Embed Size (px)
Citation preview

PLAZMAFEREZ UYGULAMALARI
Prof.Dr.İdil YENİCESU
Gazi Üniversitesi Tıp FakültesiPed.Hematoloji ve Onkoloji Bilim Dalı



Amaç
• Goodpasture Sendromunda olduğu gibi istenmeyen maddelerin uzaklaştırılması (anti-Glomerüler Bazal Membran Antikoru)
• İstenmeyen maddeleri uzaklaştırmanın yanısıra eksik olanı yerine koymak (TTP, ADAMTS13 antikoru ve ADAMTS13)
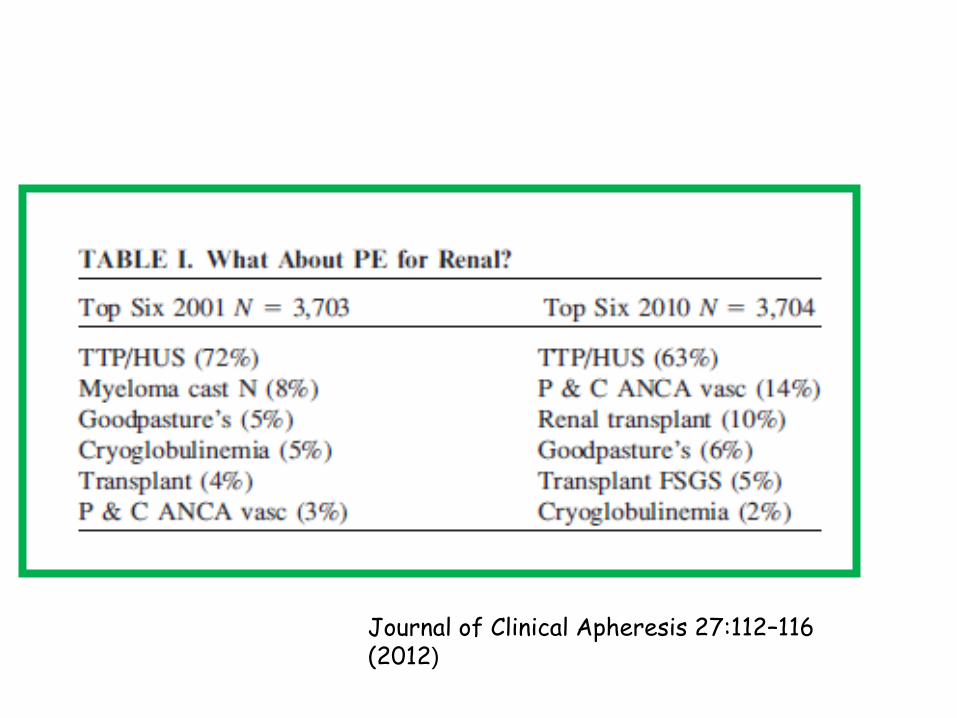
Journal of Clinical Apheresis 27:112–116 (2012)

