Embed Size (px)
Citation preview

Asian J Oral Maxillofac Surg. 2009;21:51-53.
© 2009 Asian Association of Oral and Maxillofacial Surgeons. 51
CASE REPORT
Dermoid Cyst with Fistula on the Dorsum of the Tongue
Yoshiyuki Mori, Hideto Saijo, Hisako Fujihara, Yoko Tanaka, Yujiro Maeda, Nobuko Hayashi,Daichi Chikazu, Mitsuyoshi Iino, Tsuyoshi Takato
Department of Oral and Maxillofacial Surgery, Dentistry and Orthodontics, University of Tokyo Hospital, Tokyo, Japan
AbstractA 32-year-old woman presented with difficulty in swallowing and swelling of the tongue. A fistula was seen on the dorsum of the tongue. As T2-weighted magnetic resonance imaging showed a high signal intensity lesion with poorly defined margins, a provisional diagnosis of tongue lipoma or angiomyoli-poma was made. The lesion was surgically removed including the fistula. Sebaceous glands were seen in the epithelial lining on histopathological analysis, which suggested a dermoid cyst. The patient’s postoperative course was satisfactory, and no recurrence has been observed during 18 months of follow-up after surgery.
Key words: Angiomyolipoma, Dermoid cyst, Fistula, Lipoma, Sebaceous glands
Correspondence: Yoshiyuki Mori, DDS, PhD, Department of Oral and Maxillofacial Surgery, Dentistry and Orthodontics, University of Tokyo Hospital, 7-3-1 Hongo, Bunkyo-ku, Tokyo 113-8655, Japan.Tel: (81 3) 5800 8669; Fax: (81 3) 5800 6832;E-mail: [email protected]
Introduction
Dermoid cysts are believed to arise from aberrations of ectodermal tissue in the foetus or from aberrations in the epi-thelia due to trauma or surgery after birth. These cysts appear in various parts of the body, and occurrence in the mouth is reported to be around 1.6%.1 Patients with dermoid cysts ac-companied by fistula on the dorsum of the tongue have only been reported previously by Rise,2 and Korchin and Juan3 and only 1 such report was from Japan.4 This report is of a patient in whom fistula formation was seen on the dorsum of the tongue, which was possibly due to recurrent swelling of the tongue over a long period.
Case Report
The patient was a 32-year-old woman who presented in February 2007 with difficulty in swallowing and swelling of the tongue. From the age of 3 years, the patient had repeat-edly experienced swelling of the tongue from an unknown cause. The swelling had occurred more frequently in recent years. Magnetic resonance imaging (MRI) revealed a lesion in the tongue, and the patient was referred to the Department of Oral and Maxillofacial Surgery, Dentistry and Orthodon-tics, University of Tokyo Hospital, Tokyo, Japan, for detailed examination. The patient had no history of oral trauma or surgery. Systemic findings were normal. Intraorally, a firm
swelling was noted on the right side of the dorsum of the tongue. The surface mucosa of the tongue over the lesion appeared normal. A tumour was suspected.
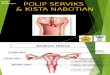
As previous T2-weighted MRI showed a high signal intensity lesion with poorly defined margins, a provisional diagnosis of tongue lipoma or angiomyolipoma was made. Tissue biopsy was scheduled, but the swelling located on the right part of the tongue became red and tender in May 2007. The lesion was elastic-firm, movable, and had clear margins. Clinical laboratory tests indicated the presence of inflam-mation (white blood cells, 7100/ L; C-reactive protein, 4.47 mg/dL). Computed tomography (CT) revealed a cystic lesion with ring enhancement (24 19 mm) in the right deep portion of the anterior half of the tongue (Figure 1a). The swelling decreased after antibiotics were administered (intra-venous piperacillin sodium 2.0 g/day for 6 days followed by oral cefditoren pivoxil 300 mg/day for 4 days). MRI taken after the inflammation had resolved showed a lesion (size, 7
6 19 mm) with distinct margins and a luminal structure in the middle of the tongue (Figure 1b).
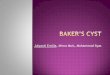
The lesion was surgically removed after the inflammation had subsided completely. Before surgery, another elevated lesion (size, 2 mm in diameter), which had not been noted previously, was seen on the surface of the dorsum of the tongue. A pale yellow cystic fluid was expressed from the dorsum of the tongue when pressure was applied to the floor of the oral cavity. A probe was inserted through the fistula and its tip reached the floor of the oral cavity (Figure 2). The fistula periphery was cut and detached along the fistulous tract, and a portion of the cyst wall was detected. The lesion was then approached from the floor of the mouth, the cyst detached from the surrounding tissue and extirpated entirely,

