Embed Size (px)
Citation preview
© Endeavour College of Natural Health endeavour.edu.au 1
NMDC221 Session 26:
Endocrine System Disease Part I
© Endeavour College of Natural Health endeavour.edu.au 2
Recommended reading
o Mahan, L.K., & Raymond, J.L. (2016). Krause’s food &
the nutrition care process (14th ed.). Pp. 619-30.
St. Louis, MO: Elsevier. (prescribed text).
© Endeavour College of Natural Health endeavour.edu.au 3
Topic Summary
Endocrine System Disease: Part I
o Principles and considerations in nutritional medicine
management of the endocrine system - Thyroid
o Review anatomy & physiology of the endocrine system
Nutritional management of specific endocrine conditions
with consideration of drug-nutrient interactions
o Hypothyroidism
o Hyperthyroidism
© Endeavour College of Natural Health endeavour.edu.au 4
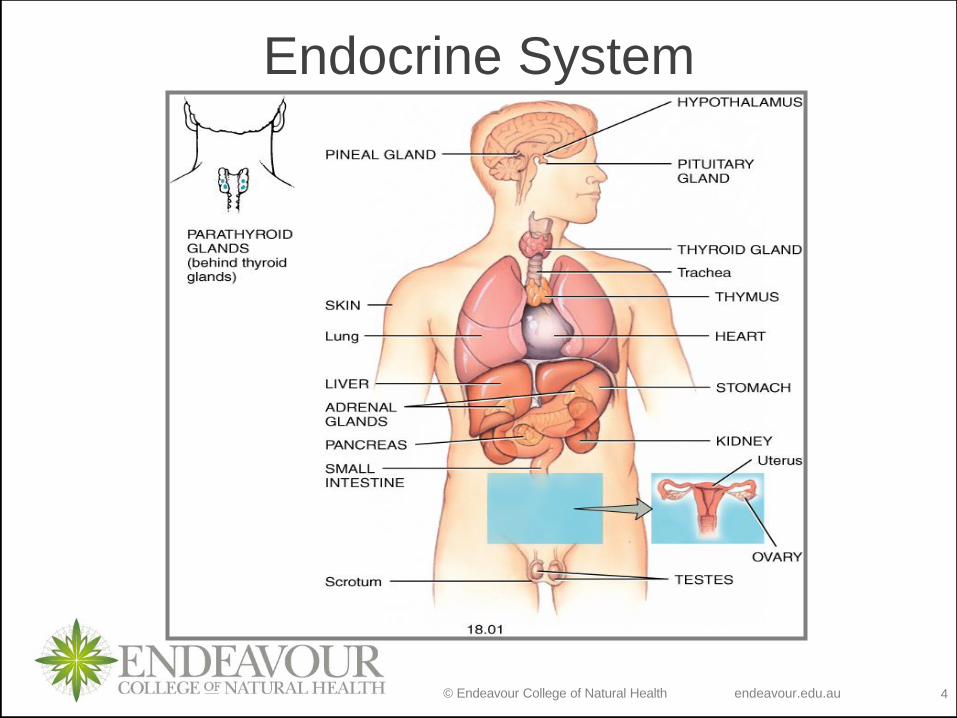
Endocrine System
© Endeavour College of Natural Health endeavour.edu.au 5
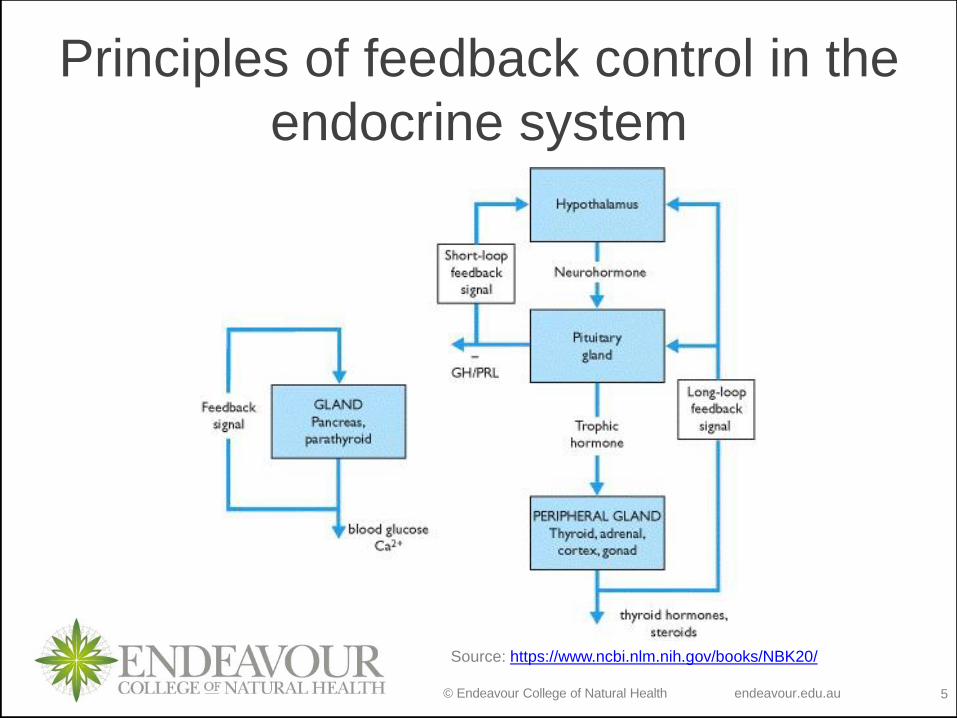
Principles of feedback control in the
endocrine system
Source: https://www.ncbi.nlm.nih.gov/books/NBK20/
© Endeavour College of Natural Health endeavour.edu.au 6
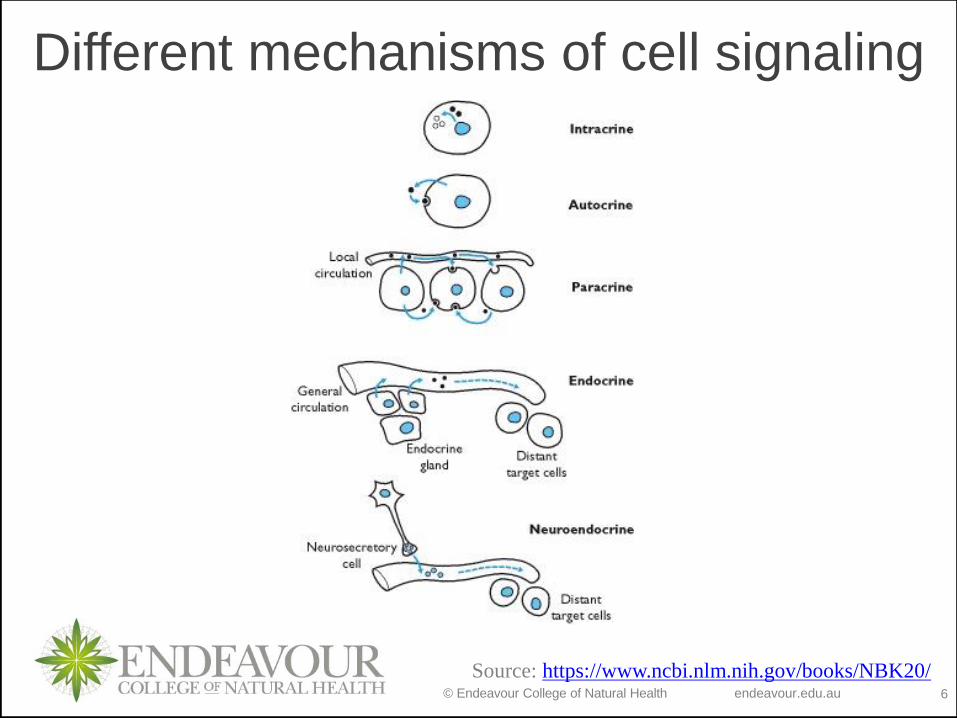
Source: https://www.ncbi.nlm.nih.gov/books/NBK20/
Different mechanisms of cell signaling
© Endeavour College of Natural Health endeavour.edu.au 7
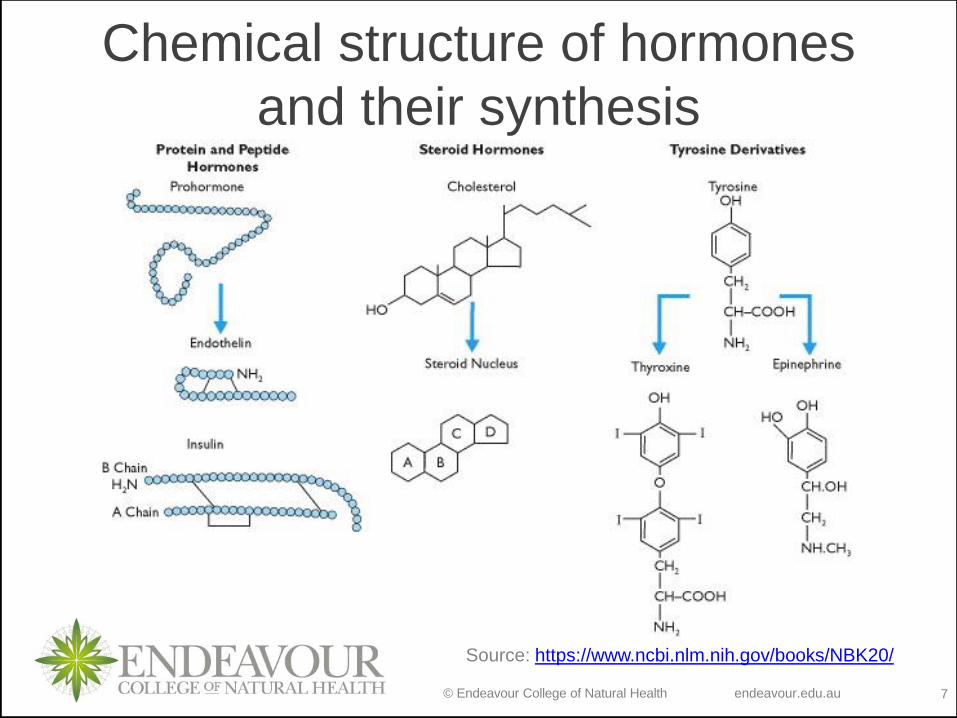
Chemical structure of hormones
and their synthesis
