Embed Size (px)
Citation preview

Dr. Huda Hammad
Dr. Wael Swelam
OBC 231 General Pathology
Diseases of the Immune System
12/22/2012

Hypersensitivity Diseases:
Mechanisms of Immune Mediated Injury
Individuals who mount immune responses against an antigen are said to be “sensitized” to that antigen.
When these responses are pathologic or excessive, the manifestations are called “hypersensitivity”.
Normally, a system of checks and balances optimizes the eradication of infecting organisms without serious injury to host tissues.
However, immune responses may be inadequately controlled or inappropriately targeted to host tissues.
In these situations, the normally beneficial response is the cause of disease.
12/22/20122

Hypersensitivity Diseases:
Mechanisms of Immune Mediated InjuryCauses of Hypersensitivity Diseases
Pathologic immune responses may be directed against different
types of antigens, and may result from various underlying
abnormalities:
1. Autoimmunity.
2. Reactions against microbes.
3. Reactions against environmental antigens.
12/22/20123

Hypersensitivity Diseases:
Mechanisms of Immune Mediated Injury
Causes of Hypersensitivity Diseases
1. Autoimmunity:
Normally, the immune system does not react against an individual's own antigens (self-tolerance).
Sometimes, self-tolerance fails, resulting in reactions against one's own cells and tissues that are called autoimmunity.
The diseases caused by autoimmunity are referred to as autoimmune diseases.
12/22/20124

Hypersensitivity Diseases:
Mechanisms of Immune Mediated InjuryCauses of Hypersensitivity Diseases
2. Reactions against microbes:
Many types of reactions against microbial antigens may cause
disease.
In some cases, the reaction may be excessive or the microbial
antigen is unusually persistent.
12/22/20125

Hypersensitivity Diseases:
Mechanisms of Immune Mediated InjuryCauses of Hypersensitivity Diseases
Reactions against microbes
Antibodies produced against
microbial immune complexes
Inflammatory Poststreptococcal
glomerulonephritis
T-cell responses against persistent microbes
sever inflammatory response
Granulomas, e.g.
Tuberculosis
Antibodies / T cells cross-react
with a host tissue
Rheumatic heart disease
During the process of eradicating the
infection host tissues injury
Cytotoxic T cells try to eliminate infected cells, and this
normal immune response damages liver cells e.g. Viral
hepatitis
12/22/20126

Hypersensitivity Diseases:
Mechanisms of Immune Mediated InjuryCauses of Hypersensitivity Diseases
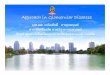
Poststreptococcal
glomerulonephritis
Tuberculos granuloma
Rheumatic heart disease
Viral hepatitis
12/22/20127

Hypersensitivity Diseases:
Mechanisms of Immune Mediated InjuryCauses of Hypersensitivity Diseases
3. Reactions against environmental antigens:
Most healthy individuals do not react strongly against common
environmental substances (e.g., pollen, animal dander, or dust
mites), but almost 20% of the population is "allergic" to these
substances.
12/22/20128

Hypersensitivity Diseases:
Mechanisms of Immune Mediated Injury
Causes of Hypersensitivity Diseases
These hypersensitivity diseases tend to be chronic, often
debilitating, and pose therapeutic challenges.
Since chronic inflammation is a major component of these
disorders, they are sometimes grouped under the term
immune-mediated inflammatory diseases.
12/22/20129

Hypersensitivity Diseases:
Mechanisms of Immune Mediated InjuryTypes of Hypersensitivity Diseases
Hypersensitivity reactions are traditionally subdivided into four types.
1. Immediate (type I) hypersensitivity.
2. Antibody-mediated (type II) hypersensitivity.
3. Immune complex-mediated (type III) hypersensitivity.
4. T-cell-mediated (type IV) hypersensitivity.
The first three are variations on antibody-mediated injury, whereas the fourth is
cell mediated.
This classification of immune-mediated disease is not perfect, because several
immune reactions may coexist in one disease.
12/22/201210

