Embed Size (px)
Citation preview

8/2/2019 Pé e tornozelo - Traumatologia
http://slidepdf.com/reader/full/pe-e-tornozelo-traumatologia 1/29
INTRODUCTION
The foot and ankle act to both support and propel thebody and are well adapted for these roles. During run-ning and jumping, loads well in excess of 10 timesbody weight are transmitted through the ankle and
foot. If this loading is excessive, or excessively repeated, it can lead to foot and ankle injuries.
The ankle is a close-fitting hinge-like joint of whichthe two parts interlock like a mortise (the box formedby the distal ends of the tibia and fibula) and tenon(the upward projecting talus). The mortise bones areheld together as a syndesmosis by the distal (inferior)tibiofibular and interosseous ligaments, and the talusis prevented from slipping out of the mortise by themedial and lateral collateral ligaments and joint cap-sule. The peroneal tendons provide additional stabil-ity.
The ankle moves only in one plane (flexion/extension), but with a complex axis of rotation, actually rolling forward as the talus goes into plantar flexion;sideways movement is prevented by the malleolar but-tresses and the collateral ligaments, but the bony con-straint lessens as the ankle flexes. If the talus is forced totilt or rotate, something must give: the ligaments, themalleoli or both. Movements of the talus into internalor external rotation come about from a rotatory forceupon the foot, or more commonly inversion/supinationof the foot, which, through the orientation of the sub-talar joint, causes external rotation of the talus. When-ever a fracture of the malleolus is seen, it is importantto ask about the associated ligament injury.
ANKLE LIGAMENT INJURIES
Ankle sprains are the most common of all sports-related injuries, accounting for over 25 per cent of cases. They are probably even more common inpedestrians and country walkers who stumble on stair- ways, pavements and potholes.
In more than 75 per cent of cases it is the lateral lig-ament complex that is injured, in particular the ante-rior talofibular and calcaneofibular ligaments. Medialligament injuries are usually associated with a fractureor joint injury.
A sudden twist of the ankle momentarily tenses thestructures around the joint. This may amount to nomore than a painful wrenching of the soft tissues – what is commonly called a sprained ankle . If moresevere force is applied, the ligaments may be strainedto the point of rupture. With a partial tear , most of the ligament remains intact and, once it has healed, itis able to support the weight of the body. With a com-
plete tear , the ligament may still heal but it neverregains its original form and the joint will probably beunstable.
Functional anatomy
The lateral collateral ligaments consist of the anteriortalofibular, the posterior talofibular and (betweenthem) the calcaneofibular ligaments. The anteriortalofibular ligament (ATFL) runs almost horizontally from the anterior edge of the lateral malleolus to theneck of the talus; it is relaxed in dorsiflexion and tensein plantarflexion. In plantarflexion the ligament essen-tially changes its orientation from horizontal withrespect to the floor, to almost vertical. Thus the liga-ment at greatest stretch, and most vulnerable, withthe foot plantar-flexed is the ATFL – hence thepropensity for ATFL injury with the plantar-flexed,
inverting, foot (down a pot-hole, off a kerb, etc). Thecalcaneofibular ligament stretches from the tip of thelateral malleolus to the posterolateral part of the cal-caneum, thus it helps also to stabilize the subtalar joint. Maximum tension is produced by inversion anddorsiflexion of the ankle. The posterior talofibular lig-ament runs from the posterior border of the lateralmalleolus to the posterior part of the talus.
The medial collateral (deltoid) ligament consists of superficial and deep portions. The superficial fibresspread like a fan from the medial malleolus as far
Injuries of the ankleand foot 31Gavin Bowyer

8/2/2019 Pé e tornozelo - Traumatologia
http://slidepdf.com/reader/full/pe-e-tornozelo-traumatologia 2/29
anteriorly as the navicular and inferiorly to the calca-neum and talus. Its chief function is to resist eversionof the hindfoot. The deep portion is intra-articular,running directly from the medial malleolus to themedial surface of the talus. Its principal effect is toprevent external rotation of the talus. The combinedaction of restraining eversion and external rotationmakes the deltoid ligament the major stabilizer of theankle.
The distal tibiofibular joint is held by four ligaments:anterior, posterior, inferior transverse and the interosseous ‘ligament’, which is really a thickened part
of the interosseous membrane. This strong ligamentcomplex still permits some movement at the tibio-fibular joint during flexion and extension of the ankle.