Source: https://www.ncbi.nlm.nih.gov/books/NBK20/
© Endeavour College of Natural Health endeavour.edu.au 8
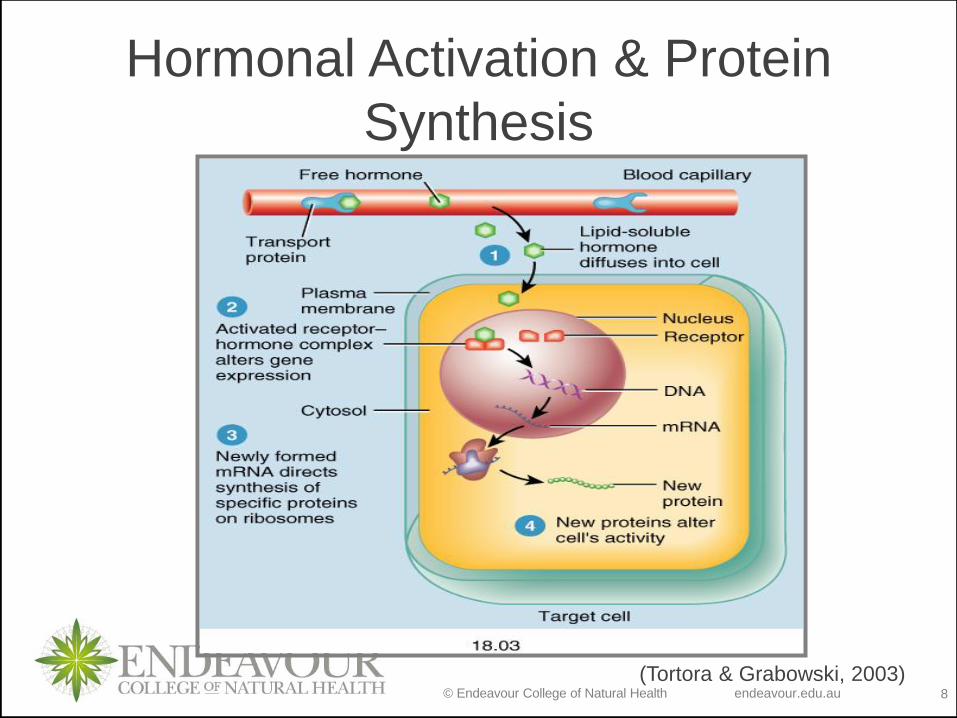
(Tortora & Grabowski, 2003)
Hormonal Activation & Protein
Synthesis
© Endeavour College of Natural Health endeavour.edu.au 9
THYROID GLAND
© Endeavour College of Natural Health endeavour.edu.au 10
Autoimmunity and molecular
mimicry
© Endeavour College of Natural Health endeavour.edu.au 11
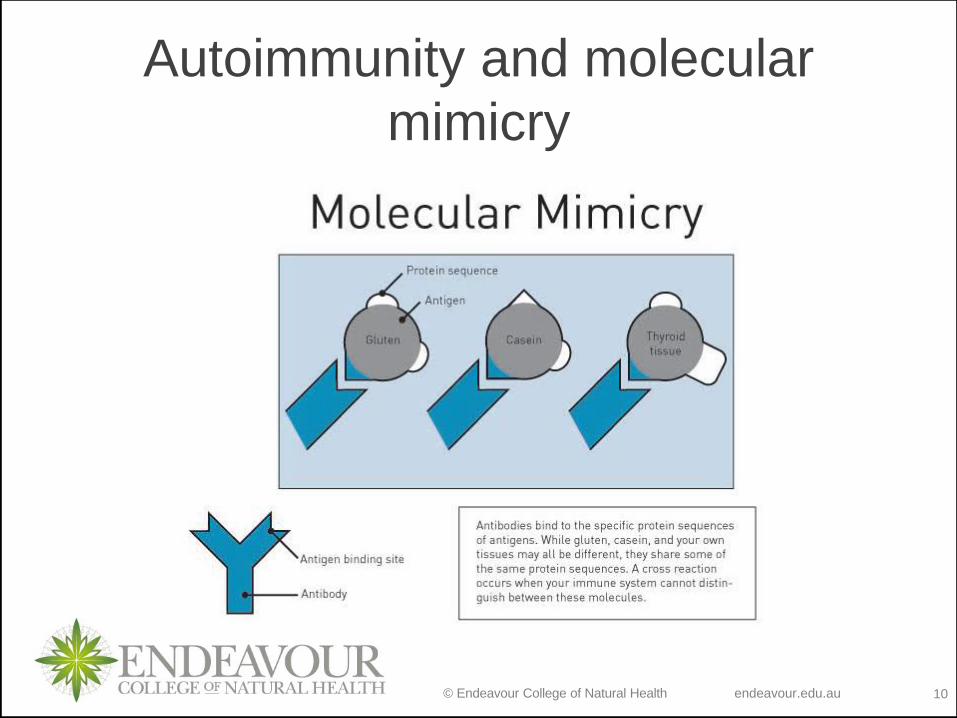
Mimicry
o Each time your body is exposed to a possible trigger,
your immune system memorizes its structure, specifically
its protein sequence, so that it can develop the perfect
defense to that pathogen and recognize it in the future.
o However, our immune system’s recognition system isn’t
perfect; as long as a molecule’s structure and protein
sequences are similar enough, the immune system can
be fooled into attacking look-a-like molecules that are
actually your body’s tissue, causing autoimmune
disease. Unfortunately for the thyroid, it has two common
risks - gluten and casein made worse by leaky gut.
© Endeavour College of Natural Health endeavour.edu.au 12
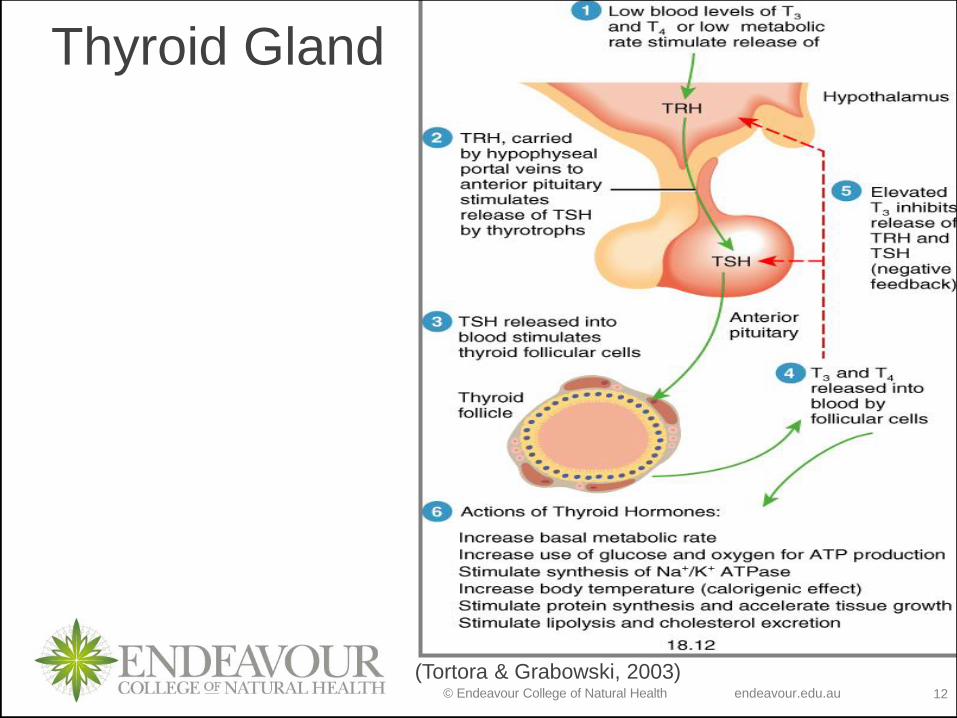
(Tortora & Grabowski, 2003)
Thyroid Gland
© Endeavour College of Natural Health endeavour.edu.au 13
Thyroid
Thyroid factor in control of:
o Basal metabolic rate (including respiratory rate,
heart rate and body temperature).
