-
7/24/2019 teori lapmat
1/9
Hindawi Publishing CorporationBioMed Research
InternationalVolume , Article ID ,pageshttp://dx.doi.org/.//
Review ArticleAlbumin Reduces Paracentesis-Induced Circulatory
Dysfunctionand Reduces Death and Renal Impairment among Patients
withCirrhosis and Infection: A Systematic Review and
Meta-Analysis
Chun Shing Kwok,1 Lukasz Krupa,1Ash Mahtani,2 Duncan Kaye,2
Simon M. Rushbrook,1
Martin G. Phillips,1 and William Gelson1
Norfolk and Norwich University Hospital, Colney Lane, Norwich NR
UY, UK Norwich Medical School, University of East Anglia, Norwich
NR J, UK
Correspondence should be addressed to William Gelson;
[email protected]
Received April ; Revised July ; Accepted August
Academic Editor: Ahmed Abdel-Lati
Copyright Chun Shing Kwok et al. Tis is an open access article
distributed under the Creative Commons AttributionLicense, which
permits unrestricted use, distribution, and reproduction in any
medium, provided the original work is properlycited.
Background.Studies have suggested that albumin has a value in
cirrhotic patients undergoing paracentesis but its value in
inectionand sepsis is less clear. We planned to perorm a
meta-analysis o the risk o adverse outcomes in cirrhotic patients
with andwithout albumin use.Methods.We searched MEDLINE and EMBASE
in January or randomized studies o cirrhotic patientsthat reported
the risk o adverse events and mortality with albumin and no albumin
exposure. We perormed random effectsmeta-analysis and assessed
heterogeneity using theI2 statistic.Results.Our review included
studies covering , patients. Teuse o albumin in paracentesis was
associated with signicantly reduced risk o paracentesis-induced
circulatory dysunction (OR. %, CI ..) and there was a nonsignicant
difference in death, encephalopathy, hyponatraemia, readmission,
and renalimpairment. Comparedto the other volume expanders, albumin
use showed no difference in clinical outcomes. In cirrhotic
patientswith any inection, there was a signicant reductionin
mortality (OR .%, CI ..) andrenal impairment (OR .%,CI ..) when
albumin was used. Conclusion. Te use o albumin in cirrhotic
patients is valuable in patients with any inectionand it reduces
the risk o circulatory dysunction among patients undergoing
paracentesis.
1. Introduction
Intravenous administration o human albumin solution is
requently used in patients with decompensated liver cir-rhosis
during the drainage o ascites. In the absence ointravenous albumin,
postparacentesis circulatory dysunc-tion occurs in approximately %
o patients [, ] and isassociated with increased mortality because o
hepatorenalsyndrome and dilutional hyponatraemia [,]. In
addition,albumin administration is recommended in patients
withspontaneous bacterial peritonitis (SBP) [,].
Albumin is a plasma expander that increases car-diac preload and
peripheral vascular resistance, attenuatesendothelial dysunction,
reduces renal ailure, and improvessurvival [, ]. As a result,
albumin is widely accepted asa therapy in large volume paracentesis
and spontaneous
bacterial peritonitis, but the evidence supporting this
therapyin other settings is less clear.
Bacterial inections are common in patients with
advanced cirrhosis and are a major cause o hospitaladmissions
and mortality []. Approximately % ocirrhotic patients with severe
inection develop renal ailureand this is a poor prognostic actor
[]. Te inectionthat most ofen causes renal ailure is spontaneous
bacterialperitonitis, ollowed by urinary tract inection and
cellulitis.
Few data exist regarding the effect o albumin adminis-tration in
patients with non-SBP inections. Te question owhether albumin
inusion also improves outcome in patientswith bacterial inections
otherthan SBP remains unanswered.Studies to date ailed to answer
this question due to smallsample size [] and urther research should
be perormed toanswer this question.
-
7/24/2019 teori lapmat
2/9
BioMed Research International
In this systematic review, we provide a comprehensiveand
up-to-date overview o the existing evidence regardingthe use o
albumin in cirrhotic patients. We were speci-cally interested in
three questions. Is albumin benecial incirrhotic patients
undergoing large volume paracentesis? Isalbumin useul in cirrhotic
patients with inections, with
particular ocus on SBP and non-SBP inections? Is albuminsuperior
to other volume expanders in cirrhotic patients?