Pathology
The common ‘twisted ankle’ is due to unbalancedloading with the ankle inverted and plantarflexed.First the anterior talofibular and then the calcane-ofibular ligament is strained; sometimes the talocal-caneal ligaments also are injured. If fibres are tornthere is bleeding into the soft tissues. The tip of themalleolus may be avulsed and in some cases the per-oneal tendons are injured. There may be a small frac-ture of an adjacent tarsal bone or (on the lateral side)the base of the fifth metatarsal.
ACUTE INJURY OF LATERAL LIGAMENTS
Clinical features
A history of a twisting injury followed by pain andswelling could suggest anything from a minor sprain
to a fracture. If the patient is able to walk, and bruiing is only faint and slow to appear, it is probably sprain; if bruising is marked and the patient unable tput any weight on the foot, this suggests a morsevere injury. Tenderness is maximal just distal anslightly anterior to the lateral malleolus. The slighteattempt at passive inversion of the ankle is extremepainful. It is impossible to test for abnormal mobili without using local or general anaesthesia.
With all ankle injuries it is essential to examine thentire leg and foot; undisplaced fractures of the fibuor the tarsal bones, or even the fifth metatarsal bon
are easily missed and injuries of the distal tibiofibula joint and the peroneal tendon sheath cause featurthat mimic those of a lateral ligament strain.
Imaging
About 15 per cent of ankle sprains reaching the Emegency Department are associated with an ankle frature. This complication can be excluded by obtaininan x-ray, but there are doubts as to whether apatients with ankle injuries should be subjected tx-ray examination. Almost 2 decades ago The Ottaw
Ankle Rules were developed to assist in making thdecision. X-ray examination is called for if there i(1) pain around the malleolus; (2) inability to tak weight on the ankle immediately after the injur(3) inability to take four steps in the EmergenDepartment; (4) bone tenderness at the posterioedge or tip of the medial or lateral malleolus or thbase of the fifth metatarsal bone.
If x-ray examination is considered necessary, anteroposterior, lateral and ‘mortise’ (30-degree obliqu views of the ankle should be obtained. Localized so
F R A C T U R E S A N D
J O I N T I N
J U R I E S
908
31
(a) (b) (c)
(d) (e) (f)
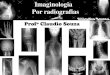
31.1 Ankle ligament injuries(a) Schematic diagram showing thmortise-and-tenon articulation andmain ligaments of the ankle.(b) The three components of thelateral collateral ligament. (c) Thecommonest injury is a partial tear one or other component of the lateral ligament. Following a com-plete tear, the talus may be displaced in the ankle mortise; thetibiofibular ligament may have ruptured as well, shown here insomewhat exaggerated form.(d) Stress x-ray showing talar tilt.(e,f) X-rays demonstrating anteroposterior instability. Pullingthe foot forward under the tibiacauses the talus to shift appreciabat the ankle joint; this is usuallyseen after recurrent sprains.
AnteriortalofibularPosterior
talofibular
Calcaneofibular

8/2/2019 Pé e tornozelo - Traumatologia
http://slidepdf.com/reader/full/pe-e-tornozelo-traumatologia 3/29
tissue swelling and, in some cases, a small avulsionfracture of the tip of the lateral malleolus or the an-terolateral surface of the talus may be the only corrob-orative signs of a lateral ligament injury. However, it isimportant to exclude other injuries, such as an undis-placed fibular fracture or diastasis of the tibiofibular syn-desmosis. If tenderness extends onto the foot, or if swelling is so severe that the area cannot be properly ex-amined, additional x-rays of the foot are essential.
Persistent inability to weightbear over 1 week orlonger should call for re-examination and review of allthe initial ‘negative’ x-rays. For patients who have hadpersistent pain, swelling, instability and impairedfunction over 6 weeks or longer, despite appropriateearly treatment, magnetic resonance imaging (MRI)or computed tomography (CT) will be required toassess the extent of soft tissue injury or subtle bony changes.
Treatment
Initial treatment consists of rest, ice, c ompression andelevation (RICE), which is continued for 1–3 weeksdepending on the severity of the injury and theresponse to treatment. Cold compresses should beapplied for about 20 minutes every 2 hours, and afterany activity that exacerbates the symptoms.
More recently the acronym has been extended to‘PRICE’ by adding protection (crutches, splint orbrace) and still further to ‘PRICER’, adding rehabili-tation (supported return to function). The principlesremain the same – a phased approach, to support theinjured part during the first few weeks and then allow
early mobilization and a supported return to function. An advice leaflet for patients is probably helpful.The use of non-steroidal anti-inflammatory drugs
(NSAIDs) in the acute phase can be helpful, with theusual contraindications and caveats. There is evidencethat in acute injuries topical non-steroidal anti-inflam-matory (NSAI) gels or creams might be as beneficialas oral preparations, probably with a better risk pro-file.
