Embed Size (px)
Citation preview

J. Clin. Endocrinol. Metab. 1999 84: 1813-1816, doi: 10.1210/jc.84.6.1813
Nobuyuki Amino, Hisato Tada and Yoh Hidaka
Screening for Postpartum Thyroid Dysfunction in the General Population Is Beneficial
Society please go to: http://jcem.endojournals.org//subscriptions/ or any of the other journals published by The EndocrineJournal of Clinical Endocrinology & Metabolism To subscribe to
Copyright © The Endocrine Society. All rights reserved. Print ISSN: 0021-972X. Online

THERAPEUTIC CONTROVERSY
Screening for Postpartum Thyroiditis
NOBUYUKI AMINO, HISATO TADA, YOH HIDAKA, LAWRENCE M. CRAPO, AND
ALEX STAGNARO-GREEN
“Therapeutic Controversies” are an occasional feature of The Journal of Clinical Endocrinology &Metabolism. They present the opposing views of invited contributors on a topic. All reprints mustinclude the complete Therapeutic Controversy, so that each section can be read in context.
Screening for Postpartum Thyroid Dysfunction inthe General Population Is Beneficial
Nobuyuki Amino, Hisato Tada, and Yoh HidakaDepartment of Laboratory MedicineOsaka University Medical SchoolOsaka 565-0871, Japan
POSTPARTUM thyroid dysfunction is recognized as acommon disease among postpartum women (1),
with a prevalence rate of around 5%, i.e. 1 in 20 pregnantwomen suffers from thyroid dysfunction after parturition(2–14). To discuss whether screening for postpartum thy-roid dysfunction is beneficial, we shall examine the fol-lowing questions:
1. Are there any effective tests or protocols to screen post-partum thyroid dysfunction?
2. What is the benefit of the screening for postpartumthyroid dysfunction?
3. Does the effectiveness meet the costs?
There are effective protocols to screen postpartum thyroiddysfunction
Postpartum autoimmune thyroid dysfunction is brieflycharacterized as a postpartum exacerbation of subclinicalautoimmune thyroid disease, wherein some immunolog-ical abnormalities are observed before the onset of thyroiddysfunction. Therefore, we can detect the high-risk groupfor postpartum thyroid dysfunction by screening, in earlypregnancy, those with subclinical autoimmune thyroid-itis. Among several methods for detecting thyroid auto-immunities, the measurement of anti-thyroid microsomalantibody (MCAb) or thyroid peroxidase (TPO) antibody isthe most useful marker for detecting subclinical autoim-mune thyroiditis and, therefore, for predicting the occur-rence of postpartum thyroid dysfunction. When MCAb is
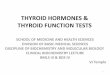
positive, there is always lymphocytic infiltration into thethyroid, indicating subclinical autoimmune thyroiditis(15) that may be exacerbated after delivery. Sixty to sev-enty percent of women with positive MCAb in early preg-nancy develop postpartum thyroid dysfunction (1). Otherinvestigators have also reported that MCAb-positive sub-jects had approximately 20 –23 times the relative risk (overnormal subjects) for developing postpartum thyroid dys-function (16, 17). On the other hand, the prevalence ofpostpartum thyroid dysfunction in the MCAb-negativesubjects in early pregnancy is estimated as 1/100 of thatin MCAb-positive subjects (Fig. 1). So, when we screen1000 early pregnant women in the general population, wecan expect to find about 50 patients with postpartum thy-roid dysfunction.
Although MCAb is a good marker for the occurrence ofpostpartum thyroid dysfunction, it gives no informationabout the type of dysfunction that will occur. Among thevarious types of dysfunctions, postpartum Graves’ diseaseis clinically the most important and is predicted by themeasurement of thyroid-stimulating antibodies (TSAb)with a sensitive bioassay (18). Our subsequent study (19)revealed that pregnant women with positive TSAb in earlypregnancy had a much higher risk of developing post-partum Graves’ disease. We observed 71 pregnant womenwith positive MCAb from early pregnancy through thepostpartum period. Among them, 7 showed positiveTSAb, and 5 of those 7 (71%) developed postpartumGraves’ disease. Thyrotoxicosis in 3 of those 5 was tran-sient and spontaneously improved within a year. Graves’disease did not occur in the TSAb-negative subjects. Anti-TSH receptor (TSHR) antibodies (TRAb) with conven-tional radio-receptor assay (thyrotropin binding inhibi-tory immunoglobulin; TBII) were not useful in predictingpostpartum Graves’ disease.
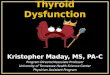
Figure 2 shows a protocol that we have tentatively em-ployed to screen for postpartum thyroid dysfunction at theoutpatient maternity clinic of the Osaka University Hos-pital for several years. In the protocol, MCAb-positivemothers are examined for thyroid status, measuring serumfree thyroxine (FT4), serum free triiodothyronine (FT3),serum thyrotropin (TSH), anti-TSHR antibody (TRAb),and antithyroglobulin (TgAb), and are observed every
Accepted March 8, 1999.Address correspondence and requests for reprints to: Alex Stagnaro-
Green, MD, Dean for Student Affairs and Medical Education, MountSinai School of Medicine, One Gustave L. Levy Place, Box 1255, NewYork, New York 10029-6574. E-mail: [email protected]. Re-prints of the Therapeutic Controversies will include all authors and allpages, as shown in the journal.
0021-972X/99/$03.00/0 Vol. 84, No. 6The Journal of Clinical Endocrinology & Metabolism Printed in U.S.A.Copyright © 1999 by The Endocrine Society
1813

4 – 8 weeks. We believe that this close observation protocolfor MCAb-positive subjects is practical in only a fewcountries, such as Japan, where the national health insur-
ance system is well-established. It should be modifiedaccording to the situation and health system of eachcountry.
FIG. 1. The prevalence of antithyroidMCAb and the occurrence of postpar-tum thyroid dysfunction among preg-nant women in the general population.
FIG. 2. A protocol to screen and followMCAb-positive mothers. MCAb, anti-thyroid microsomal antibody; FT4, freethyroxine; FT3, free triiodothyronine;TSH, thyrotropin; TRAb, anti-TSH re-ceptor antibody.
