7/31/2019 Att Thy & Suicide New
http://slidepdf.com/reader/full/att-thy-suicide-new 1/31
EFFECTIVENESS OF ATTITUDINIZE PSYCHOTHERAPY
IN ENHANCING SELF ESTEEM AND
DIMINISHING SUICIDAL IDEATION AMONG ADULTS IN PAKISTAN
Dr. Linah Askari
Assistant Professor, Psychology
College of Business Management
Institute of Business Management, Karachi
Email: [email protected]
ABSTRACT
The Attitudinize Psychotherapy; an Intervention of the New Millennium, is a complete
psychotherapy dealing effectively with all the six vital aspects concerning an emotional problem of a
human being.
In order to test the five hypotheses, the sample comprised of NO THERAPY GROUP; the Fifty-
two Male and Twenty-three Female Adult Students on which NO Attitudinize Psychotherapy would be
conducted, and for ATTITUDINIZE THERAPY GROUP; Fifty-four Male and Twenty-three Female Adult
Students on which Attitudinize Psychotherapy would be conducted. The data was collected from the
Adult students between the ages of 18–25 belonging to Iqra University, Karachi. In the Initial Phase of
BEFORE THERAPY All the Male and Female students were administered; a) Dysfunctional Attitude Scale
(Therapy Form) (Modified by Dr. Linah Askari 2003), b) Queendom’s Self–Esteem Test (2003) and c)
Adult Suicidal Ideation Questionnaire (William & Reynolds, 2005). In the Final Phase of AFTER
THERAPY, Attitudinize Therapy was conducted for fourteen weeks (75 minute session, twice a week)
on the ATTITUDINIZE THERAPY GROUP only. At the completion of this phase the whole sample was Re-
administered All the three Scales, to both the adults of NO THERAPY GROUP and the adults of
ATTITUDINIZE THERAPY GROUP. The purpose was to relate the effectiveness of the Attitudinize
Therapy with the Enhancement of Self – Esteem and Diminishing of Suicidal Ideation within the Adult
to build their lives successfully.
The results of statistical analysis reveal that (i) In Before Therapy Phase: the adults within NO
THERAPY GROUP have Mean Scores of Dysfunctional Attitude = 303.40, Self-Esteem = 51.78 &
Suicidal Ideation = 149.25 whereas ATTITUDINIZE THERAPY GP have Mean Scores of Dysfunctional
Attitude = 304.83, Self-Esteem = 50.50 & Suicidal Ideation = 150.35 (ii) In After Therapy Phase: theadults within NO THERAPY GROUP have Mean Scores of Dysfunctional Attitude = 309.26, Self-Esteem
= 50.33 & Suicidal Ideation = 153.41 whereas ATTITUDINIZE THERAPY GP have Mean Scores of
Dysfunctional Attitude = 103.94, Self-Esteem = 124.15 & Suicidal Ideation = 60.15 providing evidence
that Ultimately, Attitudinize Psychotherapy would be the BEST CHOICE.
Key words: Attitude, Self-Esteem, Suicidal Ideation, Attitudinize, Psychotherapy, Pakistan.
1

7/31/2019 Att Thy & Suicide New
http://slidepdf.com/reader/full/att-thy-suicide-new 2/31

7/31/2019 Att Thy & Suicide New
http://slidepdf.com/reader/full/att-thy-suicide-new 3/31
The roots of personality grow within the concept of Self Esteem. Each individual has a unique
identification, distinct traits, separate innovative ideas, exceptional comprehending skills and
extraordinary way of understanding the reality. When these qualities are polished with confidence,
trust and encouragement within the environment, they produce a successful Individual. Every person
struggles for the survival and reputation of its name or identification. For each and every
action/behavior there is an Attitude/Intention behind it. As it is beautifully said in the First Hadith
(Preachings of the Holy Prophet PBUH): “Innamal Aamaal-u- Binniyaat” means “All Behaviors arise
from Attitudes/Intentions.” It means that the bases of every human action and reaction are the
attitude/intention. After the arousal of a positive or a negative attitude (intention) to particular stimuli
or situation, the person starts thinking on those terms, beliefs due to his/ her past experiences arise
accordingly and hence the behavior in the connection is framed.
Bartleby (2000) defines, “Attitudinize means to assume an affected attitude; Practice or adopt
attitudes especially for effect.” When Parents, Teachers or other important people within the circle of
an individual develop a positive vision for the success of that individual, all of them struggle within
their own roles, at each developmental phase and on all stages to guide and mentor the person
towards their set goals for the positive achievements. In fact, the individual makes a mindset to prove
oneself and come up to the mark for the expectations demanded by himself and others for his success.
Webster (2003) defines, “Attitude is a complex mental state involving beliefs, feelings, values
and dispositions to act in certain ways. In addition, “Attitude is a psychological tendency expressed by
an evaluative response that can be overt or covert, cognitive, affective or behavioral.”
Kamradt and Kamradt (1999) define, “Attitude is a psychophysical structure that stores related
bits of affective, cognitive, and psychomotor learning in a manner that allows instantaneous,
subconscious access by its owner (p. 570). They view attitude as the fundamental unit of learning.”
Figure1: Components and Structure of a Discrete Attitude
(Kamradt & Kamradt, 1999).
Attitude makes a difference every hour, everyday, in everything that one does for the entire
life. Anything done with a positive attitude will work beneficially, whereas anything done with a
negative attitude will work harmfully. If one has a positive attitude, a person looks for ways to solve
the problems that one can solve, and let go off things, over which one has no control. One can develop
a positive attitude by emphasizing the good, by being tough-minded and by refusing defeat. The
greatest discovery of any generation is that human beings can alter their lives by altering the
attitudes of their minds (Schweitzer, 2002).
3
7/31/2019 Att Thy & Suicide New
http://slidepdf.com/reader/full/att-thy-suicide-new 4/31
7/31/2019 Att Thy & Suicide New
http://slidepdf.com/reader/full/att-thy-suicide-new 5/31
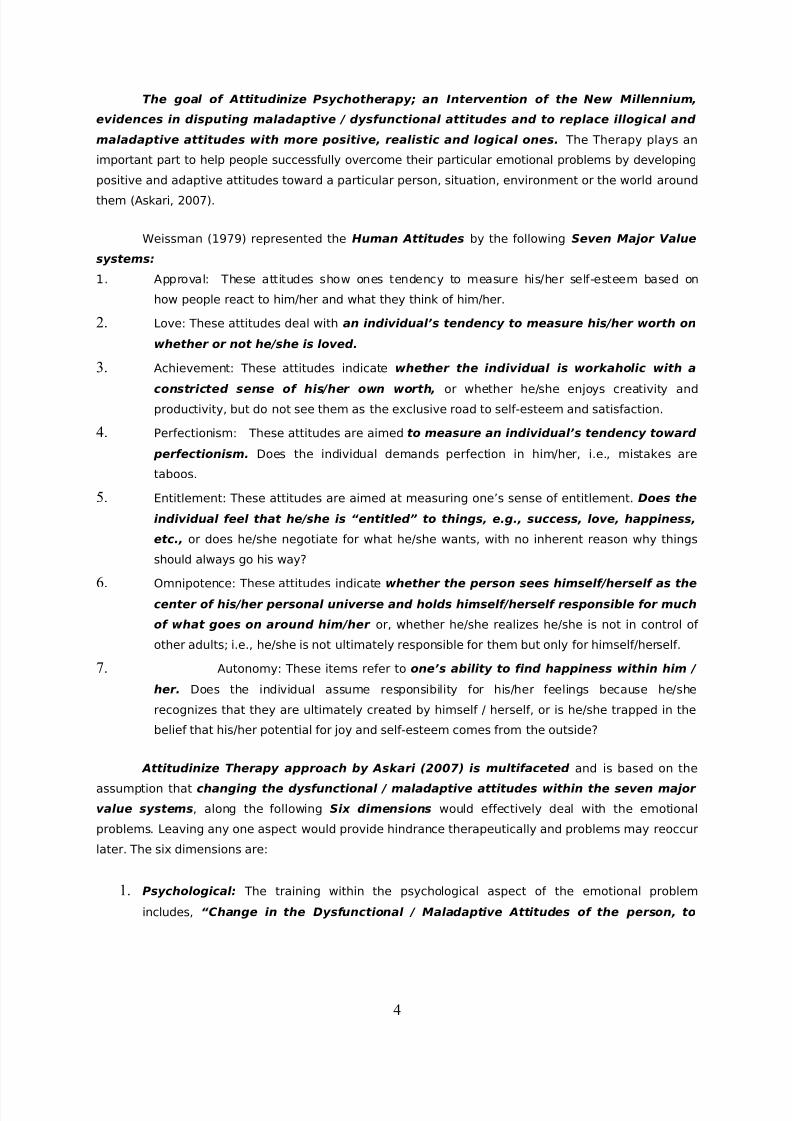
change the patterns of thinking, beliefs and behavior toward psychological self,
environment and the world around.”
2. Terminological: The training within the terminological aspect of the emotional problem
includes, “Changing of the abusive / invective attitudes and behaviors; altering
verbal and non-verbal maladaptive communications, through altering the language-
expression toward self, environment and the world around.”
3. Spiritual: The training within the spiritual aspect of the emotional problem includes,
“Changing of dysfunctional / maladaptive attitudes toward Allah (the Divine Being),
Reducing guilt and fear, and Inculcating the belief of attaining perfect justice for
self and others.”
4. Physiological: The training within the physiological aspect of the emotional problem includes,
“Changing of maladaptive attitudes toward physiological self, through deep
breathing exercise to keep oxygen balance in the body, to maintain balanced diet
consumption and control the water intake and output to stabilize the body fluids.”
5. Neuro-hormonal: Neuro-hormones are the body's chemical messengers; these hormones
stimulate the cells they are attached to. The training within the terminological aspect of the
emotional problem includes, “Inculcating an attitude that Neuro-hormonal Regulation
of one’s own body can be easily controlled through muscle relaxation exercises and
massage of pressure points of your body.”
6. Time Management: The training within the ‘time management’ aspect of the emotional
problem includes, “Changing of maladaptive attitudes toward time management and
to become positively creative and remain relaxed for most of the time in your life-
time.”
Burns (1999) proposed the Development of Better Self – Esteem inferring that, “Most
people's feelings and thoughts about themselves fluctuate somewhat based on their daily experiences.
The grade you get on an exam, how your friends treat you, ups and downs in a romantic relationship -
all can have a temporary impact on your wellbeing.” Your self-esteem, however, is something more
fundamental than the normal "ups and downs" associated with situational changes. For people with
good basic self-esteem, normal "ups and downs" may lead to temporary fluctuations in how they feel
about themselves, but only to a limited extent. In contrast, for people with poor basic self-esteem,
these "ups and downs" may make all the difference in the world.
Before you can begin to improve your self-esteem you must first believe that you can change
it. Change doesn't necessarily happen quickly or easily, but it can happen. You are not powerless!
Once you have accepted, or are at least willing to entertain the possibility that you are not powerless,
there are three steps proposed by Burns (1999) that a person can take to begin to change their self-
esteem:
5

7/31/2019 Att Thy & Suicide New
http://slidepdf.com/reader/full/att-thy-suicide-new 6/31
Step 1: Rebut the Inner Critic: The first important step in improving self-esteem is to begin
to challenge the negative messages of the critical inner voice. For example: When the Inner Critic's
Voice Catastrophizes: "She turned me down for a date! I'm so embarrassed and humiliated. No one
likes or cares about me. I'll never find a girlfriend. I'll always be alone." So Your Rebuttals to Become
Objective: "Ouch! That hurt. Well, she doesn't want to go out with me. That doesn't mean no one does.
I know I'm an attractive and nice person. I'll find someone."
Step 2: Practice Self-Nurturing: Rebutting your critical inner voice is an important first
step, but it is not enough. Since our self-esteem is in part due to how others have treated us in the
past, the second step to more healthy self-esteem is to begin to treat oneself as a worthwhile person.
Start to challenge past negative experiences or messages by nurturing and caring for yourself in ways
that show that you are valuable, competent, deserving and lovable. There are several components to
self-nurturing such as: Practice Basic Self-Care, Plan Fun & Relaxing Things For Oneself, Reward
Yourself For Your Accomplishments, Remind Yourself of Your Strengths & Achievements, Forgive
Yourself When You Don't Do All You'd Hoped and Self-Nurture Even When You Don't Feel You Deserve
It.
Step 3: Get Help from Others: Getting help from others is often the most important step a
person can take to improve his or her self-esteem, but it can also be the most difficult. People with low
self-esteem often don't ask for help because they feel they don't deserve it. But since low self-esteem
is often caused by how other people treated you in the past, you may need the help of other people in
the present to challenge the critical messages that come from negative past experiences. Here are
some ways to get help from others such as: Ask for Support from Friends, Get Help from Teachers &
Other Helpers and Talk to a Therapist. Sometimes low self-esteem can feel so painful or difficult to
overcome that the professional help of a therapist or counselor is needed. Talking to a counselor is agood way to learn more about your self-esteem issues and begin to improve your self-esteem. Hence
Attitudinize Psychotherapy would be the BEST CHOICE.
