Embed Size (px)
Citation preview

Clostridium difficile 現況與感染管制措施介紹

艱難梭菌感染: 不只是腹瀉而已!
2
Microbiol Mol Biol Rev 2013;77(4):567-81
腹瀉嚴重腹瀉併腸炎暴發性腸炎全身性併發症
暴發性暴發性
痊癒
復發
病亡
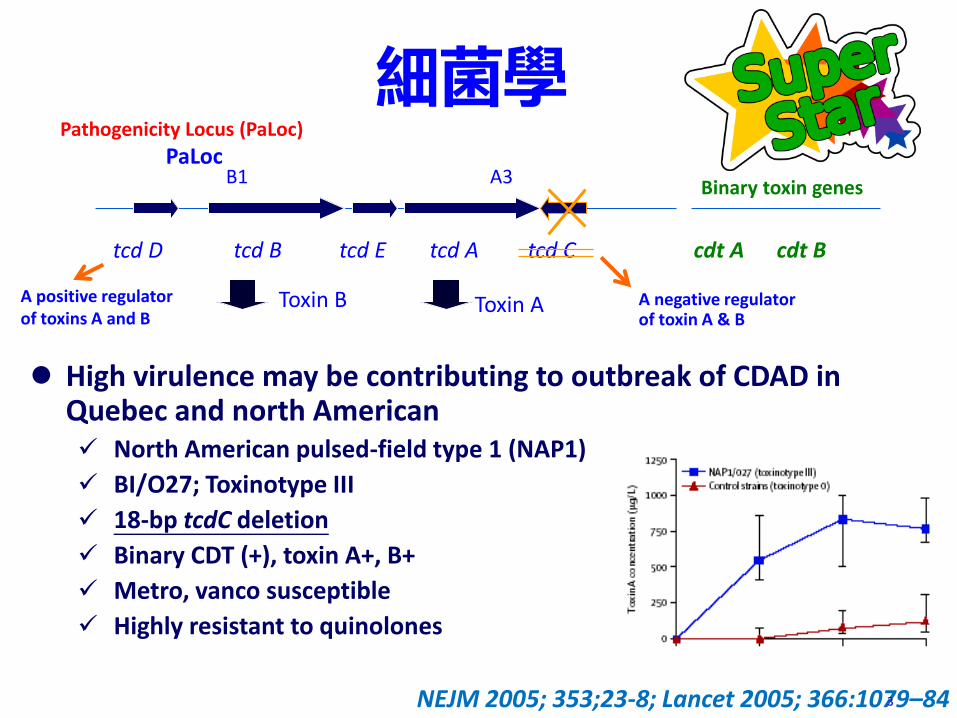
細菌學
High virulence may be contributing to outbreak of CDAD in Quebec and north American North American pulsed-field type 1 (NAP1)
BI/O27; Toxinotype III
18-bp tcdC deletion
Binary CDT (+), toxin A+, B+
Metro, vanco susceptible
Highly resistant to quinolones
Toxin B Toxin A
cdt Bcdt A
B1 A3Binary toxin genes
tcd A tcd Ctcd Etcd D tcd B
PaLoc
NEJM 2005; 353;23-8; Lancet 2005; 366:1079–84
Pathogenicity Locus (PaLoc)
A negative regulator of toxin A & B
A positive regulator of toxins A and B
3
4
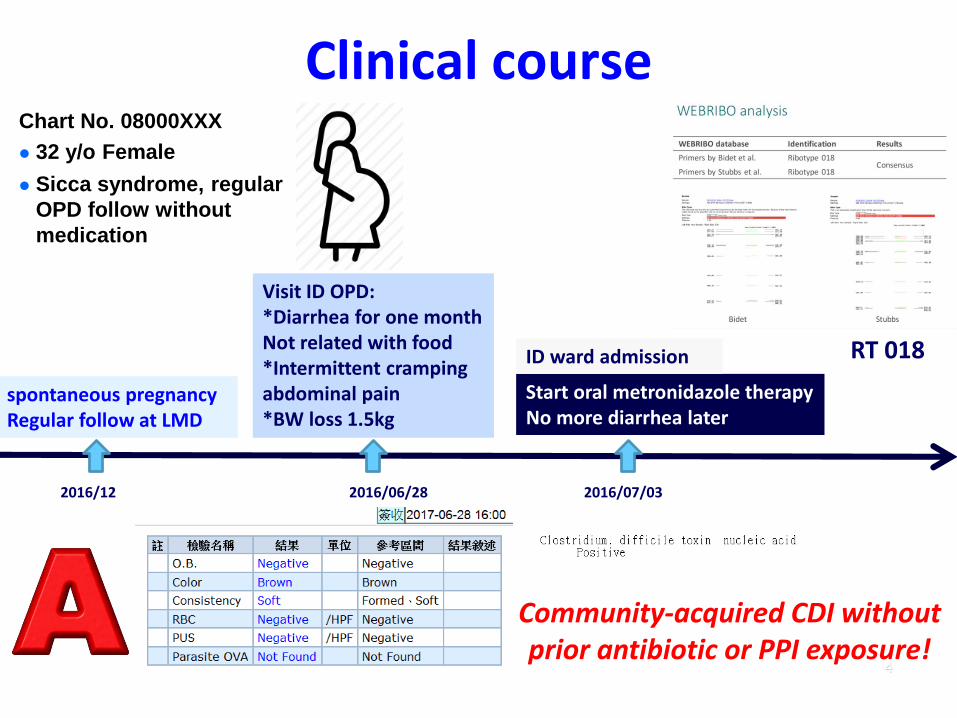
Clinical course
Visit ID OPD:*Diarrhea for one monthNot related with food*Intermittent cramping abdominal pain*BW loss 1.5kg
Start oral metronidazole therapyNo more diarrhea later
spontaneous pregnancyRegular follow at LMD
2016/12 2016/06/28
ID ward admission
2016/07/03
Chart No. 08000XXX
32 y/o Female
Sicca syndrome, regular
OPD follow without
medication
RT 018
Community-acquired CDI without prior antibiotic or PPI exposure!
5
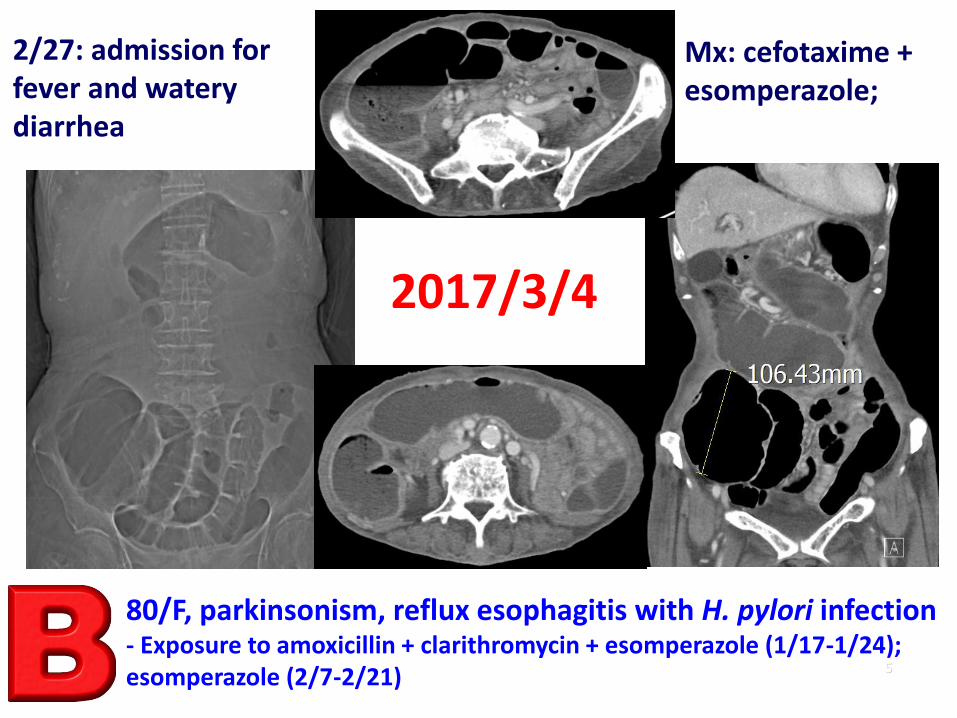
2017/3/4
80/F, parkinsonism, reflux esophagitis with H. pylori infection- Exposure to amoxicillin + clarithromycin + esomperazole (1/17-1/24); esomperazole (2/7-2/21)
2/27: admission for fever and watery diarrhea
Mx: cefotaxime + esomperazole;
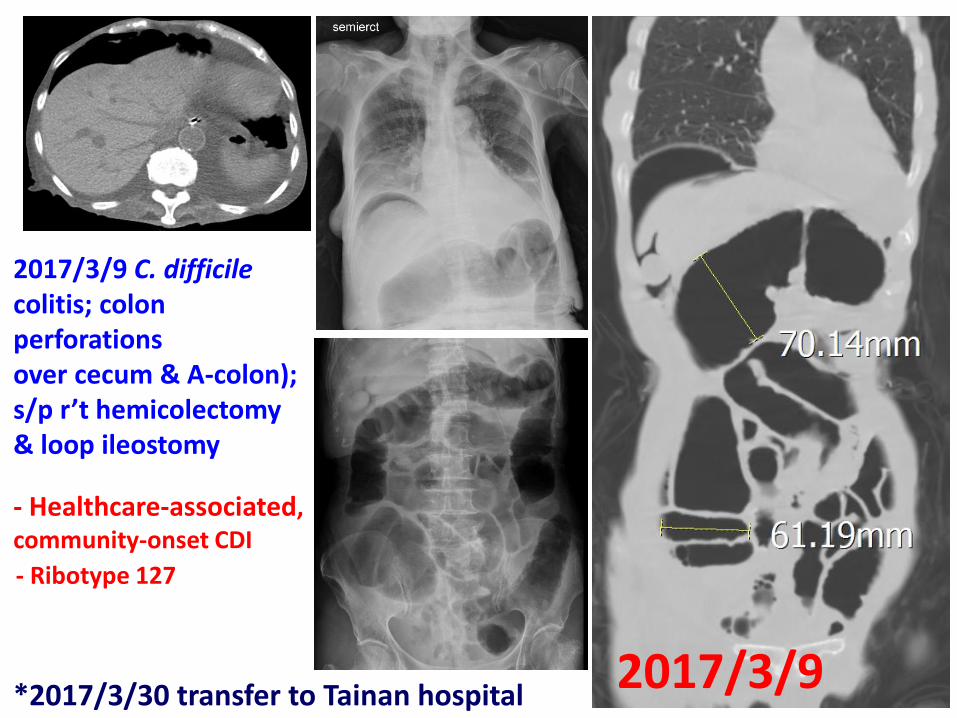
62017/3/9
2017/3/9 C. difficilecolitis; colon perforations over cecum & A-colon); s/p r’t hemicolectomy & loop ileostomy
*2017/3/30 transfer to Tainan hospital
- Ribotype 127
- Healthcare-associated, community-onset CDI
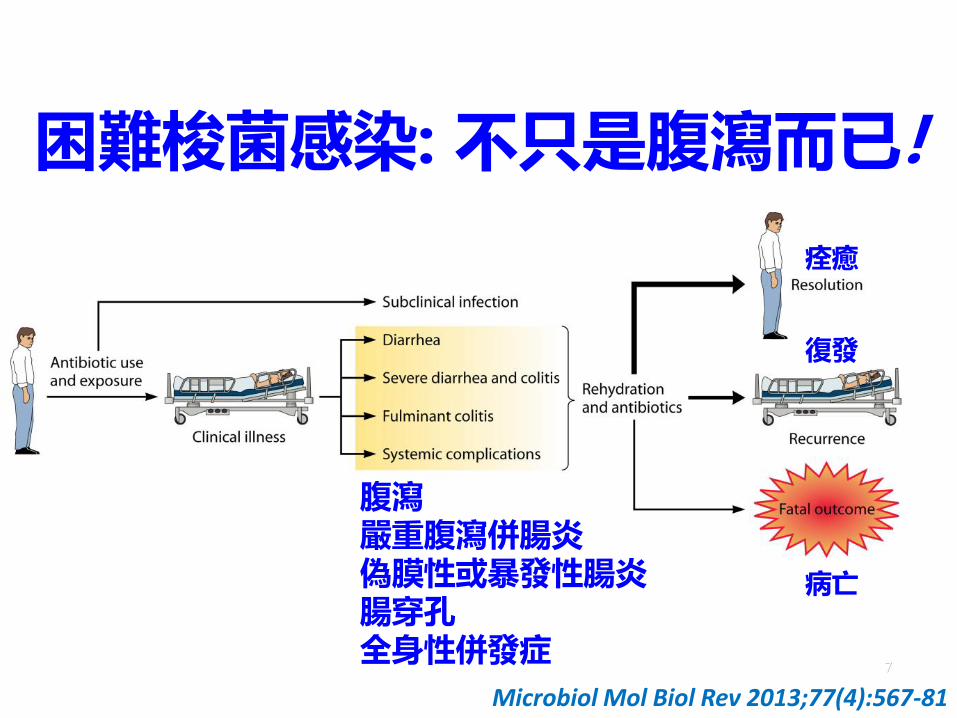
困難梭菌感染: 不只是腹瀉而已!
7
Microbiol Mol Biol Rev 2013;77(4):567-81
腹瀉嚴重腹瀉併腸炎偽膜性或暴發性腸炎腸穿孔全身性併發症
暴發性暴發性
痊癒
復發
病亡

