Embed Size (px)
Citation preview

Một trường hợp viêm phổi
Ths. Bs. Dương Minh NgọcBộ môn Nội
Đại học Y dược Tp. Hồ Chí Minh
Hành chính
Bệnh nhân nữ, sinh năm 1961
Nhập viện ngày 25/4/2019
Địa chỉ: Gò Công Tây – Tiền Giang

Lí do nhập viện
Đau bụng thượng vị

Bệnh sử
Cách nhập viện 01 ngày, bệnh nhân đau bụng thượng vị tăng dần kèm buồn nôn, tiêu lỏng nhập Bv đa khoa Trung tâm Tiền Giang chuyển bệnh viện Chợ Rẫy
Tiền căn: đái tháo đường típ 2 đang điều trị bằng thuốc uống Lúc nhập viện: GCS 15 điểm Nhịp thở 20, mạch 92, huyết áp 110/70, nhiệt độ 37 Tim nghe rõ, đều; phổi không ran; bụng ấn đau thượng vị, đề kháng +/-

CLS nhập viện 25/4/19
Hgb 112 g/L, Hct 33.8%; WBC 6.43 G/L, Neu 84.7%; Plt 290 G/L
Glucose 196 mg/dL
AST 172 U/L, ALT 161 U/L
BUN 14 mg/dL, Creatinin 0.69 mg/dL
Amylase 1280 U/L, Lipase 913 U/L
Triglyceride 53 mg/dL
CRP 51.2 mg/L
CT: viêm tụy cấp, Bathalzar E, CTSI 4 điểm
Chẩn đoán lúc vào
VIÊM TỤY CẤP NGÀY 1 CTSI 4 ĐIỂM – ĐÁI THÁO ĐƯỜNG TÍP 2

25/4 2/5Lâm sàng Bệnh nhân tỉnh, tiếp xúc tốt, sinh hiệu ổnCận lâm sàng
WBC 6.43 G/L, Neu 84.7%Amylase máu 1280 U/L, Lipase 913 U/LTriglyceride 53 mg/dLCRP 51.2 mg/LCT: viêm tụy cấp, Bathalzar E, CTSI 4 điểm
Điều trị Ringer lactateOmeprazole TramadolSandostatinLantus Insulin
Diễn biến
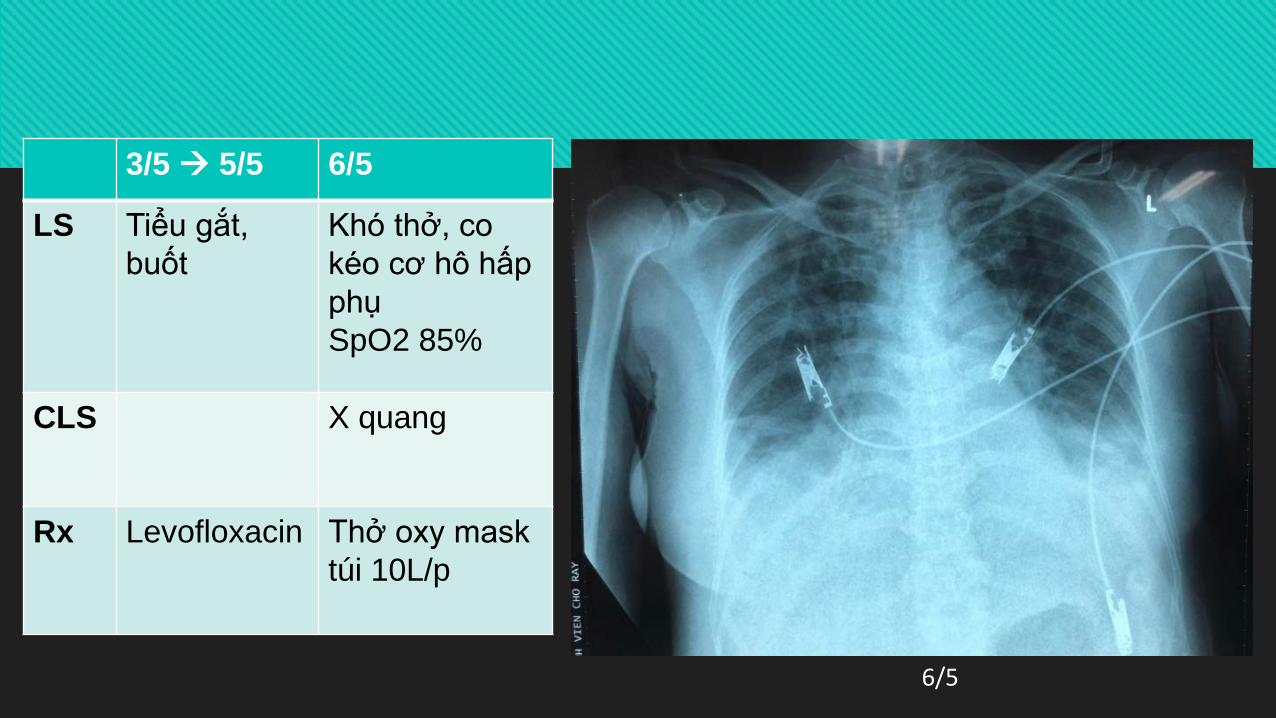
3/5 5/5 6/5
LS Tiểu gắt, buốt
Khó thở, co kéo cơ hô hấp phụSpO2 85%
CLS X quang
Rx Levofloxacin Thở oxy mask túi 10L/p
6/5

