Embed Size (px)
Citation preview
Case study from Mexico
PRIMARY HEALTH CARE SYSTEMS (PRIMASYS)


Case study from Mexico
PRIMARY HEALTH CARE SYSTEMS (PRIMASYS)
Jacqueline Alcalde-Rabanal,a Victor Becerril-Montekio,a Julio Montañez-Hernandez,a Olga Espinosa-Henao,a Rafael Lozano,b Luis García-Bello,a Elliot Lagunas-Alarcon,a Alejandro Torres-Grimaldoa
a. National Institute of Public Health, Centre for Health Systems Researchb. Institute for Health Metrics and Evaluation, UW

PRIMARY HEALTH CARE SYSTEMS (PRIMASYS)
WHO/HIS/HSR/17.26
© World Health Organization 2017
Some rights reserved. This work is available under the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 IGO licence (CC BY-NC-SA 3.0 IGO; https://creativecommons.org/licenses/by-nc-sa/3.0/igo).
Under the terms of this licence, you may copy, redistribute and adapt the work for non-commercial purposes, provided the work is appropriately cited, as indicated below. In any use of this work, there should be no suggestion that WHO endorses any specific organization, products or services. The use of the WHO logo is not permitted. If you adapt the work, then you must license your work under the same or equivalent Creative Commons licence. If you create a translation of this work, you should add the following disclaimer along with the suggested citation: “This translation was not created by the World Health Organization (WHO). WHO is not responsible for the content or accuracy of this translation. The original English edition shall be the binding and authentic edition”.
Any mediation relating to disputes arising under the licence shall be conducted in accordance with the mediation rules of the World Intellectual Property Organization.
Suggested citation. Primary health care systems (PRIMASYS): case study from Mexico. Geneva: World Health Organization; 2017. Licence: CC BY-NC-SA 3.0 IGO.
Cataloguing-in-Publication (CIP) data. CIP data are available at http://apps.who.int/iris.
Sales, rights and licensing. To purchase WHO publications, see http://apps.who.int/bookorders. To submit requests for commercial use and queries on rights and licensing, see http://www.who.int/about/licensing.
Third-party materials. If you wish to reuse material from this work that is attributed to a third party, such as tables, figures or images, it is your responsibility to determine whether permission is needed for that reuse and to obtain permission from the copyright holder. The risk of claims resulting from infringement of any third-party-owned component in the work rests solely with the user.
General disclaimers. The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of WHO concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted and dashed lines on maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by WHO in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
All reasonable precautions have been taken by WHO to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall WHO be liable for damages arising from its use.
The named authors alone are responsible for the views expressed in this publication.
Editing and design by Inís Communication – www.iniscommunication.com
CASE STUDY FROM MEXICO
Contents
Abbreviations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
Background to PRIMASYS case studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
1. Objectives . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
1.1 General objective . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
1.2 Specific objectives . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
2. Methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
2.1 Sources of information . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
2.2 Key informants . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
3. Overview of Mexican health care system . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
4. Timeline of key developments in Mexican health system . . . . . . . . . . . . . . . . . . . . . . . . . 8
5. Governance . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
6. Financing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
7. Human resources for health . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
8. Planning and implementation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
9. Regulatory process . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
10. Monitoring and information system . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
11. Policy considerations and ways forward . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
Annex 1. Key informants for Mexico PRIMASYS case study . . . . . . . . . . . . . . . . . . . . . . . . . 35
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36
iv PRIMARY HEALTH CARE SYSTEMS (PRIMASYS)
FiguresFigure 1. Structure of the Mexican health system. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
Figure 2. Timeline of key developments in the Mexican health system . . . . . . . . . . . . . . . . . 10
Figure 3. Primary health care in Mexico. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
Figure 4. IMSS primary health care organization . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
Figure 5. Percentage of public expenditure on primary health care, national and by source of financing, Mexico 2014 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
Figure 6. Percentage of total public health expenditure on PHC by state, Mexico 2014 . . . . . . . 17
Figure 7. Per capita PHCE by state (US$), Mexico 2014. . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
Figure 8. Distribution of health personnel in hospitals and primary health facilities (%) . . . . . . . 20
Figure 9. Density of physicians per 1000 inhabitants, 2013–2015, in various categories . . . . . . . 21
Figure 10. Density of physicians per 1000 inhabitants in primary health facilities by state, 2015 . . 22
Figure 11. Density of nurses per 1000 inhabitants, 2013–2015, in various categories . . . . . . . . . 22
Figure 12. Density of nurses per 1000 inhabitants in primary health facilities by state, 2015 . . . . . 23
Figure 13. Rural/urban density of physician and nurses per 1000 inhabitants in primary health facilities, Ministry of Health, by state, 2015 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
Figure 14. Density of community health workers per 1000 inhabitants in Ministry of Health first-level care facilities, 2013–2015 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
Figure 15. Density of community health workers per 1000 inhabitants in Ministry of Health first-level care facilities, by state, 2015. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
Figure 16. Number and percentage density of traditional midwives by state, Mexico, 2016 . . . . . 25
TablesTable 1. Sources of information for Mexico PRIMASYS case study . . . . . . . . . . . . . . . . . . . . . 4
Table 2. Number of primary health facilities and hospitals in Mexico, 2013–2015 . . . . . . . . . . . . 6
Table 3. Mexico: demographic and health indicators . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Table 4. Distribution of total health expenditure on primary health care, by financing agent . . . . 15
Table 5. Ministry of Health expenditure on PHC for population with no social security, by health programme (US$), Mexico 2014 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
Table 6. Categories of personnel in primary health facilities in Mexico . . . . . . . . . . . . . . . . . . 21
Table 7. Physicians and nurses availability in primary health facilities by institution . . . . . . . . . . 21
Table 8. Health care services: infrastructure offered, by institution, Mexico 2015 . . . . . . . . . . . . 26
Table 9. Follow-up and outcome indicators related to PHC. . . . . . . . . . . . . . . . . . . . . . . . . 31
1CASE STUDY FROM MEXICO
Abbreviations
AFASPE Public Health Actions in Federated Entities
CAUSES Universal Health Services Catalogue
CLUES National Catalogue of Health Facilities
COFEPRIS Federal Commission for Protection against Sanitary Risks
CONEVAL National Council for the Evaluation of Social Development Policy
CPG clinical practice guide
DGIS General Directorate of Health Information
ENSANUT National Health and Nutrition Survey
FASSA Health Care Services Contributions Fund
GDP gross domestic product
ICD-10 International Classification of Diseases and Related Health Problems, 10th Revision
IMSS Mexican Social Security Institute
INEGI National Statistics and Geography Institute
ISSFAM Social Security Institute for the Mexican Armed Forces
ISSSTE Institute for Social Security and Services for State Workers
MAI Comprehensive Health Care Model
MOPS Health Promotion Operational Model
OECD Organisation for Economic Co-operation and Development
PHC primary health care
PHCE primary health care expenditure
PHCE% PHC expenditure as a percentage of total health expenditure
PPP purchasing power parity
PROGRESA Education, Health and Nutrition Conditional Cash Transfer Programme
SEMAR Marine Secretariat
SESA States Health Services
SICUENTAS Federal and State Health Accounts Subsystem
SiNaCEAM National System for the Certification of Medical Care Establishments
SINAIS National System of Health Information
SINERHIAS Information System on Medical Equipment, Infrastructure and Human Resources for Health Care
SIODM Millennium Development Goals Information System
SPSS Social Protection for Health System

2 PRIMARY HEALTH CARE SYSTEMS (PRIMASYS)
Background to PRIMASYS case studies
Health systems around the globe still fall short of providing accessible, good-quality, comprehensive and integrated care. As the global health community is setting ambitious goals of universal health coverage and health equity in line with the 2030 Agenda for Sustainable Development, there is increasing interest in access to and utilization of primary health care in low- and middle-income countries. A wide array of stakeholders, including development agencies, global health funders, policy planners and health system decision-makers, require a better understanding of primary health care systems in order to plan and support complex health system interventions. There is thus a need to fill the knowledge gaps concerning strategic information on front-line primary health care systems at national and subnational levels in low- and middle-income settings.
The Alliance for Health Policy and Systems Research, in collaboration with the Bill & Melinda Gates Foundation, is developing a set of 20 case studies of primary health care systems in selected low- and middle-income countries as part of an initiative entitled Primary Care Systems Profiles and Performance (PRIMASYS). PRIMASYS aims to advance the science of primary health care in low- and middle-income countries in order to support efforts to strengthen primary health care systems and improve the implementation, effectiveness and efficiency of primary health care interventions worldwide. The PRIMASYS case studies cover key aspects of primary health care systems, including policy development and implementation, financing, integration of primary health care into comprehensive health systems, scope, quality and coverage of care, governance and organization, and monitoring and evaluation of system performance.
The Alliance has developed full and abridged versions of the 20 PRIMASYS case studies. The abridged version provides an overview of the primary health care system, tailored to a primary audience of policy-makers and global health stakeholders interested in understanding the key entry points to strengthen primary health care systems. The comprehensive case study provides an in-depth assessment of the system for an audience of researchers and stakeholders who wish to gain deeper insight into the determinants and performance of primary health care systems in selected low- and middle-income countries. Furthermore, the case studies will serve as the basis for a multicountry analysis of primary health care systems, focusing on the implementation of policies and programmes, and the barriers to and facilitators of primary health care system reform. Evidence from the case studies and the multi-country analysis will in turn provide strategic evidence to enhance the performance and responsiveness of primary health care systems in low- and middle-income countries.
3CASE STUDY FROM MEXICO
1. Objectives
1.1 General objectiveThe general objective of this case study is to analyse the structure, processes and outcomes of the Mexican primary care system in order to draw cross-cutting lessons and to better understand the determinants of its key successes and failures.
1.2 Specific objectivesThe specific objectives of the case study are:
• to summarize key aspects of the structures, processes and outcomes of the country’s primary care system that reflect their performance in the areas of service organization, governance, human resources and financing;
• to elaborate specific pathways that have contributed to notable successes or failures in the country’s primary care system;
• to promote learning among relevant stakeholders in order to motivate policy change.
4 PRIMARY HEALTH CARE SYSTEMS (PRIMASYS)
2. Methods
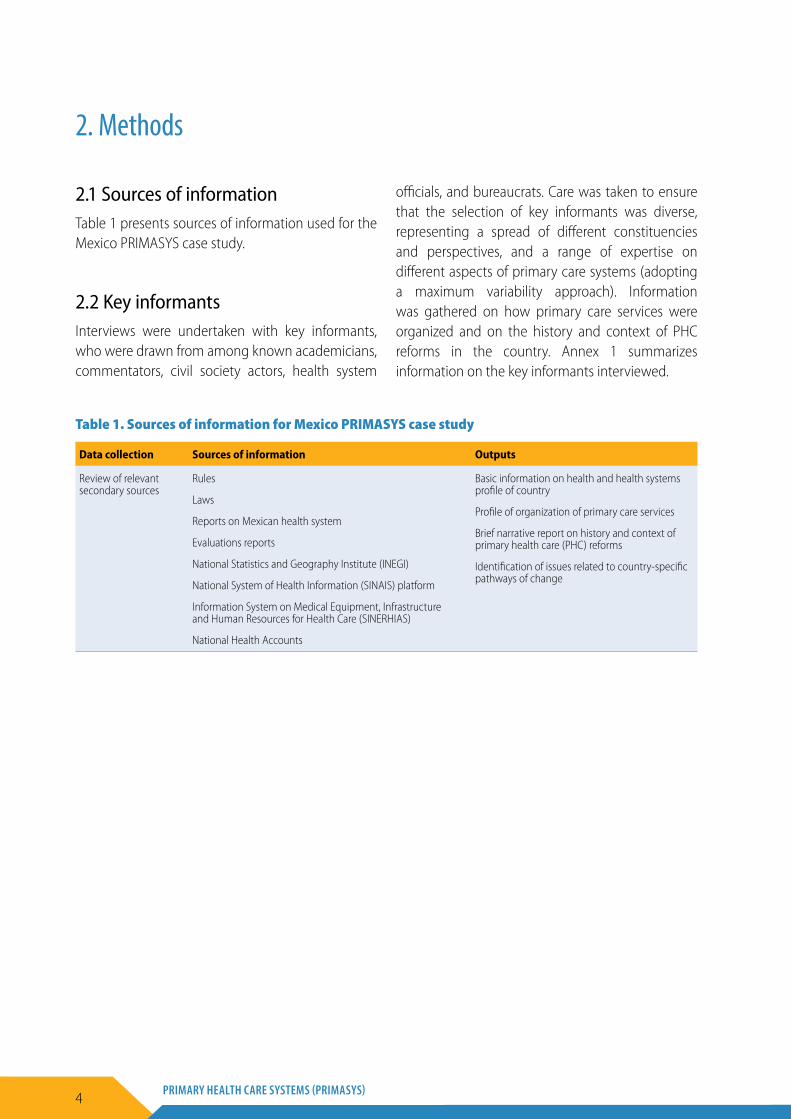
2.1 Sources of information Table 1 presents sources of information used for the Mexico PRIMASYS case study.
2.2 Key informants Interviews were undertaken with key informants, who were drawn from among known academicians, commentators, civil society actors, health system
officials, and bureaucrats. Care was taken to ensure that the selection of key informants was diverse, representing a spread of different constituencies and perspectives, and a range of expertise on different aspects of primary care systems (adopting a maximum variability approach). Information was gathered on how primary care services were organized and on the history and context of PHC reforms in the country. Annex 1 summarizes information on the key informants interviewed.
Table 1. Sources of information for Mexico PRIMASYS case study
Data collection Sources of information Outputs
Review of relevant secondary sources
Rules
Laws
Reports on Mexican health system
Evaluations reports
National Statistics and Geography Institute (INEGI)
National System of Health Information (SINAIS) platform
Information System on Medical Equipment, Infrastructure and Human Resources for Health Care (SINERHIAS)
National Health Accounts
Basic information on health and health systems profile of country
Profile of organization of primary care services
Brief narrative report on history and context of primary health care (PHC) reforms
Identification of issues related to country-specific pathways of change

