Embed Size (px)
Citation preview

Pneumonia
고려대 호흡기 내과 이은주

Case 1
M/70
CC: dyspnea (onset; 2 days ago)
PI : 1 개월 전 URI Sx 있어 local 에서 medication 하였으나 호전 없고 일주일 전부터 pneumonia 에 준해 통원 치료 중 내원 3-4 일 전부터 fever 발생하고 2 일 전부터 dyspnea 발생하여 내원
Smoker: 1* 40 PY
PHx : DM/ HTN/TBc/Hepatitis (+/-/-/-)

ROS : C/S(+/+): yellowish, blood tinged(+) F/C(+/+) dyspnea, NYHA III-IV
P/Ex : V/S 120/80-84/min-28/min-38.6C crackle on RMLF + RLLF
Lab : CBC 12600 – 13.6 – 205K (NØ 93.0%) ABGA(R/A) 7.45- 33- 54- 22.9- 89% urinary Ag S. pneumoniae(+) Sputum G/S, culture: group 4 G(+) cocci in chains G(+) cocci in clusters S. pneumoniae

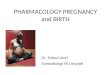
CXR, 내원시

Sputum G/S, culture
Tx
ICU ceftriaxone + levofloxacin
O2 supply

Case 2
F/26
CC: Fever, cough, sputum, myalgia (onset: 2 days ago) PI : 특이 병력 없던 분으로 2 일전부터 갑자기 발생한 high fever, cough, sputum, myalgia 로 타병원 내원 후 Influenza 진단 및 CXR 상 pneumonia 발생하여 항생제 사용 중 tachycardia, tachypnea 악화 되어 전원 옴

ROS : C/S(+/+): expectoration 못함 F/C (+/+) pleuritic chest pain(+) dyspnea, NYHA IV P/Ex : V/S 130/80- 130/min- 23/min- 38`C decreased lung sound with mild crackle
LAB: CBC 2000-13.6- 135k (NØ 79.7%) Sputum & BAL – G(+) cocci cluster S. aureus - Influenza A

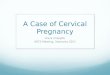
chest x ray- initial & f/u

chest CT

Typical : S. pneumonia, H. influenza, S. aureus, K. pneumoniae.. acute, intense productive cough - purulent, bloody
pleuritic chest pain leukocytosis, neutrophilia CXR – lobar consolidaiton, air bronchogram
Atypical : gradual onset, fever, nonproductive cough relatively normal WBC, no demonstrable bacterial
pathogen M. pneumoniae, Chlamydophilia, C. burnetii, Legionella,
Virus..
Typical vs. Atypical pneumonia

Elements important for local CAP guidelines

Site of care decisions – hospital admission decision-1
Characteristic points
Age
Men age
Women Age-10
Nursing home resident +10
Coexisting illnesses
Neoplastic dz +30
Liver dz +20
CHF +10
Cerebrovascular dz +10
Renal dz +10
Characteristic points
Physical Examination Findings
Altered mental status +20
RR ≥ 30/min +20
SBP <90 mmHg +20
Temperature <35 or >40 +15
pulse ≥ 125/min +10
Laboratory / X-ray Findings
Arterial pH < 7.35 +30
BUN >30 mg/dL +20
Na <130mmol/L +20
Glucose ≥ 250 mg/dL +10
Hematocrit < 30% +10
PaO2 <60mmHg +10
Pleural effusion +10
Pneumonia Severity Index (PSI)

Site of care decisions – hospital admission decision-2
Pneumonia Severity Index (PSI)
Risk Group (# of points) Mortality
I (pts not calculated) 0-0.4%
II ( ≤ 70) 0.4-0.7%
III (71-90) 0-2.8%
IV (91-130) 8.2-9.3%
V (>130) 27-31.1%
Age<50 without active ca, liver dz, CVA, renal dz
with normal V/S, normal mental status Risk Group I
Out Pt
Observation unit
In Pt

Site of care decisions – hospital admission decision-3
CURB-65 Confusion
Uremia (BUN >20mg/d ) Respiratory rate ( ≥ 30/min) Low Blood pr. (sys. ≤ 90mmHg or dia. ≤ 60mmHg) Age > 65 0-1 : Out pt. 2 : general ward ≥ 3 : ICU

Site of care decisions – hospital admission decision-4
Whether PSI or CURB-65 is superior unclear, but preferred CURB-65 PSI : limiting its practicality in a busy ED 주로 mortality 에 중점 not severity CURB-65 : not as extensively studied as PSI severity 에 중점
그 외 Admission Ix : Cx, exacerbation of underlying dz, oral medication 불가 , multiple risk factors, saturation ≤ 90% (or Pa O2 ≤ 60mmHg),
shock, decompensated coexisting illness, pleural effusion, social problem(dependent/ no caregiver), 이전 치료에 반응 없을
때

Site of care decisions – ICU admission decision-1
Criteria for severe community-acquired pneumonia
Minor criteria ( 3 개 이상 ) Respiratory rate ≥ 30 /min PaO2/FiO2 ratio ≤ 250 Multilobar infiltrates Confusion/disorientation Uremia (BUN ≥ 20 mg/dL) Leukopenia (WBC <4000 cells/mm3) Thrombocytopenia (platelet <100,000 cells/mm3) Hypothermia (core temperature, < 36ºC) Hypotension requiring aggressive fluid resuscitation
Major criteria Invasive mechanical ventilation Septic shock with the need for vasopressors

Diagnostic testing-1
Recommendations for diagnostic testing remain controversial.
Routine diagnostic tests to identify an etiologic diagnosis are optional for outpt.
Pre Tx Blood culture/sputum study should be obtained from inpt.
For severe CAP, blood culture, sputum G/S & culture, urinary antigen tests for Legionella pneumophila & Streptococcus pneumonia.
For intubated pt., an endotracheal aspirate sample should be obtained.