1814 THERAPEUTIC CONTROVERSY JCE & M • 1999Vol 84 • No 6

The benefits of screening postpartum thyroid dysfunction
Although postpartum thyroid dysfunction may be tran-sient in many cases (20), we should pay close attention to thepossibility that mothers with thyroid dysfunction alreadytired from the birth and from taking care of a newborn, mayfeel terribly worn out and helpless or may become ill in bed.Postpartum depression, which in severe cases may result ina forced double suicide of mother and baby (called “Shinjuh”in Japanese), can be screened by MCAb measurement, al-though postpartum depression may occur not in associationwith thyroid dysfunction (17, 21–23) but with antithyroidMCAb (24, 25). The main benefit of screening for postpartumthyroid dysfunction is the opportunity to improve the qual-ity of life of mothers who may suffer from the above symp-toms. Even when the patient does not want drug therapy, shebenefits by being informed about what is happening to her.From our experience, patients with mild to moderate thyroiddysfunction can live well with the support of family withoutmedication. Further, prevention of future episodes of post-partum thyroid dysfunction may be possible. We have ex-perienced one case of successful prevention. The patient haddeveloped severe postpartum thyroid dysfunction in each ofher previous parturitions, and she did not want to repeat thecondition after the next delivery. Moderate doses of glu-cocorticoid, gradually decreased and stopped in one month,suppressed her thyroid dysfunction to only a small fluctu-ation within the normal range.
Postpartum Graves’ disease accounts for 11.4% of post-partum thyroid dysfunctions (occurring in 0.54% of all moth-ers in the general population) (19). Conversely, 40% ofGraves’ patients 20–39 yr old, who have had one or moredeliveries, developed their disease during the postpartumperiod (26). Diagnosis of postpartum Graves’ disease early,while it is mild, may easily lead to remission and may reduceGraves’ disease in older age. In our experience, the early startof antithyroid therapy reduces the period of therapy by half(19). Antithyroid therapy may be a good choice for first-linetherapy (27) because postpartum Graves’ hyperthyroidism isoften transient and because mothers may not want to inter-rupt breast-feeding to undergo radioiodine therapy.
An additional benefit to screening with anti-MCAb anti-bodies in early pregnancy may be not only to find postpar-tum thyroid dysfunction, but also to find mothers at high riskfor spontaneous abortion. In our prospective study, the spon-taneous abortion rate in MCAb-positive mothers was twiceas high as that in MCAb-negative mothers (28).
There has been no analysis of the cost-effectiveness ofscreening for postpartum thyroid dysfunction
The cost of MCAb measurement to screen for the occur-rence of postpartum thyroid dysfunction is low when we usesemiquantitative particle agglutination tests. However, thy-roid function tests and anti-TSHR antibody measurement forMCAb-positive subjects are not cheap, especially when pa-tients are observed closely and are tested repeatedly. On theother hand, the main benefit of screening for postpartumthyroid dysfunction is improving the mother’s quality of life,which is difficult to numerically assess. Heyslip et al. (29)tried to estimate the costs of several screening methods and
concluded that MCAb measurement is the most cost-effec-tive, but their report compares only the screening methodsfor postpartum thyroid dysfunction; they did not analyze thebenefit of mothers’ quality of life, nor did they discuss cost-effectiveness compared with the screening for other diseasesor other health services. Indeed, there seems no analysis ofthe cost-effectiveness of screening for postpartum thyroiddysfunction (23, 30). However, the observation protocol wedescribe can be modified to be less expensive, and screeningsubjects may be restricted to certain high-risk groups, suchas the patients with IDDM. We believe an optimized systemof screening will be found whose costs are acceptable for eachsociety.
We experimentally applied TSAb to the second-linescreening of MCAb-positive mothers and found that TSAbgives predictive information on potential development ofpostpartum Graves’ disease. TSAb measurement is obvi-ously too expensive, and the procedure is too complicated toapply screening to the general population. However, weexpect the development of a more sensitive radioreceptorassay may change the situation (31).
Conclusion
The benefit of screening for postpartum thyroid dysfunc-tion mainly concerns elusive, nonquantitative parameters—the quality of life of mothers—that can be difficult to assess.However, we would hope to find an acceptable, cost-effec-tive system of screening for postpartum thyroid dysfunction.
References
1. Amino N, Tada H, Hidaka Y. 1996 Autoimmune thyroid disease and preg-nancy. J Endocrinol Invest. 19:59–70
2. Amino N, Mori H, Iwatani Y, et al. 1982 High prevalence of transient post-partum thyrotoxicosis and hypothyroidism. N Engl J Med. 306:849–852.
3. Jansson R, Bernander S, Karlsson A, Levin K, Nilsson G. 1984 Autoimmunethyroid dysfunction in the postpartum period. J Clin Endocrinol Metab.58:681–687.
4. Walfish P, Chan J. 1985 Postpartum hyperthyroidism. Clin Endocrinol Metab.14:417–447.
5. Freeman R, Rosen H, Thysen B. 1986 Incidence of thyroid dysfunction in anunselected postpartum population. Arch Intern Med. 146:1361–1364.
6. Nikolai TF, Turney SL, Roberts RC. 1987 Postpartum lymphocytic thyroiditis.Prevalence, clinical course, and long-term follow-up. Arch Intern Med.147:221–224.
7. Lervang HH, Pryds O, Kristensen HP. 1987 Thyroid dysfunction after deliv-ery: incidence and clinical course. Acta Med Scand. 222:369–374.
8. Fung HYM, Kologlu M, Collison K, et al. 1988 Postpartum thyroid dysfunc-tion in Mid Glamorgan. Br Med J. 296:241–244.
9. Rasmussen NG, Hornnes PJ, Hoiter-Madsen M, Feldt-Rasmussen U, Hege-dus L. 1990 Thyroid size and function in healthy pregnant women with thyroidautoantibodies. Acta Endocrinol (Copenh). 123:395–401.
10. Rajatanavin R, Chailurkit LO, Tirarungsikul K, Chalayondeja W, JittivanichU, Puapradit W. 1990 Postpartum thyroid dysfunction in Bangkok: a geo-graphical variation in the prevalence. Acta Endocrinol (Copenh). 122:283–287.
11. Roti E, Bianconi L, Gardini E, et al. 1991 Postpartum thyroid dysfunction inan Italian population residing in an area of mild iodine deficiency. J EndocrinolInvest. 14:669–674.
12. Lobig H, Bohn W, Mau J, Schatz H. 1991 Prevalence of postpartum thyroiditisin two iodine-deficient regions of Germany. In: Scherbaum W, Bogner U,Weinheimer B, and Bottazzo G, eds. Autoimmune thyroiditis. Berlin: Springer-Verlag; 185–193.
13. Walfish PG, Meyerson J, Provias JP, Vargas MT, Papsis FR. 1992 Prevalenceand characteristics of post-partum thyroid dysfunction: Results of a surveyfrom Toronto, Canada. J Endocrinol Invest. 15:265–272.
14. Stagnaro-Green A, Roman SH, Cobin RH, el-Harazy E, Wallenstein S, Da-vies TF. 1992 A prospective study of lymphocyte-initiated immunosuppres-sion in normal pregnancy: evidence of a T-cell etiology for postpartum thyroiddysfunction. J Clin Endocrinol Metab. 74:645–653.
15. Yoshida H, Amino N, Yagawa K, et al. 1978 Association of serum antithyroid
THERAPEUTIC CONTROVERSY 1815

antibodies with lymphocytic infiltration of the thyroid gland: studies of sev-enty autopsied cases. J Clin Endocrinol Metab. 46:859–862.