o Up-regulates β receptor sensitivity to
catecholamines (adrenalin & noradrenalin)
o Stimulate protein synthesis, triglyceride
breakdown and glucose metabolism for cellular
metabolism
o Enhance cholesterol excretion in bile
o Growth & development
(Tortora & Grabowski, 2003)
© Endeavour College of Natural Health endeavour.edu.au 14
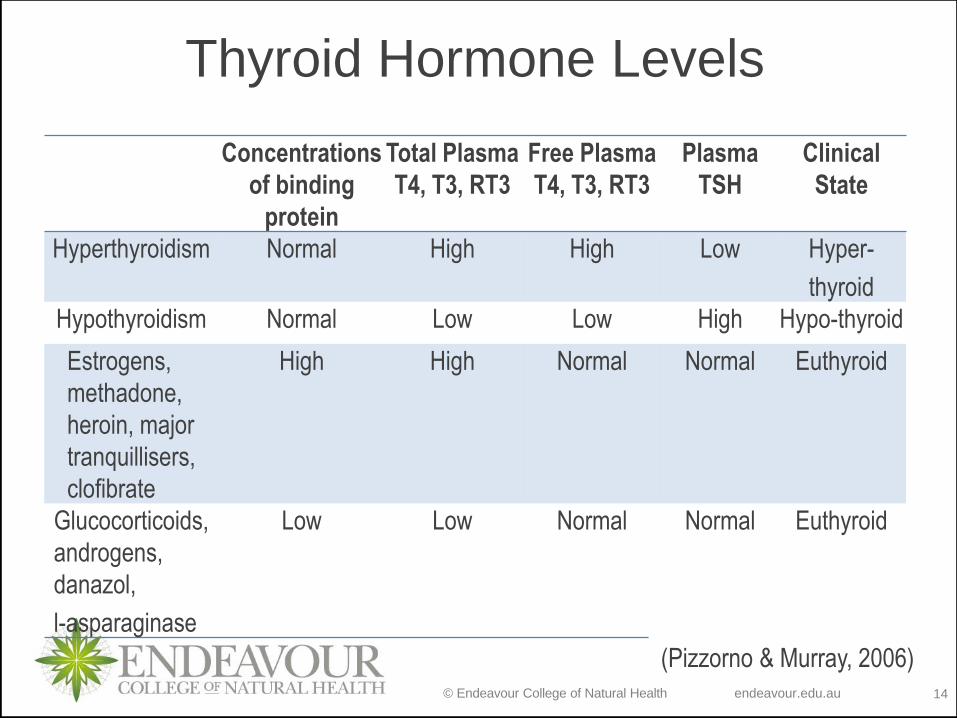
Thyroid Hormone Levels
Concentrations
of binding
protein
Total Plasma
T4, T3, RT3
Free Plasma
T4, T3, RT3
Plasma
TSH
Clinical
State
Hyperthyroidism Normal High High Low Hyper-
thyroid
Hypothyroidism Normal Low Low High Hypo-thyroid
Estrogens,
methadone,
heroin, major
tranquillisers,
clofibrate
High High Normal Normal Euthyroid
Glucocorticoids,
androgens,
danazol,
l-asparaginase
Low Low Normal Normal Euthyroid
(Pizzorno & Murray, 2006)
© Endeavour College of Natural Health endeavour.edu.au 15
Hyperthyroidism
© Endeavour College of Natural Health endeavour.edu.au 16
Hyperthyroidism
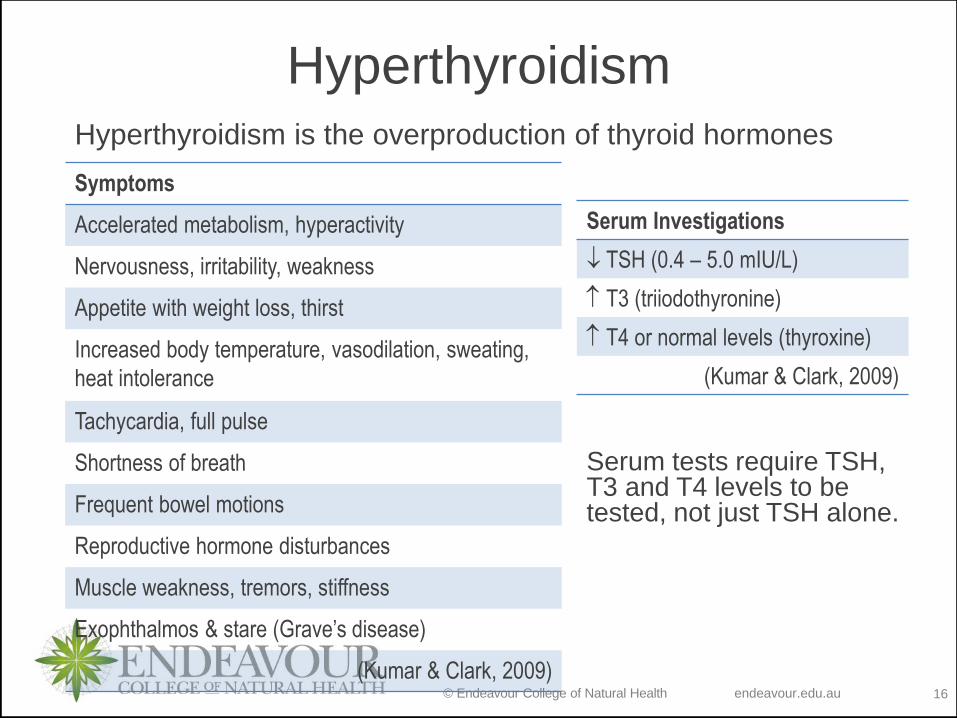
Serum tests require TSH, T3 and T4 levels to be tested, not just TSH alone.
Symptoms
Accelerated metabolism, hyperactivity
Nervousness, irritability, weakness
Appetite with weight loss, thirst
Increased body temperature, vasodilation, sweating,
heat intolerance
Tachycardia, full pulse
Shortness of breath
Frequent bowel motions
Reproductive hormone disturbances
Muscle weakness, tremors, stiffness
Exophthalmos & stare (Grave’s disease)
(Kumar & Clark, 2009)
Serum Investigations
TSH (0.4 – 5.0 mIU/L)
T3 (triiodothyronine)
T4 or normal levels (thyroxine)
(Kumar & Clark, 2009)
Hyperthyroidism is the overproduction of thyroid hormones
© Endeavour College of Natural Health endeavour.edu.au 17
Hyperthyroidism
Graves’ Disease
o Auto-immune (most common hyperthyroid condition)
where antibodies mimic TSH activity. As this is not
regulated by normal negative feedback mechanisms, the
thyroid gland is constantly stimulated to grow & produce
hormones. Uncontrolled production of TSH leads to the
characteristic presentation of goitre.
o Exophthalmos (protruding eyes – oedema behind eyes)
is the characteristic of Grave’s disease.
o Other common symptoms of hyperthyroidism present
o Pathology presents with TSH receptor autoantibodies
(Habra & Sarlis, 2005; Kumar & Clark, 2009)
© Endeavour College of Natural Health endeavour.edu.au 18
Hyperthyroidism
Sub Acute Thyroiditis
o Symptoms usually follow URTI of viral origin
o Symptoms include asthenia, malaise, pain over thyroid
or referred to lower jaw, ear, or occiput.
o Less common, acute onset with severe pain over thyroid,
fever, sometime thyrotoxicosis.
o Symptoms may continue (smoulder) for weeks/months &
eventually subside with return to normal thyroid function.
(Kumar & Clark, 2009)
© Endeavour College of Natural Health endeavour.edu.au 19
Hyperthyroidism
Female Reproductive Hormones
o Sudden changes to female reproductive hormones
(menarche, pregnancy, oral contraceptive use) can
cause a transient rise in thyroxine-binding globulin
(TBG) and TSH.
o This in turn increases total T4 and T3 levels.
o This can result in thyroid enlargement and hyperthyroid
symptoms.