2. Methods
.. Eligibility Criteria. We selected randomized controlledtrials
(RCs) that evaluated the use o human serum albuminin patients with
cirrhosis. Te specic inclusion criteria orthe studies were ()
parallel group randomized trial withalbumin in one o the treatment
arms or any duration otherapy; () placebo or alternative control
arm; () clearreporting o adverse events. Te adverse events o
interestwere death, encephalopathy, hyponatraemia,
paracentesis-
induced circulatory dysunction, readmission, renal impair-ment,
gastrointestinal bleeding, inection resolution, andsepsis/severe
inection. Tere was no restriction on cirrhoticpatients and those
with tense ascites requiring paracentesis,and those with inections
including SBP were included.
.. Search Strategy. We searched MEDLINE and EMBASEthrough OvidSP
in January using the Haynes opti-mized search strategy (Health
Inormation Research Unit,McMaster University) (see Supplementary
Material avail-able online athttp://dx.doi.org/.//) []. Wealso
checked the bibliographies o the included trials and
recent review articles or relevant studies.
.. Study Selection and Data Extraction. One reviewer(Chun Shing
Kwok) and one o two other reviewers (AshMahtani or Duncan Kaye)
independently scanned all titlesand abstracts or studies that met
the inclusion criteria andexcluded any articles that clearly did
not ull the selectioncriteria. Full reports o potentially relevant
trials and studieswere retrieved and independently checked by two
reviewers(Lukasz Krupa and William Gelson). We then
independentlycollected inormation on study design, drug exposure,
studylocation, characteristics o participants, and relevant
out-comes onto a spreadsheet (Chun Shing Kwok, Ash Mahtani,
and Duncan Kaye). Where there was any uncertainty
ordiscrepancies, the article was discussed between the
reviewers(Lukasz Krupa, Simon M. Rushbrook, Martin G. Phillips,and
William Gelson) to determine i the studies should beincluded. We
also contacted authors i there were any areasthat required
clarication.
.. Risk of Bias Assessment. We evaluated the quality ostudies in
accordance with the recommendations o theCochrane Handbook and this
assessment included sequencegeneration, allocation concealment,
blinding o participant,personnel and outcome assessors, incomplete
outcome data,
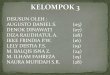
Articles retrieved
rom PubMed
Articles selected afer screening o title and
Articles excluded afer detailed screening to
16 different articles selected or inclusion in
the meta-analysis
Articles retrieved
rom Embase search
search (N = 223)
abstract (N = 74)
specic criteria (N = 39)
(N = 500)
F : Flow diagram o the process o article selection or
meta-analysis.
selective reporting, and baseline differences in
participants[].
We aimed to generate unnel plots to assess the possibilityo
publication bias, provided that there were > studiesavailable in
the meta-analysis, with no evidence o substantialstatistical
heterogeneity.
.. Data Analysis. We used RevMan . (NordicCochrane Centre) to
conduct random effects meta-analysisusing pooled odds ratios (OR).
We chose to pool rawoutcome data to yield unadjusted risk ratios
(which maybe particularly susceptible to conounding). In view o
thepotential diversity o study participants and interventions,we
chose to perorm sensitivity analysis based on groupings:
() cirrhotic patients receiving paracentesis,
() cirrhotic patients receiving albumin compared toother volume
expanders,
() cirrhotic patients with inections, SBP, and
non-SBPinections.
.. Statistical Heterogeneity. Statistical heterogeneity was
assessed using 2 statistic, with 2 values o % repre-senting a
moderate level o heterogeneity [].
3. Results
Te search results yielded relevant RCs with , patientsrom Egypt,
France, Korea, Argentina, Mexico, Spain, USA,Italy, andChina. Four
studies [, , , ] evaluated albumin
versus no albumin/saline, and eight studies [, , , ,
-
7/24/2019 teori lapmat
3/9
BioMed Research International
: Study design, patient characteristics and selection
criteria.