7/5 8/5Lâm sàng
Khó thở, lơ mơSuy hô hấp
Khó thở giảmSốt 39.5 độ C
Điều trị Đặt nội khí quảnImipenemCiprofloxacin
Rút NKQ thở oxy mask túiImipenemCiprofloxacin
Diễn biến

9/5 15/5
Lâm sàng Còn khó thởSuy hô hấp, SpO2 88%Ho khan Hết sốtPhổi: ran nổ
Cận lâm sàng
WBC 8.3 K/uL, Neu 88%X quang phổi
Điều trị Thở oxy mask túiImipenemCiprofloxacin
9/5
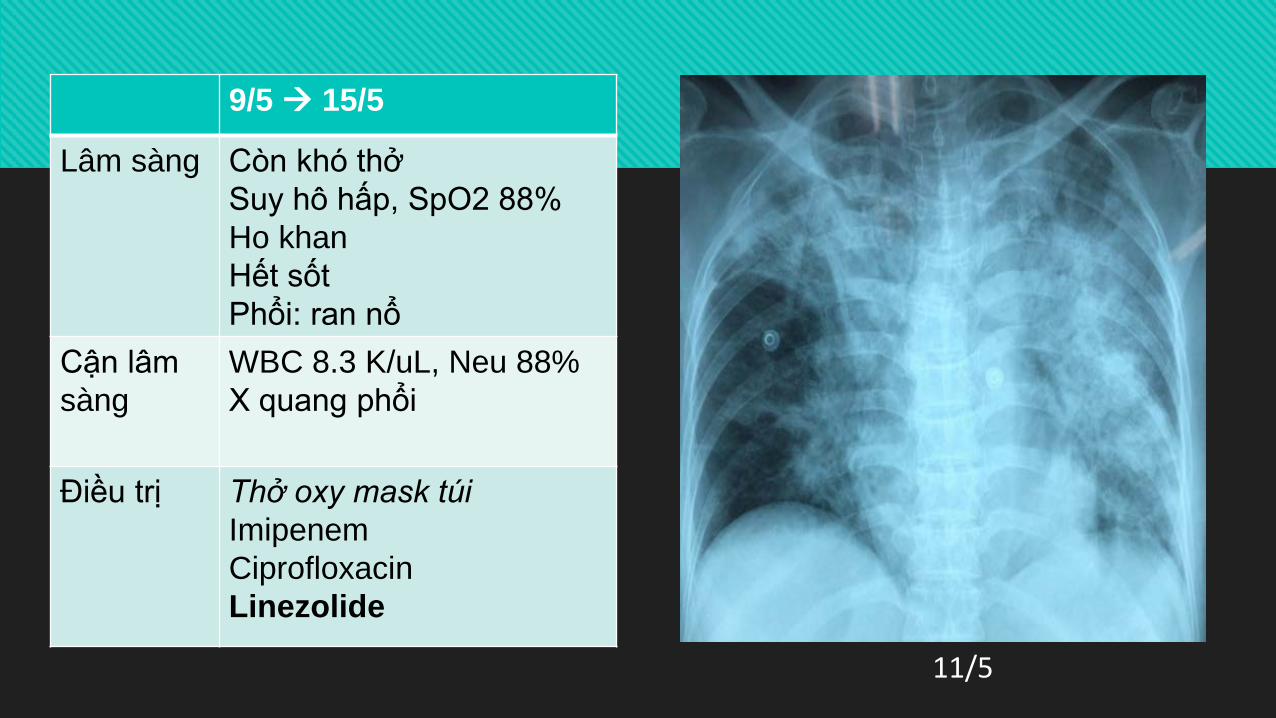
11/5
9/5 15/5