Reinherz, Tanner, Berger, Beardslee and Fitzmaurice (2006) studied across a wide variety of
indicators, with adolescent and adult subjects for suicidal ideation. It was reported that
significantly poorer functioning was found by subjects at age 30 for those having suicidal ideation in
adolescence as compared to their peers without suicidal ideation in adolescence. Interviewers rated
subjects with suicidal ideation as having significantly lower levels of global functioning and social and
occupational functioning than subjects without suicidal ideation. Self-reported coping and self-esteem
were lower in subjects with suicidal ideation; interpersonal problems and reports of needing social
support were higher for this group.
Therefore, Adolescent Suicidal Ideation was Predictive of Psychopathology, Suicidal Behavior, and
Compromised Functioning at Age 30, in adulthood. Research Findings underscore the importance of
considering suicidal ideation in adolescence as a marker of severe distress and a predictor of
compromised functioning, indicating the need for early identification and continued intervention.
Additional factors that point to an increased risk for suicide in depressed individuals are:
6
7/31/2019 Att Thy & Suicide New
http://slidepdf.com/reader/full/att-thy-suicide-new 7/31
Anxiety, agitation, or enraged behavior
Isolation, segregation and seclusion from the environment
Drug and/or alcohol use or abuse
History of physical or emotional illness
Feelings of hopelessness or desperation
Ultimately, Attitudinize Psychotherapy would be the BEST CHOICE.
Literature Review
The meaning of high self-esteem is currently under close empirical scrutiny. High self-esteem
is typically viewed as beneficial for individuals due to its association with markers of psychological
adjustment (Diener, 1984; Kaplan, 1975; Robins, Hendin, & Trzesniewski, 2001; Tennen & Affleck,
1993). Secure high self-esteem, which can be traced to the work of Carl Rogers (1959, 1961), reflects
positive attitudes toward the self that are realistic, well-anchored, and resistant to threat.
So what degree of self-esteem do people have that never even graduated high school? A study
conducted at the University of Maine (McCaul, Donaldson, Colodarci, & Davis, 1992) examined just
that. The high school and beyond data base was used to investigate the experiences of drop outs and
high school graduates (control group), four years after the projected date of graduation. Specifically,
dropouts and graduates with no post-secondary education were compared on the following: Self-
esteem, satisfaction at work, political/social participation measures, and number of jobs. Multiple
regression analyses were used to determine the degree to which dropping out explained variance in
these measures. Dropouts differed from graduates on every personal and social adjustment measure.
Differences on these measures were much more significant in males (dropouts vs. graduates), than in
females (dropouts vs. graduates).
In the article published by Goliath (2005), large number of studies has been accumulated
within this concern. Adolescent / Adult suicide is a worldwide problem, but it is of particular concern in
highly industrialized nations such as the United States (Conner, Duberstein, Conwell, Seidlitz, & Caine,
2001); Kurtz & Derevensky, 1993). The suicide rate in the United States has tripled since 1960, making
it the third leading cause of death among adolescents and the second leading cause of death among
the college-age population (National Mental Health Association, 1997). Although it is estimated that
approximately 14 adolescents in the United States commit suicide each day, the actual number is two
to three times higher (American Psychiatric Association, 1996; 1998). Understandably, these alarming
statistics have stimulated great concern in the public at large and have led social scientists to warn of
an impending rise in the number of suicides and suicidal attempts among adolescents (Berman &
Jobes, 1994; Griffiths, Farley, & Fraser, 1986; Watt & Sharp, 2002). Much of the research literature
appears to be focused on suicide per se. However, professionals are increasingly paying attention to
the antecedent behaviors. According to Bush and Pargament (1995), suicidal behavior is often
preceded by thoughts, threats, and unsuccessful attempts at suicide. Similarly, Cole, Protinsky, and
Cross (1992) noted that suicide was the completed process of a continuum that began with suicidal
7

7/31/2019 Att Thy & Suicide New
http://slidepdf.com/reader/full/att-thy-suicide-new 8/31
ideation, followed by an attempt at suicide, and finally completed suicide. Suicidal ideation is a
preoccupation with intrusive thoughts of ending one's own life (Cole, Protinsky, & Cross, 1992; Harter,
Marold, & Whitesell, 1992) while suicide is the completed act of taking ones life (National Mental
Health Association, 2002). Because of this progression from thought to action, it is fitting that
researchers explore the notion of suicidal ideation in greater depth. (Studies referred from Goliath,
2005).
This study examined the phenomenological relationship among stress, self-esteem, and
suicidal ideation in adolescents. Much of the research to date has focused on the associations of stress
and self-esteem to actual suicide but not to ideation. Moreover, the majority of studies have examined
the relationships in clinical populations. Thus, we know little about the associations of these processes
in non-clinical populations. The present study investigated the relationship among cumulative negative
life experiences (stress), self-esteem, and suicidal ideation in a non-clinical population of college
students. Selye (1974) defined stress as a response of the human body to any stimulus that disrupts
the individual's homeostasis. Because these responses are unavoidable, individuals are faced with the
constant urge to maintain internal balance. Accordingly, any experience that affects one's homeostasis
is considered to be stress (Rice, 1992). Social scientists have expanded Hans Selye's notion of
physiological stress to include social, cognitive, and psychological or mental stress. Mullis, Youngs,
Mullis, and Rathge (1993) proposed that stress is a function of an individual's appraisal of a life
stressor and therefore, a cognitive process. Similarly, Lazarus (1993) contended that the extent to
which individuals experience stress is determined by their subjective evaluations of their experiences.
Therefore, if individuals appraise an event as traumatic, they will experience more stress from the
experience than will individuals who appraise the event as non-significant. Researchers (e.g., Bartle-
Haring, Rosen, & Stith, 2002; Ferrer-Wreder, Lorente, Kurtines, Briones, Bussell, Berman, & Arrufat,
2002) have noted the importance of reducing stress by helping youth develop positive perceptions of the self in order to avoid catastrophic socioemotional outcomes such as suicidal behavior. Indeed,
exposure to stress by youth has been linked to severe emotional and psychological problems (Bartle-
Haring, Rosen, & Stith, 2002; Gonzales, Tein, Sandler, & Friedman, 2001), a known precursor to suicide
(Teen suicide, 1998). (Studies referred from Goliath, 2005).
Mc Gee, Williams and Nada-Raja (2001) examined the longitudinal relationship between family
characteristics in early childhood, self-esteem, hopelessness and thoughts of self-harm in the mid-
childhood years, and suicidal ideation at ages 18 and 21. Path analysis was used to establish separate
models for boys and girls. The results suggested different pathways to later suicidal ideation for boys
and girls. For boys, suicidal ideation seemed to have stronger roots in childhood, with significant pathsfrom low self-esteem and hopelessness to early thoughts of self-harm and thence to later ideation. For
girls, self-esteem had a small but significant direct effect on later suicidal ideation. The findings
provide support for the idea that individual characteristics such as feelings of hopelessness and low
self-esteem act as generative mechanisms, linking early childhood family characteristics to suicidal
ideation in early adulthood.
8

7/31/2019 Att Thy & Suicide New
http://slidepdf.com/reader/full/att-thy-suicide-new 9/31
Hong, Li, Fang, Wai, and Xiong (2007) proposed, China accounts for nearly a half of the
suicides in the world, but little is known about the risk factors of suicidal ideation among general
Chinese population. This study examines the association between stressful life events, self-esteem and
suicidal ideation among three community-based samples in China: rural residents, rural-to-urban
migrants and urban residents. Representative samples of rural-to-urban migrants (n=1006) and urban
residents (n=1000) were recruited in Beijing. The sample of rural residents (n=1020) was recruited
from 8 provinces from where 75% of migrant sample originated. All participants completed a cross-
sectional survey. Multivariate logistic regressions were employed for data analyses. The Results
evidenced that Approximately 9.2% of total participants had suicidal ideation in the past 6 months,
and the rate was slightly higher among urban residents and females. A significant dose-response
relationship was observed between the number of stressful life events and suicidal ideation. In
multivariate regression model, both stressful life events and self-esteem were significantly associated
with elevated risk of suicidal ideation among three groups of participants. No moderating effect of self-
esteem was observed in the relationship between stressful life events and suicidal ideation. It was
concluded that Stressful life events and self-esteem were two significant risk factors for suicidal
ideation among Chinese population. Appropriate intervention and education programs that aim at
reducing suicide risks need to consider these two important factors.
Sterud, Hem, Lau, and Ekeberg (2008) produced the first paper on suicidal ideation and
attempts among ambulance personnel. This study aimed to investigate levels of suicidal ideation and
suicide attempts among ambulance personnel, and to identify important correlates and the factors to
which ambulance personnel attribute their serious suicidal ideation. In conclusion, ambulance
personnel reported a moderate level of suicidal ideation and suicide attempts. Although serious
suicidal ideation was rarely attributed to working conditions in general, this study suggests that job-
related factors like emotional exhaustion and bullying may be of importance which greatly lowers theself-esteem.
Wagner, Rouleau, and Joiner (2000) conducted this study to determine whether there are
changes in the cognitive factors of attributional style, hopelessness, and self-esteem when suicidal
ideation fades in psychiatrically hospitalized children and adolescents. The cognitive factors of
attributional style, hopelessness, and self-esteem were assessed in subjects aged 7–17 years (50 with
and 50 without suicidal ideation) at admission and discharge from a psychiatric hospital. The results
revealed: For subjects with suicidal ideation, attributional style became significantly more positive and
hopelessness was decreased from admission to discharge, by which time suicidal ideation had faded.
There was no association between self-esteem and suicidal ideation after control for depression. Thesechanges in cognitive factors were not seen in the group without suicidal ideation. There were no
significant differences between children and adolescents in the pattern of results. It was concluded
that Change in attributional style was shown to be a factor significantly related to the resolution of
suicidal ideation in children and adolescents. This cognitive style could be specifically addressed in
psychotherapy with depressed children and adolescents as a means of reducing suicidal ideation.
These results may have an implication for reducing the length of psychiatric inpatient stays.
9
7/31/2019 Att Thy & Suicide New
http://slidepdf.com/reader/full/att-thy-suicide-new 10/31
Although low self-esteem has been associated with suicidal ideation in adolescents (De Man &
Leduc, 1995), after control for depression in our study, there were no significant changes in the level of
self-esteem when suicidal ideation was resolved. Since self-esteem is a depressive symptom, this
finding is not particularly surprising. This result is consistent with the findings of Marciano and Kazdin
(1994), who reported that self-esteem did not discriminate between children with and without suicidal
ideation when depression was controlled for.
The cognitive model of psychopathology described by Beck (1976) has led to characterization
of the negative thinking that typifies depressed individuals (Beck, 1991). A negative cognitive shift
occurs in which a person disregards positive information and focuses on negative information. This
results in negative beliefs and assumptions. Beck, Steer and Brown (1993) have examined these
dysfunctional attitudes and their relationship to suicidal ideation in adult psychiatric outpatients. They
found that although dysfunctional attitudes such as a need for approval were related to suicidal
ideation, they were not as significantly related as a history of a suicide attempt and the degree of
hopelessness about the future. Pinto and Whisman (1996) reported that negative views of oneself and
others led to negative affect and suicidal ideation in a sample of psychiatrically hospitalized
adolescents.
Attitudinize Psychotherapy Technique includes Motivational Interviewing
elaborated by Group Health Centre for Health Promotion (2003) “client-centered, directive method for
enhancing intrinsic motivation to change by exploring and resolving ambivalence.” The Attitudinize
therapy can be learned by the person / client. The person then needs to take what has been learned,
practice it at home (when they are alone and not feeling self-conscious, for approximately thirty
minutes a day), and through means of repetition, and get that “new learning” down into the brain over
and over again. Just like learning at school or an institution. It enables you to begin believing, feeling
and acting, differently. This takes persistence, practice, and patience, but when a person sticks with
this therapy, and does not give up, noticeable progress begins to occur.
Persistency is the next key. These solutions must be practiced every day for three months or
longer. It is essential that the brain receive these new, rational, forward moving messages so that
attitude can be changed. The neural pathways in the mind "absorb" the attitudinize therapy and it
begins to become a part of the person allowing permanent change to occur. After granting the
intricacies, the mastery of these concepts is needed for treating the emotional problems successfully.
Method
Sample of the present study comprised of 106 Male and 46 Female Adult Students of Iqra
University, Karachi. It was selected through Random Sampling Technique.
Procedure of the study comprises of Two phases. In order to test the hypotheses, the sample
comprised of NO THERAPY GROUP; the Fifty-two Male and Twenty-three Female Adult Students on
which NO Attitudinize Psychotherapy would be conducted, and for ATTITUDINIZE THERAPY GROUP;
10
7/31/2019 Att Thy & Suicide New
http://slidepdf.com/reader/full/att-thy-suicide-new 11/31
Fifty-four Male and Twenty-three Female Adult Students on which Attitudinize Psychotherapy would be
conducted. The data was collected from the Adult students between the ages of 18–25 belonging to
Iqra University, Karachi. In the Initial Phase of BEFORE THERAPY All the Male and Female students were
administered; a) Dysfunctional Attitude Scale (Therapy Form) (Modified by Dr. Linah Askari 2003), b)
Queendom’s Self–Esteem Test (2003) and c) Adult Suicidal Ideation Questionnaire (William & Reynolds,
2005). In the Final Phase of AFTER THERAPY, Attitudinize Therapy was conducted for fourteen weeks
(75 minute session, twice a week) on the ATTITUDINIZE THERAPY GROUP only. At the completion of
this phase the whole sample was Re-administered All the three Scales, to both the students of NO
THERAPY GROUP and the students of ATTITUDINIZE THERAPY GROUP. The purpose was to relate the
effectiveness of the Attitudinize Therapy with the Enhancement of Self – Esteem and Reduction of
Suicidal Ideation within the Adult students.
