Embed Size (px)
DESCRIPTION
Thyroid Orbitopathy & Glaucoma. 高雄醫學大學 眼科 張丞賢. Graves orbitopathy Thyroid associated ophthalmopathy Thyroid eye disease. Shared autoantigen? *EO Muscles 64Kd protein *Adipocyte TSH receptor glycosaminoglycan. Thyroid Orbitopathy. TO Thyroid Orbit - PowerPoint PPT Presentation
Citation preview

Thyroid OrbitopathyThyroid Orbitopathy& Glaucoma& Glaucoma
高雄醫學大學 眼科高雄醫學大學 眼科
張丞賢張丞賢



Thyroid OrbitopathyThyroid Orbitopathy• Graves orbitopathyGraves orbitopathy• Thyroid associated ophthalmopathyThyroid associated ophthalmopathy• Thyroid eye diseaseThyroid eye disease Shared autoantigen?Shared autoantigen?
*EO Muscles*EO Muscles64Kd protein64Kd protein*Adipocyte*AdipocyteTSH receptorTSH receptorglycosaminoglycanglycosaminoglycan
TOTO
Thyroid OrbitThyroid OrbitAutoimmune inflammatioAutoimmune inflammatio
nn

Thyroid Orbitopathy (TO)Thyroid Orbitopathy (TO)• NNo signo sign• OOnly sign: nly sign: lid retraction, lid lag, staringlid retraction, lid lag, staring
• SSoft tissue sign: oft tissue sign: chemosis, congested conj.chemosis, congested conj.
• PProptosisroptosis• EExtraocular myopathyxtraocular myopathy• CCorneal epithelial defects (Corneal Ulcer)orneal epithelial defects (Corneal Ulcer)• SSight (Optic neuropathy)ight (Optic neuropathy)
American Thyroid Association 1977American Thyroid Association 1977
• IOP?IOP?
• GlaucomaGlaucoma
??

QuestionsQuestions• Do TO patients tend to have glaucoma? Do TO patients tend to have glaucoma?
or ocular hypertension only. or ocular hypertension only.
• TO-associated ocular hypertension, how TO-associated ocular hypertension, how
does it happen? What is the mechanism?does it happen? What is the mechanism?
• TO-associated ocular hypertension, do TO-associated ocular hypertension, do
we have to treat? How should we treat?we have to treat? How should we treat?

Question oneQuestion one
• Do TO patients tend to have glaucoma? Do TO patients tend to have glaucoma?
Or ocular hypertension only.Or ocular hypertension only.

Do TO patients tend to have Do TO patients tend to have ocular hypertension or ocular hypertension or glaucoma?glaucoma?• The The prevalenceprevalence of ocular hypertension of ocular hypertension
and glaucoma in TO patientsand glaucoma in TO patients• TO patients vs. NormalTO patients vs. Normal
• Ocular HT (22-30 mmHg) :Ocular HT (22-30 mmHg) : 24% (124/500) vs. 5% ??? 24% (124/500) vs. 5% ???
• Glaucoma (Disc & VF)/Ocular HTGlaucoma (Disc & VF)/Ocular HT :: 2% vs. 2.7%(IOP 21-25 mmHg), 12% (IOP 26-30 mm2% vs. 2.7%(IOP 21-25 mmHg), 12% (IOP 26-30 mmHg) 43 months followHg) 43 months follow
• Cockerham, Kennerdell et al, Ophthalmology 1997Cockerham, Kennerdell et al, Ophthalmology 1997

Is the above finding Is the above finding consistent?consistent?
• Prevalence of ocular H/T and glaucoma iPrevalence of ocular H/T and glaucoma in a Dutch TO studyn a Dutch TO study• Ocular H/TOcular H/T: 4.8% : 4.8% (23/482)(23/482)
• Glaucoma (POAG)Glaucoma (POAG): 0.8% : 0.8% (4/482)(4/482) vs 1.1% Dut vs 1.1% Dutch general populationch general population
Kalmann & Mourits BJO 1998Kalmann & Mourits BJO 1998
Why???? Why???? American vs. EuropeanAmerican vs. European