Functional treatment, i.e. ‘protected mobilization’,leads to earlier recovery of all grades of injury – with-out jeopardizing stability – than either rigid immobi-lization or early operative treatment.
OPERATIVE TREATMENTIf the ankle does not start to settle within 1 or 2 weeksof starting RICE, further review and investigation arecalled for. Persistent problems at 12 weeks after injury,despite physiotherapy, may signal the need for opera-tive treatment. Residual complaints of ankle pain andstiffness, a sensation of instability or giving way andintermittent swelling are suggestive of cartilage damage or impinging scar tissue within the ankle. Arthroscopic repair or ligament substitution is now
effective in many cases, allowing a return to full func-tion and sports.
RECURRENT LATERAL INSTABILITY
Recurrent sprains are potentially associated withadded cartilage damage, and warrant careful investi-gation by MRI, arthroscopy and examination under
anaesthesia.
Clinical features
The patient gives a history of a ‘sprained ankle’ thatnever quite seems to recover and is followed by recur-rent ‘giving way’ or a feeling of instability when walk-ing on uneven surfaces. This is said to occur in about20 per cent of cases after acute lateral collateral liga-ment tears (Colville, 1994).
The ankle looks normal and passive movements arefull, however stress tests for abnormal lateral ligament
laxity may show either excessive talar tilting in thesagittal plane or anterior displacement (an anteriordrawer sign) in the coronal plane. In the chronicphase these tests are painless and can be performedeither manually or with the use of special mechanicalstress devices. Both ankles are tested, so as to allow comparison of the abnormal with the normal side.
Talar tilt test With the ankle held in the neutral position,the examiner stabilizes the tibia by grasping the leg with one hand above the ankle; the other hand is thenused to force the heel into maximum inversion. Therange of movement can be estimated clinically and com-
pared with that of the normal ankle. The exact degreeof talar tilt can also be measured by x-rays, which shouldbe taken with the ankles in 30 degrees of internal rota-tion (mortise views); 15 degrees of talar tilt (or 5 degrees more than in the normal ankle) is regarded asabnormal. Inversion laxity suggests injury to both thecalcaneofibular and anterior talofibular ligaments.
Anterior drawer test The patient should be sitting withthe knee flexed to 90 degrees and the ankle in 10degrees of plantarflexion. The lower leg is stabilized with one hand while the other hand forces the patient’sheel forward under the tibia. In a positive test the talus
can be felt sliding forwards and backwards. Theposition of the talus is verified by lateral x-rays; anteriordisplacement of 10 mm (or 5 mm more than on thenormal side) indicates abnormal laxity of the anteriortalofibular ligament. With an isolated tear of theanterior talofibular ligament, the anterior drawer testmay be positive in the absence of abnormal talar tilt.(Note : A positive anterior drawer test can sometimesbe obtained in normal, asymptomatic individuals; thefinding should always be considered in conjunction with other symptoms and signs).

8/2/2019 Pé e tornozelo - Traumatologia
http://slidepdf.com/reader/full/pe-e-tornozelo-traumatologia 4/29
Treatment
Recurrent ‘giving way’ can sometimes be preventedby modifying shoe-wear, raising the outer side of theheel and extending it laterally. More effectively, thesecondary dynamic ankle stabilizers, the peronei, canbe strengthened and brought into play by specificphysiotherapy regimes. Ankle exercises to strengthenthe peroneal muscles are helpful, and a light brace canbe worn during stressful activities.
If, in spite of these measures, the patient continuesto experience mechanical instability (true giving way)during everyday activities, reconstruction of the lat-eral ligament should be considered. More commonly the persisting problem will be functional instability, in which the patient does not trust the ankle, and thereare recurrent episodes in which the patient has rapidly or suddenly to unload the ankle, probably because of
inhibitory feedback from the injured ankle.Most patients with functional instability can be
improved and returned to sport by arthroscopic
debridement of the impinging tissue within the ank joint, followed by physiotherapy.