Statistical Analysis of the obtained scores revealed the significance of differences for the
Enhancement of Self – Esteem through the application of Attitudinize Psychotherapy between the TWO
Groups after completion of the Therapy and No Therapy. The Means, Standard Deviations, Pearson
correlation coefficients, one sample t-test, One Way ANOVA were computed along with Mean-plots,
Mean Graphs, Pie-Charts and Percent Count Graphs for data analysis.
Results
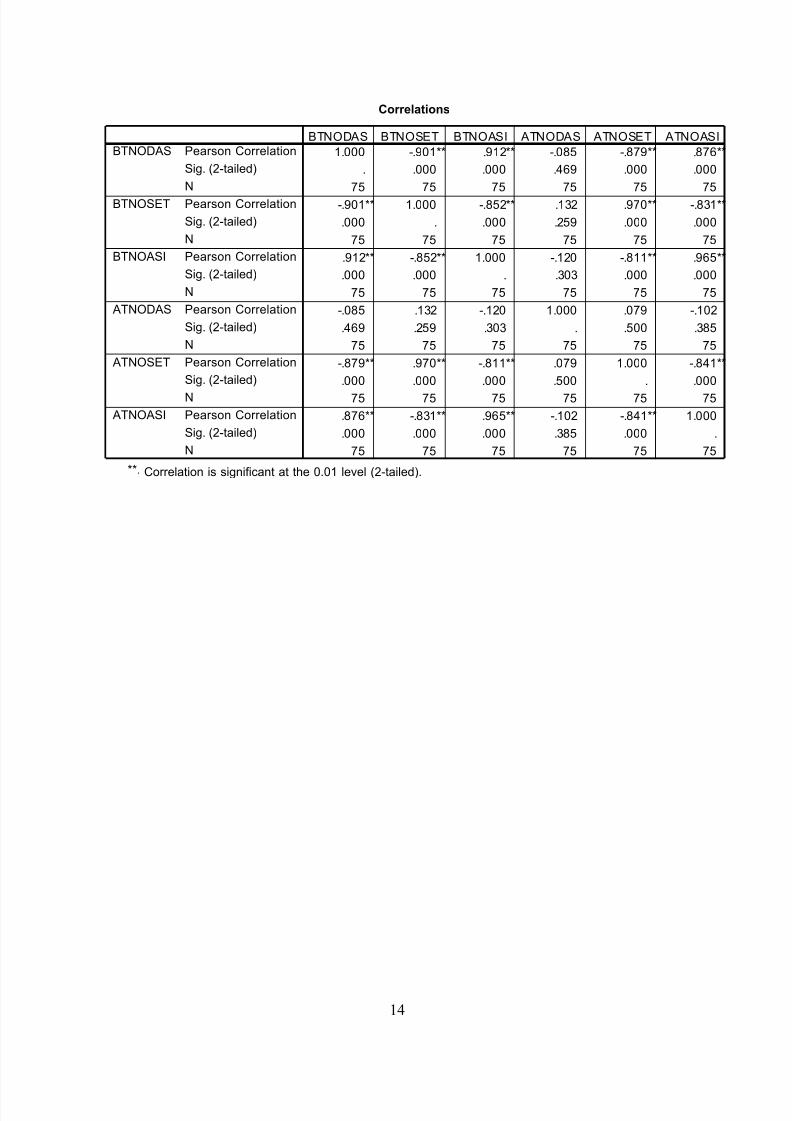
The data was statistically analyzed among the following groups. BTNODAS – “Before Therapy,
No Therapy Group, Dysfunctional Attitude Scale”. BTNOSET – “Before Therapy, No Therapy Group,
Self-Esteem Test”. BTNOASI – “Before Therapy, No Therapy Group, Adult Suicide Ideation
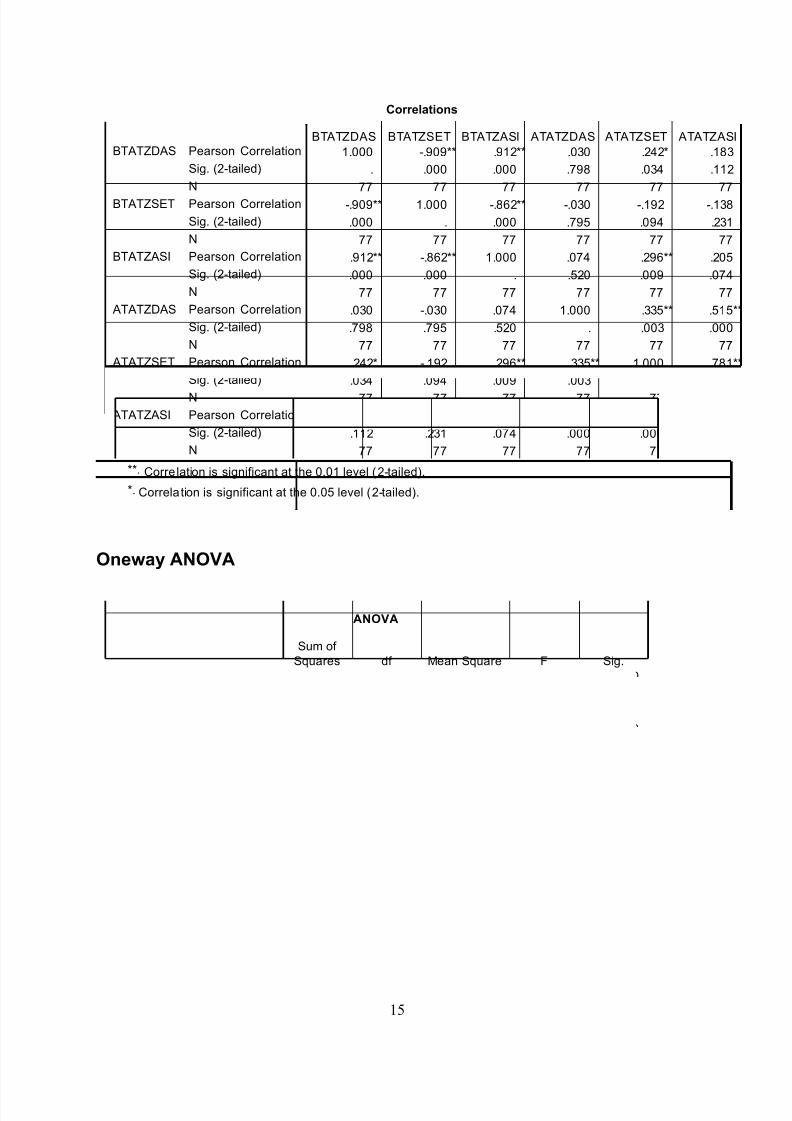
Questionnaire”. BTATZDAS – “Before Therapy, Attitudinize Therapy Group, Dysfunctional Attitude
Scale”. BTATZSET – “Before Therapy, Attitudinize Therapy Group, Self-Esteem Test”. BTATZASI –
“Before Therapy, Attitudinize Therapy Group, Adult Suicide Ideation Questionnaire”.
ATNODAS – “After Therapy, No Therapy Group, Dysfunctional Attitude Scale”. ATNOSET –
“After Therapy, No Therapy Group, Self-Esteem Test”. ATNOASI – “After Therapy, No Therapy Group,
Adult Suicide Ideation Questionnaire”. ATATZDAS – “After Therapy, Attitudinize Therapy Group,
Dysfunctional Attitude Scale”. ATATZSET – “After Therapy, Attitudinize Therapy Group, Self-Esteem
Test”. ATATZASI – “After Therapy, Attitudinize Therapy Group, Adult Suicide Ideation Questionnaire”.
The following Hypotheses proved their significance through the statistical analysis, and the
summarized results are presented below:
1) There is More Positive Correlation between scores of Dysfunctional Attitudes and Suicidal
Ideation, i.e., The Higher the Dysfunctional Attitudes the Higher will be the Suicidal Ideation,
and Vice Versa.
2) There is More Negative Correlation between scores of Dysfunctional Attitudes and Self-Esteem,
i.e., The Higher the Dysfunctional Attitudes the Lower will be the Self-Esteem, and Vice Versa.
11
7/31/2019 Att Thy & Suicide New
http://slidepdf.com/reader/full/att-thy-suicide-new 12/31
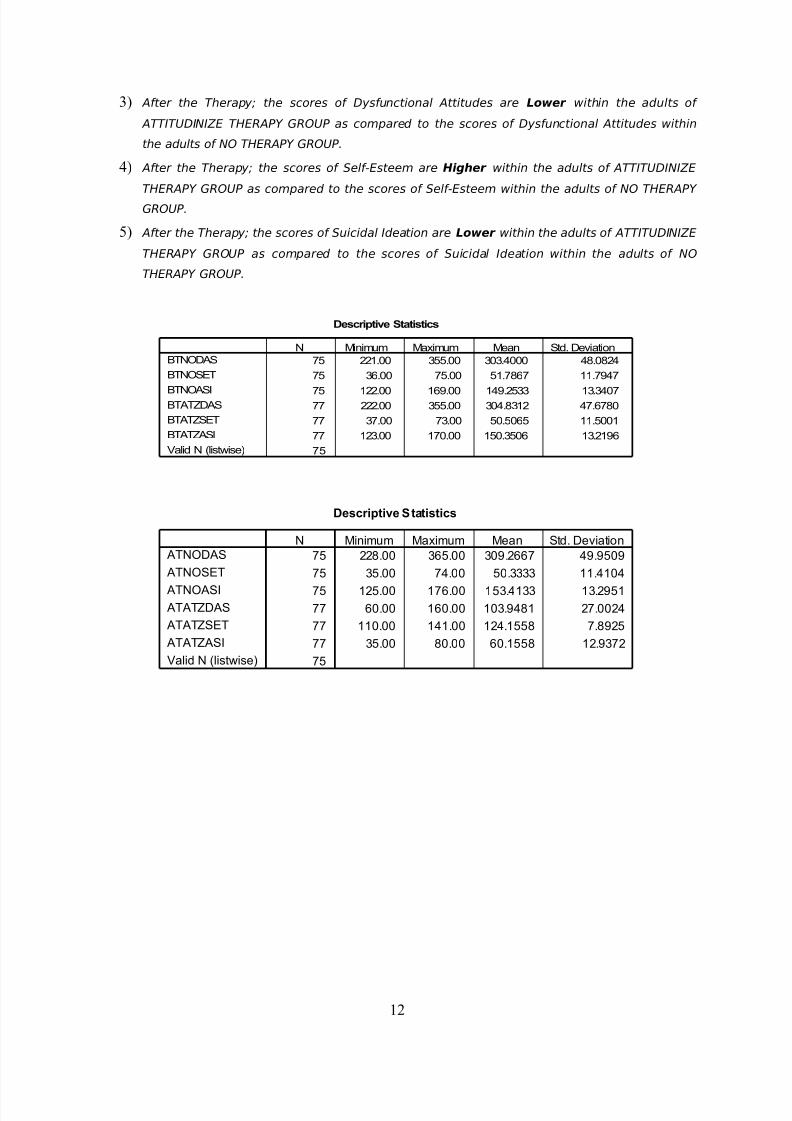
3) After the Therapy; the scores of Dysfunctional Attitudes are Lower within the adults of
ATTITUDINIZE THERAPY GROUP as compared to the scores of Dysfunctional Attitudes within
the adults of NO THERAPY GROUP.
4) After the Therapy; the scores of Self-Esteem are Higher within the adults of ATTITUDINIZE
THERAPY GROUP as compared to the scores of Self-Esteem within the adults of NO THERAPY
GROUP.
5) After the Therapy; the scores of Suicidal Ideation are Lower within the adults of ATTITUDINIZE
THERAPY GROUP as compared to the scores of Suicidal Ideation within the adults of NO
THERAPY GROUP.