8
2012美國困難梭菌感染的臨床衝擊
延長住院天數
每天死於困梭菌人數
困梭菌與醫療照顧相關性
困梭菌感染醫院平均費用(2009)
9
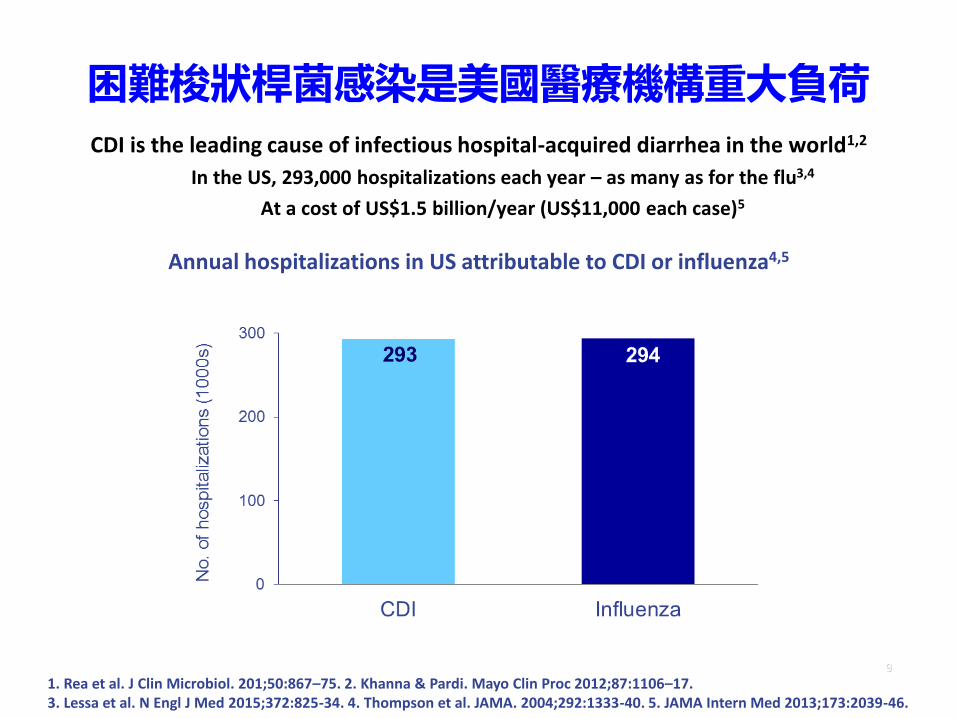
困難梭狀桿菌感染是美國醫療機構重大負荷
CDI is the leading cause of infectious hospital-acquired diarrhea in the world1,2
In the US, 293,000 hospitalizations each year – as many as for the flu3,4
At a cost of US$1.5 billion/year (US$11,000 each case)5
1. Rea et al. J Clin Microbiol. 201;50:867–75. 2. Khanna & Pardi. Mayo Clin Proc 2012;87:1106–17. 3. Lessa et al. N Engl J Med 2015;372:825-34. 4. Thompson et al. JAMA. 2004;292:1333-40. 5. JAMA Intern Med 2013;173:2039-46.
Annual hospitalizations in US attributable to CDI or influenza4,5
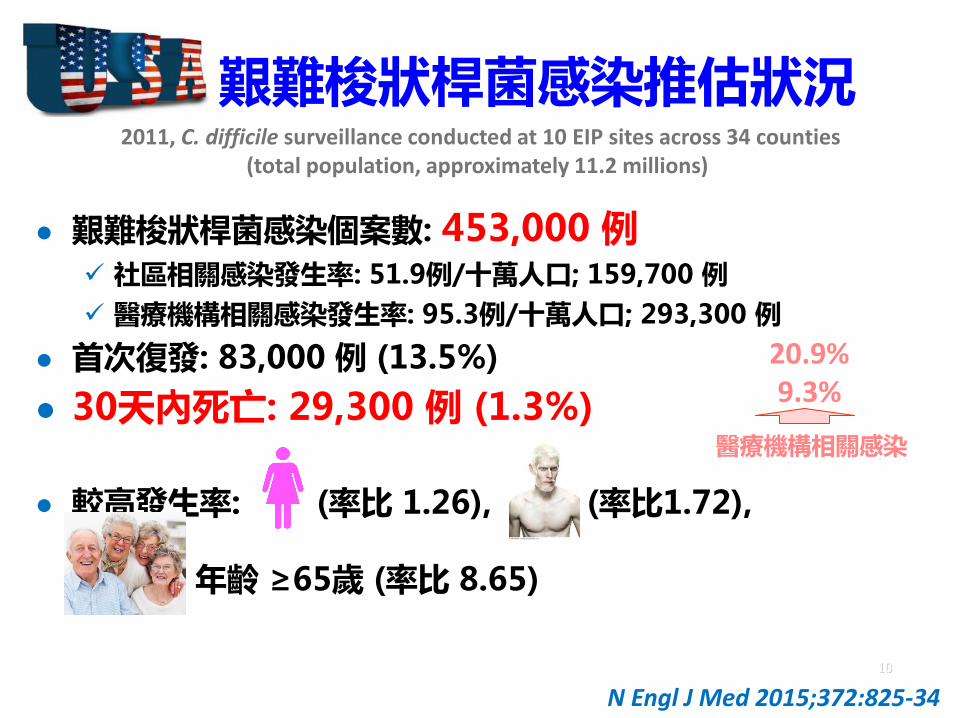
艱難梭狀桿菌感染推估狀況
艱難梭狀桿菌感染個案數: 453,000 例 社區相關感染發生率: 51.9例/十萬人口; 159,700 例
醫療機構相關感染發生率: 95.3例/十萬人口; 293,300 例
首次復發: 83,000 例 (13.5%)
30天內死亡: 29,300 例 (1.3%)
較高發生率: (率比 1.26), (率比1.72),
年齡 ≥65歲 (率比 8.65)
10
N Engl J Med 2015;372:825-34
2011, C. difficile surveillance conducted at 10 EIP sites across 34 counties (total population, approximately 11.2 millions)
醫療機構相關感染
20.9%9.3%
11
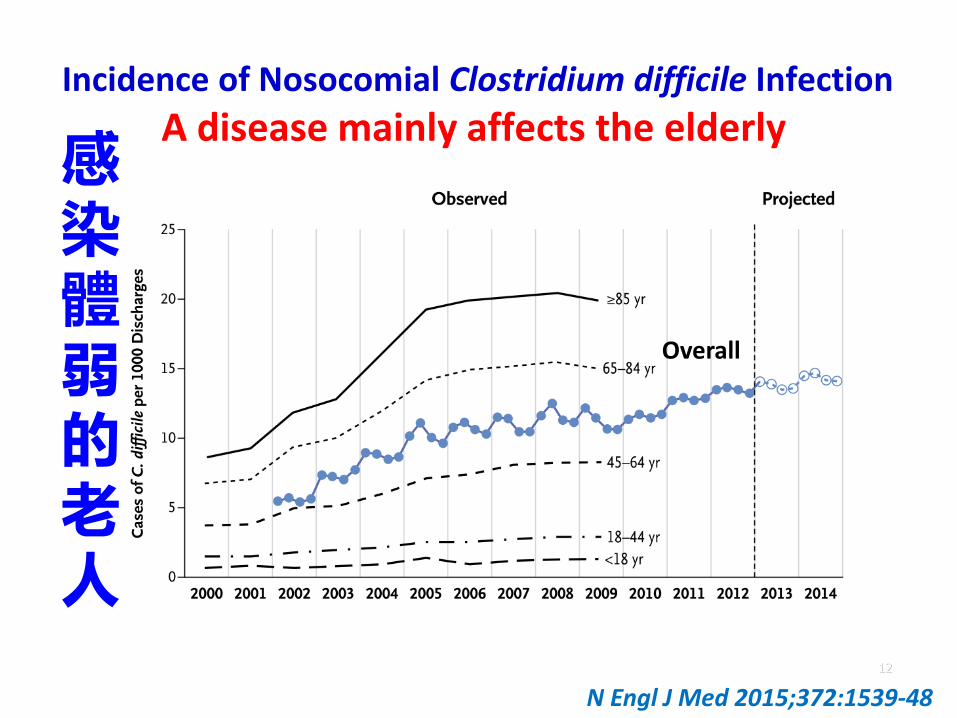
Incidence of Nosocomial Clostridium difficile Infection
A disease mainly affects the elderly
12
Overall
N Engl J Med 2015;372:1539-48
感染體弱的老人

13
檢測頻率與感染發生率之相關性
歐洲艱難梭菌
英國
愛爾蘭
芬蘭
- C. difficile ribotypes 027 (176, 244) , 078 (126, 127)
困難梭狀桿菌 高致病性菌株
15
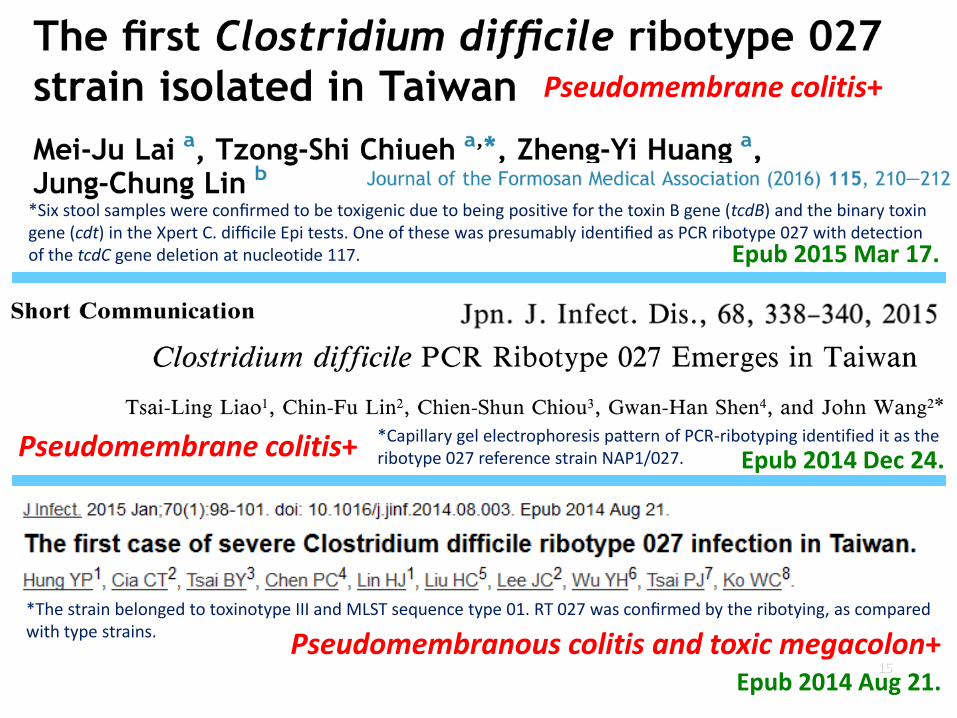
*Six stool samples were confirmed to be toxigenic due to being positive for the toxin B gene (tcdB) and the binary toxin gene (cdt) in the Xpert C. difficile Epi tests. One of these was presumably identified as PCR ribotype 027 with detection of the tcdC gene deletion at nucleotide 117.
Pseudomembrane colitis+
Pseudomembrane colitis+
*Capillary gel electrophoresis pattern of PCR-ribotyping identified it as the ribotype 027 reference strain NAP1/027.
Pseudomembranous colitis and toxic megacolon+*The strain belonged to toxinotype III and MLST sequence type 01. RT 027 was confirmed by the ribotying, as compared with type strains.
Epub 2014 Dec 24.
Epub 2014 Aug 21.
Epub 2015 Mar 17.

