Embed Size (px)
Citation preview

MANEIG DEL SHOCK SÈPTIC (I LA SEPSIS GREU)
Pedro Castro RebolloÀrea de Vigilancia IntensivaHospital Clínic de Barcelona
Curs de Formació Continuada de la Societat Catalanobalear de
Medicina Interna 2015
10 de Juny de 2015

AGENDA
• Què són la sepsis greu i el shock sèptic?
• Cóm es diagnostiquen?
• Cóm es tracten?

CAS CLÍNIC
Pacient dona de 42 anys d’ edat que es portada per alteració del
nivell de consciència.
ANTECEDENTS:
• Ex-politoxicomania (ingrés per deshabituació 2 setmanes abans).
En tractament amb metadona.
• Infecció per VHC (sense hepatopatia)
MALALTIA ACTUAL:
Quadre de 24 hores d’evolució de malestar general, nàusees,
vòmits i diarrees sense productes patològics. La seva parella, en
intentar despertar-la pel matí, observa que no respon i avisa al
SEM.

CAS CLÍNIC
EXPLORACIÓ FÍSICA:
SEM: Somnolenta, pupil·les reactives, PA 97/70 mmHg, FC 140
bpm, SpO2 95% basal, Tª 39ºC, glucèmia capil·lar 84.
Urgències: Afectació de l’estat general. CGS 8. PA 80/40 mmHg.
FC 148 bpm, FR 32 rpm, SpO2 84% basal. Hipofonesi hemitòrax
dret. Abdomen normal. No signes meningis. Mobilitza les 4
extremitats.
Què té la pacient?
Què fem?

QUÈ SÓN?. CONCEPTE
Sepsis: Síndrome causada per una resposta
desproporcionada o inapropiada del cos davant
una infecció

FISIOPATOLOGIA
Vincent JL, Lancet 2013

FISIOPATOLOGIA
Respuesta inflamatoria inapropiada
Alteración de la microcirculación
Alteración de la macrocirculación
- Microtrombosis- Vasodilatación- Disf. Mitocondrial- ↑ permeabilidad- ↓ DO2
Venosa Arterial
Disfunción miocárdica
- Vasodilatación- Hipotensión- ↓ Precarga-↓ DO2
- ↓ Gasto cardíaco - Hipotensión-Hipoperfusión-↓ DO2 P. Castro

QUÈ SÓN?. DEFINICIÓ
Bone RC, Chest 1992

QUÈ SÓN?. DEFINICIÓ
Modificado de Castro P, en Farreras–Rozman 2012
Definiciones relacionadas con sepsis
SRIS
(1) Temperatura < 36ºC o > 38ºC(2) Frecuencia cardiaca > 90 lpm(3) Frecuencia respiratoria > 20 rpm o PaCO2 < 32 mmHg (o necesidad
de ventilación mecánica)(4) Leucocitos en sangre > 12x109/L, o < 4x109/L o >10% de formas
inmaduras (bandas)
SepsisInfección con 2 o más signos de SRIS* o con algunos signos deinflamación sistémica en respuesta a la infección**
Sepsis grave
Sepsis asociada a disfunción orgánica o hiperlactacidemia
Shock séptico
Sepsis grave con hipotensión pese a aporte adecuado de líquidos ohiperlactacidemia
*Definición de 1ª Conferencia de Consenso (1991); **Definición de 2ª Conferencia de Consenso (2001)

QUÈ SÓN?. DEFINICIÓ
Modificado de Levy MM, Crit Care Med 2003
Criterios diagnósticos de sepsis (Conferencia Consenso 2001)Infección (documentada o sospechada) y alguno de los siguientes
Variables generales
Fiebre (Tª central >38,3ºC) Hipotermia (Tª central <36ºC)
FC >90 lpm o >2DS de valor normal Taquipnea
Alteración del sensorio Edema significativo o balance positivo (>20 ml/kg en 24h)
Hiperglucemia (>120 mg/dl) sin DM
Variables inflamatorias
Leucocitosis (>12000 /µl) o >10% bandas Leucopenia (<4000 /µl)
PCR > 2DS valor normal Procalcitonina >2DS valor normal
Variables hemodinámicas
Hipotensión arterial (PAS <90 mmHg, PAM < 70 mmHg, o ↓ PAS >40 mmHg o 2 DS valor normal)
SvO2 >70%
IC > 3,5 L/min/m2
Variables de disfunción orgánica
Hipoxemia (PaO2/FiO2 < 300) Oliguria aguda (<0,5 ml/Kg/h) o ↑Cr >0,5 mg/dL
INR >1,5 o TTPA >60 segundos Íleo
Plaquetas <100.000/µl Bilirrubina total >4 mg/dL
Variables de perfusión tisular
Lactato > 1 mmol/L ↓ Relleno capilar o livideces