Descriptive Statistics
75 221.00 355.00 303.4000 48.0824
75 36.00 75.00 51.7867 11.7947
75 122.00 169.00 149.2533 13.340777 222.00 355.00 304.8312 47.6780
77 37.00 73.00 50.5065 11.5001
77 123.00 170.00 150.3506 13.2196
75
BTNODAS
BTNOSET
BTNOASIBTATZDAS
BTATZSET
BTATZASI
Valid N (listwise)
N Minimum Maximum Mean Std. Deviation
Descriptive Statistics
75 228.00 365.00 309.2667 49.9509
75 35.00 74.00 50.3333 11.4104
75 125.00 176.00 153.4133 13.2951
77 60.00 160.00 103.9481 27.0024
77 110.00 141.00 124.1558 7.8925
77 35.00 80.00 60.1558 12.9372
75
ATNODAS
ATNOSET
ATNOASI ATATZDAS
ATATZSET
ATATZASI
Valid N (listwise)
N Minimum Maximum Mean Std. Deviation
12
7/31/2019 Att Thy & Suicide New
http://slidepdf.com/reader/full/att-thy-suicide-new 13/31
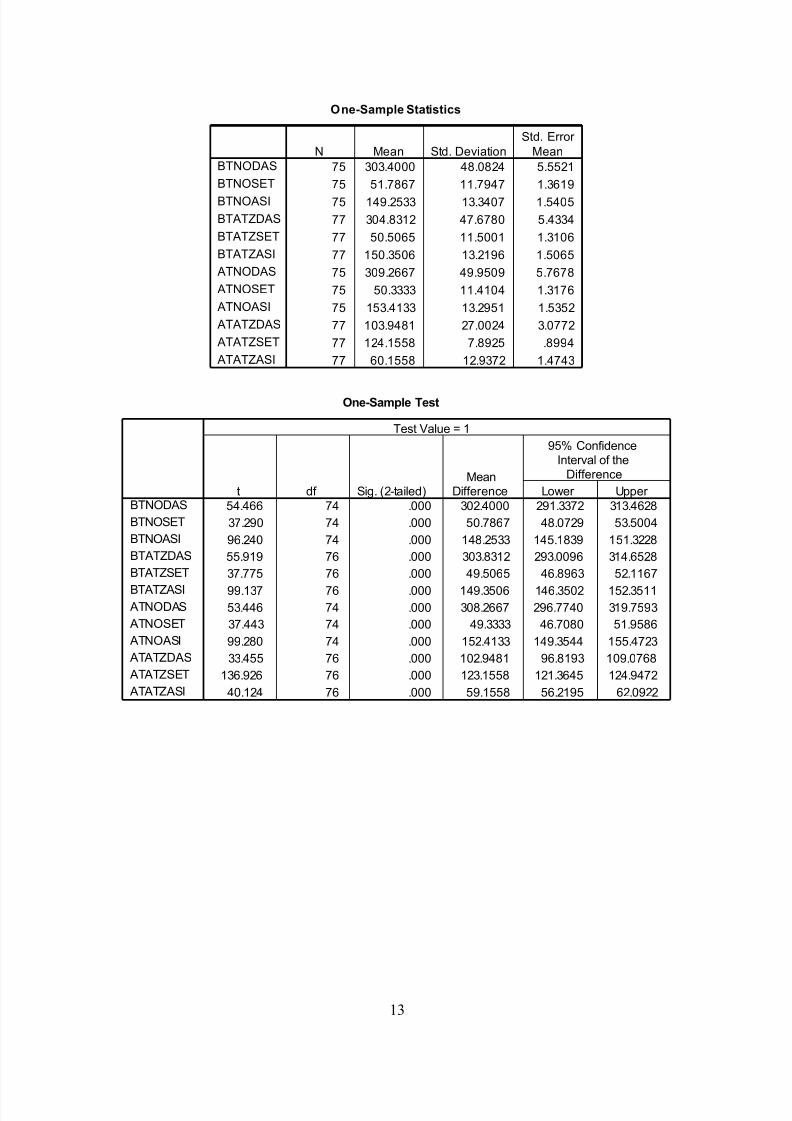
One-Sample Statistics
75 303.4000 48.0824 5.5521
75 51.7867 11.7947 1.3619
75 149.2533 13.3407 1.5405
77 304.8312 47.6780 5.4334
77 50.5065 11.5001 1.3106
77 150.3506 13.2196 1.5065
75 309.2667 49.9509 5.7678
75 50.3333 11.4104 1.3176
75 153.4133 13.2951 1.5352
77 103.9481 27.0024 3.0772
77 124.1558 7.8925 .8994
77 60.1558 12.9372 1.4743
BTNODAS
BTNOSET
BTNOASI
BTATZDAS
BTATZSET
BTATZASI
ATNODAS
ATNOSET
ATNOASI
ATATZDAS
ATATZSET
ATATZASI
N Mean Std. Deviation
Std. Error
Mean
One-Sample Test
54.466 74 .000 302.4000 291.3372 313.4628
37.290 74 .000 50.7867 48.0729 53.5004
96.240 74 .000 148.2533 145.1839 151.3228
55.919 76 .000 303.8312 293.0096 314.6528
37.775 76 .000 49.5065 46.8963 52.1167
99.137 76 .000 149.3506 146.3502 152.351153.446 74 .000 308.2667 296.7740 319.7593
37.443 74 .000 49.3333 46.7080 51.9586
99.280 74 .000 152.4133 149.3544 155.4723
33.455 76 .000 102.9481 96.8193 109.0768
136.926 76 .000 123.1558 121.3645 124.9472
40.124 76 .000 59.1558 56.2195 62.0922
BTNODAS
BTNOSET
BTNOASI
BTATZDAS
BTATZSET
BTATZASI ATNODAS
ATNOSET
ATNOASI
ATATZDAS
ATATZSET
ATATZASI
t df Sig. (2-tailed)Mean
Difference Lower Upper
95% ConfidenceInterval of the
Difference
Test Value = 1
13
7/31/2019 Att Thy & Suicide New
http://slidepdf.com/reader/full/att-thy-suicide-new 14/31
Correlations
1.000 -.901** .912** -.085 -.879** .876**
. .000 .000 .469 .000 .000
75 75 75 75 75 75
-.901** 1.000 -.852** .132 .970** -.831**
.000 . .000 .259 .000 .000
75 75 75 75 75 75
.912** -.852** 1.000 -.120 -.811** .965**
.000 .000 . .303 .000 .000
75 75 75 75 75 75
-.085 .132 -.120 1.000 .079 -.102
.469 .259 .303 . .500 .385
75 75 75 75 75 75
-.879** .970** -.811** .079 1.000 -.841**
.000 .000 .000 .500 . .000
75 75 75 75 75 75
.876** -.831** .965** -.102 -.841** 1.000
.000 .000 .000 .385 .000 .
75 75 75 75 75 75
Pearson Correlation
Sig. (2-tailed)
N
Pearson Correlation
Sig. (2-tailed)
N
Pearson Correlation
Sig. (2-tailed)
N
Pearson Correlation
Sig. (2-tailed)
N
Pearson Correlation
Sig. (2-tailed)
N
Pearson Correlation
Sig. (2-tailed)
N
BTNODAS
BTNOSET
BTNOASI
ATNODAS
ATNOSET
ATNOASI
BTNODAS BTNOSET BTNOASI ATNODAS ATNOSET ATNOASI
Correlation is significant at the 0.01 level (2-tailed).**.
14
7/31/2019 Att Thy & Suicide New
http://slidepdf.com/reader/full/att-thy-suicide-new 15/31
Correlations
1.000 -.909** .912** .030 .242* .183
. .000 .000 .798 .034 .112
77 77 77 77 77 77
-.909** 1.000 -.862** -.030 -.192 -.138
.000 . .000 .795 .094 .231
77 77 77 77 77 77
.912** -.862** 1.000 .074 .296** .205
.000 .000 . .520 .009 .074
77 77 77 77 77 77
.030 -.030 .074 1.000 .335** .515**
.798 .795 .520 . .003 .000
77 77 77 77 77 77
.242* -.192 .296** .335** 1.000 .781**
.034 .094 .009 .003 . .000
77 77 77 77 77 77
.183 -.138 .205 .515** .781** 1.000
.112 .231 .074 .000 .000 .
77 77 77 77 77 77
Pearson Correlation
Sig. (2-tailed)
N
Pearson Correlation
Sig. (2-tailed)
N
Pearson Correlation
Sig. (2-tailed)
N
Pearson Correlation
Sig. (2-tailed)
N
Pearson Correlation
Sig. (2-tailed)
N
Pearson Correlation
Sig. (2-tailed)
N
BTATZDAS
BTATZSET
BTATZASI
ATATZDAS
ATATZSET
ATATZASI
BTATZDAS BTATZSET BTATZASI ATATZDAS ATATZSET ATATZASI
Correlation is significant at the 0.01 level (2-tailed).**.
Correlation is significant at the 0.05 level (2-tailed).*.
Oneway ANOVA
ANOVA
9983.087 52 191.982 13.559 .000
311.500 22 14.159
10294.587 74
12300.353 52 236.545 5.983 .000
869.833 22 39.538
13170.187 74
Between Groups
Within Groups
Total
Between Groups
Within Groups
Total
BTNOSET
BTNOASI
Sum of
Squares df Mean Square F Sig.
15
7/31/2019 Att Thy & Suicide New
http://slidepdf.com/reader/full/att-thy-suicide-new 16/31
Means Plots
BTNODAS
354.00
351.00
348.00
344.00
340.00
337.00
333.00
328.00
322.00
315.00
305.00
255.00
247.00
243.00
235.00
230.00
226.00
221.00
M e a n o f B T N O S E T
80
70
60
50
40
30
BTNODAS
354.00
351.00
348.00
344.00
340.00
337.00
333.00
328.00
322.00
315.00
305.00
255.00
247.00
243.00
235.00
230.00
226.00
221.00
M e a n o f B T N O A S I
180
170
160
150
140
130
120
110
Oneway ANOVA
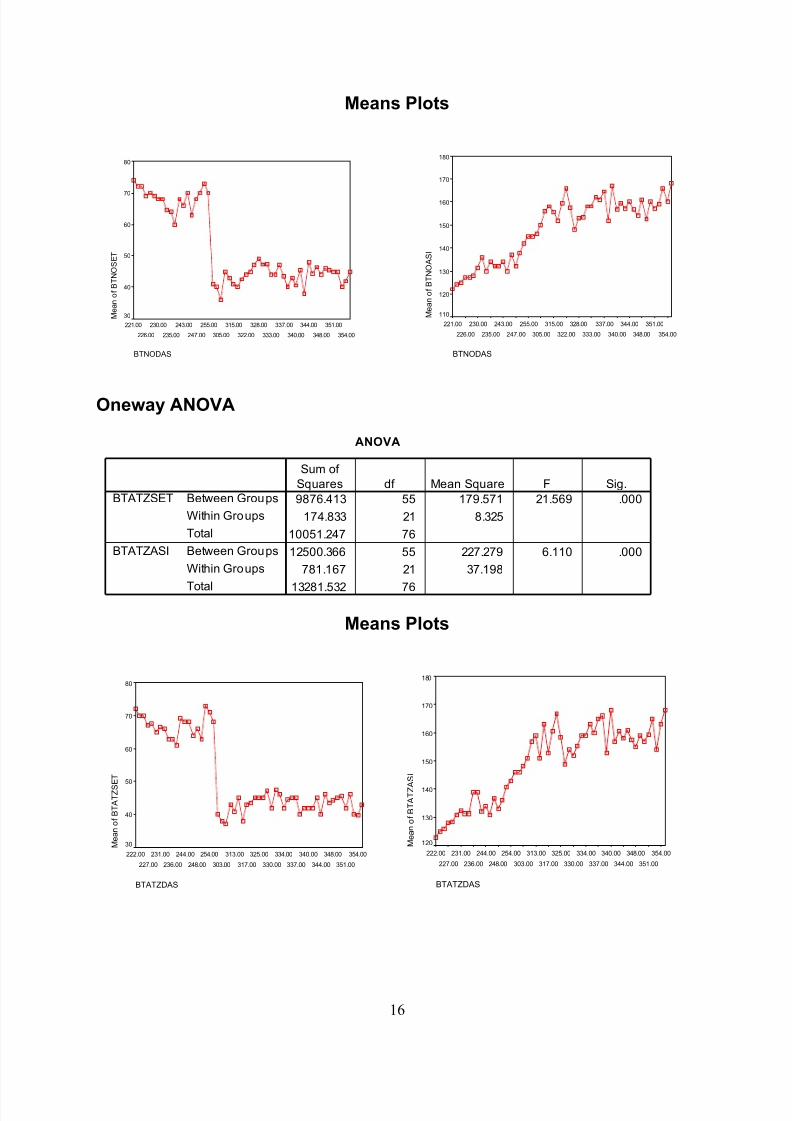
ANOVA
9876.413 55 179.571 21.569 .000
174.833 21 8.325
10051.247 76
12500.366 55 227.279 6.110 .000
781.167 21 37.198
13281.532 76
Between Groups
Within Groups
Total
Between Groups
Within Groups
Total
BTATZSET
BTATZASI
Sum of
Squares df Mean Square F Sig.
