Embed Size (px)
Citation preview
Stroke Guidelines
November 19, 2011
Clinical Practice Guidelines
American Stroke Association Guidelines are comprehensive statements that provide
the highest level of scientific evidence for clinical practice. The 6 flagship or core Guidelines of the Stroke Council are: – Primary Prevention of Stroke (2010) – Prevention of Stroke in Patients with Stroke or TIA (2010) – Early Management of Acute Ischemic Stroke (2007) – Management of Spontaneous Intracerebral Hemorrhage (2010) – Management of Subarachnoid Hemorrhage (2009) – Stroke Rehabilitation (2005)
Clinical Practice Guidelines • Panel of physicians
– Vascular neurology
– Neurocritical care
– Emergency medicine
– Neurosurgery
– Interventional neuroradiology/endovascular neurosurgery
• Goal: Provide updated recommendations for care w/i first hours of stroke
Protocols/Order Sets
Acute Evaluation Orders
Stroke Alert Process Document
Thromoblytic Orders
tPA Monitoring Protocol
Admission Orders
Discharge Orders NIHSS/tPA Comm form
• Dysphagia Screen
• DVT Prophylaxis
• Insulin Orders
• Interdisciplinary Plan of Care
Prehospital Management & Field Treatment • Use of 911 system supported to speed access to stroke tx • Stroke should be a priority dispatch • Public awareness campaigns needed to increase pts who can be
treated within time window • Education programs for physicians, hospital personnel and EMS
personnel to increase pts who are treated • Brief but standardized EMS assessments to identify stroke • Begin stroke management in field with use of protocols • Rapid transport to nearest appropriate facility • Telemedicine may facilitate stroke evaluation and treatment