Study Design; year o study;
country Number o participants
Meanage
Male%
Selection criteria
Abdel-Khalek andAri []
Randomized trial; Apr to Feb ; Egypt.
; albumin; hydroxyethyl starch.
Patients with cirrhosis and tenseascites which were unresponsive
tolow-sodium diet and diuretic therapy.
Altman et al. []
Randomized trial; uncleardates; France.
; albumin; hydroxyethyl starch.
Patients with cirrhosis and tense
ascites.
Choi et al. [] Randomized trial; Jun
to Feb ; Korea.; albumin; noalbumin.
Patients with cirrhosis and
spontaneous bacterial peritonitis.
Fassio et al. []Randomized trial; Apr to Mar ; Argentina.
; albumin ; dextran-.
Patients with cirrhosis and tense
ascites.
Garcia-Compeanet al. []
Randomized trial; uncleardates; Mexico.
; albumin; noalbumin.
Patients with cirrhosis and tense
ascites.
Garca-Compeanet al. []
Randomized trial; uncleardates; France.
; albumin ; dextran-.
Patients with cirrhosis and tense
ascites.
Gines et al. [] Randomized trial; Jul to
Dec , Spain.; albumin; noalbumin.
Patients with cirrhosis and tense
ascites.
Gines et al. [] Randomized trial; uncleardates, Spain.
; albumin ;dextran- ; polygeline.
Patients with cirrhosis and tenseascites.
Guevara et al. []
Randomized trial; uncleardates; Spain.
; albumin andantibiotics; antibiotics.
Patients with cirrhosis andnon-spontaneous bacterial
peritonitisinections.
Moreau et al. []
Randomized pilot study;May Jun ; France.
; albumin; polygeline.
Patients with cirrhosis and ascites whoneeded to receive a
plasma expanderbecause o paracentesis, renalimpairment or marked
hyponatraemia.
Nazar et al. []Randomized trial; uncleardates; Spain.
; albumin andantibiotics; antibiotics.
NA NA Patients with cirrhosis and non-SBP
inections.
Planas et al. [] Randomized trial; USA. ; albumin;
dextran-.
Patients with cirrhosis and tenseascites treated with
paracentesis.
Salemo [] Randomized trial; MayJuly ; Italy.
; albumin; hemaccel.
Patients with cirrhosis and reractoryascites.
Sola-Vera et al. []
Randomized trial; JanDec ; Spain.
; albumin; saline. Patients with cirrhosis and tense
ascites.
Sort et al. [] Randomized trial; Nov
Sept ; Spain.; ceotaxime andalbumin; ceotaxime.
Patients with cirrhosis and
spontaneous bacterial peritonitis.
Xue et al. [] Randomized trial; unclear
dates; China.; albumin andcefriaxone; cefriaxone.
NA NA Patients with cirrhosis, ascites and
spontaneous bacterial peritonitis.
NA: not available.
,,,] compared plasma expander to albumin. Fourother studies [,,]
o cirrhotic patients with inection
compared the use o antibiotics with and without albumin.Study
durations varied rom days to months. Te processo selection is shown
in Figureand the main characteristicso the included studies are
described in able . Te outcomes,interventions,and quality
assessments o the included studiesare shown in ableand
Supplementary Material .
For methodological quality assessment, the majority otrials (
trials) had adequate sequence generation or ran-domization but only
two trials had adequate allocation con-cealment (Supplementary
Material ). Blinding o patients,personnel, andoutcome assessors was
unclear in the majorityo studies and most studies did not have any
evidence oselective reporting and baseline difference.
.. Is Albumin Useful in Paracentesis? Tree studies wereincluded
in the analysis o whether albumin was useul in
paracentesis [,, ]. Te use o albumin was associatedwith
signicant reduction in paracentesis-induced circula-tory dysunction
(OR . % CI ..). No signicantdifference was observed or the risk o
any other outcomeswith and without albumin use. Tere was a
nonsignicanttrend towards reduction in hyponatraemia,
paracentesis-induced circulatory dysunction, readmission, and
renalimpairment.