(Dal Maso et al. 2009)
© Endeavour College of Natural Health endeavour.edu.au 20
Hyperthyroidism
Nutritional Considerations
Iodine
o Kelp and iodine containing supplements and drugs
(iodinated contrast agents, amiodarone) are substrates
for thyroxine synthesis. This is usually evident in
individuals that present with sub-acute hyperthyroidism
or an underlying goitre
(Habra & Sarlis, 2005; Kumar & Clark, 2009)
Tyrosine
o Avoid Tyrosine in excessive concentration – a substrate
for Thyroxine (T4) production
(Pizzorno & Murray, 2006)
© Endeavour College of Natural Health endeavour.edu.au 21
Hyperthyroidism
Treatment Aims
o Reduce high cortisol;
• exogenous – food intolerances, stimulants
• endogenous – immune dysregulation, imbalances in
neurotransmitters, inflammatory markers)
o Support of overactive metabolic pathways, organs and
systems through nutrient-dense foods, antioxidants,
energy-production cofactors and other specific nutrients
as indicated e.g. calcium
o Support co-morbid organ dysfunction that may present
o Minimize hyper-stimulation to thyroid
(Sarris & Wardle, 2010)
© Endeavour College of Natural Health endeavour.edu.au 22
Hyperthyroidism
Treatment Aims
o Support the breakdown of T4 via phase II detoxification
(glucuronidation)
o Assess protein status [IW x 0.9 x EF (1.1-1.5)]
o Assess fat status:
• High consumption of (W3) EFA rich food, moderate
MUFA and PUFA and decreased SFA’s.
o Assess carbohydrate status
o Assess required kilojoule intake given BMR and REE
(Pizzorno & Murray, 2006; Gropper et al. 2009)
© Endeavour College of Natural Health endeavour.edu.au 23
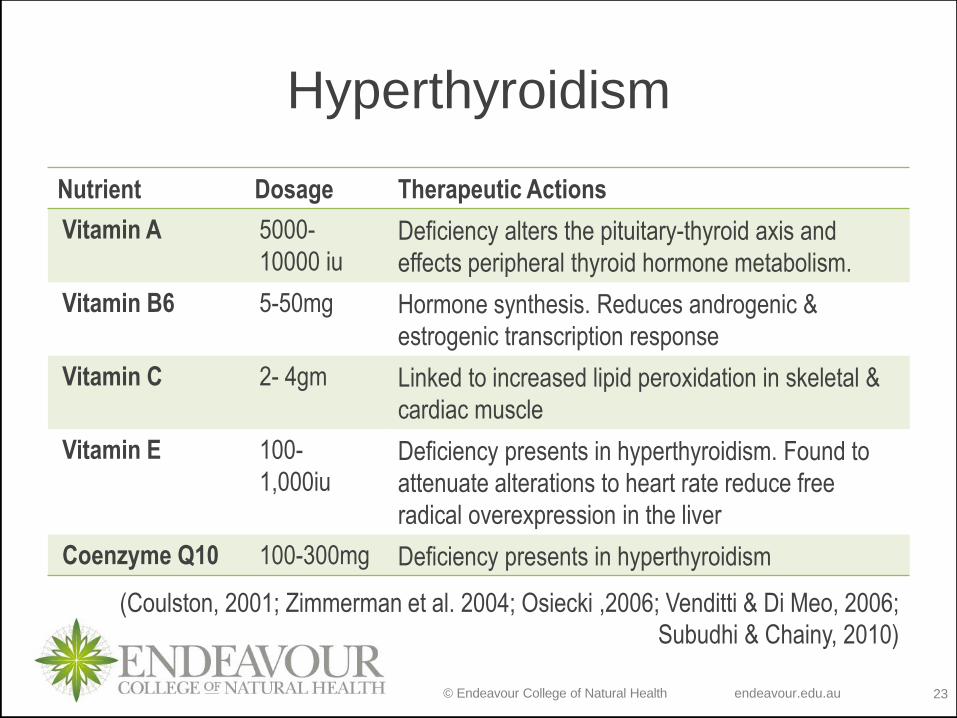
Hyperthyroidism
Nutrient Dosage Therapeutic Actions
Vitamin A 5000-
10000 iuDeficiency alters the pituitary-thyroid axis and
effects peripheral thyroid hormone metabolism.
Vitamin B6 5-50mg Hormone synthesis. Reduces androgenic &
estrogenic transcription response
Vitamin C 2- 4gm Linked to increased lipid peroxidation in skeletal &
cardiac muscle
Vitamin E 100-
1,000iuDeficiency presents in hyperthyroidism. Found to
attenuate alterations to heart rate reduce free
radical overexpression in the liver
Coenzyme Q10 100-300mg Deficiency presents in hyperthyroidism
(Coulston, 2001; Zimmerman et al. 2004; Osiecki ,2006; Venditti & Di Meo, 2006;
Subudhi & Chainy, 2010)
© Endeavour College of Natural Health endeavour.edu.au 24
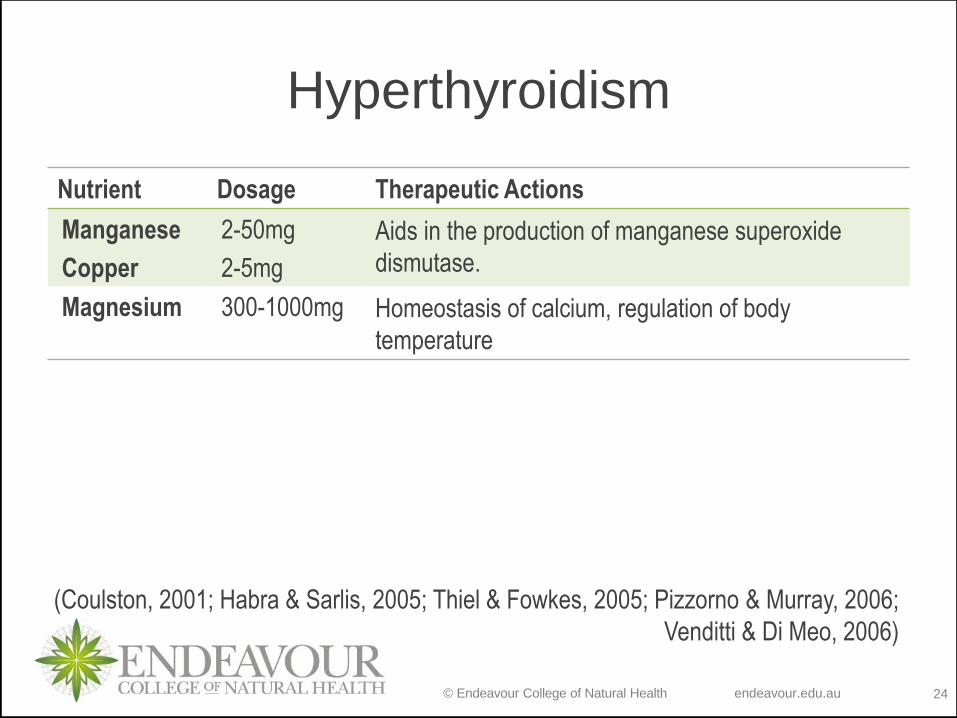
Hyperthyroidism
Nutrient Dosage Therapeutic Actions
Manganese
Copper
2-50mg
2-5mg
Aids in the production of manganese superoxide
dismutase.
