Embed Size (px)
DESCRIPTION
Preoperative PET-CT in papillary thyroid cancer. Chung- Ang University, Korea Department of Surgery. Byung Seup Kim, Ju Won Seok , Han suk Ryu , Kyung Ho Kang, Sung Jun Park, Bo Youn Cho. Introduction. FDG. PET – CT. 2-[fluorine-18] f luoro-2- d eoxy- glucose. Introduction. - PowerPoint PPT Presentation
Citation preview

Preoperative PET-CT in papillary thyroid cancer
Chung-Ang University, KoreaDepartment of Surgery
Byung Seup Kim, Ju Won Seok, Han suk Ryu, Kyung Ho Kang, Sung Jun Park, Bo Youn Cho

Introduction
PET – CT 2-[fluorine-18]fluoro-2-deoxy- glucose
FDG

Introduction
Meaning of FDG -uptake
Rate of uptake of FDG is proportional to
metabolic activity
An introduction to PET-CT imaging. Radigraphics 2004; 523-543
Uptake of FDG
Metabolic activity

Flip – flop phenomenon
PTC

Introduction
About Primary le-sion
We evaluated the FDG uptake of papillary thy-roid cancer in preoperative PET CT.

Method
FNAB :Papillary thy-roid cancer
Preoperative PET-CT
Operation
Period : 2011.3.1 ~ 2012. 2. 29PTC was preoperatively confirmed by FANBCND was routinely performed.Preoperative PET CT was performed when patient argeed it Enrolled patients : 194

Divided into PET negative(-) and positive(+) group
Negative ;Absence of FDG up-tatke
Postive ;Presence of FDG up-take
VS.
Method
Backgroud : surrounding thyroid tis-sue

Method
1. Analyze the cliniopathologic factors related to PET (+)2. .Analyze quantity of SUVmax value according to clinicopathologic factors
SUVmax : maximal standardized uptake value SUVmax of PET negative patient = SUV of surrounding thy-roid tissue

ResultsPET sensitivity
① Primary tumor : 71.7% (138/194 pa-tients)
② Central lymph node metz. : 4.3% (3/70 patients)
③ Lateral lymph node metz. : 62.5% (15/24 pa-tients) False positive : 1.1%

ResultsTable 1-1. PET-CT and clinicopathologic parameters
Variables PET (-) PET (+) P value(n=56, 28.9%) (n=138, 71.7%)
Sex Male 19 (33.9 %) 21 (15.2%) 0.004
Female 37 (66.1%) 117 (84.8%) Age < 45 years 22 (39.3%) 61 (44.2%) 0.530
≥ 45 years 34 (60.7%) 77 (55.8%) Size ≤ 1cm 49 (87.5%) 77 (55.8%) <0.001
> 1cm 7 (12.5%) 61 (44.2%) Multicenticity Absence 31 (55.4%) 71 (51.4%) 0.621
Presence 25 (44.6%) 67 (48.6%) Extrathyroidal extension Absence 43 (76.8%) 87 (63.0%) 0.065
Presence 13 (23.2%) 51 (37.0%) Lymph node metastasis Absence 33 (58.9%) 67 (48.6%) 0.190
Presence 23 (41.1%) 71 (51.4%)

Table 1-2. PET-CT and clinicopathologic parameters
Variables PET (-) PET (+) P value(n=56, 28.9%) (n=138, 71.7%)
Coexisting pathology 0.001 None 31 (55.4%) 41 (29.7%) Nodular hyperplasia (NH) 18 (32.1%) 40 (29.0%) Hashimoto thyroiditis (HT) 5 (8.9%) 36 (26.1%) NHa+ HTb 2 (3.6%) 21 (15.2%)Subtype of PTC 0.001 Classic 38 (67.9%) 110 (79.7%) Follicular variant 17 (30.4%) 12 (8.7%) Oncocytic variant 1 (1.8%) 14 (10.1%) Solid 0 (0%) 1 (0.7%) Tall cell variant 0 (0%) 1 (0.7%)
Coexisting pathology 0.001 Abscence 31 (43.1%) 41 (56.9%) Presence 25 (20.5%) 97 (79.5%)Subtype of PTC <0.001 Non-follicular variant 39 (23.6%) 126 (76.4%) Follicular variant 17 (58.6%) 12 (41.4%)