Ribotype 027 in Asia, 2017
2007
2006
2014
2008
2008
2012

Ribotype 078 in Asia, 2017
2011
2014
2015

PLoS ONE 2017; 12(5): e0176797
• Pooled CDI incidence (11 studies): 53/100,000 patient-days Pooled CDI incidence (10 studies, non-ICU): 49/100,000 patient-days
• Pooled CDI rate (18 studies): 3.2 cases/1,000 admissions• Pooled CDI-related mortality rate: 8.9%
USA: 6.4%
• Ribotype 027: 0.3% CDRN (US): 21% EUCLID: 19%
Europe: 41/100,000 patient-days EUCLID: 70 (7-287)/100,000 patient-days Spain: 38/100,000 patient-days USA: 54/100,000 patient-days
Clostridium difficile infection in Asia A systematic review and meta-analysis of incidence and impact
The incidence and impact of CDI in Asia is similar to that noted in the West
19
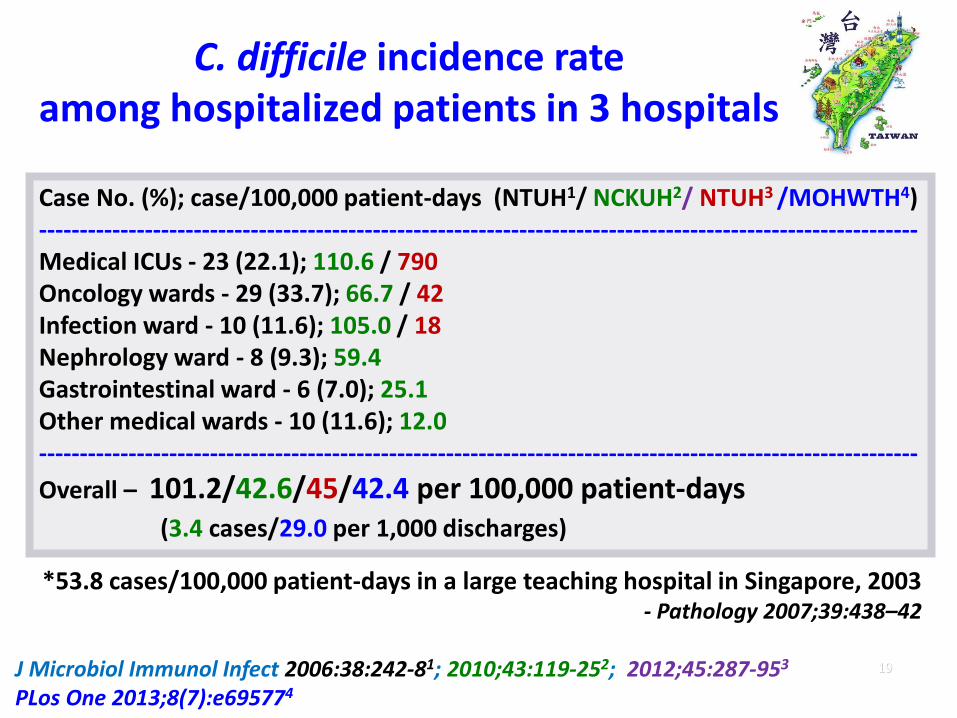
C. difficile incidence rate among hospitalized patients in 3 hospitals
Case No. (%); case/100,000 patient-days (NTUH1/ NCKUH2/ NTUH3 /MOHWTH4)------------------------------------------------------------------------------------------------------------Medical ICUs - 23 (22.1); 110.6 / 790Oncology wards - 29 (33.7); 66.7 / 42Infection ward - 10 (11.6); 105.0 / 18Nephrology ward - 8 (9.3); 59.4Gastrointestinal ward - 6 (7.0); 25.1Other medical wards - 10 (11.6); 12.0------------------------------------------------------------------------------------------------------------
Overall – 101.2/42.6/45/42.4 per 100,000 patient-days (3.4 cases/29.0 per 1,000 discharges)
J Microbiol Immunol Infect 2006:38:242-81; 2010;43:119-252; 2012;45:287-953
PLos One 2013;8(7):e695774
*53.8 cases/100,000 patient-days in a large teaching hospital in Singapore, 2003 - Pathology 2007;39:438–42
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
0
50
100
150
200
250
300
350
400
450
500
550
600
650
700
Positive
Negative
Pos.%
2020
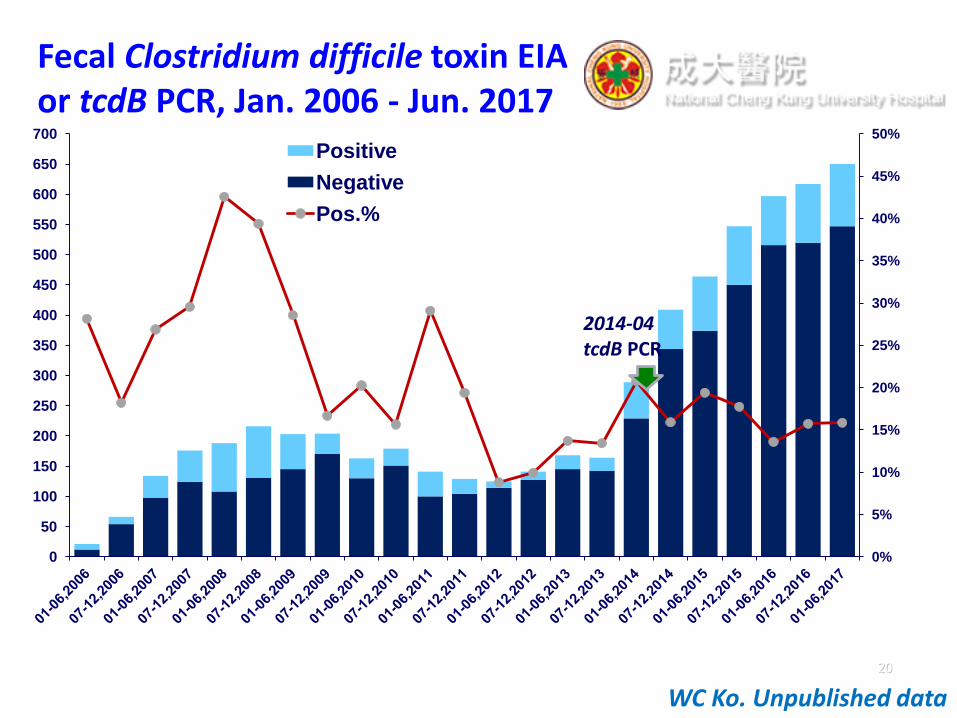
Fecal Clostridium difficile toxin EIA or tcdB PCR, Jan. 2006 - Jun. 2017
WC Ko. Unpublished data
2014-04tcdB PCR

Hospital No. of toxigenic
isolates/no. of
isolates
collected
Rate (%) of
toxigenic
isolates
collected
Year
Total test
no./ 100,000
patient-day
Positive
tests no.
/100,000
patient-day
Positive
test
rate (%)
A 227/331 68.6
2015 194.4 45.8 23.6
2016 284.7 63.0 22.1
B 94/194 48.5
2015 52.3 7.3 14.0
2016 43.2 5.8 13.4
C 149/153 97.4
2015 149.9 26.3 17.5
2016 214.3 32.6 15.2
D 310/329 94.2
2015 260.5 48.2 18.5
2016 312.9 45.9 14.7
E 124/192 64.6
2015 284.6 30.3 10.6
2016 196.6 11.7 6.0
Geographic distribution and isolate numbers of
clinical C. difficile isolates and laboratory burden of C. difficile tests in 5 hospitals

Toxin gene and ribotype distribution of 904 clinical C. difficile isolates in 5 Taiwan hospitals, 2015-2016
tcdA+/tcdB+/cdtA+/cdtB+/
tcdC deletion (81)- RT 027 lineage: 19% (15)
- RT 078 lineage: 75% (61)
tcdA+/tcdB+/cdtA+/cdtB+ (87): 93% (81) tcdC deletion
tcdA+/tcdB+ (794): 11% (87) cdtA+/cdtB+
toxigenic (904): 88% (794) tcdA+/tcdB+; 12% (110) tcdA-/tcdB+- 91% (100) RT 017

23
艱難梭菌感染風險因素
高致病性菌株
老年 (大於65歲)
長期住院
免疫功能低下或抑制
先前艱難梭菌感染
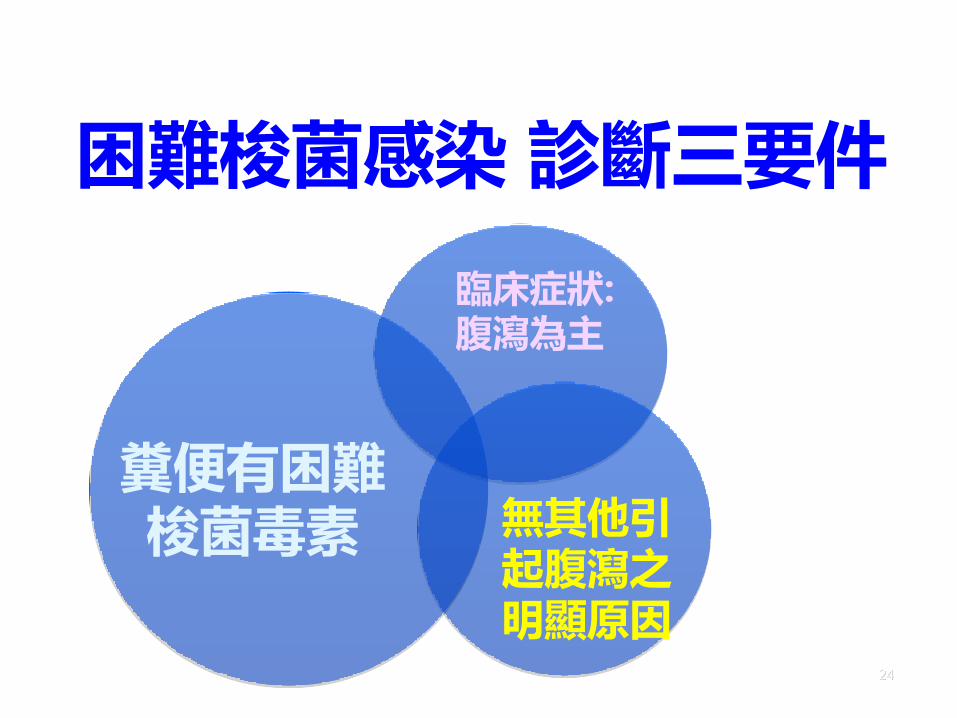
困難梭菌感染 診斷三要件
24
糞便有困難梭菌毒素 無其他引
起腹瀉之明顯原因
臨床症狀: 腹瀉為主