Lâm sàng Còn khó thởSuy hô hấp, SpO2 88%Ho khan Hết sốtPhổi: ran nổ
Cận lâm sàng
WBC 8.3 K/uL, Neu 88%X quang phổi
Điều trị Thở oxy mask túiImipenemCiprofloxacinLinezolide
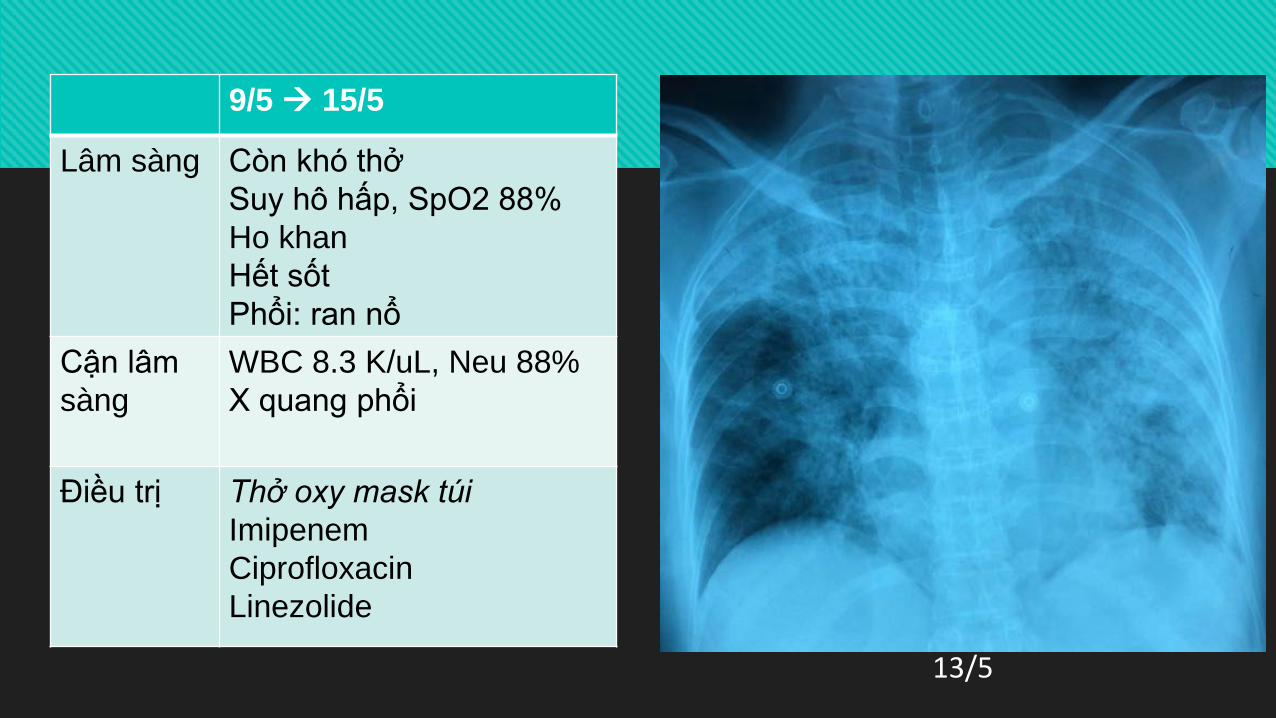
13/5
9/5 15/5
Lâm sàng Còn khó thởSuy hô hấp, SpO2 88%Ho khan Hết sốtPhổi: ran nổ
Cận lâm sàng
WBC 8.3 K/uL, Neu 88%X quang phổi
Điều trị Thở oxy mask túiImipenemCiprofloxacinLinezolide