.. Is Albumin Better Tan Other Volume Expanders in
Para-centesis? Eight studies evaluatedthe use o volume
expanderscompared to albumin [, ,, , , , , ]. None
-
7/24/2019 teori lapmat
4/9
BioMed Research International
: reatment groups, ollowup, and results.
Study Albumin group Control group Duration o ollowup Results
Abdel-Khalek andAri []
Paracentesis and IV %albumin g/L o ascitic uidremoved.
Paracentesis andhydroxyethyl starch%.
Up to months.
Bacterial inection / versus /,death / versus /, encephalopathy/
versus /, GI bleeding /versus /, readmissions / versus
/.
Altman et al. []
Paracentesis and IV %albumin mL i
-
7/24/2019 teori lapmat
5/9
BioMed Research International
: Continued.
Study Albumin group Control group Duration o ollowup Results
Sola-Vera et al. []
Paracentesis and IV %albumin g/L o ascitic uidremoved.
Paracentesis and mL o .%saline/L o ascitesremoved.
NA.
Death / versus /, hyponatraemia/ versus /, PICD / versus/, renal
impairment / versus/.
Sort et al. []
IV ceotaxime g dosingbased on serum creatinineand % albumin .
g/kgduring rst hours, then g/kg on day .
IV ceotaxime dosingbased on creatinine.
NA.
Death in hospital / versus /,death at three months / versus/,
inection resolution /versus /, renal impairment /versus /.
Xue et al. []
IV cefriaxone plus IValbumin .. g/kg within hours o enrolment,
thensame amount on rd day andevery days thereafer.
IV cefriaxone g/dayadjusted based onserum creatinine.
NA. Renal impairment / versus /,
deaths / versus /.
NA: not available.
o these studies compared the use o albumin versus othervolume
expanders outside o the paracentesis context. Teuse o albumin
resulted in no signicant advantage in risko death, encephalopathy,
hyponatraemia, gastrointestinalbleeding, readmission, renal
impairment, and sepsis/severeinection.
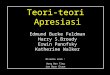
.. Is Albumin Useful in Infections/Sepsis?Five studies
wereincluded in the analysis o albumin use in sepsis. wo studies[,]
included participants with non-SBP inection whilethree studies
included participants with SBP [,,]. In thecontext o any inection,
the use o albumin was associated
with reduced risk o death OR . % CI ..,2
= 24% and renal impairment OR . % CI .., 2 = 34%. Tere was a
nonsignicant trend towardsinection resolution and increased risk o
hyponatraemia.Subgroup analysis considering SBP showed that the
albuminuse was associated with reduced risk o death. No
signicantdifference was observed or non-SBP inection (able).
Tepooled results o the risk evaluations are shown in Figure and
able.
4. Discussion
Our results suggest that albumin has a value in the
treatment
o cirrhotic patients in the contexts o large volume
para-centesis and inections. Tere is no signicant advantage
oalbumin compared to other plasma expanders or paracente-sis. In
paracentesis, albumin reduces the risk o paracentesis-induced
circulatory dysunction. In cases o cirrhotic patientswith
inections, death and renal impairment can be reducedwith the use o
albumin. Tereore, cirrhotic patients at highrisk o circulatory
dysunction during paracentesis shouldreceive albumin or an
alternative plasma expander, andcirrhotic patients with sepsis or
inection at high risk o renalimpairment or death should receive
albumin.
Broadly, our ndings support the AASLD and EASLrecommendations or
the management o large volume
paracentesis [, ]. Te use o other plasma expanders isnot
supported as there is insufficient evidence according tothe
guidelines. While albumin may cost more than plasmaexpanders, the
use o albumin is justied as there is evidencethat there are ewer
-day liver related events among thepatients treated with albumin
[]. Both guidelines supportthe use o albumin in spontaneous
bacterial peritonitis [,]but there are currently no guidelines or
non-SBP inections.