困難梭狀芽孢桿菌感染(CDI-Clostridium difficile Infection; code: GI-CDI)
困難梭狀芽孢桿菌感染收案至少須符合任一標準: 標準1:非固體化糞便 (即糞便形狀會隨容器形狀改變)檢查顯示產毒性困難梭狀芽孢桿菌
(toxin-producing C. difficile) 陽性。
標準2:經手術 (包括內鏡檢查) 或組織病理學檢查發現有偽膜性結腸炎證據。
註釋 標準1 感染日期 (DOE),應依非固體化糞便檢體採集日期認計,非糞便性狀開始改變日期。
須有產毒性困難梭狀芽孢桿菌檢驗陽性及非固體化糞便 2項條件並存,才符合標準1。
通報注意事項 如病人同時檢出其他腸道致病原,除通報困難梭狀芽孢桿菌感染 (CDI)外,應依病人所符合
判定標準,同時通報腸胃炎 (GE)或胃腸道感染 (GIT)。
應依第一章所揭示重複感染期 (RIT)原則,判定個案是否符合再次通報新困難梭狀芽孢桿菌感染事件。
胃腸炎不包括困難梭狀芽孢桿菌感染。
25
- 美國國家醫療保健安全網 (NHSN)2017年版工作手冊
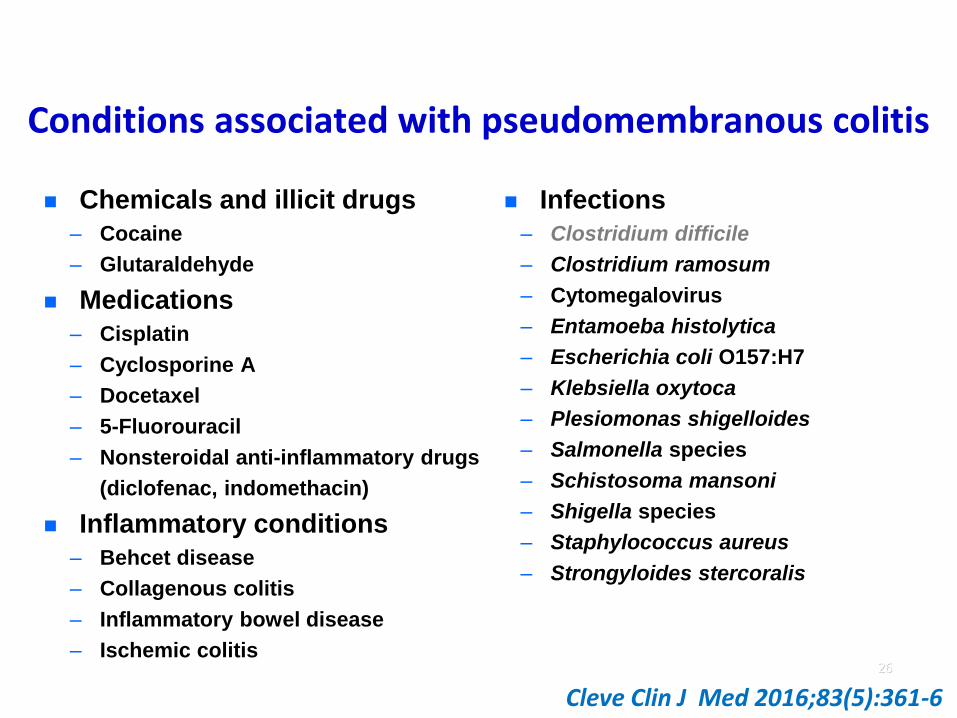
Conditions associated with pseudomembranous colitis
Chemicals and illicit drugs
– Cocaine
– Glutaraldehyde
Medications
– Cisplatin
– Cyclosporine A
– Docetaxel
– 5-Fluorouracil
– Nonsteroidal anti-inflammatory drugs
(diclofenac, indomethacin)
Inflammatory conditions
– Behcet disease
– Collagenous colitis
– Inflammatory bowel disease
– Ischemic colitis
Infections
– Clostridium difficile
– Clostridium ramosum
– Cytomegalovirus
– Entamoeba histolytica
– Escherichia coli O157:H7
– Klebsiella oxytoca
– Plesiomonas shigelloides
– Salmonella species
– Schistosoma mansoni
– Shigella species
– Staphylococcus aureus
– Strongyloides stercoralis
26
Cleve Clin J Med 2016;83(5):361-6
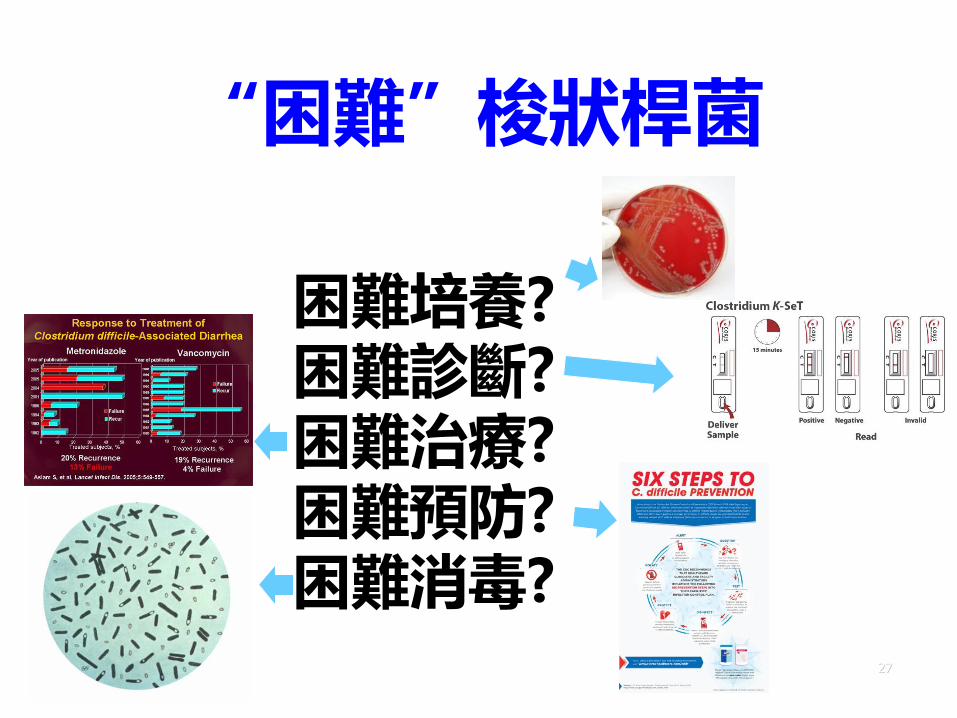
困難培養?困難診斷?困難治療?困難預防?困難消毒?
27
“困難”梭狀桿菌
28
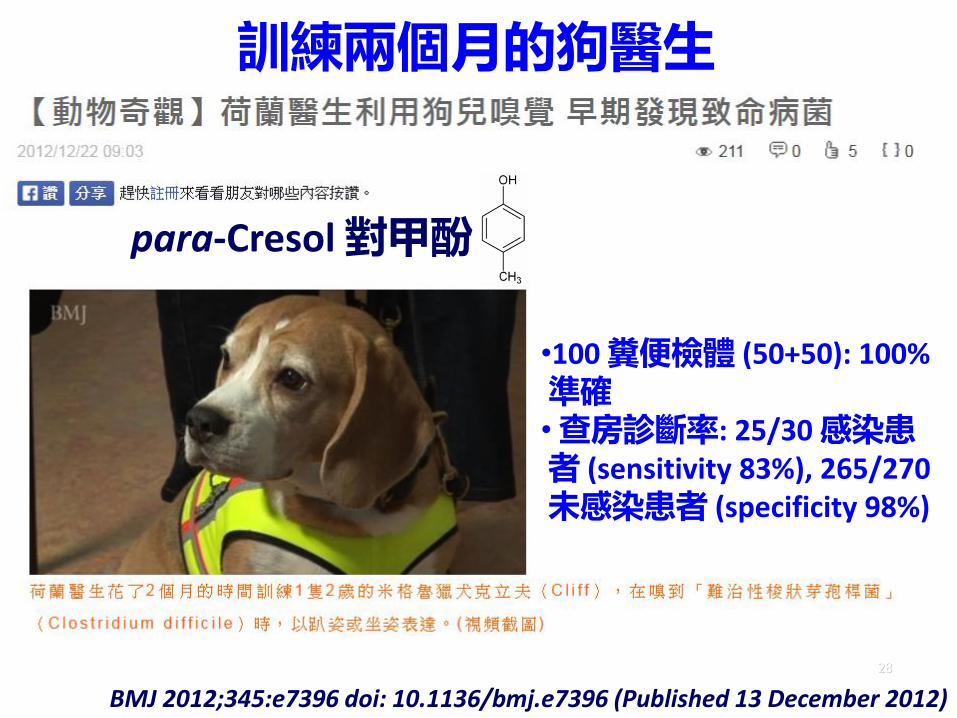
•100 糞便檢體 (50+50): 100% 準確• 查房診斷率: 25/30 感染患者 (sensitivity 83%), 265/270 未感染患者 (specificity 98%)
BMJ 2012;345:e7396 doi: 10.1136/bmj.e7396 (Published 13 December 2012)
訓練兩個月的狗醫生
para-Cresol 對甲酚

巧克力品牌?
1
7
6
5
4
3
2
Bristol Stool Chart

艱難梭菌感染診斷方式: 臨床效能
30
JAMA 2015;313(4):398-408
檢驗項目 敏感性 專一性
谷氨酸去氫酶免疫螢光法
GDH EIA 0.88-0.92 0.89-0.93
核酸複製檢測 NAAT 0.87-0.92 0.94-0.97
毒素免疫螢光法 Toxin EIA 0.73-0.87 0.97-0.98
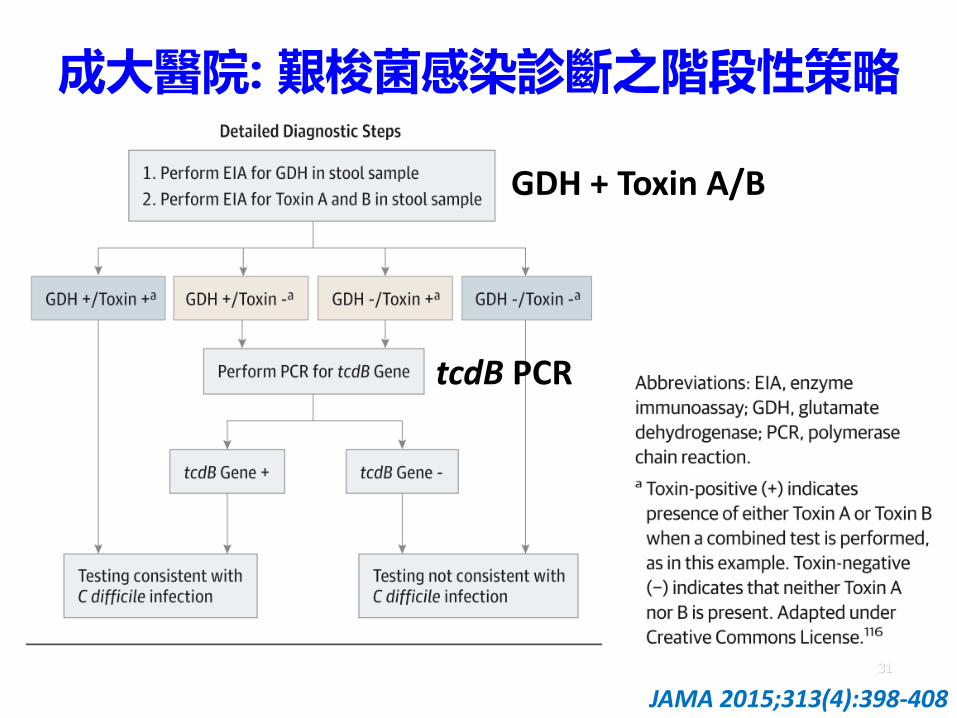
成大醫院: 艱梭菌感染診斷之階段性策略
31
JAMA 2015;313(4):398-408
GDH + Toxin A/B
tcdB PCR

困難梭狀桿菌: 預防與控制 Healthcare settings
– Infection control
Surveillance
Prevention strategiesEarly detection and isolation
Contact precautions
Hand hygiene
Environmental cleaning
– Antibiotic stewardship
– Avoiding gastric acid suppression
32
Investigational areas: Use of probiotics Asymptomatic carriers
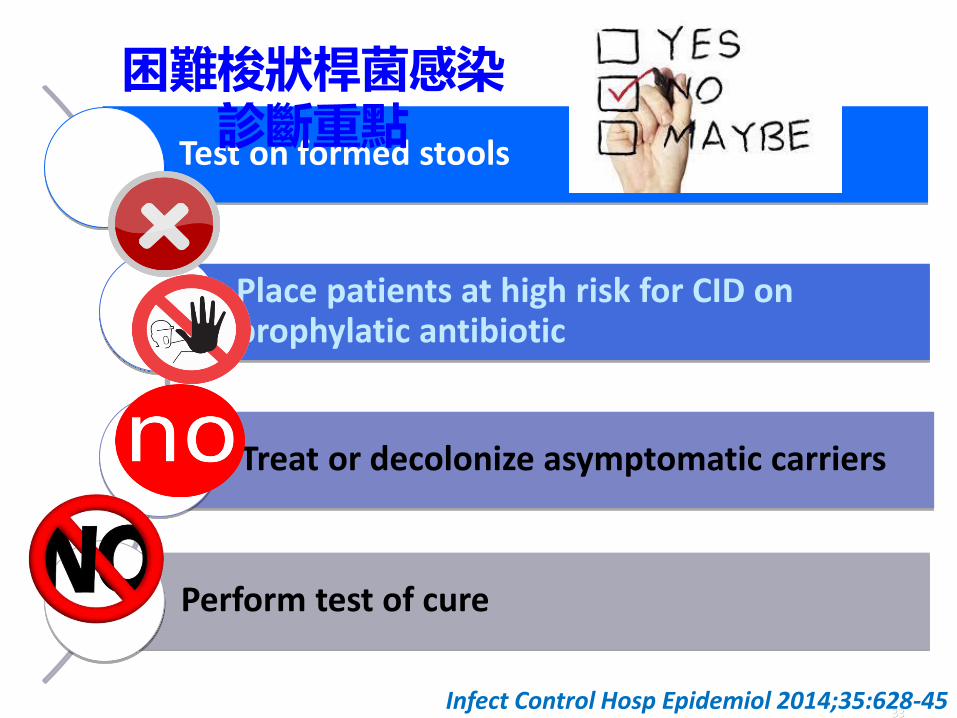
Test on formed stools
Place patients at high risk for CID on prophylatic antibiotic
Treat or decolonize asymptomatic carriers
Perform test of cure
33Infect Control Hosp Epidemiol 2014;35:628-45
困難梭狀桿菌感染診斷重點

困難梭狀桿菌: 預防與控制
Healthcare settings
– Infection control
盛行率監視 Prevention strategies
Early detection and isolation
Contact precautions
Hand hygiene
Environmental cleaning
– Antibiotic stewardship
– Avoiding gastric acid suppression
34
Investigational areas: Use of probiotics Asymptomatic carriers
困難梭狀桿菌: 預防與控制
Healthcare settings
– Infection control
Surveillance
Prevention strategies
早期偵測和隔離Contact precautions
Hand hygiene
Environmental cleaning
– Antibiotic stewardship
– Avoiding gastric acid suppression
35
Investigational areas: Use of probiotics Asymptomatic carriers