ResultsTable 2. PET positivity and cliniocopathologic parameters by logistic regression
Variable Hazard ratio (95% CIb) P value
Sex Male 1 (reference) 0.021
Female 2.843 ( 1.171 - 6.905)
Size ≤ 1cm 1 (reference) < 0.001
> 1cm 8.090 (3.000 - 21.813)
Coexisting pathology Absence 1 (reference) 0.005
Presence 2.983 (1.393 - 6.386)
Subtype of PTCa Follicular variant 1 (reference) 0.003
Non-follicular variant 4.032 (1.619 - 10.038) PTCa Papillary thyroid cancer

2. Analysis for quantity of FDG uptake

SUVmax
Kolmogorov-Smirnove goodness
P < 0.001
Non normally distributed data

Table 3. SUVmax by clinicopathologic parameters
Variables N Median Q25 - Q75 P valueSex Male 40 1.850 1.000 - 4.175 0.042 Female 154 2.700 1.575 - 4.400 Age < 45 years 83 2.700 1.000 - 4.200 0.658 ≥ 45 years 111 2.500 1.000 - 4.400 Tumor size ≤ 1cm 126 2.100 1.000 - 3.000 0.001 > 1cm 68 4.900 2.900 -10.200 Multicenticity Absence 102 2.600 1.000 - 4.525 0.888 Presence 92 2.600 1.000 - 4.300 Extrathyroidal extension Absence 130 2.300 1.000 - 3.300 < 0.001 Presence 64 4.00 1.900 - 9.400 Lymph node metastasis Absence 100 2.400 1.000 - 3.400 0.017 Presence 94 3.000 1.125 - 5.000 Coexisting pathology 0.253 None 72 2.150 1.875 - 4.225 Nodular hyperplasia (NH) 58 2.300 1.000 – 4.150 Hashimoti thyroiditis (HT) 35 2.800 2.400 – 4.100 NH + HT 22 3.450 2.475 – 4.475Subtype of PTC (Papillary thyroid cancer) 0.001 Classic 148 2.750 1.000 – 4.875 Follicular variant 29 1.000 1.000 – 2.450 Oncocytic variant 15 2.900 2.300 – 3.200 Solid 1 2.100 Not availabled
Tall cell variant 1 8.300 Not availabled
d The number of case was only one so that quartile was not available

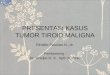
P value < 0.001
SUVmax 2.6 sensitivity 70.3% specificity 60.0%
Analysis for quantity of FDG uptake
Relationship between extrathyroidal extension and SUVmax
ROC curve
1-specificity

Results
ETE (-) (n=130, 67.0%)
ETE (+)(n=64, 33.0%) P value
Lymph node metz.
(+) 52 (40.0%) 42 (65.6%) 0.001
Size > 1cm 31 (23.8%) 64 (33.0%) < 0.001
Age ≥ 45 years 74 (56.9%) 37 (57.8%) 0.906
Female 107 (82.3%) 47 (73.4%) 0.151
Multicenticity 59 (45.7%) 33 (51.6%) 0.446
SUVmax ≥ 2.6 55 (42.3%) 45 (70.3%) <0.001
Subtype (follicular) 24 (18.5%) 4 (6.3%) 0.029
Coexisting pathology 82 (63.1%) 40 (62.5%) 0.938
Cliniopathologic factors and Extrathyroidal exnte-sion by univariate analysis