5CASE STUDY FROM MEXICO
3. Overview of Mexican health care system
Mexico is located between the United States of America and Central America. According to a 2015 survey (between two censuses), the estimated population of Mexico was 119.5 million people in that year, with a projected 137 million by 2030 (1). In 2015, the population aged under 15 years represented 27% of the total population, people aged between 15 and 64 represented 65% and those above 65 were 7.2%. Mexico has undergone an increasing urbanization process. In 1950 around 43% of the population lived in urban areas; by 1990 this population represented 71%, attaining 79% in 2015 (2). According to the National Council for the Evaluation of Social Development Policy (CONEVAL, for its Spanish initials),1 in 2014, 46% of the population lived in poverty, of which 36.6% lived in moderate poverty and 9.6% in extreme poverty (3).
In accordance with the 10th Revision of the International Classification of Diseases and Related Health Problems (ICD-10), the main mortality causes were diabetes mellitus, ischaemic heart diseases, cerebrovascular disease, cirrhosis and other chronic liver diseases, and chronic obstructive pulmonary disease. At the same time, there has been a significant increase in risk factors, such as obesity and overweight, physical inactivity, consumption of high caloric content food, as well as use of tobacco, alcohol and illicit drugs (4).
The Mexican economy has experienced a long-term decrease of its growth rate during the last three decades. In 2015, Mexico’s gross domestic product (GDP) was US$ 1143.79 billion, while the GDP value of Mexico represented 1.84% of the world economy. According to per capita GDP, Mexico is ranked 76th among 196 countries. The Gini coefficient, measuring inequality of income, was 0.503, placing Mexico as a country with a significant income inequality. Total health expenditure as a proportion
of GDP is 5.78%, below the percentage of other Latin American countries such as Uruguay and Brazil (both 8.9%). Public health expenditure is 53% of total health expenditure, while out-of-pocket expenditure accounts for 41%.
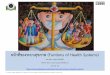
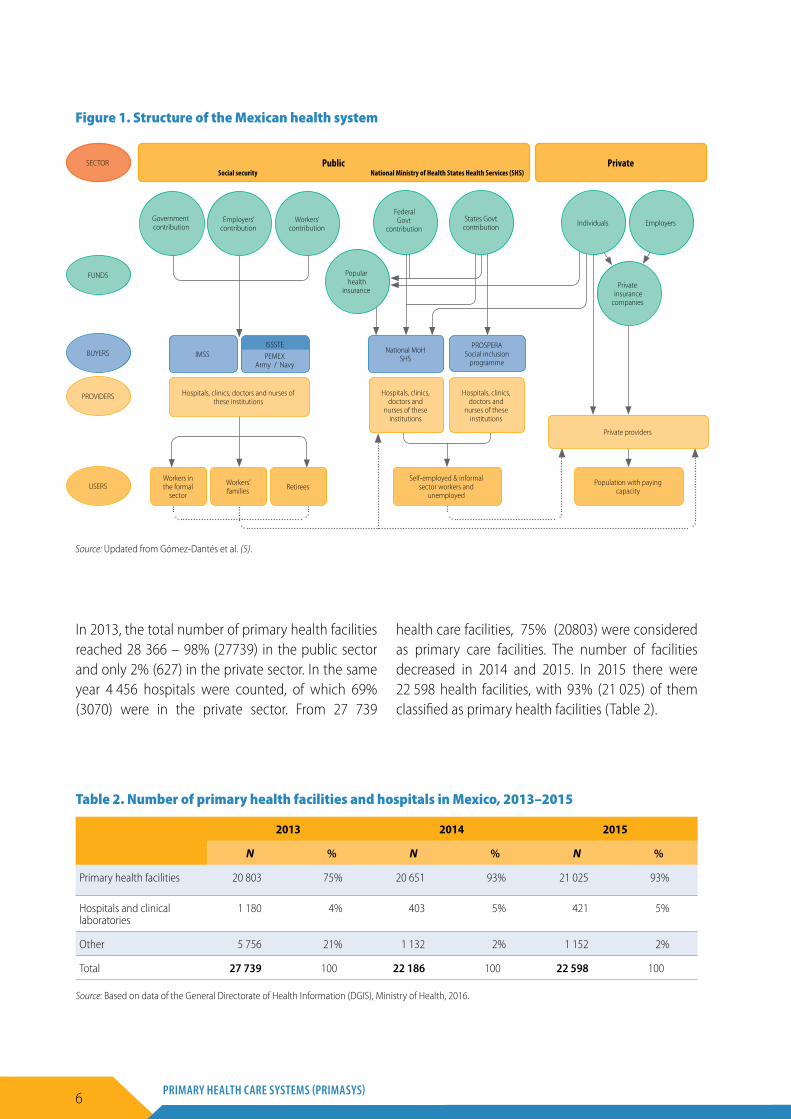
Figure 1 presents the structure of the Mexican health system (5, 6). Despite the efforts of the recent reform, today Mexicans still have access to very different levels of health coverage, and receive health care from separate institutions that are independent from one another.
The public sector is responsible for the health care of the beneficiaries of the social security institutions as well as of the population outside the social security system. The social insurance covers the health care of the employees and their families and offers advantages such as retirement insurance. The Mexican Social Security Institute (IMSS) covers the employees of the formal private sector; the Institute for Social Security and Services for State Workers (ISSSTE) covers the employees of the federal and states governments. The national oil company (PEMEX) covers its employees; and the employees of the army and the navy are covered by the Social Security Institute for the Mexican Armed Forces (ISSFAM) and the Marine Secretariat (SEMAR). The population outside the social security is covered by the Social Protection for Health System (SPSS) (7), through the Popular Health Insurance, which is provided by the Federal Ministry of Health and States Health Services (SESA). On the other hand, the private sector offers health care to very diverse populations (from people lacking employment in the formal sector to the wealthiest populations). All of them buy a range of health care services of varying cost and quality from private medical offices, clinics, hospitals and insurance companies (5, 8).
1 To facilitate identification, all initials of Mexican institutions are provided as they are originally written in Spanish.
6 PRIMARY HEALTH CARE SYSTEMS (PRIMASYS)
In 2013, the total number of primary health facilities reached 28 366 – 98% (27739) in the public sector and only 2% (627) in the private sector. In the same year 4 456 hospitals were counted, of which 69% (3070) were in the private sector. From 27 739
health care facilities, 75% (20803) were considered as primary care facilities. The number of facilities decreased in 2014 and 2015. In 2015 there were 22 598 health facilities, with 93% (21 025) of them classified as primary health facilities (Table 2).
Table 2. Number of primary health facilities and hospitals in Mexico, 2013–2015
2013 2014 2015
N % N % N %
Primary health facilities 20 803 75% 20 651 93% 21 025 93%
Hospitals and clinical laboratories
1 180 4% 403 5% 421 5%
Other 5 756 21% 1 132 2% 1 152 2%
Total 27 739 100 22 186 100 22 598 100
Source: Based on data of the General Directorate of Health Information (DGIS), Ministry of Health, 2016.
Figure 1. Structure of the Mexican health system
Source: Updated from Gómez-Dantés et al. (5).
Public PrivateSECTORSocial security National Ministry of Health States Health Services (SHS)
Government contribution
FUNDS
BUYERS
Federal Govt
contributionIndividualsEmployers’
contributionStates Govt
contribution EmployersWorkers’ contribution
Popular health
insurancePrivate
insurance companies
IMSS National MoH SHS
PROSPERA Social inclusion
programme
Hospitals, clinics, doctors and
nurses of these institutions
Private providers
Hospitals, clinics, doctors and
nurses of these institutions
PEMEX Army / Navy
PROVIDERS
USERS
Hospitals, clinics, doctors and nurses of these institutions
Workers in the formal
sector
Workers’ families Retirees
Self-employed & informal sector workers and
unemployed
Population with paying capacity
ISSSTE
7CASE STUDY FROM MEXICO
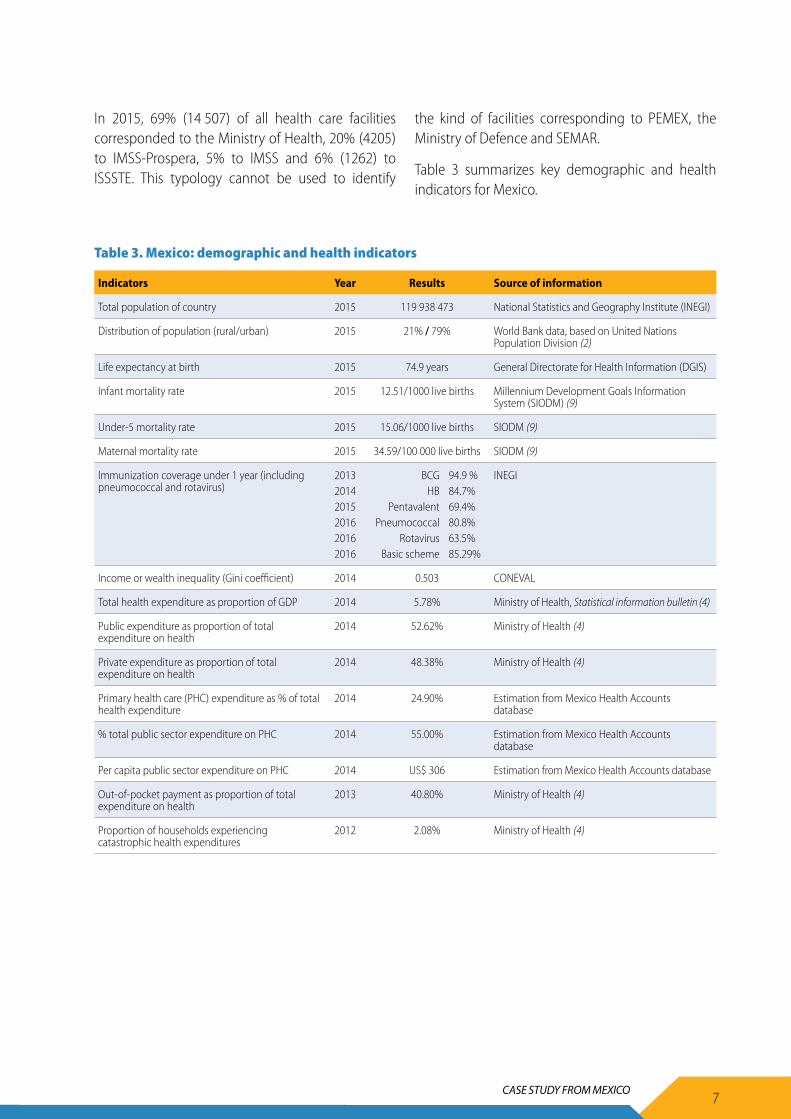
In 2015, 69% (14 507) of all health care facilities corresponded to the Ministry of Health, 20% (4205) to IMSS-Prospera, 5% to IMSS and 6% (1262) to ISSSTE. This typology cannot be used to identify
the kind of facilities corresponding to PEMEX, the Ministry of Defence and SEMAR.
Table 3 summarizes key demographic and health indicators for Mexico.
Table 3. Mexico: demographic and health indicators
Indicators Year Results Source of information
Total population of country 2015 119 938 473 National Statistics and Geography Institute (INEGI)
Distribution of population (rural/urban) 2015 21% / 79% World Bank data, based on United Nations Population Division (2)
Life expectancy at birth 2015 74.9 years General Directorate for Health Information (DGIS)
Infant mortality rate 2015 12.51/1000 live births Millennium Development Goals Information System (SIODM) (9)
Under-5 mortality rate 2015 15.06/1000 live births SIODM (9)
Maternal mortality rate 2015 34.59/100 000 live births SIODM (9)
Immunization coverage under 1 year (including pneumococcal and rotavirus)
201320142015201620162016
BCGHB
PentavalentPneumococcal
RotavirusBasic scheme
94.9 %84.7% 69.4% 80.8% 63.5% 85.29%
INEGI
Income or wealth inequality (Gini coefficient) 2014 0.503 CONEVAL
Total health expenditure as proportion of GDP 2014 5.78% Ministry of Health, Statistical information bulletin (4)
Public expenditure as proportion of total expenditure on health
2014 52.62% Ministry of Health (4)
Private expenditure as proportion of total expenditure on health
2014 48.38% Ministry of Health (4)
Primary health care (PHC) expenditure as % of total health expenditure
2014 24.90% Estimation from Mexico Health Accounts database
% total public sector expenditure on PHC 2014 55.00% Estimation from Mexico Health Accounts database
Per capita public sector expenditure on PHC 2014 US$ 306 Estimation from Mexico Health Accounts database
Out-of-pocket payment as proportion of total expenditure on health
2013 40.80% Ministry of Health (4)
Proportion of households experiencing catastrophic health expenditures
2012 2.08% Ministry of Health (4)

8 PRIMARY HEALTH CARE SYSTEMS (PRIMASYS)
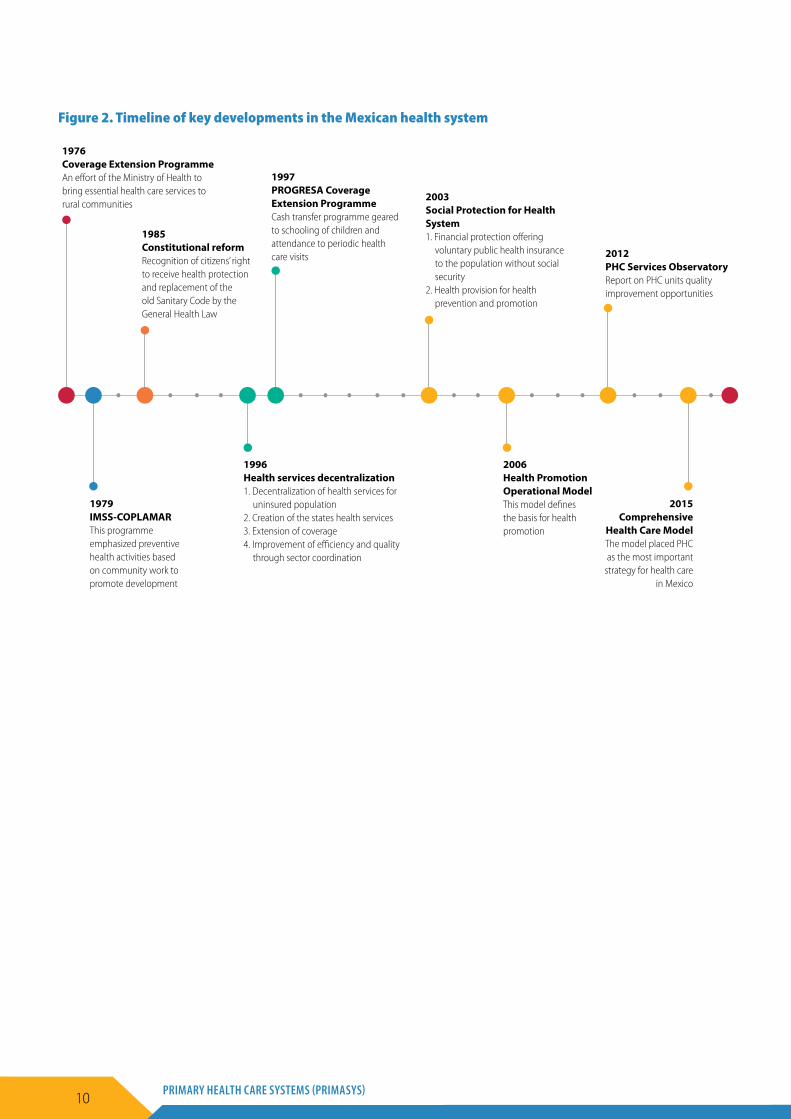
4. Timeline of key developments in Mexican health system
Coverage Extension Programme. Launched in 1976 by the Ministry of Health, the Coverage Extension Programme aimed to extend coverage of essential health care services to rural communities with geographical access difficulties. It encompassed establishment of itinerant medical teams and construction of primary care facilities and rural hospitals in the jurisdictions (10, 11). The programme also included actions to strengthen community participation, preventive medicine, health promotion and environmental care. Physicians, nurses, basic sanitary technicians, empirical midwives and health promoters received training. In 1978, the programme was complemented by the Rural Community Programme, focused on difficult-to-reach localities with less than 2500 inhabitants. Emphasis was placed on family planning, prenatal care, and care for children aged under 5 years. Both programmes were merged in 1981 to form the Rural Health Programme, which in 1985 became the Rural Zones Coverage Extension Strategy functioning for the whole country (12).
IMSS-COPLAMAR. Created in 1979, this programme was funded by the federal government and managed by IMSS. Its objective was to develop a comprehensive care model based on the recommendations of the Alma-Ata Declaration on Primary Health Care (1978). It was implemented in clinics and hospitals of difficult access, mainly in indigenous zones, and included traditional medicine. The programme was implemented in 3024 health facilities in 1981 and offered health care to 14 million people. It developed actions to strengthen community committees and health promoters and incorporated recently licensed doctors or those working in the social services, as well as nursing auxiliaries. In 1985, the programme consolidated its health promotion activities in such a way that it highly contributed to the decrease in the incidence of communicable diseases (13, 14).
Constitutional reform. The General Health Law regulates the right to health protection of
all Mexicans. Article 27 defines the basic health services as (a) education for health and basic sanitation promotion; (b) prevention and control of communicable and noncommunicable diseases; and (c) comprehensive care, including preventive, curative, palliative and rehabilitation activities. It also stipulates that health promotion is part of medical care, and should be provided according to the age, sex, physical and psychological determinants of each person. Article 28 refers to access to a basic package of supplies in primary care facilities of the institutions of the National Health System. Article 51 asserts the right of users to freely and voluntarily choose the doctor in the primary health care facility where they are registered. Finally, Articles 110 and 112 define the health promotion and education actions.
Health services decentralization. In 1983, the decentralization of health services started in 14 states (15, 16). Health services for the uninsured population became a responsibility of the state governments. The states decided to implement a primary care model emphasizing immunization, oral rehydration, access to drinking water and education of women in reproductive and sexual health (17). In 1989 sanitary jurisdictions were created to strengthen decentralization of resources and decision-making at the local level (18). In 1993, all states, including the Federal District, participated in the decentralization process. Functions were normalized and resources were increased for the newly created States Health Services (Servicios Estatales de Salud, SESA). In order to continue increasing the access of the uninsured population to basic health care services, the Coverage Extension Programme was updated in 1995, to be implemented by each SESA. Finally, in 1996, the National Agreement for the Decentralization of Health Services was signed confirming the states’ responsibility for health care services and preventive medicine provision to all the insured population (15, 17, 19).