16. Solomon BL, Fein HG, Smallridge RC. 1993 Usefulness of antimicrosomalantibody titers in the diagnosis and treatment of postpartum thyroiditis. J FamPract. 36:177–182.
17. Pop VJM, de Rooy HA, Vader HL, van der Heide D, van Son MM, KomproeIH. 1993 Microsomal antibodies during gestation in relation to postpartumthyroid dysfunction and depression. Acta Endocrinol (Copenh). 129:26–30.
18. Tamaki H, Amino N, Aozasa M, Mori M, Tanazawa O, Miyai K. 1987 Serialchanges in thyroid-stimulating antibody and thyrotropin binding inhibitorimmunoglobulin at the time of postpartum occurrence of thyrotoxicosis inGraves’ disease. J Clin Endocrinol Metab. 65:324–330.
19. Hidaka Y, Tamaki H, Iwatani Y, Tada H, Mitsuda N, Amino N. 1994 Pre-diction of postpartum onset of Graves’ thyrotoxicosis by measurement ofthyroid stimulating antibody in early pregnancy. Clin Endocrinol (Oxf).41:15–20.
20. Amino N, Tada H, Hidaka Y. 1996 The spectrum of postpartum thyroiddysfunction: diagnosis, management, and long-term prognosis. Endocr Pract.2:406–410.
21. Harris B, Fung H, Johns S, et al. 1989 Transient postpartum thyroid dysfunc-tion and postnatal depression. J Affect Disord. 17:243–249.
22. Pop VJM, Rooy HAM, Vader HL, et al. 1991 Postpartum thyroid dysfunctionand depression in an unselected population. New Engl J Med. 324:1815–1816.
23. Lazarus JH, Harris B, Parkes AB. 1996 Antenatal screening of thyroid anti-bodies. Lancet. 348:1516–1517.
24. Harris B, Othman S, Davies JA, et al. 1992 Association between postpartumthyroid dysfunction and thyroid antibodies and depression. BMJ. 305:152–156.
25. Pop VJ, Maartens LH, Leusink G, et al. 1998 Are autoimmune thyroid dys-function and depression related? J Clin Endocrinol Metab. 83:3194–3197.
26. Tada H, Hidaka Y, Itoh E, et al. 1994 Prevalence of postpartum onset of diseasewithin patients with Graves’ disease of child-bearing age. Endocr J. 41:325–327.
27. Amino N, Tada H. 1997 Postpartum thyroid disease. In: Bardin CW, ed.Current therapy in endocrinology and metabolism, 6th ed. Philadelphia:Mosby-Year Book, Inc.; 327–330.
28. Iijama T, Tada H, Hidaka Y, Mitsuda N, Murata Y, Amino N. 1997 Effects ofautoantibodies on the course of pregnancy and fatal growth. Obstet Gynecol.90:364–369.
29. Haylip CC, Fein HG, O’Donnel VM, et al. 1988 The value of serum antimi-crosomal antibody testing in screening for symptomatic postpartum thyroiddysfunction. Am J Obstet Gynecol. 159:203–209.
30. Ball S. 1996 Antenatal screening of thyroid antibodies. Lancet. 348:906–907.31. Watabnabe Y, Tada H, Hidaka Y, et al. 1999 Polyethylene glycol increases the
detection of anti-thyrotropin (TSH) receptor antibodies by a radioreceptorassay. Clin Chem. 45:407–409.
The Time Is Not Ripe To Screen
Lawrence M. CrapoDivision of EndocrinologyStanford University School of Medicine and
Santa Clara Valley Medical CenterSan Jose, California 95128
AT FIRST GLANCE, screening for postpartum thyroid-itis (PPT) appears to be an attractive and possibly even
a cost-effective strategy. The disorder is quite common, af-fecting in the range of 4–6% of all postpartum women (1). Inthe United States, where there are approximately 4 millionlive births annually (2), this means that PPT afflicts nearly200,000 women each year. The symptoms associated withPPT are often subtle and difficult to distinguish from symp-toms frequently present during the postpartum period.Those women at high risk for PPT are easy to identify be-cause PPT is an autoimmune disease in which most patientshave elevated serum levels of thyroid autoantibodies. It isgenerally assumed that over 20% of women with PPT willeventually develop permanent hypothyroidism within a 5-yrperiod (3, 4). Finally, PPT is easy to treat when symptoms arepresent by employing beta-blockers for the hyperthyroidphase and levothyroxine for the hypothyroid phase of thedisorder (5).
On closer scrutiny, however, the screening strategy losessome of its initial appeal. Although PPT is common, symp-toms during the hyperthyroid and hypothyroid phases of the
illness are often mild in degree and brief in duration and,consequently, may not require treatment. When symptomsare moderate or severe in degree they should be recognizedclinically, although this will require more education of pri-mary care physicians and postpartum patients about PPT.Which thyroid autoantibody assay should be used for screen-ing and when the assay should be performed have not beencompletely resolved. Furthermore, there is a lack of knowl-edge about how to follow patients with a positive antibodyassay. Should a serum TSH level be done only when they aresymptomatic, or should serial TSH levels be done and, if so,at what intervals? Finally and most importantly, there hasbeen no prospective diagnostic and therapeutic trial to datethat tells us whether or not a screening program would bebeneficial.
We will initially discuss screening for thyroid disease ingeneral to set the stage for a detailed discussion of screeningfor PPT. Available data and studies on these important issueswill lead to the conclusion that the time is not yet ripe torecommend a screening program for all pregnant or post-partum women to identify those who are at risk for or whohave PPT.
Screening for thyroid disease in general
In general, screening may be defined as testing for thepresence of a disease or the risk of a disease when no knownsigns or symptoms of the disease are present, with the pur-pose of improving health outcomes in the target population(6). Screening recommendations for thyroid disease involvean assessment of age, gender, family history, and associatedphysiologic or pathophysiologic conditions. In addition tospecifying who should be screened, such recommendationsalso need to specify which tests should be employed, howfrequently they should be employed, and where they shouldbe employed.
Presently, there is only one universally agreed-upon strat-egy in screening for thyroid disease, which is that neonatesshould be screened for congenital hypothyroidism with ablood TSH or total T4 assay shortly after birth in the hospital.In 1990, the American Thyroid Association (ATA) recom-mended against screening for thyroid disease in asymptom-atic subjects in the general population who were not at highrisk for thyroid disease and its consequences (7). The Cana-dian Task Force on the Periodic Health Examination in 1994(8), and the United States Preventative Services Task Force(USPSTF) in 1996 (9), concurred in this recommendationagainst general screening. All agencies recommend screen-ing for hypothyroidism in neonates even though it is infre-quent (1 case per 4,000 births). The ATA recommends screen-ing with tests of thyroid function in certain higher risksituations, such as in elderly patients, those with a familyhistory of thyroid disease, individuals with autoimmunediseases such as type I diabetes mellitus, and in postpartumwomen at 4–8 weeks (7). The USPSTF adds the high riskgroup of persons with Down’s syndrome, and notes that atthe present time there is insufficient evidence to recommendfor or against screening for thyroid disease in any of thechildhood or adult high risk groups, including postpartumwomen (9). They do recommend that clinicians should re-
1816 THERAPEUTIC CONTROVERSY JCE & M • 1999Vol 84 • No 6

main alert for subtle signs and symptoms of thyroid dys-function and keep a low threshold for evaluating thyroidstatus in such high risk subjects.