16 22/5Lâm sàng
Sốt giảmHo đàm đụcCòn suy hô hấp
Cận lâm sàng
Cấy đàm: vi khuẩn: không mọcCandida dubliniensis nhạy Vori, amB, FlucystosineWBC: 6.4, Neu 84%CT ngực 18/5
Điều trị
Thở oxy mask túi 10 L/phútImipenem Linezolide Colistin
X quang phổi 16/5
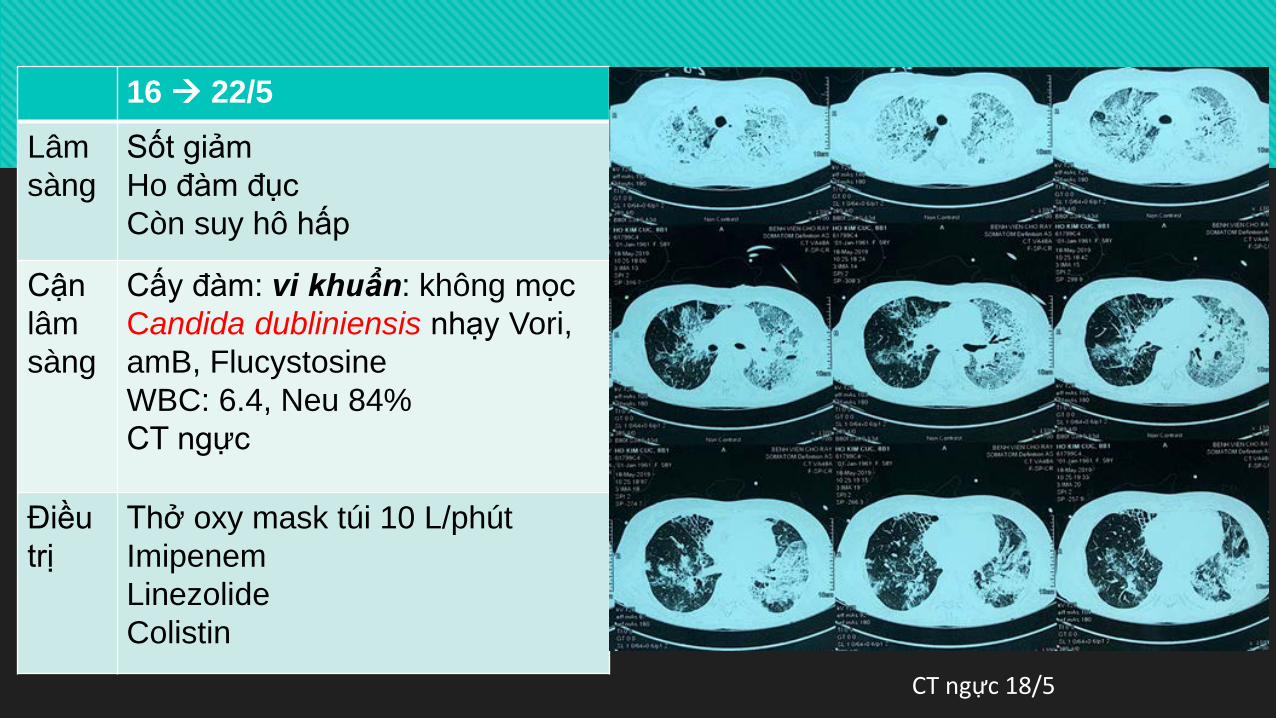
16 22/5Lâm sàng
Sốt giảmHo đàm đụcCòn suy hô hấp
Cận lâm sàng
Cấy đàm: vi khuẩn: không mọcCandida dubliniensis nhạy Vori, amB, FlucystosineWBC: 6.4, Neu 84%CT ngực
Điều trị
Thở oxy mask túi 10 L/phútImipenemLinezolideColistin