12/22/201211

Hypersensitivity Diseases:
Mechanisms of Immune Mediated Injury
Types of Hypersensitivity Diseases
Immediate (type I) hypersensitivity
Some of these mediators are released
within minutes from sensitized mast
cells causing the intense immediate reactions associated with conditions
such as systemic anaphylaxis.
Others, such as cytokines, are
responsible for the inflammation seen
in late-phase reactions.
12/22/201212

Sequence of events in immediate (type 1)
hypersensitivity
Action Mediator
Vasodilation, increased
vascular permeability
Histamine
PAF (platelet activating Factor)
Leukotrienes C4, D4, E4
Neutral proteases that activate
complement and kinins
Prostaglandin D2
Smooth muscle spasm Leukotrienes C4, D4, E4
Histamine
Prostaglandins
PAF
Cellular infiltration Cytokines (e.g., chemokines,
TNF)
Leukotriene B4
Eosinophil and neutrophil
chemotactic factors (not defined
biochemically)
12/22/2012
13

Hypersensitivity Diseases:
Mechanisms of Immune Mediated Injury
Types of Hypersensitivity Diseases
Immediate (type I) hypersensitivity
Often, the IgE-triggered reaction has two well-defined phases:
(1) the immediate response: vasodilation, vascular leakage, and
smooth muscle spasm, within 5 to 30 minutes after exposure to an
allergen and subsiding by 60 minutes.
(2) a second, late-phase reaction: in 2 to 8 hours later and may last
for several days, inflammation and tissue destruction, such as
mucosal epithelial cell damage. Dominated by neutrophils,
eosinophils, and lymphocytes, especially TH2 cells.
12/22/201214

Hypersensitivity Diseases:
Mechanisms of Immune Mediated Injury
Types of Hypersensitivity Diseases
Immediate (type I) hypersensitivity
Clinical and Pathologic
Manifestations :
Systemic anaphylaxis:
Within minutes of an exposure in a
sensitized host, itching, urticaria
(hives), and skin erythema appear,
followed in short order by profound
respiratory difficulty caused by
pulmonary bronchoconstriction and
accentuated by hypersecretion of
mucus.
Laryngeal edema may exacerbate
matters by causing upper airway
obstruction.
12/22/201215

Hypersensitivity Diseases:
Mechanisms of Immune Mediated Injury
Types of Hypersensitivity Diseases
Immediate (type I) hypersensitivity
Clinical and Pathologic Manifestations :
Systemic anaphylaxis:
The musculature of the entire gastrointestinal tract may be affected, with resultant vomiting, abdominal cramps, and diarrhea.
Without immediate intervention, there may be systemic vasodilation with fall in blood pressure (anaphylactic shock), and the patient may progress to circulatory collapse and death within minutes.
12/22/201216

Hypersensitivity Diseases:
Mechanisms of Immune Mediated Injury
Types of Hypersensitivity Diseases
Immediate (type I) hypersensitivity
Clinical and pathologic manifestations :
Local reactions generally occur when the antigen is confined to a particular site, such as :
1. Skin (contact urticaria),
2. Gastrointestinal tract (ingestion diarrhea), or
3. Lung (inhalation bronchoconstriction).
12/22/201217

12/22/201218

Hypersensitivity Diseases:
Mechanisms of Immune Mediated Injury
Types of Hypersensitivity Diseases
Antibody-mediated (type II) hypersensitivity
Caused by antibodies directed against target antigens on
the surface of cells or other tissue components.
The antigens may be normal molecules intrinsic to cell
membranes or extracellular matrix, or they may be
adsorbed exogenous antigens (e.g., a drug metabolite).
12/22/201219

Hypersensitivity Diseases:
Mechanisms of Immune Mediated Injury
Types of Hypersensitivity Diseases
Antibody-mediated (type II) hypersensitivity
Antibody-mediated abnormalities are the underlying cause of many human diseases; examples include:
1. Autoimmune hemolytic anemia.
2. Autoimmune thrombocytopenic purpura.
3. Pemphigus vulgaris.
4. Vasculitis caused by ANCA.
5. Goodpasture syndrome.
6. Acute rheumatic fever.
7. Myasthenia gravis
8. Graves disease (hyperthyroidism).
9. Insulin-resistant diabetes.
10. Pernicious anemia.12/22/201220

