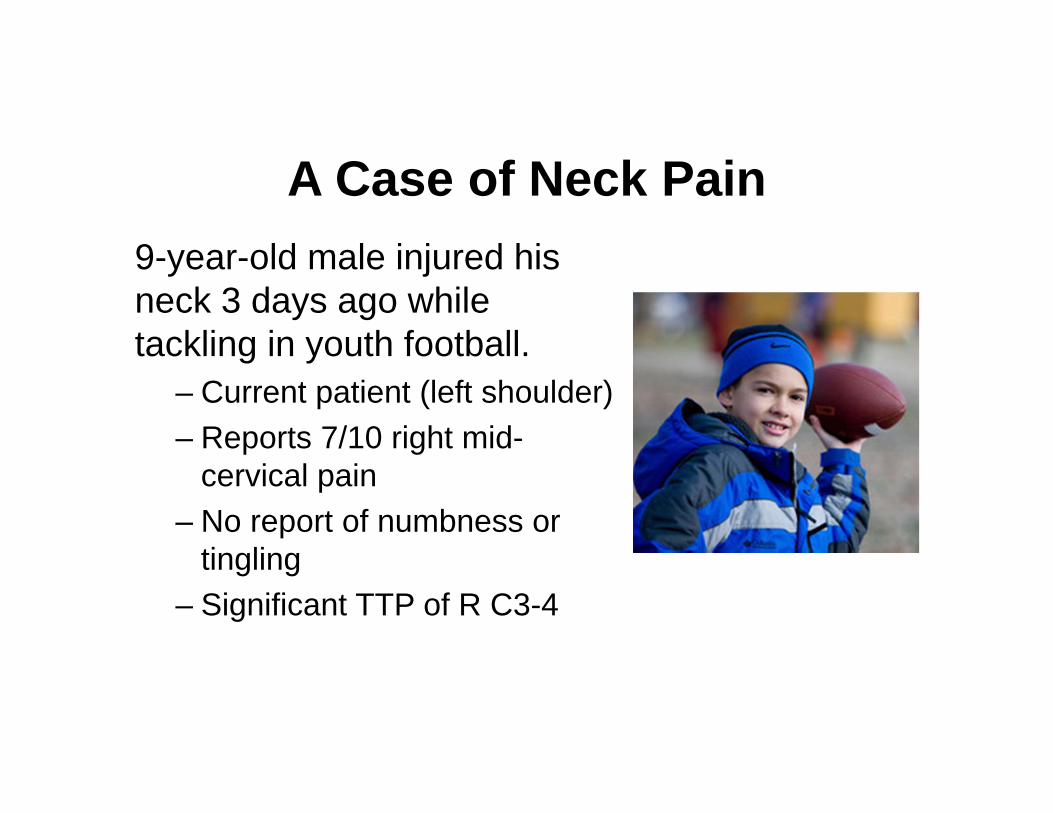
A Case of Neck Pain9-year-old male injured his neck 3 days ago while tackling in youth football.
– Current patient (left shoulder)– Reports 7/10 right mid-
cervical pain– No report of numbness or
tingling– Significant TTP of R C3-4

A Case of Neck Pain
9-year-old male injured during youth football
– Patient maintained consciousness– Not a helmet-to-helmet collision – Active cervical ROM
Flexion 65 deg. Ext 20 deg.*Rotation L 75 deg. R 50 deg*.
– Difficulty sleeping at night due to pain– No signs or symptoms of concussion
Should We Utilize Manual Therapy with this Patient?

………………..……………………………………………………………………………………………………………………………………..
Are there contraindications for manual therapy?
• Unable to rule out cervical fracture.– No imaging to rule out fracture.
– Canadian C-spine Rules not sensitive enough.

Thumbs Down

A Case of Swimmers Shoulder
• Clinical diagnosis of secondary GH impingement and multi-directional instability.
• Generalized hypermobility notedBeighton score of 6 out of 9
11-year-old female with R shoulder pain

A Case of Swimmers Shoulder
+ Hawkins-Kennedy+ Painful Arc+ ER weakness+ Excessive anterior
GH joint laxity+ Sulcus sign- Apprehension
11-year-old female with R shoulder pain

Should We Utilize Manual Therapy with this Patient?

