Embed Size (px)
Citation preview

TECHNOLOGIES
DRUG DISCOVERY
TODAY
Modeling of human tumor xenograftsand dose rationale in oncologyMonica Simeoni1,*, Giuseppe De Nicolao2, Paolo Magni2,
Maurizio Rocchetti3, Italo Poggesi41Clinical Pharmacology Modelling & Simulation, GlaxoSmithKline, Uxbridge, UB11 1BT, United Kingdom2Dipartimento di Ingegneria Industriale e dell’Informazione, Via Ferrata 1, 27100 Pavia, Italy3Independent Consultant, Via T. Grossi 13, 20017 Rho, Milan, Italy4Advanced PKPD Modeling & Simulation, Janssen Research & Development, Milan, Italy
Drug Discovery Today: Technologies Vol. 10, No. 3 2013
Editors-in-Chief
Kelvin Lam – Simplex Pharma Advisors, Inc., Arlington, MA, USA
Henk Timmerman – Vrije Universiteit, The Netherlands
Translational Pharmacology: From Animal to Man and Back
Xenograft models are commonly used in oncology
drug development. Although there are discussions
about their ability to generate meaningful data for
the translation from animal to humans, it appears that
better data quality and better design of the preclinical
experiments, together with appropriate data analysis
approaches could make these data more informative
for clinical development. An approach based on math-
ematical modeling is necessary to derive experiment-
independent parameters which can be linked with
clinically relevant endpoints. Moreover, the inclusion
of biomarkers as predictors of efficacy is a key step
towards a more general mechanism-based strategy.
Introduction
Xenograft models are the most popular preclinical models for
evaluating the anticancer activity of new compounds under
development in the oncology therapeutic area [1]. Despite
some limitations, their implementation is relatively easy and
requires limited resources. Recently, several mathematical
models have been introduced to describe the relationship
between the drug pharmacokinetic and the dynamics of
tumor growth (PK/PD models) in these experiments (see
for instance the reviews from Bonate [2] and Della Pasqua
[3]). These mathematical models are generally based on
*Corresponding author.: M. Simeoni ([email protected])
1740-6749/$ � 2012 Elsevier Ltd. All rights reserved. http://dx.doi.org/10.1016/j.ddtec.2012
Section editor:Oscar Della Pasqua – Leiden/Amsterdam Center for DrugResearch, Leiden, The Netherlands.
biological and physiological grounds, so that their para-
meters can be associated with biological mechanisms and
processes. Furthermore, these models may be used as predic-
tive tools for anticipating the outcome of new dosing regi-
mens and for the optimization of the preclinical
experimental design. It is of note that the predictive value
of animal models does not only rely on experimental vari-
ables (i.e. what is effectively measured), but also on the ability
to identify the underlying physiological processes. Mathe-
matical models can be the suitable tools for extracting the
descriptors of these processes, which can be translated from
preclinical to clinical setting. The purpose of this paper is to
give a general, although not exhaustive, view of the applica-
tion of mathematical modeling as a translational tool for the
interpretation of experimental tumor growth data in xeno-
graft models.
Tumor xenograft models
The use of animal models for cancer chemotherapy studies
was already reported in late 1940s [4]. The use of human
tumors transplanted into animal models (xenografts) faced
initially the problem of tissue rejection by the immune reac-
tion of the host. The most important advance in human
xenograft models has been the introduction of the athymic
.07.004 e365

Drug Discovery Today: Technologies | Translational Pharmacology: From Animal to Man and Back Vol. 10, No. 3 2013
nude mice: animals resulting from the inheritance of a reces-
sive mutation, hairless and exhibiting the congenital absence
of thymus [5]. The consequent inhibition of T-lymphocytes
with reduced capacity to reject ‘foreign’ tissue allowed the
successful transplantation of human tumors, either by direct
implantation of patient biopsy material or via inoculation of
continuous human tumor cell lines [5,6]. The easiest experi-
ment is the subcutaneous xenograft, in which tumor frag-
ments or tumor cell suspensions are implanted ectopically
into the flanks of athymic mice. When the tumors reach a
pre-specified volume, mice are randomized into control and
treated groups and the tumor growth in the different groups
is evaluated by recording the dimensions of the tumors at
selected time points, for instance using calipers or other
techniques. Experimental results are then summarized using
different metrics, such as the ratio of treated to control tumor
weight at a pre-specified time, or the difference in time
(treated-control; tumor delay) to reach a predefined tumor
weight [7].
In general, different issues should be considered to describe
the predictivity of the outcome in xenograft models. One
aspect concerns the assessment of active vs. nonactive com-
pounds. Several experimental factors need to be identified
and controlled to make the xenograft models effective for the
screening of new compounds, for instance, the appropriate
choice of tumor models, the experimental conditions, the
dosing regimens and the exposure achieved during the
experiments, the experimental endpoints and an accurate
statistical assessment to compare the experimental groups
[8]. A retrospective study of National Cancer Institute on 39
cytotoxic anticancer drugs showed that 45% of the 33 agents
with activity in one-third or more of tested pre-clinical xeno-
graft models (median 12 xenograft models per agent) had also
clinical activity (P = 0.04) [9]. However, activity within a
particular histological type of xenograft generally did not
predict clinical activity in the same tumor, with the exception
of non-small cell lung cancer. Several considerations may
explain the examples in which the xenograft model was not
able to identify the active compounds. One potential reason
for the of lack of predictivity may be found in the fact that
tumors are implanted subcutaneously in the animal flank
(ectopically), so these models may not mimic tumors of other
origins. Furthermore, these models, in contrast to the clinical
scenario, do not develop metastases. This motivated the
development of xenograft orthotopic models where
the tumor is implanted in the originary tissue in which the
primary tumor developed [1]. A new promising and sophis-
ticated class of animal models of human cancer are the
genetically engineered models [10], either transgenic or
endogenous. Many experimental models now exist that accu-
rately mimic the pathophysiological and molecular features
of human malignancies, but further investigations are
required to assess if they can replace the xenograft models,
e366 www.drugdiscoverytoday.com
or if the two classes have validity in different diagnostic
applications [1].