Mechanisms of Antibody-Mediated Diseases:
A.
Hypersensitivity Diseases:
Mechanisms of Immune Mediated Injury
Types of Hypersensitivity Diseases
Antibody-mediated (type II) hypersensitivity
12/22/201221

Hypersensitivity Diseases:
Mechanisms of Immune Mediated Injury
Types of Hypersensitivity Diseases
Antibody-mediated (type II) hypersensitivity
Mechanisms of Antibody-Mediated Diseases:
C. Antibodies can bind to cell surface receptors or essential molecules, and cause
functional derangements (either inhibition or unregulated activation) without cell
injury, e.g. myasthenia gravis, Grave’s disease (hyperthyroidism).
12/22/201222

Hypersensitivity Diseases:
Mechanisms of Immune Mediated Injury
Types of Hypersensitivity Diseases
Immune complex-mediated (type III)
Caused by antibodies binding to antigens to form complexes
that circulate and may deposit in vascular beds and stimulate
inflammation, typically secondary to complement activation.
Tissue injury in these diseases is the result of the inflammation.
The antigens in these complexes may be exogenous antigens,
such as microbial proteins, or endogenous antigens, such as
nucleoproteins.
It is only when these complexes are produced in large amounts,
persist, and are deposited in tissues that they are pathogenic.
12/22/201223

Hypersensitivity Diseases:
Mechanisms of Immune Mediated Injury
Types of Hypersensitivity Diseases
Imm
un
e co
mp
lex-
med
iate
d
(typ
e II
I)
Systemic
1) Formation of antigen-antibody complexes in the circulation.
2) Deposition of the immune complexes in various tissues, thus initiating
3) An inflammatory reaction in various sites throughout the body
Local
Excess amount of initial antibody immune complexes precipitated at
the site of injection and trigger the same inflammatory reaction as in
systemic immune complex disease
12/22/201224

Hypersensitivity Diseases:
Mechanisms of Immune Mediated Injury
Types of Hypersensitivity Diseases
Immune complex-mediated (type III)
Disease Antigen Involved Clinicopathologic
Manifestations
Systemic lupus
erythematosus
Nuclear antigens Nephritis, skin lesions,
arthritis, others
Poststreptococcal
glomerulonephritis
Streptococcal cell wall
antigen(s); may be "planted"
in glomerular basement
membrane
Nephritis
Polyarteritis nodosa Hepatitis B virus antigen Hepatitis B virus antigen
Reactive arthritis Bacterial antigens (Yersinia) Acute arthritis
Serum sickness Various proteins, such as
foreign serum protein (horse
anti-thymocyte globulin)
Arthritis, vasculitis, nephritis
Arthus reaction
(experimental)
Various foreign proteins Cutaneous vasculitis
12/22/201225

Hypersensitivity Diseases:
Mechanisms of Immune Mediated Injury
Types of Hypersensitivity Diseases
T-cell-mediated (type IV) hypersensitivity
Mechanisms of T-cell-mediated (type IV) hypersensitivity reactions:
12/22/201226

Hypersensitivity Diseases:
Mechanisms of Immune Mediated Injury
Types of Hypersensitivity Diseases
T-cell-mediated (type IV) hypersensitivity
Mechanisms of T-cell-mediated (type IV) hypersensitivity reactions:
B. Direct cell cytotoxicity, mediated by CD8+ T cells.
12/22/201227

Hypersensitivity Diseases:
Mechanisms of Immune Mediated Injury
Types of Hypersensitivity Diseases
T-cell-mediated (type IV) hypersensitivity
This group of diseases has received great interest because many
of the newly designed biologic therapies developed to target
abnormal T-cell reactions.
Several autoimmune disorders, as well as pathologic reactions to
environmental chemicals and persistent microbes, are now
known to be caused by T cells.
12/22/201228