CT ngực 18/5
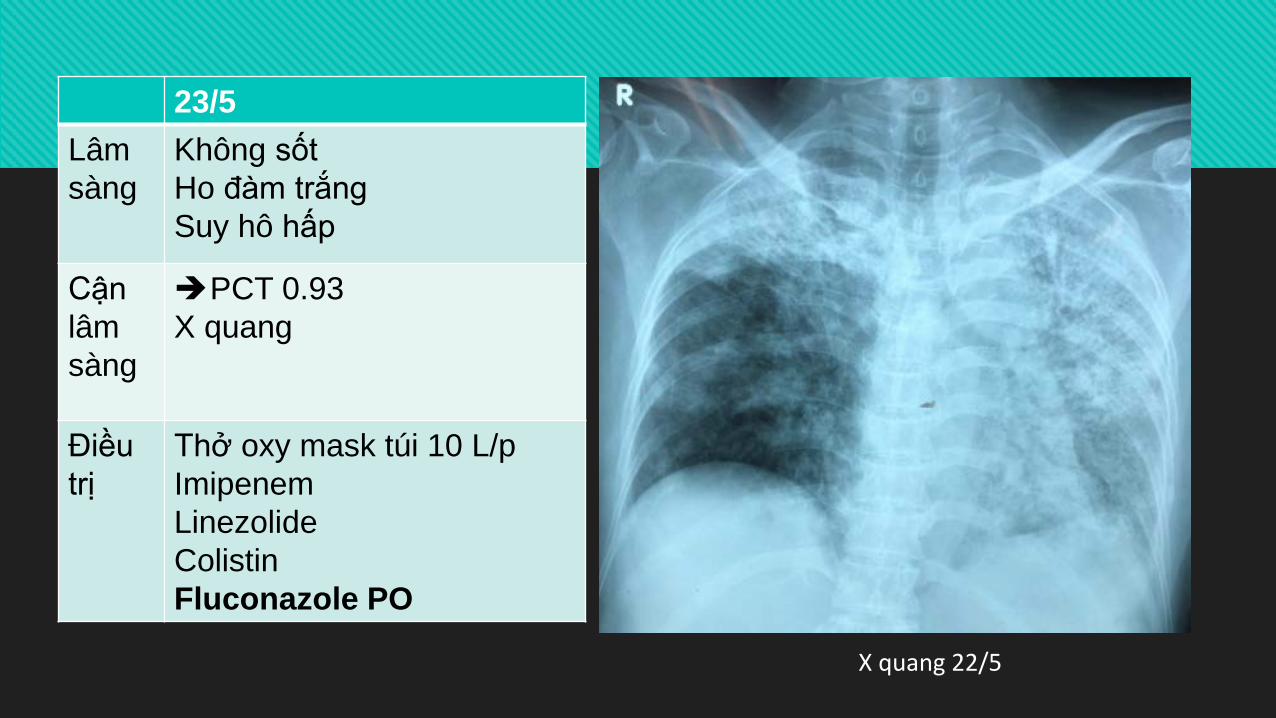
23/5Lâm sàng
Không sốtHo đàm trắngSuy hô hấp
Cận lâm sàng
PCT 0.93X quang
Điều trị
Thở oxy mask túi 10 L/pImipenemLinezolideColistinFluconazole PO
X quang 22/5
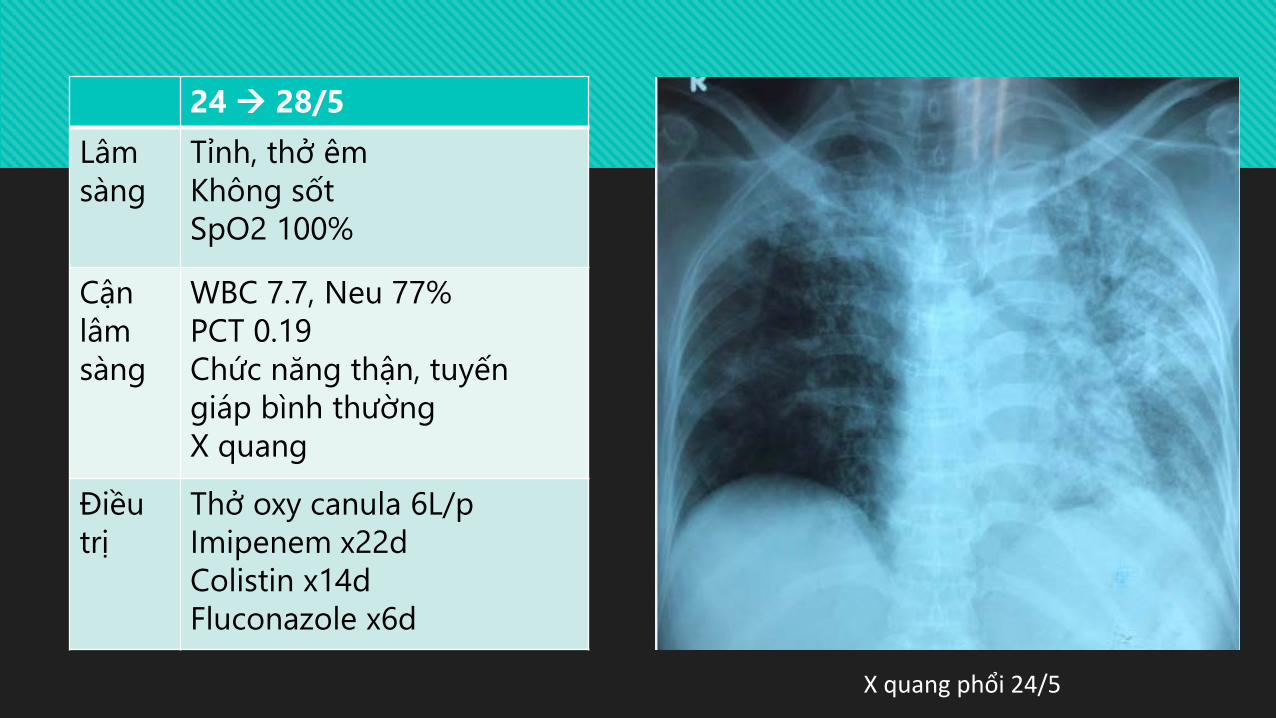
24 28/5Lâm sàng
Tỉnh, thở êmKhông sốtSpO2 100%
Cận lâm sàng
WBC 7.7, Neu 77%PCT 0.19Chức năng thận, tuyếngiáp bình thườngX quang
Điều trị
Thở oxy canula 6L/pImipenem x22dColistin x14dFluconazole x6d
X quang phổi 24/5