Most of the tumor growth inhibition metrics are not
invariant with respect to the experimental conditions. For
instance, the time to maximal value of the tumor growth
inhibition was shown to be dose-, time- and dosing regimen-
dependent [11]. Only mathematical models that are able to
describe tumor growth by dissecting the system-specific prop-
erties can provide compound-specific and experiment-inde-
pendent model parameters. These models can help improve
the experimental design (e.g. predicting the effect of untested
dose levels and dosing regimens) before setting up a confir-
matory experiment, thus contributing to reduce costs of
experiments and number of animals used. It is indeed our
opinion that in many cases, the failure to correlate animal
and clinical results [12] could be attributed to inappropriate
experimental conditions and/or parameter representation of
compound potency.
Mathematical models for tumor growth
In the past 40 years different mathematical models were built
on xenograft animal model data in an attempt to predict the
exposures at different doses and regimens in animals. On one
hand, mathematical modeling provides a more robust way to
summarize pharmacokinetic and pharmacodynamic proper-
ties; on the other hand, it can be even more important as a
translational tool able to provide rational predictions of
clinical findings from the outcome of preclinical experi-
ments. Mathematical models can be grouped into three main
categories: descriptive (empirical), mechanistic and large
scale/system biology models.
The first proposed models were of a descriptive nature like
the logistic function, the von Bertalanffy growth equation
and the Gompertz function [13] which describe the growth
processes of biological organisms, but are based on para-
meters lacking a full biological basis.
Anna Kane Laird in 1964 [14] was the first scientist to use
the Gompertz curve to fit in vitro data of tumor growth
successfully. The same model was subsequently utilized in
animals [15] and humans [16–19]. To be potentially valid for
translational purposes, a model should be able to predict the
expected outcome at different dosing levels and schedules
from the tested regimens in terms of few meaningful para-
meters amenable to being extrapolated to humans. In this
respect, although these models were able to describe and
compare studies, nevertheless, they had difficulties to allow
for changes of dose levels and schedules.
Although the boundary between empirical and mechan-
istic models is not always sharp, a distinctive feature is that
the latter models account for the physiology underlying the
interplay between the tumor growth process and the drug
action without necessarily going into deeper details about the
involved biological mechanism. Two examples are given by

Vol. 10, No. 3 2013 Drug Discovery Today: Technologies | Translational Pharmacology: From Animal to Man and Back
the models of Simeoni et al. [20,21] and Lobo and Balthazar
[22]. Notably, the existence of specific model parameters
representative of drug potency is a key opportunity for trans-
lational purposes. These models were also called Cell Distri-
bution Model (CDM) and Signal Distribution Model (SDM)
respectively [23]. The first one describes the unperturbed
tumor growth with an exponential phase, followed by a
linear one; the drug acts hitting the tumor cells that even-
tually go to death through a transit compartment model
which takes into account the delayed drug response. It has
also been shown that Simeoni’s model can be formally
derived from a minimal set of basic assumptions formulated
at cellular level [24]. By contrast, in the SDM the drug acts
upon a receptor which initiates a signal transduction cascade
whose final product is a modulation of the killing effect
against tumor cells. The necessity to introduce a transit
compartment model to describe the chemotherapeutic effect
was confirmed in the subsequent modifications of the model
by Jumbe et al. [25] and by Sung et al. [26].
The CDM [20] has also been modified to cope with combi-
nation therapies, to serve as a guide in the selection of clinical
doses and the optimal timing of administration of anticancer
agents so as to maximize tumor suppression [27]. To take into
account possible drug interactions, Koch et al. [28] intro-
duced a multiplicative factor on the action of one of the
two drugs. Both models were proposed for drugs with the
same mechanism of action. Rocchetti et al. [29] proposed a
null-interaction model that combines two single drug tumor
growth inhibition (TGI) models (essentially applying the Bliss
independence criterion in a dynamic context). The proposed
model can simulate the behavior of non-interacting drugs,
whereas synergistic or antagonistic behaviors are highlighted
as deviations from the simulated one.