Dermoid Cyst with Fistula
52 Asian J Oral Maxillofac Surg. Vol 21, Nos 1 & 2, 2009
including the fistula. The extirpated specimen was 34 12 6 mm in size. Histopathologically, the fistulous tract was
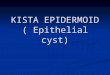
found to originate from the tongue surface and was connect-ed to the cystic lesion. The wall of the cystic lesion was lined with stratified squamous epithelium, and parakeratosis was seen. Although the contents of the cyst were not confirmed, a diagnosis of dermoid cyst was made based on the sebaceous glands observed in the connective wall of the cyst (Figure 3). The patient’s postoperative course was satisfactory, and no recurrence has been observed 18 months after surgery.
Discussion
Dermoid and epidermoid cysts have been reported to oc-cur in all body parts, but occurrence in the oral region is comparatively rare.5 These cysts are mostly considered to be congenital, generally produced by aberrant introduction of
ectodermal tissue into the union of the first and second bra-chial arches during the foetal period.6,7 In the oral region, the floor of the mouth is a common site of onset. Cysts occurring after birth are probably due to epithelial aberration because of trauma or surgical treatment. Therefore, unlike congenital cysts, dermoid or epidermoid cysts that are caused by trauma or surgical treatment often manifest away from the midline.8 It is thus essential that patients in whom cysts are found away from the midline be interviewed regarding any history of trauma or surgery. Reports of dermoid cysts accompanied by fistulae are extremely rare. An extensive literature review revealed reports of only 2 patients from other countries2,3 and 1 in Japan.4
In the present patient, while recurrent swelling of the lower part of the tongue had been experienced since a very young age, the condition was not examined closely or diagnosed definitively. A fistula was seen in the centre of the
Figure 1. Preoperative imaging. (a) Computed tomography during acute inflammation showed a cystic lesion in the center of the tongue (arrow). (b) T1-weighted magnetic resonance imaging during resolution of inflammation showed a luminal structure in the centre of the tongue (arrow).
Figure 2. Intraoperative photographs. (a) Pale yellow pus is seen leaking from the fistula on the dorsum of the tongue (arrow). (b) A probe inserted through the fistula reached the floor of the mouth.
a b
a b

Mori, Saijo, Fujihara, et al
Asian J Oral Maxillofac Surg. Vol 21, Nos 1 & 2, 2009 53
tongue for this patient. Taking into account the development of fistulae, as swelling was experienced repeatedly from an early age, it was assumed that the fistula had formed through the lingual septum, where the tissue is relatively weak, due to internal pressures associated with the swelling. Although dermoid and epidermoid cysts often develop congenitally, they are rarely discovered in early childhood unless they become enlarged. Such cysts are commonly detected during puberty, which may be related to the cyst’s slow growth, and the increased functions and enlargement of sweat and sebaceous glands during puberty.9 Cysts are sometimes discovered during this period due to exacerbation by inflam-mation. Caution is warranted for such patients, as respiratory difficulties may also occur.10
Meyer’s classifications are generally used for the defini-tive diagnosis of these cysts.9 Meyer classified cysts into 3 histological types — epidermoid, dermoid, and teratoid. The lesion was diagnosed as a dermoid cyst in this patient as histopathological analysis revealed a stratified squamous epithelial lining and sebaceous glands in the cyst wall.
MRI, CT with contrast, and ultrasound are effective diagnostic techniques.11 However, in patients with an ac-companying fistula, dermoid cysts may be small during non-inflammatory periods and therefore may not be observable
even if imaging is done at these times. The fistula was not clear at initial presentation for this patient, but could be identi-fied on the surface of the dorsum of the tongue when inflamed. Where cysts are accompanied by fistulae, inflammation tends to recur due to the existence of the fistula, and the cyst may not enlarge considerably or swelling may stop while still mild due to drainage through the fistula. As a result, it is difficult to arrive at a definitive diagnosis for such patients and detection is delayed. Therefore, special attention should be given during diagnostic imaging. Malignant transformation of sublingual dermoid cysts has also been reported,12 and this calls for careful monitoring during clinical management.
References1. Turetschek K, Hospodka H, Steiner E. Epidermoid cyst of the floor of
the mouth: diagnostic imaging by sonography, computed tomography
and magnetic resonance imaging. Br J Radiol. 1995;68:205-7.
2. Rise EN. Dermoid cysts of the tongue and floor of the mouth. Arch
Otolaryngol. 1964;80:12-5.
3. Korchin L, Juan S. Dermoid cyst with lingual sinus tract. Oral Surg.
1974;37:175-8.
4. Kanematsu N, Yoshida Y, Takahashi G, Takada K, Noguchi M, Maeda
K, et al. A case of dermoid cyst of the tongue. J Jpn Stomatol Soc.
1983;32:600-5. [Article in Japanese.]
5. New GB, Erich JB. Dermoid cysts of the head and neck. Surg Gynecol
Obstet. 1973;65:48-55.
6. Shafer WG, Hme MK, Levy BM, editors. A textbook of oral pathology.
4th ed. Philadelphia: Saunders; 1983:78-9.
7. Colp R. Dermoid cysts of the floor of the mouth. Surg Gynecol Obstset.
1925;40:183-95.
8. Masliah MK, Blain S, Sanders B. Dermoid cysts of the oral regions in
children. J Pedod. 1979;3:221-34.
9. Meyer I. Dermoid cysts of the floor of the mouth. Oral Surg. 1955;
8:1149.
10. Longo F, Maremonti P, Mangone GM, De Maria G, Califano L.
Midline (dermoid) cysts of the floor of the mouth: report of 16 cases
and review of surgical techniques. Plast Reconstr Surg. 2003;112:
1560-5.
11. Seah TE, Sufyan W, Singh B. Case report of a dermoid cyst at the floor
of the mouth. Ann Acad Med. 2004;33:77-9.
12. Devine JC, Jones DC. Craniomatous transformation of a sublingual
dermoid cyst. Int J Oral Maxillofac Surg. 2000;29:126-7.
Figure 3. Histopathological examination of the extirpated specimen showed sebaceous glands in the connective wall of the cyst, which was lined with stratified squamous epithelium (haematoxylin and eosin; original magnification, × 100).