– Use where lack of expertise prevents access to PSC for tPA eligibility
– Providers w/ stroke expertise, response time targets, plan for pts disposition
– Users provide emergency diagnosis & treatment as defined for PSCs
Stroke Center Certification • Primary Stroke Center development strongly recommended
– Comprehensive stroke center
• External certification
• EMS should bypass hospitals w/o stroke resources to closest treating stroke facility for suspected stroke patients
Emergency Evaluation and Diagnosis
• Organized protocol for the emergency evaluation of patients with suspected stroke
– Goal to complete evaluation and decide treatment within 60 minutes of arrival
– Designate an acute stroke team that includes physicians, nurses, and laboratory/ radiology personnel
• Stroke rating scale is recommended
– NIHSS
• Limited number of hematologic, coagulation, and biochemistry tests during the initial emergency evaluation
• Chest x-ray for selected patients
– Acute cardiac or pulmonary disease
• EKG
Early Diagnosis: Brain and Vascular Imaging • Brain imaging prior to any specific stroke treatment
– CT adequate in most instances
– Should be interpreted by physician w/ appropriate expertise
– Some findings may be associated w/ poor outcome after stroke
– Advanced imaging may help with stroke diagnosis
– Except for evidence of hemorrhage, no finding should preclude IV tPA tx w/i 3 hr window
– Additional imaging needed for IA tap, surgical procedures or endovascular intervention
– Advanced imaging should not delay tx w/ IV tPA for eligible pts
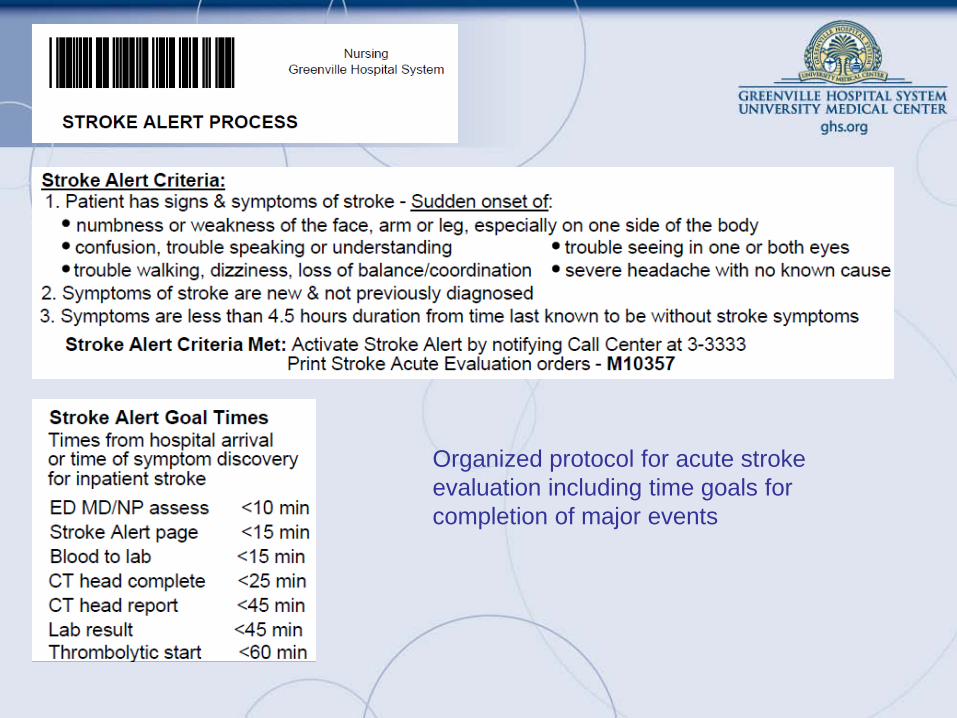