Disease Specificity of Pathogenic T
cells
Clinicopathologic
Manifestations
Type 1 diabetes mellitus Antigens of pancreatic islet βcells
(insulin, glutamic acid
decarboxylase, others)
Antigens of pancreatic islet βcells
(insulin, glutamic acid
decarboxylase, others)
Multiple sclerosis Protein antigens in CNS myelin
(myelin basic protein, proteolipid
protein)
Demyelination in CNS with
perivascular inflammation;
paralysis, ocular lesions
Rheumatoid arthritis Unknown antigen in joint
synovium (type II collagen?); role
of antibodies?
Demyelination in CNS with
perivascular inflammation;
paralysis, ocular lesions
Peripheral neuropathy; Guillain-
Barré syndrome?
Protein antigens of peripheral
nerve myelin
Demyelination in CNS with
perivascular inflammation;
paralysis, ocular lesions
Inflammatory bowel disease
(Crohn's disease)
Unknown antigen; may be derived
from intestinal microbes
Chronic inflammation of ileum
and colon, often with granulomas;
fibrosis, stricture
Contact dermatitis Environmental chemicals, e.g.,
poison ivy (pentadecylcatechol)
Dermatitis, with itching; usually
short-lived, may be chronic with
persistent exposure
12/22/201229

12/22/201230

12/22/201231

Surgical difficulties
Graft rejection
Organ shortage
Rejection of transplants
Transplantation problems
12/22/201232

Transplant Immunology Outline: Graft compatibility
Rejection = Recipient recognizes graft as foreign, and destroys it
Autograft Within same person
Isograft Between identical twins
Allograft Between genetically different people
Xenograft Between different species
12/22/201233

Histocompatible: antigenically similar to the host
Histoincompatible: antigenically different from the host
MHC antigens are the MOST IMPORTANT
ABO antigens are also important
Minor histocompatiblity antigens are less important
Histocompatibility
12/22/201234

Gene collection on chromosome 6
Three regions: class I, class II,
class III
Class I gene products
• HLA-A, HLA-B, HLA-C
• expressed on nearly all cells
• present antigen to TC cells
Class II gene products
• DP, DQ, DR
• expressed on antigen-
presenting cells
• present antigen to TH cells
Compatibility: HLA complex
12/22/201235

12/22/201236

12/22/201237

Compatibility
MHC class I II III
Region A B C DP DQ DR C4, C2, BF
Gene
products
HLA-
A
HLA-
B
HLA-
CDP DQ DR
C' proteins
TNF-
TNF-
12/22/201238

Compatibility
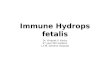
parents
four possible
haplotype
combinations of
children
a/b c/d
a/c a/d b/c b/d
♂ ♀
12/22/201239

Compatibility
1 7 w3 2 1 1
2 8 w2 3 2 2
11 35 w1 7 3 4
3 44 w4 4 1 3
A B C DR DQ DP
haplotypes
a
b
c
d
HLA alleles
12/22/201240

Compatibility
ice
cream
haplotypes
a
b
c
d
pop fruit veggiecookieyum
yum
Vault
De
w
12/22/201241

The more matching alleles between donor and host, the better!
Matching the class II antigens is more important than matching the
class I antigens.
One or two class I mismatches = no big deal
One or two class II mismatches = big deal
Mismatches in both class I and II = very big deal
Compatibility: HLA inheritance
12/22/201242

gra
ft s
urv
ival, %
50
100
63 12
time after transplant, months
0 0
1 or 2 0
3 or 4 0
0 1 or 2
1 or 2 1 or 2
3 or 4 1 or 2
number of mismatches
Class I Class II
12/22/201243

Transplant Immunology Outline
Introduction
Graft compatibility
Graft rejection
12/22/201244

Any two people (except identical twins) will express some
HLA proteins that are different.
Every recipient will recognize, and react against, at least
some foreign antigens in the graft
Rejection is complex, with lots of killing mechanisms.
Rejection
12/22/201245