Magnesium 300-1000mg Homeostasis of calcium, regulation of body
temperature
(Coulston, 2001; Habra & Sarlis, 2005; Thiel & Fowkes, 2005; Pizzorno & Murray, 2006;
Venditti & Di Meo, 2006)
© Endeavour College of Natural Health endeavour.edu.au 25
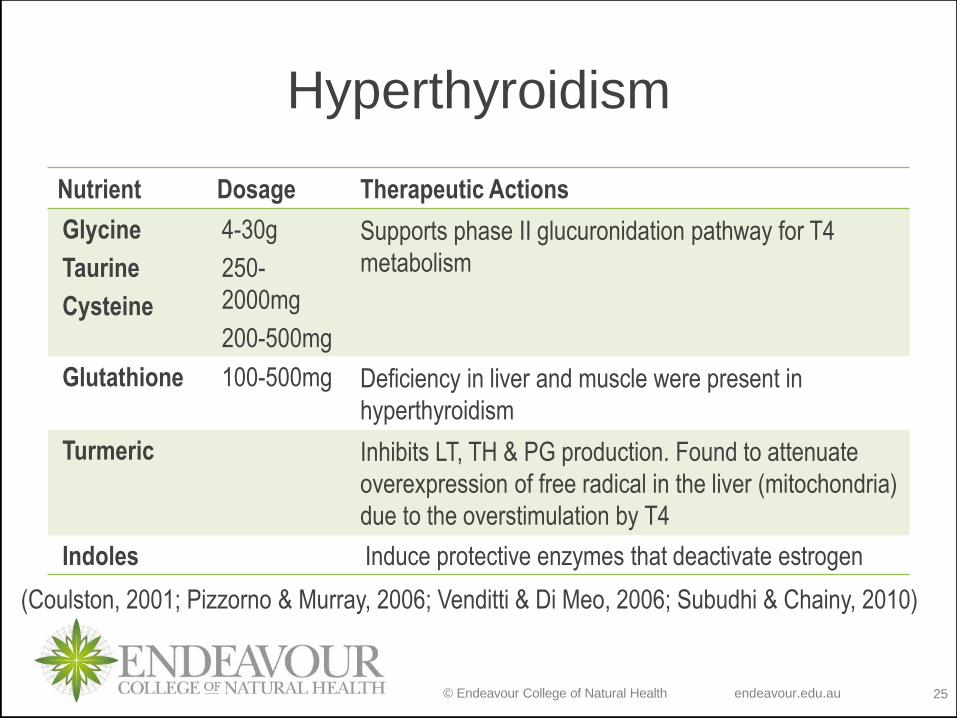
Hyperthyroidism
Nutrient Dosage Therapeutic Actions
Glycine
Taurine
Cysteine
4-30g
250-
2000mg
200-500mg
Supports phase II glucuronidation pathway for T4
metabolism
Glutathione 100-500mg Deficiency in liver and muscle were present in
hyperthyroidism
Turmeric Inhibits LT, TH & PG production. Found to attenuate
overexpression of free radical in the liver (mitochondria)
due to the overstimulation by T4
Indoles Induce protective enzymes that deactivate estrogen
(Coulston, 2001; Pizzorno & Murray, 2006; Venditti & Di Meo, 2006; Subudhi & Chainy, 2010)
© Endeavour College of Natural Health endeavour.edu.au 26
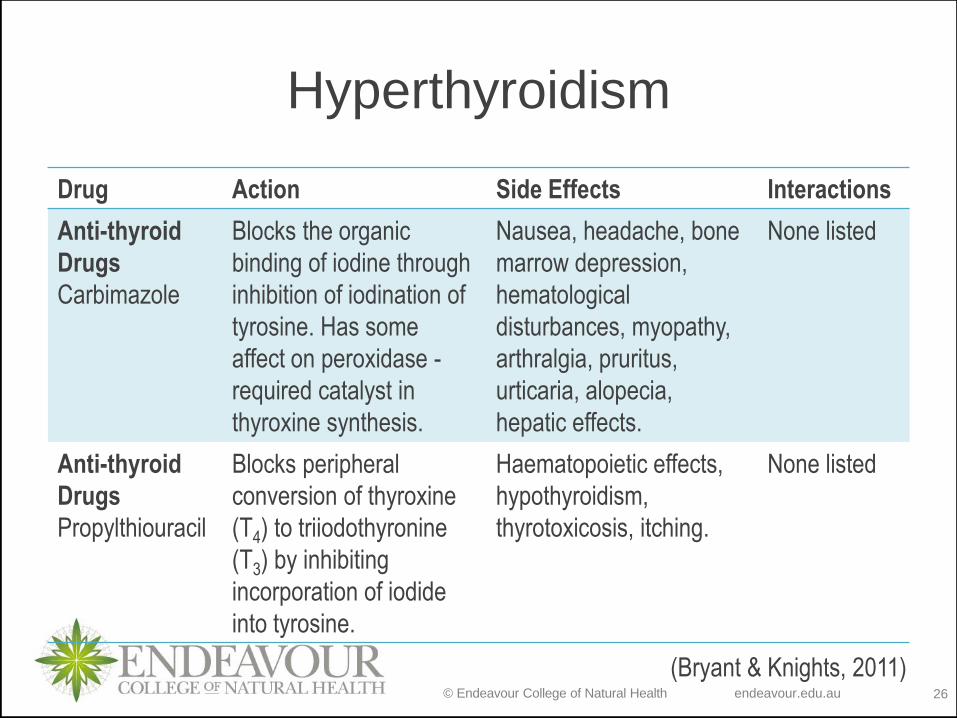
Hyperthyroidism
Drug Action Side Effects Interactions
Anti-thyroid
Drugs
Carbimazole
Blocks the organic
binding of iodine through
inhibition of iodination of
tyrosine. Has some
affect on peroxidase -
required catalyst in
thyroxine synthesis.
Nausea, headache, bone
marrow depression,
hematological
disturbances, myopathy,
arthralgia, pruritus,
urticaria, alopecia,
hepatic effects.
None listed
Anti-thyroid
Drugs
Propylthiouracil
Blocks peripheral
conversion of thyroxine
(T4) to triiodothyronine
(T3) by inhibiting
incorporation of iodide
into tyrosine.
Haematopoietic effects,
hypothyroidism,
thyrotoxicosis, itching.
None listed
(Bryant & Knights, 2011)
© Endeavour College of Natural Health endeavour.edu.au 27
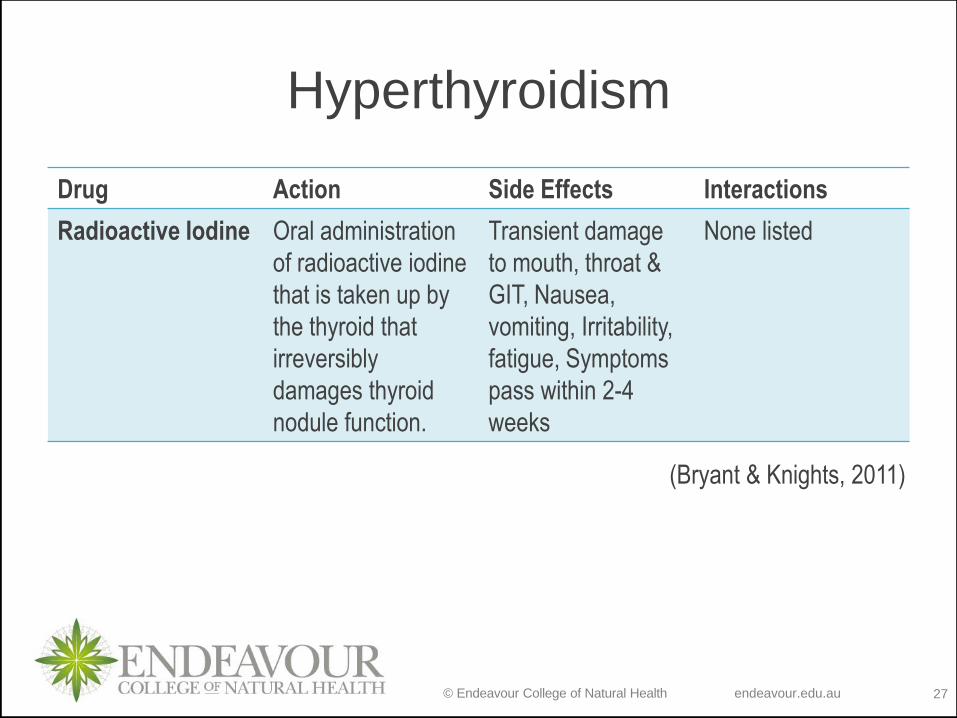
Hyperthyroidism
Drug Action Side Effects Interactions
Radioactive Iodine Oral administration
of radioactive iodine
that is taken up by
the thyroid that
irreversibly
damages thyroid
nodule function.
Transient damage
to mouth, throat &
GIT, Nausea,
vomiting, Irritability,
fatigue, Symptoms
pass within 2-4
weeks
None listed
(Bryant & Knights, 2011)
© Endeavour College of Natural Health endeavour.edu.au 28
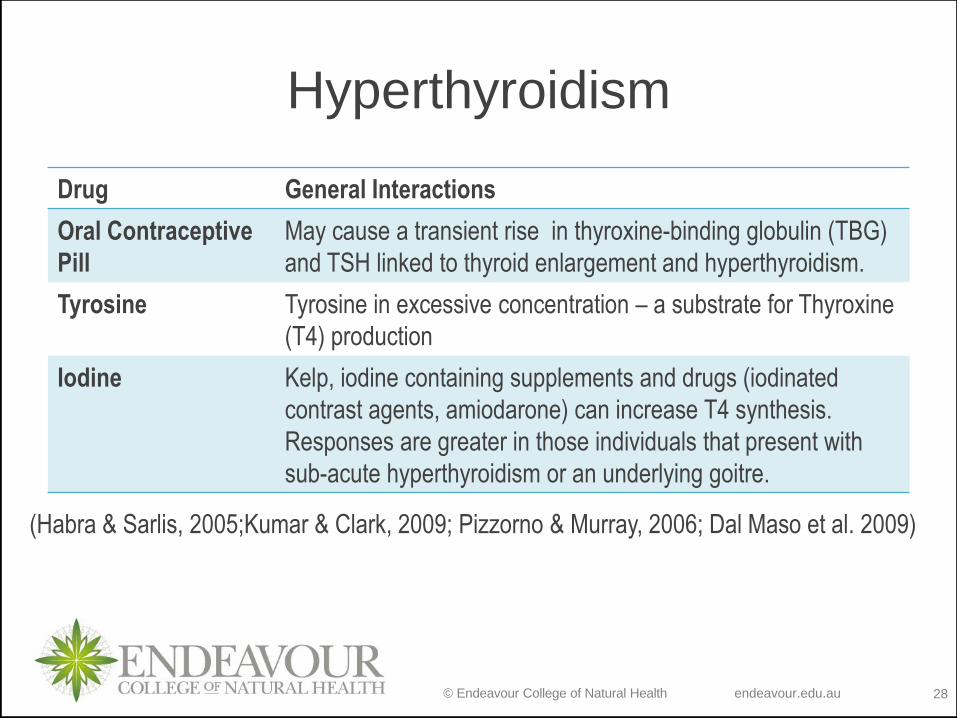
Hyperthyroidism
Drug General Interactions
Oral Contraceptive
Pill
May cause a transient rise in thyroxine-binding globulin (TBG)
and TSH linked to thyroid enlargement and hyperthyroidism.