Organized protocol for acute stroke evaluation including time goals for completion of major events
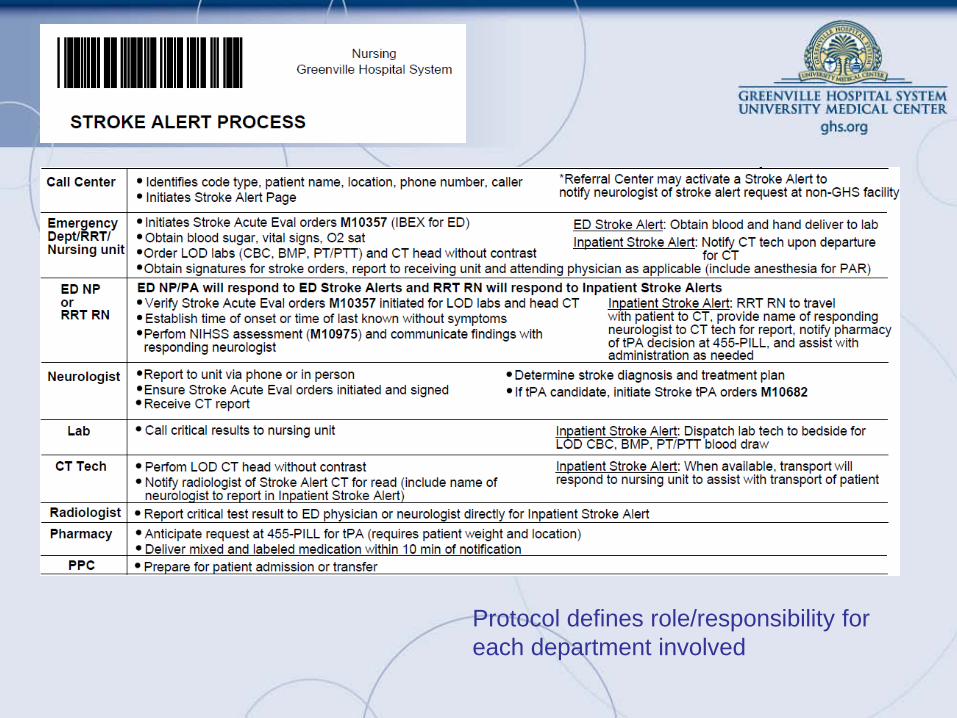
Protocol defines role/responsibility for each department involved
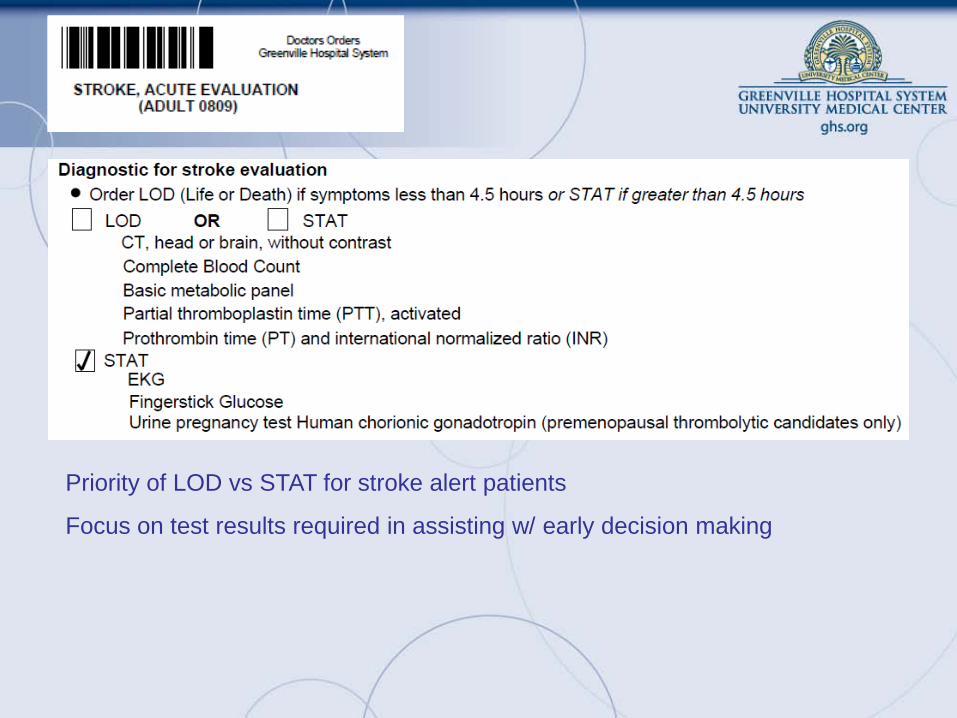
Priority of LOD vs STAT for stroke alert patients
Focus on test results required in assisting w/ early decision making
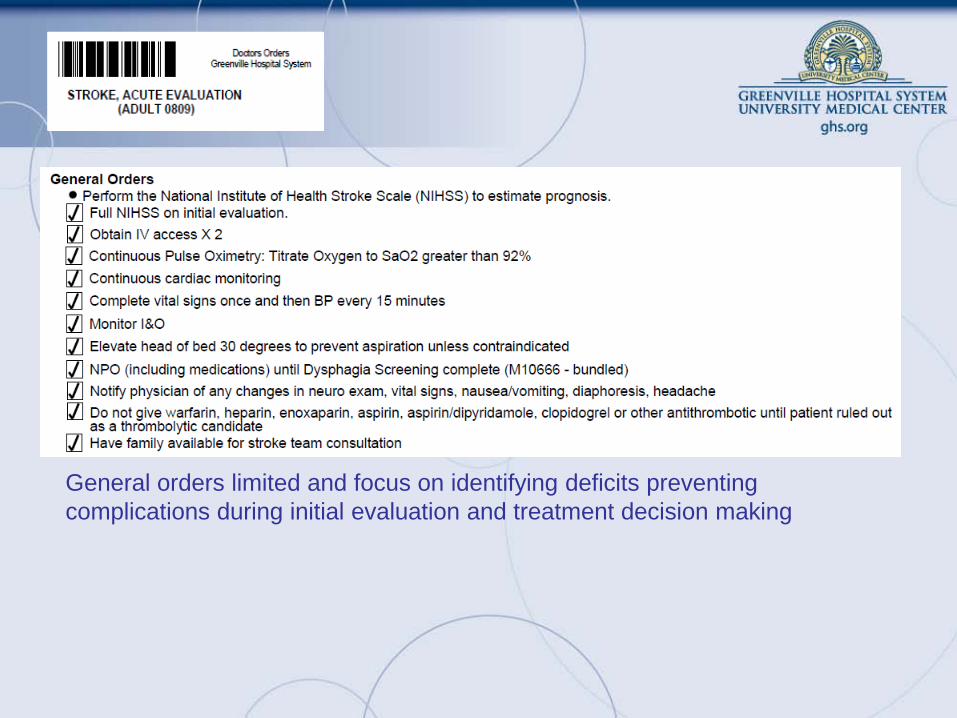
General orders limited and focus on identifying deficits preventing complications during initial evaluation and treatment decision making
Intravenous Thrombolysis • IV tPA is recommended for selected pts w/i 3 hr of stroke onset
• Criteria for eligibility used to determine appropriate candidates
• Monitoring after treatment should follow recommended regimen
• Monitoring for sx of hemorrhage and angioedema required
• BP responsive to treatment may not exclude IV tPA administration
• Seizure may not exclude patient from IV tPA tx if physician convinced symptoms related to stroke
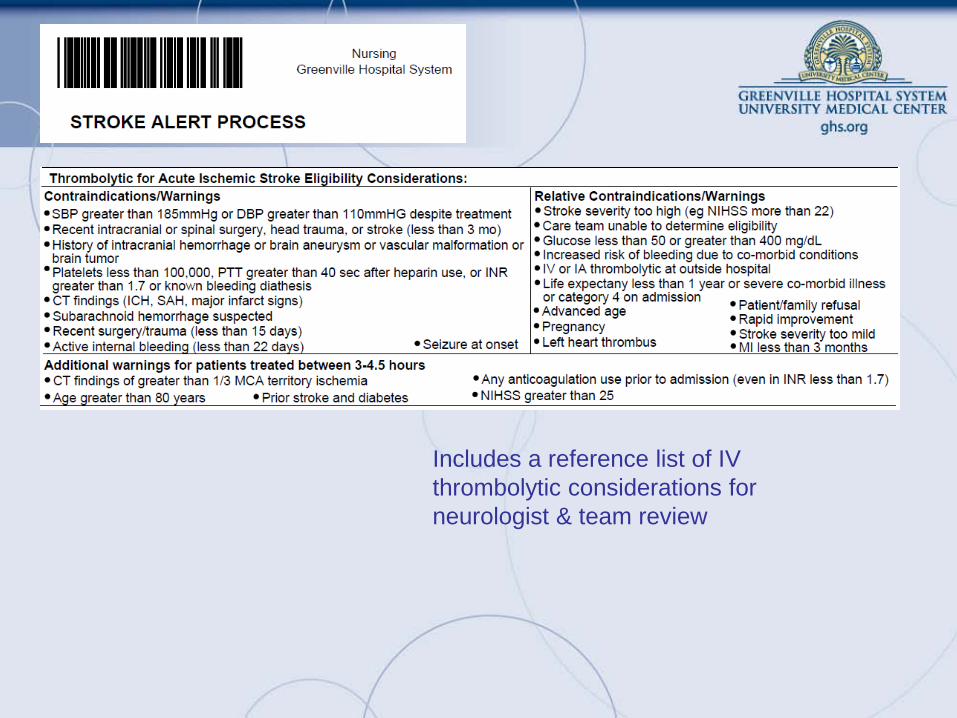
Includes a reference list of IV thrombolytic considerations for neurologist & team review
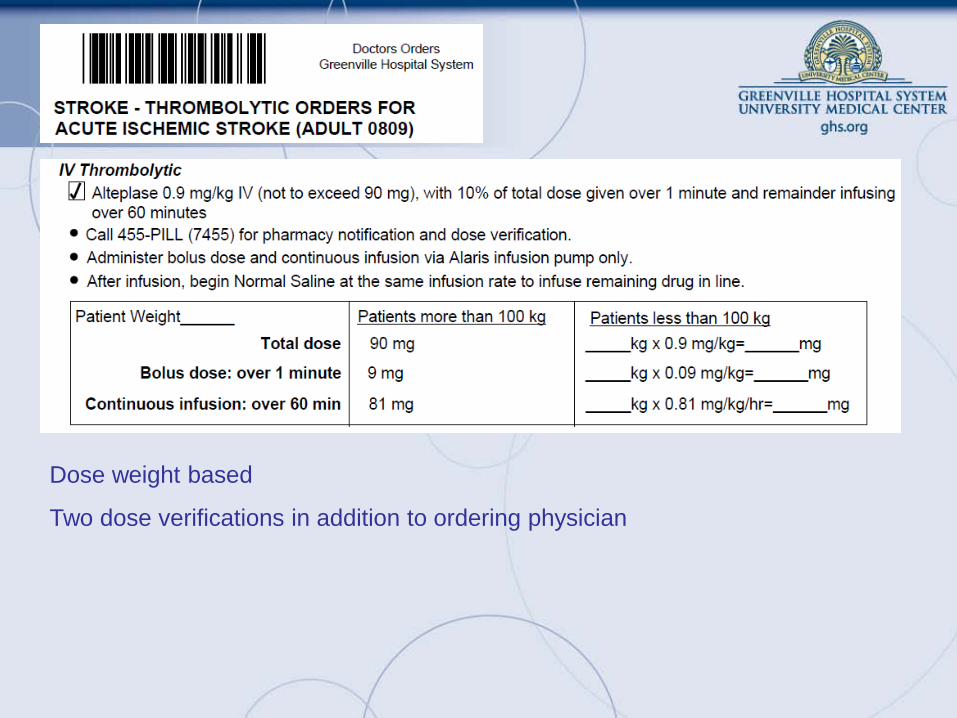
Dose weight based
Two dose verifications in addition to ordering physician
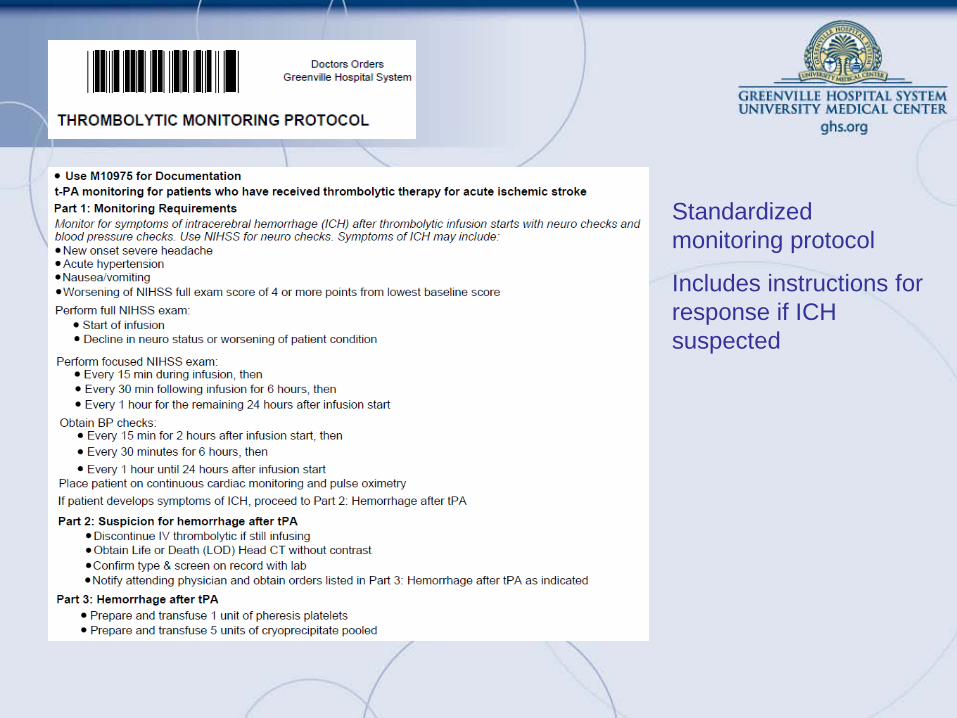
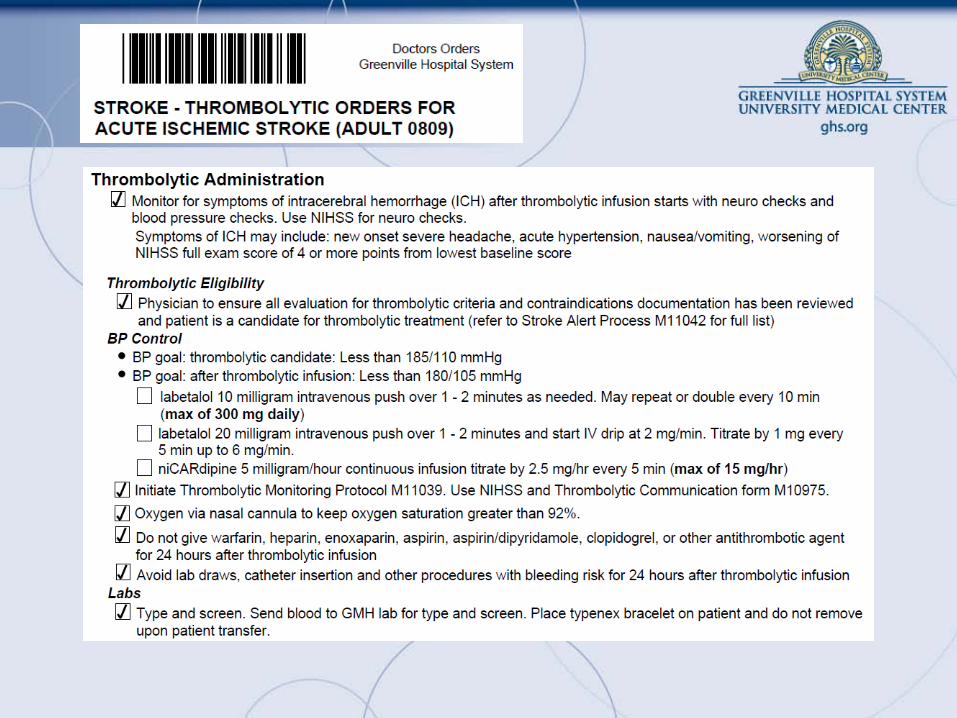
Standardized monitoring protocol
Includes instructions for response if ICH suspected
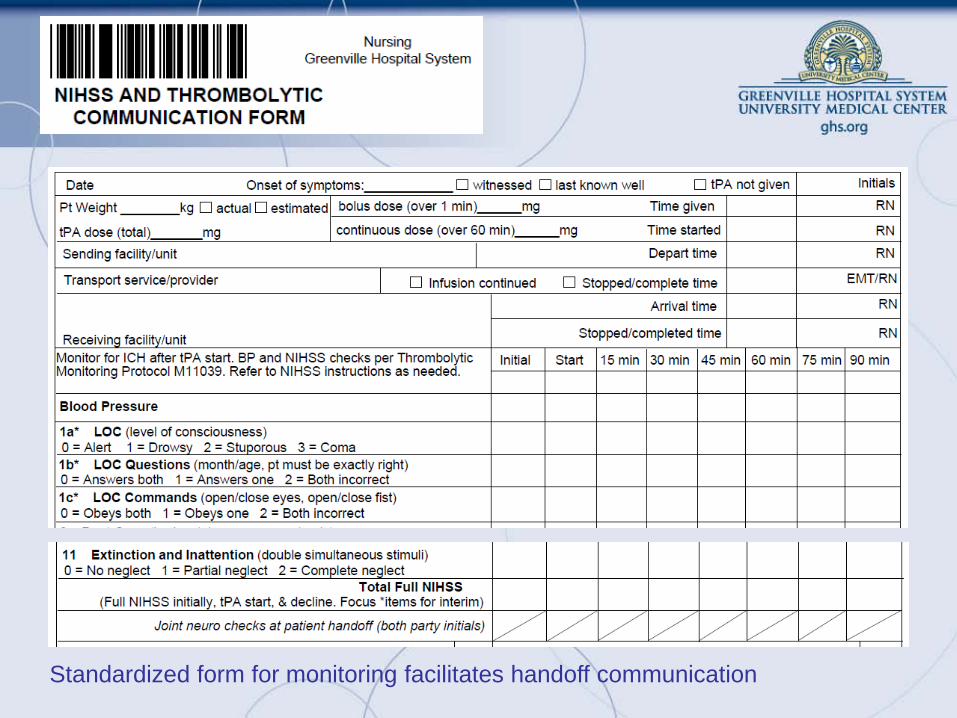
Standardized form for monitoring facilitates handoff communication
Intra-Arterial Thrombolysis • IA thrombolysis an option for selected patients
– < 6 hrs of onset
– MCA occlusion