Various operations for mechanical stabilization adescribed; they fall mainly into two groups: (1) thothat aim to repair or tighten the ligaments, (2) thothat are designed to construct a ‘check-rein’ againthe unstable movement. The Broström–Karlsson oGould operation is an example of the first type: thanterior talofibular and calcaneofibular ligaments arexposed and repaired, usually by an overlapping or ‘double-breasting’ – technique (Karlsson et a1988). In the second type of operation a substituligament is constructed by using peroneus brevis tact as a tenodesis and prevent sudden movements int varus (Chrisman and Snook, 1969). The disadvatages of the non-anatomic reconstructions are ththey sacrifice or partially sacrifice the secondary stablizers, the peroneal tendons.
Postoperatively the ankle is immobilized in eversiofor 2 weeks; a below-knee cast is then applied foanother 4 weeks, during which time the patient ca
F R A C T U R E S A N D
J O I N T I N
J U R I E S
910
31
a
(a) (b)
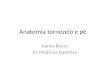
31.3 Recurrent lateral instability – operative treatment (a) The lax anterior talofibular and calcaneofibular ligamentcan be reinforced by a double-breasting technique (the Boström–Karlsson operation). (b) Another way of augmenting thelateral ligament is to re-route part of the peroneus brevis tendon so that is acts as a check-rein (tenodesis) (The Chrisman operation).
(a) (b)
31.2 Recurrent lateral instability – special tests(a) Anterior drawer test : When the heel is drawnforwards under the tibia, the abnormally lax ligamentsallow the talus to displace anteriorly. (b) Talar tilt test :Forcibly inverting the ankle causes the talus to tiltabnormally in the mortise. For both tests comparisonwith the normal side is important.

8/2/2019 Pé e tornozelo - Traumatologia
http://slidepdf.com/reader/full/pe-e-tornozelo-traumatologia 5/29
bear weight. Thereafter, a removable brace is wornand exercises are encouraged. The brace can usually be discarded after 3 months but it may need to beused from time to time for sports activities.
DELTOID LIGAMENT TEARS
Rupture of the deltoid ligament is usually associated
with either a fracture of the distal end of the fibula ortearing of the distal tibiofibular ligaments (or both). Theeffect is to destabilize the talus and allow it to move intoeversion and external rotation. The diagnosis is made by x-ray: there is widening of the medial joint space in themortise view; sometimes the talus is tilted, and diasta-sis of the tibiofibular joint may be obvious.
When there is a deltoid ligament or medial malleo-lar injury but no apparent lateral disruption at theankle, it is important to look for a fracture or disloca-tion of the proximal fibula – the highly unstable Mais- soneuve injury .
Treatment
Provided the medial joint space is completely reduced,the ligament will heal. The fibular fracture or diastasismust be accurately reduced, if necessary by open oper-ation and internal fixation. Occasionally the medial joint space cannot be reduced; it should then beexplored in order to free any soft tissue trapped in the joint. A below-knee cast is applied with the footplantigrade and is retained for 8 weeks.
DISLOCATION OF PERONEAL TENDONS
Acute dislocation of the peroneal tendons may accom-pany – or may be mistaken for – a lateral ligamentstrain. Tell-tale signs on x-ray are an oblique fracture of the lateral malleolus (the so-called ‘rim fracture’) or asmall flake of bone lying lateral to the lateral malleolus(avulsion of the retinaculum). Treatment in a below-knee cast for 6 weeks will help in a proportion of cases;the remainder will complain of residual symptoms.
Recurrent subluxation or dislocation is unmistak-able; the patient can demonstrate that the peroneal
tendons dislocate forwards over the fibula during dor-siflexion and eversion. Treatment is operative and isbased on the observation that the attachment of theretinaculum to the periosteum on the front of thefibula has come adrift, creating a pouch into which thetendons displace. Using non-absorbable suturesthrough drill holes in the bone, the normal anatomy is recreated (Das De and Balasubramaniam, 1985). An alternative approach is to modify the morphology of the distal fibula, posteriorly translating a shelf of bone to constrain the tendons mechanically in a deep-
ened posterior channel. Whichever method of stabi-lization is used, it is important to also assess the stateof the tendons themselves, as an associated longitudi-nal split tear is commonly found, and this will lead tocontinuing pain and dysfunction around the lateralborder of the ankle if it is not repaired.
TEARS OF INFERIOR TIBIOFIBULAR
LIGAMENTS
The inferior tibiofibular ligaments may be torn, allow-
ing partial or complete separation of the tibiofibular joint (diastasis). Complete diastasis, with tearing of both the anterior and posterior fibres, follows a severeabduction strain. Partial diastasis, with tearing of only the anterior fibres, is due to an external rotationforce. These injuries may occur in isolation, but they are usually associated with fractures of the malleoli orrupture of the collateral ligaments.