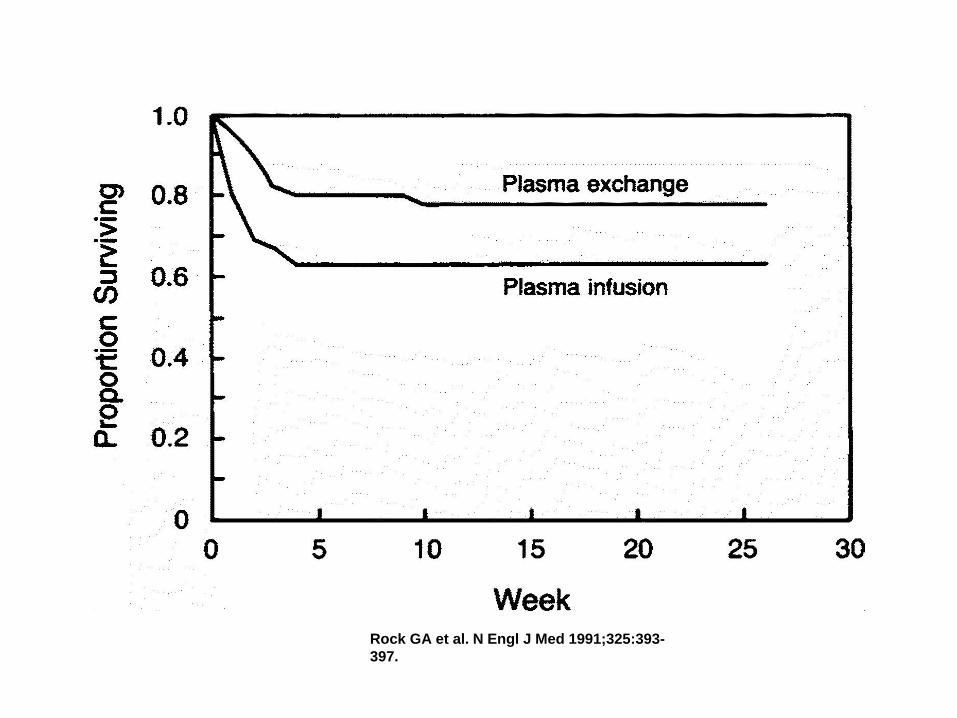
Survival of Patients with Thrombotic Thrombocytopenic Purpura.
Rock GA et al. N Engl J Med 1991;325:393-
397.
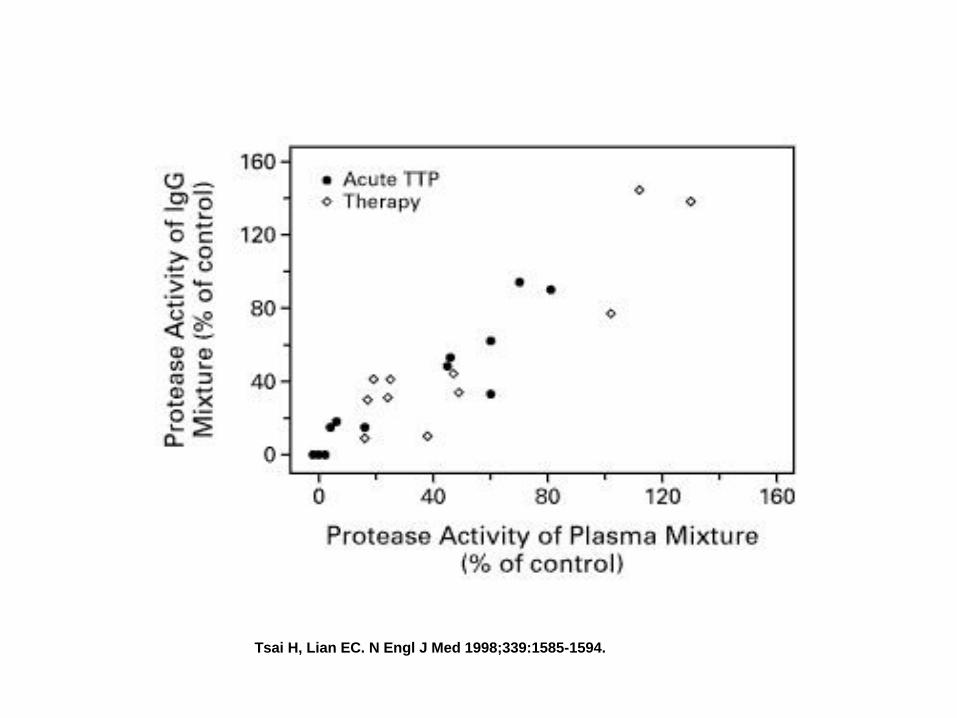
Inhibitory Activity of IgG from 12 Patients with Acute Thrombotic Thrombocytopenic Purpura (TTP) and from 11 Patients after Plasma-Exchange Therapy Was Instituted as a Function of the
Inhibitory Activity of Plasma Samples from Which IgG Was Isolated.
Tsai H, Lian EC. N Engl J Med 1998;339:1585-1594.
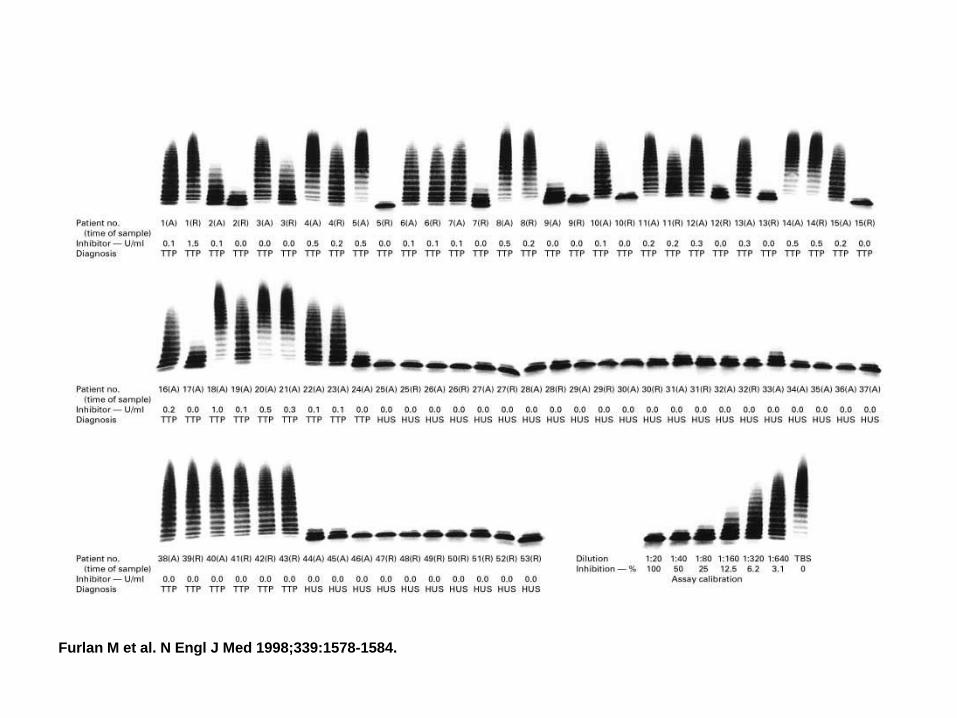
Activity of von Willebrand Factor–Cleaving Protease and the Level of Its Inhibitor in 24 Patients with Nonfamilial Thrombotic Thrombocytopenic Purpura (Patients 1 to 24), 13 Patients with
Nonfamilial Hemolytic–Uremic Syndrome (Patients 25 to 37), 6 Patients with Familial Thrombotic Thrombocytopenic Purpura (Patients 38 to 43), and 10 Patients with Familial Hemolytic–Uremic
Syndrome (Patients 44 to 53).
Furlan M et al. N Engl J Med 1998;339:1578-1584.