– Not otherwise eligible for IV tPA
• Requires access to experienced stroke center
– Angiography
– Qualified interventionalists
• Availability should not preclude IV tap tx for eligible pts
General Supportive Care & Treatment of Acute Complications
• Airway & vent support for pts w/ decreased LOC or airway compromise
• O2 for hypoxia
• Treat & avoid fever
• Cardiac monitoring for a-fib & other arrhythmias for at least 24 hrs
• Goal for normoglycemia
– Treat hypoglycemia
– Hyperglycemia during 1st 2r hrs associated w/ poor outcomes
– Treat at >140 to 185 mg/dL
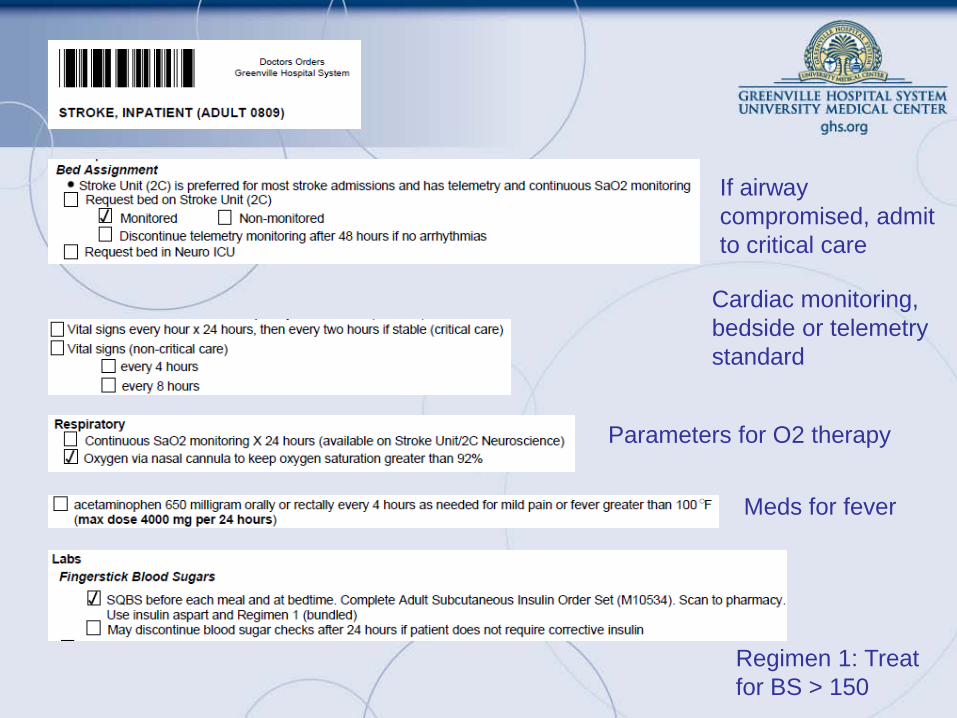
If airway compromised, admit to critical care
Parameters for O2 therapy
Meds for fever
Regimen 1: Treat for BS > 150
Cardiac monitoring, bedside or telemetry standard
General Supportive Care & Treatment of Acute Complications
• Cautious management of hypertension
– May spontaneously decline w/i first 24 hrs of stroke onset
– Treat if other medical indications
– If eligible for IV tPA treat to goal of <185/110 before tx and then maintain <180/105 for 24 hrs after
– Same BP parameters for IA tPA
– Reasonable goal to lower by 15% in first 24 hrs of stroke if markedly elevated (i.e. SBP >220 or DBP >120
– Suggested meds include
• Labetalol 10 to 20 mg IV over 1 to 2 minutes, may repeat 1 • Nitropaste 1 to 2 inches • Nicardipine infusion, 5 mg/h, titrate up by 2.5 mg/h at 5- to 15-minute
intervals, maximum dose 15 mg/h; when desired blood pressure attained, reduce to 3 mg/h
General Supportive Care & Treatment of Acute Complications
– Antihypertensive meds may be restarted at 24 hr if preexisting hypertension and neurologically stable unless otherwise contraindicated