24 28/5Lâm sàng
Tỉnh, thở êmKhông sốtSpO2 100%
Cận lâm sàng
X quangNSPQ
Điều trị
Thở oxy canula 6L/pImipenem x22dColistin x14dFluconazole x6d
X quang phổi 27/5

Nội soi phế quản 28/5
Rửa phế quản phế nang + bấm sinh thiết xuyên phế quản
Đọng ít đàm phế quản trái
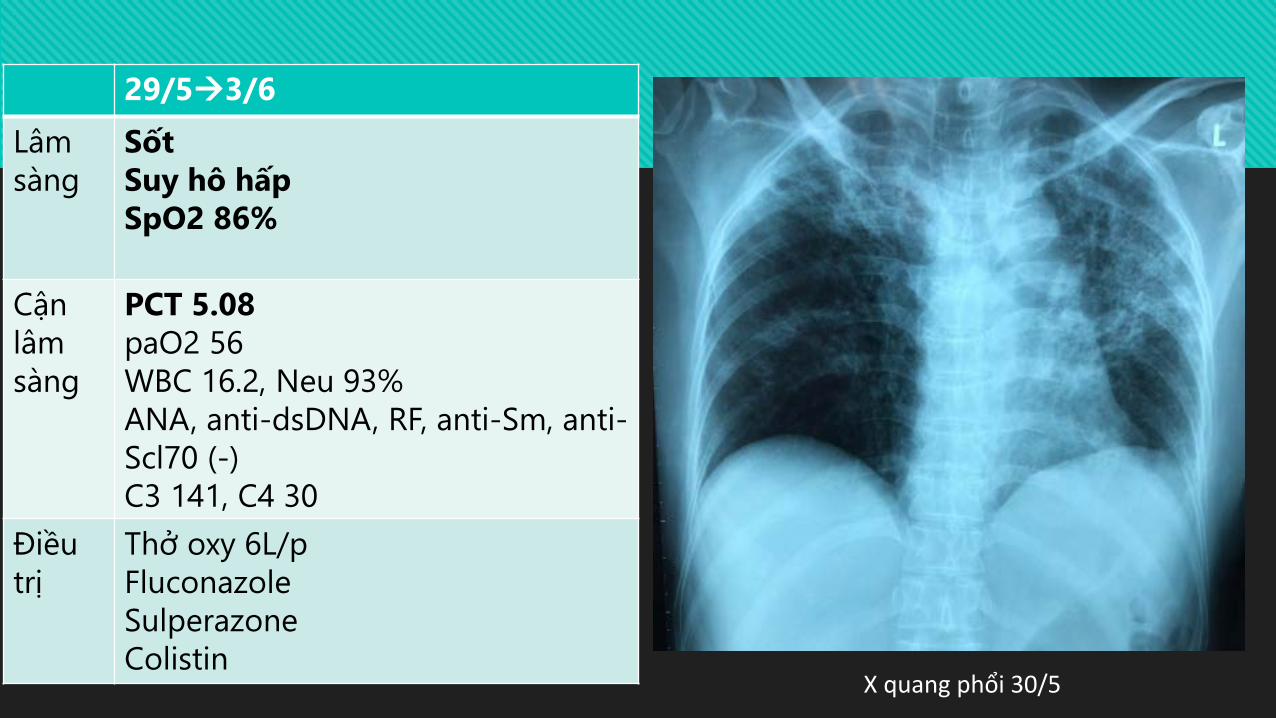
X quang phổi 30/5
29/53/6Lâm sàng
SốtSuy hô hấpSpO2 86%
Cận lâm sàng
PCT 5.08paO2 56WBC 16.2, Neu 93%ANA, anti-dsDNA, RF, anti-Sm, anti-Scl70 (-)C3 141, C4 30
Điều trị
Thở oxy 6L/pFluconazoleSulperazoneColistin