Tere are a number o potential explanationsor our nd-ings. Human
albumin is a major plasma protein and acts asan intravascular
volume expander. It is produced in the liverand its concentration
is reduced with hepatic dysunction.It is responsible or % o the
colloid osmotic pressure o
plasma; thereore, the intravenous administration o albuminis
associated with a rapid increase in the circulating blood
volume. In the context o inection and sepsis, the
acuteinammatory response has a vasodilatory effect. Tis leadsto
circulatory collapse which is compounded by a lack oalbumin to
maintain oncotic pressure in the intravascularcompartment. In
addition, it has other physiological unc-tions such as transport o
water insoluble endogenous andexogenous substances such as
anti-inammatory mediators,hormones, and antibiotics in sepsis. It
also acts as a circu-latory antioxidant which may prevent cellular
injury romreactive oxygen species in sepsis and ischaemia.
Our review builds on the nding o the meta-analysis by
Bernardi et al. []. Similar to their ndings, we ound thatthe use
o albumin reduces the risk o paracentesis-inducedcirculatory
dysunction. However, we did not nd that therewasany signicant
difference when albumin wascomparedtoother volume expanders. Teir
study was limited to patientsreceiving paracentesis while our study
also considers patientswith inection.
Our study has several advantages. All the studies includedwere
prospective randomized trials. We were able to considercirrhotic
patients in several different settings including thoserequiring
paracentesis with tense ascites as well as those withSBP and
non-SBP inection. In addition, we were able to con-sider a variety
o outcomes including death, encephalopathy,
-
7/24/2019 teori lapmat
6/9
BioMed Research International
Albumin No albuminStudy or subgroup
EventsWeight
TotalEventsTotal
1.1.1 Death
Choi 2002 3 21 2 19 6.1%
Guevara 2012 8 56 10 54 11.7%
Sort 1999 14 63 26 63 13.8%
Xue 2002 5 56 17 56 11.2%Subtotal (95% CI) 196 192 42.9%
Total events 30 55
Choi 2002 4 21 2 19 6.5%
Subtotal (95% CI) 21 19 6.5%
Total events 4 2
Heterogeneity: Not applicable
1.1.3 Inection resolution
Nazar 2009 55 56 50 54 4.9%
Sort 1999 62 63 59 63 5.0%
Subtotal (95% CI) 119 117 9.9%
Total events 117 109
1.1.4 Renal impairment
Choi 2002 3 21 1 19 4.5%
Guevara 2012 1 56 4 54 4.9%
Nazar 2009 3 56 4 54 8.0%
Sort 1999 6 63 21 63 12.0%
Xue 2002 5 56 19 56 11.3%
Subtotal (95% CI) 252 246 40.7%
Total events 18 49
Test or overall effect:Z = 2.46 (P = 0.01)
Test or overall effect:Z = 0.74 (P = 0.46)
Test or overall effect:Z = 1.82 (P = 0.07)
Test or overall effect:Z = 2.65 (P = 0.008)
Heterogeneity: 2 = 0.00; 2 = 0.00, d= 1 (P = 0.98);I2 = 0%
Heterogeneity: 2 = 0.09; 2 = 3.93, d= 3 (P = 0.27);I2 = 24%
Heterogeneity: 2 = 0.28; 2 = 6.09, d= 4 (P = 0.19);I2 = 34%
Odds ratio Odds ratio
M-H, random, 95% CI M-H, random, 95% CI
1.42 [0.21, 9.55]
0.73 [0.27, 2.02]
0.41 [0.19, 0.88]
0.22 [0.08, 0.66]0.46 [0.25, 0.86]
2.00 [0.32, 12.41]
2.00 [0.32, 12.41]
4.40 [0.48, 40.70]
4.20 [0.46, 38.71]
4.30 [0.89, 20.70]
3.00 [0.28, 31.63]
0.23 [0.02, 2.10]
0.71 [0.15, 3.32]
0.21 [0.08, 0.57]
0.19 [0.07, 0.56]
0.34 [0.15, 0.75]
1.1.2 Hyponatraemia
0.01 0.1
Favours albumin
1 10 100
Favours no albumin
F : Albumin versus no albumin among cirrhotic patients with
inections.
hyponatraemia, paracentesis-induced circulatory dysunc-tion,
readmission renal impairment, gastrointestinal bleed,
inection resolution, and sepsis/severe inection.Tere are several
limitations in this review. Te quality
o the studies is generally poor as blinding was not
used.Furthermore, the sample size o the studies is small and onlya
ew studies were included in each pooled analysis. Teduration o
ollowup was also variable among the studies.