Extrathyroidal extension and clinicopathologic factors by mulivariate analysis
Variable Hazard ratio (95% CI) P-value
Lymph node metz. Absence 1 (reference) 0.046
Presence 2.063 ( 1.014 – 4.199)
Size ≤ 1cm 1 (reference) 0.016
> 1cm 2.552( 1.193 – 5.460)
SUVmax < 2.6 1 (reference) 0.316
≥ 2.6 1.488 (0.684 – 3.238)
Subtype Follicular variant 1 (reference) 0.114
Non follicular variant 4.469 (1.757 – 11.371)
→ SUVmax was not related to extrathyroidal ex-tension

Results
LN metz. (-) (n=100, 51.5%)
LN metz. (+)(n=94, 48.5%) P-value
Extrathyroidal ext.
(+)22 (22.0%) 42 (44.7%) 0.001
Size > 1cm 25 (25.0%) 43 (45.7%) 0.002
Age ≥ 45 years 72 (72.0%) 39 (41.5%) <0.001
Female 81(81.0%) 73 (77.7%) 0.565
Multicenticity 45 (45.5%) 47 (50.0%) 0.527
SUVmax ≥ 2.9 38 (38.0%) 49 (52.1%) 0.048
Subtype(follicular) 20 (20.0%) 8 (8.5%) 0.023
Coexisting pathology 65 (65.0%) 57 (60.6%) 0.530
Cliniopathologic factors and lymph node metastasis by univariate analysis

Variable Hazard ratio (95% CI) P value
ETE Absence 1 (reference) 0.011
Presence 2.503 ( 1.231 – 5.090)
Size ≤ 1cm 1 (reference) 0.081
> 1cm 1.972( 0.919 – 4.234)
Age < 45 years 0.245 (0.129 – 0.466) <0.001
≥ 45 years 1 (reference)
SUVmax < 2.9 1 (reference) 0.884
≥ 2.9 0.947 (0.455 – 1.971)
Subtype Follicular variant 1 (reference) 0.103
Non-follicular variant 2.255 (0.848 – 5.993)
Lymph node metastasis and clinicopathologic factors by mulivariate analysis
→ SUVmax was not related to lymph node metastasis

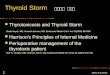
Subtype
P value < 0.001
FDG 2.0 sensitivity 70.9% specificity 69.0 %
Relationship between Non-follicular subtype and SUVmax
ROC curve
1-specificity

Results
Non follicular (n=165, 85.1%)
follicular(n=29, 14.9%) P-value
Extrathyroidal ex-tension 60 (36.1%) 4 (14.3%) 0.018
Lymph node metz. 86 (51.8) 9 (28.6%) 0.042
Size > 1cm 62 (37.3%) 6 (21.4%) 0.079
Age ≥ 45 years 94 (56.6%) 17 (60.7) 0.686
Female 133 (80.7%) 21 (71.4%) 0.261
Multicenticity 81 (49.1%) 12 (39.3%) 0.337
SUVmax ≥ 2.0 117 (70.9%) 9 (28.6%) <0.001
Coexisting pathology 107 (64.5%) 15 (53.6%) 0.270
Cliniopathologic factors and subtype of PTC by univariate analysis

Non-follicular variant and clinicopathologic fac-tors
by mulivariate analysis
Variable Hazard ratio (95%
CI)P value
Extrathyroidal
extensionAbsence 1 (reference) 0.092
Presence2.690 (0.851 -
8.502)
Lymph node
metastasisAbsence 1 (reference) 0.141
Presence1.964 (0.800 –
4.820)
SUVmax of primary
lesion< 2.0 1 (reference) <0.001
≥ 2.05.044 (2.111 –
12.056)

Conclusion
The usefulness of preoperative PET-CT for PTC was not yet certain.
PET positive results and SUVmax had no relation to signifi-cant clinical factors such as extrathyroidal extension and lymph node metastasis.
PET negative results or low SUVmax indicate the possibility of follicular variant subtype in papillar thyroid cancer.

Thank you for your at-tention