Measurement of IOPMeasurement of IOP
• ApplanationApplanation
• Slight upgaze Slight upgaze
• IOP increased with upgazeIOP increased with upgaze
• Compression of episcleral vein by Compression of episcleral vein by
enlarged inferior rectus musclesenlarged inferior rectus muscles


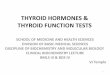
IOP change on different IOP change on different vertical gazevertical gaze
Reader A. Ophthalmology 1982Reader A. Ophthalmology 1982
14
15
16
17
18
19
20
21
22
-25 -20 -15 -10 -5 0 5 10 15 20 25
Angle of Gaze (degree)
IO
P (m
mH
g)


TO: Augmented TO: Augmented Δ IOP in upgazΔ IOP in upgazee
• Normal: 0.6 Normal: 0.6 ± 0.2 ± 0.2 mmHgmmHg
• Graves’ patients without exophthalmos: 4.Graves’ patients without exophthalmos: 4.8 ± 0.4 8 ± 0.4 mmHgmmHg
• Graves’ patients with exophthalmos: 9.2 ± Graves’ patients with exophthalmos: 9.2 ± 1 1 mmHgmmHg
• 81 patients81 patients
Gamblin et al. NEJM 1983Gamblin et al. NEJM 1983

• Δ IOP increased with exophthalmosΔ IOP increased with exophthalmos

Time and Increased IOP (Time and Increased IOP (ΔΔIOP)IOP) GamGam
blin GT et al, N Eng J Med 1983)blin GT et al, N Eng J Med 1983)
0
20
40
60
80
100
0-1 (25) 2-3 (13) 4-10 (23) >10 (15)
Years elapsed since diagnosis of Graves' disease (PatientNo.)
per
centa
ge (%
)

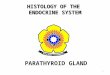
Augmented Increase of IOP on UpgazeAugmented Increase of IOP on Upgaze Spierer A, Eisenstein Z. Ophthalmolgy 1991Spierer A, Eisenstein Z. Ophthalmolgy 1991
0
5
10
15
20
25
30
0 1 2 3 4 5 6 7 8 9 10 11 12
dIOP
% S
ubje
cts
GravesControl

Augmented Increase of IOP on UpgazeAugmented Increase of IOP on Upgaze Spierer A, Eisenstein Z. Ophthalmolgy 1991Spierer A, Eisenstein Z. Ophthalmolgy 1991
0
5
10
15
20
25
30
0 1 2 3 4 5 6 7 8 9 10 11 12
dIOP (mmHg)
% S
ubje
cts
Non-infiltrative
Infiltrative
Control

Other evidence- Increased IOP at upgaOther evidence- Increased IOP at upgazeze
• Adhesive myopathyAdhesive myopathy
• Blow-out orbital fracture with inferior Blow-out orbital fracture with inferior
rectus muscle incarcerationrectus muscle incarceration
• Orbital myositisOrbital myositis
Zappia et al. AJO 1971Zappia et al. AJO 1971

Back to the Question of Different Back to the Question of Different
Prevalence of Ocular Prevalence of Ocular
Hypertension in TOHypertension in TO
• American vs. European StudiesAmerican vs. European Studies
• Ethnic?Ethnic?
• Black, Hispanic and Indian (First Black, Hispanic and Indian (First
Nations) in American Study?Nations) in American Study?

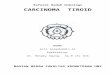
Different subgroups of TO patients and IODifferent subgroups of TO patients and IO
PP Cockerham KP et al, Ophthalmology 1997Cockerham KP et al, Ophthalmology 1997
100%
75%
60%
25%
0%
20%
40%
60%
80%
100%
120%
enlarged EOM
limited EOM proptosis diplopiaper
centa
ge o
f oc
ula
r hyp
erte
nsi
on

Caucasian vs. OrientalCaucasian vs. Oriental
• Japanese studyJapanese study• 13% 13% (14/104)(14/104):: (7 POAG + 7 NTG) / TO (7 POAG + 7 NTG) / TO
Ohtsuka & Nakamura Am J Ophthalmol 2000Ohtsuka & Nakamura Am J Ophthalmol 2000
• Question?Question?• NTG or compressive optic neuropathyNTG or compressive optic neuropathy
• Difference of VF/optic disc change?Difference of VF/optic disc change?