QUÈ SÓN?. DEFINICIÓ
Zhao H, Crit Care Med 2012

QUÈ SÓN?. DEFINICIÓ
Vincent JL, Lancet 2013
“The terms severe sepsis and sepsis have often beenused interchangeably. To clarify this situation, we believeevidence of organ dysfunction should be included in the
criteria for sepsis—ie, sepsis should be defined as asystemic response to infection with the presence of some
degree of organ dysfunction”

EPIDEMIOLOGIA DE LA SEPSIS A ESPANYA
Esteban A, Crit Care Med 2007
4 months prospective study (Madrid)
15.852 admitted patients
SEPSIS 4.4% (Incidence >300 cases x 100.000 adults/year)
SEVERE SEPSIS 28.3%
SEPTIC SHOCK 29.6%
MORTALITY
6.7%
20.7%
45.7%

EPIDEMIOLOGIA DE LA SEPSIS
Kaukonen KM, JAMA 2014
Retrospective study, n=101.064 patients with severe sepsis / septic shock in
Australia and New Zealand

EPIDEMIOLOGIA DE LA SEPSIS
Kaukonen KM, JAMA 2014

CAS CLÍNIC
EXPLORACIÓ FÍSICA:
SEM: Somnolenta, pupil·les reactives, PA 97/70 mmHg, FC 140
bpm, SpO2 95% basal, Tª 39ºC, glucèmia capil·lar 84.
Urgències: Afectació de l’estat general. CGS 8. PA 80/40 mmHg.
FC 148 bpm, FR 32 rpm, SpO2 84% basal. Hipofonesi hemitòrax
dret. Abdomen normal. No signes meningis. Mobilitza les 4
extremitats.
Què té la pacient?Què fem?

DIAGNÒSTIC
1. Diagnòstic de la síndrome
a) SRIS no infecciós
b) Sepsis
c) Sepsis greu
d) Shock sèptic
2. Diagnòstic del focus
3. Diagnòstic etiològic

DIAGNÒSTIC. SEPSIS VS SRIS NO INFECCIÓS
• Diferents entitats poden provocar SRIS: reaccions farmacològiques, fenòmens autoimmunes, ...
• Ens basem en la clínica, les dades microbiològiques i analítiques (biomarcadors) per pensar en un procés sèptic
Especificidad Sensibilidad Ventajas InconvenientesLeucocitos + +++ Sensible Inespecífico
PCR ++ ++ Barato Respuesta tardíaBaja especificidad
PCT ++++ + Inducciónrápida
Baja sensibilidad para infección local
Caro
IL-6 + +++ Sensible Poca correlación congravedad
NO hem de tractar TOT procés febril com infecciós, però
davant el dubte…

DIAGNÒSTIC. SEPSIS VS SG / SS
• HIPOTENSIÓ* NO ÉS EQUIVALENT A SHOCK (necessitemevidència de perfusió tissular inadequada)
“Shock is best defined as a life-threatening, generalized form ofacute circulatory failure associated with inadequate oxygenutilization by the cells. It is a state in which the circulation isunable to deliver sufficient oxygen to meet the demands of thetissues, resulting in cellular dysfunction”
*PAS < 90 mm Hg ó ↓≥40 mm Hg de la basal ó PAM < 65 mm Hg Cecconi M, Intensive Care Med 2014

DIAGNÒSTIC. SEPSIS VS SG / SS
• SHOCK NO REQUEREIX LA PRESÈNCIA D’HIPOTENSIÓ*(SHOCK CRÍPTIC)
─ Alteracions de la microcirculació
─ Mecanismes compensadors / Fàrmacs
─ Desplaçament de la corba d'autoregulació a la dreta
Cecconi M, Intensive Care Med 2014*PAS < 90 mm Hg ó ↓≥40 mm Hg de la basal ó PAM < 65 mm Hg

HTA I AUTOREGULACIÓ
Strandgaard S, Br Med J 1973
És important conèixer la
pressió arterial “habitual” del
pacient (anamnesi, revisió
ingressos previs, signes
d’hipertensió arterial).