– Avoid hypotension by correcting hypovolemia and treating cardiac arrhythmias that may reduce cardiac output
• Hyperbaric oxygen not recommended except for cause due to air embolism
• Hypothermia for stroke w/o sufficient evidence for recommendation
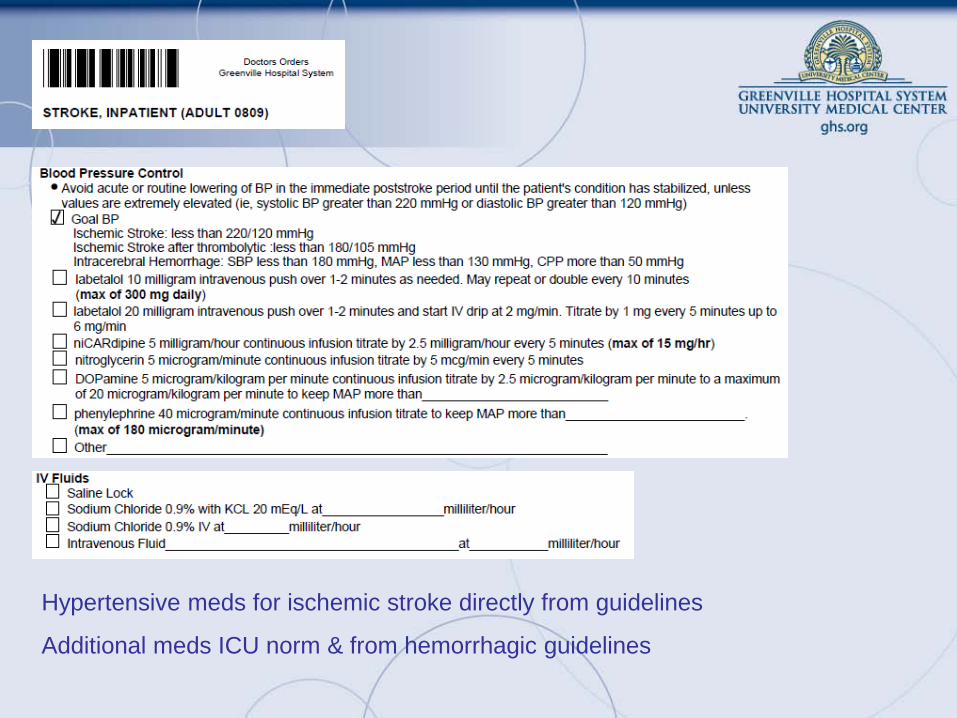
Hypertensive meds for ischemic stroke directly from guidelines
Additional meds ICU norm & from hemorrhagic guidelines
Anticoagulants • Urgent anticoagulation not recommended to:
– prevent early recurrent stroke – halt neurologic worsening – improve outcome after AIS
• Not recommended in lieu of IV tap for otherwise eligible pts
• Not recommended for moderate to severe strokes due to risk of ICH
• Anticoagulation w/i 24 hrs after IV tPA not recommended
Antiplatelet Agents • ASA 325 mg w/i 24-48 hrs recommended for most pts • ASA not a substitute for other acute interventions including IV tap • ASA in addition to IV tPA not recommended in 1st 24 hrs • Clopidogrel alone or w/ ASA not rec for AIS treatment • IV antiplatelent agents to inhibit gpIIb/IIIa not recommended outside of
clinical trials
Antiplatelet Agents Secondary stroke prevention
• Non-cardioembolic IS or TIA use antiplatelet instead of oral anticoagulants
• Options for initial therapy include:
– ASA 50-325mg
– ASA+ER dipyridamole 200 mg BID
– Clopidogrel 75mg
• ASA + Clopidogrel increases risk of hemorrhage, routine use for secondary prevention not recommended
(Guidelines for the Prevention of Stroke in Patients With Stroke or Transient, Stroke 2011)
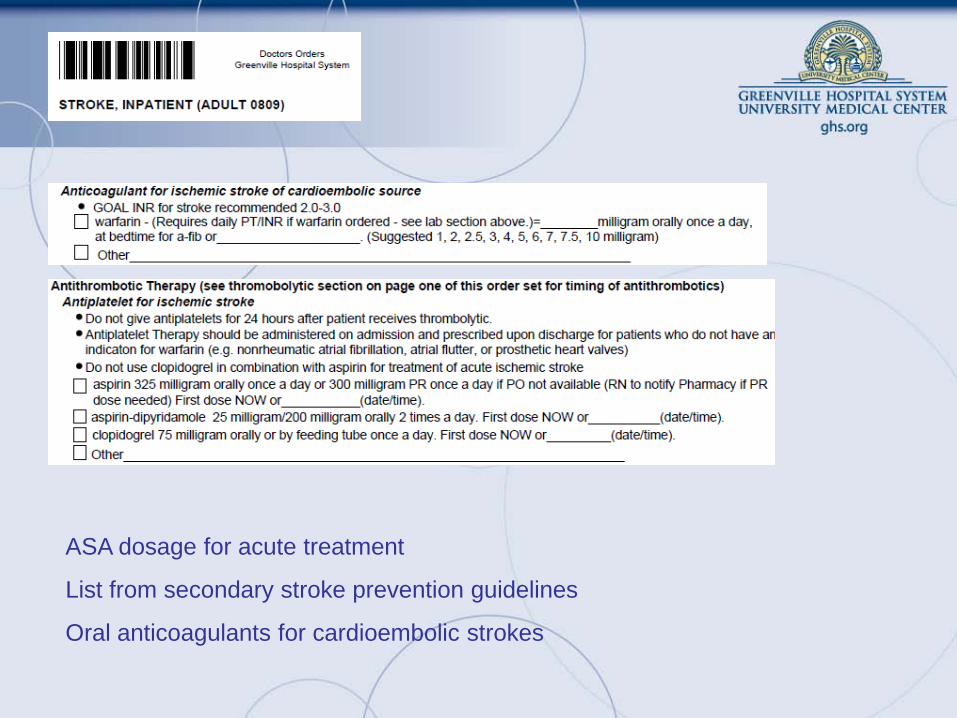
ASA dosage for acute treatment