Are there contraindications for manual therapy?
Generalized Hypermobility is considered a precaution by most, a few consider it a contraindication.
– When treating a patient with hypermobility, the therapist should examine opposite motions and neighboring segments to find out if any restrictions exist.

Risks vs Benefits
• Risks: Manual therapy done incorrectly could increase the patient’s hypermobility and multi-directional instability.
• Benefits: Restoring motion to neighboring segments could improve proper GH joint mechanics- 2 case studies support this theory.7, 27

Trial Manual Therapy
Target restricted areas:– Posterior Shoulder– Pec Minor– Thoracic Extension– Scapular thoracic

A Case Acute Ankle Sprain
– 5-days post injury
– Does not participate in sports
– Fell off obstacle course and rolled his ankle
– No imaging performed
– Presents to clinic on crutches and ACE wrap
15-year-old male with L inversion ankle sprain

A Case of Acute Ankle Sprain
– Patient is able to walk in clinic without use of crutches with antalgic gait
– TTP at ATFL – Talar Tilt, Anterior drawer + (pain)– No tenderness at medial/lateral
malleoli, navicular or base 5th
metatarsal– Mild swelling noted upon visual
examination
15-year-old male with L inversion ankle sprain

Should We Utilize Manual Therapy with this Patient?

Are there contraindications for manual therapy?
• Rule out fracture with the Ottawa Ankle Rules.
• No other precautions or contraindications noted

Risks vs Benefits
Risks: Minimal. No adverse reaction noted in research for this population
Benefits: Short and long-term benefits noted with use of manual therapy for acute ankle sprain.44, 45
Trial Manual Therapy!

………………..……………………………………………………………………………………………………………………………………..
Conclusion• Manual therapy can be an effective way to
minimize pain and maximize function in pediatric orthopedic patients.
• Weigh the risks and benefits before proceeding
• Rely on patient history, your clinical expertise, and the patient’s preference until there is better research to guide EBP.

References1. Ahlqwist A, Hagman M, Kjellby-Wendt G, Beckung E. Physical therapy treatment of back complaints on children and adolescents. Spine. 2008;33(20):E721-7. Epub 2008/09/17.2. Alqarni AM, Schneiders AG, Cook CE, Hendrick PA. Clinical tests to diagnose lumbar spondylolysis and spondylolisthesis: A systematic review. Physical therapy in sport : official journal of the Association of Chartered Physiotherapists in Sports Medicine. 2015. Epub 2015/03/24.3. Bialosky JE, Bishop MD, Price DD, Robinson ME, George SZ. The mechanisms of manual therapy in the treatment of musculoskeletal pain: a comprehensive model. Manual therapy. 2009;14(5):531-8. Epub 2008/11/26.4. Blanch P. Conservative management of shoulder pain in swimming. Physical Therapy in Sport. 2004;5(3):109-24.5. Bruggeman G. Biomechanics in gymnastics. Med Sport Science. 1987;25:142 Y 76.6. Calvo-Munoz I, Gomez-Conesa A, Sanchez-Meca J. Physical therapy treatments for low back pain in children and adolescents: a meta-analysis. BMC musculoskeletal disorders. 2013;14:55. Epub 2013/02/05.7. Carson PA. The rehabilitation of a competitive swimmer with an asymmetrical breaststroke movement pattern. Manual therapy. 1999;4(2):100-6. Epub 1999/10/06.8. Chen KC, Chiu EH. Adolescent idiopathic scoliosis treated by spinal manipulation: a case study. Journal of alternative and complementary medicine (New York, NY). 2008;14(6):749-51. Epub 2008/08/05.