A promising extension of the mechanistic models is repre-
sented by the inclusion of biomarkers. For instance, Bueno
et al. considered the percentage of phosphorylated Smad2 and
Smad3 (pSmad) as biomarkers that drive the inhibition of
tumor growth, described by a CDM [30]. Yamazaki et al. linked
the inhibitory response of cMet phosphorylation in tumor to
the plasma concentration of an anticancer agent, a competi-
tive ATP-binding of cMet kinase, using an effect-compartment
model. They found that the EC90 of the PK-biomarker model
corresponds to the EC50 of the indirect model describing the
tumor growth, suggesting that near-complete inhibition of
cMet phosphorylation is required to significantly inhibit
tumor growth [31]. An analogous approach was implemented
by Salphati et al. [32] who obtained similar IC50 values with
separate indirect response models relating the pharmacoki-
netics of a PI3K inhibitor and the inhibition of Akt and PRAS40
phosphorylation. Using an integrated pharmacokinetic-bio-
marker-tumor growth model, the authors claimed that 30%
continuous inhibition of phosphorylated Akt signal would be
required to achieve tumor stasis.
Another interesting problem is to understand how the
mathematical models developed for in vivo preclinical
experiments can be applied to the in vitro settings. In most
cases, the analyses of in vitro experiments are limited to the
calculation of EC50 values at a given exposure duration [33]
or the description of the inhibition surfaces as a function of
concentrations and exposure times [34,35]. Mechanistic
models were used (signal transduction model vs. phase-
specific and phase-nonspecific model) to describe the delay
between methotrexate exposure and observable tumor
growth inhibition [22]. A more recent investigation, cover-
ing ten commercial anticancer drugs and four compounds in
early discovery phase, demonstrated that the CDM [20] can
be effectively applied also to in vitro data [36]. Differently
from its in vivo version, the cell proliferation did not slow
down to linear but remained exponential for all observed
sizes of cell cultures in the conditions adopted in these
experiments.
Large scale/system biology models try to mimic in fine
detail the biological pathways and physiological processes
involved. We can group them in continuum, and discrete
cell-based models [37,38]. In continuum models the tumor is
treated as a continuous mass, few cell populations are iden-
tified, subcellular processes are not considered and, usually,
stochastic methods are not used [39,40]. By contrast, discrete
cell-based models see the tumor as a collection of interacting
cells (e.g. [40–43]) and are more suitable to describe phenom-
ena like metastases. Large scale/system biology models make
a set of assumptions about tumor growth, involving cell-cycle
kinetics and biochemical processes, such as those related to
antiangiogenetic and/or immunological responses [44,45].
The simplest heterogeneous models split tumor cells into
proliferating and quiescent ones, while more complex mod-
els describe the cell population as age-structured and take
into account subpopulations related to specific phases of the
cell cycle [46–48]. These models have a much larger number
of parameters compared with the empirical and mechanistic
ones, so that extensive quantitative observations (e.g. flow
cytometry analyses, biochemical and immunological marker
measurements, and so forth) are needed to avoid identifia-
bility problems. A compromise between large scale and the
mechanistic models is the ‘model of spheroid growth’
recently proposed by Ribba et al. [49].
Different techniques can be used in a model-based data
analysis depending on the quality of the data, the collection
scheme and the number of subjects. Estimates of the indi-
vidual PK/PD parameters can be obtained from each indivi-
dual profile, or the mean study parameters can be estimated
either from the average treatment profiles [20,22], or from a
population of profiles using a non-linear mixed effect mod-
eling approach [50]. The last technique has the benefit to
evaluate the inter-individual variability of the parameters
within and across studies [51,52]. Designing the studies for
www.drugdiscoverytoday.com e367

Drug Discovery Today: Technologies | Translational Pharmacology: From Animal to Man and Back Vol. 10, No. 3 2013
Table 1. Variety of experimental conditions and designs used in some xenograft studies. (Lines separate different studies.)
Ref Drug Cell line n per