Tyrosine Tyrosine in excessive concentration – a substrate for Thyroxine
(T4) production
Iodine Kelp, iodine containing supplements and drugs (iodinated
contrast agents, amiodarone) can increase T4 synthesis.
Responses are greater in those individuals that present with
sub-acute hyperthyroidism or an underlying goitre.
(Habra & Sarlis, 2005;Kumar & Clark, 2009; Pizzorno & Murray, 2006; Dal Maso et al. 2009)
© Endeavour College of Natural Health endeavour.edu.au 29
Hypothyroidism
© Endeavour College of Natural Health endeavour.edu.au 30
Hypothyroidism
Under Active Thyroid Function
Precursors to hypothyroidism:
o Surgical intervention of the thyroid gland
(hyperthyroid)
o Radioactive iodine or radiation (hyperthyroid)
o Iodine deficiency
o Environmental toxicity
o Auto-immune disorders
(Habra & Sarlis, 2005; Pizzorno & Murray, 2006)
© Endeavour College of Natural Health endeavour.edu.au 31
Hypothyroidism
Primary causes;
o Iodine deficiency
o Autoimmune disease: Hashimoto’s thyroiditis
o Iatrogenic (radiation, surgery and drugs)
Main secondary cause;
o Hypopituitarism
(Hywood, 2004)
© Endeavour College of Natural Health endeavour.edu.au 32
Hypothyroidism
Symptoms
Reduced metabolism – fatigue, cold intolerance,
weight gain/ inability to lose weight
Depression, psychosis/ dementia, poor memory,
Constipation
Reproductive hormone dysfunction, poor libido
Goitre (Hashimoto’s thyroiditis, Iodine
deficiency)
Hypotension, bradycardia, anaemia
Dry brittle hair, dry, coarse skin, loss of
eyebrows
Myalgia, muscle weakness, arthralgia
(Kumar & Clark, 2009)
Serum Pathology
TSH (0.4 – 5.0 mIU/L)
T3 (triiodothyronine)
T4 (thyroxine)
(Kumar & Clark, 2009)
TSH, T3 and T4 should be measured, not just TSH or TSH and T4 as T3 can be elevated with normal T4.
(
© Endeavour College of Natural Health endeavour.edu.au 33
Hypothyroidism
Hashimoto’s Disease
o An autoimmune antibody presentation to thyroid
peroxidase enzyme (responsible for liberating iodine for
combination with tyrosine).
o Characteristic goitre presentation is due low levels of T4
& T3 not negatively feeding back to the pituitary to
attenuate TSH production. This high level of TSH causes
swelling of the thyroid tissue.
o Usual characteristics of hypothyroidism present.
(Kumar & Clark, 2009)
© Endeavour College of Natural Health endeavour.edu.au 34
Hypothyroidism
Iodine Bioavailability Factors
Goitrogens
o Block the binding of iodine to thyroglobulin. Food
sources include raw brassica vegetables, tobacco, millet,
soy and catechins from tea.
(Gruner T, in: Sarris and Wardle 2015)
© Endeavour College of Natural Health endeavour.edu.au 35
Hypothyroidism
Iodine Bioavailability Factors
Lithium
o “Lithium therapy can cause hypothyroidism in 5–15% of
patients and goitre in as many as 37%.”
Iodine-containing drugs - iodinated contrast agents,
amiodarone, and iodine-containing supplements
o High levels of iodine containing drugs can cause
transient suppression of thyroid hormones.
(Habra & Sarlis, 2005)
© Endeavour College of Natural Health endeavour.edu.au 36
Hypothyroidism
Iodine Bioavailability Factors
Tricyclic Antidepressants
Can alter:
o iodine uptake by thyroid cells
o form non-bioavailable complexes with inorganic iodine
making it unavailable for TH synthesis
o inhibit the activity of thyroid peroxidase and enhance the
conversion of T4 to T3—or to rT3—by stimulation of
deiodinases
(Habra & Sarlis, 2005)
© Endeavour College of Natural Health endeavour.edu.au 37
Hypothyroidism
Other Factors
Increased Oxidative Stress
o Poor liver and peripheral metabolism of ethanol can
result in enhanced free radical generation.
o This has been found to cause “…HPT axis dysfunction
and peripheral thyroid hormone reduction.”
(Valeix et al. 2008)
Saturated Fats
o Saturated fats decrease T3 levels and promote body fat
accumulation.
(Pizzorno & Murray 2006)
© Endeavour College of Natural Health endeavour.edu.au 38
Hypothyroidism
Other Factors
Elevated IL-6
o Elevated serum IL-6 concentrations were also correlated
with…alterations in TH levels…”(Habra & Sarlis, 2005).
o IL-6 has been found to “…inhibit 5’-deiodinase.” (Sarris &
Wardle, 2010, p. 329)
Smoking
o Smoking can decrease thyroid hormone secretion and its
peripheral circulation.
(Pizzorno & Murray, 2006)
© Endeavour College of Natural Health endeavour.edu.au 39
Hypothyroidism
Other Factors
Hypercortisolism
Excess cortisol has been found to partially suppress TSH secretion.
Elevated cortisol leads to:
o Reduction in active T3 and increases in reverse T3
o Reduced peripheral hormone metabolism by inhibition of the enzyme 5’-deiodinase
o Potential to present with autoimmune disease, such as Hashimoto’s disease
(Hywood, 2004; Habra & Sarlis, 2005)
© Endeavour College of Natural Health endeavour.edu.au 40
Hypothyroidism
Other Factors
Manganese
o TSH binding to thyroid plasma membranes is strongly
inhibited by manganese.
o Through negative feedback, the increased circulation of
TSH would inhibit further TSH from the pituitary resulting
is a subsequent reduction in T4 production.
o Manganese has been linked to changes in regulating the
deiodinase enzymes through unknown mechanism
(Soldin & Aschner, 2007)
© Endeavour College of Natural Health endeavour.edu.au 41
Hypothyroidism
Alcohol
o Valeix et al. (2008) found that moderate alcohol
consumption levels of 3 standard drinks for males and
1.5 standard drinks for females statistically increased the
risk for thyroid volume enlargement.
o This was present in individuals that were not iodine
deficient.
Mercury
o Environmental mercury vapour exposure is linked to
reduced T3 and increased reverse T3. This is
exacerbated with iodine deficiency.
(Sarris & Wardle, 2010)
© Endeavour College of Natural Health endeavour.edu.au 42
Hypothyroidism
Treatment Aims
o Ensure precursors (tyrosine, iodine) and cofactors
(selenium, zinc) for thyroid hormone production are
replete.
o Review of food intolerances/gut dysfunction – gluten,
candida
o Treat autoimmune components
o Support optimal energy production
o Support co-morbid organ dysfunction that may present
o Assess protein status [IW x 0.9 x EF (1.1-1.5)]
o Assess fat status:
• High consumption of (W3) EFA rich food, moderate
MUFA and PUFA and decreased SFA’s.
(Groper et al. 2009; Sarris & Wardle, 2010)
© Endeavour College of Natural Health endeavour.edu.au 43
Hypothyroidism
Treatment Aims
o Reduce high cortisol;
• exogenous – food intolerances, stimulants
• endogenous – immune dysregulation, imbalances in
neurotransmitters, inflammatory markers
o Increase thyroid hormone precursors and cofactors in
production and conversion
o Assess and support dysfunction caused by drug usage
o Support of antioxidant defense system
(Sarris & Wardle, 2010)
© Endeavour College of Natural Health endeavour.edu.au 44
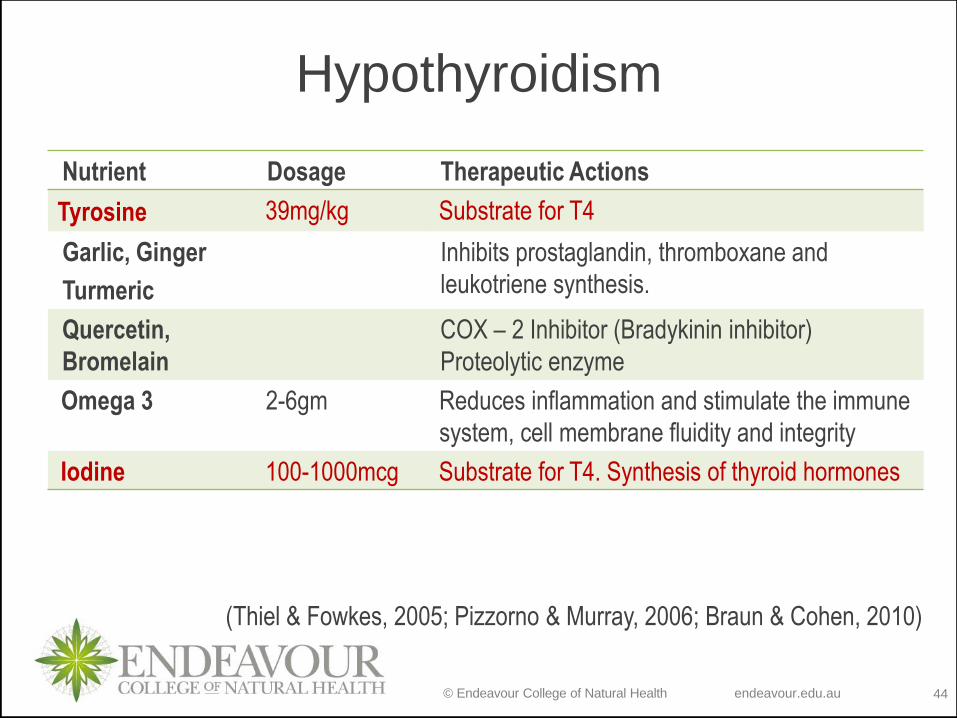
Hypothyroidism
Nutrient Dosage Therapeutic Actions
Tyrosine 39mg/kg Substrate for T4
Garlic, Ginger
Turmeric
Inhibits prostaglandin, thromboxane and
leukotriene synthesis.