9CASE STUDY FROM MEXICO
Education, Health and Nutrition Conditional Cash Transfer Programme (Programa de Educación, Salud y Alimentación, PROGRESA). This was implemented in 1997 as a part of the social policy aiming to provide health care to families living in extreme poverty in rural zones. The programme integrated health, nutrition and education components and was based on conditional cash transfers to families (20). Health care was developed using mobile facilities in which a doctor, a nurse and a health promoter participated, offering (a) a basic package of health care services including 14 interventions; (b) prevention and care of malnutrition in children aged under 4 years and pregnant or breastfeeding women; and (c) an educational programme including 25 sessions. In 2000, the programme reached around 2 million families and was transformed into the Oportunidades Human Development Programme. It is presently called Prospera and reaches around 6.1 million families in rural, urban and semi-urban areas (10, 21, 22).
Social Protection for Health System (SPSS). The last major reform was the incorporation of the SPSS into the General Health Law in 2003. This reform aimed to offer health protection for the population that had no social security coverage, mainly the poorest. It offers a basic services package defined in the Universal Health Services Catalogue (CAUSES), which includes preventive health and health promotion activities as well as diagnosis, treatment and rehabilitation according to the country’s epidemiological profile (23). CAUSES started offering coverage for 91 interventions in 2004 and already covered 283 interventions in 2012. This practically covers 95% of the outpatient and general hospital care of the Ministry of Health. The system had affiliated around 50 million Mexicans by 2014. CAUSES continues to grow and now includes some high-cost treatments in an effort to attain universal health coverage (24–26).
Health Promotion Operational Model (MOPS). This was developed in 2006 by the General Directorate for Health Promotion of the Ministry of Health in response to the need to strengthen health promotion
in the country (27). The model included four major components: (a) personal risks management and identification of health determinants; (b) development of health competencies through individual counselling and community workshops; (c) social participation and fostering creation of social networks aiming to empower communities; and (d) development of healthy environments, which includes natural resources protection (27, 28).
Primary Health Care Services Observatory. In 2012, the General Directorate for Performance Evaluation of the Ministry of Health published an important report on the current situation and improvement opportunities for all health care facilities of the Ministry of Health related to PHC. The report was launched in an effort to emphasize the importance of strengthening the primary health facilities as an efficient strategy to respond to the needs and expectations of the population. It provides information on the conditions and availability of PHC facilities, and their equipment and human resources (29).
Comprehensive Health Care Model (MAI). This model was developed in 2015 by the General Directorate for Health Planning and Development of the Ministry of Health. Its aim is to contribute to the standardization of services and practices in the health sector and to optimize resources and health infrastructure utilization. At the same time it aims to encourage the mechanisms and processes of democratic participation of citizens in order to achieve effective and universal access to health protection. In relation to PHC, the model proposes to (a) renovate and strengthen the PHC strategy; (b) establish, reorganize and articulate the integrated health services networks; (c) reorganize, reorient and strengthen the sanitary jurisdictions; and (d) promote participation of citizens as the main agent for cultural change. The model emphasizes PHC as the main entry point to the health system and the first reference for health promotion and disease prevention. It also stresses that outpatient care is the domain in which most of the care needs should be resolved.
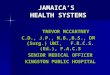
Figure 2 presents a timeline of key developments in the Mexican health system.
10 PRIMARY HEALTH CARE SYSTEMS (PRIMASYS)
Figure 2. Timeline of key developments in the Mexican health system
1979 IMSS-COPLAMAR This programme emphasized preventive health activities based on community work to promote development
1976 Coverage Extension Programme An effort of the Ministry of Health to bring essential health care services to rural communities
1996 Health services decentralization 1. Decentralization of health services for uninsured population 2. Creation of the states health services 3. Extension of coverage 4. Improvement of efficiency and quality through sector coordination
2003 Social Protection for Health System1. Financial protection offering voluntary public health insurance to the population without social security 2. Health provision for health prevention and promotion
1997 PROGRESA Coverage Extension Programme Cash transfer programme geared to schooling of children and attendance to periodic health care visits
2006 Health Promotion Operational Model This model defines the basis for health promotion
2015 Comprehensive
Health Care ModelThe model placed PHC as the most important
strategy for health care in Mexico
2012 PHC Services ObservatoryReport on PHC units quality improvement opportunities
1985 Constitutional reform Recognition of citizens’ right to receive health protection and replacement of the old Sanitary Code by the General Health Law
11CASE STUDY FROM MEXICO
5. Governance
Governance has been defined as “the culture and institutional environment in which citizens and stakeholders interact among themselves and participate in public affairs” (30). It addresses the ways in which a society, including its government and decision-makers, the private sector and civil society, interact and are organized to provide health care to their populations (31).
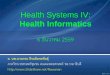
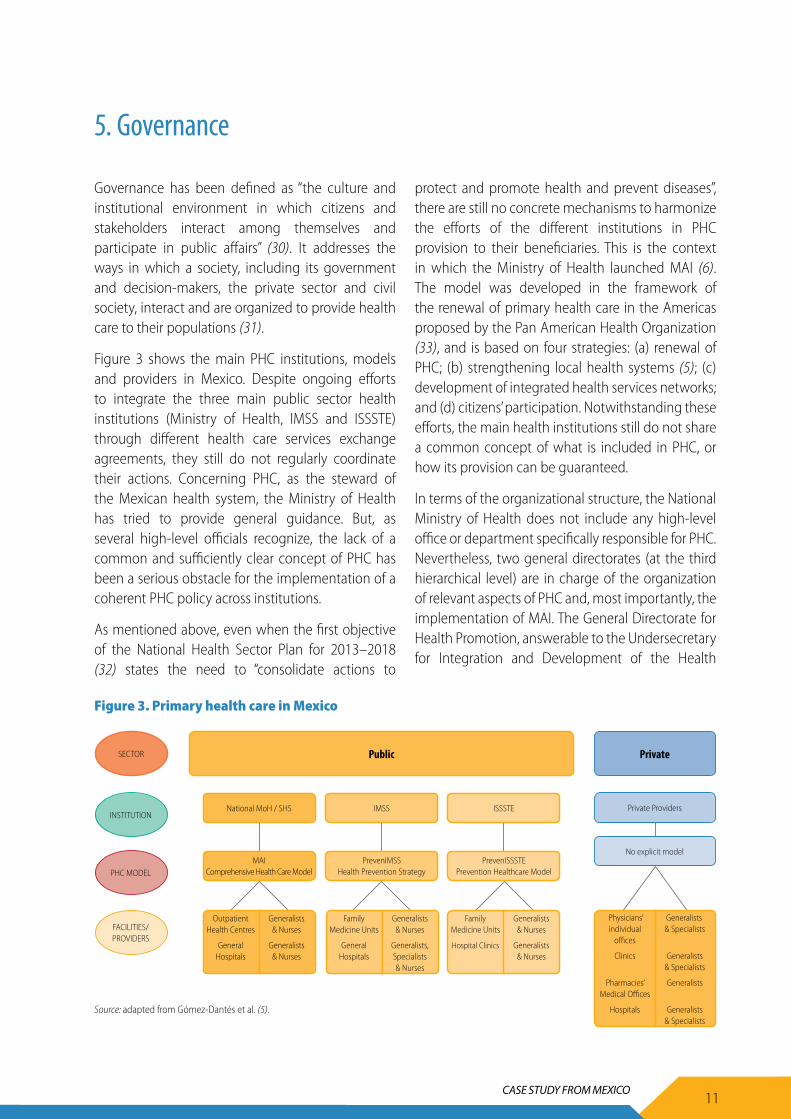
Figure 3 shows the main PHC institutions, models and providers in Mexico. Despite ongoing efforts to integrate the three main public sector health institutions (Ministry of Health, IMSS and ISSSTE) through different health care services exchange agreements, they still do not regularly coordinate their actions. Concerning PHC, as the steward of the Mexican health system, the Ministry of Health has tried to provide general guidance. But, as several high-level officials recognize, the lack of a common and sufficiently clear concept of PHC has been a serious obstacle for the implementation of a coherent PHC policy across institutions.
As mentioned above, even when the first objective of the National Health Sector Plan for 2013–2018 (32) states the need to “consolidate actions to
protect and promote health and prevent diseases”, there are still no concrete mechanisms to harmonize the efforts of the different institutions in PHC provision to their beneficiaries. This is the context in which the Ministry of Health launched MAI (6). The model was developed in the framework of the renewal of primary health care in the Americas proposed by the Pan American Health Organization (33), and is based on four strategies: (a) renewal of PHC; (b) strengthening local health systems (5); (c) development of integrated health services networks; and (d) citizens’ participation. Notwithstanding these efforts, the main health institutions still do not share a common concept of what is included in PHC, or how its provision can be guaranteed.
In terms of the organizational structure, the National Ministry of Health does not include any high-level office or department specifically responsible for PHC. Nevertheless, two general directorates (at the third hierarchical level) are in charge of the organization of relevant aspects of PHC and, most importantly, the implementation of MAI. The General Directorate for Health Promotion, answerable to the Undersecretary for Integration and Development of the Health
Public
National MoH / SHS
MAI Comprehensive Health Care Model
IMSS
PrevenIMSS Health Prevention Strategy
ISSSTE
PrevenISSSTE Prevention Healthcare Model
Private Providers
No explicit model
PrivateSECTOR
INSTITUTION
PHC MODEL
FACILITIES/ PROVIDERS
Physicians’ individual
offices
Clinics
Pharmacies’
Medical Offices
Hospitals
Outpatient Health Centres
General Hospitals
Generalists & Nurses
Generalists & Nurses
Family Medicine Units
General Hospitals
Generalists & Nurses
Generalists, Specialists & Nurses
Family Medicine Units
Hospital Clinics
Generalists & Nurses
Generalists & Nurses
Generalists & Specialists
Generalists & Specialists
Generalists
Generalists
& Specialists
Figure 3. Primary health care in Mexico
Source: adapted from Gómez-Dantés et al. (5).
12 PRIMARY HEALTH CARE SYSTEMS (PRIMASYS)
Sector, is responsible for a series of specific action programmes directly linked with PHC: health promotion, social determinants of health, healthy communities and environments, nutrition and physical activity. Likewise, the General Directorate for Health Planning and Development includes structures that are responsible for ambulatory health care and extending coverage, planning health services networks, planning services exchange and even the inclusion of traditional medicine.
As an expression of the federal character of the country, the autonomy of each SESA creates a wide range of modalities for PHC provision adapted to each state. As in the Federal Ministry of Health, each SESA includes several entities with PHC responsibilities. However, except in the SESA in the states of Puebla and Michoacán, they seldom include offices with explicit links to PHC. The only similar entities in the rest of the states are subdirectorates for health promotion and disease prevention (Quintana Roo), prevention and promotion departments (Hidalgo), and first-level services and health promotion
regulation departments (Morelos). Generally speaking, these structures of the different states’ public health services do not necessarily include all the strategic elements or the activities of MAI.
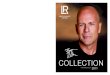
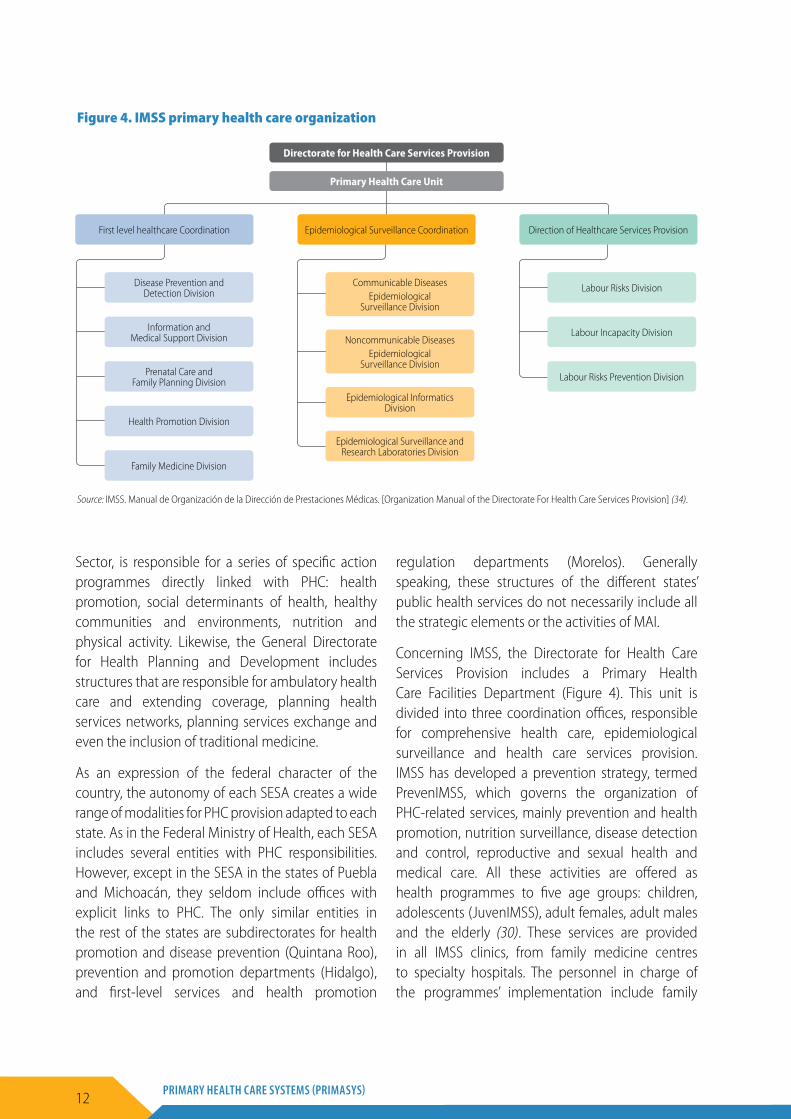
Concerning IMSS, the Directorate for Health Care Services Provision includes a Primary Health Care Facilities Department (Figure 4). This unit is divided into three coordination offices, responsible for comprehensive health care, epidemiological surveillance and health care services provision. IMSS has developed a prevention strategy, termed PrevenIMSS, which governs the organization of PHC-related services, mainly prevention and health promotion, nutrition surveillance, disease detection and control, reproductive and sexual health and medical care. All these activities are offered as health programmes to five age groups: children, adolescents (JuvenIMSS), adult females, adult males and the elderly (30). These services are provided in all IMSS clinics, from family medicine centres to specialty hospitals. The personnel in charge of the programmes’ implementation include family
Directorate for Health Care Services Provision
Primary Health Care Unit
First level healthcare Coordination
Disease Prevention and Detection Division
Communicable Diseases Epidemiological
Surveillance Division
Noncommunicable Diseases Epidemiological
Surveillance Division
Labour Risks Division
Prenatal Care and Family Planning Division
Epidemiological Informatics Division
Epidemiological Surveillance and Research Laboratories Division
Labour Risks Prevention Division
Family Medicine Division
Information and Medical Support Division Labour Incapacity Division
Health Promotion Division
Direction of Healthcare Services ProvisionEpidemiological Surveillance Coordination
Figure 4. IMSS primary health care organization
Source: IMSS. Manual de Organización de la Dirección de Prestaciones Médicas. [Organization Manual of the Directorate For Health Care Services Provision] (34).

13CASE STUDY FROM MEXICO
medicine physicians and nurses, but specialists are also trained into them.
ISSSTE also lacks an explicitly PHC-linked office. Nevertheless, the Subdirectorate for Health Promotion and Disease Prevention, which is part of the Medical Directorate, does have an Office of Family Medical Care Services. This office is responsible for the first-level health facilities network. Besides, another office is responsible for the prevention of chronic degenerative diseases and another department is in charge of the regional and local health systems. ISSSTE has also developed a preventive health care model – PrevenISSSTE – whose main objective is “to provide comprehensive health care and to promote the social, biological and psychological development of beneficiaries … with special emphasis on health promotion and diseases prevention activities” (5). The model is a responsibility of the Subdirectorate for Health Promotion and Disease Prevention and is offered in all family medicine clinics and hospitals. A scale-up of PrevenISSSTE was launched in 2010, based on an online platform where beneficiaries can obtain information on risk factors associated with chronic diseases and recommendations on how to deal with them. A telephone hotline is also available as a support programme within the platform.
The fourth public institution is the PEMEX Health Services. Its PHC-related structure includes the Administration for Preventive Medicine, which embraces the Unit for Preventive Health and Preventive Medicine. Within the latter, the Department for Primary Prevention and Community Action and the Department for Secondary Prevention and Assistance are mandated to perform PHC-related activities.
Finally, the public health sector includes the health care services provided to the personnel in the army and the navy, together with their families. Though each of these institutions includes particular organisms in charge of health care in general, the available information on their structure is not enough to identify departments linked to PHC. Nevertheless, the organization manual of the army’s health services
or ISSFAM does mention an agreement related to the subrogation of medical care services to be provided by ISSSTE (32, 35). In the case of the navy, the General Directorate for Naval Health comes under the General Directorate for Human Resources. In this instance, in the classification of the units and facilities for naval health for 2012, a basic notion of PHC can be discerned in the way the responsibilities for what is termed the first level of care are described: “aspects of health promotion and protection, outpatient early diagnosis and timely treatment … [and] referral actions towards other levels of care” (36).
On the other hand, even if there is no structured policy, organizational measures or complete information on the role of the private sector in relation to PHC, this sector certainly plays a relevant role in offering first-contact health care to the population, even to those who benefit from other forms of health coverage. Between 2000 and 2012, around 40% of out-of-pocket spending was dedicated to consultation with private providers, and the proportion of private consultations in the total of outpatient consultations increased from 31% to 38.9% (37). These figures are illustrative of the relevance of the private sector in providing PHC.
Striving to fight self-medication, in 2010 the national health authorities restricted the sale of antibiotics only to patients who presented a medical prescription. As a result, between 2010 and 2014 the number of doctors’ offices adjacent to private pharmacies increased by over 240% (38, 39). In an effort to regulate this phenomenon, at the end of 2013, the Federal Commission for Protection against Sanitary Risks (COFEPRIS) of the Ministry of Health launched the Strategy for Strengthening Regulation of Pharmacies and Medical Offices. According to a 2015 report by COFEPRIS, there was an improvement in compliance with the good practice guidelines, attaining an overall percentage of 75%, with 80.27% compliance with the guidelines on doctors’ offices pertaining to pharmacy chains. As part of the effort, these doctors’ offices are also being included in the National Catalogue of Health Facilities (CLUES), which will ensure improved surveillance (38).