group
Route Dose (mg/kg) Dose
scheme
Start
day
Sampling times (days)
[20] CPT11 HCT116 5 IV bolus Control, 45, 60 qd1 13 qd 13–22, qd 25–28,
32, 36
Paclitaxel A2780 8 IV bolus Control, 30 q4dx3 8 qd 9–20, 22, 24, 27, 35
Paclitaxel A2780 8 IV bolus Control, 30 q4dx3 13 eod 9–19, 23, 28, 31
5-FU HCT116 8 IV bolus Control, 50 qwx2 8 8, 12, 15, 19, 22, 26
5-FU HCT116 8 IV bolus Control, 50 qwx4 8 10, 14, 17, 21, 24, 28, 31
A A2780 8 IV bolus Control, 60 tidx1, bidx4,
qdx11
9 8, qd 10–23, eod
23–29, 33
B A2780 8 IV bolus Control, 15, 30 bidx5 13 15, 17, 19, 23, 28, 31
B A2780 8 IV inf Control, 83/day 7 days 9 7, 10, 12, 14, 15, 16, 17
[21] A A2780 8 IV bolus Control, 45 qd10 13 13, 15, 19, 21, 23, 26,
29, 33, 37, 42
[22] MTX Ehrlich
ascites cells
10,000 cell/ml In vitro Control, 0.19, 2,
14, 140 mg/ml
24 h Days 1, 3, 5, 7, 9, 11,
13, 15, 17, 20, 22, 24
MTX Sarcoma
180 cells
5000 cell/ml In vitro Control, 0.19, 2,
14, 140 mg/ml
25 h Days 1, 2, 3, 5, 7, 9, 11,
13, 14, 15, 17, 19, 21
[23] Paclitaxel
(Taxol-SUV)
Murine
Colon-26
10 IV Control, 10, 40, 60 (qdx3)qwx3 8 qd 8–13, 15–18,
20–25, 28, 30
[24] Docetaxel A2780 8 IV bolus Control, 10 qd1, q4dx1 8 7, 9, 10, 12, 13, 15, 17,
19, 21, 23, 26, 28, 30
Drug B A2780 7 IV inf Control, 15/day 5 days 7.5 eod 7–19
Drug C A2780 8 Gastric
gavage
Control, 20, 30, 40 10 days 8 8, 10, 14, 16, 18,
21, 24, 28, 31
[25] TDM-1 MMTV-HER2 Fo5 IV 1, 3, 10, 15, 30 q3wx3 biwx10, qw from 11w
TDM-1 MMTV-HER2 Fo5 IV 3.3, 5, 10 qwx9 biwx10, qw from 11w
TDM-1 MMTV-HER2 Fo5 IV 15 q3wx3 biwx10, qw from 11w
TDM-1 BT474EEI IV 0.3, 1, 3, 10, 15 q3wx3 biwx10, qw from 11w
TDM-1 BT474EEI IV 3.3, 5, 10 qwx9 biwx10, qw from 11w
TDM-1 BT474EEI IV 6, 9, 18 q2wx5 biwx10, qw from 11w
TDM-1 BT474EEI IV 15 q3wx3 biwx10, qw from 11w
Trastuzumab BT474EEI IV 15 q3wx3 biwx10, qw from 11w
[26] 5-FU HCT116 In vitro Control, 1,
10, 50, 100 ng/ml
144 h 0, 24, 48, 72, 144 h
5-FU SW480 In vitro Control, 10,
100, 500,
1000 ng/ml
144 h 0, 24, 48, 72, 144 h
5-FU COLO320DM In vitro 100, 1000 ng/ml 144 h
UFT Colon cancer Oral 60/day 28 days qd 0–14, eod 14–26
[30] LY2157299 Human Calu6 10 Oral Control, 75 bidx20 7–10 6, 10, 13, 17, 20, 24, 26
LY2157299 Human Calu6 36 Oral Control bidx 7–10 Once a week for
one month
LY2157299 Human Calu6 10 Oral 75 bidx10 7–10 4, 10, 14
LY2157299 Human Calu6 10 Oral 75 bidx15 7–10 4, 10, 14, 17, 21
LY2157299 Human Calu6 20 Oral 75 bidx20 7–10 4, 10, 14, 17, 21, 24, 28
LY2157299 Human MX1 10 Oral Control, 75 tidx20 7–10 4, 7, 10, 14, 17,
19, 21, 24, 27, 32
[31] PF02341066 GTL16 Oral
gavage
8.5, 17, 34 9–11
e368 www.drugdiscoverytoday.com

Vol. 10, No. 3 2013 Drug Discovery Today: Technologies | Translational Pharmacology: From Animal to Man and Back
Table 1 (Continued )
Ref Drug Cell line n per
group
Route Dose (mg/kg) Dose
scheme
Start
day
Sampling times (days)
[32] GDC-0941 MCF7.1 10 Oral Control, 12.5, 25,
50, 75, 100, 200
qd (16–21 days) 0, 4, 10, 18, 24,
32, 38 after dose
GDC-0941 MCF7.1 10 Oral Control, 12.5, 25,
37.5, 50, 100
bid (16–21days) 0, 6, 12, 16, 26,
32 after dose
GDC-0941 MCF7.1 10 Oral Control, 200 qd, eod, e3d
(16–21 days)
0, 6, 12, 16, 26, 32,
40 after dose
IV: intravenous; q: every; qd: once a day; q#d: every # days; eod: every other day; bid: twice a day; tid: three times a day; qw: every week; biw: twice a week.
being suitable for the selected modeling technique should be
the recommended way to proceed. This could result in a
reduction in the number of animals involved in the study
and in a more accurate estimate of the model parameters,
In vitro data
Biomarker data
Co
Preclinical tumor gr
Time (h)
% p
Sm
ad
Time (h)
0.001 0.01
1000
10
120
100
80
60
40
20
00 4 8
controls
0.0390625 µM
0.3125 µM
2.5 µM
0.009765625 µM
0.078125 µM
0.625 µM
5 µM
1.25 µM
0.15625 µM
0.01953125 µM
0 24 48 72
105
104
103
102
Nº
of c
ells
(a)
(b)
Sys
tem
ic e
xpos
ure
(mg×
h/L)
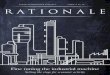
Figure 1. In this cartoon, the application of model-based approaches is proposed
structure of the Simeoni’s tumor growth inhibition model (upper boxes) and the re
anticancer agents (lower graph) is reported [54,55]. At the periphery of the circl
oncology therapeutic area are shown: from bottom left, in clockwise order: model
[30], modeling of combination data in xenograft experiments [29], modeling of t
improving their ability to translate clinically. Indeed, so far,
preclinical studies have been designed without applying
optimal design strategies (some study designs are shown
in Table 1).