Means Plots
BTATZDAS
354.00
351.00
348.00
344.00
340.00
337.00
334.00
330.00
325.00
317.00
313.00
303.00
254.00
248.00
244.00
236.00
231.00
227.00
222.00
M e a n o f B T A T Z S E T
80
70
60
50
40
30
BTATZDAS
354.00
351.00
348.00
344.00
340.00
337.00
334.00
330.00
325.00
317.00
313.00
303.00
254.00
248.00
244.00
236.00
231.00
227.00
222.00
M e a n o f B T A T Z A
S I
180
170
160
150
140
130
120
16
7/31/2019 Att Thy & Suicide New
http://slidepdf.com/reader/full/att-thy-suicide-new 17/31
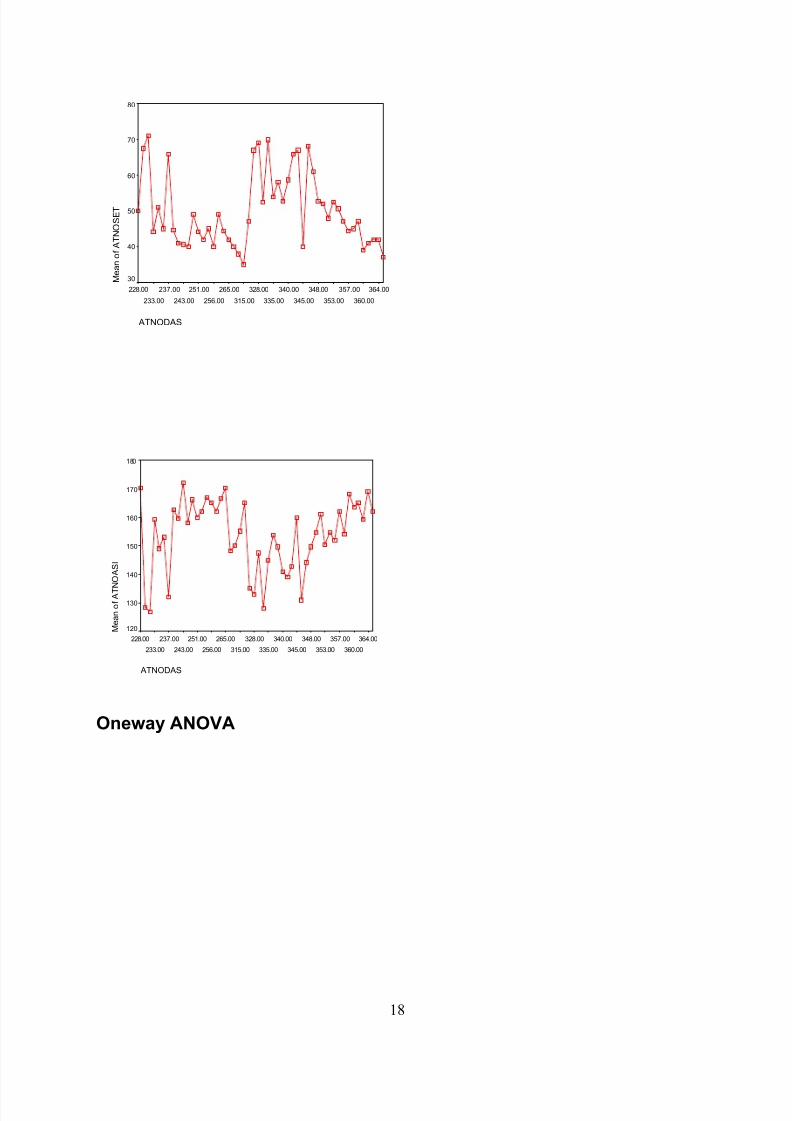
Oneway ANOVA
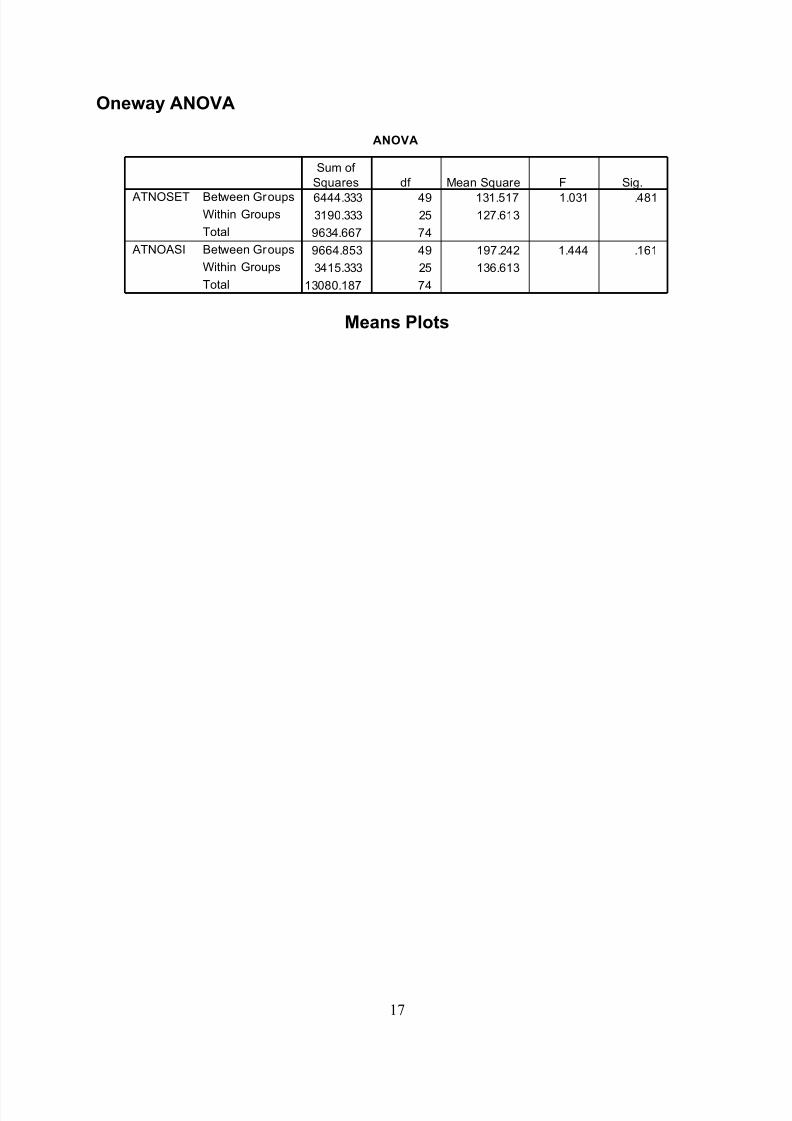
ANOVA
6444.333 49 131.517 1.031 .481
3190.333 25 127.613
9634.667 74
9664.853 49 197.242 1.444 .161
3415.333 25 136.613
13080.187 74
Between GroupsWithin Groups
Total
Between Groups
Within Groups
Total
ATNOSET
ATNOASI
Sum of
Squares df Mean Square F Sig.
Means Plots
17
7/31/2019 Att Thy & Suicide New
http://slidepdf.com/reader/full/att-thy-suicide-new 18/31
ATNODAS
364.00
360.00
357.00
353.00
348.00
345.00
340.00
335.00
328.00
315.00
265.00
256.00
251.00
243.00
237.00
233.00
228.00
M e a n o f A T N O S E T
80
70
60
50
40
30
ATNODAS
364.00
360.00
357.00
353.00
348.00
345.00
340.00
335.00
328.00
315.00
265.00
256.00
251.00
243.00
237.00
233.00
228.00
M e a n o f A T N O A S I
180
170
160
150
140
130
120
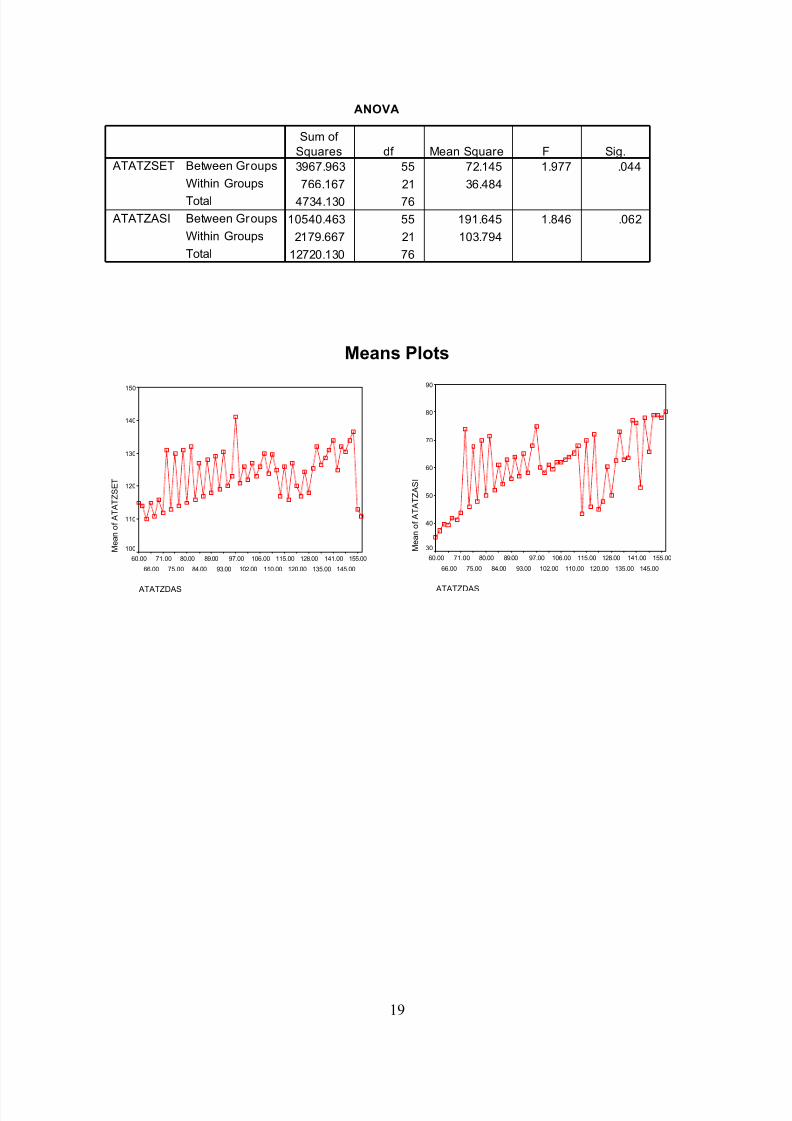
Oneway ANOVA
18
7/31/2019 Att Thy & Suicide New
http://slidepdf.com/reader/full/att-thy-suicide-new 19/31
ANOVA
3967.963 55 72.145 1.977 .044
766.167 21 36.484
4734.130 76
10540.463 55 191.645 1.846 .062
2179.667 21 103.794
12720.130 76
Between Groups
Within Groups
Total
Between Groups
Within Groups
Total
ATATZSET
ATATZASI
Sum of
Squares df Mean Square F Sig.