List from secondary stroke prevention guidelines
Oral anticoagulants for cardioembolic strokes
Induced Hypertension for the Management of AIS • Drug-induced hypertension may be prescribed in exceptional cases
– Use of neuro & cardiac monitoring needed
– Not recommended outside of clinical trials for most patients
• Data on the safety and effectiveness of carotid endarterectomy and other operations for treatment of patients with acute ischemic stroke are not sufficient to permit a recommendation.
• Surgical procedures may have serious risks and may not favorably alter the outcome of the patient.
Surgical Interventions
Endovascular Interventions • Although the MERCI device is a reasonable intervention for
extraction of intra-arterial thrombi in carefully selected patients, the panel also recognizes that the utility of the device in improving outcomes after stroke is unclear (Class IIb, Level of Evidence B).
– The panel also recommends that the device be studied in additional clinical trials that will define its role in the emergency management of stroke.
• The usefulness of other mechanical endovascular treatments is not established (Class IIb, Level of Evidence C). – These devices should be used in the setting of clinical trials.
Combination Reperfusion Therapy in Acute Stroke • At present, combinations of interventions to restore perfusion cannot
be recommended outside the setting of clinical trials (Class III, Level of Evidence B).
• At present, no intervention with putative neuroprotective actions has been established as effective in improving outcomes after stroke, and therefore none currently can be recommended (Class III, Level of Evidence A).