Clinical features
Following a twisting injury, the patient complains of pain in the front of the ankle. There is swelling and
marked tenderness directly over the inferior tibiofibu-lar joint. A ‘squeeze test’ has been described by Hop-kinson et al. (1990); when the leg is firmly compressedsome way above the ankle, the patient experiences painover the syndesmosis. Be sure, though, to exclude afracture before carrying out the test.
X-ray
With a partial tear the fibula usually lies in its normalposition and the x-ray looks normal. With a complete
(a)
(b)
31.4 Dislocation of peroneal tendons (a) On move-ment of the ankle, the peroneal tendons slip forwards overthe lateral malleolus. (b) The anterior part of the retinacu-lum is being reconstructed.

8/2/2019 Pé e tornozelo - Traumatologia
http://slidepdf.com/reader/full/pe-e-tornozelo-traumatologia 6/29
tear the tibiofibular joint is separated and the anklemortise is widened; sometimes this becomes apparentonly when the ankle is stressed in abduction. Theremay be associated fractures of the distal tibia or fibula,or an isolated fracture more proximally in the fibula.
Treatment
Partial tears can be treated by strapping the ankle
firmly for 2–3 weeks. Thereafter exercises are encour-aged.
Complete tears are best managed by internal fixation with a transverse screw just above the joint. This mustbe done as soon as possible so that the tibiofibularspace does not become clogged with organizinghaematoma and fibrous tissue. If the patient is seenlate and the ankle is painful and unstable, open clear-ance of the syndesmosis and transverse screw fixationmay be warranted. The ankle is immobilized in plasterfor 8 weeks, after which the screw is removed. How-ever, some degree of instability usually persists.
MALLEOLAR FRACTURES OF THEANKLE
Fractures and fracture dislocations of the ankle arecommon. Most are low-energy fractures of one orboth malleoli, usually caused by a twisting mecha-nism. Less common are the more severe fracturesinvolving the tibial plafond, the pilon fractures, which
are high-energy injuries often caused by a fall from aheight.The patient usually presents with a history of a
twisting injury, usually with the ankle going intoinversion, followed by immediate pain, swelling anddifficulty weightbearing. Bruising often comes outsoon after injury.
One such injury was described by Percival Pott in1768, and the group as a whole was for a long timereferred to as Pott’s fracture – although as with many eponyms, he was not the first to notice or describe it,and what became known by this eponym was not what he described anyway!
The most obvious injury is a fracture of one or bothmalleoli; often, though, the ‘invisible’ part of the injury – rupture of one or more ligaments – is just as serious.
Mechanism of injury
The patient stumbles and falls. Usually the foot isanchored to the ground while the body lunges for- ward. The ankle is twisted and the talus tilts and/orrotates forcibly in the mortise, causing a low-energy fracture of one or both malleoli, with or without
associated injuries of the ligaments. If a malleolus pushed off, it usually fractures obliquely; if it is pulleoff, it fractures transversely. The precise fracture patern is determined by: (1) the position of the foo(2) the direction of force at the moment of injurThe foot may be either pronated or supinated and thforce upon the talus is towards adduction, abductioor external rotation, or a combination of these.
Pathological anatomy
There is no completely satisfactory classification oankle fractures. Lauge-Hansen (1950) grouped theinjuries according to the likely position of the foot anthe direction of force at the moment of fracture. This useful as a guide to the method of reductio(reverse the pathological force); it also gives a pointto the associated ligament injuries. However, sompeople find this classification overly complicated. Foa detailed description the reader is referred to thoriginal paper by Lauge-Hansen (1950).
A simpler (perhaps too simple) classification is thof Danis and Weber (Müller et al., 1991), whicfocuses on the fibular fracture. Type A is a transversfracture of the fibula below the tibiofibular syndesmosis, perhaps associated with an oblique or vertical frature of the medial malleolus; this is almost certainly aadduction (or adduction and internal rotation) injurType B is an oblique fracture of the fibula in the sagital plane (and therefore better seen in the lateral xray) at the level of the syndesmosis; often there is alsan avulsion injury on the medial side (a torn deltoiligament or fracture of the medial malleolus). This
probably an external rotation injury and it may bassociated with a tear of the anterior tibiofibular ligment. Type C is a more severe injury, above the levof the syndesmosis, which means that the tibiofibulligament and part of the interosseous membrane muhave been torn. This is due to severe abduction orcombination of abduction and external rotation Associated injuries are an avulsion fracture of tmedial malleolus (or rupture of the medial collaterligament), a posterior malleolar fracture and diastasof the tibiofibular joint.