Quercetin,
Bromelain
COX – 2 Inhibitor (Bradykinin inhibitor)
Proteolytic enzyme
Omega 3 2-6gm Reduces inflammation and stimulate the immune
system, cell membrane fluidity and integrity
Iodine 100-1000mcg Substrate for T4. Synthesis of thyroid hormones
(Thiel & Fowkes, 2005; Pizzorno & Murray, 2006; Braun & Cohen, 2010)
© Endeavour College of Natural Health endeavour.edu.au 45
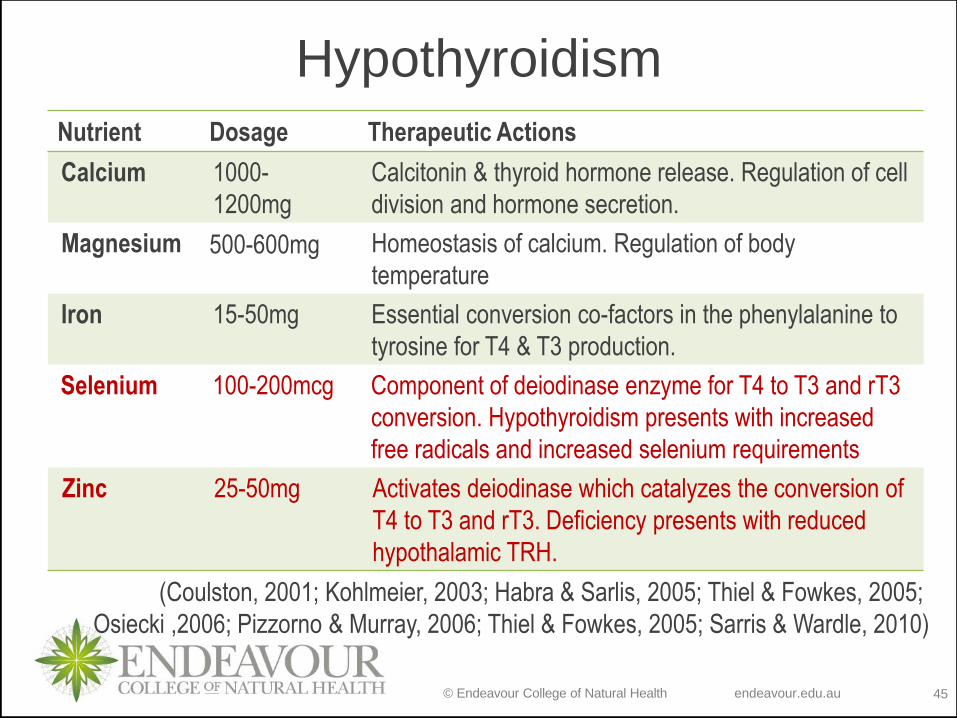
Hypothyroidism
Nutrient Dosage Therapeutic Actions
Calcium 1000-
1200mg
Calcitonin & thyroid hormone release. Regulation of cell
division and hormone secretion.
Magnesium 500-600mg Homeostasis of calcium. Regulation of body
temperature
Iron 15-50mg Essential conversion co-factors in the phenylalanine to
tyrosine for T4 & T3 production.
Selenium 100-200mcg Component of deiodinase enzyme for T4 to T3 and rT3
conversion. Hypothyroidism presents with increased
free radicals and increased selenium requirements
Zinc 25-50mg Activates deiodinase which catalyzes the conversion of
T4 to T3 and rT3. Deficiency presents with reduced
hypothalamic TRH.
(Coulston, 2001; Kohlmeier, 2003; Habra & Sarlis, 2005; Thiel & Fowkes, 2005;
Osiecki ,2006; Pizzorno & Murray, 2006; Thiel & Fowkes, 2005; Sarris & Wardle, 2010)
© Endeavour College of Natural Health endeavour.edu.au 46
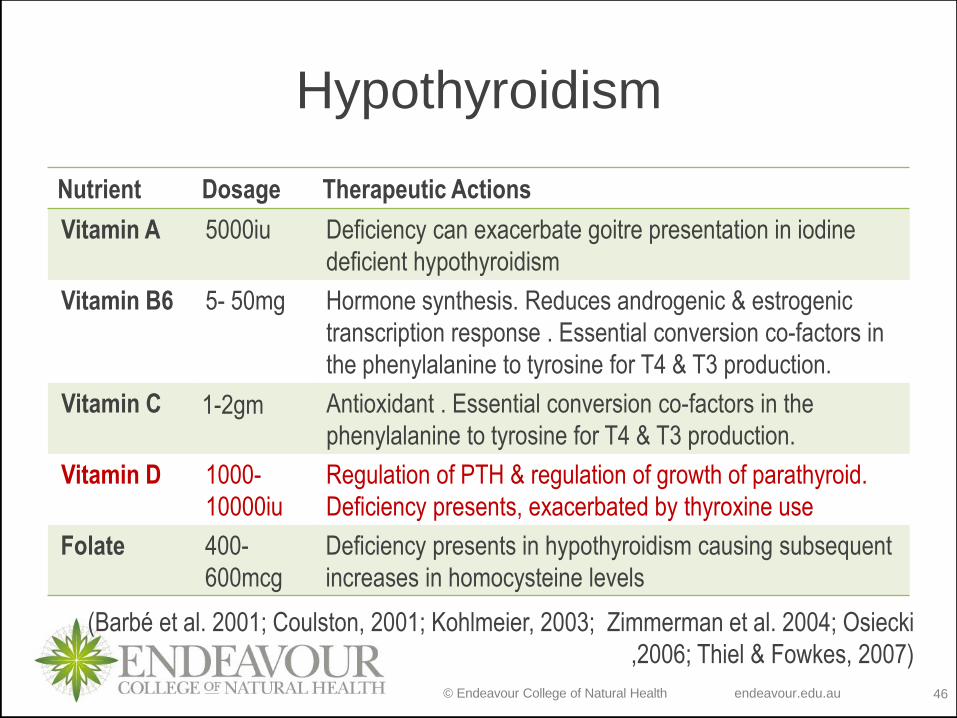
Hypothyroidism
Nutrient Dosage Therapeutic Actions
Vitamin A 5000iu Deficiency can exacerbate goitre presentation in iodine
deficient hypothyroidism
Vitamin B6 5- 50mg Hormone synthesis. Reduces androgenic & estrogenic
transcription response . Essential conversion co-factors in
the phenylalanine to tyrosine for T4 & T3 production.
Vitamin C 1-2gm Antioxidant . Essential conversion co-factors in the
phenylalanine to tyrosine for T4 & T3 production.
Vitamin D 1000-
10000iu
Regulation of PTH & regulation of growth of parathyroid.
Deficiency presents, exacerbated by thyroxine use
Folate 400-
600mcg
Deficiency presents in hypothyroidism causing subsequent
increases in homocysteine levels
(Barbé et al. 2001; Coulston, 2001; Kohlmeier, 2003; Zimmerman et al. 2004; Osiecki
,2006; Thiel & Fowkes, 2007)
© Endeavour College of Natural Health endeavour.edu.au 47
Hypothyroidism
Therapeutic Actions
Iodine
o Iodine is required for T4 and T3 production. Seaweed
sources are a good bioavailable source of iodine, and
countries with traditionally low intakes of seaweed may
present commonly with deficiencies.
(Thiel & Fowkes, 2005)
Zinc
o “Circulating triiodothyronine and thyroxine are decreased
in zinc deficiency, as is the hypothalamic thyroid-
releasing hormone”
(Thiel & Fowkes, 2005, p. 811)
© Endeavour College of Natural Health endeavour.edu.au 48
Hypothyroidism
Therapeutic Actions
Selenium
o Selenium is an integral component of peripheral
conversion enzymes for T4 to T3 or reverse
(iodothyronine deiodinases). Deficiency of that mineral
will exacerbate hypothyroidism.
o Hypothyroidism is linked to increased free radical
presentation in the liver, depleting this mineral as it is
funnelled into glutathione-peroxidase formation.