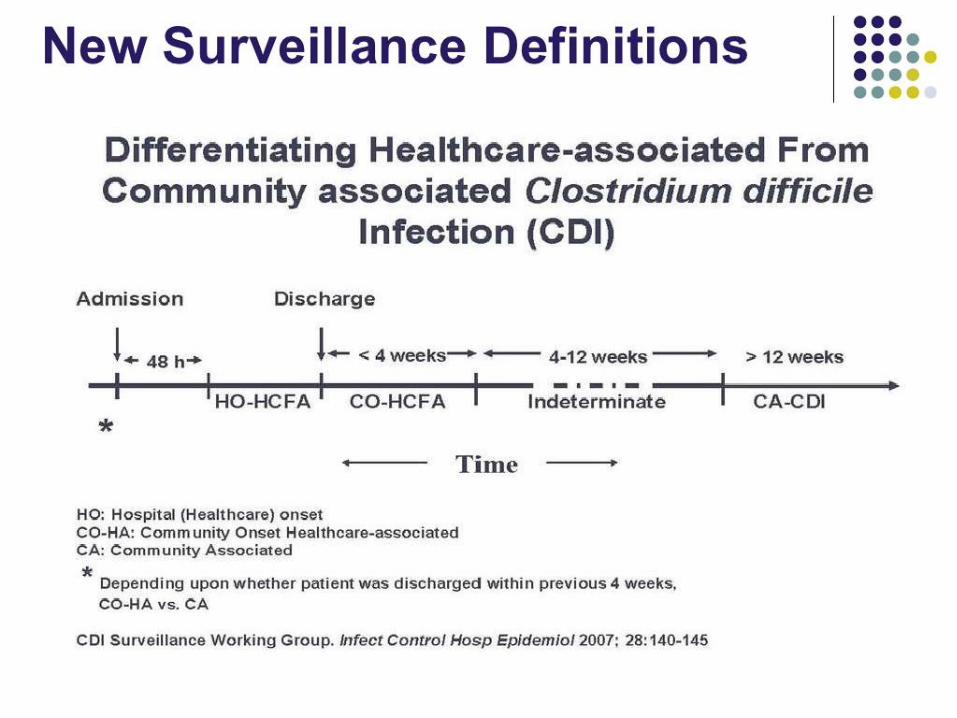
困難梭狀桿菌感染:監測定義 Healthcare facility-onset, healthcare facility-associated
– symptom onset >3 days after admission to a healthcare facility, with day of admission being day 1
Community-onset, healthcare facility-associated
– symptom onset in the community or ≤3 days from admission, provided symptom onset was <4 weeks after the last discharge from a healthcare facility
Community-associated
– symptom onset in the community or ≤ 3 days after admission to a healthcare facility, provided that symptom onset was >12 weeks after the last discharge from a healthcare facility
36
Infect Control Hosp Epidemiol 2014;35:628-645
困難梭狀桿菌: 預防與控制
Healthcare settings
– Infection control
Surveillance
Prevention strategiesEarly detection and isolation
接觸隔離Hand hygiene
Environmental cleaning
– Antibiotic stewardship
– Avoiding gastric acid suppression
37
Investigational areas: Use of probiotics Asymptomatic carriers
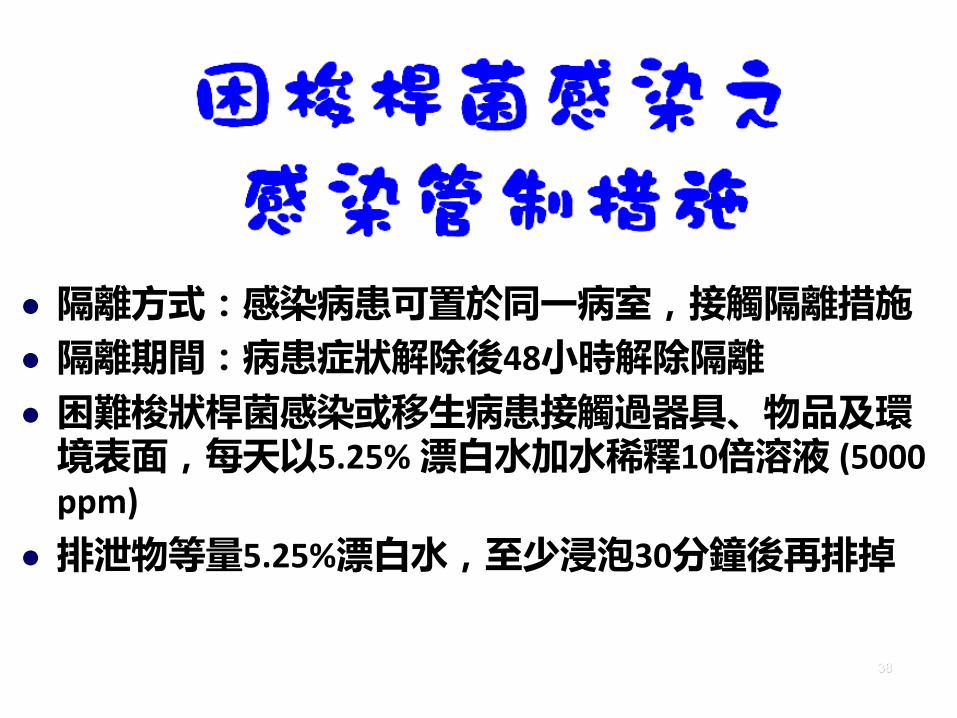
隔離方式:感染病患可置於同一病室,接觸隔離措施
隔離期間:病患症狀解除後48小時解除隔離
困難梭狀桿菌感染或移生病患接觸過器具、物品及環境表面,每天以5.25% 漂白水加水稀釋10倍溶液 (5000 ppm)
排泄物等量5.25%漂白水,至少浸泡30分鐘後再排掉
38

困難梭狀桿菌感染患者之接觸隔離
Hand hygiene
Gloves GownsSingle-patient room
39
Quality of evidence -I: high; II: moderate; III: low
Infect Control Hosp Epidemiol 2014;35:628-45
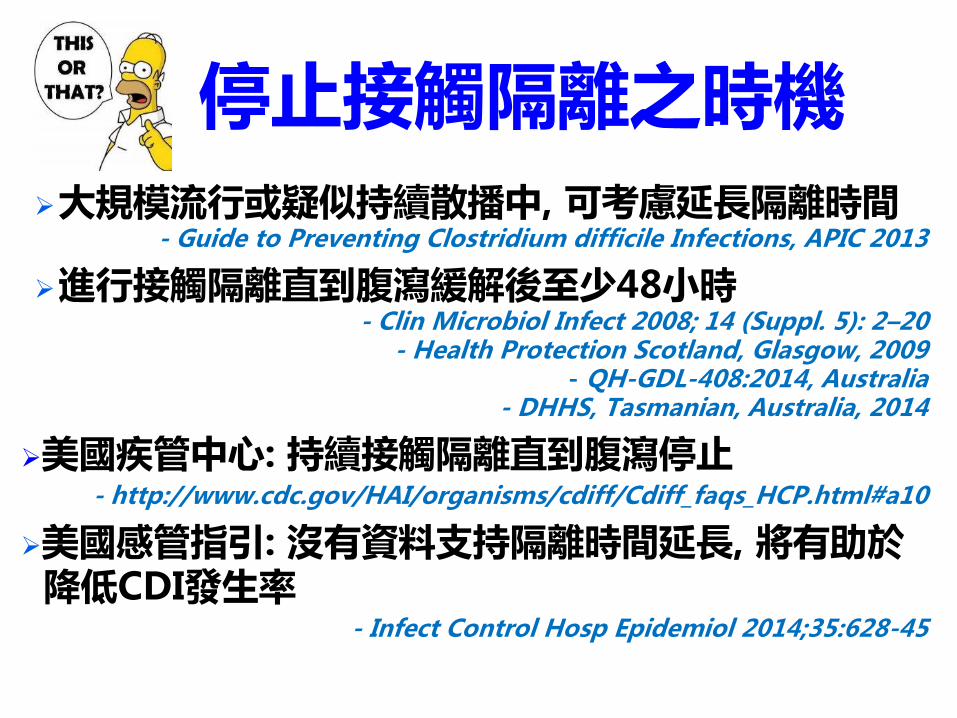
停止接觸隔離之時機大規模流行或疑似持續散播中, 可考慮延長隔離時間
- Guide to Preventing Clostridium difficile Infections, APIC 2013
進行接觸隔離直到腹瀉緩解後至少48小時- Clin Microbiol Infect 2008; 14 (Suppl. 5): 2–20
- Health Protection Scotland, Glasgow, 2009- QH-GDL-408:2014, Australia
- DHHS, Tasmanian, Australia, 2014
美國疾管中心: 持續接觸隔離直到腹瀉停止- http://www.cdc.gov/HAI/organisms/cdiff/Cdiff_faqs_HCP.html#a10
美國感管指引: 沒有資料支持隔離時間延長, 將有助於降低CDI發生率
- Infect Control Hosp Epidemiol 2014;35:628-45
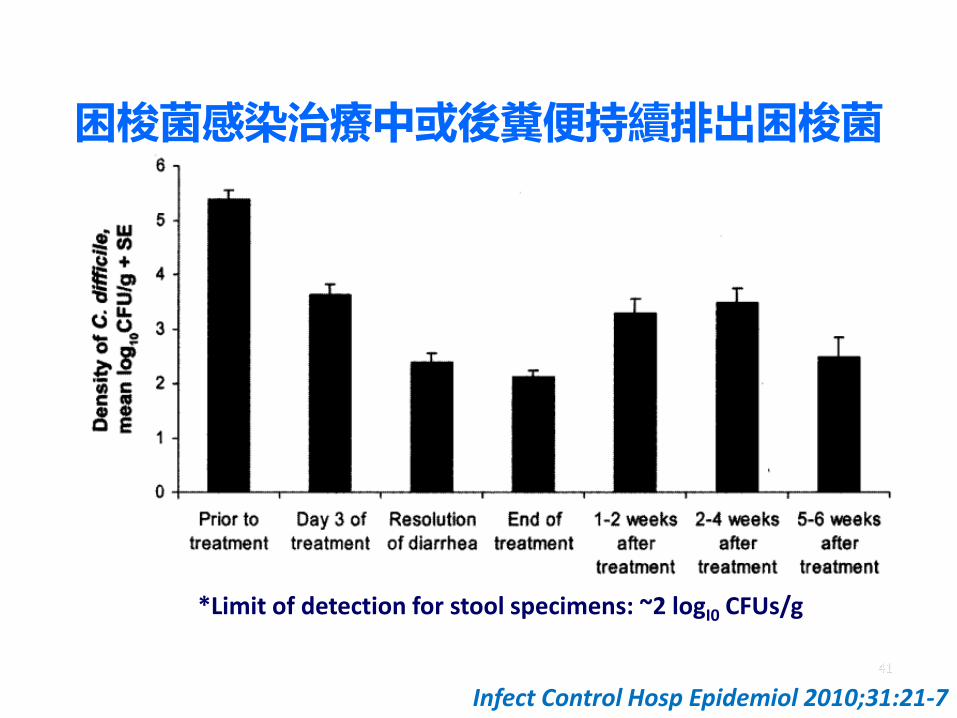
困梭菌感染治療中或後糞便持續排出困梭菌
41
*Limit of detection for stool specimens: ~2 logI0 CFUs/g
Infect Control Hosp Epidemiol 2010;31:21-7
困難梭狀桿菌: 預防與控制 Healthcare settings
– Infection control
Surveillance
Prevention strategiesEarly detection and isolation
Contact precautions
手部衛生Environmental cleaning
– Antibiotic stewardship
– Avoiding gastric acid suppression
42
Investigational areas: Use of probiotics Asymptomatic carriers

43
溫肥皂水洗手優先酒精洗手劑對艱難梭菌無效
Infect Control Hosp Epidemiol 2009;30:939-44
*溫肥皂水>冷肥皂水>酒精洗手劑
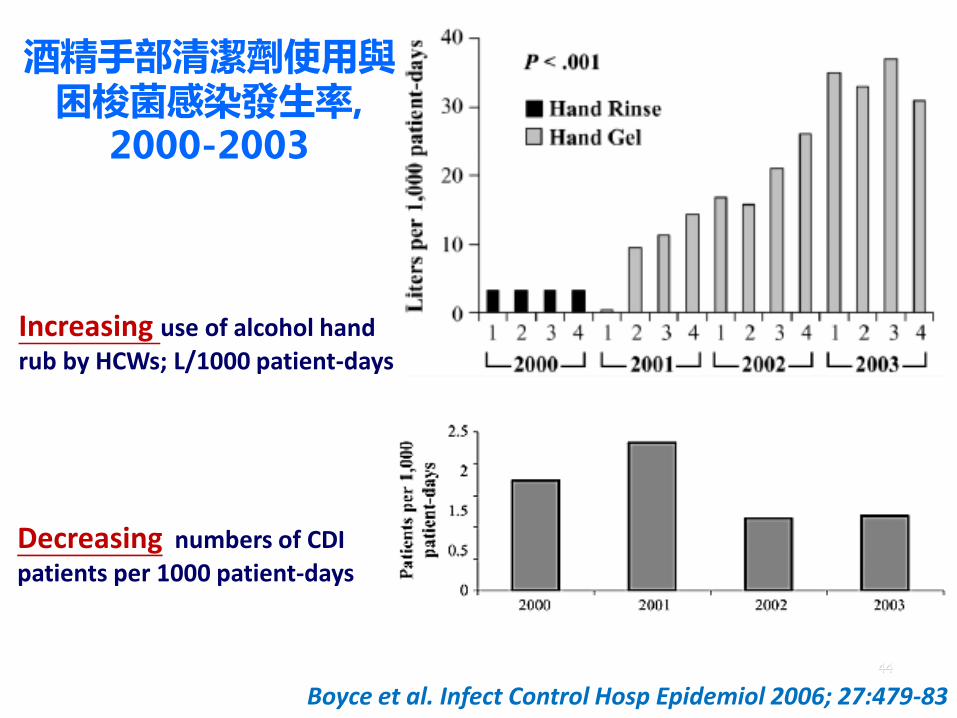
44
酒精手部清潔劑使用與困梭菌感染發生率,
2000-2003
Boyce et al. Infect Control Hosp Epidemiol 2006; 27:479-83
Increasing use of alcohol hand
rub by HCWs; L/1000 patient-days
Decreasing numbers of CDI
patients per 1000 patient-days
困難梭狀桿菌: 預防與控制
Healthcare settings
– Infection control
Surveillance
Prevention strategiesEarly detection and isolation
Contact precautions
Hand hygiene
環境清潔
– Antibiotic stewardship
– Avoiding gastric acid suppression
45
Investigational areas: Use of probiotics Asymptomatic carriers
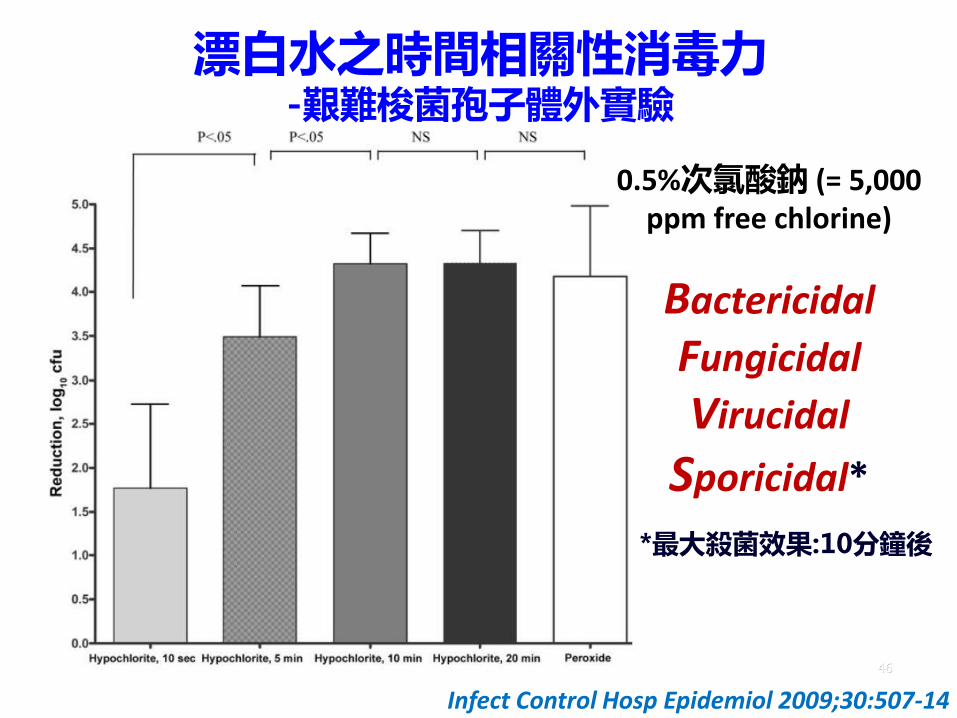
漂白水之時間相關性消毒力-艱難梭菌孢子體外實驗
46
Infect Control Hosp Epidemiol 2009;30:507-14
0.5%次氯酸鈉 (= 5,000 ppm free chlorine)
Bactericidal
Fungicidal
Virucidal
Sporicidal*
*最大殺菌效果:10分鐘後