Clinical features Ankle fractures are seen in skiers, footballers anclimbers; an older group includes women with posmenopausal osteoporosis.
A history of a severe twisting injury, followed bintense pain and inability to stand on the leg suggessomething more serious than a simple sprain. Thankle is swollen and deformity may be obvious. Thsite of tenderness is important; if both the medial anlateral sides are tender, a double injury (bony or ligmentous) must be suspected.
F R A C T U R E S A N D
J O I N T I N
J U R I E S
912
31

8/2/2019 Pé e tornozelo - Traumatologia
http://slidepdf.com/reader/full/pe-e-tornozelo-traumatologia 7/29
X-ray
At least three views are needed: anteroposterior, lat-eral and a 30-degree oblique ‘mortise’ view. The levelof the fibular fracture is often best seen in the lateral view; diastasis may not be appreciated without themortise view. Further x-rays may be needed toexclude a proximal fibular fracture.
From a careful study of the x-rays it should be pos-
sible to reconstruct the mechanism of injury. The fourmost common patterns are shown in Figure 31.5.
Treatment
Swelling is usually rapid and severe, particularly in thehigher energy injuries. If the injury is not dealt with within a few hours, definitive treatment may have tobe deferred for several days while the leg is elevated sothat the swelling can subside; this can be hastened by using a foot pump (which also reduces the risk of deep-vein thrombosis).
Fractures are visible on x-ray; ligaments are not. Always look for clues to the invisible ligament injury – widening of the tibiofibular space, asymmetry of the
talotibial space, widening of the medial joint space, ortilting of the talus – before deciding on a course of action.
Like other intra-articular injuries, ankle fracturesmust be accurately reduced and held if later mechani-cal dysfunction is to be prevented. Persistent displace-ment of the talus, or a step in the articular surface,leads to increased stress and predisposes to secondary osteoarthritis.
In assessing the accuracy of reduction, four objec-tives must be met: (1) the fibula must be restored toits full length; (2) the talus must sit squarely in themortise, with the talar and tibial articular surfaces par-allel; (3) the medial joint space must be restored to itsnormal width, i.e. the same width as the tibio-talarspace (about 4 mm); (4) oblique x-rays must show that there is no tibiofibular diastasis.
Ankle fractures are often unstable. Whatever themethod of reduction and fixation, the position mustbe checked by x-ray during the period of healing.
UNDISPLACED FRACTURESThe first step is to decide whether the injury is stableor unstable. An isolated, undisplaced Danis –Weber
(a) (b) (c) (d)
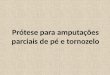
31.5 Ankle fractures – classification The Danis–Weber classification is based on the level of the fibular fracture. (a)Type A – a fibular fracture below the syndesmosis and an oblique fracture of the medial malleolus (caused by forcedsupination and adduction of the foot). (b) Type B – fracture at the syndesmosis, often associated with disruption of theanterior fibres of the tibiofibular ligament and fracture of the posterior and/or medial malleolus, or disruption of themedial ligament (caused by forced supination and external rotation). (c) Type C – a fibular fracture above the syndesmosis;the tibiofibular ligament must be torn, or else (d) the ligament avulses a small piece of the tibia. Here, again, there mustalso be disruption on the medial side of the joint – either a medial malleolar fracture or rupture of the deltoid ligament.

8/2/2019 Pé e tornozelo - Traumatologia
http://slidepdf.com/reader/full/pe-e-tornozelo-traumatologia 8/29
type A fracture is stable and will need minimal splin-tage: a firm bandage or stirrup brace is applied mainly for comfort until the fracture heals.
Undisplaced type B fractures are potentially unstableonly if the tibiofibular ligament is torn or avulsed, orif there is a significant medial-sided injury. X-rays willshow if the syndesmosis or mortise is intact; if it is, abelow-knee cast is applied with the ankle in the neutral (anatomical) position. The plaster may need
to be split and, if so, it must be completed or replaced when swelling has subsided. A check x-ray is taken at2 weeks to confirm that the fracture remains undis-placed. An overboot is fitted and the patient is taught to walk correctly as soon as possible. The cast can usually be discarded after 6–8 weeks. Ankle and footmovements are regained by active exercises when theplaster is removed. As with any lower limb fracture,the leg must not be allowed to dangle idly – it mustbe exercised and elevated.