mbinations
Clinical tumor growth
Survival
owth
observed
observed
individualprediction
populationprediction
3
2
1
00 7
fitting of single agents
simulation of combinationassuming additivity
14 21 28 35 42 49 56 63
0 7 14 21 28 35 42 49 56 63
90% predicted
Time (arbitrary units)
k2 (L/mg×h)
Time (arbitrary units)
Time (days)
Time (days)
TW
(g)
3
2
1
0
TW
(g)
tum
or w
eigh
t (ar
bitr
ary
units
)
prob
abili
ty o
vera
ll su
rviv
al 1
25
20
15
10
5
00 200 400 600 800 1000
0.75
0.5
0.250.1 1 10
00 0.5 1 1.5 2 2.5 3 3.5 4
Drug Discovery Today: Technologies
in the continuum of oncology drug development. In the central panel, the
lationship between the potency parameter k2 and the clinical dose of known
e, some of the achievements to support the model-based development in
ing of in vitro data [49], modeling of biomarkers connected to tumor growth
umor growth in human patients and prediction of overall survival [60].
www.drugdiscoverytoday.com e369

Drug Discovery Today: Technologies | Translational Pharmacology: From Animal to Man and Back Vol. 10, No. 3 2013
Dose rationale in the clinics
Until a few years ago, the approaches used to anticipate the
clinical dose from the information gained in xenograft mod-
els were very empirical. ‘A new drug should at a minimum
achieve an AUC in humans that equals the effective AUC in
animals’ [53]: this was considered the condition necessary
(but not sufficient) for a new compound to enter into phase
III clinical stage. More recently, it has been shown that the
model-based approach can provide rational quantitative
guidelines based on specific parameters of the mathematical
model estimated in the preclinical experimental model. In
general, the availability of experiment-independent, drug-
specific, model-based parameters is key to translate the pre-
clinical knowledge into the clinical setting [54]. For instance,
a parameter of Simeoni’s model describes the anticancer
potency of a compound [20]. Then, a significant correlation
was found between this potency parameter and the systemic
exposures (area under the drug plasma concentration–time
curve) of well-established anticancer drugs associated with
standard therapies in clinics (see central portion of Fig. 1)
[55]. In drug development, this correlation could anticipate
the dose levels that need to be reached in future clinical
studies to observe a clinical benefit. In fact, for a compound
whose development was interrupted due to lack of efficacy,
we retrospectively found that its maximum tolerated dose
was much lower than the model-predicted clinical dose. This
example suggests that this correlation – besides anticipating
the clinical dose for a new compound – could be used to kill
faster (or, alternatively, minimize the resources for further
development of) a compound with low probability of success.
As already mentioned, the mathematical models of tumor
growth have been recently integrated within mechanism-
based models incorporating the relationship between drug
exposure and biomarkers modulation. This approach,
together with a deeper understanding of the preclinical set-
ting, aims to identify biomarker levels that correlate with
therapeutic response. Referring to the examples previously
quoted, an integrated model may help predict the likelihood
of tumor growth inhibition in humans from the inhibition of
cMet phosphorylation [31], or the extent of suppression of
the PI3K pathway measured by pAkt inhibition [32].
Although such extrapolations assume that the relationship
between PD marker response and antitumor activity is similar
in human and xenograft models, this approach may help find
the appropriate dosing regimen and guide the dose escalation
to rapidly achieve efficacious systemic exposure in the clinic.
Based on the outcome of these integrated preclinical models,
rapid turnaround of the analysis of biomarker modulation
data in the clinical trials can be treated in a more quantitative
manner, defining the path forward for the development of
new anticancer compounds and designing study adaptations
(as the adoption of different dose levels and dosing regimen)
in early clinical trials. In addition, in-target and off-target
e370 www.drugdiscoverytoday.com
effects can be more thoroughly examined and evaluated in
terms of risk–benefit ratio, providing the basis for the assess-
ment of the utility curves of a new compound.
Conclusions
In this brief review we have described what information can
be achieved from the modeling of xenograft data, especially
with regard to the dose rationale to be used in the clinics.
An interesting question is the possibility of extending in
vivo modeling approaches also to the earlier in vitro studies.
Indeed, the possibility of predicting the time course of the
effect may be very helpful both for candidate ranking pur-
poses and the design of experimental protocols in preclinical
species. It has been shown that CDM can be effectively
applied also to in vitro data [30]. At this time, the major open
challenge is demonstrating whether and how in vitro models
could be used to predict results of in vivo studies.
Another area that is booming is the application of models
to combination therapy. Some modeling attempts were
recently reported in the literature [27–29]. The definition
of a general combination model able to predict the inhibition
of the tumor growth curve in response to interacting drugs
given in combination is still an open issue. Although the
main rationale to combine anticancer agents in the clinic is to
obtain better or similar responses in comparison to single
agent therapies but with reduced adverse effects, the integra-
tion of safety and tolerability issues in the mathematical
approaches has still to be realized [56].