14 PRIMARY HEALTH CARE SYSTEMS (PRIMASYS)
While there is an effort to foster health promotion and preventive activities in these facilities, this regulation does not stipulate what health care services may or may not be provided. Some consider that the intrinsic commercial interests of pharmacies imply a lack of interest in preventive measures and follow-up of patients, which is contrary to good-quality PHC. Further strengthening of regulations and incorporation of the use of electronic clinical files and other mechanisms that would guarantee correct follow-up with patients have thus been proposed.
Mexico has over 4500 civil society organizations involved in health promotion, sanitary and health care activities.2 Even though they are not all in line with a clear PHC vision, and do not necessarily foster activities related to health promotion, 59% of them include social assistance among their main activities. These organizations are mostly dedicated to some sort of health care services provision or health promotion, prevention and education activities. Many of them are focused on treating addiction, chronic diseases, and mental health issues, and offer family-targeted services.
2 Information system of the federal register of civil society organizations.
15CASE STUDY FROM MEXICO
6. Financing
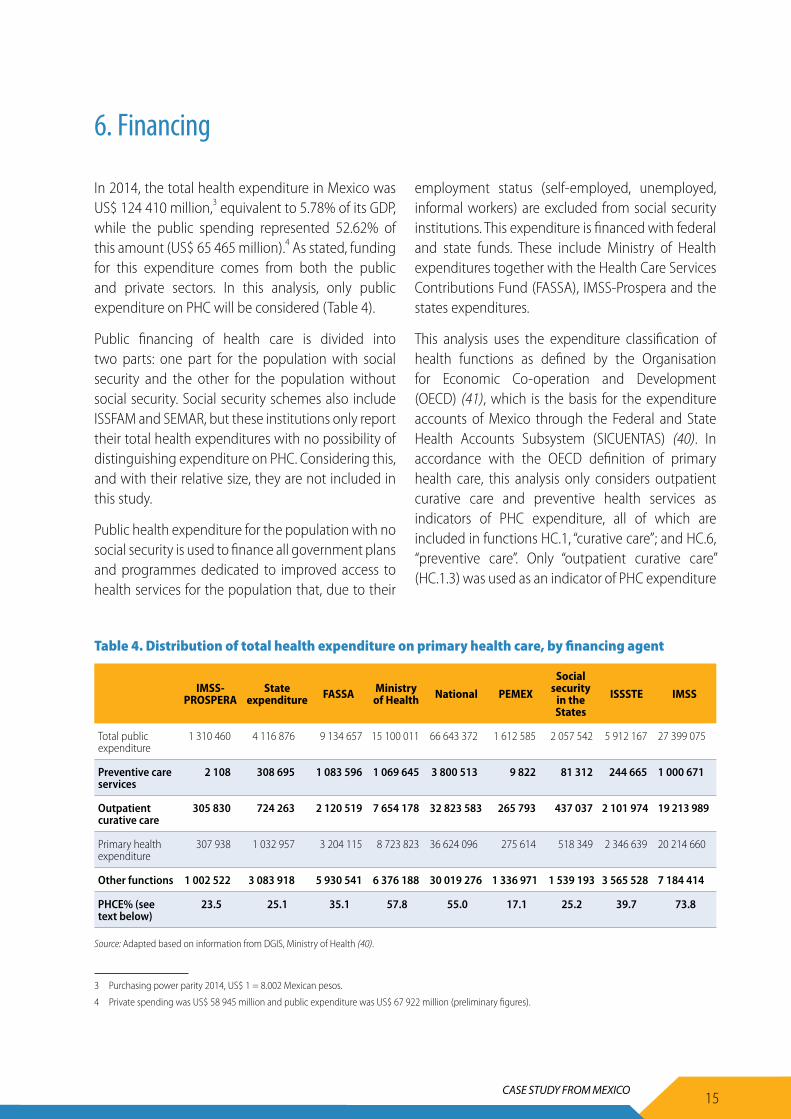
In 2014, the total health expenditure in Mexico was US$ 124 410 million,3 equivalent to 5.78% of its GDP, while the public spending represented 52.62% of this amount (US$ 65 465 million).4 As stated, funding for this expenditure comes from both the public and private sectors. In this analysis, only public expenditure on PHC will be considered (Table 4).
Public financing of health care is divided into two parts: one part for the population with social security and the other for the population without social security. Social security schemes also include ISSFAM and SEMAR, but these institutions only report their total health expenditures with no possibility of distinguishing expenditure on PHC. Considering this, and with their relative size, they are not included in this study.
Public health expenditure for the population with no social security is used to finance all government plans and programmes dedicated to improved access to health services for the population that, due to their
employment status (self-employed, unemployed, informal workers) are excluded from social security institutions. This expenditure is financed with federal and state funds. These include Ministry of Health expenditures together with the Health Care Services Contributions Fund (FASSA), IMSS-Prospera and the states expenditures.
This analysis uses the expenditure classification of health functions as defined by the Organisation for Economic Co-operation and Development (OECD) (41), which is the basis for the expenditure accounts of Mexico through the Federal and State Health Accounts Subsystem (SICUENTAS) (40). In accordance with the OECD definition of primary health care, this analysis only considers outpatient curative care and preventive health services as indicators of PHC expenditure, all of which are included in functions HC.1, “curative care”; and HC.6, “preventive care”. Only “outpatient curative care” (HC.1.3) was used as an indicator of PHC expenditure
Table 4. Distribution of total health expenditure on primary health care, by financing agent
IMSS-PROSPERA
State expenditure FASSA Ministry
of Health National PEMEX
Social security
in the States
ISSSTE IMSS
Total public expenditure
1 310 460 4 116 876 9 134 657 15 100 011 66 643 372 1 612 585 2 057 542 5 912 167 27 399 075
Preventive care services
2 108 308 695 1 083 596 1 069 645 3 800 513 9 822 81 312 244 665 1 000 671
Outpatient curative care
305 830 724 263 2 120 519 7 654 178 32 823 583 265 793 437 037 2 101 974 19 213 989
Primary health expenditure
307 938 1 032 957 3 204 115 8 723 823 36 624 096 275 614 518 349 2 346 639 20 214 660
Other functions 1 002 522 3 083 918 5 930 541 6 376 188 30 019 276 1 336 971 1 539 193 3 565 528 7 184 414
PHCE% (see text below)
23.5 25.1 35.1 57.8 55.0 17.1 25.2 39.7 73.8
Source: Adapted based on information from DGIS, Ministry of Health (40).
3 Purchasing power parity 2014, US$ 1 = 8.002 Mexican pesos.
4 Private spending was US$ 58 945 million and public expenditure was US$ 67 922 million (preliminary figures).
16 PRIMARY HEALTH CARE SYSTEMS (PRIMASYS)
(Figure 5). So PHC expenditure as a percentage of total health expenditure (PHCE%) and per capita PHC expenditure are determined by the following formulas:
outpatient curative care expenditure (HC.1.3) + preventive care expenditure (HC.6)
total health expenditure (H)
PHCE% =
outpatient curative care expenditure (HC.1.3) + preventive care expenditure (HC.6)
total population
Per capita PHCE =
The year of analysis is 2014. All monetary figures are in US dollars and the conversion from Mexican pesos
was made using the purchasing power parity (PPP) for 2014, which was 8.002 pesos per US dollar (42, 43).
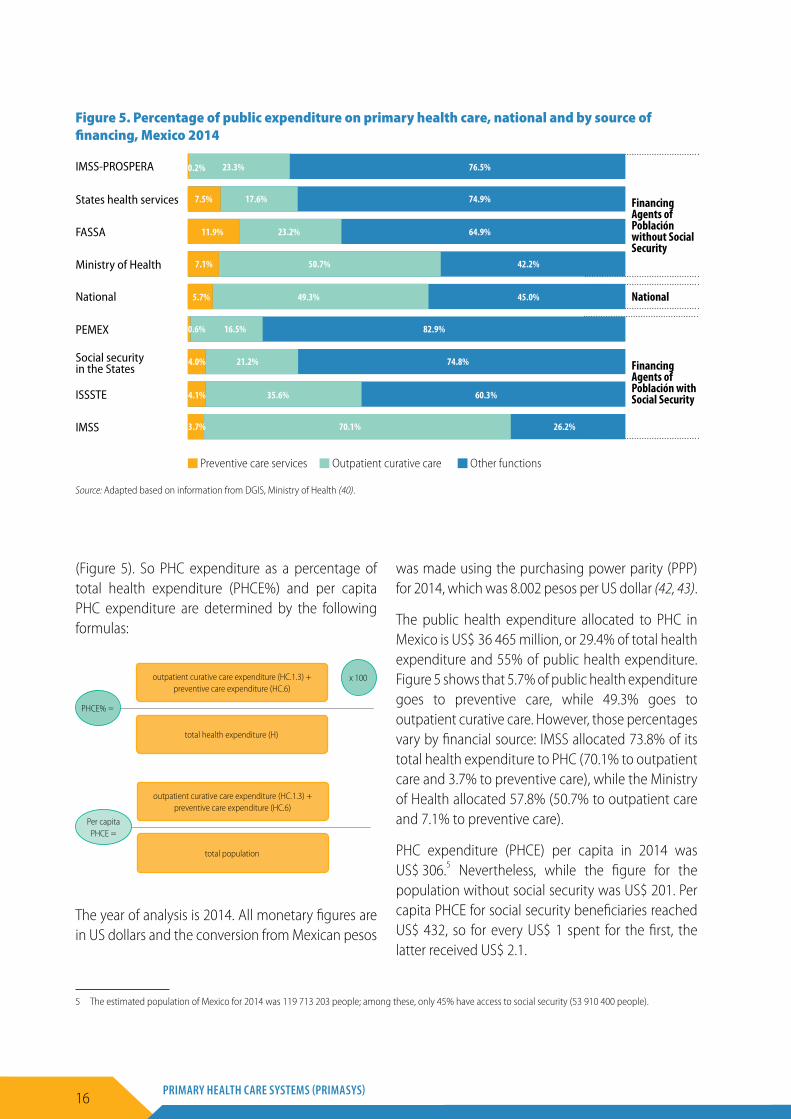
The public health expenditure allocated to PHC in Mexico is US$ 36 465 million, or 29.4% of total health expenditure and 55% of public health expenditure. Figure 5 shows that 5.7% of public health expenditure goes to preventive care, while 49.3% goes to outpatient curative care. However, those percentages vary by financial source: IMSS allocated 73.8% of its total health expenditure to PHC (70.1% to outpatient care and 3.7% to preventive care), while the Ministry of Health allocated 57.8% (50.7% to outpatient care and 7.1% to preventive care).
PHC expenditure (PHCE) per capita in 2014 was US$ 306.5 Nevertheless, while the figure for the population without social security was US$ 201. Per capita PHCE for social security beneficiaries reached US$ 432, so for every US$ 1 spent for the first, the latter received US$ 2.1.
Figure 5. Percentage of public expenditure on primary health care, national and by source of financing, Mexico 2014
Source: Adapted based on information from DGIS, Ministry of Health (40).
IMSS-PROSPERA
States health services
FASSA
Ministry of Health
National
PEMEX
Social security in the States
ISSSTE
IMSS
Financing Agents of Población without Social Security
Financing Agents of Población with Social Security
National
23.3% 76.5%
74.9%
64.9%
42.2%
45.0%
82.9%
74.8%
60.3%
26.2%
7.5%
11.9%
7.1%
5.7%
0.6%
0.2%
4.0%
4.1%
3.7% 70.1%
35.6%
21.2%
16.5%
49.3%
50.7%
23.2%
17.6%
Preventive care services Outpatient curative care Other functions
x 100
5 The estimated population of Mexico for 2014 was 119 713 203 people; among these, only 45% have access to social security (53 910 400 people).
17CASE STUDY FROM MEXICO
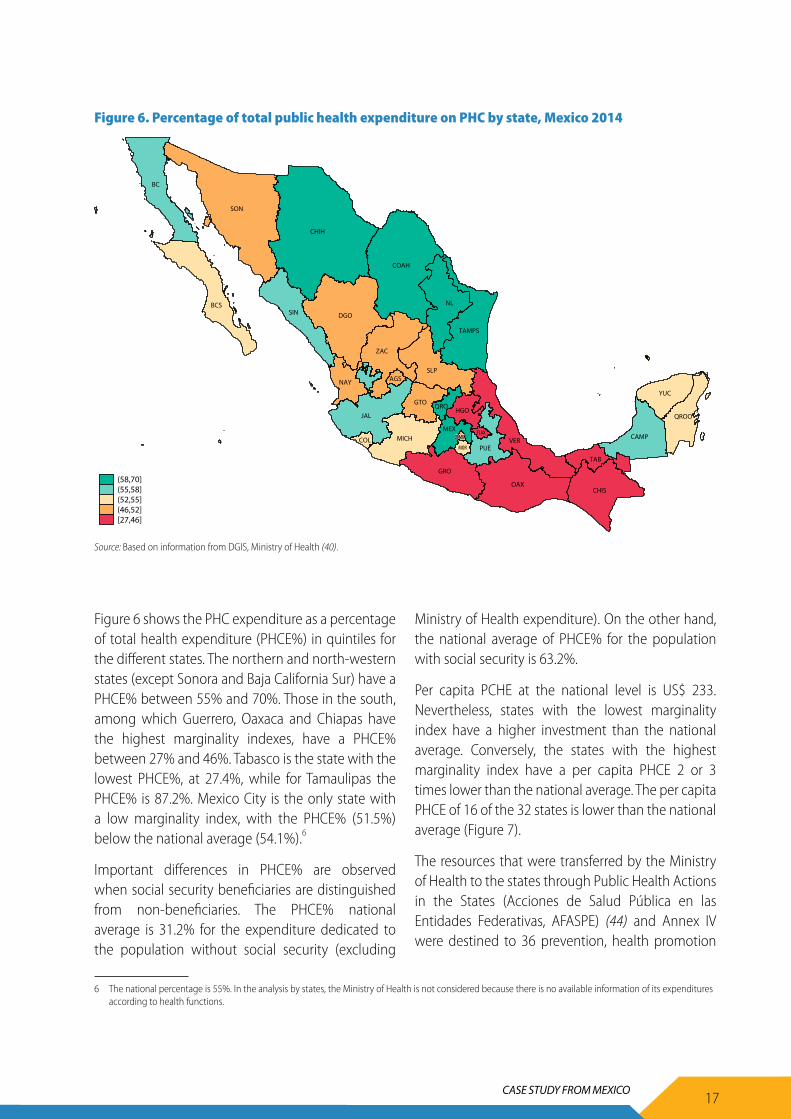
Figure 6 shows the PHC expenditure as a percentage of total health expenditure (PHCE%) in quintiles for the different states. The northern and north-western states (except Sonora and Baja California Sur) have a PHCE% between 55% and 70%. Those in the south, among which Guerrero, Oaxaca and Chiapas have the highest marginality indexes, have a PHCE% between 27% and 46%. Tabasco is the state with the lowest PHCE%, at 27.4%, while for Tamaulipas the PHCE% is 87.2%. Mexico City is the only state with a low marginality index, with the PHCE% (51.5%) below the national average (54.1%).6
Important differences in PHCE% are observed when social security beneficiaries are distinguished from non-beneficiaries. The PHCE% national average is 31.2% for the expenditure dedicated to the population without social security (excluding
Ministry of Health expenditure). On the other hand, the national average of PHCE% for the population with social security is 63.2%.
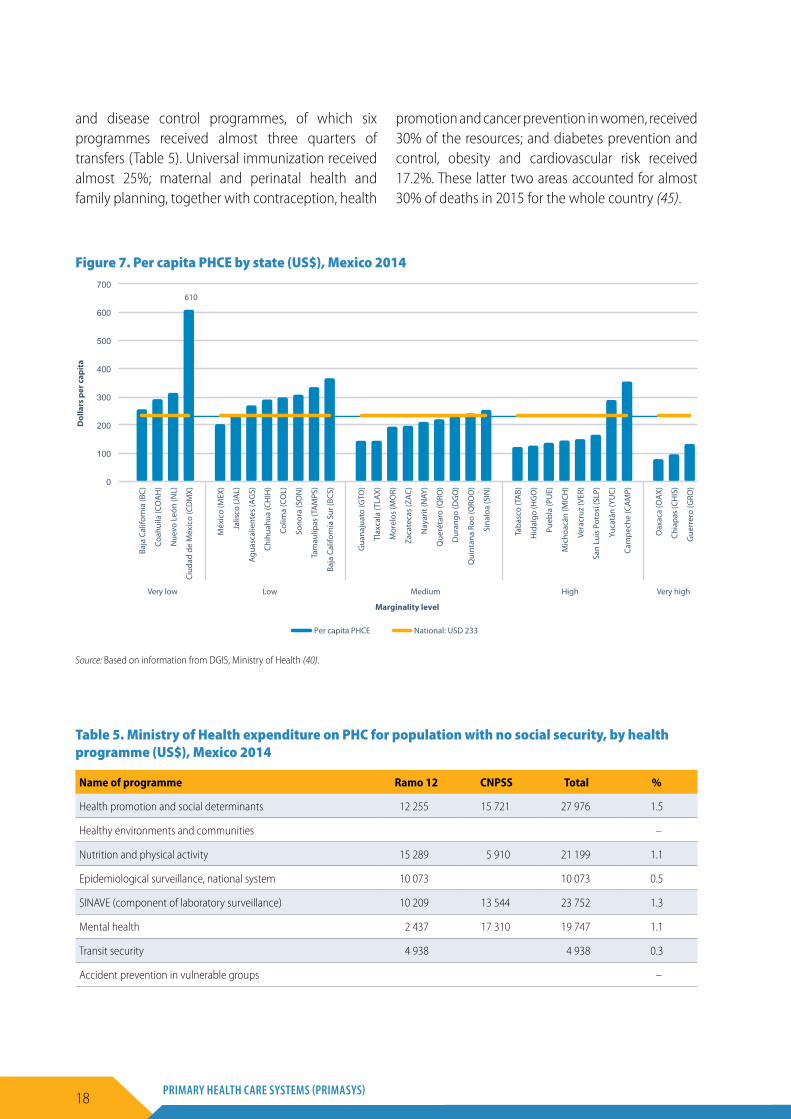
Per capita PCHE at the national level is US$ 233. Nevertheless, states with the lowest marginality index have a higher investment than the national average. Conversely, the states with the highest marginality index have a per capita PHCE 2 or 3 times lower than the national average. The per capita PHCE of 16 of the 32 states is lower than the national average (Figure 7).
The resources that were transferred by the Ministry of Health to the states through Public Health Actions in the States (Acciones de Salud Pública en las Entidades Federativas, AFASPE) (44) and Annex IV were destined to 36 prevention, health promotion
AGS
BC
BCS
CAMP
COAH
COL
CHIS
CHIH
DGO
GTO
GRO
HGOJAL
MEXMICH
MOR
NAY
NL
OAX
PUE
QROQROO
SLP
SIN
SON
TAB
TAMPS
TLAXVER
YUC
ZAC
(58,70](55,58](52,55](46,52][27,46]
Source: DGIS
Figure 6. Percentage of total public health expenditure on PHC by state, Mexico 2014
Source: Based on information from DGIS, Ministry of Health (40).
6 The national percentage is 55%. In the analysis by states, the Ministry of Health is not considered because there is no available information of its expenditures according to health functions.
18 PRIMARY HEALTH CARE SYSTEMS (PRIMASYS)
and disease control programmes, of which six programmes received almost three quarters of transfers (Table 5). Universal immunization received almost 25%; maternal and perinatal health and family planning, together with contraception, health
promotion and cancer prevention in women, received 30% of the resources; and diabetes prevention and control, obesity and cardiovascular risk received 17.2%. These latter two areas accounted for almost 30% of deaths in 2015 for the whole country (45).
Table 5. Ministry of Health expenditure on PHC for population with no social security, by health programme (US$), Mexico 2014
Name of programme Ramo 12 CNPSS Total %
Health promotion and social determinants 12 255 15 721 27 976 1.5
Healthy environments and communities –
Nutrition and physical activity 15 289 5 910 21 199 1.1
Epidemiological surveillance, national system 10 073 10 073 0.5
SINAVE (component of laboratory surveillance) 10 209 13 544 23 752 1.3
Mental health 2 437 17 310 19 747 1.1
Transit security 4 938 4 938 0.3
Accident prevention in vulnerable groups –
610
0
100
200
300
400
500
600
700
Baja
Cal
iforn
ia (B
C)
Coah
uila
(CO
AH
)
Nue
vo L
eón
(NL)
Ciud
ad d
e M
éxic
o (C
DM
X)
Méx
ico
(MEX
)
Jalis
co (J
AL)
Agu
asca
lient
es (A
GS)
Chih
uahu
a (C
HIH
)
Colim
a (C
OL)
Sono
ra (S
ON
)
Tam
aulip
as (T
AM
PS)
Baja
Cal
iforn
ia S
ur (B
CS)
Gua
naju
ato
(GTO
)
Tlax
cala
(TLA
X)
Mor
elos
(MO
R)
Zaca
teca
s (Z
AC)
Nay
arit
(NAY
)
Que
réta
ro (Q
RO)
Dur
ango
(DG
O)
Qui
ntan
a Ro
o (Q
ROO
)
Sina
loa
(SIN
)
Taba
sco
(TA
B)
Hid
algo
(HG
O)
Pueb
la (P
UE)
Mic
hoac
án (M
ICH
)
Vera
cruz
(VER
)
San
Luis
Pot
osí (
SLP)
Yuca
tán
(YU
C)
Cam
pech
e (C
AM
P)
Oax
aca
(OA
X)
Chia
pas
(CH
IS)
Gue
rrer
o (G
RO)
Very low Low Medium High Very high
Dol
lars
per
cap
ita
Per capita PHCE National: USD 233
Marginality level
Figure 7. Per capita PHCE by state (US$), Mexico 2014
Source: Based on information from DGIS, Ministry of Health (40).

19CASE STUDY FROM MEXICO
Name of programme Ramo 12 CNPSS Total %
Women cancer prevention and control 70 202 93 573 163 775 8.7
Maternal and perinatal health 67 877 162 160 230 037 12.2
Reproductive and sexual health for adolescents 10 908 10 978 21 885 1.2
Family planning and contraception 4 787 165 290 170 076 9.1
Family and gender violence prevention and care 17 833 12 932 30 765 1.6
Gender equality in health 606 606 0.0
Human rabies prevention and control 1 002 5 535 6 537 0.3
Brucellosis prevention and control 22 185 207 0.0
Rickettsiosis, rabies prevention and control 594 55 648 0.0
Dengue and other vectors prevention and control 40 227 28 664 68 891 3.7
Malaria prevention and control 2 740 1 638 4 378 0.2
Onchocerciasis elimination –
Chagas disease prevention and control 320 24 586 24 905 1.3
Leishmaniasis prevention and control 79 977 1 057 0.1
Scorpion sting prevention and control 130 10 896 11 025 0.6
Diabetes prevention and control 7 004 158 276 165 280 8.8
Obesity and cardiovascular risk prevention and control 18 845 138 537 157 381 8.4
Ageing health care 347 12 022 12 369 0.7
Prevention, detection and control of oral health problems 310 60 554 60 864 3.2
Tuberculosis prevention and control 1 495 25 662 27 156 1.4
Leprosy elimination 499 499 0.0
Epidemiological emergencies and disaster care 3 002 3 002 0.2
Diarrhoeal diseases, water and cholera prevention 1 250 2 359 3 609 0.2
Addiction prevention and treatment 24 740 11 960 36 700 2.0
Response to HIV/AIDS and STIs 8 381 33 123 41 504 2.2
Universal immunization 157 878 300 883 458 761 24.4
Children and adolescent health 3 792 62 110 65 902 3.5
Cancer in childhood and adolescence 1 965 1 488 3 453 0.2
Total 501 533 1 377 425 1 878 958 100
Source: AFASPE (44).