V.F. of compressive optic V.F. of compressive optic neuropathyneuropathy
• The most common defects found with compThe most common defects found with compression of the optic nerve anterior to the chiression of the optic nerve anterior to the chiasma include asma include enlarged blind spot, relative cenlarged blind spot, relative central scotoma,entral scotoma, and and constrictionconstriction. .
• Nearly all typesNearly all types of visual field abnormalities of visual field abnormalities have been reported with compression of the have been reported with compression of the optic nerve. optic nerve.

Vancouver (UBC TO data)Vancouver (UBC TO data)
• Ocular Ocular
Hypertension Hypertension
Prevalence Prevalence
= 4/85 = 4/85
= 4.7% = 4.7% 0
5
10
15
20
25
30
0 10 20 30 40
Proptosis (Hertel's exophthalmometry, mm)
IOP (m
mH
g)

Vancouver (UBC TO data)Vancouver (UBC TO data)
• Increase of IOIncrease of IO
P at upgaze > P at upgaze >
7mmHg = 77mmHg = 7
/81 = 8./81 = 8.
6%6%0
2
4
6
8
10
12
14
16
18
0 10 20 30 40
Proptosis (Hertel's exophthalmometry, mm)
Incr
ease
d IO
P a
t upga
ze (m
mH
g)

TO-associated ocular TO-associated ocular
hypertension, how does it hypertension, how does it
happen? What is the mechanism?happen? What is the mechanism?
• Angle closure?Angle closure?
• Trabecular meshwork, resistance?Trabecular meshwork, resistance?
• Ciliary body, Ciliary body, ovoverproduction of aqueous?erproduction of aqueous?
• Orbit, congested?Orbit, congested?
HypothesisHypothesis??

Hypothesis of ocHypothesis of ocular H/T in ular H/T in TOTO
• Enlarged Enlarged extraocular musclesextraocular muscles• Accumulation of glycosaminoglycan in Accumulation of glycosaminoglycan in
orbitorbit Increased orbital pressureIncreased orbital pressure Increased orbital venous pressure (OVP)Increased orbital venous pressure (OVP) Increased episcleral vein pressure (EVP)Increased episcleral vein pressure (EVP) Increased IOPIncreased IOP
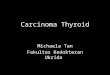
OVP OVP ææ EVP EVP ææ IOP IOP

OVP OVP ææ EVP EVP ææ IOP IOP
• OVP: orbital veOVP: orbital venous pressurenous pressure
• EVP: episcleral EVP: episcleral vein pressurevein pressure
• MAP: mean artMAP: mean arteral pressureeral pressure
Reitsamerand & KReitsamerand & Kiel 2002 IVOSiel 2002 IVOS
Rabbit model
0
5
10
15
20
25
30
0 20 40 60 80 100 120
MAP (mmHg)
Pres
sure
(mm
Hg)
OVP
EVP
IOP

The initial steps of the The initial steps of the hypothesishypothesis
• Enlarged extra-ocular musclesEnlarged extra-ocular muscles• Accumulation of glycosaminoglycan in orbitAccumulation of glycosaminoglycan in orbit
?? ?? Increased orbital pressure Increased orbital pressure
VOP VOP
EVPEVP
IOP Orbital decompressionIOP Orbital decompression

Intraorbital PressureIntraorbital Pressure(Retrobulbar Pressure, RBP)(Retrobulbar Pressure, RBP)
• Normal “steady state” RBP 3-4.5 mmHgNormal “steady state” RBP 3-4.5 mmHg
Otto JA et al, BJO1996Otto JA et al, BJO1996
0
10
20
30
40
501 2
3R 3L
4 5 6 7 8 9
Patient No.
Ret
robu
lbar
pre
ssure
(m
mH
g)
Preoppostop

To-associated Ocular To-associated Ocular
HypertensionHypertension
Do we have to treat? How should Do we have to treat? How should
we treat? we treat?
• What is the indication to treat?What is the indication to treat?
• IOP?IOP?
• Will treat patients with IOP between 22 Will treat patients with IOP between 22
and 26 mmHg? Or between 26 and 30?and 26 mmHg? Or between 26 and 30?
• Other parametersOther parameters
• Optic discOptic disc
• Visual fieldVisual field