4/6Lâm sàng
SốtKhông hoPhổi ran nổSpO2 88-92%
Cận lâm sàng
Cấy DRPQ: Candida tropicalis nhạy caspofungin, amB, khángfluconazole; vi khuẩn: không mọc; AFB(-)PCT 3.6
Điều trị Thở oxy 6L/pSulperazoneColistinAmphotericin B
Diễn biến
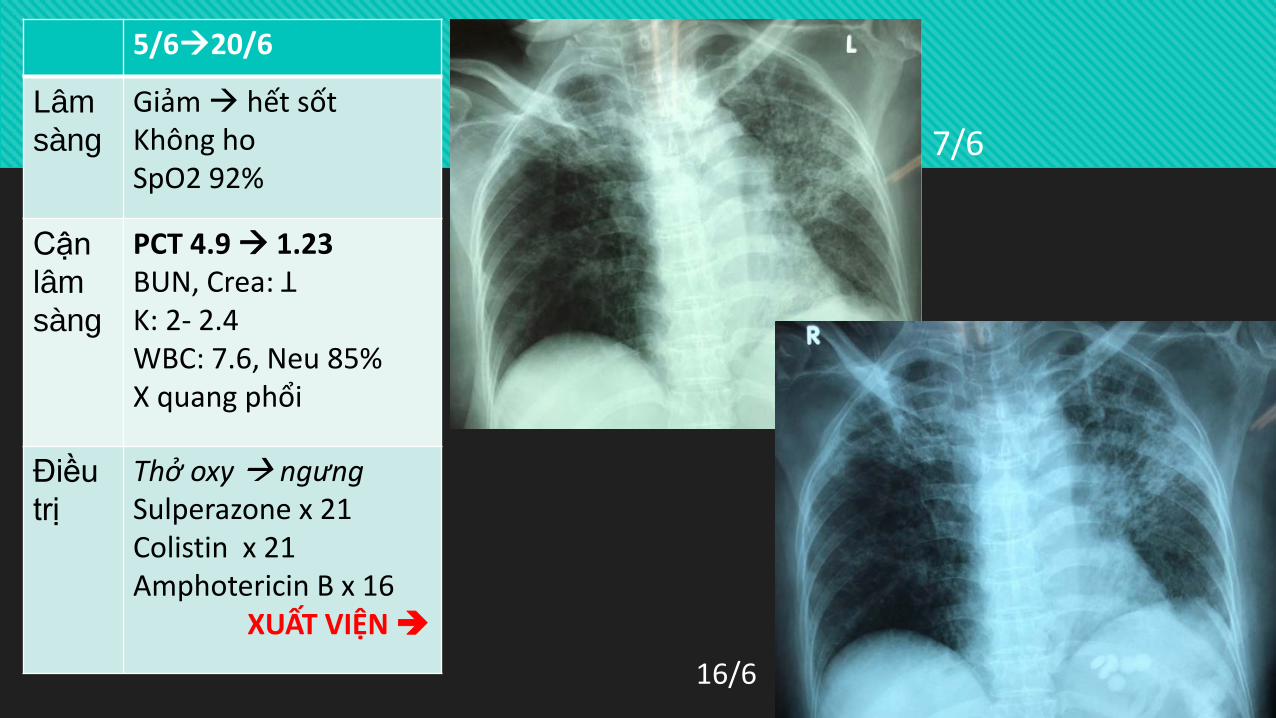
5/620/6
Lâm sàng
Giảm hết sốtKhông hoSpO2 92%
Cận lâm sàng
PCT 4.9 1.23BUN, Crea: ꓕK: 2- 2.4WBC: 7.6, Neu 85%X quang phổi
Điều trị
Thở oxy ngưngSulperazone x 21Colistin x 21Amphotericin B x 16
XUẤT VIỆN
7/6
16/6
Vấn đề
Yếu tố nguy cơ nhiễm nấm xâm lấn?
Thời điểm quyết định dùng thuốc kháng nấm?
Chọn loại nào?