Neuroprotective Agents
Admission to the Hospital and General Acute Treatment • Stroke order sets • Stroke units recommended
– Comprehensive specialized stroke care – Incorporation of rehabilitation – Early mobilization
• Swallow assessment before any PO – Alternate nutrition/hydration via feeding tube while efforts to
restore swallowing – Nutritional supplements not needed
• Measures to prevent & treat pneumonia or UTI – Prophylactic antibiotics not recommended – Avoid indwelling catheters when possible
Admission to the Hospital and General Acute Treatment • DVT prophlyaxis w/ SQ anticoagulants for immobilized pts
• ASA less effective than anticoagulants
• Intermittent external compression devices recommende for those who cannot receive anticoagulants
• Treatment/management of other medical issues
• Early interventions to prevent recurrent stroke
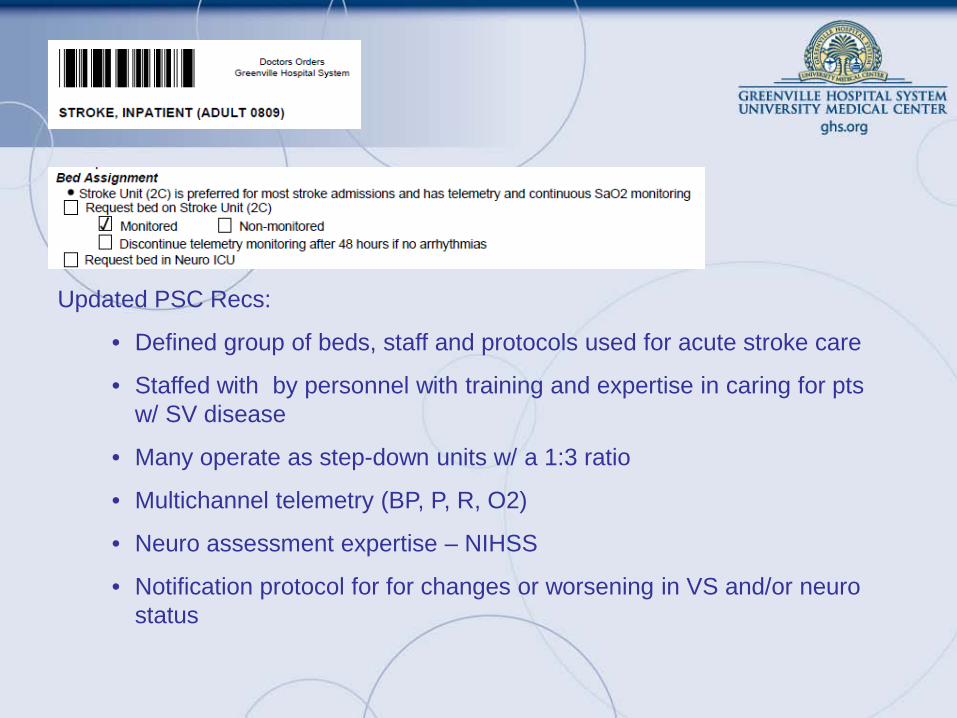
Updated PSC Recs:
• Defined group of beds, staff and protocols used for acute stroke care
• Staffed with by personnel with training and expertise in caring for pts w/ SV disease
• Many operate as step-down units w/ a 1:3 ratio
• Multichannel telemetry (BP, P, R, O2)
• Neuro assessment expertise – NIHSS
• Notification protocol for for changes or worsening in VS and/or neuro status
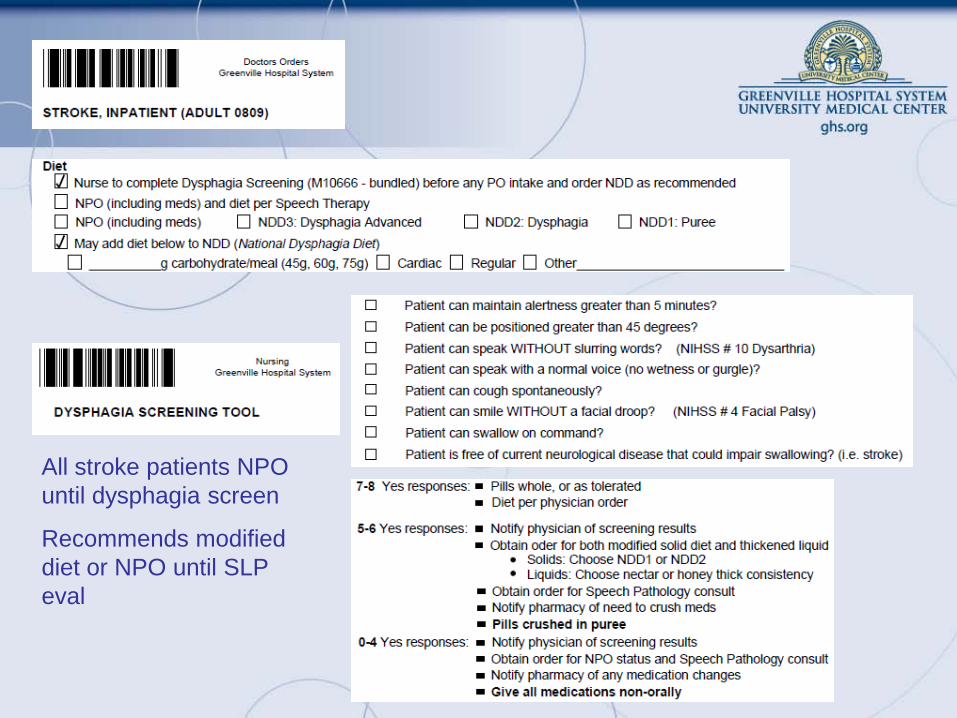
All stroke patients NPO until dysphagia screen
Recommends modified diet or NPO until SLP eval
Treatment of Acute Neurological Complications • Major infarctions higher risk for cerebral edema and increased ICP
– Measures to decrease risk and monitor for neuro worsening recommended