Plazma değişim prensipleri
• Mümkün olan en kısa sürede başlanmalıdır.
• Kötü gidiş için bağımsız risk faktörüdür.
• Ancak TPD gecikecek ise plazma infüzyonu seçenek olmalıdır.– Ann Hematol. 1995;70(6): 319–323.
• İlk üç gün günlük ve 1.5 plazma hacmi(60 ml/kg)
• Nörolojik bulgularda ilerleme veya kardiyak tutulum var ise(troponin artışı) günde iki kez de yapılabilir.
• Rituximab ve steroid klirensi ne olacak?
• En az 12 saat
• Mümkün ise gün aşırı TPD
• Değil ise sık Rituximab uygulaması(3 günde bir gibi)

Trombosit sayısı iki gün üst üste
150 binin üzerinde ise TPD sonlandırılır.

• aHUS hastaları hızla tedavi edilmelidir.
• Genetik sonuçlar çıkana kadar plazma infüzyonu yapılabilir.– 60-65 ml/kg/hafta
– 20 ml/kg/hafta idame
• MCP mutasyonlarında TPD etkisizdir.
• İlk seçenek TPD’dir.– 5 gün üst üste+ 2 hafta haftada 5 gün+2 hafta haftada 3 gün
ve 33.gün değerlendirme