Modeling approaches similar to those so far illustrated
within the preclinical setting have also been developed for
describing and, potentially, predicting growth of tumor in
patients. Some of these approaches have been used to gen-
erate hypotheses to be tested in the clinics. For instance, the
Norton–Simon hypothesis [19] indicated that the regression
rate of tumor mass after a chemotherapeutic agent is directly
proportional to the rate of growth for an unperturbed tumor
of that size. This suggested that in clinical practice dose-dense
regimens may be more effective than alternative regimens
and this was demonstrated in two different clinical settings
[57,58]. Tumor growth models are becoming more and more
popular to describe clinical data, for instance in non-small
cell lung cancer patients [59]. In other cases, the tumor
growth models have been used in late clinical phases as
significant covariates for describing relevant clinical end-
points such as overall survival [60]. In other model-based
approaches, markers such as PSA were proposed for modeling
using PKPD approaches [61]: within such models which
consider the potential effect of anticancer agents, these mar-
kers may be also used to assess the potential effect on the
clinical endpoint (e.g. progression-free survival, overall sur-
vival), in turn validating the clinical relevance of the bio-
marker itself. Thus, finding an appropriate, quantitative
translational link between the compound effects in xenograft

Vol. 10, No. 3 2013 Drug Discovery Today: Technologies | Translational Pharmacology: From Animal to Man and Back
experimental models and the corresponding effects of tumor
reduction in the clinical situation, and further resorting to
the approaches linking tumor growth (or, more generally,
intermediate markers of antitumor effects) with survival end-
points would allow to have a full end-to-end description of
the potential development paths of new anticancer treat-
ments.
Oncology is a very active area for the investigation of
model-based approaches: this may be due to the fact that
the mechanisms of tumor generation, development and
spread – although heterogeneous and not fully understood
– are very active areas of basic research. While there are several
model-based approaches available for addressing specific
issues in the oncology therapeutic area, it seems that we
are still moving in the ‘model-aided’ and not in the
‘model-based’ paradigm [62]. The use of the model-based
approach could become more widespread in the presence
of the consensus on behalf of the regulatory authorities. The
new regulatory framework provides recommendations for
nonclinical evaluations supporting the development of antic-
ancer pharmaceuticals [63,64] and recognizes the value of the
model-based approach [65–67]. Consequently new qualifica-
tion pathways for the integration of novel methodologies,
including modeling and simulation have recently been made
available [68]. Indeed model-based drug development
appears particularly suited to integrate in vitro and in vivo,
preclinical and clinical data to allow a better characterization
of new compounds and provide elements for their differen-
tiation from the anticancer drugs already available [62,69]. A
more thorough characterization of the mechanisms of cel-
lular proliferation and metastasis, the adoption of appropri-
ate modeling tools for interpreting the experimental
outcomes and a better understanding of the relationship
between molecular markers and relevant clinical endpoints
can be integrated in a modeling approach centered on tumor
growth modeling (Fig. 1). This approach – discriminating
between the biological system characteristics and drug action
– can pave the way of drug development in the oncology
therapeutic area (Fig. 1).
References1 Liu, M. and Hicklin, D. (2011) Human tumor xenograft efficacy models. In
Tumor Models in Cancer Research, Cancer Drug Discovery and Development
(Teicher, B.A., ed.), Springer Science+Business Media
2 Bonate, P.L. (2011) Modeling tumor growth in oncology. In
Pharmacokinetics in Drug Development (Bonate, P.L. and Howard, D.R.,
eds), American Association of Pharmaceutical Scientists, LLC
3 Della Pasqua, O.E. (2011) PKPD and disease modeling: concepts and
applications to oncology. In Clinical Trial Simulations (Kimko, H.H.C. and
Peck, C.C., eds), AAPS Advances in the Pharmaceutical Sciences Series 1,
Springer Science + Business Media, LLC
4 Woodhouse, D.L. (1947) Chemotherapy investigations in cancer; with
reference to the influence of certain organic dibasic acids, diamino
compounds and nitro compounds on tumors in mice. Cancer Res. 7,
398–401
5 Mattern, J. et al. (1988) Human tumor xenografts as model for drug testing.
Cancer Metastasis Rev. 7, 263–284
6 Rygaard, J. et al. (1969) Heterotransplantation of a human malignant
tumour to the mouse mutant ‘nude’. Acta Pathol. Microbiol. Scand. 77, 758–
760
7 Bissery, M.C. et al. (1996) Experimental antitumor activity and
pharmacokinetics of camptothecin analog irinotecan (CPT-11) in mice.
Anticancer Drugs 7, 437–460
8 Hollingshead, M.G. (2008) Antitumor efficacy testing in rodents. J. Natl.
Cancer Inst. 100, 1500–1510
9 Kelland, L.R. (2004) Of mice and men: values and liabilities of the athymic
nude mouse model in anticancer drug development. Eur. J. Cancer 40, 827–
836
10 Walrath, J.C. et al. (2010) Genetically engineered mouse models in cancer
research. Adv. Cancer Res. 106, 113–164
11 Rocchetti, M. et al. (2005) Pharmacokinetic-pharmacodynamic model for
predicting tumour growth inhibition in mice: a useful tool in oncology
drug development. Basic Clin. Pharmacol. Toxicol. 265–268
12 Voskoglou-Nomikos, T. et al. (2003) Clinical predictive value of the in vitro
cell line, human xenograft, and mouse allograft preclinical cancer models.