Diagnostic testing-3

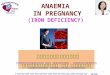
Antibiotic Tx -1
a: influenza A & B, adenoV, RSV, parainfluenza, metapnpeumoV, HSV, VZV,
SARS, measles
Decreasing order of frequency
S. pneumonia: M/C
P. aeruginosa
: chronic oral steroid
bronchopulmonary dz
alcoholism
frequent antibiotic therapy
Atypical organisms
: G/S, 표준 Culture 에 안 자라
M.pneumoniae, C. pneumoniae,
Legionella, respiratory V.
Anaerobic coverage Ix
: aspiration
+ LOC (alcohol/drug overdose/seizure)
+ gingival dz/esophageal motility dz

Antibiotic Tx -2

Drug-resistant S. pneumoniae (DRSP)
: age<2 or >65yr
ß-lactam therapy within the previous 3 months
alcoholism
medical comorbidities
immunosuppressive illness or therapy
exposure to a child in a day care center
CA-MRSA
: end-stage renal dz, injection drug abuse,
prior influenza/antibiotic therapy
Antibiotic Tx -3

Antibiotic Tx –outpt.
Macrolide
: active against S. pneumonia
& atypical pathogens
azithromycin
-active against H.influenza
ß-lactam
: high dose amoxicilline(1g x3/d)
augmentin (2g x 2/d)
ceftriaxone,
cefpodoxime, cefuroxime 등 .
Telithromycin
: multidrug resistant S. pneumomiae

Antibiotic Tx –inpt.
Ertapenem : equivalent to ceftriaxone, activity against anaerobe, DRSP, enterobacteriaceae (not Pseudo)
ICU pt
: combination not respiratory quinolone mono.

Antibiotic Tx –special concerns
Pseudomonas
: combination Tx
oral quinolone 을 최근 쓴 적 있다면 aminoglycoside 포함 regimen 선호
CA-MRSA
: more susceptible to bactrim, quinolone, clindamycin, erythromycin than hospital acquired.

Antibiotic Tx -6

Antibiotic Tx -7

Pathogen 이 밝혀지면 pathogen directed therapy.
: IV oral change 시 경구 항생제 choice 에 도움 Severe ill pt 에서는 combination therapy 의 효과가 극대화 됨 .
pathogen 밝혀진 후 monotherapy 로의 전환은
주로 non-ICU pt. 에서
Influenza A 의 경우 Sx 발생 48hr 이내 oseltamivir/ zanamivir
투여 .
AI(H5N1) 인 경우 oseltamivir
± antibiotics targeting S. pneumoniae, S. aureus.
IV acyclovir – V-Z virus, H-S virus pneumonia
Antibiotic Tx -8

Time to first antibiotics dose : as soon as possible (<8hr, in ED)
Switch from IV to oral therapy : hemodynamically stable & improving clinically & able to ingest medication & normally functioning GI tract 같은 agent/drug class 의 po medication 으로 주로 전환 β-lactam+macrolide macrolide alone 가능 (if DRSP(-) & G(-) enteric pathogen 아닐 때 )
Antibiotic Tx -9

Discharge : as soon as they are clinically stable, no other active
problems po medication 동안 입원관찰은 필요하지 않음 .
Duration of Antibiotic therapy : 최소 5 일 이상 , 주로 7-10 일 이상 afebrile for 48-72hr 이상
cavities (or tissue necrosis), Pseudomonas, bacteremic S. aureus 의 경우 (endocarditis, meningitis...) 에는
길게 .
Antibiotic Tx -10

Mx of nonresponding pneumonia

Reevaluate the initial microbiological results. - 내성 균 vs. cover 되지 않는 균 vs.nosocomial superinfection
인지 ..
Repeat blood culture
G(-) bacilli (not Pseudo, MRSA 등의 내성균 ) 의 해석에 주의 d/t early colonization after initiation of antibiotic Tx
Other cause- catheter, urinary, abdominal, skin infection
Stopping β-lactam to exclude drug fever
Mx of nonresponding pneumonia

Chest CT – pulmonary embolism, effusion, abscess, airway
obstruction 감별 .
Thoracentesis - empyema, parapneumonic effusion
Bronchoscopy, BAL - pulmonary hemorrhage, AEP, virus (lymphocyte dominant)
Mx of nonresponding pneumonia

Influenza vaccination Ix : age ≥ 50 yr, household contacts of high-risk persons, health care workers, others at risk for influenza
complications
Intranasally administered live attenuated vaccine : alternative vaccine for persons 5-49 yrs of without
underling dz (immunodeficiency, asthma, chronic medical dz)
Pneumococcal vaccine Ix
discharge 나 OPD 에서 시행 ( 독감의 경우엔 가을 /겨울 )
Prevention-1

Prevention-2

Smoking cessation : risk of pneumococcal bacteremia, Legionella.
Respiratory hygiene measures : hand hygiene, masks, tissues for pts with cough respiratory infection 의 전파 감소시킴
Prevention-3