• TPD genellikle graft kaybını önlemekte yetersiz kalmaktadır.
• Bu nedenle transplantasyondan hemen önce proflaktik olarak yapılması önerilmektedir.
• Etkinlik ???
– Proflaktik olarak yapılan ve yapılmayanlar arasında fark var ANCAK…
• Le Quintrec M, Zuber J, Moulin B, Kamar N, Jablonski M, Lionet A, Chatelet V,Mousson C,Mourad G, Bridoux F, Cassuto E, Loirat C, Rondeau E, Delahousse M,
Frémeaux-Bacchi V (2013)Complement genes strongly predict recurrence and graft outcome in adult renal transplant recipients with atypical hemolytic and uremic
syndrome. Am J Transplant 13:663–675.
• Saland JM, Ruggenenti P, Remuzzi G, Consensus Study Group (2009) Liver–kidney transplantation to cure atypical hemolytic uremic syndrome. J Am Soc Nephrol
20:940–949 75.
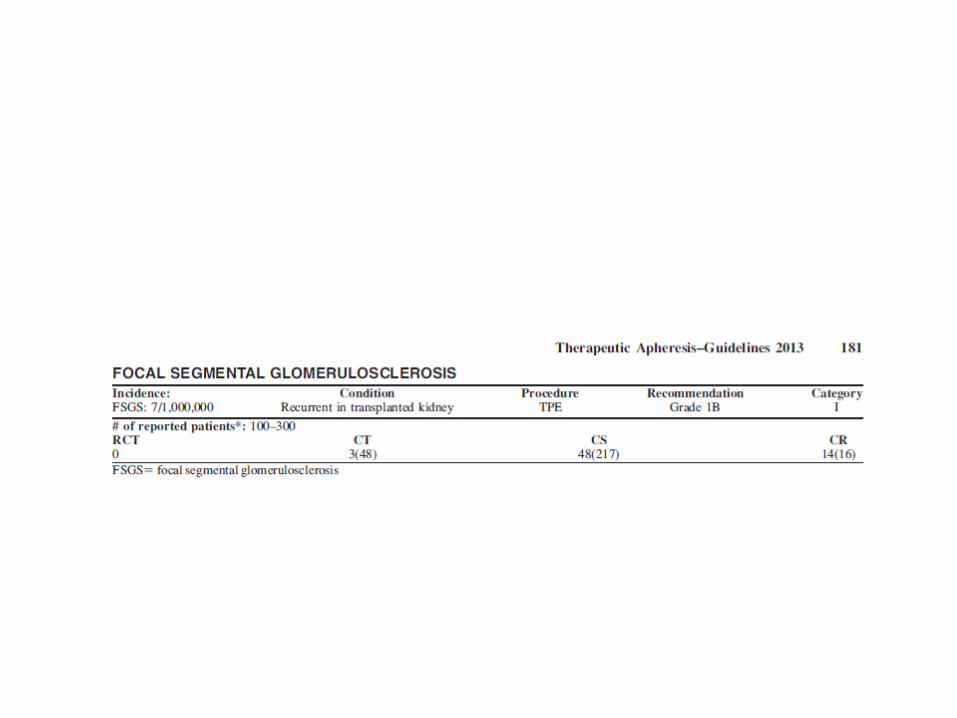
FSGS
• En az 40 yıldır FSGS’nin böbrek transplantasyonu sonrası tekrarlayabileceğini biliyoruz.
• TPD’in bu hasta grubunda etkinliğini kanıtlayan çok sayıda çalışma mevcut.
• Hoyer JR, Vernier RL, Najarian JS, Raij L, Simmons RL, Michael AF: Recurrence of idiopathic nephrotic syndrome after renal transplantation, 1972. J Am Soc Nephrol 12:1994–2002.
• Meyrier A: Nephrotic focal segmental glomerulosclerosis in 2004: an update. Nephrol Dial Transplant 19:2437–2444, 2004.
• Valdivia P, Gonzalez Roncero F, Gentil MA, Jimenez F, Algarra G, Pereira P, Rivera M, Suner M, Cabello V, Toro J, Mateos J: Plasmapheresis for the prophylaxis and treatment of recurrent focal segmental glomerulosclerosis following renal transplant. Transplant Proc 37:1473–1474, 2005.
• Schachter ME, Monahan M, Radhakrishnan J, Crew J, Pollak M, Ratner L, Valeri AM, Stokes MB, Appel GB: Recurrent focal segmental glomerulosclerosis in the renal allograft: single center experience in the era of modern immunosuppression. Clin Nephrol 74:173– 181, 2010.
• Ponticelli C, Glassock RJ: Posttransplant recurrence of primary glomerulonephritis. Clin J Am Soc Nephrol 5:2363–2372, 2010.
• Zimmerman SW: Plasmapheresis and dipyridamole for recurrent focal glomerular sclerosis. Nephron 40:241–245, 1985.
• Gungor O, Sen S, Kircelli F, Yilmaz M, Sarsik B, Ozkahya M, Hoscoskun C, Ok E, Toz H: Plasmapheresis therapy in renal transplant patients: five-year experience. Transplant Proc 43:853–857, 2011.
• Tsagalis G, Psimenou E, Nakopoulou L, Laggouranis A: Combination treatment with plasmapheresis and rituximab for recurrent focal segmental glomerulosclerosis after renal transplantation. Artif Organs 35:420–425, 2011.
• Moroni G, Gallelli B, Quaglini S, Banfi G, Montagnino G, Messa P: Long-term outcome of renal transplantation in adults with focal segmental glomerulosclerosis. Transpl Int 23:208–216, 2010.
• Gonzalez E, Ettenger R, Rianthavorn P, Tsai E, Malekzadeh M: Preemptive plasmapheresis and recurrence of focal segmental glomerulosclerosis in pediatric renal transplantation. Pediatr Transplant 15:495–501, 2011.