We would recommend three studies o albumin andplasma expanders
which are in the context o paracentesis,non-SBP, and SBP inections.
In addition to clinical outcomessuch as need or death,
encephalopathy, hyponatraemia, GIbleeding, readmission, renal
impairment, sepsis, and need orliver transplant, this study should
urther consider the costimplications. Te most important o the
possible studies is
that o albumin versus plasma expanders in inections (non-SBP and
SBP) as these questions have not been answered.
In addition, a study o different doses o albumin could
helpdetermine the dosing regimen that would lead to the
bestclinical outcomes. We believe that the ideal trial would bean
adequately powered multicentre double-blinded trial thathas ollowup
o at least month and corrects or liver diseaseseverity.
5. Conclusions
In conclusion, the ndings o this meta-analysis support theuse o
albumin or preventing paracentesis-induced circula-tory collapse
and reducing the risk o death and renal ailurein cirrhotic patients
with inections limited to SBP. More
-
7/24/2019 teori lapmat
7/9
BioMed Research International
: Summary o results.
Outcome or subgroup Studies Participants Odds ratio (% condence
interval)
Is albumin useful in paracentesis?
.. Death . (., .)
.. Encephalopathy . (., .)
.. Hyponatraemia . (., .).. Paracentesis-induced circulatory
dysunction . (., .)
.. Readmission . (., .)
.. Renal impairment . (., .)
Is albumin better than other volume expander in
paracentesis?
.. Death . (., .)
.. Encephalopathy . (., .)
.. Hyponatraemia . (., .)
.. Gastrointestinal bleeding . (., .)
.. Readmission . (., .)
.. Renal impairment . (., .)
.. Sepsis/severe inection . (., .)
Is albumin useful in infections overall?.. Death . (., .)
.. Hyponatraemia . (., .)
.. Inection resolution . (., .)
.. Renal impairment . (., .)
Is albumin useful in spontaneous bacterial peritonitis?
.. Death . (., .)
.. Inection resolution . (., .)
.. Renal impairment . (., .)
Is albumin useful in non-spontaneous bacterial peritonitis
infections?
.. Death . (., .)
.. Inection resolution . (., .)
.. Renal impairment . (., .)
studies are needed to evaluate i albumin reduces adverseoutcomes
among cirrhotic patients without paracentesis orinections. Tere is
no evidence to support the use o albuminover other plasma expanders
or paracentesis.
Conflict of Interests
Chun Shing Kwok, Lukasz Krupa, Ash Mahtani, DuncanKaye, Simon M.
Rushbrook, Martin G. Phillips, and WilliamGelson have no conict o
interests to declare. No undingwas received.
Authors Contribution
William Gelson conceptualised the review. Chun ShingKwok, Lukasz
Krupa, and William Gelson developed theprotocol. Chun Shing Kwok,
Duncan Kaye, and Ash Mahtaniabstracted the data. Chun Shing Kwok
analysed the data. Allauthors were involved in writing the paper.
William Gelsonwill act as the guarantor or the paper.
References
[] L. Ruiz-Del-Arbol, A. Monescillo, W. Jimenez, A.
Garcia-Plaza,V. Arroyo, and J. Rodes, Paracentesis-induced
circulatorydysunction: mechanism and effect on hepatic
hemodynamicsin cirrhosis, Gastroenterology, vol. , no. , pp. ,
.
[] P. Gines, L. ito, V. Arroyo et al., Randomized
comparativestudy o therapeutic paracentesis with and without
intravenous
albumin in cirrhosis, Gastroenterology, vol. , no. , pp. , .
[] P. Gines and A. Cardenas, Te management o ascites
andhyponatremia in cirrhosis,Seminars in Liver Disease, vol. ,no. ,
pp. , .
[] F. Salerno, M. Guevara, M. Bernardi et al., Reractory
ascites:pathogenesis, denition and therapy o a severe
complicationin patients with cirrhosis,Liver International, vol. ,
no. , pp., .