20 PRIMARY HEALTH CARE SYSTEMS (PRIMASYS)
7. Human resources for health
The total number of health workers grew from 800 417 in 2013 to 895 600 in 2015, a 12% increase (including private sector health personnel). Of the 2015 figure, 27% (238 949) were doctors, 35% (315 042) were nurses, 4% (39 344) were other health professionals (social workers, nutritionists and psychologists), 9% (83 818) were technicians and 24% (218 447) were laboratory, administration and other personnel. Figure 8 shows the distribution of all these categories, which are mainly located in hospitals (between 54.36 % and 71.55%). Nearly 5% of medical interns and 3% of nursing interns worked in primary health facilities. These trends continued between 2013 and 2015.
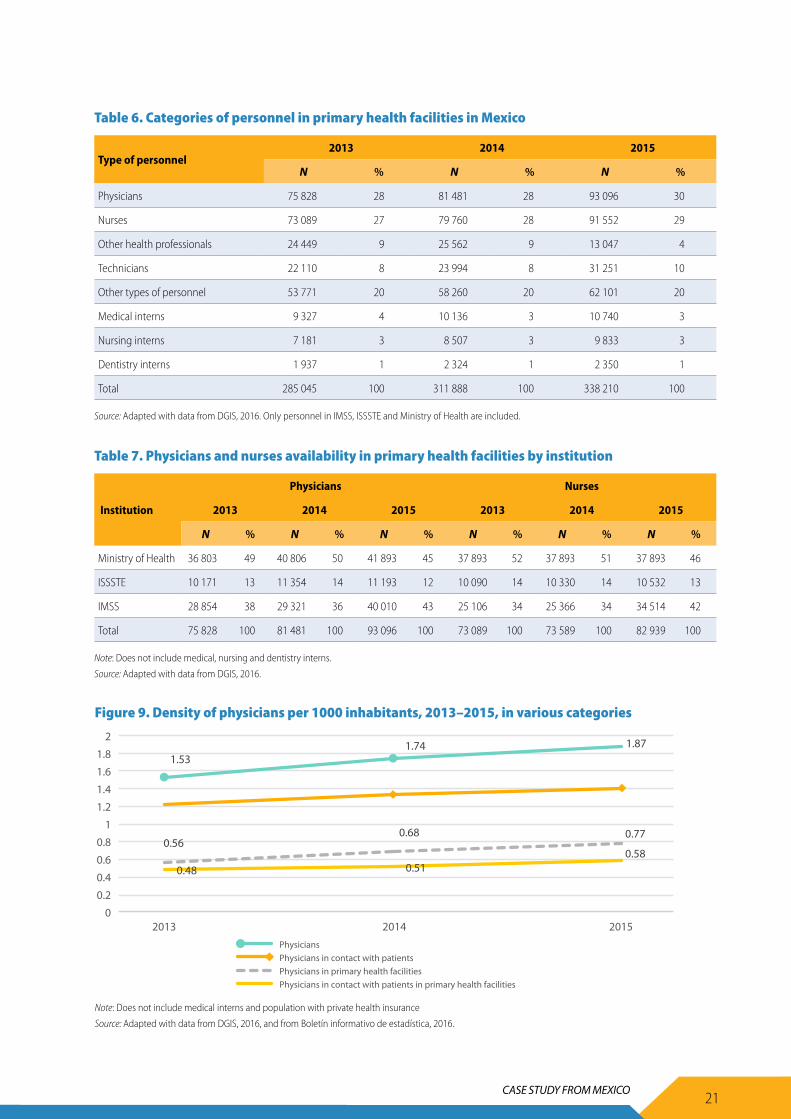
Around a third of the human resources for health in first-level facilities between 2013 and 2015 were physicians and another third were nurses (Table 6). The proportion of other health professionals, such as dentists, nutritionists and psychologists, decreased by 5% between 2014 and 2015. The proportions of other personnel remained stable.
The distribution of medical and nursing personnel according to the institutions in which they work has
generally been stable. The Ministry of Health has the largest proportion of physicians and nurses, followed by IMSS and then ISSSTE (Table 7).
Figure 9 presents the density of physicians in the country. The total density of doctors is 1.81 per 1000 inhabitants, an increase compared to 2013. Nevertheless, this is far below OECD estimated averages of 3.2 doctors and 8.8 nurses per 1000 inhabitants (46). If when estimating the density of physicians only those who perform care activities (physicians in contact with patients) are included, this indicator is even lower. A significant proportion of physicians are dedicated to other tasks, such as administration, teaching and research. The density declines even further when considering those physicians in contact with patients at the primary health facilities.
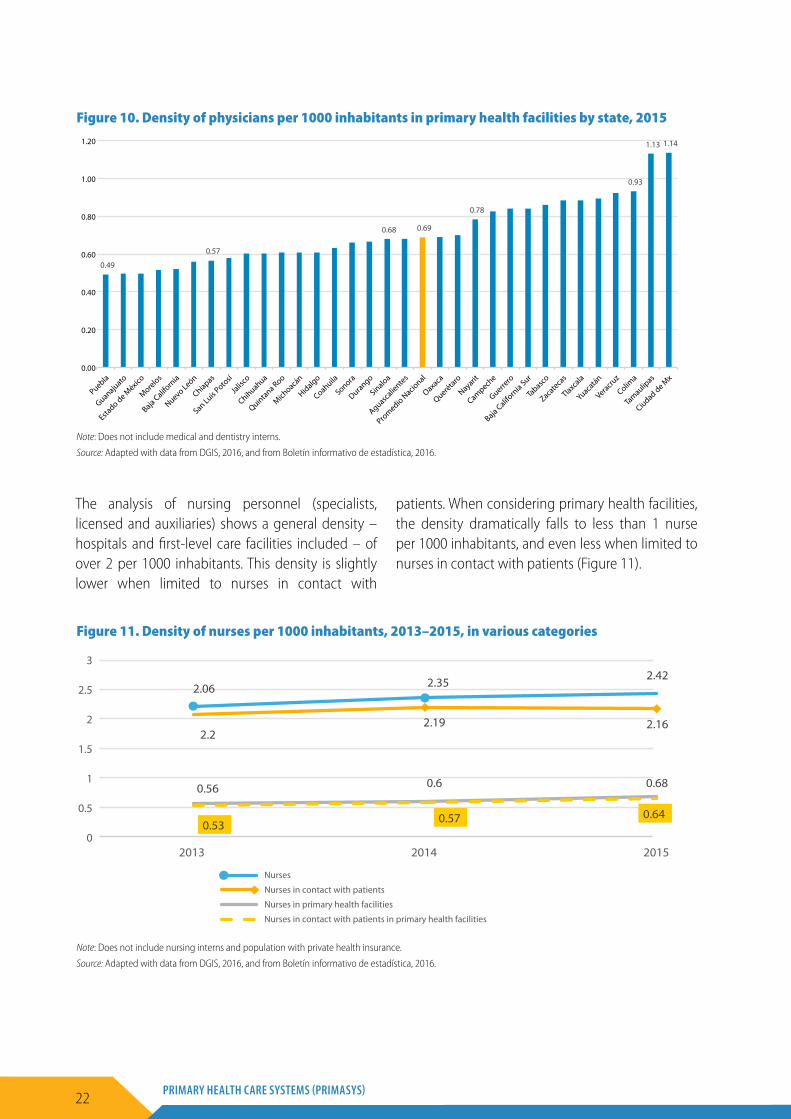
Finally, the analysis of the density of physicians in primary health facilities by state shows significant disparities and gaps for 2015. While the Ciudad de México has 1.14 doctors per 1000 inhabitants, 30 states do not even reach 1 doctor per 1000 inhabitants (Figure 10).
56.03
55.95
54.36
69.88
68.78
65.92
56.50
57.21
65.04
65.07
64.23
61.16
71.55
70.86
69.00
4.68
4.91
4.73
2.73
3.49
3.84
34.42
34.27
36.19
24.70
24.77
27.00
43.50
42.79
34.96
34.93
35.77
38.84
28.45
29.14
31.00
4.86
4.87
4.72
2.69
2.96
3.25
Physicians 2013 (N=193 026)
Physicians 2014 (N=208 201)
Physicians 2015 (N=227 567)
Nurses 2013 (N=266 859)
Nurses 2014 (N=287 603)
Nurses 2015 (N=302 719)
Other health professionals 2013 (N=56 200)
Other health professionals 2014 (N=59 740)
Other health professionals 2015 (N=37 317)
Technicians 2013 (N=63 307)
Technicians 2014 (N=67 072)
Technicians 2015 (N=80 469)
Other types of personnel 2013 (N=188 973)
Other types of personnel 2014 (N=199 939)
Other types of personnel 2015 (N=200 308)
Hospital graduated Hospital interns First level graduated First level interns
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Figure 8. Distribution of health personnel in hospitals and primary health facilities (%)
Source: Adapted with data from DGIS, 2016. Only personnel in IMSS, ISSSTE and Ministry of Health are included.
21CASE STUDY FROM MEXICO
Table 6. Categories of personnel in primary health facilities in Mexico
Type of personnel2013 2014 2015
N % N % N %
Physicians 75 828 28 81 481 28 93 096 30
Nurses 73 089 27 79 760 28 91 552 29
Other health professionals 24 449 9 25 562 9 13 047 4
Technicians 22 110 8 23 994 8 31 251 10
Other types of personnel 53 771 20 58 260 20 62 101 20
Medical interns 9 327 4 10 136 3 10 740 3
Nursing interns 7 181 3 8 507 3 9 833 3
Dentistry interns 1 937 1 2 324 1 2 350 1
Total 285 045 100 311 888 100 338 210 100
Source: Adapted with data from DGIS, 2016. Only personnel in IMSS, ISSSTE and Ministry of Health are included.
Table 7. Physicians and nurses availability in primary health facilities by institution
Institution
Physicians Nurses
2013 2014 2015 2013 2014 2015
N % N % N % N % N % N %
Ministry of Health 36 803 49 40 806 50 41 893 45 37 893 52 37 893 51 37 893 46
ISSSTE 10 171 13 11 354 14 11 193 12 10 090 14 10 330 14 10 532 13
IMSS 28 854 38 29 321 36 40 010 43 25 106 34 25 366 34 34 514 42
Total 75 828 100 81 481 100 93 096 100 73 089 100 73 589 100 82 939 100
Note: Does not include medical, nursing and dentistry interns.
Source: Adapted with data from DGIS, 2016.
1.53 1.74 1.87
0.56 0.68 0.77
0.48 0.51 0.58
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
2
2013 2014 2015 Physicians Physicians in contact with patients Physicians in primary health facilities Physicians in contact with patients in primary health facilities
2.2
2.35 2.42 2.06
2.19 2.16
0.56 0.6 0.68
0.53 0.57 0.64
0
0.5
1
1.5
2
2.5
3
2013 2014 2015
Nurses
Nurses in contact with patients
Nurses in primary health facilities
Nurses in contact with patients in primary health facilities
Figure 9. Density of physicians per 1000 inhabitants, 2013–2015, in various categories
Note: Does not include medical interns and population with private health insurance
Source: Adapted with data from DGIS, 2016, and from Boletín informativo de estadística, 2016.
22 PRIMARY HEALTH CARE SYSTEMS (PRIMASYS)
The analysis of nursing personnel (specialists, licensed and auxiliaries) shows a general density – hospitals and first-level care facilities included – of over 2 per 1000 inhabitants. This density is slightly lower when limited to nurses in contact with
patients. When considering primary health facilities, the density dramatically falls to less than 1 nurse per 1000 inhabitants, and even less when limited to nurses in contact with patients (Figure 11).
0.49
0.57
0.68 0.69
0.78
0.93
1.13 1.14
0.00
0.20
0.40
0.60
0.80
1.00
1.20
0.59
0.68
0.81
0.98
1.41
0.00
0.20
0.40
0.60
0.80
1.00
1.20
1.40
1.60
Puebla
Guanajuato
Estado de M
éxico
Morelos
Baja Californ
ia
Nuevo León
Chiapas
San Luis Poto
sí
Jalis
co
Chihuahua
Quintana Roo
Michoacá
n
Hidalgo
Coahuila
Sonora
Durango
Sinaloa
Aguascalie
ntes
Promedio N
acional
Oaxaca
Querétaro
Nayarit
Campeche
Guerrero
Baja Californ
ia Sur
Tabasco
Zacateca
s
Tlaxcala
Yuacatán
Veracruz
Colima
Tamaulip
as
Ciudad de Mx
Nuevo León
Estado de M
éxico
Puebla
Jalis
co
Baja Californ
ia
Coahuilia
Sonora
Morelos
San Luis Poto
sí
Chihuahua
Aguascalie
ntes
Quintana Roo
Michoacá
n
Guanajuato
Sinaloa
Querétaro
Promedio N
acional
Chiapas
Durango
Hidalgo
Nayarit
Oaxaca
Baja Californ
ia Sur
Tabasco
Campeche
Tlaxcala
Ciudad de Mx
Guerrero
Colima
Veracruz
Yuacatán
Zacateca
s
Tamaulip
as
Figure 10. Density of physicians per 1000 inhabitants in primary health facilities by state, 2015
Note: Does not include medical and dentistry interns.
Source: Adapted with data from DGIS, 2016, and from Boletín informativo de estadística, 2016.
1.53 1.74 1.87
0.56 0.68 0.77
0.48 0.51 0.58
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
2
2013 2014 2015 Physicians Physicians in contact with patients Physicians in primary health facilities Physicians in contact with patients in primary health facilities
2.2
2.35 2.42 2.06
2.19 2.16
0.56 0.6 0.68
0.53 0.57 0.64
0
0.5
1
1.5
2
2.5
3
2013 2014 2015
Nurses
Nurses in contact with patients
Nurses in primary health facilities
Nurses in contact with patients in primary health facilities
Figure 11. Density of nurses per 1000 inhabitants, 2013–2015, in various categories
Note: Does not include nursing interns and population with private health insurance.
Source: Adapted with data from DGIS, 2016, and from Boletín informativo de estadística, 2016.
23CASE STUDY FROM MEXICO
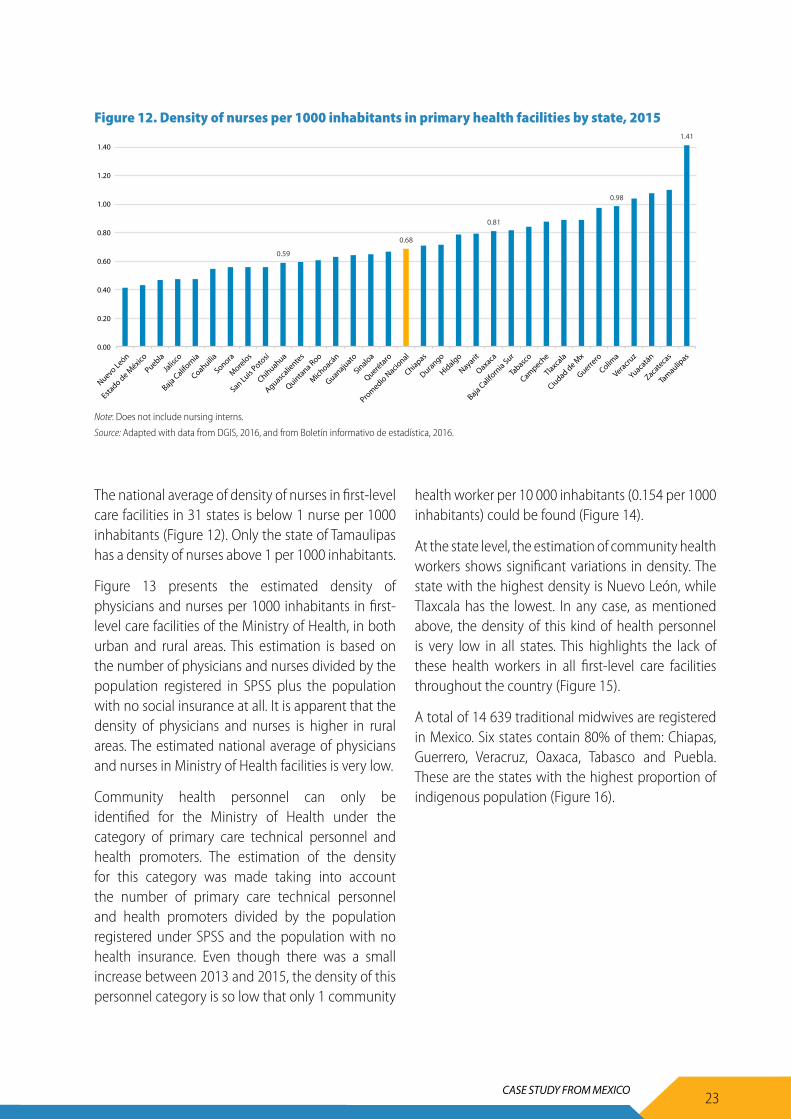
The national average of density of nurses in first-level care facilities in 31 states is below 1 nurse per 1000 inhabitants (Figure 12). Only the state of Tamaulipas has a density of nurses above 1 per 1000 inhabitants.
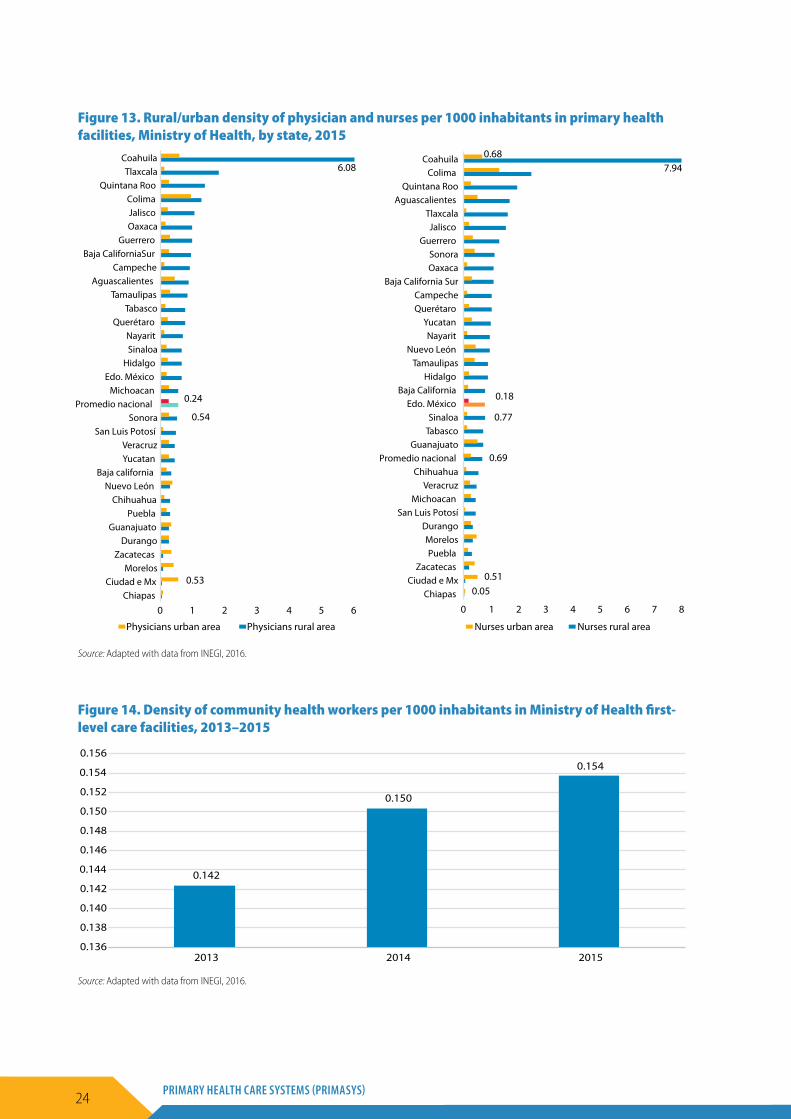
Figure 13 presents the estimated density of physicians and nurses per 1000 inhabitants in first-level care facilities of the Ministry of Health, in both urban and rural areas. This estimation is based on the number of physicians and nurses divided by the population registered in SPSS plus the population with no social insurance at all. It is apparent that the density of physicians and nurses is higher in rural areas. The estimated national average of physicians and nurses in Ministry of Health facilities is very low.
Community health personnel can only be identified for the Ministry of Health under the category of primary care technical personnel and health promoters. The estimation of the density for this category was made taking into account the number of primary care technical personnel and health promoters divided by the population registered under SPSS and the population with no health insurance. Even though there was a small increase between 2013 and 2015, the density of this personnel category is so low that only 1 community
health worker per 10 000 inhabitants (0.154 per 1000 inhabitants) could be found (Figure 14).
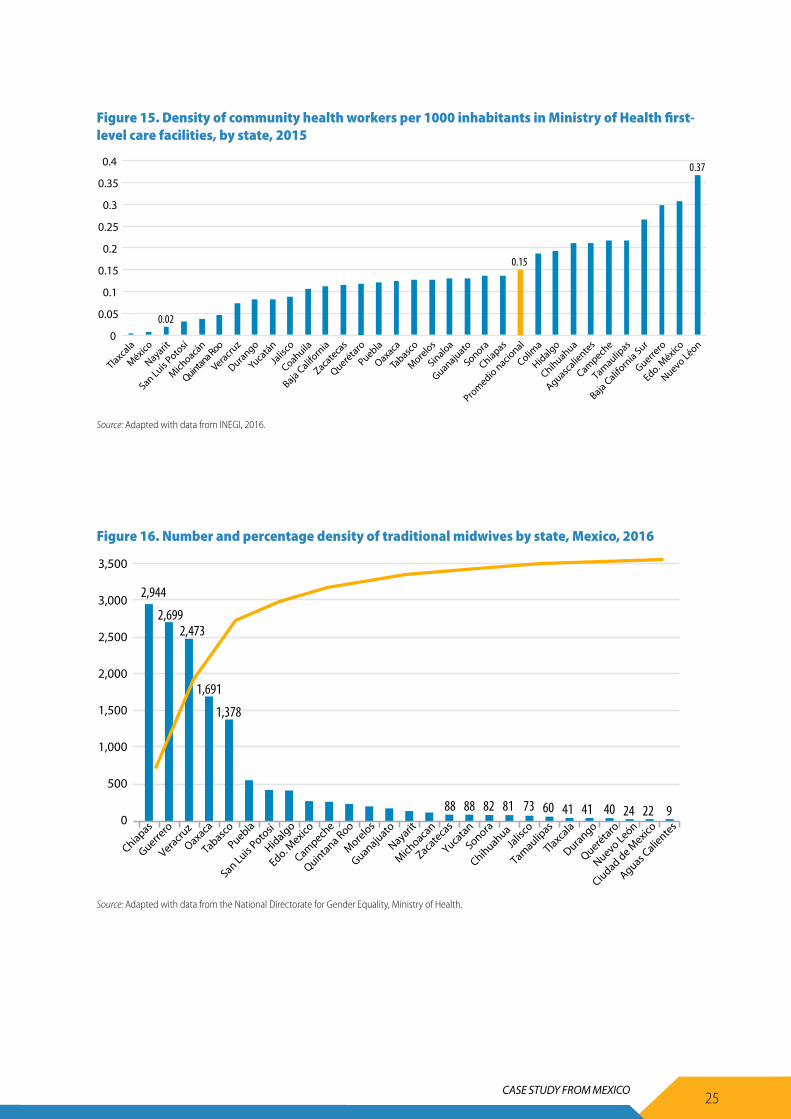
At the state level, the estimation of community health workers shows significant variations in density. The state with the highest density is Nuevo León, while Tlaxcala has the lowest. In any case, as mentioned above, the density of this kind of health personnel is very low in all states. This highlights the lack of these health workers in all first-level care facilities throughout the country (Figure 15).
A total of 14 639 traditional midwives are registered in Mexico. Six states contain 80% of them: Chiapas, Guerrero, Veracruz, Oaxaca, Tabasco and Puebla. These are the states with the highest proportion of indigenous population (Figure 16).
0.49
0.57
0.68 0.69
0.78
0.93
1.13 1.14
0.00
0.20
0.40
0.60
0.80
1.00
1.20
0.59
0.68
0.81
0.98
1.41
0.00
0.20
0.40
0.60
0.80
1.00
1.20
1.40
1.60
Puebla
Guanajuato
Estado de M
éxico
Morelos
Baja Californ
ia
Nuevo León
Chiapas
San Luis Poto
sí
Jalis
co
Chihuahua
Quintana Roo
Michoacá
n
Hidalgo
Coahuila
Sonora
Durango
Sinaloa
Aguascalie
ntes
Promedio N
acional
Oaxaca
Querétaro
Nayarit
Campeche
Guerrero
Baja Californ
ia Sur
Tabasco
Zacateca
s
Tlaxcala
Yuacatán
Veracruz
Colima
Tamaulip
as
Ciudad de Mx
Nuevo León
Estado de M
éxico
Puebla
Jalis
co
Baja Californ
ia
Coahuilia
Sonora
Morelos
San Luis Poto
sí
Chihuahua
Aguascalie
ntes
Quintana Roo
Michoacá
n
Guanajuato
Sinaloa
Querétaro
Promedio N
acional
Chiapas
Durango
Hidalgo
Nayarit
Oaxaca
Baja Californ
ia Sur
Tabasco
Campeche
Tlaxcala
Ciudad de Mx
Guerrero
Colima
Veracruz
Yuacatán
Zacateca
s
Tamaulip
as
Figure 12. Density of nurses per 1000 inhabitants in primary health facilities by state, 2015
Note: Does not include nursing interns.
Source: Adapted with data from DGIS, 2016, and from Boletín informativo de estadística, 2016.
24 PRIMARY HEALTH CARE SYSTEMS (PRIMASYS)
0.05
0.69
0.77
7.94
0.51
0.18
0.68
0 1 2 3 4 5 6 7 8Chiapas
Ciudad e Mx Zacatecas
Puebla Morelos
Durango San Luis Potosí
Michoacan Veracruz
Chihuahua Promedio nacional
Guanajuato Tabasco Sinaloa
Edo. México Baja California
Hidalgo Tamaulipas
Nuevo León Nayarit
Yucatan Querétaro Campeche
Baja California Sur Oaxaca Sonora
Guerrero Jalisco
Tlaxcala Aguascalientes
Quintana Roo Colima
Coahuila
Nurses urban area Nurses rural area
0.54
6.08
0.53
0.24
0 2 4 531 6Chiapas
Ciudad e Mx Morelos
Zacatecas Durango
Guanajuato Puebla
Chihuahua Nuevo León
Baja california Yucatan Veracruz
San Luis Potosí Sonora
Promedio nacional Michoacan
Edo. México Hidalgo
Sinaloa Nayarit
Querétaro Tabasco
Tamaulipas Aguascalientes
Campeche Baja CaliforniaSur
Guerrero Oaxaca Jalisco
Colima Quintana Roo
Tlaxcala Coahuila
Physicians urban area Physicians rural area
Figure 13. Rural/urban density of physician and nurses per 1000 inhabitants in primary health facilities, Ministry of Health, by state, 2015
Source: Adapted with data from INEGI, 2016.
0.142
0.150
0.154
0.136
0.138
0.140
0.142
0.144
0.146
0.148
0.150
0.152
0.154
0.156
2013 2014 2015
Figure 14. Density of community health workers per 1000 inhabitants in Ministry of Health first-level care facilities, 2013–2015
Source: Adapted with data from INEGI, 2016.
25CASE STUDY FROM MEXICO
0.02
0.15
0.37
0
0.05
0.1
0.15
0.2
0.25
0.3
0.35
0.4
Tlaxcala
Nayarit
México
San Luis Poto
sí
Michoacá
n
Coahuila
Baja Californ
ia
Zacateca
s
Puebla
Querétaro
Oaxaca
Tabasco
Morelos
Sinaloa
Guanajuato
Sonora
Chiapas
Promedio nacio
nal
Colima
Hidalgo
Chihuahua
Aguascalie
ntes
Campeche
Tamaulipas
Baja Californ
ia Sur
Guerrero
Edo. México
Nuevo Léon
Veracruz
Quintana R
oo
Durango
Yucatán
Jalis
co
Figure 15. Density of community health workers per 1000 inhabitants in Ministry of Health first-level care facilities, by state, 2015
Source: Adapted with data from INEGI, 2016.
0
500
1,000
1,500
2,000
2,500
3,000
3,500
Chiapas
Guerrero
Veracruz
Oaxaca
Puebla
Hidalgo
Campeche
Morelos
Nayarit
Zacateca
s
Tabasco
San Luis Poto
sí
Edo. Mexico
Quintana Roo
Guanajuato
Michoaca
n
Yucatan
Sonora
Chihuahua
Jalis
co
Tamaulipas
Tlaxcala
Durango
Querétaro
Nuevo León
Ciudad de Mexico
Aguas Calie
ntes
2,944
2,6992,473
1,691
1,3781,378
88 88 82 81 73 60 41 41 40 24 22 9
Figure 16. Number and percentage density of traditional midwives by state, Mexico, 2016
Source: Adapted with data from the National Directorate for Gender Equality, Ministry of Health.