• Erişkinlerde transplant sonrası rekürens %23’lerde ancak çocuklarda oran daha da yüksektir.
• Transplant sonrası ilk 10 gün 0.5gr/günden yüksek proteinüri rölaps olduğunu düşündürmelidir.
• 3gr/günün üzerindeki proteinürinin TPD’den yarar görmesi beklenmez.

• TPD ile birlikte steroid ve siklofosfamid standart tedavi iken
• MMF ve Rituximab da kullanılmaktadır.– Schachter ME, Monahan M, Radhakrishnan J, Crew J, Pollak M, Ratner L, Valeri AM, Stokes MB, Appel GB: Recurrent focal segmental
glomerulosclerosis in the renal allograft: single center experience in the era of modern immunosuppression. Clin Nephrol 74:173– 181, 2010.
– Tsagalis G, Psimenou E, Nakopoulou L, Laggouranis A: Combination treatment with plasmapheresis and rituximab for recurrent focal
segmental glomerulosclerosis after renal transplantation. Artif Organs 35:420–425, 2011.

FSGS’de TPD prensipleri
• İlk üç gün günlük daha sonra ise haftada 3 gün iki hafta süre ile işlem gerçekleştirilir.
• Bu aşamadan sonra idrar protein ve serum kreatinin değerleri ölçülerek remisyon elde edilene kadar haftada 2-3 olacak şekilde devam edilir.
– Szczepiorkowski ZM, Winters JL, Bandarenko N, Kim HC, Linenberger ML, Marques MB, Sarode R, Schwartz J, Weinstein R, Shaz BH: Guidelines on the use of therapeutic apheresis in clinical practice—evidence-based approach from the Apheresis Applications Committee of the American Society for Apheresis. J Clin Apher 25:83–177, 2010.
– Valdivia P, Gonzalez Roncero F, Gentil MA, Jimenez F, Algarra G, Pereira P, Rivera M, Suner M, Cabello V, Toro J, Mateos J: Plasmapheresis for the prophylaxis and treatment of recurrent focal segmental glomerulosclerosis following renal transplant. Transplant Proc 37:1473–1474, 2005.
– Moroni G, Gallelli B, Quaglini S, Banfi G, Montagnino G, Messa P: Long-term outcome of renal transplantation in adults with focal segmental glomerulosclerosis. Transpl Int 23:208–216, 2010.
– Gonzalez E, Ettenger R, Rianthavorn P, Tsai E, Malekzadeh M: Preemptive plasmapheresis and recurrence of focal segmental glomerulosclerosis in pediatric renal transplantation. Pediatr Transplant 15:495–501,
2011.
– Schachter ME, Monahan M, Radhakrishnan J, Crew J, Pollak M, Ratner L, Valeri AM, Stokes MB, Appel GB: Recurrent focal segmental glomerulosclerosis in the renal allograft: single center experience in the era of
modern immunosuppression. Clin Nephrol 74:173–181, 2010.
• İmmünabsorpsiyon
• LDL aferezi
• Double filtrasyon
Komplikasyonlar
• Enfeksiyon(1.48/1000 ve 1.59/1000)
• Damar yolu problemleri(1.48/1000 ve 1.59/1000)

Komplikasyonlar-II
• Aferez ilişkili olanlar;– TPD: %6.9
– DFPP: %9.7
– En sık hipotansiyon ve işlemin erken bitirilmek zorunda kalınması