References9. Clifford SN, Fritz JM. Children and adolescents with low back pain: a descriptive study of physical examination and outcome measurement. The Journal of orthopaedic and sports physical therapy. 2003;33(9):513-22. Epub 2003/10/04.10. DeVocht JW, Pickar JG, Wilder DG. Spinal manipulation alters electromyographic activity of paraspinalmuscles: a descriptive study. Journal of manipulative and physiological therapeutics. 2005;28(7):465-71. Epub 2005/09/27.11. d'Hemecourt PA, Luke A. Sport-specific biomechanics of spinal injuries in aesthetic athletes (dancers, gymnasts, and figure skaters). Clinics in sports medicine. 2012;31(3):397-408. Epub 2012/06/05.12. Ehrlich PF, Wee C, Drongowski R, Rana AR. Canadian C-spine Rule and the National Emergency X-Radiography Utilization Low-Risk Criteria for C-spine radiography in young trauma patients. Journal of pediatric surgery. 2009;44(5):987-91. Epub 2009/05/13.13. Evans DW. Mechanisms and effects of spinal high-velocity, low-amplitude thrust manipulation: previous theories. Journal of manipulative and physiological therapeutics. 2002;25(4):251-62. Epub 2002/05/22.14. Flynn T, Fritz J, Whitman J, Wainner R, Magel J, Rendeiro D, et al. A clinical prediction rule for classifying
patients with low back pain who demonstrate short-term improvement with spinal manipulation. Spine. 2002;27(24):2835-43. Epub 2002/12/18.
15. Fritz JM, Koppenhaver SL, Kawchuk GN, Teyhen DS, Hebert JJ, Childs JD. Preliminary investigation of the mechanisms underlying the effects of manipulation: exploration of a multivariate model including spinal stiffness, multifidus recruitment, and clinical findings. Spine. 2011;36(21):1772-81. Epub 2011/03/02.16. Frost DM, Beach T, Fenwick C, Callaghan J, McGill S. Is there a low-back cost to hip-centric exercise? Quantifying the lumbar spine joint compression and shear forces during movements used to overload the hips. Journal of sports sciences. 2012;30(9):859-70. Epub 2012/04/04.

References17. Gal. Biomechanical studies of spinal manipulative therapy (SMT) quantifying the movements of vertebral bodies during SMT. Journal of CCA. 1994;38(1):1518. Gatt CJ, Jr., Hosea TM, Palumbo RC, Zawadsky JP. Impact loading of the lumbar spine during football blocking. Am J Sports Med. 1997;25(3):317-21.19. Gatterbauer A. Contraindications in Osteopathy. Vienna: Danube University Krem; 2009.20. Grindstaff TL, Beazell JR, Sauer LD, Magrum EM, Ingersoll CD, Hertel J. Immediate effects of a tibiofibular joint manipulation on lower extremity H-reflex measurements in individuals with chronic ankle instability. Journal of electromyography and kinesiology : official journal of the International Society of Electrophysiological Kinesiology. 2011;21(4):652-8. Epub 2011/05/07.21. Haun DW, Kettner NW. Spondylolysis and spondylolisthesis: a narrative review of etiology, diagnosis, and conservative management. Journal of chiropractic medicine. 2005;4(4):206-17. Epub 2005/01/01.22. Hayden JA, Mior SA, Verhoef MJ. Evaluation of chiropractic management of pediatric patients with low back pain: a prospective cohort study. Journal of manipulative and physiological therapeutics. 2003;26(1):1-8. Epub 2003/01/18.23. Hestbaek L, Leboeuf-Yde C, Kyvik KO, Manniche C. The course of low back pain from adolescence to adulthood: eight-year follow-up of 9600 twins. Spine. 2006;31(4):468-72. Epub 2006/02/17.24. Humphreys BK. Possible adverse events in children treated by manual therapy: a review. Chiropractic & osteopathy. 2010;18:12. Epub 2010/06/08.25. Koppenhaver SL, Fritz JM, Hebert JJ, Kawchuk GN, Childs JD, Parent EC, et al. Association between changes in abdominal and lumbar multifidus muscle thickness and clinical improvement after spinal manipulation. The Journal of orthopaedic and sports physical therapy. 2011;41(6):389-99. Epub 2011/04/08.