Means Plots
ATATZDAS
155.00
145.00
141.00
135.00
128.00
120.00
115.00
110.00
106.00
102.00
97.00
93.00
89.00
84.00
80.00
75.00
71.00
66.00
60.00
M e a n o f A T A T Z S E T
150
140
130
120
110
100
ATATZDAS
155.00
145.00
141.00
135.00
128.00
120.00
115.00
110.00
106.00
102.00
97.00
93.00
89.00
84.00
80.00
75.00
71.00
66.00
60.00
M e a n o f A T A T Z A S I
90
80
70
60
50
40
30
19
7/31/2019 Att Thy & Suicide New
http://slidepdf.com/reader/full/att-thy-suicide-new 20/31
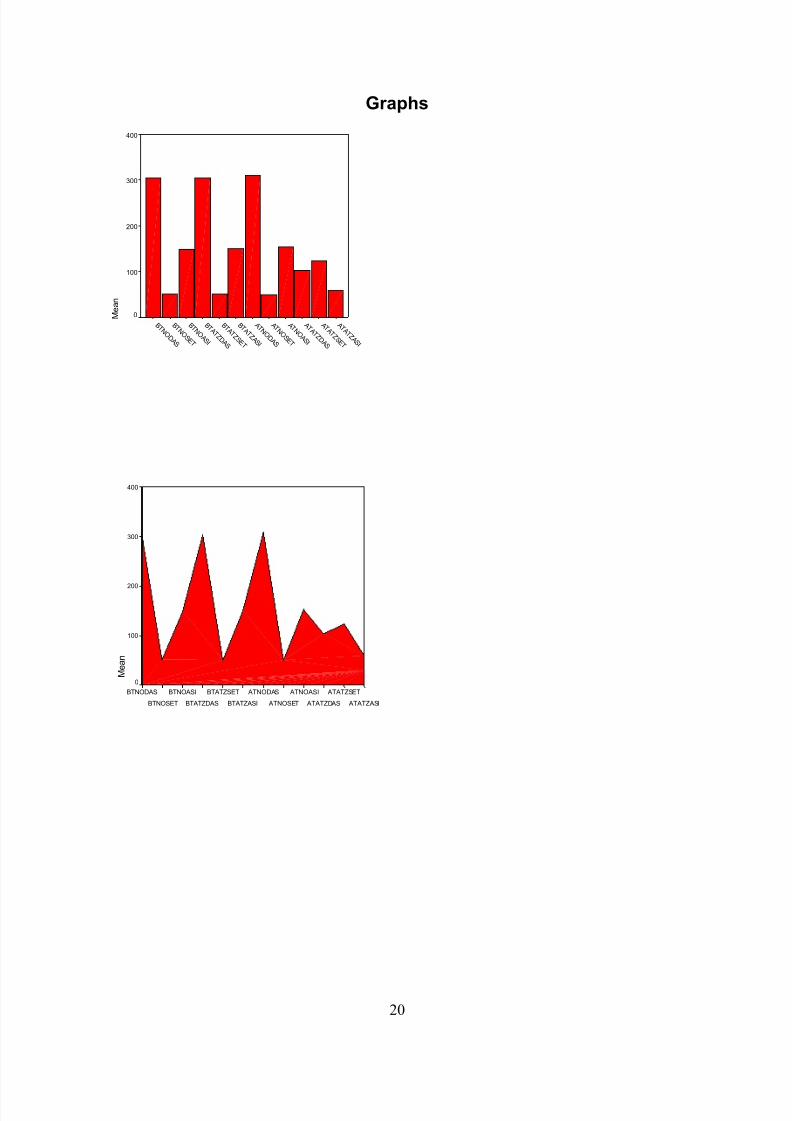
Graphs
A T A T Z A S I
A T A T Z S E T
A T A T Z D A S
A T N O A S I
A T N O S E T
A T N O D A S
B T A T Z A S I
B T A T Z S E T
B T A T Z D A S
B T N O A S I
B T N O S E T
B T N O D A S
M e a n
400
300
200
100
0
ATATZASI
ATATZSET
ATATZDAS
ATNOASI
ATNOSET
ATNODAS
BTATZASI
BTATZSET
BTATZDAS
BTNOASI
BTNOSET
BTNODAS
M e a n
400
300
200
100
0
20
7/31/2019 Att Thy & Suicide New
http://slidepdf.com/reader/full/att-thy-suicide-new 21/31
ATATZASI
ATATZSET
ATATZDAS
ATNOASI
ATNOSET
ATNODAS
BTATZASI BTATZSET
BTATZDAS
BTNOASI
BTNOSET
BTNODAS
A T N O S E T
B T A T Z S E T
B T N O S E T
A T A T Z A S I
A T A T Z D A S
A T A T Z S E T
B T N O A S I
B T A T Z A S I
A T N O A S I
B T N O D A S
B T A T Z D A S
A T N O D A S
C o u n t
160000
140000
120000
100000
80000
60000
40000
20000
0
P er c en t
100
50
077399316111941126511506
227552281223195
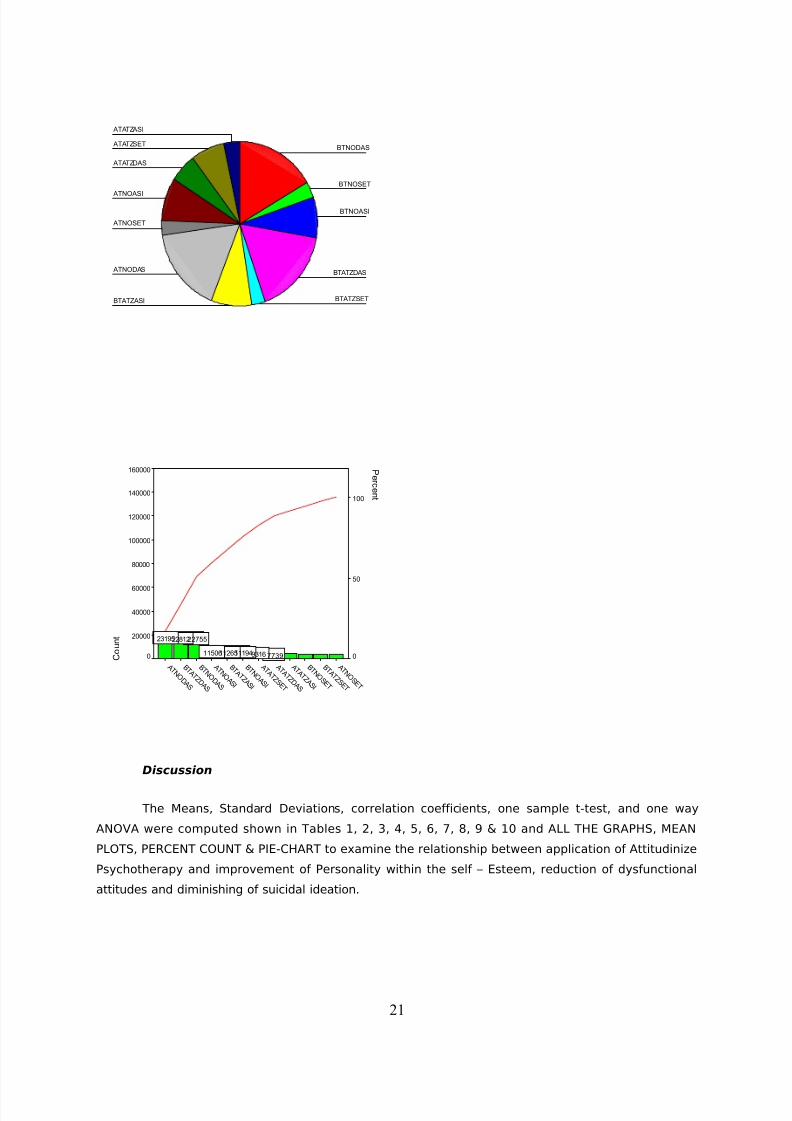
Discussion
The Means, Standard Deviations, correlation coefficients, one sample t-test, and one way
ANOVA were computed shown in Tables 1, 2, 3, 4, 5, 6, 7, 8, 9 & 10 and ALL THE GRAPHS, MEAN
PLOTS, PERCENT COUNT & PIE-CHART to examine the relationship between application of Attitudinize
Psychotherapy and improvement of Personality within the self – Esteem, reduction of dysfunctional
attitudes and diminishing of suicidal ideation.
21
7/31/2019 Att Thy & Suicide New
http://slidepdf.com/reader/full/att-thy-suicide-new 22/31
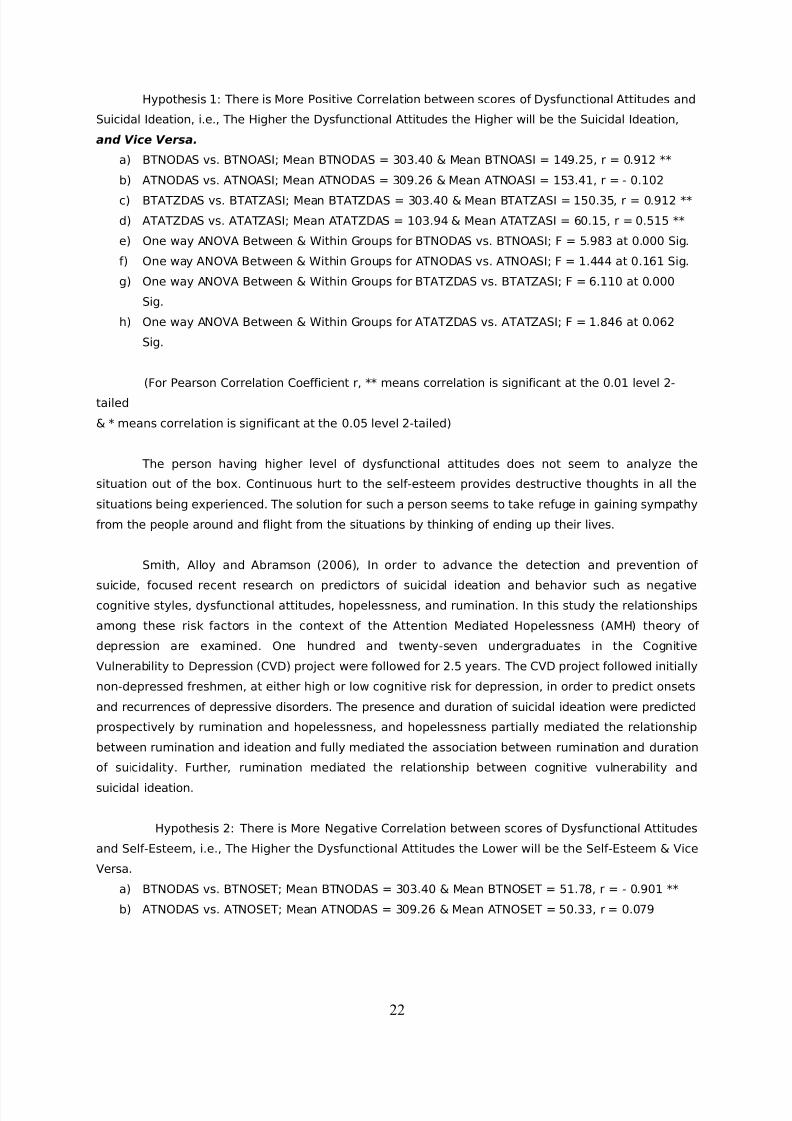
Hypothesis 1: There is More Positive Correlation between scores of Dysfunctional Attitudes and
Suicidal Ideation, i.e., The Higher the Dysfunctional Attitudes the Higher will be the Suicidal Ideation,
and Vice Versa.
a) BTNODAS vs. BTNOASI; Mean BTNODAS = 303.40 & Mean BTNOASI = 149.25, r = 0.912 **
b) ATNODAS vs. ATNOASI; Mean ATNODAS = 309.26 & Mean ATNOASI = 153.41, r = - 0.102
c) BTATZDAS vs. BTATZASI; Mean BTATZDAS = 303.40 & Mean BTATZASI = 150.35, r = 0.912 **
d) ATATZDAS vs. ATATZASI; Mean ATATZDAS = 103.94 & Mean ATATZASI = 60.15, r = 0.515 **
e) One way ANOVA Between & Within Groups for BTNODAS vs. BTNOASI; F = 5.983 at 0.000 Sig.
f) One way ANOVA Between & Within Groups for ATNODAS vs. ATNOASI; F = 1.444 at 0.161 Sig.
g) One way ANOVA Between & Within Groups for BTATZDAS vs. BTATZASI; F = 6.110 at 0.000
Sig.
h) One way ANOVA Between & Within Groups for ATATZDAS vs. ATATZASI; F = 1.846 at 0.062
Sig.
(For Pearson Correlation Coefficient r, ** means correlation is significant at the 0.01 level 2-
tailed
& * means correlation is significant at the 0.05 level 2-tailed)
The person having higher level of dysfunctional attitudes does not seem to analyze the
situation out of the box. Continuous hurt to the self-esteem provides destructive thoughts in all the
situations being experienced. The solution for such a person seems to take refuge in gaining sympathy
from the people around and flight from the situations by thinking of ending up their lives.
Smith, Alloy and Abramson (2006), In order to advance the detection and prevention of
suicide, focused recent research on predictors of suicidal ideation and behavior such as negativecognitive styles, dysfunctional attitudes, hopelessness, and rumination. In this study the relationships
among these risk factors in the context of the Attention Mediated Hopelessness (AMH) theory of
depression are examined. One hundred and twenty-seven undergraduates in the Cognitive
Vulnerability to Depression (CVD) project were followed for 2.5 years. The CVD project followed initially
non-depressed freshmen, at either high or low cognitive risk for depression, in order to predict onsets
and recurrences of depressive disorders. The presence and duration of suicidal ideation were predicted
prospectively by rumination and hopelessness, and hopelessness partially mediated the relationship
between rumination and ideation and fully mediated the association between rumination and duration
of suicidality. Further, rumination mediated the relationship between cognitive vulnerability and
suicidal ideation.