Recently, one study has demonstrated by cost-utility de-cision analysis that it is cost-effective to screen for mild thy-roid failure with a serum TSH assay at 5-yr intervals startingat age 35 yr for both men and women, and that such screeningis especially recommended for elderly women (10). Morerecently, the American College of Physicians has recom-mended screening for unsuspected but symptomatic hypo-thyroidism and hyperthyroidism in women over 50 yr of age,employing a sensitive serum TSH assay (11, 12). They furthernote that there is insufficient evidence at present to recom-mend for or against screening for subclinical hypothyroidismor subclinical hyperthyroidism, although this latter recom-mendation has been criticized (13).
Thus, from the general literature on screening for thyroiddisease, there is little to help guide us in a decision aboutscreening for PPT, and what there is remains controversial.In the presence of conflicting recommendations from pres-tigious national agencies, and in the absence of publishedcost-benefit analyses or prospective controlled clinical trials,we are compelled to form a conclusion about the merits ofscreening for PPT on other grounds, employing availablestudies on the epidemiologic, laboratory, and clinical char-acteristics of PPT.
Screening for postpartum thyroiditis
In order to develop a strategy of screening for PPT it isnecessary to review the epidemiology of the disorder andassess its varied clinical manifestations so we can answer thequestions of what are we screening for, what tests should weuse for screening, when we should screen, and whether ornot screening is superior to clinical ascertainment of PPT.
PPT is an autoimmune disorder characterized by a de-structive lymphocytic infiltration of the thyroid gland, veryoften with accompanying circulating thyroid autoantibodies,which can manifest itself as transient hyperthyroidism, tran-sient hypothyroidism, or permanent hypothyroidism. Thesemanifestations result from activation of immunologicalchanges that occur in the first postpartum year. The symp-toms of PPT are those of hyperthyroidism or hypothyroidismadded to a background of symptoms commonly found in thepostpartum period, such as fatigue, tiredness, depression,emotional lability, and anxiety. These symptoms can be mildor severe and transient or prolonged. Thus, PPT is a proteandisorder with varied presentations at varied times hiding inthe shadow of common postpartum symptoms, which ren-ders the development of a screening strategy very difficult.
The epidemiology of PPT is presented in Table 1, where theoutcome of 1,000 hypothetical unselected postpartumwomen is traced, assuming that 5% of the women will de-velop PPT, 10% of the women will be positive for serumthyroid peroxidase autoantibodies (TPO-Ab), nearly 50% ofthe women with a positive TPO-Ab titer will develop PPT,and that 90% of women with PPT will have a positiveTPO-Ab titer. The data in this table have been derived fromseveral reviews of numerous studies on the incidence of PPTand the prevalence of positive TPO-Ab titers in postpartumwomen (1, 14). The incidence of PPT in these studies variesby over an order of magnitude from 1.1% to 16.7%, whichmay be explained in part by variations in geographical lo-cation, definition of PPT, duration of studies, and frequencyof testing. A critical evaluation of many of the studies sug-gests that the incidence of symptomatic PPT is about 5% (1).The incidence data on permanent overt hypothyroidism inTable 1 and Table 2 has been derived from 5 separate studiesin which patients with PPT have been followed for 3–5 yr (3,4, 15–17).
What is the purpose of screening for PPT? The simpleanswer to this question is that the purpose is to alleviatesymptoms from hypothyroidism and transient hyperthy-roidism and to identify women who are at risk for subse-quent permanent hypothyroidism, as well as PPT in futurepregnancies. But is screening really necessary to carry outthis purpose, or could the purpose be accomplished withoutscreening through careful attention to clinical detail by phy-sicians who care for postpartum women? Unfortunately, noprospective studies have yet been conducted that answer thisquestion. The symptoms of hyperthyroidism and hypothy-roidism blend with and are notoriously difficult to separatefrom other symptoms associated with the postpartum state.Some of the symptoms of hyperthyroidism and hypothy-roidism may be found more frequently in postpartumwomen with PPT and/or positive TPO-Ab titers, comparedto those without PPT (18–20). However, the clinical distinc-tion between these two groups of postpartum women can bequite difficult. Depression may be more frequent and severein women with PPT (21–23). Nevertheless, when symptomsare mild in degree and transient in duration, it is unlikely thattreatment is necessary, and equally unlikely that patients willseek medical attention. If symptoms are severe enough indegree and duration to bring patients to medical attention,then clinicians should test for thyroid dysfunction anyway,and screening would not be necessary. All postpartumwomen, whether or not screening is done, should be en-couraged by their physicians to seek medical attention if theyhave troublesome symptoms and not automatically attribute
TABLE 1. Epidemiology of postpartum thyroiditis
Total numberof women
Women with positiveTPO-Ab titers
Women with negativeTPO-Ab titers
Postpartum women 1000 100 900Women with PPT 50 45 5Women with permanent hypothyroidism by 5 yr 9 9 0
The data in this table assumes that, for 1,000 unselected postpartum women, 5% will develop postpartum thyroiditis (PPT), and 90% of thesewomen will be positive for serum thyroid peroxidase autoantibodies (TPO-Ab). It is further assumed that nearly 50% of women with positiveserum TPO-Ab titers will develop PPT, and that, in these women, permanent hypothyroidism develops at an average rate of 3.6% per yr, withan overall incidence rate of 1.8 cases/1000 women/yr. See the text and Table 2 for references and calculations to support these assumptions.
THERAPEUTIC CONTROVERSY 1817

a lack of well-being to the postpartum state. In particular, allpostpartum women with depression should be tested forthyroid dysfunction as depression can be a life-threateningdisorder and needs to be treated promptly.