• Hydrocephalus secondary to IS affecting cerebellum can be treated w/ ventricular drain
• Surgical decompression for cerebellar infarction
• Recurrent seizures should be treated
• Osmotherapy & hyperventilation unproven and may delay decompressive surgery.
• Decompressive surgery for malignant edema of the cerebral hemisphere may be life-saving, but the impact of morbidity is unknown
• Both the age of the patient and the side of the infarction (dominant versus nondominant hemisphere) may affect decisions about surgery.
Treatment of Acute Neurological Complications • No specific recommendation is made for treatment of patients with
asymptomatic hemorrhagic transformation after ischemic stroke
– Treatment of symptomatic hemorrhagic transformation is addressed in the intracerebral hemorrhage management guideline being issued contemporaneously with this statement
– Measures to lessen the likelihood of hemorrhagic complications of thrombolytic agents or other interventions to restore or improve perfusion such as careful control of arterial blood pressure are recommended.
• Corticosteroids are not recommended for treatment of cerebral edema and increased intracranial pressure
• Prophylactic administration of anticonvulsants to patients with stroke but who have not had seizures is not recommended
Palliative Care
• The family should be given the opportunity to select or withhold medical interventions. In such situation, the medical care may emphasize measures to keep the patient comfortable and to support the family during the terminal aspects of the stroke.





