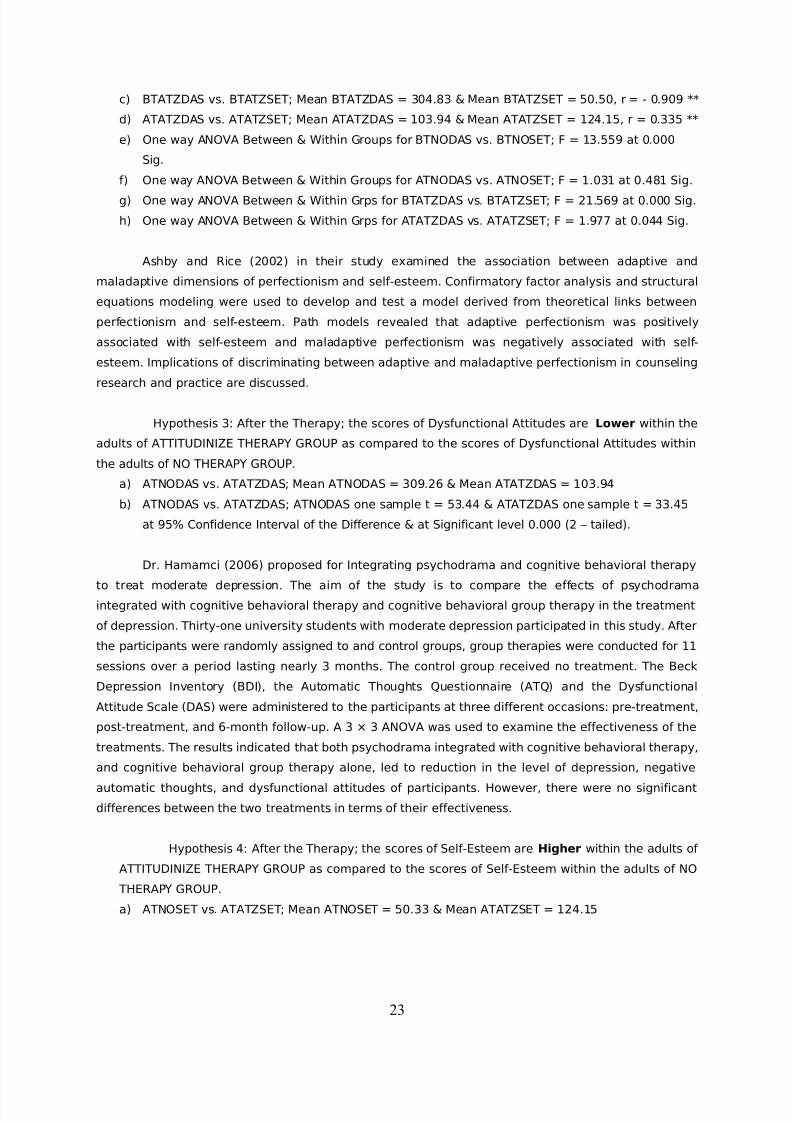
Hypothesis 2: There is More Negative Correlation between scores of Dysfunctional Attitudes
and Self-Esteem, i.e., The Higher the Dysfunctional Attitudes the Lower will be the Self-Esteem & Vice
Versa.
a) BTNODAS vs. BTNOSET; Mean BTNODAS = 303.40 & Mean BTNOSET = 51.78, r = - 0.901 **
b) ATNODAS vs. ATNOSET; Mean ATNODAS = 309.26 & Mean ATNOSET = 50.33, r = 0.079
22
7/31/2019 Att Thy & Suicide New
http://slidepdf.com/reader/full/att-thy-suicide-new 23/31
c) BTATZDAS vs. BTATZSET; Mean BTATZDAS = 304.83 & Mean BTATZSET = 50.50, r = - 0.909 **
d) ATATZDAS vs. ATATZSET; Mean ATATZDAS = 103.94 & Mean ATATZSET = 124.15, r = 0.335 **
e) One way ANOVA Between & Within Groups for BTNODAS vs. BTNOSET; F = 13.559 at 0.000
Sig.
f) One way ANOVA Between & Within Groups for ATNODAS vs. ATNOSET; F = 1.031 at 0.481 Sig.
g) One way ANOVA Between & Within Grps for BTATZDAS vs. BTATZSET; F = 21.569 at 0.000 Sig.
h) One way ANOVA Between & Within Grps for ATATZDAS vs. ATATZSET; F = 1.977 at 0.044 Sig.
Ashby and Rice (2002) in their study examined the association between adaptive and
maladaptive dimensions of perfectionism and self-esteem. Confirmatory factor analysis and structural
equations modeling were used to develop and test a model derived from theoretical links between
perfectionism and self-esteem. Path models revealed that adaptive perfectionism was positively
associated with self-esteem and maladaptive perfectionism was negatively associated with self-
esteem. Implications of discriminating between adaptive and maladaptive perfectionism in counseling
research and practice are discussed.
Hypothesis 3: After the Therapy; the scores of Dysfunctional Attitudes are Lower within the
adults of ATTITUDINIZE THERAPY GROUP as compared to the scores of Dysfunctional Attitudes within
the adults of NO THERAPY GROUP.
a) ATNODAS vs. ATATZDAS; Mean ATNODAS = 309.26 & Mean ATATZDAS = 103.94
b) ATNODAS vs. ATATZDAS; ATNODAS one sample t = 53.44 & ATATZDAS one sample t = 33.45
at 95% Confidence Interval of the Difference & at Significant level 0.000 (2 – tailed).
Dr. Hamamci (2006) proposed for Integrating psychodrama and cognitive behavioral therapy
to treat moderate depression. The aim of the study is to compare the effects of psychodramaintegrated with cognitive behavioral therapy and cognitive behavioral group therapy in the treatment
of depression. Thirty-one university students with moderate depression participated in this study. After
the participants were randomly assigned to and control groups, group therapies were conducted for 11
sessions over a period lasting nearly 3 months. The control group received no treatment. The Beck
Depression Inventory (BDI), the Automatic Thoughts Questionnaire (ATQ) and the Dysfunctional
Attitude Scale (DAS) were administered to the participants at three different occasions: pre-treatment,
post-treatment, and 6-month follow-up. A 3 × 3 ANOVA was used to examine the effectiveness of the
treatments. The results indicated that both psychodrama integrated with cognitive behavioral therapy,
and cognitive behavioral group therapy alone, led to reduction in the level of depression, negative
automatic thoughts, and dysfunctional attitudes of participants. However, there were no significant
differences between the two treatments in terms of their effectiveness.
Hypothesis 4: After the Therapy; the scores of Self-Esteem are Higher within the adults of
ATTITUDINIZE THERAPY GROUP as compared to the scores of Self-Esteem within the adults of NO
THERAPY GROUP.
a) ATNOSET vs. ATATZSET; Mean ATNOSET = 50.33 & Mean ATATZSET = 124.15
23

7/31/2019 Att Thy & Suicide New
http://slidepdf.com/reader/full/att-thy-suicide-new 24/31
b) ATNOSET vs. ATATZSET; ATNOSET one sample t = 37.44 & ATATZSET one sample t = 136.92
at 95% Confidence Interval of the Difference & at Significant level 0.000 (2 – tailed).
Powell, Newgent and Lee (2006) in this study on Group cinema therapy proposed for using
metaphor to enhance adolescent self-esteem. It examines the effectiveness of a cinema therapy
intervention at enhancing the perceived self-esteem of 16 youth with a serious emotional disturbance.Participants completed the Rosenberg Self-Esteem Scale (RSE) at pre-, post-, and 1-week follow-up
within a 6-week coping skills group in which a brief cinema therapy intervention is introduced to a
treatment and delayed treatment group. A control group was used, which only received the coping
skills training. Results of a split-plot analysis of variance (ANOVA) with one between-groups factor and
one repeated-measures factor revealed no significant differences within or between groups, however,
meaningful differences between the three groups were found. Implications for counselors and
therapists are discussed.
Hypothesis 5: After the Therapy; the scores of Suicidal Ideation are Lower within the
adults of ATTITUDINIZE THERAPY GROUP as compared to the scores of Suicidal Ideation within theadults of NO THERAPY GROUP.
c) ATNOASI vs. ATATZASI; Mean ATNOASI = 153.41 & Mean ATATZASI = 60.15
d) ATNOASI vs. ATATZASI; ATNOASI one sample t = 99.28 & ATATZASI one sample t = 40.12 at
95% Confidence Interval of the Difference & at Significant level 0.000 (2 – tailed).
Schwenk (2004) studied upon Reducing Suicidal Ideation in Elders, stating it is Possible, but
Expensive. Primary care-based interventions to reduce suicide risk in older patients are appealing but
are relatively unstudied. Researchers enrolled 598 elders (age, >60) with depression diagnoses from
20 primary care practices in the U.S. in a 1-year trial of a primary care-based intervention. Practices
were randomized to provide usual care or intervention. The intervention consisted of physician
education (with algorithmic approaches to depression treatment); trained care managers with mental
health expertise who provided treatment recommendations, clinical monitoring, and frequent follow-
up; and financial support for medication (citalopram, supplied by the manufacturer) and
psychotherapy. Results reveal, In the intervention group, the prevalence of suicidal ideation dropped
from 29% at baseline to 17% at 8 months and to 15% at 12 months. In the usual-care group, the
prevalence dropped from 20% at baseline to 19% at 8 months and to 13% at 12 months. Given the
higher baseline prevalence in the intervention group, the decline at 8 months was significantly greater
in the intervention group than in the usual-care group. Compared with usual care, intervention yielded
significantly larger declines in depression severity (measured by questionnaire scores) at 4, 8, and 12
months; number of patients in remission at 8 or 12 months was similar in both groups. Actual suicide
attempts were too uncommon to evaluate (one in each group). The statistical significance of the
decline in the suicidal ideation rate with intervention derives mostly from an unexplained higher
baseline rate in the intervention group than in the usual-care group. Intervention costs were not
calculated, but clearly this approach was expensive and probably could not be supported in usual
practice. We would have learned more from this study if medication and psychotherapy had been
provided at no cost to both groups.
24
7/31/2019 Att Thy & Suicide New
http://slidepdf.com/reader/full/att-thy-suicide-new 25/31
Statistically significant results reveal that Attitudinize Psychotherapy employs a positive,
active, educational approach that focuses on how to change the attitudes and on seeking solutions
rather than just simply talking about the past or “exploring” ones feelings and problems. Attitudinize
Psychotherapy is typically provided within an emotionally supportive, empathic relationship, giving
opportunity to express feelings and receive caring in addition to working directly on positive attitude
change in thinking and lifestyle. The treatment is often short term because it is based on a clear
attitude conceptualization that guides the treatment process. Attitudinize Psychotherapy emphasizes a
collaborative relationship between the therapist and the client wherein they work together to specify
goals and to implement the treatment strategies. Each client is assisted in using strategies /
techniques that will help in resolving current areas of difficulty as well as learning skills that will be
useful in preventing relapse and in dealing with future life challenges.
Attitudinize Psychotherapy directly teaches specific ways to examine and correct dysfunctional
thinking patterns or beliefs, those that are causing or contributing to problems in ones life within the
personality. Behavioral strategies are often used with Attitudinize Psychotherapy to develop skills such
as assertiveness or problem solving. Often we need “reality experiments” to prove to ourselves that
what we fear really is not true, or that we could cope with particular circumstances, or that we are
capable of changing certain habits, or that we can easily delete our own low self – esteem and lack of
confidence, by learning and practicing an effective personality improving strategy. The results of this
type of therapy may include a sense of freedom from old patterns, greater opportunity to pursue new
life opportunities, improve personality to a maximum level, reduce distress, and enhance a greater
sense of confidence and self-esteem.
Ramakrishna was born with congenital cataract. By the age of 22, he was totally blind.
Today he is General Manager with the Industrial Development Bank of India. He credits his
mathematical ability and technology as the two most important pillars of his success. We will let his
words do the talking and reflect on his journey to success. Ramakrishna (2007) says:
“I often question myself, did I really succeed? If so what is the success formula? What is that I
would like to share with those who want to succeed? Well, I believe success is a journey, not a
destination. I invented a secret recipe of success, which unlike the three or so routine courses of meal,
has eight courses to taste and dwell on. These are: vIsion, Dream, focUs, dirEction, mind Tuning,
Toughness, perseverAnce and sTruggle. Now collect the capitalized letters of these eight steps and
reshuffle them to form the mantra of my success ‘ATTITUDE’.”
Conclusion
It is imperative to constantly keep a check on ones attitudes (cognition/thought, feeling and
behavior) in all the six dimensions i.e., Physiologically, Psychologically, Terminologically, within Time
Management, Neuro-harmonically and Spiritually. Evidence is provided that attitudinize psychotherapy
25

7/31/2019 Att Thy & Suicide New
http://slidepdf.com/reader/full/att-thy-suicide-new 26/31
enables the individual for Self-Conditioning constantly for turning all the dysfunctional attitudes into
positive/adaptive attitudes. Once the individual is determined to keep one self tuned into the adaptive
attitudes most of the time, towards self, environment and the world around them, enhances the self
esteem of the individual to a higher level most of the time and the self identity, meaning of life, worth
of life remains intact, boosts the ego and keeps the person motivated enthusiastically for life ahead.
Cannon (2003) proposes, Hopelessness is a significant predictor of suicidality, but not all
depressed patients feel hopeless. If clinicians can predict hopelessness, they may be able to identify
those patients at risk of suicide and focus interventions on factors associated with hopelessness. In
this study, we examined potential predictors of hopelessness in a sample of depressed outpatients.
Methods: In this study, we examined potential demographic, diagnostic, and symptom predictors of
hopelessness in a sample of 138 medication-free outpatients (73 women and 65 men) with a primary
diagnosis of major depression. The significance of predictors was evaluated in both simple and
multiple regression analyses. Results were Consistent with previous studies, we found no significant
associations between demographic and diagnostic variables and greater hopelessness. Hopelessness
was significantly associated with greater depression severity, poor problem solving abilities as
assessed by the Problem Solving Inventory, and each of two measures of dysfunctional cognitions (the
Dysfunctional Attitudes Scale and the Cognitions Questionnaire). In a stepwise multiple regression
equation, however, only dysfunctional cognitions and poor problem solving offered non-redundant
prediction of hopelessness scores, and accounted for 20% of the variance in these scores. These
findings, identifying clinical correlates of hopelessness, provide clinicians with potential additional
targets for assessment and treatment of suicidal risk. In particular, clinical attention to dysfunctional
attitudes and problem solving skills may be important for further reduction of hopelessness and
perhaps suicidal risk.
The findings are statistically modest and provide an insight to the effectiveness of the
Attitudinize Psychotherapy. Friedenberg and Gillis (2006) in an experimental study reveal that a
frequent goal in psychotherapy is the modification of low self-esteem. While such modification is
accomplished most often in an indirect manner, it is possible to apply attitude change techniques
directly to this purpose. In this study, 36 college students who had scored poorly on a standardized
measure of self-esteem were exposed to a videotaped counter-attitudinal message under conditions of
either high or low credibility; controls did not view the videotape. Results were consistent across
several esteem measures and demonstrated significant positive changes in esteem for Ss exposed to
the high credibility communication. The possibilities of adapting attitude change techniques to
psychotherapy are considered.