References26. Lanthois PE, Pollard H. Spondylolysis in a professional fast bowler. A case study. Australasian chiropractic & osteopathy : journal of the Chiropractic & Osteopathic College of Australasia. 1997;6(1):1-9. Epub 1997/03/01.27. Leao Almeida GP, De Souza VL, Barbosa G, Santos MB, Saccol MF, Cohen M. Swimmer's shoulder in young athlete: rehabilitation with emphasis on manual therapy and stabilization of shoulder complex. Manual therapy. 2011;16(5):510-5. Epub 2011/01/22.28. Libetta C, Burke D, Brennan P, Yassa J. Validation of the Ottawa ankle rules in children. Journal of accident & emergency medicine. 1999;16(5):342-4. Epub 1999/10/03.29. Loudon JK, Reiman MP, Sylvain J. The efficacy of manual joint mobilisation/manipulation in treatment of lateral ankle sprains: a systematic review. British journal of sports medicine. 2014;48(5):365-70. Epub 2013/08/28.30. McDevitt A, Young J, Mintken P, Cleland J. Regional interdependence and manual therapy directed at the thoracic spine. Journal of Manual & Manipulative Therapy.0(0):2042618615Y.0000000005.31. Ndetan H, Evans MW, Jr., Hawk C, Walker C. Chiropractic or osteopathic manipulation for children in the United States: an analysis of data from the 2007 National Health Interview Survey. Journal of alternative and complementary medicine (New York, NY). 2012;18(4):347-53. Epub 2012/03/06.32. O'Neal ML. The pediatric spine: anatomical and dynamic considerations preceding manipulation. Comprehensive therapy. 2003;29(2-3):124-9. Epub 2003/11/11.

References33. Pellow JE, Brantingham JW. The efficacy of adjusting the ankle in the treatment of subacute and chronic grade I and grade II ankle inversion sprains. Journal of manipulative and physiological therapeutics. 2001;24(1):17-24.34. Pickar JG. Neurophysiological effects of spinal manipulation. The spine journal : official journal of the North American Spine Society. 2002;2(5):357-71. Epub 2003/11/01.35. Puentedura EJ, O'Grady WH. Safety of thrust joint manipulation in the thoracic spine: a systematic review. Journal of Manual & Manipulative Therapy.0(0):2042618615Y.0000000012.36. Redwood D. Advances in manual therapy for children. Journal of alternative and complementary medicine (New York, NY). 2011;17(3):185-6. Epub 2011/03/23.37. Robertson J. The Ottawa Knee Rules accurately identified fractures in children with knee injuries. Evidence-based nursing. 2004;7(1):24. Epub 2004/03/05.38. Selhorst M, Selhorst B. Lumbar manipulation and exercise for the treatment of acute low back pain in adolescents: a randomized controlled trial. Journal of Manual & Manipulative Therapy. 2015;0(0):2042618614Y.0000000099.39. Todd AJ, Carroll MT, Robinson A, Mitchell EK. Adverse Events Due to Chiropractic and Other Manual Therapies for Infants and Children: A Review of the Literature. Journal of manipulative and physiological therapeutics. 2014. Epub 2014/12/03.

References40. Vaughn DW, Kenyon LK, Sobeck CM, Smith RE. Spinal manual therapy interventions for pediatric patients: a systematic review. The Journal of manual & manipulative therapy. 2012;20(3):153-9. Epub 2013/08/02.41. Vohra S, Johnston BC, Cramer K, Humphreys K. Adverse events associated with pediatric spinal manipulation: a systematic review. Pediatrics. 2007;119(1):e275-83. Epub 2006/12/21.42. Riddle G, Ross O, Spellane V. Orthopedic issues and treatment strategies for the pediatric
patient. Exercise Considerations for the pediatric patient. APTA. 200943. Micheli LJ, Wood R. Back pain in young athletes. Significant differences from adults in causes and
patterns. Archives of pediatrics & adolescent medicine. 1995;149(1):15-8. Epub 1995/01/01.44. Cleland JA, Mintken PE, McDevitt A, Bieniek ML, Carpenter KJ, Kulp K, et al. Manual physical
therapy and exercise versus supervised home exercise in the management of patients with inversion ankle sprain: a multicenter randomized clinical trial. The Journal of orthopaedic and sports physical therapy. 2013;43(7):443-55. Epub 2013/05/01.
45. Whitman JM, Cleland JA, Mintken PE, Keirns M, Bieniek ML, Albin SR, et al. Predicting short-term response to thrust and nonthrust manipulation and exercise in patients post inversion ankle sprain. The Journal of orthopaedic and sports physical therapy. 2009;39(3):188-200. Epub2009/03/03.