YẾU TỐ NGUY CƠ NHIỄM NẤM XÂM LẤN
Nhiễm trùng huyết, sốc nhiễmtrùng
Nuôi ăn hoàn toàn bằng đườngtĩnh mạch
Phẫu thuật Quần cư Candida nhiều nơi Thở máy xâm lấn Catheter tĩnh mạch trung tâm
Thông tiểu Kháng sinh phổ rộng > 5 ngày
trong 2 tuần qua Điều trị thay thế thận Đái tháo đường phụ thuộc
insulin Ức chế miễn dịch: bệnh/thuốc Ghép tạng
Ther Clin Risk Manag. 2014; 10: 95–105Ann Intensive Care. 2011; 1: 50

THỜI ĐIỂM DÙNG THUỐC KHÁNG NẤM

Nhiễm Candida xâm lấn

What Is the Role of Empiric Treatment for Suspected Invasive Candidiasis in Nonneutropenic Patients in the ICU?
Empiric antifungal therapy should be considered in critically ill patients with risk factors for invasive candidiasis and no other known cause of fever and should be based on clinical assessment of risk factors, surrogate markers for invasive candidiasis, and/or culture data from nonsterile sites
Empiric antifungal therapy should be started as soon as possible in patients who have the above risk factors and who have clinical signs of septic shock
β-D-glucan, mannan-antimannan antibodies,
và PCR testing
Limited clinical studies have evaluated the efficacy of empiric strategies.

What Is the Role of Empiric Treatment for Suspected Invasive Candidiasis in Nonneutropenic Patients in the ICU?
Preferred empiric therapy for suspected candidiasis in nonneutropenic patients in the ICU is an echinocandin (caspofungin: loading dose of 70 mg, then 50 mg daily; micafungin: 100 mg daily; anidulafungin: loading dose of 200 mg, then 100 mg daily)
Fluconazole, 800-mg (12 mg/kg) loading dose, then 400 mg (6 mg/kg) daily, is an acceptable alternative for patients who have had no recent azole exposure and are not colonized with azole-resistant Candida species
Fluconazole may be considered in hemodynamically stable patients who are colonized with azole-susceptible Candida species or who have no prior exposure to azoles.
Widespread use of antifungal agents must be balanced against the cost, the risk of toxicity, and the emergence of resistance.

What Is the Role of Empiric Treatment for Suspected Invasive Candidiasis in Nonneutropenic Patients in the ICU?
Lipid formulation AmB, 3–5 mg/kg daily, is an alternative if there is intolerance to other antifungal agents
Recommended duration of empiric therapy for suspected invasive candidiasis in those patients who improve is 2 weeks, the same as for treatment of documented candidemia

Kết luận
Phương tiện chẩn đoán nấm: không có sẵn
Cấy bệnh phẩm thông thường (đàm, nước tiểu): ít giá trị
Quyết định điều trị kháng nấm: khó khăn
Thuốc kháng nấm: đắt tiền, độc tính
Hướng dẫn điều trị: có sẵn sử dụng như thế nào?