If a screening program for PPT is employed, what testsshould be used and when should they be done? If all post-partum women were screened with a sensitive TSH assay at2- to 3-month intervals, then nearly all cases of PPT wouldbe detected. However, this strategy is clearly impractical andtoo costly. In the United States, where there are 4 million livebirths per year, this would entail approximately 12 millionTSH assays at a cost of about 250 million dollars per year. Amore reasonable strategy would be to screen all postpartumwomen with a sensitive thyroid autoantibody assay, such asTPO-Ab, and then follow the women testing positive withseveral TSH assays during the 1-yr postpartum period. Fromthe data in Table 1, this would entail 4 million TPO-Ab assaysand about 1.2 million TSH assays per year at a cost of about100 million dollars per year to detect 200,000 cases of PPT ata cost of $500 per case detected, many of which would bemild and would not need treatment. A clinical approach todetection of PPT would cost 30–50 million dollars per year,assuming that 30–50% of 4 million postpartum women weresymptomatic and tested with a single TSH assay, and that allpostpartum women received a $2 pamphlet alerting them tothe symptoms of PPT. It is possible that benefits from aprogram employing clinical astuteness would be comparableto a screening program. However, an accurate cost-benefit isnot possible until good studies are available detailing theclinical presentation of PPT and how they respond to ther-apy. Unfortunately, no study has yet been published to dem-onstrate that such a screening strategy would be superior incost or in benefit to thorough clinical assessment of post-partum women. Although the sensitivity of the TPO-Ab as-say in identifying women who will develop PPT is generallyabout 90%, the range in a number of studies is from 50–100%(14). In a recent, thorough study from The Netherlands thesensitivity was 67%. This means that screening with aTPO-Ab assay would miss 33% of the women who developPPT and, thus, casts doubt on the recommendation of thisstrategy for all countries (24, 25). Certain women with aknown high risk for PPT, such as those with type I diabetesmellitus, previous autoimmune thyroid disease (AITD), or astrong family history of AITD should be followed closelyunder any circumstances by thorough clinical and, if neces-sary, biochemical scrutiny (26–28).
Even if screening for PPT is not superior to careful clinical
assessment in the diagnosis and treatment of symptomatictransient hyperthyroidism or hypothyroidism, shouldscreening be employed to identify postpartum women whoare at risk for permanent overt hypothyroidism? The long-term sequelae of PPT have been recently reviewed (29), andthe results of those studies that have followed patients withPPT for 3 yr or longer are summarized in Table 2. Severalimportant observations can be extracted from this table. First,the mean rate of progression from PPT to permanent overthypothyroidism over a 5-yr period in the 5 studies is 3.6% peryear. This is very close to the rate at which all adult womenin the community with a positive TPO-Ab titer progress tospontaneous overt hypothyroidism as determined in the re-nowned Wickham survey, which observed rates of 4.3% peryear when the serum TSH level was elevated, and 2.1% peryear when the TSH level was normal (30). Second, the meanrate of progression of all postpartum women to permanentovert hypothyroidism over a 5-yr period in the 5 studies is1.8 cases/1000 women/yr, very close to the rate at which allwomen develop spontaneous hypothyroidism (3.5 cases/1000 women/yr for all women, and 1.4 cases/1000 wom-en/yr for young women in their child-bearing years) seen inthe Wickham survey (30). Thus, the rate of progression tospontaneous permanent hypothyroidism in postpartumwomen with and without PPT is virtually the same as the rateseen in the Wickham survey in all young women with andwithout positive TPO-Ab titers.
Conclusion
The time is not yet ripe to recommend a screening programfor all postpartum women to detect PPT, even though thedisorder is common. The basic problem is that there is a lackof knowledge at present about how to screen, when to screen,and whether or not treatment makes a difference for thosewomen with unrecognized mild or moderate thyroid dys-function. Permanent hypothyroidism occurs at about thesame rate of incidence in postpartum women as in all youngwomen, and in both groups is confined almost exclusively tothose with preexisting AITD. Whether or not young women,including postpartum women, should be screened to detectthose who have or are at risk for permanent hypothyroidismremains an open question until further studies clarify theissue.
Finally, a recommendation against screening postpartumwomen for PPT at the present time should not be construedto mean that clinical vigilance is not warranted. In general,
TABLE 2. Progression of postpartum thyroiditis to permanent overt hypothyroidism
Patientswith PPT
Patients withpermanent HYPO
Years offollow-up
Progression to permanent HYPO(per 100 women with PPT/yr)
Progression to permanent HYPO(per 1000 postpartum women/yr)
Study(ref)
25 3 3 4.0 2.0 Nikolai (16)44 9 5 4.1 2.1 Taichi (3)31 5 5 3.2 1.6 Jansson (15)43 4 3.5 2.7 1.4 Othman (4)40 6 4 3.7 1.9 Soloman (17)
This table presents the rate of progression from postpartum thyroiditis (PPT) to permanent overt hypothyroidism (HYPO) in percent peryear based on long-term follow-up data from five separate studies. It also presents the rate of progression of 1000 normal postpartum womento permanent hypothyroidism in cases per year by assuming that patients with PPT represent about 5% of their original cohort of all postpartumwomen.
1818 THERAPEUTIC CONTROVERSY JCE & M • 1999Vol 84 • No 6

the thorough care that women receive during their preg-nancy has no counterpart during their first postpartum year,as attention in the family and in the medical system shiftsfrom the mother to the infant. Thus, there is a compellingneed to educate postpartum women and the physicians whocare for them about PPT and other important postpartumafflictions.
References
1. Gerstein HC. 1990 How common is postpartum thyroiditis. A methodologicoverview of the literature. Arch Intern Med. 150:1397–1400.
2. Guyer B, Martin JA, MacDorman MF, Anderson RN, Strobino DM. 1997Annual summary of vital statistics—1996. Pediatrics. 100:905–918.
3. Tachi J, Amino N, Tamaki H, Aozasa M, Iwatani Y, Miyai K. 1988 Long-termfollow-up and HLA association in patients with postpartum hypothyroidism.J Clin Endocrinol Metab. 66:480–484.
4. Othman S, Phillips DIW, Parkes JH, et al. 1990 A long-term follow-up ofpostpartum thyroiditis. Clin Endocrinol. 32:559–564.
5. Roti E, Emerson CH. 1992 Clinical review 29: postpartum thyroiditis. J ClinEndocrinol Metab. 74:3–5.
6. Eddy DM. 1991 How to think about screening. In: Eddy DM, ed. Commonscreening tests. Philadelphia: American College of Physicians; 1–21.
7. Surks MI, Chopra IJ, Mariash CN, Nicoloff JT, Solomon DH. 1990 AmericanThyroid Association guidelines for use of laboratory tests in thyroid disorders.JAMA. 263:1529–1532.
8. Canadian Task Force on the Periodic Health Examination. 1994 The Canadianguide to clinical preventive health care. Ottawa: Canada CommunicationGroup; 1994:611–618.
9. Report of the U.S. Preventive Services Task Force. 2nd ed. Screening forthyroid disease. 1996 In: Guide to clinical preventive services: an assessmentof the effectiveness of 169 interventions. Washington, DC: US Gov Pr Office;209–218.
10. Danese MD, Powe NR, Sawin CT, Ladenson PW. 1996 Screening for mildthyroid failure at the periodic health examination—a decision and cost-effec-tiveness analysis. JAMA. 276:285–292.