Undisplaced type C fractures are deceivingly inno-cent-looking but are often accompanied by disruption
of the medial joint structures as well as the tibiofibu-lar syndesmosis and interosseous membrane. Thesedefects may become apparent only when the fracturedisplaces in a cast; arguably, therefore, type C frac-tures are better fixed from the outset.
DISPLACED FRACTURESReduction of these joint disruptions is a prerequisiteto all further treatment; knowledge of the causalmechanism (and this is where the Lauge-Hansen clas-sification is useful) helps to guide the method of
closed reduction. Although internal fixation is usually performed to stabilize the reduction, not all such frac-tures require surgery.
Displaced Weber type A fractures The medial malleolfracture is nearly vertical and after closed reduction often remains unstable; internal fixation of thmalleolar fragment with one or two screws directealmost parallel to the ankle joint is advisable. A perfereduction should be aimed for, with accurarestoration of the tibial articular surface. Loose bonfragments are removed. The lateral malleolar fracturunless it is already perfectly reduced and stable, shoul
be fixed with a plate and screws or tension-ban wiring. Postoperatively a ‘walking cast’ or removabsplintage boot is applied for 6 weeks; the advantage removable splintage is that early physiotherapy can bcommenced.
Displaced Weber type B fractures The most commofracture pattern is a spiral fracture of the fibula and aoblique fracture of the medial malleolus. The causmechanism is external rotation of the ankle when thfoot is caught in a supinated position. Closed reductiotherefore needs traction (to disimpact the fracture) anthen internal rotation of the foot. If closed reductiosucceeds, a cast is applied, following the same routinas for undisplaced fractures. Failure of closed reductio(sometimes a torn medial ligament is caught ibetween the talus and medial malleolus) or laredisplacement calls for operative treatment.
Type B fractures may also be caused by abductionoften the lateral aspect of the fibula is comminuteand the fracture line more horizontal. Despite accurate reduction (the ankle is adducted and the foosupinated), these injuries are unstable and oftepoorly controlled in a cast; internal fixation is therefore preferred.
Displaced Weber type C fractures The fibular fracture well above the syndesmosis and frequently there a
F R A C T U R E S A N D
J O I N T I N
J U R I E S
914
31
(a) (b) (c) (d)
31.6 Ankle fractures – stable or unstable? (a) Stable fracture: in this Danis–Weber type B fracture the tibiofibularsyndesmosis has held; the surfaces of the tibia and talus are precisely parallel and the width of the joint space is regularboth superiorly and medially. (b) Slight subluxation: the syndesmosis is intact but the talus has moved laterally with thedistal fibular fragment; the medial joint space is too wide, signifying a deltoid ligament rupture. It is vital, after reduction othe fibular fracture, to check that the medial joint space is normal; if it is not, the ligament has probably been trapped inthe joint and it must be freed so as to allow perfect re-positioning of the talus. (c) Fracture–dislocation: in this high fibularfracture the syndesmosis has given way, the medial collatoral ligament has been torn and the talus is displaced and tilted.The fibula must be fixed to full length and the tibiofibular joint secured before the ankle can be stabilized. (d) Posterior fracture–dislocation: if the posterior margin of the tibia is fractured, the talus may be displaced upwards. The fragmentmust be replaced and fixed securely.

8/2/2019 Pé e tornozelo - Traumatologia
http://slidepdf.com/reader/full/pe-e-tornozelo-traumatologia 9/29
associated medial and posterior malleolar fragments. An isolated type C fibular fracture should raise strong
suspicions of major ligament damage to thesyndesmosis and medial side of the joint. Almost alltype C fractures are unstable and will need openreduction and internal fixation. The first step is toreduce the fibula, restoring its length and alignment;the fracture is then stabilized using a plate and screws.If there is a medial fracture, this also is fixed. Thesyndesmosis is then checked, using a hook to pull thefibula laterally. If the joint opens out, it means that theligaments are torn; the syndesmosis is stabilized by inserting a transverse screw across from the fibula intothe tibia (the ankle should be held in 10 degrees of
dorsiflexion when the screw is inserted).Fracture subluxations more than 1 or 2 weeks old
may prove difficult to reduce because of clot organi-
zation in the syndesmosis. Granulation tissue shouldbe removed from the syndesmosis and transverse
tibiofibular fixation secured.
Postoperative management After open reduction andfixation of ankle fractures, movements should beregained before applying a below-knee plaster cast, orremovable support boot. The patient is then allowedpartial weightbearing with crutches; the support isretained until the fractures have consolidated (anythingfrom 6–12 weeks).