26 PRIMARY HEALTH CARE SYSTEMS (PRIMASYS)
8. Planning and implementation
In the absence of a generally accepted conceptual framework for PHC, each health care institution in the Mexican health system implements its own model. Nevertheless, most of them define PHC as outpatient care and the entrance to the health system. Based on this definition they provide a range of relevant interventions at the individual, family and community levels. Those interventions can be organized into two broad categories:
• Public health interventions. These include those interventions that are intended to reach the whole population. They fall under the responsibility of the Ministry of Health, the SESAs, and other public and private institutions, and include health promotion and health education, immunization, timely detection of risk factors, family planning and epidemiological surveillance.
• Low-complexity interventions. These include health education, preventive and curative medical care, and rehabilitation, and are the responsibility of the integrated health services networks. They include pregnancy and delivery care services, emergencies, injuries, oral health, chronic diseases detection, some types of cancer, sexually transmitted diseases and mental health.
According to the planning processes, 85% of all interventions should be provided in first-level care facilities, mostly dedicated to outpatient care. The basic human resources in this level include a physician, a nurse and a health promoter. Besides, facilities in locations with high indigenous populations should also include interpreters or must assure that the personnel have the necessary communication
abilities. Complementary teams include specialized nurses, gynaecologist, psychologist, paediatrician, nutritionist, dentist, social workers and midwives. Nevertheless, quite often these teams are incomplete.
At the state level, primary care operation plans are used to develop diagnostics and plan goals for programmes in the following areas: prevention (chronic diseases, vector-borne diseases and mental diseases); epidemiology (respiratory diseases and diarrhoea); first-level care (self-care promotion and healthy lifestyles according to lifelines, oral health, nutrition, physical activity, improved access for rural communities); childhood and adolescence (immunization, breastfeeding promotion, accident prevention, injuries and adolescent pregnancy); and reproductive health (maternal and child health, breast and uterine cancer prevention) (47–50).
In 2015 (Table 8), 22 072 outpatient health units, 4456 hospitals, 88 390 medical offices, 9235 operation theatres and 184 112 beds were available for the provision of these services. While 94% of the primary health facilities were part of the public sector, 73% of the hospitals and operation rooms were in the private sector (4). In relation to the primary health facilities of the SESAs with amplified services or with hospitalization, only 321 had a clinical laboratory, 143 had images services, 264 had electrocardiography and only 81 had ultrasound equipment (29). The actors who participated in the interviews said that the number of first-level care facilities is slowly growing, and they are saturated with the high demand for their services. At the same time, equipment is insufficient and needs to be improved.
Table 8. Health care services: infrastructure offered, by institution, Mexico 2015
Type of service Min. of Health IMSS IMSS Prospera ISSSTE Othera Private Total
Primary health facilities 14 387 1 143 4 198 1 063 654 627 22 072Hospitals 741 265 80 111 189 3 070 4 456Medical offices 39 639 18 121 5 058 6 619 5 546 13 407 88 390Operation rooms 1 891 1 469 122 330 429 4 994 9 235Total beds 62 270 47 463 3 931 10 749 10 185 44 514 184 112
a. Including PEMEX, Ministry of Defence, SEMAR.
Source: DGIS, 2015.

27CASE STUDY FROM MEXICO
The private sector is very important in health care services provision. For every public hospital there are 2.3 private hospitals. Nevertheless, most private hospitals have less than 20 beds and function mainly as outpatient clinics, offering PHC and some specialized diagnostic and treatment services (51).
Referral and counter-referral systems have been developed since 1988, mainly under the Ministry of Health, which has formulated a compulsory manual for all of its medical facilities. In 1994 another effort was launched to strengthen coordination between units, including through an improved information system and personnel training. In 1996 hospital directors and sanitary jurisdiction authorities were incorporated into the system as representatives of the first level of care (52, 53).
In the MAI PHC model, the sanitary jurisdictions of the Ministry of Health are considered as responsible for the organization of the integrated health services networks. The latter may include units from another jurisdiction or state, and integration of public and private providers may even be considered. This proposal tries to guarantee continuous care on the basis of health care networks and to ensure coordination and articulation among institutions. The definitions of referral and counter-referral outpatient, specialized, hospital and emergency care have been made according to demographic and epidemiological profiles and are the basis for identifying pathologies needing care beyond the first level (6).
According to the interviewed actors, the referral and counter-referral system between first-level care facilities and hospitals still presents several problems, even within the different institutions. Pathologies that can be taken care of in the first level of care may be referred to hospitals, while other referrals are held back. Some patients do not reach the referral institutions and opt for the private sector because of extended waiting times. Counter-referrals to the original facility are rare because of a lack of follow-up of patients or because the patients are cured.
Concerning patients’ participation, the 1973 Social Security Law included community participation (54). Nevertheless, it was not until 2001 that the post of “citizens’ representative” was created as part of the National Crusade for Quality. This should help improve the quality of follow-up health care. In addition, a National Network of Citizens’ Representatives was created in 2009 (5, 55). In 2016 there were 14 798 citizens’ representatives in 14 506 health facilities.
Their responsibilities include:
• conduct surveys on the patients’ perception of quality and of health care professionals in the medical facilities;
• disseminate information on the rights of patients, fostering their protection and accountability;
• make propositions for improvements and establish agreements with the medical facilities’ authorities and personnel;
• request information on quality of care and patients security projects;
• participate in the state’s Quality of Health Care Committee and in the Quality and Patients’ Security Committee.
Nevertheless, despite the large number of citizens’ representatives, many of them are influenced by the health workers and cannot function with real autonomy in order to represent the citizens rather than the health institutions.

28 PRIMARY HEALTH CARE SYSTEMS (PRIMASYS)
9. Regulatory process
The main coordination and regulatory organism is the General Health Council (Consejo de Salubridad General). It is founded in the Mexican Constitution (Article 73, paragraph XVI) as well as in several articles of the General Health Law. The General Health Council is formed by the Health Minister, the directors of the National System for Integral Family Development and the National Science and Technology Council, the medical directors of IMSS and ISSSTE, and representatives of health-related academic institutions (5, 56, 57). The General Health Council’s responsibilities regarding PHC include (a) to elaborate, disseminate and update the basic supplies list for the first level of care, together with the Ministry of Health and other public institutions; (b) to elaborate, publish and update the generic medicines catalogue; and (c) to establish quality evaluation actions for the certification of health care facilities, thus defining the PHC clinics’ certification standards (58, 59).
The stewardship of the health system is a responsibility of the federal government and is a function of the Ministry of Health, which regulates all institutions, programmes, policies and services in the health sector. Despite being the regulator, the Ministry of Health exercises only weak stewardship and the stakeholders that were interviewed recognized the existence of good coordination mechanisms between the Ministry of Health and other public health institutions. Concerning PHC, the weakness of the Ministry of Health has led to the definition of different models and services.
Regarding the states’ health care services or SESAs, since 1986 the Ministry of Health has employed the National Health Council as the mechanism to coordinate planning, budgeting and assessment of public health. In 1995, this council was restructured as a permanent coordination mechanism between the federation and the state governments that supports the decentralization of health services. Its
main functions are (a) to establish the coordination guidelines for general public health care; (b) to unify criteria for the implementation of public health programmes; (c) to promote priority health programmes; and (d) to propose complementary financing strategies in public health (19, 57, 60). The regulation of health care is also collaboratively carried out with the participation of civil society organizations and professional associations (5, 8). At the state level, the sanitary jurisdiction is the technical and administration entity responsible for the coordination of PHC, for organization of outpatient care, for ensuring the quality of and access to health care services, and for organizing intersectoral participation to address the social determinants of health (6).
The main functions of the sanitary jurisdictions include:
• organizing and surveillance of medical care and public health according to the established norms;
• monitoring the quality standards in the first-level care units;
• supporting the elaboration of the states’ health diagnostics and programmes;
• updating the states’ health care model;• coordinating social participation in health matters;• supporting sanitary surveillance.
Concerning IMSS, according to Article 139 of its internal regulation, the different delegations are responsible for the operation of institutional health services, except for those performed by the specialty medical facilities. The delegations determine budgets and the resources for each health facility in order to comply with the work programmes. Delegations are integrated with a number of governing and administrative entities, including subdelegations, directorates, and normative and coordinating units (61).

29CASE STUDY FROM MEXICO
In the case of ISSSTE, delegations have responsibilities in defined health territories. They are decentralized units of the institute that support the General Director and the Council Directorate in planning, coordination, organization, operation, delivery and supervision of insurance, benefits and services (62).
Between 2001 and 2006, the National Crusade for Quality was implemented as an inter-institutional initiative by the federal government to “improve health services quality, taking it to acceptable levels throughout the country, and making sure that the population is aware of the improvement”. The achievements of the National Crusade for Quality include the creation of an ethics and behaviour code for all health professionals, human resources training in quality issues, development of health information systems, standardization of procedures, results monitoring, implementation of institutional continuous improvement systems, performance recognition, and strengthening of citizens’ participation through the citizens’ representatives (63). At the same time, the crusade fostered certification of health facilities, mainly primary health facilities, through the National System for the Certification of Medical Care Establishments (SiNaCEAM) (59).
In order to foster adherence to health care protocols in the first level of care, the Action Programme for the Development of Clinical Practice Guides (CPGs) was launched in 2008 together with the Sector Strategic Plan for the Dissemination, Training and Follow-up of CPGs. A total of 786 CPGs have been developed, of which 143 correspond to health care at the first level of care. These include 5 CPGs for breast, cervical and prostate cancer, 22 for maternal and child health, 15 for children’s health, 8 for reproductive and sexual health, 8 more for mental health, 16 for chronic diseases and 10 for infectious diseases (64).
On the other hand, an estimated 30% of all people with some kind of health insurance scheme (including the Popular Health Insurance) use the private sector’s outpatient health care services. Medical offices adjacent to pharmacies have skyrocketed in recent
years (56). No clear mechanisms are in place to regulate the quality of care in these facilities (26, 51).
Accreditation of nursing and medical schools is guided by the Mexican Council for Medical Education and the Mexican Council for the Accreditation and Certification of Nursing, which are both recognized by the Council for the Accreditation of Higher Education. Despite the existence of these organizations, full accreditation of all the programmes in the country has not been achieved. In fact, only 44 of 80 medical schools and only a few of the 600 nursing training programmes have been accredited. Awarding degrees and certification is the responsibility of universities and other higher education institutions, together with the Ministry of Education’s General Directorate for Professions, which is in charge of awarding physicians’ licences.
Concerning PHC education, Mexico has an academic structure for postgraduate studies. In 1994 the Mexican College of Family Medicine was founded, gathering around 36 state-level primary care associations and medical colleges. Some universities have family medicine departments, and the Mexican Council for the Certification of Family Medicine can certify specialists in family medicine (56). Regarding undergraduate education in medicine, there is no information on the inclusion of PHC in the curricula of any of the universities. Similarly, there is a great variety of schools training nurses at technical and Bachelor of Arts level, but there is no information on the curricula for PHC nurses. Unfortunately nurses are still being trained only to become the aids of physicians, while their potential for strengthening PHC is neglected (65).