11. American College of Physicians. 1998 Clinical guideline, part 1. Screening forthyroid disease. Ann Intern Med. 129:141–143.
12. Helfand M, Redfern CC. 1998 Clinical guideline, part 2. Screening for thyroiddisease: an update. Ann Intern Med. 129:144–158.
13. Cooper DS. 1998 Subclinical thyroid disease: a clinician’s perspective. AnnIntern Med. 129:135–138.
14. Stagnaro-Green A. 1993 Postpartum thyroiditis—prevalence, etiology, andclinical implications. Thyroid Today. 16:1–11.
15. Jansson R, Dahlberg PA, Karlson FA. 1988 Postpartum thyroiditis. Bailliere’sClin Endocrinol Metab. 2:619–635.
16. Nikolai TF, Turney SL, Roberts RC. 1987 Postpartum lymphocytic thyroiditis-prevalence, clinical course, and long-term follow-up. Arch Intern Med.147:221–224.
17. Solomon BL, Fein HG, Smallridge RC. 1993 Usefulness of antimicrosomalantibody titers in the diagnosis and treatment of postpartum thyroiditis. J FamPract. 36:177–182.
18. Amino N, Mori H, Iwatani Y, et al. 1982 High prevalence of transient post-partum thyrotoxicosis and hypothyroidism. N Engl J Med. 306:849–852.
19. Hayslip CC, Fein HG, O’Donnell VM, et al. 1988 The value of serum anti-microsomal antibody testing in screening for symptomatic postpartum thyroiddysfunction. Amer J Obstet Gynecol. 159:203–209.
20. Lazarus JH, Hall R, Othman S, et al. 1996 The clinical spectrum of postpartumthyroid disease. QJ Med. 89:429–435.
21. Pop VJM, de Rooy HAM, Vader HL, et al. 1991 Postpartum thyroid dys-function and depression in an unselected population. N Engl J Med. 324:1815–1816 (letter).
22. Harris B, Othman S, Davies JA, et al. 1992 Association between postpartumthyroid dysfunction and thyroid antibodies and depression. BMJ. 305:152–156.
23. Pop VJM, de Rooy HAM, Vader HL, van der Heide D, van Son MM, Kom-proe IH. 1993 Microsomal antibodies during gestation in relation to postpar-tum thyroid dysfunction and depression. Acta Endocrinol. 129:26–30.
24. Kuijpens JL, Pop VJ, Vader HL, Drexhage HA, Wiersinga WM. 1998 Pre-diction of postpartum thyroid dysfunction: can it be improved? Eur J Endo-crinol. 139:36–43.
25. Kuijpens JL, de Haan-Meulman M, Vader HL, Pop VJ, Wiersinga WM,Dreshage HA. 1998 Cell-mediated immunity and postpartum thyroid dys-function: a possibility for the prediction of disease? J Clin Endocrinol Metab.83:1959–1966.
26. Gerstein HC. 1993 Incidence of postpartum thyroid dysfunction in patientswith type I diabetes mellitus. Ann Intern Med. 118:419–423.
27. Alvarez-Marfany M, Roman SH, Drexler AJ, Robertson C, Stagnaro-GreenA. 1994 Long-term prospective study of postpartum thyroid dysfunction in
women with insulin dependent diabetes mellitus. J Clin Endocrinol Metab.79:10–16.
28. Weetman AP. 1994 Editorial: Insulin-dependent diabetes mellitus and post-partum thyroiditis: an important association. J Clin Endocrinol Metab. 79:7–9.
29. Smallridge RC. 1996 Postpartum thyroid dysfunction: a frequently undiag-nosed endocrine disorder. The Endocrinologist. 6:44–50.
30. Vanderpump MPJ, Tunbridge WMG, French JM, et al. 1995 The incidence ofthyroid disorders in the community: a twenty-year follow-up of the Wickhamsurvey. Clin Endocrinol. 43:55–68.
31. Lazarus JH. 1998 Prediction of postpartum thyroiditis. Eur J Endocrinol.139:12–13.
32. Ball S. 1996 Antenatal screening of thyroid antibodies. Lancet. 349:906–907.
Postpartum Thyroiditis:The Case For Selective Screening
Alex Stagnaro-GreenDivision of Endocrinology and MetabolismDepartment of Medicine
Mount Sinai School of MedicineNew York, New York 10029
POSTPARTUM thyroiditis is one of the most commondiseases of the thyroid and has important clinical se-
quelae. In studies in North America postpartum thyroiditisaffects between 6.0–8.8% of all pregnant women (1–3). Post-partum thyroiditis also has clearly defined morbidities.Women with postpartum thyroiditis may experience symp-toms in both the hyperthyroid and hypothyroid phase, andmay have an increased incidence of postpartum depression(4, 5). Long-term follow-up reveals that approximately 25%of women with postpartum thyroiditis develop permanentprimary hypothyroidism within 5 yr of delivery (6, 7). Fur-thermore, the presence of thyroid autoantibodies in the firsttrimester of pregnancy is associated with an increased rate ofspontaneous abortion (8–11). Given both the prevalence ofthe disorder and the associated morbidities, the argument forscreening for postpartum thyroiditis seems iron clad, andone can only wonder why a screening program for postpar-tum thyroiditis has not already been instituted.
On the other hand, screening for postpartum thyroiditis isan enormous undertaking with tremendous fiscal implica-tions. Every pregnant women would need to be screened forthe presence of thyroid peroxidase autoantibodies. Womenwho test positive would require a minimum of two mea-surements of TSH in the postpartum (3 and 6 months). Fur-thermore, the following three unproven assumptions under-lie the argument for screening; a) that the optimal screeningstrategy is known, b) that treating women with postpartumthyroiditis would decrease the incidence or severity of post-partum depression, and c) that treating postpartum thyroid-itis would decrease the incidence of, or the symptoms asso-ciated with, long-term primary hypothyroidism. Given thesearguments, it now appears that screening for postpartumthyroiditis is premature and a questionable use of limitedfiscal resources.
Given the powerful but conflicting, scientific, fiscal, andemotional arguments for screening for postpartum thyroid-itis the clinician is left in a quandary. A rational approach toresolve the screening debate requires the following fourquestions be addressed:
1. Is postpartum thyroiditis a common enough clinicalentity to warrant screening?
THERAPEUTIC CONTROVERSY 1819

2. Are there important morbidities associated with post-partum thyroiditis?
3. Can the morbidities of postpartum thyroiditis be pre-vented with levothyroxine therapy?
4. Is there an inexpensive, easily available, and accuratescreening test?
Prevalence
Worldwide, the prevalence of postpartum thyroiditis var-ies widely, from 1.1% in Thailand to 16.7% in the UnitedKingdom (12, 13). The disparity is explained both by truegeographic differences in prevalence rates as well as by crit-ical study design issues such as the length of follow-up in thepostpartum period and the frequency of screening. Studiesperformed in the United States and Canada that extend be-yond three months postpartum have revealed similar prev-alence rates (6% in Canada, 6.7% in Wisconsin, and 8.8% inthe New York Metropolitan area) (1–3). In women with TypeI diabetes mellitus, another autoimmune disorder, the prev-alence in North America is substantially higher at 25%(14–15).