困難梭狀桿菌: 預防與控制
Healthcare settings
– Infection control
Surveillance
Prevention strategiesEarly detection and isolation
Contact precautions
Hand hygiene
Environmental cleaning
–抗生素管理計畫– Avoiding gastric acid suppression
47
Investigational areas: Use of probiotics Asymptomatic carriers
Antibiotic strategies to reduce CDI risk
Restrict cephalosporins or clindamycin use
Reduce unnecessary antibiotic use
Reduce prolonged antibiotic duration
Avoid the use of multiple antibiotic classes
Promote de-escalation of broad-spectrum therapy ASAP
48
J Antimicrob Chemother 2017; 72: 1–18
- balloon squeezing effect
抗生素管理計畫
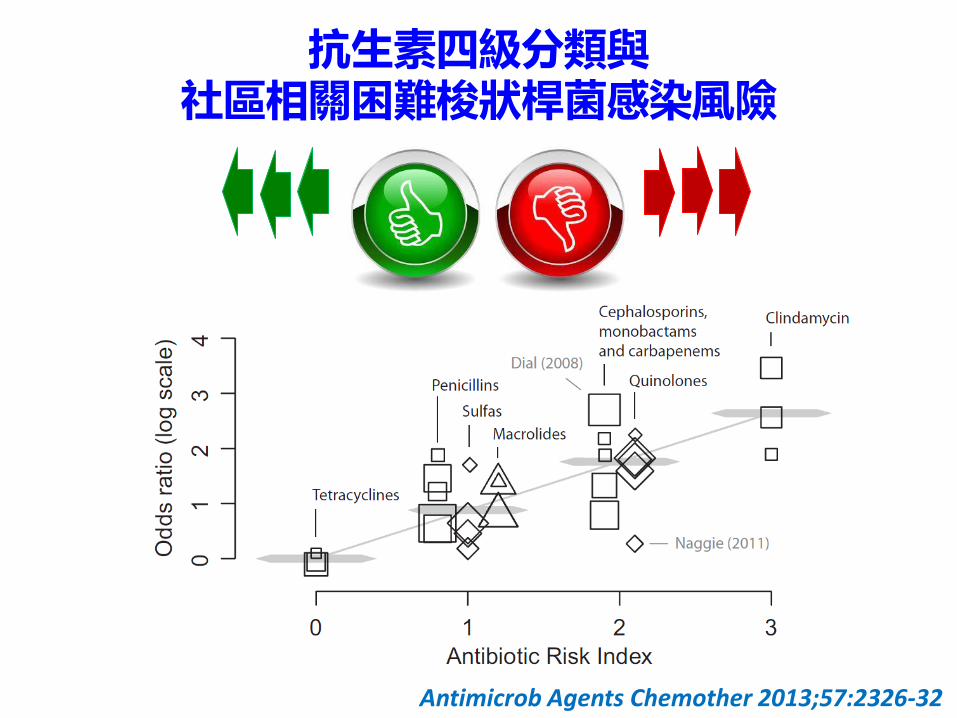
抗生素四級分類與社區相關困難梭狀桿菌感染風險
Antimicrob Agents Chemother 2013;57:2326-32
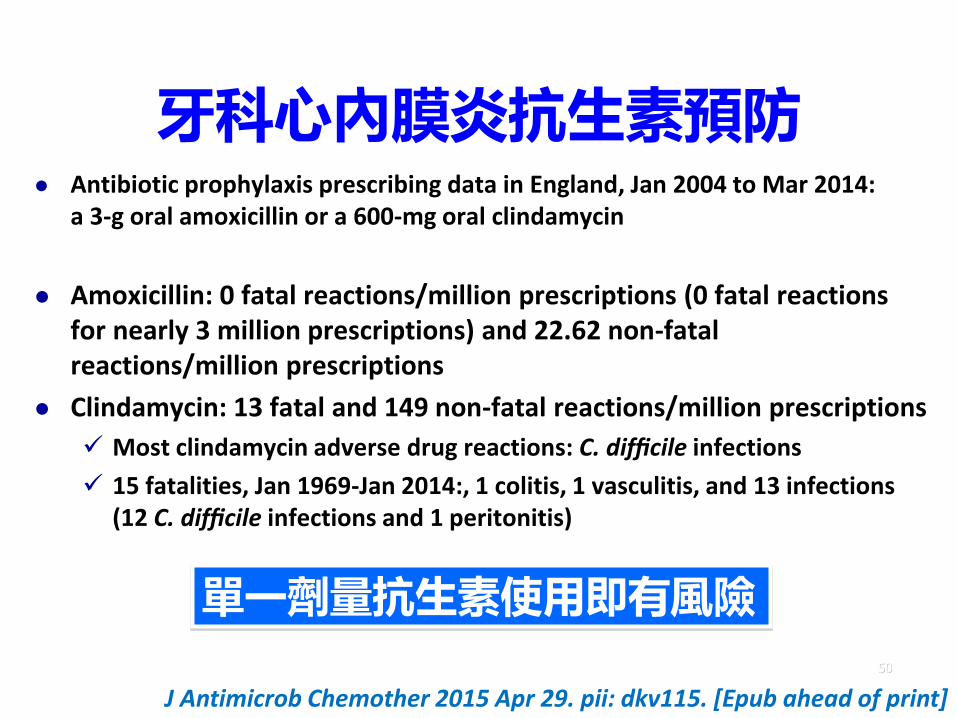
牙科心內膜炎抗生素預防 Antibiotic prophylaxis prescribing data in England, Jan 2004 to Mar 2014:
a 3-g oral amoxicillin or a 600-mg oral clindamycin
Amoxicillin: 0 fatal reactions/million prescriptions (0 fatal reactions for nearly 3 million prescriptions) and 22.62 non-fatal reactions/million prescriptions
Clindamycin: 13 fatal and 149 non-fatal reactions/million prescriptions
Most clindamycin adverse drug reactions: C. difficile infections
15 fatalities, Jan 1969-Jan 2014:, 1 colitis, 1 vasculitis, and 13 infections (12 C. difficile infections and 1 peritonitis)
50
J Antimicrob Chemother 2015 Apr 29. pii: dkv115. [Epub ahead of print]
單一劑量抗生素使用即有風險
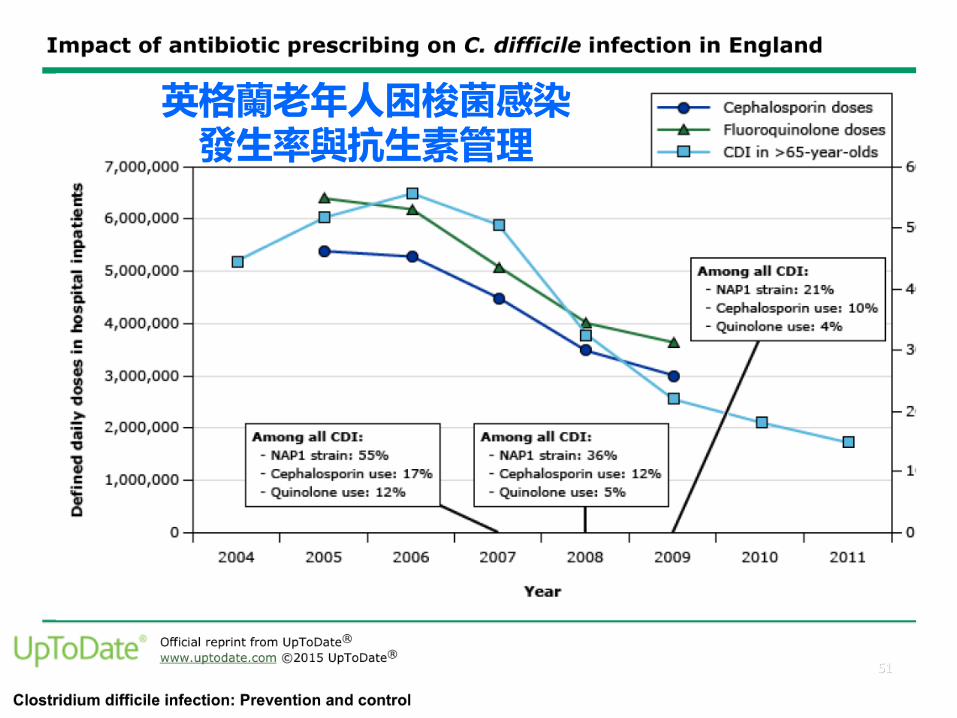
51
英格蘭老年人困梭菌感染發生率與抗生素管理
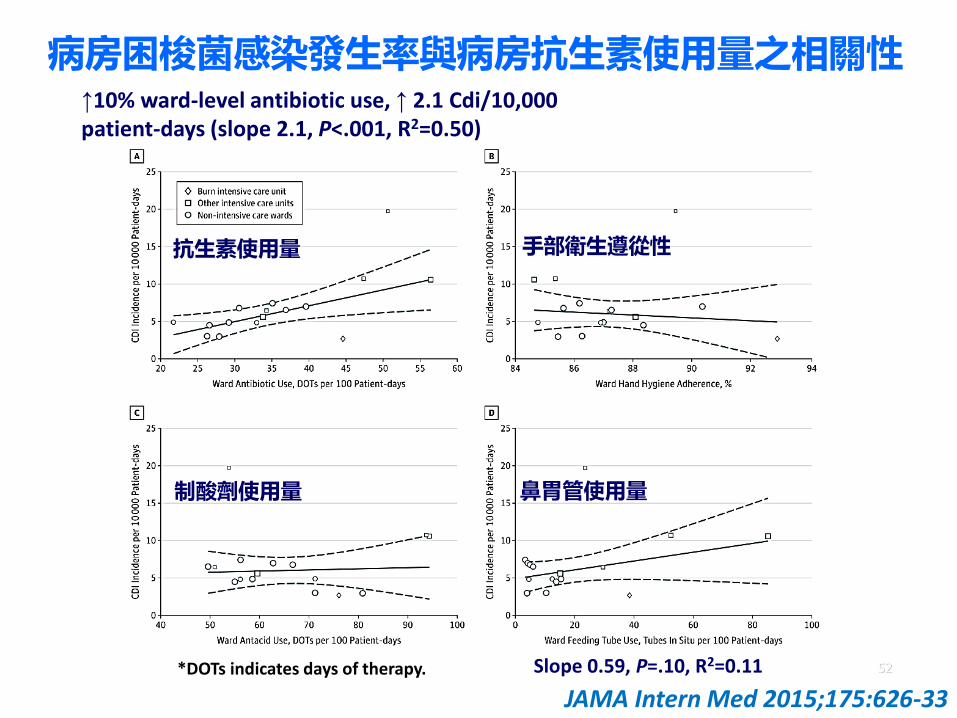
病房困梭菌感染發生率與病房抗生素使用量之相關性
52*DOTs indicates days of therapy.
JAMA Intern Med 2015;175:626-33
↑10% ward-level antibiotic use, ↑ 2.1 Cdi/10,000 patient-days (slope 2.1, P<.001, R2=0.50)
Slope 0.59, P=.10, R2=0.11
d
抗生素使用量
鼻胃管使用量
手部衛生遵從性
制酸劑使用量
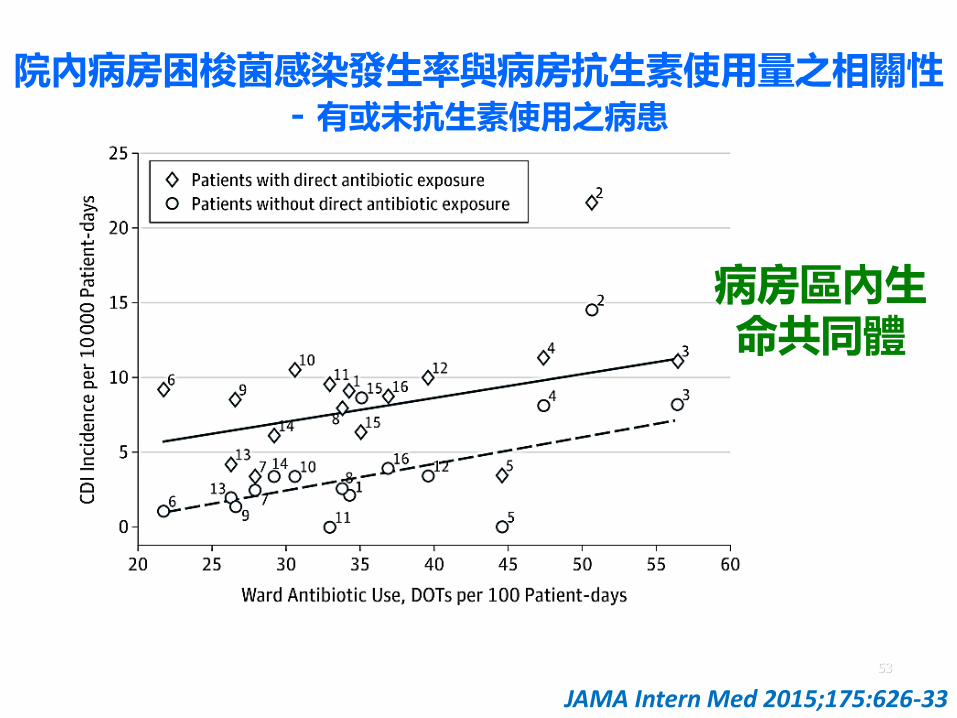
院內病房困梭菌感染發生率與病房抗生素使用量之相關性- 有或未抗生素使用之病患
53
JAMA Intern Med 2015;175:626-33
病房區內生命共同體
困難梭狀桿菌: 預防與控制
Healthcare settings
– Infection control
Surveillance
Prevention strategiesEarly detection and isolation
Contact precautions
Hand hygiene
Environmental cleaning
Chlorhexidine bathing
– Antibiotic stewardship
–避免胃酸抑制54
Investigational areas: Use of probiotics Asymptomatic carriers
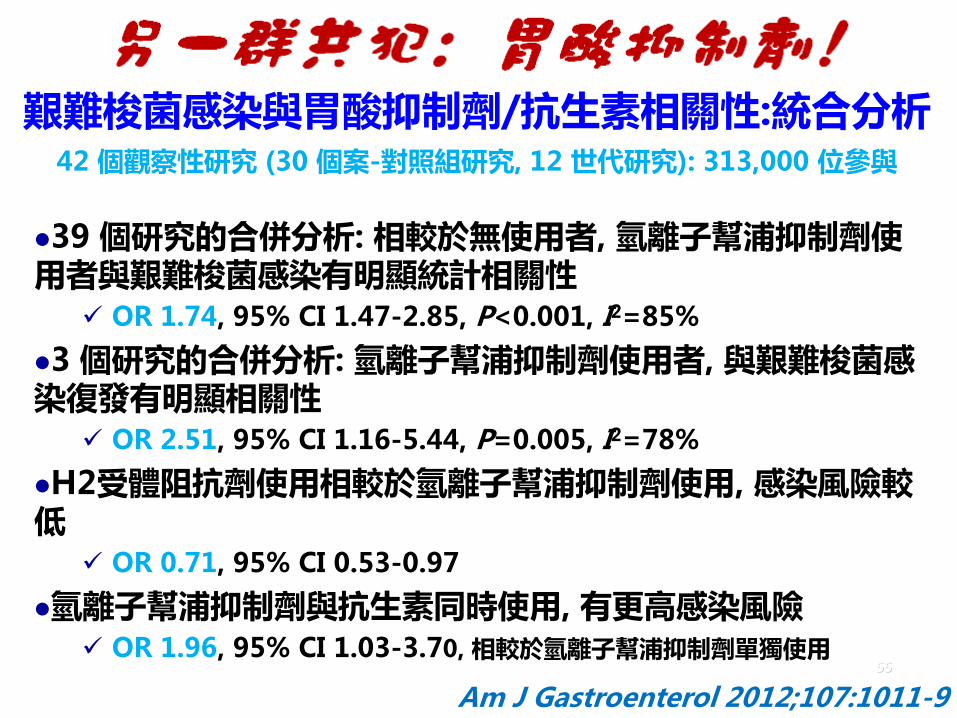
艱難梭菌感染與胃酸抑制劑/抗生素相關性:統合分析42 個觀察性研究 (30 個案-對照組研究, 12 世代研究): 313,000 位參與
39 個研究的合併分析: 相較於無使用者, 氫離子幫浦抑制劑使用者與艱難梭菌感染有明顯統計相關性
OR 1.74, 95% CI 1.47-2.85, P<0.001, I2=85%
3 個研究的合併分析: 氫離子幫浦抑制劑使用者, 與艱難梭菌感染復發有明顯相關性
OR 2.51, 95% CI 1.16-5.44, P=0.005, I2=78%
H2受體阻抗劑使用相較於氫離子幫浦抑制劑使用, 感染風險較低
OR 0.71, 95% CI 0.53-0.97
氫離子幫浦抑制劑與抗生素同時使用, 有更高感染風險 OR 1.96, 95% CI 1.03-3.70, 相較於氫離子幫浦抑制劑單獨使用
55
Am J Gastroenterol 2012;107:1011-9