Clin. Cancer Res. 9, 4227–4239
13 Marusic, M. (1996) Mathematical models of tumor growth. The Lecture
Presented at the Mathematical Colloquium in Osijek Organized by Croatian
Mathematical Society – Division Osijek, June 7, 1996
14 Laird, A.K. (1964) Dynamics of tumor growth. Br. J. Cancer 18, 490–502
15 Simpson-Herren, and Lloyd, (1970) Kinetic parameter and growth curves
for experimental tumor systems. Cancer Chemotherapy Rep. 54, 143–174
16 Sullivan, P.W. and Salmon, S.E. (1972) Kinetics of tumor growth and
regression in IgG multiple myeloma. J. Clin. Invest. 51, 1697–1708
17 Norton, L. et al. (1976) Predicting the course of Gompertzian growth.
Nature (Lond.) 264, 542–545
18 Norton, L. and Simon, R. (1977) Growth curve of an experimental solid
tumor following radiotherapy. J. Natl. Cancer Inst. (Bethesda) 58, 1735–
1741
19 Simon, R. and Norton, L. (2006) The Norton-Simon hypothesis: designing
more effective and less toxic chemotherapeutic regimens. Nat. Clin. Pract.
Oncol. 3, 406–407
20 Simeoni, M. et al. (2004) Predictive pharmacokinetic–pharmacodynamic
modeling of tumor growth kinetics in xenograft models after
administration of anticancer agents. Cancer Res. 64, 1094–1101
21 Magni, P. et al. (2006) A mathematical model to study the effects of drug
administration on tumor growth dynamics. Math. Biosci. 200, 127–151
22 Lobo, E.D. and Balthasar, J.P. (2002) Pharmacodynamic modeling of
chemotherapeutic effects: application of a transit compartment model to
characterize methotrexate effects in vitro. AAPS PharmSci. 4, E42
23 Yang, J. et al. (2010) Comparison of two pharmacodynamic transduction
models for the analysis of tumor therapeutic responses in model systems.
AAPS J. 12, 1–10
24 Magni, P. et al. (2008) A minimal model of tumor growth inhibition. IEEE
Trans. Biomed. Eng. 55, 2683–2690
25 Jumbe, N.L. et al. (2010) Modeling the efficacy of trastuzumab-DM1, an
antibody drug conjugate, in mice. J. Pharmacokinet. Pharmacodyn. 37, 221–
242
26 Sung, J.H. et al. (2009) A combined pharmacokinetic–pharmacodynamic
(PK–PD) model for tumor growth in the rat with UFT administration. J.
Pharm. Sci. 98, 1885–1904
27 Goteti, K. et al. (2010) Preclinical pharmacokinetic/pharmacodynamic
models to predict synergistic effects of co-administered anti-cancer agents.
J. Cancer Chemother. Pharmacol. 66, 245–254
28 Koch, G. et al. (2009) Modeling of tumor growth and anticancer effects of
combination therapy. J. Pharmacokinet. Pharmacodyn. 36, 179–197
29 Rocchetti, M. et al. (2009) Testing additivity of anticancer agents in pre-
clinical studies: a PK/PD modelling approach. Eur. J. Cancer 45, 3336–3346
30 Bueno, L. et al. (2008) Semi-mechanistic modelling of the tumour growth
inhibitory effects of LY2157299, a new type I receptor TGF-beta kinase
antagonist, in mice. Eur. J. Cancer 44, 142–150
31 Yamazaki, S. et al. (2008) Pharmacokinetic–pharmacodynamic modeling
of biomarker response and tumor growth inhibition to an orally available
www.drugdiscoverytoday.com e371

Drug Discovery Today: Technologies | Translational Pharmacology: From Animal to Man and Back Vol. 10, No. 3 2013
cMet kinase inhibitor in human tumor xenograft mouse models. Drug Met.
Disp. 36, 1267–1274
32 Salphati, L. et al. (2010) Pharmacokinetic–pharmacodynamic modeling of
tumor growth inhibition and biomarker modulation by the novel
phosphatidylinositol 3-kinase inhibitor GDC-0941. Drug Met. Disp. 38,
1436–1442
33 Kalns, J.E. et al. (1995) Design and analysis of in vitro antitumor
pharmacodynamic studies. Cancer Res. 55, 5315–5322
34 Millenbaugh, N.J. et al. (2000) A pharmacodynamic analysis method to
determine the relative importance of drug concentration and treatment
time on effect. Cancer Chemother. Pharmacol. 45, 265–272
35 Germani, M. et al. (2003 Dec) In vitro cell growth pharmacodynamic
studies: a new nonparametric approach to determining the relative
importance of drug concentration and treatment time. Cancer Chemother.
Pharmacol. 52, 507–513
36 Del Bene, F. et al. (2009) A model-based approach to the in vitro evaluation
of anticancer activity. Cancer Chemother. Pharmacol. 63, 827–836
37 Roose, T. et al. (2008) Mathematical models of avascular tumor growth.
SIAM Rev. 49, 179–208
38 Lowengrub, J.S. et al. (2010) Nonlinear modelling of cancer: bridging the
gap between cells and tumours. Nonlinearity 23, R1–R91
39 Byrne, H.M. (2010) Dissecting cancer through mathematics: from the cell
to the animal model. Nat. Rev. Cancer 10, 221–230
40 Owen, M.R. et al. (2004) Mathematical modelling of the use of
macrophages as vehicles for drug delivery to hypoxic tumour sites. J.
Theor. Biol. 226, 377–391
41 Jiang, Y. et al. (2005) A multiscale model for avascular tumor growth.
Biophys. J. 89, 3884–3894 Erratum in: Biophys J. 91(2): 775
42 Ribba, B. et al. (2006) A multiscale mathematical model of avascular tumor
growth to investigate the therapeutic benefit of anti-invasive agents. J.