Risk of subsequent glaucomatous visuRisk of subsequent glaucomatous visual field lossal field loss Sommer AJO 1989Sommer AJO 1989
Armaly et al.Armaly et al.1-13 year follow1-13 year follow
David et al.David et al.Mean follow 43 Mean follow 43
monthsmonths
IOP IOP (mmH(mmH
g)g)
Risk Risk (%)(%)
IOP IOP (mmHg)(mmHg)
Risk Risk (%)(%)
<16<16 0.80.816-1916-19 1.41.4 21-2521-25 2.72.720-2320-23 3.13.1 26-3026-30 12.012.0≧≧2424 8.48.4 >30>30 41.241.2

Risk factors for developing Risk factors for developing
Glaucoma in TO, Ocular Glaucoma in TO, Ocular
hypertensionhypertension• Degree of PropotosisDegree of Propotosis• Degree of MyopathyDegree of Myopathy• Exposure to corticosteroidExposure to corticosteroid• Prior anti-glaucoma therapyPrior anti-glaucoma therapy• Family history of glaucomaFamily history of glaucoma• Duration of active orbitopathyDuration of active orbitopathy
Cockerham et al, Ophthalmology 1997Cockerham et al, Ophthalmology 1997

To-associated Ocular To-associated Ocular
HypertensionHypertension
Do we have to treat? How should Do we have to treat? How should
we treat? we treat? • Reduce the aqueous production – Reduce the aqueous production –
blocker, CAI, blocker, CAI, 2 agonist2 agonist• Facilitate aqueous outflow – Facilitate aqueous outflow –
• Miotics, Miotics, agonist agonist• ProstaglandinProstaglandin
• Hyperosmotic agentHyperosmotic agent• Sugar-based mediSugar-based mediccation, Manitolation, Manitol
• Others? Others? • Surgery, TRBCSurgery, TRBC

Orbital DecompressionOrbital Decompression Kalmann and Mourits BJO 1Kalmann and Mourits BJO 1
998, Dev et al. 1998 CJO998, Dev et al. 1998 CJO
1012141618202224262830
Preop. Postop.
IOP
(mm
Hg)
23 18 mmHg

IOP decreased after Tx in TOIOP decreased after Tx in TO• Inferior rectus muscle recessionInferior rectus muscle recession
Kalmann and Mouritiz BJO1998Kalmann and Mouritiz BJO1998
• Botulinum toxin injection for myopathic strabismusBotulinum toxin injection for myopathic strabismusKikkawa et al. AJO 2003Kikkawa et al. AJO 2003

How about Hypothyroidism?How about Hypothyroidism?
• TO mostly hyperthyroidismTO mostly hyperthyroidism
• HypothyroidismHypothyroidism
• No proptosisNo proptosis
• No enlargement of EOMNo enlargement of EOM
• No restrictive myopathyNo restrictive myopathy

Hypothyroidism Hypothyroidism
association with POAG or association with POAG or
NTGNTG
• Controversial Controversial
• AutoimmuneAutoimmune
• Deposition of mucopolysacharide in trabecualr mesDeposition of mucopolysacharide in trabecualr mes
hworkhwork

ConclusionConclusion• Ocular Hypertension in TOOcular Hypertension in TO
• Subgroup of enlarged / restrictive EOMSubgroup of enlarged / restrictive EOM
• D.D. compressive optic neuropathyD.D. compressive optic neuropathy• TreatmentTreatment
• Medical : inhibition of aqueous production, Medical : inhibition of aqueous production, -blocker, CAI-blocker, CAI
• Orbital decompression, muscle recession, botulinum iOrbital decompression, muscle recession, botulinum injectionnjection

AppreciationAppreciation• 吳國揚 會長吳國揚 會長• 蔡榮坤 主任蔡榮坤 主任• 高醫眼科 所有住院醫師高醫眼科 所有住院醫師• 林玫琪 小姐 林玫琪 小姐 (MSD)(MSD)• 林斐嬋 小姐 林斐嬋 小姐 (( 南區眼科醫師會秘書南區眼科醫師會秘書 ))
• 南區眼科醫師南區眼科醫師