Cumulative meta-analysis of risk of developing CDI with
proton-pump inhibitor
56J Hosp Infect 2017 Aug 22. doi: 10.1016/j.jhin.2017.08.017
*Since 2011, the overall association between PPI use and risk of developing CDI has remained relatively stable within an effect size between OR 1.20 and 1.26.
*50 studies with a total of342,532 individuals were included in the final meta-analysis.
*Pooled analysis of 50 studies showed a significant association between PPI use and risk of developing CDI, OR 1.26 (95% CI 1.12-1.39, P<0.001)
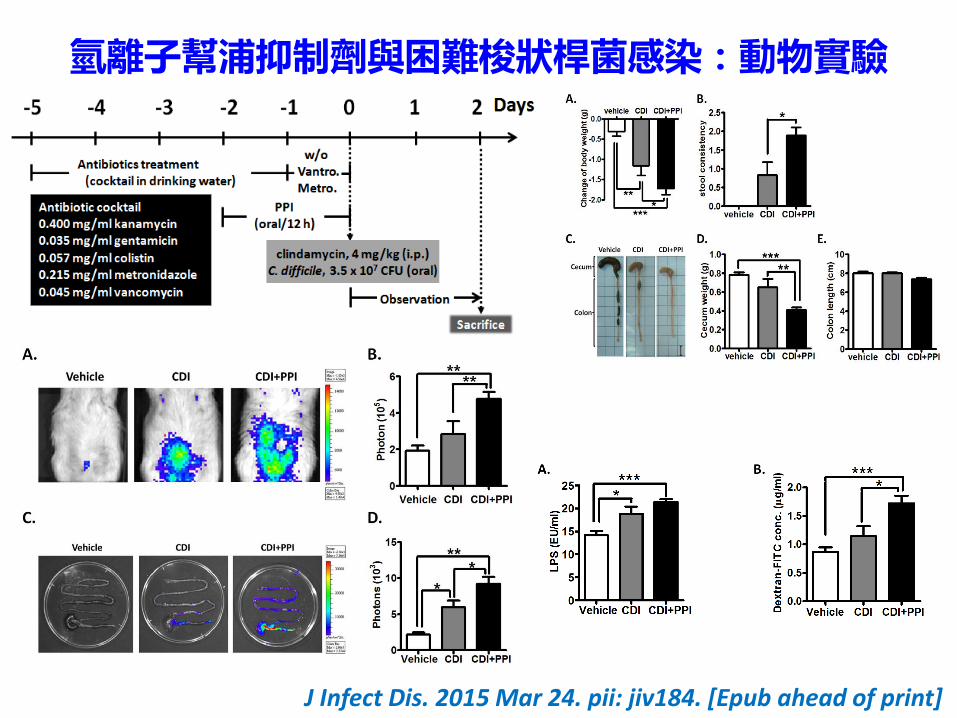
氫離子幫浦抑制劑與困難梭狀桿菌感染:動物實驗
J Infect Dis. 2015 Mar 24. pii: jiv184. [Epub ahead of print]

困難梭狀桿菌: 預防與控制 Healthcare settings
– Infection control
Surveillance
Prevention strategiesEarly detection and isolation
Contact precautions
Hand hygiene
Environmental cleaning
– Antibiotic stewardship
– Avoiding gastric acid suppression
58
Investigational areas:
益生菌 Asymptomatic carriers
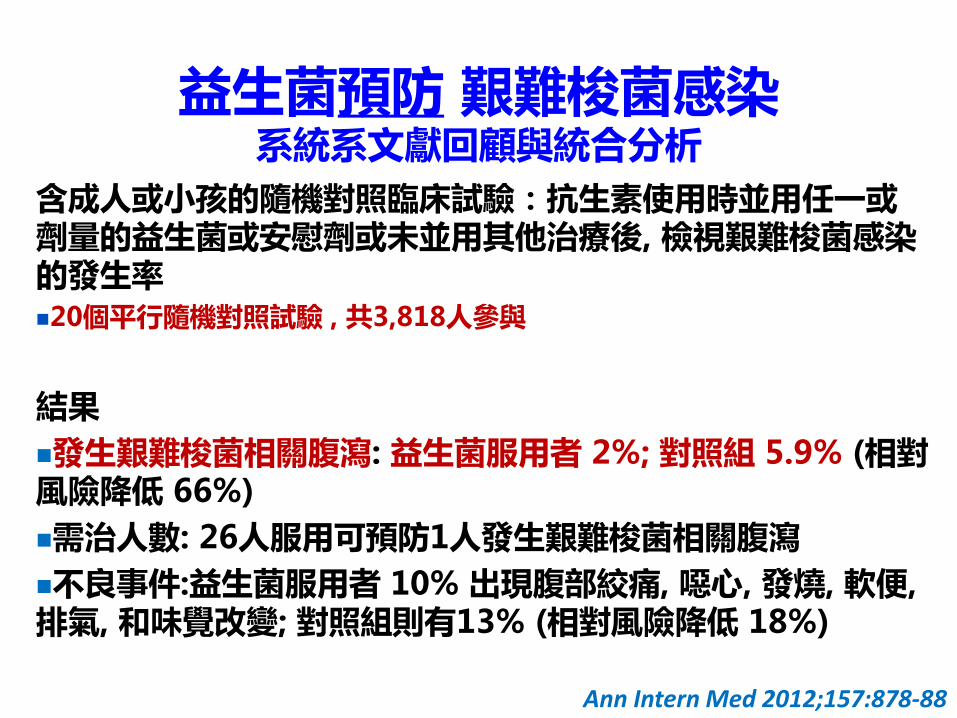
益生菌預防 艱難梭菌感染系統系文獻回顧與統合分析
含成人或小孩的隨機對照臨床試驗:抗生素使用時並用任一或劑量的益生菌或安慰劑或未並用其他治療後, 檢視艱難梭菌感染的發生率20個平行隨機對照試驗 , 共3,818人參與
結果
發生艱難梭菌相關腹瀉: 益生菌服用者 2%; 對照組 5.9% (相對風險降低 66%)
需治人數: 26人服用可預防1人發生艱難梭菌相關腹瀉
不良事件:益生菌服用者 10% 出現腹部絞痛, 噁心, 發燒, 軟便, 排氣, 和味覺改變; 對照組則有13% (相對風險降低 18%)
Ann Intern Med 2012;157:878-88