Rejection
How do recipient cells know which cells to kill?
12/22/201246

T-cell-mediated rejection
Antibody-mediated rejection
Rejection
Two mechanisms of rejection
12/22/201247

CD8+ CTLs kill graft cells directly
CD4+ cells trigger a delayed hypersensitivity reaction
T-cell mediated rejection
12/22/201248

CTL Killing
Delayed Hypersensitivity
12/22/201249

Preformed antibodies
• Anti-HLA or anti-ABO
• Rejection occurs immediately
(“hyperacute”)
• Antibodies cause thrombosis
• Rare these days
Newly-made antibodies
• Appear within days to years
• Usually directed against graft
endothelium
• Cause damage by: Helping complement kill graft cells
Opsonizing graft cells (yummy!)
Antibody-mediated rejection
12/22/201250

Target cell is coated with IgG
Effector cell* has receptors for Fc fragment
Effector cell binds to target cell
Target cell is lysed
Antibody-dependant cell-mediated cytotoxicity (ADCC)
* Macrophage, Neutrophil, or NK Cell 12/22/201251

Clinical types of Rejection
Hyper-acute rejection
• Within hours
• Preexisting anti-donor antibodies
• Rare these days
• “Accelerated” is similar
Acute rejection
• Starts at about 10 days
• Cell-mediated
Chronic rejection
• Months to years after transplant
• Humoral and cell-mediated mechanisms
• Hard to prevent
• Hard to treat
12/22/201252

Acute cellular (t) Acute humoral
Chronic12/22/201253

12/22/201254

12/22/201255

Autoimmune Diseases
The immune reaction to self-antigens, or autoimmunity, is
the cause of certain human diseases.
A growing number of entities have been attributed to
this process (see table in next slide).
12/22/201256

Organ-Specific Systemic
Hashimoto thyroiditis Systemic lupus erythematosus
Autoimmune hemolytic anemia Rheumatoid arthritis
Autoimmune atrophic gastritis of pernicious
anemia
Sjögren syndrome
Multiple sclerosis Reiter syndrome
Autoimmune orchitis Inflammatory myopathies*
Goodpasture syndrome Systemic sclerosis (scleroderma)*
Autoimmune thrombocytopenia Polyarteritis nodosa*
Insulin-dependent diabetes mellitus
Myasthenia gravis
Graves' disease
Primary biliary cirrhosis*
Autoimmune (chronic active) hepatitis*
Ulcerative colitis *The evidence supporting an autoimmune basis
of these disorders is not strong. 12/22/201257

Autoimmune Diseases The evidence that the diseases listed in the previous table are the
result of autoimmune reactions is more persuasive for some than
for others.
For example, the presence of multiple autoantibodies accounts for
many of the clinical and pathologic manifestations of SLE.
Moreover, these autoantibodies can be identified within lesions by
immunofluorescence and electron-microscopic techniques.
12/22/201258

Autoimmune Diseases
In many other disorders, an autoimmune etiology is
suspected but is unproven.
In some cases of apparent autoimmunity, the response may be
directed against an exogenous antigen, such as a microbial
protein.
Autoimmune diseases range from those in which specific
immune responses are directed against one particular organ
or cell type, to multisystem diseases.
In the systemic diseases, the lesions affect principally the
connective tissue and blood vessels of the various organs
involved. These diseases are often referred to as "collagen
vascular" or "connective tissue" disorders.12/22/201259

Autoimmune Diseases: Self-Tolerance
Autoimmunity implies loss of self-tolerance.
Immunological tolerance is unresponsiveness to an antigen
that is induced by exposure of specific lymphocytes to that
antigen.
Self-tolerance refers to a lack of immune responsiveness to
one's own tissue antigens.
12/22/201260

Autoimmune Diseases
Self-Tolerance
During the generation of billions of antigen receptors in
developing T and B lymphocytes, receptors are produced that
can recognize self-antigens.
Several mechanisms work in concert to prevent immune
reactions against one's own antigens.
These mechanisms are broadly divided into two groups:
central tolerance and peripheral tolerance.
12/22/201261