30 PRIMARY HEALTH CARE SYSTEMS (PRIMASYS)
10. Monitoring and information system
Mexico has a long history concerning health information systems. In 1930, the Sanitary Statistics Section was established to register demographic and epidemiological information in order to help prioritize public health actions. In 1986, aiming to evaluate the coverage of PHC services, a study in the different states was undertaken, considering 13 indicators. Eight indicators measured maternal and child health coverage, immunization, nutritional guidance and the control of endemic diseases. The other indicators were related to the availability and use of health care services (66). The results showed a country with a medium coverage in PHC (64.94/100 points), with extreme results between states. Coahuila reached 84.62 points while Chiapas only achieved 43.92 points (67). Also in 1986, the National Health Survey System was put in place to assess the nutrition and health conditions, as well as the impact and coverage of health programmes. In 1995 the National Epidemiological Surveillance System was created to consolidate the information from all health institutions in order to identify health risks and threats (68–70).
Presently, Mexico has a broad Health Information System that includes information from the different public and private institutions. The information areas include information on the population’s opinion about health care services, health expenditures, resources and availability of health care services, damages and risks, and births and deaths. This information is available through censuses, surveys and administrative registers. One of the main problems is that administrative registers are operated by and are only available for each institution. Only those of the Ministry of Health are available through a public platform. Otherwise, the information from surveys and censuses is freely available. Mexico has several information sources using different indicators to carry out monitoring and assessment of outpatient care:
• demographic events registers• population and housing censuses• ordinary registers of the health services• epidemiological surveillance data• sample-based surveys (population surveys)• disease registers• other sectoral information sources (economic,
political, social welfare).
With support from the World Health Organization, evaluation has been carried out of the performance of health systems, including outpatient care (71). The evaluation includes 57 indicators (72), of which 23 correspond to health conditions (maternal and child health, chronic diseases, breast and cervical cancer, and diseases of children aged under 5 years, among others). Another 15 indicators are related to the availability and accessibility of health services (immunization, access to antenatal care and institutional delivery), 5 more refer to technical and interpersonal quality (delivery of prescribed drugs, explanation of health status in the first level of care and waiting times), 15 are related to acceptability and efficiency (percentage of patients that are satisfied with health care in the first level, daily general consultation average per physician), and 3 are related to adolescents, drinking water, and percentage of communities that have been certified as healthy. These assessments are the responsibility of the General Directorate for Performance Evaluation of the Ministry of Health. In addition, a follow-up of the fulfilment of the objectives of the Health Sector Programme using 16 results indicators regularly takes place. Table 9 shows the indicators related to PHC.

31CASE STUDY FROM MEXICO
Table 9. Follow-up and outcome indicators related to PHC
Indicator 2014 2015 2016 Goal 2018 Source
% immunization coverage of complete scheme in children aged under 1 year
88.91 90.68 88.50 90.0 Databases of:National Centre for Children’s and Adolescents’ HealthBirth information subsystem, National Health Information System
Breast cancer mortality rate (per 100 000 women aged 25 years or older)
17.59 18.03 18.78 16.0 Mortality databases:National Institute of Statistics, Geography and Informatics / Ministry of Health: National Health Information SystemPopulation projections 2010–2050: National Population Council
Cervical cancer mortality rate (per 100 000 women aged 25 years or older)
11.94 11.52 11.58 10.0 Mortality databases:National Institute of Statistics, Geography and Informatics / Ministry of Health: National Health Information SystemPopulation projections 2010–2050: National Population Council
Uncontrolled diabetes with short-term complications: hospitalization (rate per 100 000 public health users aged 15 years or older)
15.67 15.10 ND 16.0 Health sector hospital discharge databasesNational Health Information System Population projections, National Population Council
Infant mortality rate (per 1000 live births)
12.51 12.52 12.32 10.1 Mortality databases:INEGI/Ministry of HealthBirth information subsystem, National Health Information System
Maternal mortality ratio (deaths per 100 000 live births)
38.94 34.59 ND 30.0 Mortality databases:National Institute of Statistics, Geography and Informatics / Ministry of HealthBirth information subsystem, National Health Information System
% of chlorinated water according to the specification of the Mexican Official Norm
90.70 91.60 ND 93.0 Federal Sanitary System; Federal Commission for Protection against Sanitary Risks (COFEPRIS)
% of public expenditure on health care provision and public health activities outside the health facilities
91.68 91.41 ND 85.0 Volume IV, Financial Resources of the Bulletin of the Statistical Information of the Federal and States Health Accounts System
% complete delivery of prescribed drugs
NA 68.97 NA 90.0 Biannual measure indicator. Source: National Health and Nutrition Survey (ENSANUT) 20122015 survey follow-up of indicators of PROSESA 2013–2018
% of the population lacking access to health care services
18.16 NA ND 6.0 Source: Socioeconomic conditions module associated with the National Survey of Household Revenues and Expenditures of the National Institute of Statistics, Geography and Informatics% of the population with public
health coverage that uses health care public services
63.29 NA ND 80.0
% of households in the first income quintile with catastrophic health expenditures
4.53 NA ND 3.5
ND = not determined; NA = not available.
Source: DGED, 2017.
The evaluation of the implementation of CPGs showed a 27% compliance rate for the hypertension CPG (47% SESA, 31% ISSSTE, 34% IMSS); 47% compliance for the antenatal care CPG (47% SESA, 39% ISSSTE, 54% IMSS); and 50% compliance for the
diabetes CPG (51% SESA, 39% ISSSTE, 54% IMSS). In the case of diabetes, for instance, there are 13 CPGs, of which 4 are relevant in the first level of care (73, 74). Recent studies suggest that the quality and the implementation of CPGs for chronic disease care

32 PRIMARY HEALTH CARE SYSTEMS (PRIMASYS)
at the first level, including diabetes, hypertension, dyslipidemia, overweight/obesity and cardiovascular risk, have a compliance rate ranging from 39% to 53%. The maternal and child health CPGs have similar figures (75, 76).
According to the National Health and Nutrition Survey (ENSANUT), 2012, one out of eight users of PHC services would avoid using them because of long waiting times, mistreatment or lack of improvements in health conditions. Limited health care service schedules and personnel and equipment deficiencies add to these challenges (56). ENSANUT 2016 reports an average waiting time of 70.9 minutes for patients with diabetes, hypertension and dyslipidemia. SESAs and IMSS-Prospera show the longest waiting times (91.1 and 81.8 minutes, respectively). In addition, 77.1% of the patients received all the prescribed drugs, of which 34.9% were for IMSS and 25.6% for SESA. Concerning the outcome of care, 72.2% of interviewees considered their health conditions had improved because of the care they received (77).