Eland (2005) conducted research on Self Esteem Improvement, to know ‘What Does It Takes
and How Important Is It?’ The researcher proposes, “To be honest, it probably takes less than most
people would ever believe. Your desire, commitment and consistency are the most important success
factors - and last but not least good tools to accomplish the task of improving your self esteem and
confidence. Only one can tell how important it is. Self-esteem is fundamental. It is related to your self
26

7/31/2019 Att Thy & Suicide New
http://slidepdf.com/reader/full/att-thy-suicide-new 27/31
worth and how you value yourself. Thus, building self-esteem is basic for your happiness and a good
life. Low self-esteem causes mental illness like depression and anxiety. Other people's desires can
seem more important than yours. The Inner, nagging voice of disapproval makes you powerless even
minor challenges seem impossible to overcome. This is a condition you don't have to stay in a minute
longer!
Then, how can I get out of it and really develop a high self-esteem, reduce dysfunctional
attitudes and diminish suicidal ideation you may ask? The first is to admit and accept your fear -
stop denying your bad self image - face it and from there start working with yourself. Then, set your
goal as precisely as you can. Commit to your goal. Then follow a plan containing a set of self-
esteem building activities to reach it; acceptance of dysfunctional attitudes can greatly help to work
for diminishing your suicidal ideation. Be nice to yourself. Reward yourself when you have reached a
sub-goal or a milestone. Give yourself a teaser from time to time. This is considered a vital part of
the knowledge of how to build self-confidence. Just know that your desire and commitment for
improving your self-esteem, reducing dysfunctional attitudes and diminishing suicidal ideation are
most important. If you really don't want an improvement, no program or self esteem exercise can
help you. But can I get help to develop my desire and commitment, you may ask? Yes, you can.
This is a major element in every quality program for improving your self-image, reducing
dysfunctional attitudes and diminishing suicidal ideation.
ACKNOWLEDGMENT
Dr. Linah Askari deeply thanks Almighty Allah Pak for the completion of the research. The
President - Mr. Shahjehan S. Karim, Executive Director Admissions – Ms. Sabina Mohsin, Executive
Director Academics – Mr. Talib S. Karim, Dean CBM – Dr. Javed Akbar Ansari and Administration
Personnel of Institute of Business Management, and my family & colleagues for their guidance and
Cooperation, in conducting and compiling the research. And the committee of SELF, Fifth Self Biennial
International Conference - UAE University for the opportunity granted for paper presentation.
REFERENCES
27
7/31/2019 Att Thy & Suicide New
http://slidepdf.com/reader/full/att-thy-suicide-new 28/31
American Psychiatric Association. ( 1996; 1998). Adolescent commit suicide. In: GOLIATH-Business
Knowledge on Demand. Adolescence (2005), Stress, Self-Esteem and Suicidal Ideation in late
adolescents. http://goliath.ecnext.com/
Ashby, Jeffrey S. A1 & Rice, Kenneth G. A2 (2002). Perfectionism, Dysfunctional Attitudes, and Self-
Esteem: A Structural Equations Analysis. Journal of Counseling & Development, Issue: Volume
80, Number 2 / Spring 2002. A1 Department of Counseling and Psychological Services, Georgia
State University, Atlanta & A2 Department of Counseling, Educational Psychology, and Special
Education, Michigan State University, East Lansing
http://aca.metapress.com/app/home/contribution.asp?
referrer=parent&backto=issue,9,13;journal,27,36;linkingpublicationresults,1:112973,1
Askari, Linah. (2005). Mother’s Dysfunctional Attitude and Depressive Symptoms in
Children. Pakistan Journal of Psychology, June, 36(1), 39-55. University of Karachi, Pakistan.
Askari, Linah. (2007). The Attitudinize Psychotherapy; Intervention of the New Millennium. Karachi-
Pakistan: South Asia Publications. University Press.
Bartleby. (2000). “Attitudinize” The American Heritage® Dictionary of the English
Language, Fourth Edition. Published by the Houghton Mifflin Company. Bartleby.com
Beck, A. T. (1976). Cognitive Therapy and Emotional Disorders. New York, Intern. Universities Press.
Beck, A. T. (1991). Cognitive therapy: a 30-year retrospective. American Psychology; 46:368–375
[CrossRef] [Medline]
Beck, A. T., Steer, R. A., Brown, G. (1993). Dysfunctional attitudes and suicidal ideation in psychiatric
outpatients. Suicide Life Threat Behavior; 23:11–20 [Medline]
Burns, David D. (1999). Ten Days to Improving Self – Esteem. The Counseling and Mental
Health Centre. New York: Quill, The University of Texas at Austin, 100 West
Dean Keeton St. 1 University Station A3500 ...
www.utexas.edu/student/cmhc/booklets/selfesteem/selfest.htmlCannon, B. (2003). Dysfunctional attitudes and poor problem solving skills predict hopelessness in
major
depression. Journal of Affective Disorders, Volume 55, Issue 1, Pages 45-49.
Conner, Duberstein, Conwell, Seidlitz, & Caine. (2001). Adolescent’s suicide. In: GOLIATH-Business
Knowledge on Demand. Adolescence (2005), Stress, Self-Esteem and Suicidal Ideation in late
adolescents. http://goliath.ecnext.com/
De Man, A. F., Leduc, C. P. (1995). Suicidal ideation in high school students: depression and other
correlates. Journal of Clinical Psychology; 51:173–181 [Medline]
Diener, E. (1984). Subjective well-being. Psychological Bulletin, 95, 542-575.
Eland, W. (2005). Doing business as 1st-Self-Improvement.net. “Self Esteem Improvement
- What Does It Take and How Important Is It?” LLC USA.
http://www.1st-self-improvement.net/self_esteem_improvement.htm
Friedenberg, William P., & Gillis, John S. (2006). An experimental study of the
effectiveness of attitude change techniques for enhancing self-esteem. Journal of
Clinical Psychology , Volume 33 Issue 4, February, Pages 1120 – 1124. Copyright
© 2008 Wiley Periodicals, Inc., A Wiley Company. Correspondence to John S.
28
7/31/2019 Att Thy & Suicide New
http://slidepdf.com/reader/full/att-thy-suicide-new 29/31
Gillis, Ph. D., Department of Psychology, Oregon State University, Corvallis, Oregon
97331.website:http://www3.interscience.wiley.com/journal/112466408/ abstract?
CRETRY=1&SRETRY=0
Group Health Centre for Health Promotion (2003). Motivational Interviewing: An
Overview, Presentation Overview. MI Basic Principles.
www.ctri.wisc.edu/sub_dept/presentations/pres_womenconf/
MotivationalInter09-03.ppt
Hamamci, Zeynep. (2006). Integrating psychodrama and cognitive behavioral therapy to treat
moderate
depression. The Arts in Psychotherapy Volume 33, Issue 3, 2006, Pages 199-207, Turkey
aUniversity of Gaziantep, Faculty of Education
http://www.sciencedirect.com/science?_ob=ArticleURL&_udi=B6V9J-4JSFV6W-
1&_user=10&_rdoc=1&_fmt=&_orig=search&_sort=d&view=c&_version=1&_urlVersion=0&_u
serid=10&md5=0a49f9a2d4acb5802ef39b629a2794de
Hong, Yan., Li, Xiaoming., Fang, Xiaoyi., Wai, Xinjiekou., Xiong, Oing (2007). Stressful life events, self-
esteem, and suicidal ideation among three comparative samples of Chinese population.
(APHA)
American Public Health Association, Scientific Session & Event Listing. [email protected]
Kaplan, H. B. (1975). Self-attitudes and deviant behavior . Pacific Palisades, CA: Goodyear.
Kamradt, T. F., & Kamradt, E. J. (1999). Structured Design for Attitudinal Instruction
(p. 570). In Zhou, Ying. (2001). NJ., Instructional-Design Theories and Models: A
Knowledge Base. Volume II. Lawrence Erlbaum Associates, Publishers: Mahwah,
Kelly, K. R., & Jordan, L. K. (1990). Effects of academic achievement and gender on
academic and social self-concept: A replication study. Journal of Counseling and Development,
69, 173- 177.Kurtz & Derevensky. (1993). Suicide a problem. In: GOLIATH-Business Knowledge on Demand.
Adolescence (2005), Stress, Self-Esteem and Suicidal Ideation in late adolescents.
http://goliath.ecnext.com/
Larrson, B., Ivarsson, T. (1998). Clinical characteristics of adolescent psychiatric inpatients who have
attempted suicide. European Child Adolescent Psychiatry; 7:201–208 [CrossRef] [Medline]
McCaul, E. J., Donaldson, G. A., Colardarci, T., & Davis, W. E. (1992). Consequences of
dropping out of high school: Findings from high school and beyond.
Journal of Educational Research, 85, 198-207.
McGee, Rob., Williams, Sheila & Nada-Raja, Shyamala. (2001). Low Self-Esteem and Hopelessness in
Childhood and Suicidal Ideation in Early Adulthood. Journal of Abnormal Child Psychology, Vol.
29 Number 4; Springer Netherlands.
Marciano, P. L., Kazdin, A. E. (1994). Self-esteem, depression, hopelessness, and suicidal intent among
psychiatrically disturbed inpatient children. Journal of Clinical Child Psychology; 23:151–160
National Mental Health Association. (1997). The suicide rate in the United States. In: GOLIATH-Business
29
7/31/2019 Att Thy & Suicide New
http://slidepdf.com/reader/full/att-thy-suicide-new 30/31
Knowledge on Demand. Adolescence (2005), Stress, Self-Esteem and Suicidal Ideation in late
adolescents. http://goliath.ecnext.com/
Pinto, A., & Whisman, M. A. (1996). Negative affect and cognitive biases in suicidal and non-suicidal
hospitalized adolescents. Journal of American Academy Child Adolescent Psychiatry; 35:158–
165
Powell, Michael Lee., Newgent, Rebecca A.., 7 Lee, Sang Min. (2006). Group cinematherapy: Using
metaphor to enhance adolescent self-esteem. The Arts in Psychotherapy , Volume 33, Issue 3,
April, 2006, Pages 247-253. aUniversity of Arkansas, Fayetteville, 136 Graduate Education
Building Fayetteville, AR 72701, USA.
http://www.sciencedirect.com/science?_ob=ArticleURL&_udi=B6V9J-4JRVFKD-
5&_user=10&_rdoc=1&_fmt=&_orig=search&_sort=d&view=c&_acct=C000050221&_version=
1&_urlVersion=0&_userid=10&md5=180e2e2d01b19f096d78d4ac88b83bae
Queendom. (2003). Queendom the land of Tests; Attitude & Lifestyle – Self Esteem Test
http://discoveryhealth.queendom.com/questions/self_esteem_abridged_1.html
Ramakrishna, K. (2007). Personality development: attitude makes the difference, Eyeway.org. Website:
http://www.eyeway.org/inspire/pd-attit.htm
Reinherz, Helen Z., Tanner, Jennifer L., Berger, Sasha R., Beardslee, William R. & Fitzmaurice, Garrett
M.
(2006). Adolescent Suicidal Ideation as Predictive of Psychopathology, Suicidal Behavior, and
Compromised Functioning at Age 30. American Journal of Psychiatry, 163:1226–1232.
www.naswma.org/publications/
Robins, R. W., Hendin, H. M., & Trzesniewski, K. H. (2001). Measuring global self-esteem:
Construct validation of a single-item measure and the Rosenberg Self-Esteem Scale.
Personality and Social Psychology Bulletin, 27, 151-161.Rogers, C. R. (1959). A theory of therapy, personality, and interpersonal relationships, as
developed in the client-centered framework. In S. Koch (Ed.), Psychology: A study of science
(Vol. 3, pp. 184-256). New York: McGraw-Hill.
Rogers, C. R. (1961). On becoming a person: A therapist’s view of psychotherapy . Boston:
Houghton Mifflin.
Schweitzer, Albert. (2002). Happiness! Developing a Positive Attitude. Training and
Organizational Development, Management Flyers, September,
http://www.positive-thinking-positive thoughts.com. In Shuja, Lina. (2005). Mother’s
Dysfunctional Attitude and Depressive Symptoms in Children. Pakistan Journal of Psychology,
June, 36(1), 39-55. University of Karachi, Pakistan.
Schwenk, Thomas L. (2004). Reducing Suicidal Ideation in Elders, Possible, but Expensive. Published in
Journal Watch General Medicine March 23.
http://general-medicine.jwatch.org/cgi/content/full/2004/323/2
Smith, Jeannette M., Alloy, Lauren B., & Abramson, Lyn Y. (2006). Cognitive Vulnerability to
Depression,
Rumination, Hopelessness, and Suicidal Ideation: Multiple Pathways to Self-Injurious Thinking.
30
7/31/2019 Att Thy & Suicide New
http://slidepdf.com/reader/full/att-thy-suicide-new 31/31
Recommended