Puskarich MA, Resuscitation 2011
MORTALITAT EN SHOCK CRÍPTIC

SIGNES D’HIPOPERFUSIÓ TISSULAR
Strehlow MC, Emerg Med Clin N Am 2010
Perf
usió
n
Piel
Gastrointestinal
Riñón
Cerebro
Corazón

SIGNES D’HIPOPERFUSIÓ TISSULAR

MARCADORS BIOQUÍMICS DE SHOCK
Si el quadre del pacient és suggestiu de shock (per història i
exploració física), és recomanable mesurar marcadors de
perfusió tissular, sobretot en absència d’ hipotensió:
• “Directes”:
• LACTAT (↑) (> 4 mmol/L ó 36 mg/dL)
• SvcO2 (↓)
• “Indirectes”:
• pH (↓)
• Excés de base (↓)
• Anion Gap (↑)
Antonelli M, Intensive Care Med 2007

CAS CLÍNIC
Analítica: PCR 30 mg/dl, Cr 1,4 mg/dl, lactat 40 mg/dl, Troponina I
2,497 ng/ml, 1500 leucòcits, TP 45%. Tòxics: metadona positiu,
resta negatiu.
Per tant, la pacient té shock sèptic
Què fem?

• Diagnòstic de focus (pneumònia, endocarditis,…): És important pel tractament antibiòtic i el control del focus
DIAGNÒSTIC DE FOCUS

CAS CLÍNIC
Sediment d’orina: 0 leucòcits
TC craneal y anàlisis LCR: Normal
Rx tòrax

CAS CLÍNIC

• Diagnòstic etiològic (germen responsable): És important pel tractament antibiòtic (empíric o dirigit, i el desescalat)
─ Tot pacient al que se li va a iniciar tractament antibiòtic hauria de tenir cultius (HC i segons focus
• Curiosament, es fan <70% dels casos y < 50% serán positius*
DIAGNÒSTIC ETIOLÒGIC
Esteban A, Crit Care Med 2007

NI EL DIAGNÒSTIC ETIOLÒGIC NI DEL FOCUS HAN DE RETARDAR L’INICI DEL TRACTAMENT
DIAGNÒSTIC DE FOCUS I ETIOLÒGIC
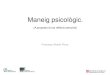
CAS CLÍNIC
UC: Negatiu (48 horas)
HC: Negatius (5 dies)
LCR: Tinció de Gram: sense gèrmens (2 hores)
Antígens urinaris pneumococ i Legionel·la: Negatius (6 hores)
Aspirat traqueal: Tinció de Gram: Bacils gramnegatius (2 hores)
Cultiu: Klebsiella Pneumoniae (24 hores). Antibiograma:
Multisensible (48h)

TRACTAMENT
• Tractament etiològic
• Tractament antibiòtic
• Control del focus
• Tractament de suport
• Reanimació inicial (Fluids ± Vasopressors)
• Manteniment posterior

TRACTAMENT ANTIBIÒTIC. RECOMANACIONS
• ADIENT. Empíric que cobreixi 100% de patògens més probables

Kumar A, Chest 2009
TRACTAMENT ANTIBIÒTIC ADIENT
Retrospective study, n=5.715 patients with septic shock(20%)

TRACTAMENT ANTIBIÒTIC. RECOMANACIONS
• ADIENT. Empíric que cobreixi 100% de patògens més probables
• PRECOÇ. El més aviat possible (primera hora)

Kumar A, Crit Care Med 2006
TRACTAMENT ANTIBIÒTIC PRECOÇRetrospective study, n=2.154
patients with septic shock
TRACTAMENT ANTIBIÒTIC. RECOMANACIONS
• ADIENT. Empíric que cobreixi 100% de patògens més probables
• PRECOÇ. El més aviat possible (primera hora)
• Endovenós, per tots els catèters disponibles i dosis altes
• Considerar característiques farmacocinètiques / farmacodinàmiques (incloent penetració en teixits)
• Considerar teràpia combinada
• Desescalar o ajustar a las 48-72 hores