[] B. A. Runyon, Management o adult patients with ascitesdue to
cirrhosis: update , AASLD Practice
Guidelines.http://www.aasld.org/practiceguidelines/Documents/ascitesup-date.pd.
-
7/24/2019 teori lapmat
8/9
BioMed Research International
[] P. Gines, P. Angeli, K. Lenz et al., EASL clinical
practiceguidelines on the management o ascites, spontaneous
bacterialperitonitis, and hepatorenal syndrome in cirrhosis,Journal
ofHepatology, vol. , no. , pp. , .
[] J. Fernandez, M. Navasa, J. C. Garcia-Pagan et al., Effect
ointravenous albumin on systemic and hepatic hemodynamicsand
vasoactive neurohormonal systems in patients with cirrho-
sis and spontaneous bacterial peritonitis,Journalof
Hepatology,vol. , no. , pp. , .
[] P. Sort, M. Navasa, V. Arroyo et al., Effect o
intravenousalbumin on renal impairment and mortality in
patientswith cir-rhosis and spontaneous bacterial peritonitis,Te
New EnglandJournal of Medicine, vol. , no. , pp. , .
[] J. Fernandez, M. Navasa, J. Gomez et al., Bacterial
inectionsin cirrhosis: epidemiological changes with invasive
proceduresand noroxacin prophylaxis, Hepatology, vol. , no. , pp. ,
.
[] F. Wong, M. Bernardi, R. Balk et al., Sepsis in cirrhosis:
reporton the th meeting o the International Ascites Club,Gut, vol.,
no. , pp. , .
[] P. andon and G. Garcia-sao, Bacterial inections, sepsis,
andmultiorgan ailure in cirrhosis,Seminars in Liver Disease, vol.,
no. , pp. , .
[] V. Arvaniti, G. DAmico, G. Fede et al., Inections in
patientswith cirrhosis increase mortality our-old and should be
usedin determining prognosis, Gastroenterology, vol. , no. , pp.,
.
[] A. Follo, J. M. Llovet, M. Navasa et al., Renal impairment
aferspontaneous bacterial peritonitis in cirrhosis:
incidence,clinicalcourse, predictive actors and prognosis,
Hepatology, vol. ,no. , pp. , .
[] . Gustot, F. Durand, D. Lebrec, J.-L. Vincent, and R.
Moreau,Severe sepsis in cirrhosis,Hepatology, vol. , no. , pp. ,
.
[] B. A. Runyon, Albumin inusion or spontaneous
bacterialperitonitis,Te Lancet, vol. , no. , pp. , .
[] P. andon and G. Garcia-sao, Renal dysunction is themost
important independent predictor o mortality in cirrhoticpatients
with spontaneous bacterial peritonitis, Clinical Gas-troenterology
and Hepatology, vol. , no. , pp. , .
[] M. Guevara, V. Arroyo, and P. Gines, Effect o albumin
onsurvival in septic cirrhotic patients other than
spontaneousbacterial peritonitis. Te question remains open, Journal
ofHepatology, vol. , no. , pp. , .
[] http://hiru.mcmaster.ca/hiru/HIRUHedges EMBASE
Strate-gies.aspx, and, http://hiru.mcmaster.ca/hiru/HIRU
HedgesMEDLINE Strategies.aspx.
[] E. E. Abdel-Khalek and S. E. Ari, Randomized trial com-
paring human albumin and hydroxyethyl starch % as
plasmaexpanders or treatment o patients with liver cirrhosis
andtense ascites ollowing large volume paracentesis,Arab Journalof
Gastroenterology, vol. , no. , pp. , .
[] C. Altman, B. Bernard, D. Roulot, R.-L. Vitte, and O.
Ink,Randomized comparative multicenter study o hydroxyethylstarch
versusalbumin as a plasmaexpander in cirrhoticpatientswith tense
ascites treated with paracentesis,European Journalof
Gastroenterology and Hepatology, vol. , no. , pp. , .
[] C. H. Choi, K. H. Han, D. Y. Kim et al., Efficacy andsaety o
large volume paracentesis in cirrhotic patients withspontaneous
bacterial peritonitis: a randomized prospectivestudy, Te Korean
Journal of Hepatology, vol. , no. , pp. , .