33CASE STUDY FROM MEXICO
11. Policy considerations and ways forward
Primary health care is a major concept used by decision-makers in Mexico. As stated by several decision-makers, there are different conceptual frameworks to define primary health care, its organizations and operational elements. A first element that needs to be reviewed is the conceptual and operative definition of PHC. Throughout this document, and following the usual Mexican definitions, reference has been made to outpatient care, but many decision-makers consider that primary health care is exclusively provided in primary health facilities, while others consider that it is provided in both primary health facilities and hospitals.
According to the National Health Plan 2013–2018, the basis of MAI is the strengthening of PHC. It is therefore first necessary to review the package of health services delivered to the population and assess if it can coherently respond to the health needs of the population. In that regard, priority should be given to the implementation, monitoring and evaluation of actions that support health promotion and disease prevention, without disregarding actions that support healing and rehabilitation.
The implementation of a PHC-oriented health care model entails strengthening the training of human resources for health so that they acquire the necessary competences to assure delivery of quality health care. It is also important to consider new occupational profiles other than just physicians and nurses as part of the PHC teams. These could include health professionals such as professional midwives, health promoters, nutritionists, psychologists and physical trainers, who could all be members of the primary health care teams.
The implementation of a health care model based on PHC is essential. This entails training health professionals to adequately manage the different aspects of health care. In this regard, the management of primary health facilities requires special attention. They need sufficient human resources, equipment, medicines, appropriate technology and other
supplies to meet the demand for and assure the delivery of high-quality health services.
The public health sector is already on course for integration of its several institutions. But the future is uncertain about what can be achieved in the short and medium terms. In the case of PHC, one clear model to guide its implementation in all public institutions will be the beginning of real integration. This includes the definition of a package of indicators that will make it possible to monitor, assess and compare what is being done throughout the public primary health system.
A large proportion of financing of primary care is dedicated to outpatient care. One major challenge is to increase expenditure on preventive care. Another challenge is the development of new information on the pertinent variables, enabling a more precise and detailed analysis of the financing of primary care.
The undeniable importance of the private sector to primary health, as the case of medical offices adjacent to pharmacies shows, underlines the need for better regulation. The Ministry of Health needs to strengthen its capacity as steward of the health system in order to transform this reality into an opportunity. The private sector could provide better information on the population’s needs and, at the same time, if it complies with the quality standards, could function as an ally provider.
At the community level, it is vital to engage citizens in formulation of the diverse interventions related to their health demands through the participation of various stakeholders and actors from civil society. Disease prevention and health promotion strategies need increased financing, given their potential to influence lifestyles and combat the risk factors behind the increasing prevalence of chronic degenerative diseases in Mexico. Finally, it is necessary to review how PHC is being financed: What are the resource allocation mechanisms? How are resources distributed among prevention, promotion, healing and rehabilitation actions? and, What budget mechanisms are in place?
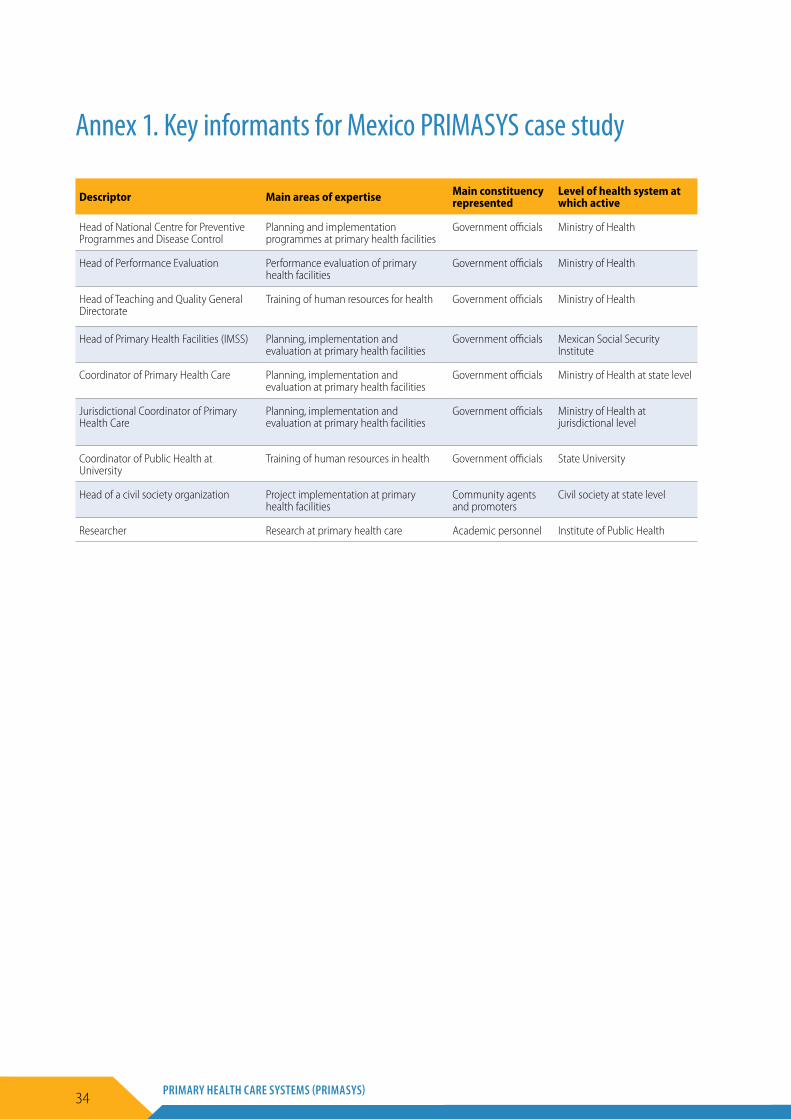
34 PRIMARY HEALTH CARE SYSTEMS (PRIMASYS)
Annex 1. Key informants for Mexico PRIMASYS case study
Descriptor Main areas of expertise Main constituency represented
Level of health system at which active
Head of National Centre for Preventive Programmes and Disease Control
Planning and implementation programmes at primary health facilities
Government officials Ministry of Health
Head of Performance Evaluation Performance evaluation of primary health facilities
Government officials Ministry of Health
Head of Teaching and Quality General Directorate
Training of human resources for health Government officials Ministry of Health
Head of Primary Health Facilities (IMSS) Planning, implementation and evaluation at primary health facilities
Government officials Mexican Social Security Institute
Coordinator of Primary Health Care Planning, implementation and evaluation at primary health facilities
Government officials Ministry of Health at state level
Jurisdictional Coordinator of Primary Health Care
Planning, implementation and evaluation at primary health facilities
Government officials Ministry of Health at jurisdictional level
Coordinator of Public Health at University
Training of human resources in health Government officials State University
Head of a civil society organization Project implementation at primary health facilities
Community agents and promoters
Civil society at state level
Researcher Research at primary health care Academic personnel Institute of Public Health
35CASE STUDY FROM MEXICO
References
1. Proyecciones de la población 2010–2015 [Population projections for 2010–2015]. National Population Council (http://www.conapo.gob.mx/es/CONAPO/Proyecciones, accessed 15 October 2017) (in Spanish).
2. World urbanization prospects: the 2014 revision. Population Division of the Department of Economic and Social Affairs, United Nations (https://esa.un.org/unpd/wup/, accessed 15 October 2017).
3. Medición de la pobreza en México: resultados de pobreza en México 2014 a nivel nacional y por entidades federativas [Poverty measures in Mexico: poverty results in Mexico in 2014 at the national and states level]. National Evaluation Council (http://www.coneval.org.mx/Medicion/Paginas/PobrezaInicio.aspx, accessed 15 October 2017) (in Spanish).
4. Boletín de información estadística 2014–2015 [2014–2015 statistical information bulletin of the Ministry of Health]. Ministry of Health (http://www.dgis.salud.gob.mx/descargas/pdf/Boletxn_InformacixnEstadxstica_14_15.pdf, accessed 15 October 2017) (in Spanish).
5. Gómez-Dantés O, Sesma S, Becerril VM, Knaul FM, Arreola H, Frenk J. Sistema de salud de México [The health system of Mexico]. Salud Pública de México. 2011;53(Suppl. 2):S220–32 (in Spanish).
6. Modelo de Atención Integral de Salud (MAI) [Comprehensive Health Care Model]. Mexico: Ministry of Health; 2015 (http://www.dgplades.salud.gob.mx/Contenidos/Documentos/Biblioteca/ModeloAtencionIntegral.pdf, accessed 15 October 2017) (in Spanish).
7. Bonilla-Chacín ME, Aguilera N. The Mexican Social Protection System in Health. Universal Health Coverage Studies Series (UNICO) No. 1. Washington (DC): World Bank; 2013.
8. Nava-Zarate N, Orellana-Centeno M, Orellana-Centeno JE, Onofre-Quilantan MG. Comparación de los sistemas de salud de México y de España [Comparison of the health systems of Mexico and Spain]. Salud en Tabasco. 2013;1928–36 (http://www.redalyc.org/articulo.oa?id=48727474007, accessed 16 October 2017) (in Spanish).
9. Sistema de Información de los Objetivos de Desarrollo del Milenio [Millennium Development Goals Information System] (http://www.objetivosdedesarrollodelmilenio.org.mx/, accessed 16 October 2017) (in Spanish).
10. Antecedentes del programa de unidades médicas móviles [Background to the mobile medical facilities programme]. Directorate for Health Planning and Development, Ministry of Health; 2015 (http://www.gob.mx/salud/articulos/antecedentes-del-programa-de-unidades-medicas-moviles?state=draft, accessed, 16 October 2017) (in Spanish).
11. Cravioto-Meneses A. Avances del programa de extensión de cobertura de servicios de salud al medio rural de México durante 1977 [Progress of the health services coverage extension programme in rural Mexico during 1977]. Boletín de la Oficina Sanitaria Panamericana. 1980;88(5) (in Spanish).
12. Acuerdo por el que se emiten las reglas de operación del programa unidades médicas móviles, para el ejercicio fiscal 2016 [Agreement stating the operation rules of the mobile medical facilities programme for the 2016 fiscal year]. Official Journal of the Federation, 30 December 2015 (in Spanish).
13. Velásquez-Díaz G. Programa IMSS-COPLAMAR [IMSS-COPLAMAR programme]. In: Salud y enfermedad en el medio rural de México [Health and disease in rural Mexico]. Mexico: Ministry of Health; 1991:413–21 (in Spanish).
14. Alvarado A, Morin-Zenteno J. Efectos del modelo de atención a la salud del programa IMSS-COPLAMAR sobre el estado de salud de la población rural marginada de México [Effects of the IMSS-COPLAMAR health care model on the health conditions of the marginalized rural population of Mexico]. Salud Pública de México. 1989;31:745–56 (in Spanish).
15. Las necesidades de atención de la salud y la organización del sistema de salud en México [Health care needs and the organization of the health system in Mexico]. In: Estudios de la OCDE sobre los sistemas de salud: México [OECD studies on health systems: Mexico]. Paris: Organisation for Economic Co-operation and Development; 2016 (http://dx.doi.org/10.1787/9789264265523–5-es, accessed 16 October 2017) (in Spanish).
16. Jaramillo-Cardona MC. La descentralización de la salud en México: avances y retrocesos [Decentralization of health in Mexico: progress and setbacks]. Revista Gerencia y Políticas de Salud. 2007;6(13):85–111 (in Spanish).
17. Frenk J, Sepulveda J, Gomez-Dantés O, Knaul F. Evidence-based health policy: three generations of reform in Mexico. Lancet. 2003;362(9396):1667–71.
36 PRIMARY HEALTH CARE SYSTEMS (PRIMASYS)
18. Kumate J, Sepúlveda J, Juan M, et al. Fortalecimiento de los sistemas locales de salud: proyecto de desarrollo de jurisdicciones sanitarias [Local health systems strengthening: project for the development of sanitary jurisdictions]. Salud Pública de México. 1994;36(6):673–93 (in Spanish).
19. Acuerdo por el que se establece la integración y objetivos del Consejo Nacional de Salud [Agreement on the establishment and integration of the National Health Council]. Official Journal of the Federation, 27 January 2009 (in Spanish).
20. Hevia de la Jara F. De Progresa a Oportunidades: efectos y límites de la corriente cívica en el gobierno de Vicente Fox [From Progresa to Oportunidades: effects and limits of the civic current in the government of Vicente Fox]. Sociológica (México). 2009;24(70):43–81 (http://www.scielo.org.mx/scielo.php?script=sci_arttext&pid=S0187–01732009000200003&lng=es&tlng=es, accessed 16 October 2017) (in Spanish).
21. La pobreza rural en América Latina: lecciones para una reorientación de las políticas [Rural poverty in Latin America: lessons for policy reorientation]. Serie Seminarios y Conferencias No. 27. Chile: CEPAL; 2003 (in Spanish).
22. Acuerdo por el que se emiten las reglas de operación del programa fortalecimiento a la atención médica, para el ejercicio fiscal 2017 [Agreement establishing the operation rules of the medical care strengthening programme for the 2017 fiscal year]. Official Journal of the Federation, 29 December 2016 (in Spanish).
23. Giedion U, Panopoulou G, Gómez-Fraga S. Diseño y ajuste de los planes explícitos de beneficios: el caso de Colombia y México [Design and adjustment of the explicit benefits plans: the cases of Colombia and Mexico]. Serie Financiamiento del Desarrollo No. 219. Chile: CEPAL; 2009 (in Spanish).
24. Nigenda G. El seguro popular de salud en México: desarrollo y retos para el futuro [Popular health insurance in Mexico: development and future challenges]. Nota Técnica de Salud No. 2. Inter-American Development Bank, Division of Social Development Programmes; 2005 (in Spanish).
25. Knaul FM, González-Pier E, Gómez-Dantés O, García-Junco D, Arreola-Ornelas H, Barraza-Lloréns M et al. Hacia la cobertura universal en salud: protección social para todos en México [Towards universal health coverage: social protection for all in Mexico]. Salud Pública de México. 2013;55(2):207–35 (http://www.scielo.org.mx/scielo.php?script=sci_arttext&pid=S0036–36342013000200013&lng=es, accessed 16 October 2017) (in Spanish).
26. Diagnóstico y recomendaciones [Diagnosis and recommendations]. In: Estudios de la OCDE sobre los sistemas de salud: México [OECD studies on health systems: Mexico]. Paris: Organisation for Economic Co-operation and Development; 2016 (http://dx.doi.org/10.1787/9789264265523–4-es, accessed 16 October 2017) (in Spanish).
27. Santos-Burgoa C, Rodríguez-Cabrera L, Rivero L, Ochoa J, Stanford A, Latinovic L et al. Implementación del modelo operativo mexicano de promoción de la salud [Implementation of the Mexican operative model for health promotion]. Preventing Chronic Disease. 2009;6(1):A32 (http://www.cdc.gov/pcd/issues/2009/jan/08_0085_es.htm, accessed 16 October 2017) (in Spanish).
28. Programa de Acción Específico: promoción de la salud y determinantes sociales 2013–2018 [Specific Action Programme: health promotion and social determinants 2013–2018]. Mexico: Ministry of Health (http://www.promocion.salud.gob.mx/dgps/interior1/programas/determinantes_sociales.html, accessed 16 October 2017) (in Spanish).
29. Observatorio de los servicios de atención primaria [Primary care services observatory]. General Directorate of Performance Evaluation, Ministry of Health; 2013 (http://www.dged.salud.gob.mx/contenidos/dess/descargas/upn/OSAP_2012.pdf, accessed 16 October 2017) (in Spanish).
30. Concept of governance. United Nations Educational, Scientific and Cultural Organization (http://www.unesco.org/new/en/education/themes/strengthening-education-systems/quality-framework/technical-notes/concept-of-governance/, accessed 16 October 2017).
31. Health system topics: governance. Geneva: World Health Organization (http://www.who.int/healthsystems/topics/stewardship/en/, accessed 16 October 2017).
32. Plan Sectorial de Salud 2013–2018 [Health Sector Plan 2013–2018]. Government of Mexico, Ministry of Health; 2013 (in Spanish).
33. La renovación de la atención primaria a la salud en las Américas [Renewal of primary health care in the Americas]. Washington (DC): OPS/OMS; 2007 (http://www2.paho.org/hq/dmdocuments/2010/Renovacion_Atencion_Primaria_Salud_Americas-OPS.pdf, accessed 16 October 2017) (in Spanish).
34. IMSS. Manual de Organización de la Dirección de Prestaciones Médicas. [Organization Manual of the Directorate For Health Care Services Provision] México, 2017. (http://www.imss.gob.mx/sites/all/statics/pdf/manualesynormas/2000-002-001.pdf, accessed 16 October 2017) (in Spanish).
37CASE STUDY FROM MEXICO
35. ISSFAM. Manual de organización [Organization manual]. ISSFAM; 2016 (https://www.gob.mx/cms/uploads/attachment/file/151974/manual_org_issfam.pdf, accessed 16 October 2017) (in Spanish).
36. Acciones y programas: Sistema de Salud Naval [Actions and programmes: Naval Health System]. Secretariat of the Navy (http://www.gob.mx/semar/acciones-y-programas/sistema-de-salud-naval-4789, accessed 16 October 2017) (in Spanish).
37. Díaz-Portillo SP, Idrovo AJ, Dreser A, Bonilla FR, Matías-Juan BWV. Consultorios adyacentes a farmacias privadas en México: infraestructura y características del personal médico y su remuneración [Clinics adjacent to private pharmacies in Mexico: infrastructure and characteristics of the physicians and their remuneration]. Salud Pública de México. 2015;(57):320–8 (in Spanish).
38. Avances de la estrategia para el fortalecimiento de la regulación en farmacias y consultorios [Progress of the strategy to strengthen regulation of pharmacies and medical offices]. COFEPRIS; 2015 (in Spanish).
39. Barraza M, Dreser A, editors. Estudio sobre la práctica de la atención médica en consultorios médicos adyacentes a farmacias privadas [Study on the practice of medical care in clinics adjacent to private pharmacies]. FUNSALUD; 2014 (in Spanish).
40. Clasificador por funciones de atención [Health care functions classifier]. General Directorate of Health Information, Subsystem of Health Accounts, Ministry of Health (http://www.dgis.salud.gob.mx/contenidos/basesdedatos/da_sicuentas_gobmx.html, accessed 16 October 2017) (in Spanish).
41. OECD, Eurostat and World Health Organization. A System of Health Accounts 2011: revised edition. Paris: OECD Publishing; 2017 (http://www.keepeek.com/Digital-Asset-Management/oecd/social-issues-migration-health/a-system-of-health-accounts-2011_9789264270985-en#page3, accessed 16 October 2017).
42. Paridades de poder de compra [Purchasing power parities]. Instituto Nacional de Geografía y Estadística (INEGI) (http://www3.inegi.org.mx/sistemas/paridades/estructura.aspx?idEstructura=115005800010&T=Paridades%20de%20poder%20de%20compra&ST=Paridades%20de%20poder%20de%20compra&tipoInfo=tipo%20de%20conversi%C3%B3n%20monetaria, accessed 17 October 2017) (in Spanish).
43. Purchasing power parities for GDP. Paris: Organisation for Economic Co-Operation and Development (http://stats.oecd.org/, accessed 17 October 2017).
44. Convenios AFASPE 2009–2017: acuerdos para el Fortalecimiento de Acciones de Salud Pública en las Entidades Federativas (AFASPE), segundo convenio modificatorio 2014 [AFASPE 2009–2017: agreements for the Public Health Actions Strengthening in the States (AFASPE), second modifying agreement 2014]. Subdirectorate for Health Promotion and Disease Prevention, Ministry of Health (http://www.spps.gob.mx/spps/convenios-afaspe.php, accessed 17 October 2017) (in Spanish).
45. Cubo de defunciones [Cube of deaths]. General Directorate of Health Information, Ministry of Health (http://www.dgis.salud.gob.mx/contenidos/basesdedatos/bdc_defunciones_gobmx.html, accessed 17 October 2017) (in Spanish).
46. OECD statistics on health 2014, Mexico in comparison (http://www.oecd.org/els/health-systems/Briefing-Note-MEXICO-2014-in-Spanish.pdf, accessed 17 October 2017).
47. Programa Anual de los Servicios de Salud 2017 [2017 Health Services Programme]. Department of Programming, Organizational Development and Transparency, Ministry of Health, state of Puebla; 2017 (http://www.ss.pue.gob.mx/images/Secretaria_de_Salud/PROGRAMA_ANUAL_DE_LOS_SSEP_2017_INTEGRADO.pdf, accessed 17 October 2017) (in Spanish).
48. Anteproyecto del plan operativo anual 2016 [Pre-project of the annual operation plan 2016]. Directorate of Planning and Development, Ministry of Health, state of Veracruz; 2016 (http://web.ssaver.gob.mx/transparencia/files/2011/10/Anteproyecto-del-POA-2016-Definitivo.pdf, accessed 17 October 2017) (in Spanish).
49. Programa operativo anual presupuestal 2017 [Operative programme budget year 2017]. Ministry of Health, state of Morelos; 2016 (https://www.hacienda.morelos.gob.mx/images/docu_planeacion/transparencia_fiscal/evaluacion_resultados/POAS2017/8.POA_2017_Secretaria_de_Salud.pdf, accessed 17 October 2017) (in Spanish).
50. Programa operativo anual 2016 [Operative programme budget year 2016]. Ministry of Health, state of Tamaulipas; 2016 (http://transparencia.tamaulipas.gob.mx/wp-content/uploads/2016/11/SSTAM-PROGRAMA-OPERATIVO-ANUAL-2016.pdf, accessed 17 October 2017) (in Spanish).
51. Fortalecer la rectoría para construir un sistema de salud centrado en la persona y orientado al uso de la información [Strengthening stewardship to build a person-centred health system oriented towards the use of information]. In: Estudios de la OCDE sobre los sistemas de salud: México [OECD studies on health systems: Mexico]. Paris: Organisation for Economic Co-operation and Development; 2016 (http://dx.doi.org/10.1787/9789264265523–6-es, accessed 17 October 2017) (in Spanish).
38 PRIMARY HEALTH CARE SYSTEMS (PRIMASYS)
52. Acuerdo No. 79 relativo a la aplicación, instrumentación y actualización del manual para la referencia y contrarreferencia de pacientes y envío de muestras y especímenes [Agreement number 79 on the application, instrumentation and update of the patients’ referral and counter-referral and samples and specimen remittance manual]. Official Journal of the Federation, 22 September 1988 (in Spanish).
53. Luo-Che L. Sistema de salud en México: un estudio de referencia y contra referencia en la atención médica en el segundo nivel de atención en el Distrito Federal Hospital General Dr Manuel Gea González [The health system in Mexico: a study on referral and counter-referral in second-level medical care in the Dr Manuel Gea González General Hospital of the Federal District]. Master in Health Sciences thesis. National Autonomous University of Mexico; 2012 (in Spanish).
54. Ley del Seguro Social [Social Security Law]. Mexican Social Security Institute; 1973 (in Spanish).
55. Instrucción 263 de 2010. Programa SICALIDAD: Red Nacional de Aval Ciudadano (RENAC). [Instruction 263 of 2010. SICALIDAD Programme: National Citizen Guarantee Network]. General Directorate of Quality and Health Education, Ministry of Health (http://www.calidad.salud.gob.mx/site/calidad/instruccion/instruccion_263.pdf, accessed 17 October 2017) (in Spanish).
56. Prestación de servicios de salud: definición de un paquete de beneficios equitativo y fortalecimiento de la atención primaria [Health services provision: definition of an equitable benefits package and primary care strengthening]. In: Estudios de la OCDE sobre los sistemas de salud: México [OECD studies on health systems: Mexico]. Paris: Organisation for Economic Co-operation and Development; 2016 (http://dx.doi.org/10.1787/9789264265523–7-es, accessed 17 October 2017) (in Spanish).
57. Soberón Acevedo G. El cambio estructural en la salud. Estructura y funciones de la Secretaría de Salud: del sector salud y del sistema nacional de salud [Structural changes in health. Structure and functions of the Ministry of Health: of the health sector and the national health system]. Salud Pública de México. 1987;127–40 (in Spanish).
58. Reglamento Interior del Consejo de Salubridad General [Internal regulations of the General Health Council]. Official Journal of the Federation, 11 December 2009 (in Spanish).
59. Sistema Nacional de Certificación de Establecimientos de Atención Médica: estándares para la certificación de clínicas de atención primaria y consulta de especialidades [National System for the Certification of Medical Establishments: standards for the certification of primary care clinics and specialties offices]. General Health Council; 2015 (in Spanish).
60. Consejo Nacional de Salud [National Health Council]. Ministry of Health; 2017 (http://www.cns.salud.gob.mx/contenidos/1_informaciongeneral.html, accessed 17 October 2017) (in Spanish).
61. Manual de organización de las subdelegaciones del IMSS [IMSS subdelegations organization manual] (http://www.imss.gob.mx/sites/all/statics/pdf/manualesynormas/9000–002–002.pdf, accessed 17 October 2017) (in Spanish).
62. Reglamento de las delegaciones del Instituto de Seguridad y Servicios Sociales de los Trabajadores del Estado [Regulations of the delegations of the Institute of Security and Social Services of the State Workers] (http://www.ordenjuridico.gob.mx/Publicaciones/pdf/R118.pdf, accessed 17 October 2017) (in Spanish).
63. Ruelas-Barajas E. La Cruzada Nacional por la Calidad de los Servicios de Salud: una estrategia de gran escala [The National Crusade for Quality of Health Services: a large-scale strategy]. In: La calidad de la atención a la salud en México a través de sus instituciones: 12 años de experiencia [Quality of health care in Mexico throughout its institutions: 12 years’ experience]. Ministry of Health; 2012 (in Spanish).
64. CENETEC. Catalogo maestro de guías de práctica clínica [Master clinical practice guides catalogue]. Ministry of Health; 2017 (in Spanish).
65. Plan Nacional de Desarrollo 2013–2018 [National Development Plan 2013–2018]. Government of Mexico; 2013 (http://www.cmic.org.mx/comisiones/sectoriales/infraestructurahidraulica/PND_PLAN_NAL_DESARR/PND-introduccion.pdf, accessed 17 October 2017) (in Spanish).
66. Joft MV, Kumate J, Barnard A. La atención primaria de salud como instrumento desarrollo en México [Primary health care as an instrument for development in Mexico]. Salud Pública de México. 1989;31:177–84 (in Spanish).
67. Valencia CJ, José MV, Olvera J, Serrano O, Mhrquez A. Regionalización de México basada en indicadores de atención primaria a la salud [Regional division of Mexico according to primary health care indicators proposed by WHO]. Salud Pública de México. 1991;33:29–37 (in Spanish).
68. Tapia-Conyer R, Kuri-Morales P, González-Urbán L, Sarti E. Evaluation and reform of Mexican National Epidemiological Surveillance System. American Journal of Public Health. 2001;91(11):1758–60.
69. Tapia-Conyer R. Una visión crítica sobre la salud pública en México [A critical vision of public health in Mexico]. Gaceta Médica de México. 2016;152:278–84 (http://www.anmm.org.mx/GMM/2016/n2/GMM_152_2016_2_278–284.pdf, accessed 17 October 2017) (in Spanish).
39CASE STUDY FROM MEXICO
70. Sepúlveda J, Tapia-Conyer R et al. Diseño y metodología de la Encuesta Nacional de Salud 2000 [National Health Survey 2000: design and methodology]. Salud Pública de México. 2007;49:Suppl 3 (in Spanish).
71. Manual de indicadores de servicios de salud [Health services indicators manual]. Ministry of Health (http://www.dged.salud.gob.mx/contenidos/dess/descargas/ind_hosp/Manual-ih.pdf, accessed 17 October 2017) (in Spanish).
72. Fichas técnicas para la construcción de los indicadores de resultado [Technical notes for the construction of results indicators]. General Directorate of Performance Evaluation, Ministry of Health; 2014. http://www.gob.mx/cms/uploads/attachment/file/56515/Fichas.pdf, accessed 17 October 2017) (in Spanish).
73. Gutiérrez-Alba G, González-Block MA, Reyes-Morales H. Desafíos en la implantación de guías de práctica clínica en instituciones públicas de México: estudio de casos multiple [Challenges in the implementation of clinical practice guidelines in major public health institutions in Mexico: A multiple case study]. Salud Pública de México. 2015;57:547–54 (in Spanish).
74. Evaluación de la difusión e implementación de las guías de práctica clínica [Assessment of the diffusion and implementation of clinical practice guides]. Mexico DF: Arapau and Associates. Ministry of Health; 2012 (in Spanish).
75. Poblano-Verástegui O, Vieyra-Romero WI, Galván-García AF, Fernández-Elorriaga M, Rodríguez-Martínez AI, Saturno-Hernández PJ. Calidad y cumplimiento de guías de práctica clínica de enfermedades crónicas no transmisibles en el primer nivel [Quality and compliance with clinical practice guidelines of chronic noncommunicable diseases in primary care]. Salud Pública de México. 2017;59:165–75 (http://www.saludpublica.mx/index.php/spm/article/view/8285, accessed 17 October 2017) (in Spanish).
76. Saturno PJ, Agüero L, Fernández M, Galván A, Poblano O, Rodriguez AL et al. Evaluación de guías de práctica clínica para el primer nivel de atención: calidad formal y apego a las guías de práctica [Assessment of the clinical practice guides for the first level of care: formal quality and adherence to the practice guides]. National Institute of Public Health; 2015 (in Spanish).
77. Encuesta Nacional de Salud y Nutrición de Medio Camino 2016 (ENSANUT MC 2016): informe final de resultados [Midterm National Health and Nutrition Survey 2016 (ENSANUT MC 2016): final results report]. National Institute of Public Health, Ministry of Health; 2016 (in Spanish).


World Health Organization
Avenue Appia 20CH-1211 Genève [email protected]://www.who.int/alliance-hpsr
This case study was developed by the Alliance for Health Policy and Systems Research, an international partnership hosted by the World Health Organization, as part of the Primary Health Care Systems (PRIMASYS) initiative. PRIMASYS is funded by the Bill & Melinda Gates Foundation, and aims to advance the science of primary health care in low- and middle-income countries in order to support efforts to strengthen primary health care systems and improve the implementation, effectiveness and efficiency of primary health care interventions worldwide. The PRIMASYS case studies cover key aspects of primary health care systems, including policy development and implementation, financing, integration of primary health care into comprehensive health systems, scope, quality and coverage of care, governance and organization, and monitoring and evaluation of system performance. The Alliance has developed full and abridged versions of the 20 PRIMASYS case studies. The abridged version provides an overview of the primary health care system, tailored to a primary audience of policy-makers and global health stakeholders interested in understanding the key entry points to strengthen primary health care systems. The comprehensive case study provides an in-depth assessment of the system for an audience of researchers and stakeholders who wish to gain deeper insight into the determinants and performance of primary health care systems in selected low- and middle-income countries.