CONTROL DEL FOCUS
• Crític en diverses patologies (perforació visceral,abscés intraabdominal, colangitis, colecistitisgangrenosa, empiema, uropatia obstructiva…)
• Pot incloure:
─ Retirada de dispositius i cossos estranys infectats(catèter, vàlvula, marcapassos)
─ Drenatge fluids infectats (empiema) o abscessos
─ Desbridament i resecció de teixits

TRACTAMENT DE SUPORT. REANIMACIÓ INICIAL
La reanimació inicial (fluids ± vasopressors) és “tan” important com el tractament antibiòtic
Natanson C, Am J Physiol 1990

REANIMACIÓ INICIAL: EGDT
Rivers E, NEJM 2001
15% Mortalitat hospitalària
(30,5 vs 46,5%)
Randomized study (130 vs 133)

REANIMACIÓ INICIAL. SURVIVING SEPSIS CAMPAIGN
Dellinger RP, Crit Care Med 2004, 2008, 2010, 2013
SURVIVING SEPSIS CAMPAIGN BUNDLESA completar en las primeras 3 horas1. Medir niveles de lactato2. Tomar HC antes de los antibióticos3. Administrar antibióticos de amplio espectro4. Administrar 30 ml/kg de cristaloide (si hay hipotensión o lactato ≥4mmol/L (36 mg/dL))A completar en las primeras 6 horas5. Administrar vasopresores (si hay hipotensión refractaria a fluidos) para mantener PAM ≥65 mmHg6. En caso de shock séptico, medir la PVC (objetivo ≥8 mmHg) y la ScvO2 (objetivo ≥70%)7. Monitorizar lactato (si estaba elevado) hasta su normalización

REANIMACIÓ INICIAL. PROTOCOLS
Tratamiento de la sepsis grave/shock séptico Hospital Clínic (2012)

REANIMACIÓ INICIAL. PROTOCOLS
The Process investigators, NEJM 2014
RCT, n= 1341 patients with septic shock
RCT, n= 1600 patients with septic shock
P=0.82
ARIS
E in
vest
igat
ors,
NEJ
M 2
014
RCT, n= 1260 patients with early septic shock
Mou
ncey
PR
, NEJ
M 2
015

REANIMACIÓ INICIAL. PROTOCOLS
Angus DC, Intensive Care Med 2015
Als tres estudis, el tractament usual necessità menys fluids,menys vasopressors, menys transfusions i mínimamonitorització de SvcO2

FLUÏDOTERÀPIA: QUANT?. AVALUACIÓ DE LA PRECÀRREGA
• En la sepsis hi ha hipovolèmia (sempre relativa i, amb freqüència, absoluta)
• L’objectiu de la fluïdoteràpia és augmentar el cabdal cardíac (i la DO2), augmentant la precàrrega
• Per valorar la precàrrega (i la resposta a fluids) podem utilitzar:─ Estimacions clíniques
─ Estimacions de precàrrega estàtica (PVC, POAP)
─ Estimacions de precàrrega dinàmica (VVS, VPP)
─ Realitzar una “prova de càrrega”

FLUÏDOTERÀPIA: QUANT?. AVALUACIÓ DE LA PRECÀRREGA ESTÀTICA
• La PVC s’utilitza com una estimació indirecta de la volèmia o
precàrrega, però no és un volum, és una pressió!!
• Tot i així, i davant la manca d’altres eines, pot ser d’utilitat
• No creure cegament en la PVC. És preferible monitoritzar les
respostes al tractament sobre la pressió arterial i, sobretot, la
perfusió tissular

FLUÏDOTERÀPIA: QUANT?. AVALUACIÓ DE LA PRECÀRREGA DINÀMICA
Perel A, Intensive Care Med 2014
• Utilitza la influència de la respiració sobre el retorn venós.
• És útil en pacients ventilats ben adaptats i en ritme sinusal.

Davant el dubte de si un pacient en shock respondrà o no a
fluïdoteràpia, és recomanable una “prova de càrrega de
volum”: administració en curt període de temps (30 minuts)
de 20-30 ml/kg de cristal·loide
FLUÏDOTERÀPIA. CÓM?. PROVA DE CÀRREGA DE VOLUM

FLUÏDOTERÀPIA. CÓM?. PROVA DE CÀRREGA DE VOLUM
Alternativa: Passive leg raising test

Murphy CV, Chest 2009
FLUÏDOTERÀPIA ADIENT. QUAN?
Retrospective analysis, n= 212 patients with SS + ALI
La fluïdoteràpia inicial millora inflamació, microcirculació, … però compte amb la fluïdoteràpia excessiva posterior.