[] E. Fassio, R. erg, G. Landeira et al., Paracentesis with
Dextran vs. paracentesis with albumin in cirrhosis with tense
ascites.Results o a randomized study,Journal of Hepatology, vol.
,no. -, pp. , .
[] D. Garcia-Compean, J. Z. Villarreal, H. B. Cuevas et al.,
otaltherapeutic paracentesis (P) with and without
intravenousalbumin in the treatment o cirrhotic tense ascites: a
random-ized controlled trial,Liver, vol. , no. , pp. , .
[] D. Garca-Compean, P. Blanc, D. Larreyet al., reatment o
cir-rhotic tense ascites with Dextran- versus albumin
associatedwith large volume paracentesis: a randomized controlled
trial,Annals of Hepatology, vol. , no. , pp. , .
[] A. Gines, G. Fernandez-Esparrach, A. Monescillo et al.,
Ran-domized trial comparing albumin, dextran , and polygelinein
cirrhotic patients with ascites treated by paracentesis,
Gas-troenterology, vol. , no. , pp. , .
[] M. Guevara, C. erra, A. Nazar, E. Sola, J. Fernandez, M.
Pavesiet al., Albumin or bacterial inections other than
spontaneousbacterial peritonitis in cirrhosis. A randomized,
controlledstudy,Journal of Hepatology, vol. , no. , pp. , .
[] R. Moreau, D.-C. Valla, I. Durand-Zaleski et al., Comparisono
outcome in patients with cirrhosis and ascites ollowingtreatment
with albumin or a synthetic colloid: a randomisedcontrolled pilot
trial,Liver International, vol. , no. , pp. , .
[] A. Nazar, M. Guevara, C. erra, M. Martin-Llahi, M. E.
Baccaro,M. Pavesi et al., Effect o albumin administration in
patientswith cirrhosis and bacterial inection other than
spontaneousbacterial peritonitis. A randomized controlled
study,Journal ofHepatology, vol. , p. S, .
[] R. Planas, P. Gines,V. Arroyo et al., Dextran-
versusalbuminas plasma expanders in cirrhotic patients with tense
ascitestreated with total paracentesis: Results o a randomized
study,Gastroenterology, vol. , no. , pp. , .
[] J. Sola-Vera, J. Minana, E. Ricart et al., Randomized trial
com-paring albumin and saline in the prevention o
paracentesis-induced circulatory dysunction in cirrhotic patients
withascites,Hepatology, vol. , no. , pp. , .
[] H. P. Xue, B. Lin, J. Z. Mo, and J. Q. Li, Effect o
albumininusion on preventing the deterioration o renal unction
inpatients with spontaneous bacterial peritonitis, Chinese
Journalof Digestive Diseases, vol. , no. , pp. , .
[] J. P. . Higgins andS. Green, Cochrane Handbook For
SystematicReviewsof Interventions Version .., Te Cochrane
Collabora-tion, ,www.cochrane-handbook.org.
[] J. P. . Higgins, S. G. Tompson, J. J. Deeks, and D. G.
Altman,Measuring inconsistency in meta-analyses, British
MedicalJournal, vol. , no. , pp. , .
[] R. Moreau, D.-C. Valla, I. Durand-Zaleski et al., Comparisono
outcome in patients with cirrhosis and ascites ollowingtreatment
with albumin or a synthetic colloid: a randomisedcontrolled pilot
trial,Liver International, vol. , no. , pp. , .
[] F. Salerno, S. Badalamenti, E. Lorenzano, P. Moser, and
P.Incerti, Randomized comparative study o hemaccel vs. albu-min
inusion afer total paracentesis in cirrhotic patients withreractory
ascites,Hepatology, vol. , no. , pp. , .
[] M. Bernardi, P. Caraceni, R. J. Navickis, and M. M.
Wilkes,Albumin inusion in patients undergoing large-volume
para-centesis: a meta-analysis o randomized trials,Hepatology,
vol., no. , pp. , .
-
7/24/2019 teori lapmat
9/9