Autoimmune Diseases
Self-Tolerance
Central tolerance
• Immature lymphocytes that recognize self-antigens in the central (generative) lymphoid organs are killed by apoptosis.
• In the B-cell lineage, some of the self-reactive lymphocytes switch to new antigen receptors that are not self-reactive
Peripheral tolerance
• Mature lymphocytes that recognize self-antigens in peripheral tissues undergo one of the following:• They become functionally
inactive (anergic),
• Or are suppressed by regulatory T lymphocytes,
• Or die by apoptosis.
12/22/201262

Autoimmune Diseases
Self-Tolerance
The variables that lead to a failure of self-tolerance and the
development of autoimmunity include:
1. Inheritance of susceptibility genes that may disrupt different
tolerance pathways.
2. Infections and tissue alterations that may expose self-
antigens and activate APCs and lymphocytes in the tissues,
altering the recognition of self-antigens.
12/22/201263

Pathogenesis of
autoimmunity
Autoimmunity arises from many
causes, including:
1) Inheritance of susceptibility genes
that may interfere with self-
tolerance,
2) Environmental triggers
(inflammation, other inflammatory
stimuli) that promote lymphocyte
entry into tissues,
3) Activation of self-reactive
lymphocytes, and tissue injury.
12/22/2012
64

Autoimmune Diseases
Systemic Lupus Erythematosus
The fundamental defect in SLE is a failure to maintain
self-tolerance.
A large number of autoantibodies is produced, classically
including antinuclear antibodies (ANAs),that can
damage tissues either directly or in the form of immune
complex deposits.
12/22/201265

12/22/2012
Lupus erythematosis pathogenesisGenetic factors
B cell
reactivity
autoantibody
productionB cells to enhance the
function of other cells
Organ damage
alter the function of T cells,
antigen-presenting cells &
cytokines production
66

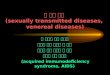
Autoimmune DiseasesSystemic Lupus Erythematosus1997 Revised Criteria for Classification of Systemic Lupus Erythematosus
Malar rash
Malar rash
Discoid rash
Photosensitivity
Oral ulceration
Arthritis12/22/201267

Autoimmune DiseasesSystemic Lupus Erythematosus1997 Revised Criteria for Classification of Systemic Lupus Erythematosus
Serositis
Renal disorders
Neurologic disorder
12/22/201268

Autoimmune DiseasesSystemic Lupus Erythematosus1997 Revised Criteria for Classification of Systemic Lupus Erythematosus
Hematologic disorder
• Hemolytic anemia: with reticulocytosis,
• Leukopenia: <4.0 ×109 cells per liter (4000 cells per mm3) total on two or more occasions
• Lymphopenia: <1.5 ×109 cells per liter (1500 cells per mm3) on two or more occasions
• Thrombocytopenia: <100 ×109
cells per liter (100 ×103 cells per mm3) in the absence of offending drugs
Immunologic disorder
• Anti-DNA antibody to native DNA in abnormal titer
• Anti-Sm: presence of antibody to Sm nuclear antigen
• Positive finding of antiphospholipid antibodies
12/22/201269

Autoimmune DiseasesSystemic Lupus Erythematosus1997 Revised Criteria for Classification of Systemic Lupus Erythematosus
11. Antinuclear antibody:
An abnormal titer of antinuclear antibody by
immunofluorescence or an equivalent assay at any point in
time and in the absence of drugs known to be associated with
drug-induced lupus syndrome.
12/22/201270

12/22/201271

Immune deficiencies
primary (inherited)
secondary (to infection, immunosuppression, etc.)
Patients more susceptible to infections and cancer
Type of infection varies:
Ig, C’ or phagocytic cell defect: bacterial infection
T cell defect: viral and fungal infections
Immune Deficiencies: Basic Concepts
12/22/201272