FLUÏDOTERÀPIA. AMB QUÈ?. CRISTAL·LOIDES VS COL·LOIDES
Effect (mL) of the infusion of 1 liter of different formulations in body compartments
FormulationIntracellular
volumeExtracellular volume
Interstitial volume Plasmatic volume0.9% NaCL -100 825 275Glucose 5% 660 255 855% NaCL -2950 2960 9905% Albumin 0 500 5006% HES 0 500 500Total blood 0 0 1000

FLUÏDOTERÀPIA. AMB QUÈ?. CRISTAL·LOIDES VS COL·LOIDES
Myburgh JA, NEJM 2012 Perner A, NEJM 2012
RCT, n= 7000 ICU patients RCT, n= 798 patients with severe sepsis patients
P = 0.07
Primary outcome: Dead at day 90:
51 vs 43%; p = 0.03

Finfer S, NEJM 2004
FLUÏDOTERÀPIA. AMB QUÈ?. CRISTAL·LOIDES VSALBÚMINA
RCT, n=6997 critically ill patients
P=0.96
4%
Randomized open-label trial, n=1818 patientswith severe sepsis / septic shock
20%
Caironi P, NEJM 2014

La reanimació es realitza amb cristaloïdes
fonamentalment, o, en pacients hipoalbuminèmics o
cirrótics, amb albúmina al 5-20%
Tratamiento de la sepsis grave/shock séptico Hospital Clínic (2012)
FLUÏDOTERÀPIA. AMB QUÈ?.

TRACTAMENT DE SUPORT INICIAL. VASOPRESSORS. QUIN?
Fármacos vasoactivos más utilizados en el shock séptico
Fármaco y dosisEfectos
α β1 β2 Dopaminérgico
Noradrenalina
0,01-3 μg/kg/min +++ ++ 0 0
Dopamina
1-5 μg/kg/min 0 + 0 ++
5-10 μg/kg/min + ++ 0 ++
10-40 μg/kg/min ++ ++ 0 ++
Adrenalina
0,04-3 μg/kg/min +++ +++ ++ 0
Fenilefrina
0,4-2 μg/kg/min +++ 0 0 0
Dobutamina
2-40 μg/kg/min 0/+ +++ ++ 0
Modificado de Castro P, en Farreras–Rozman 2012

De Backer D, NEJM 2010 De Backer D, Crit Care Med 2012
RCT, n=1679 patients with shock
TRACTAMENT DE SUPORT INICIAL. VASOPRESSORS. QUIN?

Asfar P, NEJM 2014
TRACTAMENT DE SUPORT INICIAL. VASOPRESSORS. QUANT?
RCT, open-label, n=1679 patients with septic shock
PAM 65-70 mmHg
PAM 80-85 mmHg
P=0.57 P=0.74
Pacients amb HTA crònica presentaren més fracàs renalen el grup de menor PAM
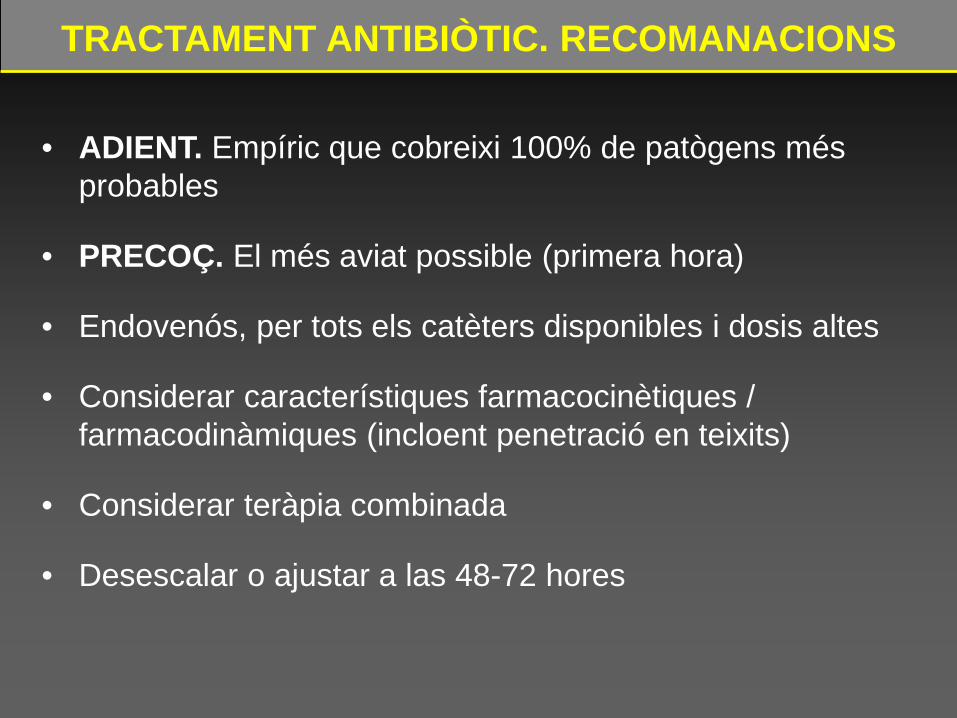
Bai X, Crit Care 2014
TRACTAMENT DE SUPORT INICIAL. VASOPRESSORS. QUAN?
Retrospective study, n=213 patients with septic shock