The highest prevalence rates of postpartum thyroiditis arefound in women with a prior history of postpartum thy-roiditis. Lazarus et al. (16) found that 69% of women who hada history of postpartum thyroiditis developed a recurrencewith a subsequent pregnancy. Twenty-five percent ofwomen who were antibody positive in the initial pregnancy,but euthyroid in the postpartum period, developed postpar-tum thyroiditis after the next delivery.
Associated morbidities
Women with postpartum thyroiditis develop both short-term and long-term complications. Although few womenrequire treatment in the hyperthyroid phase, and in factmany women are not diagnosed until they develop hypo-thyroidism, studies have revealed an increase in palpitations,heat intolerance, and tremulousness during the hyperthy-roid period (3). Classical symptoms of hypothyroidism, aswell as concentration and memory deficits, are present in thehypothyroid phase of postpartum thyroiditis (5). The finalshort-term complication is an increased incidence of post-partum depression. Studies have indicated a 38–53% inci-dence of nonpsychotic depression in women affected withpostpartum thyroiditis (4, 5). One study has even found anincreased incidence of postpartum depression in womenwho were thyroid autoantibody positive but who did notdevelop postpartum thyroiditis (17). Finally, long-term fol-low of women with postpartum thyroiditis has revealed anincidence of long term primary hypothyroidism of approx-imately 25% (6, 7).
The correlation between thyroid autoantibodies and anincrease in spontaneous abortions is also pertinent to thescreening debate. Four studies have revealed a 2- to 3-folddoubling in the rate of spontaneous miscarriage in un-selected women who screened positive for thyroid autoan-tibodies in the first trimester of pregnancy (8–11). In womenwith recurrent abortion, defined as three or more spontane-ous miscarriages without an intervening live birth, the datahas been mixed. Three of five studies have shown an in-
creased incidence of thyroid autoantibodies in women withrecurrent abortion (18–22).
Intervention/prevention
The impact of levothyroxine therapy on the short- andlong-term complications of postpartum thyroiditis is largelyunknown. Beta blockers during the hyperthyroid phase andlevothyroxine therapy in women who are hypothyroid areeffective interventions. However, whether or not levothy-roxine therapy alters the incidence or severity of the depres-sion associated with postpartum thyroiditis has not beenevaluated.
Studies attempting to prevent the occurrence of postpar-tum thyroiditis through the administration of iodide or levo-thyroxine in antibody positive women have been unsuccess-ful (23). Furthermore, at present there are no knowninterventions which, administered during the hyperthyroidor hypothyroid phase, would result in a decrease in the highrate of permanent hypothyroidism.
A recent study has demonstrated a decrease in the rate ofrecurrent abortion in women who were thyroid antibodypositive through the administration of intravenous immu-noglobulin before conception and throughout the first 8months of pregnancy (24). Replication of these results arerequired before their implementation outside of a researchsetting.
Screening
A successful screening strategy for postpartum thyroiditisdepends on the availability of an accurate test. As defined inthe Guide to Clinical Preventive Services, accuracy relates to thesensitivity, specificity, and reliability of a screening test. Inshort, “The test must be able to detect the target conditionearlier than without screening and with sufficient accuracyto avoid producing large numbers of false-positive and false-negative results. . .” (25).
Thyroid peroxidase antibody is the potential screening testof choice for postpartum thyroiditis. It is widely available,easily reproducible, and relatively cheap. Screening for thy-roid peroxidase antibodies would need to occur early inpregnancy in order to identify women who were going todevelop postpartum thyroiditis before its manifestation.Given the dramatic and well documented decrease (often toundetectable levels) in thyroid antibodies during pregnancy,screening at delivery would miss a large percentage of thecases and consequently would have an unacceptably highfalse negative rate.
Five studies have prospectively followed a cohort of an-tibody positive and antibody negative women during preg-nancy and into the postpartum (1, 13, 26–28). The positivepredictive value of thyroid peroxidase (defined as the per-centage of women who have thyroid antibodies duringpregnancy and who subsequently develop postpartum thy-roiditis) was relatively low and ranged from 30–52%. Fur-thermore, 9–39% of the women who developed postpartumthyroiditis in these studies were antibody negative duringpregnancy. The positive predictive value of thyroid perox-idase could be increased by focusing on women with high
1820 THERAPEUTIC CONTROVERSY JCE & M • 1999Vol 84 • No 6

titers of thyroid peroxidase, but this would result in an in-creased false negative rate.
The positive predictive value of thyroid peroxidase inwomen with Type I diabetes mellitus was also limited, rang-ing from 33–67% (14, 15, 29). Similarly, 17–57% of womenwith Type I diabetes who developed postpartum thyroiditis,tested negative for thyroid peroxidase antibodies duringpregnancy.
Conclusion
Despite the high prevalence of postpartum thyroiditis inthe general population, screening of all women cannot bejustified at present. The limited positive predictive value ofthyroid peroxidase antibodies, the presence of a substantialnumber of antibody negative women who develop postpar-tum thyroiditis, and the unproven efficacy of levothyroxinein preventing postpartum depression or long-term primaryhypothyroidism, makes screening all pregnant women un-tenable. Furthermore, the conflicting data on the associationof thyroid antibodies and recurrent abortion (despite theclear association between thyroid antibodies and spontane-ous miscarriage in unselected women) requires further elu-cidation before it could be used as a rationale for screening.
Two specific populations however, would clearly benefitfrom testing for postpartum thyroiditis. Specifically, womenwith a prior history of postpartum thyroiditis (prevalence ofrecurrent thyroiditis—69%) and individuals with Type I di-abetes mellitus (prevalence of postpartum thyroiditis—25%)should have TSH determinations at 3 and 6 months post-partum. In these select groups screening with thyroid per-oxidase antibodies offers no advantages. Women who ex-hibit either suppressed or elevated TSH levels would requirefurther evaluation. Whether or not women with a history ofanother autoimmune disorder (such as systemic lupus ery-thematosus or Sjogren’s disease), or who have a strong fam-ily history of autoimmune disease, should be screened is atpresent an unresolved question.
Research in the future should focus on refining screeningstrategies for postpartum thyroiditis and determining theefficacy of levothyroxine in preventing or ameliorating post-partum depression and primary hypothyroidism. In the in-terim, a dedicated effort to educate obstetricians, internists,pediatricians, family practitioners, and psychiatrists isneeded so that the acute symptoms associated with the hy-perthyroid and hypothyroid phase can be recognized, diag-nosed, and appropriately treated.