Rare!
Genetic
Can affect any part of immune system:
Adaptive (humoral or cellular)
Innate (C’, phagocytes, NK cells)
Typical patient: infant with recurrent infections
Primary importance for our class: boards
Primary Immune Deficiency Diseases: Basic
Concepts
12/22/201273

X-linked agammaglobulinemia
SCID
SCID
DiGeorge syndrome
SCID
Hyper-IgM syndrome
IgA deficiency
12/22/201274

Primary immune deficiencies
X-Linked Agammaglobulinemia
Common Variable Immunodeficiency (CVID)
Hyper-IgM Syndrome
Selective IgA Deficiency
Combined T-cell and B-cell (antibody)
deficiencies
12/22/201275

Pre-B cells can’t differentiate into B cells
Patients have no immunoglobulin
Affects males
Presents at 6 months of age (maternal Ig gone)
Recurrent bacterial infections
Treatment: intravenous pooled human Ig
X-linked Agammaglobulinemia
12/22/201276

Common variable immunodeficiency
Group of disorders characterized by
defective antibody production
Affects males and females equally
Presents in teens or twenties
Basis of Ig deficiency is variable (hence the
name) and often unknown
Patients more susceptible to infections, but
also to autoimmune disorders and
lymphoma!
12/22/201277

Severe Combined Immunodeficiency
12/22/201278

Examples of Infections in Immunodeficiencies
Pathogen Type T-Cell-Defect B-Cell DefectGranulocyte
Defect Complement Defect
Bacteria Bacterial sepsis Streptococci,
staphylococci,
Haemophilus
Staphylococci,
PseudomonasNeisserialinfections, other
pyogenic bacterial
infections
Viruses Cytomegalovirus, Epstein-Barr
virus, severe varicella, chronic
infections with respiratory and
intestinal viruses
Enteroviral
encephalitis
Fungi and
parasitesCandida, Pneumocystis carinii Severe intestinal
giardiasis
Candida, Nocardia, Aspergillus
Special features Aggressive disease with
opportunistic pathogens, failure
to clear infections
Recurrent
sinopulmonary
infections, sepsis,
chronic meningitis
12/22/201279

Disease Transmission Defect Clinical stuff
XLA X-linkedNo mature B cells;
no Ig
Infant with recurrent
bacterial infections
CVID
IgA deficiency
Hyper-IgM
DiGeorge
SCID
A good way to study immune deficiencies
12/22/2012 80

Etiology: HIV
Pathogenesis: Infection, Latency, Progressive T-Cell loss
Morphology: MANY
Clinical Expressions: Infections, Neoplasms, Progressive Immune Failure, Death, HIV+, HIV-RNA (Viral Load)
AIDS(SECONDARY IDS)
12/22/201281

Homosexual: (40%, and declining)
Intravenous drug usage (25%)
Heterosexual sex (10% and rising)
Epidemiology
12/22/201282

The enzyme reverse transcriptase (RT) is used by retroviruses to transcribe
their single-stranded RNA genome into single-stranded DNA and to
subsequently construct a complementary strand of DNA, providing a DNA
double helix capable of integration into host cell chromosomes.
Reverse transcriptase
12/22/201283

Attaching Budding
Pathogenesis
12/22/201284

Early budding
Pathogenesis
Late budding
Mature new
virions
12/22/201285

Lymphopenia
Decreased t-cell function
B-cell activation, polyclonal
Altered monocyte/macrophage function
General immune abnormalities
12/22/201286

Protozoal/Helminthic: Cryptosporidium,
PCP (Pneumocystis Carinii Pneumonia),
Toxoplasmosis
Fungal: Candida, and the usual 3
Bacterial: TB,
Nocardia,
Salmonella
Viral: CMV, HSV, VZ (Herpes Family)
AIDS related Infections
12/22/201287

PCP12/22/201288

CRYPTOSPORIDIUM 12/22/201289

Caseating granuloma 12/22/201290

Kaposi sarcoma
B-cell lymphomas
CNS lymphomas
Cervix cancer, squamous cell
Cancers related to AIDS
12/22/201291

12/22/201292