益生菌使用建議:2015
60
J Clin Gastroenterol 2015;49 Suppl 1:S69-73
其他使用時機:壞死性小腸結腸炎, 兒童腹瀉, 炎症性腸病, 躁症腸病.
無治療艱難梭菌感染之建議!
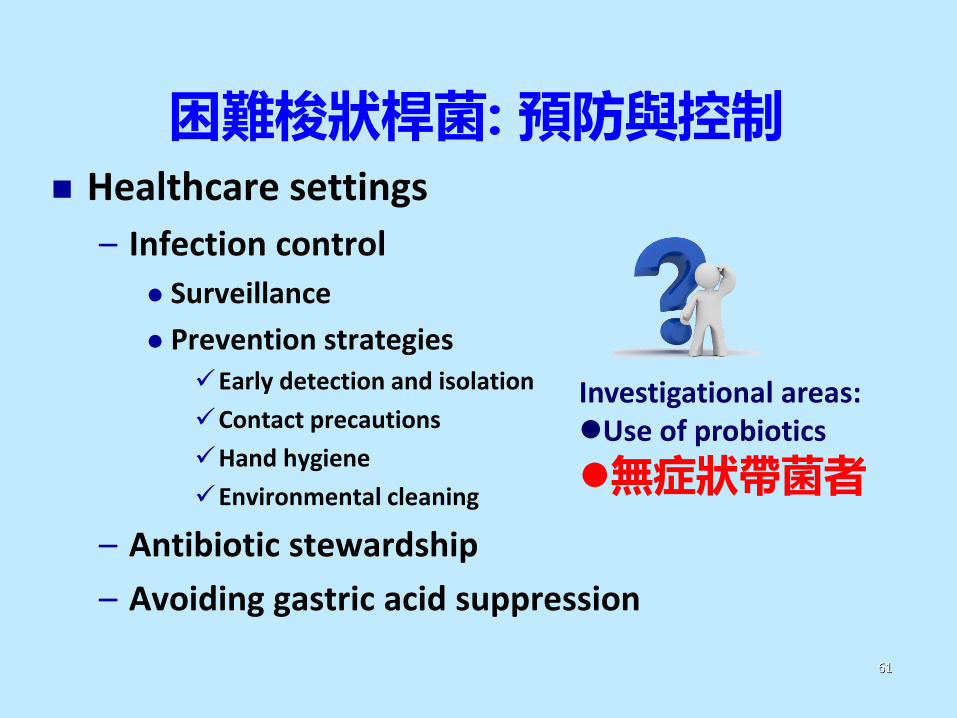
困難梭狀桿菌: 預防與控制 Healthcare settings
– Infection control
Surveillance
Prevention strategiesEarly detection and isolation
Contact precautions
Hand hygiene
Environmental cleaning
– Antibiotic stewardship
– Avoiding gastric acid suppression
61
Investigational areas:Use of probiotics
無症狀帶菌者
困難梭狀桿菌潛在來源
主要來源: 腹瀉病患
無症狀帶菌者?
水?食物?
寵物?
農場動物?
病房環境

住院時產毒性艱難梭菌定植與發生艱難梭菌感染風險: 系統系文獻回顧與統合分析
19個研究 8,725位病患
艱難梭菌定植 平均盛行率: 8.1% 隨年代漸增 (P=0.003)
北美洲研究: 10.0%
艱難梭菌感染機會: 定植患者21.8%, 非定植患者 3.4% (P=0.03, 歸因
危險度: 18.4%) - 增加6倍風險 產毒性艱難梭菌定植風險因素: 前三
個月內有住院病史 (RR 1.63)
63
Am J Gastroenterol 2015; 110:381–90
Observed (triangles) and fitted (circles) prevalence estimates, by study midyear.

住院患者毒素或非毒素困梭菌感染或移植之篩檢
64
13.15% 80.95%5.89%
7.28%
89.36%
3.36%
PLoS One 2013;8(7):e69577
入院時困梭菌移植: 19%毒素/非毒素困梭菌移植: 2.23/1 住院後發生毒素/非毒素
困梭菌移植: 2.17/1
住院患者追蹤後毒素/非毒素困梭菌移植: 2.32/1
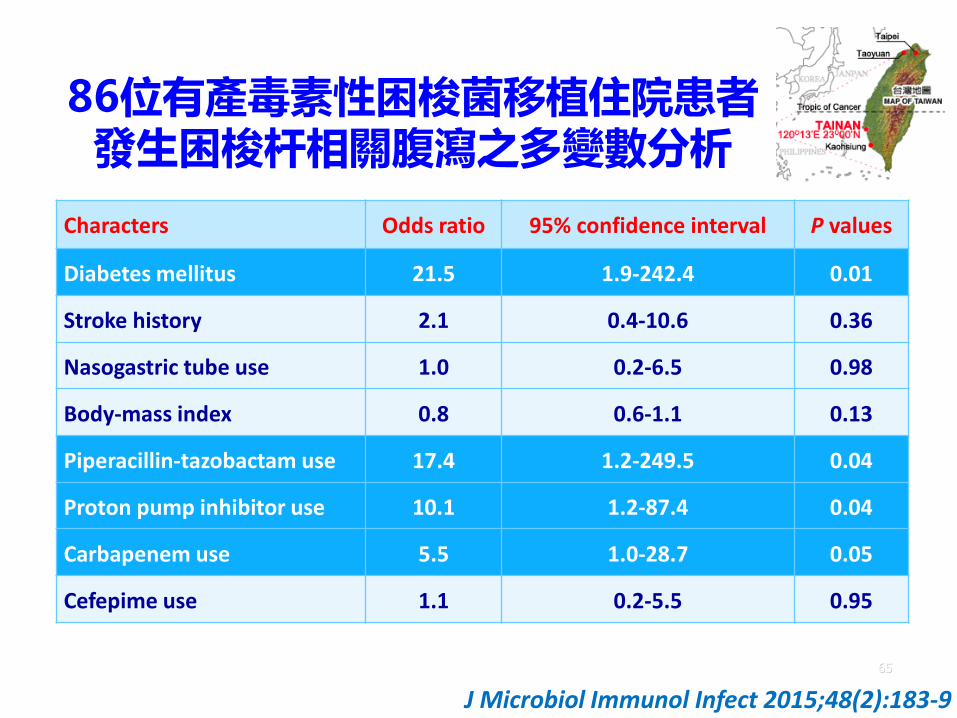
86位有產毒素性困梭菌移植住院患者發生困梭杆相關腹瀉之多變數分析
65
Characters Odds ratio 95% confidence interval P values
Diabetes mellitus 21.5 1.9-242.4 0.01
Stroke history 2.1 0.4-10.6 0.36
Nasogastric tube use 1.0 0.2-6.5 0.98
Body-mass index 0.8 0.6-1.1 0.13
Piperacillin-tazobactam use 17.4 1.2-249.5 0.04
Proton pump inhibitor use 10.1 1.2-87.4 0.04
Carbapenem use 5.5 1.0-28.7 0.05
Cefepime use 1.1 0.2-5.5 0.95
J Microbiol Immunol Infect 2015;48(2):183-9

住院時檢測及隔離帶原者對艱難梭菌感染發生率之影響
2013年11 月-2015年3 月: 加拿大魁北克省 Heart and Lung
Institute
住院篩檢: 每日肛拭一周, 送 tcdB PCR (BD GeneOhm Cdiff
Assay)
帶原者: 住院期間采接觸隔離
7,599 位患者: 368 (4.8%) 位是艱難梭菌帶原者 機構相關艱難梭菌感染*發生率:
介入前 69/100,000人日 vs. 介入後 30/100,000人日 (P<0.001)
66
JAMA Intern Med 2016;176(6):796-804
*C. difficile infection: (1) diarrhea (≥3 unformed or liquid stools in <24 hours) lasting at least 24 hours without any other known etiology, combined with a positive assay for toxigenic C. difficile; (2) visualization of pseudomembranes by colonoscopy; or (3) a histopathologic diagnosis

加拿大魁北克省 Québec Heart and Lung Institute 與其他機構每四周機構相關艱難梭菌感染發生率, Aug. 2004 - Mar. 2015
67
JAMA Intern Med 2016;176(6):796-804
研究介入措施後抗生素與氫離子幫浦抑制劑使用量與趨勢沒有變化
官方設定發生率門檻- 90例/每十萬人日 *機構相關艱難梭菌感染*發生率: 介入前 69/100,000
人日; 介入期 30/100,000人日 (P<0.001)
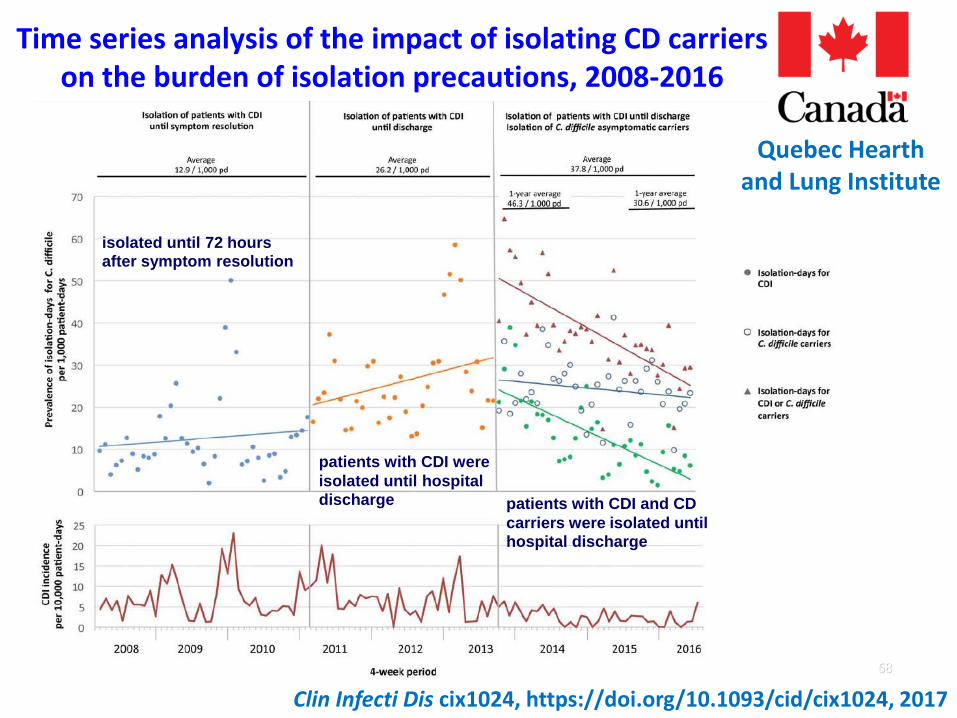
Time series analysis of the impact of isolating CD carriers on the burden of isolation precautions, 2008-2016
68
Clin Infecti Dis cix1024, https://doi.org/10.1093/cid/cix1024, 2017
Quebec Hearth and Lung Institute
isolated until 72 hours after symptom resolution
patients with CDI were
isolated until hospital discharge patients with CDI and CD
carriers were isolated until hospital discharge
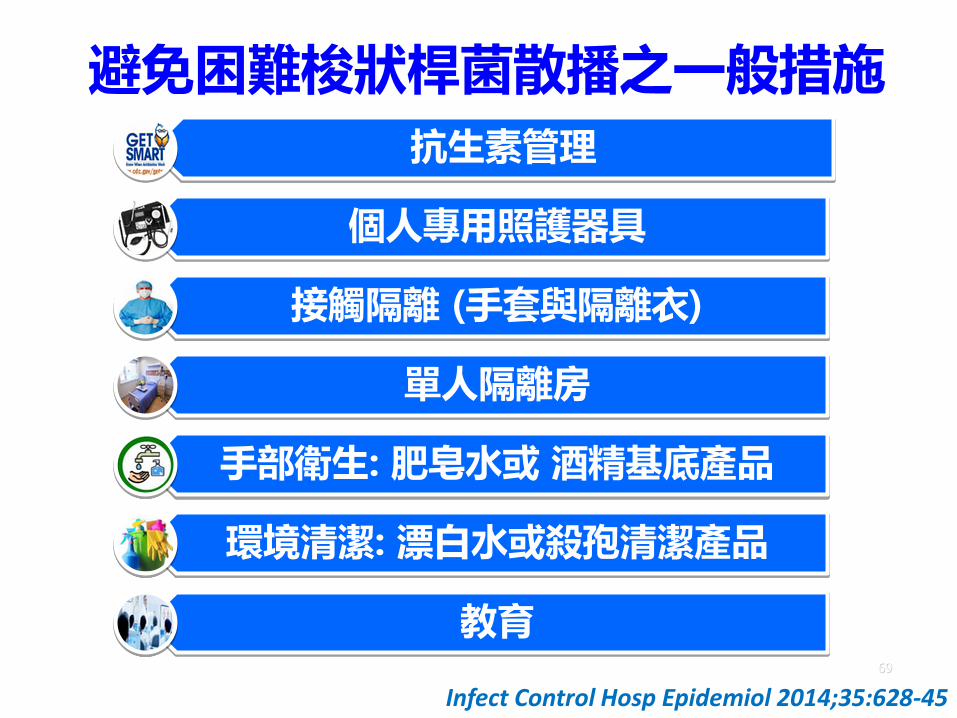
避免困難梭狀桿菌散播之一般措施
抗生素管理
個人專用照護器具
接觸隔離 (手套與隔離衣)
單人隔離房
手部衛生: 肥皂水或 酒精基底產品
環境清潔: 漂白水或殺孢清潔產品
教育69
Infect Control Hosp Epidemiol 2014;35:628-45
艱難梭菌感染-壓死感控的最後一根稻草
好發族群為數眾多
疾病復發率高
誘發因素不易去除
診斷\培養不易,需特定檢查或培養基
出現高致病性克隆
病原菌\孢子來源多樣,尤其是無症狀帶菌者
常用幹式洗手效果不佳
環境病原菌\孢子不易清除
耗費醫療成本之接觸隔離 70
宿主
病原
感控