References
1. Stagnaro-Green A, Roman, SH, Cobin, RH, El-Harazy, E, Wallenstein S,Davies, TF. 1992 A Prospective study of lymphocyte-initiated immunosup-pression in normal pregnancy: evidence of a T-cell etiology for postpartumthyroid dysfunction. J Clin Endocrinol Metab. 74:645–653.
2. Nikolai TF, Turney SL, Roberts RC. 1987 Postpartum lymphocytic thyroiditis:prevalence, clinical course, and long-term follow-up. Arch Intern Med.147:221–224.
3. Walfish PG, Meyerson J, Provias JP, Vargas MT, Papsin FR. 1992 Prevalenceand characteristics of post-partum thyroid dysfunction: results of a surveyfrom Toronto, Canada. J Endocrinol Invest. 15:265–272.
4. Pop VJM, De Rooy HAM, Vader HL, et al. 1991 Postpartum thyroid dys-
function and depression in an unselected population. N Engl Med.324:1815–1816.
5. Hayslip CC, Fein HG, O’Donnell VM, Friedman DS, Klein TA, SmallridgeRC. 1988 The value of serum antimicrosomal antibody testing in screening forsymptomatic postpartum thyroid dysfunction. Am J Obstet Gynecol.159:203–209.
6. Tachi, J, Amino, N, Tamaki, H, Aozasa M, Iwatani Y, Miyai K. Long termFollow-Up and HLA Association in Patients With Postpartum Hypothyroid-ism. Journal of Clinical Endocrinology and Metabolism. 1988;66:480–484.
7. Othman S, Phillips DIW, Parkes AG, et al. 1990 A long-term follow-up ofpostpartum thyroiditis. Clin Endocrinol. 32:559–564.
8. Stagnaro-Green A, Roman SH, Cobin, El-Harazy E, Alvarez-Marfany M,Davies, TF. 1990 Detection of at-risk pregnancy by means of highly sensitiveassays for thyroid autoantibodies. JAMA. 264:1422–1425.
9. Glinoer D, Soto MF, Bourdoux P, et al. 1991 Pregnancy in patients with mildthyroid abnormalities: maternal and neonatal repercussions. J Clin EndocrinolMetab. 73:421–427.
10. Singh A, Dantas NZ, Stone SC, Asch RH. 1995 Presence of thyroid antibodiesin early reproductive failure: biochemical versus clinical pregnancies. FertilSteril. 63:277–281.
11. Iijima T, Tada H, Hidaka Y, Mitsuda N, Murata Y, Amino N. 1997 Effects ofautoantibodies on the course of pregnancy and fetal growth. Obstet Gynecol.90:364–369.
12. Rajatanavin R, Chailurkit L, Tirarungsikul K, Chalayondeja W, JittivanichU, Puapradit W. 1990 Postpartum thyroid dysfunction in Bangkok: A geo-graphical variation in the prevalence. Acta Endocrinol. 122:283–287.
13. Fung HYM, Kologlu M, Collison K, et al. 1988 Postpartum thyroid dysfunc-tion in Mid Glamorgan. BMJ. 296:241–244.
14. Alverez-Marfany M, Roman SH, Drexler AJ, Robertson C, Stagnaro-GreenA. 1994 Long-term prospective study of postpartum thyroid dysfunction inwomen with insulin dependent diabetes mellitus. J Clin Endocrinol Metab.79:10–16.
15. Gerstein HC. 1993 Incidence of postpartum thyroid dysfunction in physicians.Ann Intern Med. 118:419–423.
16. Lazarus JH, Ammari F, Oretti R, Parkes AB, Richards CJ, Harris B. 1997Clinical aspects of recurrent postpartum thyroiditis. British J Gen Pract.47:305–308.
17. Harris B, Othman S, Davies JA. 1992 Association between postpartum thyroiddysfunction and thyroid antibodies and depression. BMJ. 305:152–156.
18. Bussen S, Steck T. 1995 Thyroid autoantibodies in euthyroid non-pregnantwomen with recurrent spontaneous abortions. Hum Reprod. 10:2983–2940.
19. Pratt D, Novotny M, Kaberlein G, Dudkiewicz A, Gleicher N. 1993 Anti-thyroid antibodies and the association with non-organ specific antibodies inrecurrent pregnancy loss. Am J Obstet Gynecol. 168:837–841.
20. Pratt DE, Kaberlein G, Dudkiewicz A, Karande V, Gleicher N. 1993 Theassociation of antithyroid antibodies in euthyroid nonpregnant women withrecurrent first trimester abortions in the next pregnancy. Fertil Steril.60:1001–1005.
21. Roberts J, Jenkins C, Wilson R. 1996 Recurrent miscarriage is associated withincreased numbers of CD5/20 positive lymphocytes and an increased inci-dence of thyroid antibodies. Eur Endocrinol. 134:84–86.
22. Esplin MS, Branch DW, Silver R, Stagnaro-Green A. 1998 Thyroid autoan-tibodies are not associated with recurrent pregnancy loss. Am J Obstet Gy-necol. 179:1583–1586.
23. Kampe O, Jansson R, Karlsson FA. 1990 Effects of l-thyroxine and iodide onthe development of autoimmune postpartum thyroiditis. J Clin EndocrinolMetab. 70:1014–1018.
24. Kiprov DD, Nachtigall RD, Weaver RC, Jacobson A, Main EK, Garovoy MR.1996 The use of intravenous immunoglobulin in recurrent pregnancy lossassociated with combined alloimmune and autoimmune abnormalities. Am JReprod Immunol. 36:228–234.
25. Report of the U.S. Preventive Services Task Force. Guide to Clinical Pre-ventive Services, 2nd ed. Baltimore: Williams and Wilkins; 1996.
26. Kuijpens JL, Hann-Meulman MDH, Vader HL, Pop VJ, Wiersinga WM,Drexhage HA. 1998 Cell-mediated immunity and postpartum thyroid dys-function: a possibility for the prediction of disease? J Clin Endocrinol Metab.83:1959–1966.
27. Pop VJM, de rooy HAM, Vader HL, van der Heide D, van Son MM, KomproeIH. 1993 Microsomal antibodies during gestation in relation to postpartumthyroid dysfunction and depression. Acta Endocrinol. 129:26–30.
28. Rasmussen NG, Hornnes PJ, Hoier-Madsen M, Feldt-Ramussen U, HegedusLaszlo. 1990 Thyroid size and function in healthy pregnant women withthyroid autoantibodies. Relation to development of postpartum thyroiditis.Acta Endocrinol. 123:395–401.
29. Bech K, Høier-Madsen M, Feldt-Rasmussen U, Jensen BM, Mølsted-Pedersen L, Kuhl C. 1991 Thyroid function and autoimmune manifestationsin insulin-dependent diabetes mellitus during and after pregnancy. Acta En-docrinologica. 124:534–539.
THERAPEUTIC CONTROVERSY 1821