TRACTAMENT AMB INOTRÒPICS. QUAN?
• En general al SG/SS reanimat el cabdal cardíac (CO) està ↑.
• Excepcions:
v Fase final SG/SS
v Pacients cardiòpates
v Disfunció miocàrdica associada a sepsis
Ø Aproximadament 40% de SG/SS
Ø Inici a las 24-48 hores del SG/SS
Ø Reversible en 7-10 dies
Zanotti-Cavazzoni SL, Curr Op Crit Care 2009; Hunter JD, Br J Anaesth 2010

• Tractament d’elecció: Dobutamina
• Idealment, fer ecocardiograma i monitoritzar cabdal
cardíac.
• Si no tenim monitorització, es pot fer “prova clínica”
• En cas d’ empitjorament amb dobutamina, valorar:
v Taquiarítmia
v Miocardiopatia hipertròfica obstructiva
v Hipovolèmia
• No utilitzar per buscar cabdal cardíac suprafisiològic
TRACTAMENT AMB INOTRÒPICS. QUAN?

TRACTAMENT DE MANTENIMENT
• Monitorització clínica, hemodinàmica I bioquímica (lactat)
• Estratègia conservadora de fluids i transfusions
• Profilaxis úlcera d'estrès
• Profilaxis trombosis venosa profunda
• Ventilació mecànica protectiva
• Corticoides per la insuficiència suprarenal relativa
• Control glicèmic amb insulina
• Tractament renal substitutiu si necessari
• Tractaments fisiopatològics:
• Proteïna C Activada recombinant (Xigris ®)

Randomized open-label trial, n=998 patientswith septic shock
7 g/dL
9 g/dL
Hébert PC, N Engl J Med 1999
Hb 7-9 g/dl
Hb 10-12 g/dl
Randomized open-label trial, n=838 critically ill patients
Holst LB, NEJM 2014
TRACTAMENT DE MANTENIMENT. TRANSFUSIÓ HEMATIES

TRACTAMENT MANTENIMENT. CORTICOIDES
Sprung CL, N Engl J Med 2008
Annane D, JAMA 2002
RCT, n=499 patients with septic shock
P=n.s. P<0.001
RCT, n=300 patients with septic shock

CONCLUSIONS
• La sepsis greu i el shock sèptic són entitats prevalents igreus
• És important un reconeixement precoç, basat en lasospita clínica i ajudat per marcadors bioquímics
• El diagnòstic etiològic i del focus són molt importants,però no han de retardar l’inici del tractament
• En el tractament inicial són fonamentals tant eltractament etiològic, que inclou l'antibiòtic (precoç iapropiat) i el control de focus, com el de suport, ambfluïdoteràpia i vasopressors

LLIBRE ELECTRÒNIC iTUNEShttps://itunes.apple.com/us/book/enfermo-critico-y-emergencias/id625996083?l=es&ls=1


Voluntario sano Shock séptico (disminución de la densidad
de vasos pequeños)
De Backer et al, Am J Resp Crit Care Med 2002
Microvasculatura sublingual
MANEJO SG/SS: SEPSIS GRAVE/SHOCK CRÍPTICO