(Thiel & Fowkes, 2005; Habra & Sarlis, 2005)
© Endeavour College of Natural Health endeavour.edu.au 49
Hypothyroidism
Therapeutic Actions
Phenylalanine / Tyrosine
o Tyrosine is a non-essential amino acid (can be converted
from phenylalanine) that is required for the production of
thyroid and adrenal hormones.
(Thiel & Fowkes, 2005)
o Deficiencies in phenylalanine or conversion co-factors
(biopterin, vitamin B6, vitamin C & iron) can reduce the
production of thyroxin & triiodothyronin.
(Kohlmeier, 2003)
© Endeavour College of Natural Health endeavour.edu.au 50
Hypothyroidism
Therapeutic Actions
Folate
o “…transient increase in both plasma homocysteine and
serum cholesterol during short-term iatrogenic
hypothyroidism…(22%)…which may confer an increased
cardiovascular risk.” (Barbé et al. 2001, p. 1845)
o Folate, not vitamin B12 was implicated in this alteration
due to alterations in enzymatic control and alterations in
renal clearance.
(Barbé et al. 2001)
© Endeavour College of Natural Health endeavour.edu.au 51
Hypothyroidism
Therapeutic Actions
Vitamin A
o Mild to moderate vitamin A deficiency increases the risk
of goitre presentation in iodine deficiency disorders.
o The “…data suggest that vitamin A supplementation
improves the efficacy of iodine supplementation to
control goitre in children with moderate vitamin A
deficiency.”
(Zimmerman et al. 2004, p. 5442)
© Endeavour College of Natural Health endeavour.edu.au 52
HypothyroidismDrug Action Side Effects Interactions
Thyroxine
(T4)
Liothyronine
(T3)
Synthetic
thyroid
hormones.
T4 is
metabolized
to T3 in
peripheral
tissue. T3 is
10X more
biologically
active than
T4 & doesn’t
require
conversion.
High dose =
palpitations,
nervousness,
insomnia,
tremor,
reduced bone
density. Will
resolve with
reduced
dosage.
T3 can be a
cardio toxic
agent
Calcium, Iron, Magnesium, Zinc: form
insoluble complexes with the drug.
Separate dose by 2 hours. Mineral
deficiencies are linked to poor thyroid
hormone production or peripheral
conversion.
Tyrosine: Additive effects as tyrosine is a
precursor to thyroid hormone
Thiocyanates & Goitrogens: Inhibits the
body’s absorption or utilization of iodine,
increasing the requirement for synthetic T4
& T3
Saturated Fats: decrease T3 levels and
promote body fat accumulation.
(Pizzorno & Murray 2006; Bullock et al, 2007 Dal Maso et al. 2009; Braun & Cohen, 2010)
© Endeavour College of Natural Health endeavour.edu.au 53
Hypothyroidism
Thyroxine & Liothyronine
Lithium, Iodine containing drugs / supplements, Tricyclic
antidepressants
o Concurrent utilization may increase the requirement for
synthetic T4 & T3
Ethanol, high free radicals, IL-6, smoking, manganese
excess and high cortisol
o Reduce peripheral thyroid hormone conversion, altering
the requirements for synthetic T4.
(Habra & Sarlis, 2005; Pizzorno & Murray, 2006; Soldin &
Aschner, 2007; Valeix et al. 2008; Sarris & Wardle, 2010)
© Endeavour College of Natural Health endeavour.edu.au 54
Referenceso Barbé et al (2001). Homocysteine, folate, vitamin B12, and
transcobalamins in patients undergoing successive hypo- and
hyperthyroid states .’The journal of clinical endocrinology &
metabolism , Vol. 86, No. 4, pp.1845-1846. Retrieved 7 April 2011
from :
http://jcem.endojournals.org.ezp01.library.qut.edu.au/cgi/content/full/8
6/4/1845
o Braun, L., & Cohen, M. (2010). Herbs and Natural Supplements Inkling : An
Evidence-Based Guide. Chatswood, NSW: Churchill Livingstone
Australia.
o Bryant, B., & Knights, K. (2014). Pharmacology for Health Professionals
ebook. Elsevier Health Sciences.
o Bullock, S., & Manias, E. (2007). Fundamentals of pharmacology. Pearson
Higher Education AU
o Coulston, AM Rock, CL & Monsen, ER 2003, Nutrition in the prevention and
treatment of disease. Academic press, UK
© Endeavour College of Natural Health endeavour.edu.au 55
Referenceso Dal Maso, L Bosetti, C La Vecchia, C & Franceschi, S (2009). Risk factors
for thyroid cancer: an epidemiological review focused on nutritional
factors. Cancer causes control. 20, 75–86. Retrieved 11 April 2011
from :
http://proquest.umi.com.ezp01.library.qut.edu.au/pqdlink?Ver=1&Exp=
04-09-2016&FMT=7&DID=1627819891&RQT=309
o Gropper, SS Smith, JL & Groff, JL (2009). Advanced nutrition and human
metabolism. 5th ed. Wadsworth, California, USA.
o Habra, M & Sarlis, NL (2005). Thyroid and aging. Reviews in endocrine and
metabolic disorders. 6, 145-154. Retreived 11 April 2011:
http://proquest.umi.com.ezp01.library.qut.edu.au/pqdweb?index=0&di
d=915775391&SrchMode=1&sid=1&Fmt=6&VInst=PROD&VType=PQ
D&RQT=309&VName=PQD&TS=1302493811&clientId=14394
o Hywood, A (2004). Effective Herbal Approaches to Thyroid Dysfunction,
MediHerb In Clinic seminar series notes
o Hosig, K. (2005). Nutrient Metabolism. Journal Of Nutrition Education &
Behavior, 37(3), 163-164.
© Endeavour College of Natural Health endeavour.edu.au 56
Referenceso Kumar, P., & Clark, M. Clinical Medicine. 2009. Edinburgh: WB Saunders.
o Osiecki, H. (2006). The physician’s handbook of clinical nutrition (7th ed.):
Bioconcepts Queensland.
o Pizzorno, J. E., & Murray, M. T. (2006). Text book of natural medicine. 3rd
ed. Churchill Livingstone Elsevier.
o Sarris, J., & Wardle, J. (2010). Clinical Naturopathy : An Evidence-based
Guide to Practice. Sydney [Australia]: Churchill Livingstone Australia.
o Soldin, O., & Aschner, M. (2007). Effects of manganese on thyroid hormone
homeostasis: Potential links. Neurotoxicology, (5), 951.
o Subudhi, U., & Chainy, G. B. (2010). Expression of hepatic antioxidant
genes in l-thyroxine-induced hyperthyroid rats: Regulation by vitamin
E and curcumin. Chemico-Biological Interactions, (2), 304.
o Thiel, R., & Fowkes, S. W. (2007). Down syndrome and thyroid dysfunction:
should nutritional support be the first-line treatment?. Medical
Hypotheses, 69(4), 809-815.
© Endeavour College of Natural Health endeavour.edu.au 57
Referenceso Tortora, GJ, Grabowski, SR ( 2003). Principles of anatomy and physiology
10th Edition; Wiley International, New York
o Valeix, P., Faure, P., Bertrais, S., Vergnaud, A., Dauchet, L., & Hercberg, S.
(2008). Effects of light to moderate alcohol consumption on thyroid volume
and thyroid function. Clinical Endocrinology, (6). 988.
o Venditti, P & Di Meo, S (2006). Thyroid hormone-induced oxidative stress.
Cellular molecular life science, 63, 414–434. Retreieved 11 April 2011
from:
http://proquest.umi.com.ezp01.library.qut.edu.au/pqdweb?index=
0&did=2044085871&SrchMode=1&sid=1&Fmt=6&VInst=PROD&V
Type=PQD&RQT=309&VName=PQD&TS=1302501816&clientId=14
394
o Zimmermann, MB Wegmuller, R Zeder, C Chaouki, N & Torresani, T
(2004). The effects of vitamin A deficiency and vitamin A
supplementation on thyroid function in goitrous children. The journal of
clinical endocrinology & metabolism, 89, 11, 5441–5447. Retreieved 7
April 2011 from:
http://jcem.endojournals.org.ezp01.library.qut.edu.au/cgi/reprint/89/11/
5441
o KW
© Endeavour College of Natural Health endeavour.edu.au 58
COMMONWEALTH OF AUSTRALIA
Copyright Regulations 1969
WARNING
This material has been reproduced and communicated to you by or on behalf of the Australian College of Natural Medicine Pty Ltd (ACNM) trading as Endeavour College of Natural Health, FIAFitnation, College of Natural Beauty, Wellnation - Pursuant Part VB of the Copyright Act 1968 (the Act).
The material in this communication may be subject to copyright under the Act. Any further reproduction or communication of this material by you may be the subject of copyright protection under the Act.
Do not remove this notice.