Theor. Biol. 243, 532–541
43 Ribba, B. et al. (2006) A multiscale mathematical model of cancer, and its
use in analyzing irradiation therapies. J. Theor. Biol. 3, 7
44 Bajzer, Z. et al. (1996) Conceptual frameworks for mathematical modeling
of tumor growth dynamics. Math. Comput. Model. 23, 31–46
45 Bellomo, N. and Preziosi, L. (2000) Modeling and mathematical problems
related to tumor evolution and its interaction with the immune system.
Math. Comput. Model. 32, m413–m452
46 Basse, B. and Ubezio, P. (2007) A Generalised age- and phase-structured
model of human tumour cell populations both unperturbed and exposed
to a range of cancer therapies. Bull. Math. Biol. 69, 1673–1690
47 Wang, Z. et al. (2007) Simulating non-small cell lung cancer with a
multiscale agent-based model. Theor. Biol. Med. Model. 4, 50
48 Zhang, L. et al. (2009) Multiscale agent-based cancer modeling. J. Math.
Biol. 58, 545–559
49 Ribba, B. et al. (2011) A model of vascular tumour growth in mice
combining longitudinal tumour size data with histological biomarkers.
Eur. J. Cancer 47, 479–490
50 Sheiner, L.B. et al. (1977) Estimation of population characteristics of
pharmacokinetic parameters from routine clinical data. J. Pharmacokin.
Pharmacodyn. 5, 445–479
51 Poggesi, I. et al. (2004). Population modeling of tumor growth in untreated
xenografted mice. Abstracts of the Annual Meeting of the Population
e372 www.drugdiscoverytoday.com
Approach Group in Europe, Uppsala PAGE 13, Abstr 535 [http://
www.page-meeting.org/?abstract=535]
52 Simeoni, M. et al. Population modeling of tumor growth inhibition in
vivo: application to anticancer drug development. Abstracts of the Annual
Meeting of the Population Approach Group in Europe, Uppsala PAGE 13,
PAGE 13 (2004) Abstr 503 [http://www.page-meeting.org/?abstract=503]
53 Roberts, T.G. et al. (2003) The phase III trial in the era of targeted therapy:
unraveling the go and no go decision. J. Clin. Oncol. 19, 3683–3695
54 Poggesi, I. et al. (2009) Antitumor efficacytesting in rodents. J. Natl. Cancer
Inst. 101, 1592–1593
55 Rocchetti, M. et al. (2007) Predicting the active doses in humans from
animal studies: a novel approach in oncology. Eur. J. Cancer 12, 1862–1868
56 Ouellet, D. (2010) Benefit–risk assessment: the use of clinical utility index.
Expert Opin. Drug Safety 9, 289–300
57 Bonadonna, G. et al. (2004) Clinical relevance of different sequencing of
doxorubicin and cyclophosphamide, methotrexate and fluorouracil in
operable breast cancer. J. Clin. Oncol. 22, 1614–1620
58 Citron, M.L. et al. (2003) Randomized trial of dose-dense versus
conventionally scheduled and sequential versus concurrent combination
chemotherapy as postoperative adjuvant treatment of node-positive
primary breast cancer: first report of Intergroup trial C9741/Cancer and
Leukemia Group B trial 9741. J. Clin. Oncol. 21, 1431–1439
59 Wang, Y. et al. (2009) Elucidation of relationship between tumor size and
survival in non-small-cell lung cancer patients can aid early decision
making in clinical drug development. Clin. Pharmacol. Ther. 86, 167–174
60 Claret, L. et al. (2009) Model-based prediction of phase III overall survival
in colorectal cancer on the basis of phase II tumor dynamics. J. Clin. Oncol.
27, 4103–4108
61 Hedican, E.B. et al. (2007) Modeling biomarker dynamics with
implications for the treatment of prostate cancer. Comput. Math. Methods
Med. 8, 77–92
62 Zhang, L. et al. (2008) Concepts and challenges in quantitative
pharmacology and model-based drug development. AAPS J. 10, 552–559
63 International Conference on Harmonisation of Technical Requirements
for Registration of Pharmaceuticals for Human Use (ICH). S9 Nonclinical
Evaluation for Anticancer Pharmaceuticals; March 2010
64 Jones, P.S. and Jones, D. (2012) New regulatory framework for cancer drug
development. Drug Discov. Today 17, 227–231
65 US Food and Drug Administration, (2004) Innovation or Stagnation:
Challenge and Opportunity on the Critical Path to New Medical Products. p. 24.
http://www.fda.gov/downloads/ScienceResearch/SpecialTopics/
CriticalPathInitiative/CriticalPathOpportunitiesReports/ucm113411.pdf
66 End-of-phase 2a meetings. FDA guidance for Industry; September 2009
67 European Medicines Agency-European Federation of Pharmaceutical
Industries and Associations modelling and simulation workshop; 30/11/
2011-01/12/2011, London (UK); http://www.ema.europa.eu/ema/
index.jsp?curl=pages/news_and_events/events/2011/07/
event_detail_000440.jsp&mid=WC0b01ac058004d5c3
68 Manolis, E.E. et al. (2011) New pathway for qualification of novel
methodologies in the European Medicines Agency. Proteomics Clin. Appl. 5,
248–255
69 Lalonde, R.L. et al. (2007) Model-based drug development. Clin. Pharmacol.
Ther. 82, 21–32