Management of the syndesmosis- or diastasis-screw remains controversial. Some advocate removal of thescrew when the syndesmosis has healed, and before
weightbearing has commenced (6 weeks is too early,10 weeks is probably more appropriate). Others arehappy to allow early weightbearing with the screw still
(a) (b) (c) (d) (f)
(e)
31.7 Ankle fractures – open treatment (1) (a,b) Danis–Weber type A fractures can often be treated conservatively, butif the medial malleolar fragment involves a large segment of the articular surface, it is best treated by accurate openreduction and internal fixation with one or two screws. (c,d) An unstable fracture–dislocation such as this almost alwaysneeds open reduction and internal fixation. The fibula should be restored to full length and fixed securely; in this case themedial malleolus also needed internal fixation; (e) and (f) show the range of ankle movement a few days after operationand before a ‘walking plaster’ was applied.
(a) (b) (c) (d) (e) (f)
31.8 Ankle fractures with diastasis – open treatment (2) (a) In this type B fracture there is partial disruption of thedistal tibiofibular syndesmosis. Treatment (b) required medial and lateral fixation as well a tibiofibular screw. (c) A type Cfracture must, inevitably, disrupt the tibiofibular ligament; in this case the medial malleolus was intact but the deltoid liga-ment was torn (look at the wider than normal medial joint space). (d) By fixing the fibular fracture and using a tibiofibularscrew, the ankle was completely reduced and it was therefore unnecessary to explore the deltoid ligament. (e) This patientpresented 5 days after his injury; he, too, had a diastasis with disruption of the deltoid ligament (f). In this case thetibiofibular joint as well as the deltoid ligament had to be explored before the ankle could be reduced.

8/2/2019 Pé e tornozelo - Traumatologia
http://slidepdf.com/reader/full/pe-e-tornozelo-traumatologia 10/29
in place, accepting that the screw may break (espe-cially if four cortices are engaged).
OPEN FRACTURESOpen fractures of the ankle pose special problems. If the fracture is not reduced and stabilized at an early stage, it may prove impossible to restore the anatomy.For this reason unstable injuries should be treated by internal fixation even in the presence of an open
wound, provided the soft tissues are not too severely damaged and the wound is not contaminated. If inter-nal fixation seems too risky, an external fixator can beused, often as a temporary spanning option. Treat-ment in other respects follows the principles outlinedin chapter 23.
Complications
EARLYVascular injury With a severe fracture-subluxation thepulses may be obliterated. The ankle should beimmediately reduced and held in a splint untildefinitive treatment has been initiated.
Wound breakdown and infection Diabetic patients areat greater than usual risk of developing wound-edgenecrosis and deep infection. In dealing with displacedfractures, these risks should be carefully weighedagainst the disadvantages of conservative treatment;casts may also cause skin problems if not well paddedand are less effective in preventing malunion.
LATEIncomplete reduction
Incomplete reduction is commonand, unless the talus fits the mortise accurately,degenerative changes may occur. This can sometimesbe prevented by a corrective osteotomy.
Non-union The medial malleolus occasionally fails tounite because a flap of periosteum is interposedbetween it and the tibia. It should be prevented by operative reduction and screw fixation.
Joint stiffness Swelling and stiffness of the ankle areusually the result of neglect in treatment of the softtissues. The patient must walk correctly in plaster and, when the plaster is removed, he or she must, until
circulatory control is regained, wear a crepe bandageand elevate the leg whenever it is not being usedactively. Physiotherapy is always helpful.
Algodystrophy This often follows fractures of the ankle.The patient complains of pain in the foot; there may beswelling and diffuse tenderness, with gradual develop-ment of trophic changes and severe osteoporosis. Man-agement is discussed in Chapter 10.
Osteoarthritis Malunion and/or incomplete reductionmay lead to secondary osteoarthritis of the ankle in
later years. Unless the ankle is unstable, symptoms caoften be managed by judicious analgesic treatment anthe use of firm, comfortable footwear. However, in thlonger term if symptoms become severe arthrodesmay be necessary.
PILON FRACTURES
Unlike the twisting injuries that cause the commoankle fractures, this injury to the ankle joint occu when a large force drives the talus upwards against thtibial plafond, like a pestle (pilon) being struck intomortar. There is considerable damage to the articulcartilage and the subchondral bone may be brokeinto several pieces; in severe cases, the comminutioextends some way up the shaft of the tibia.
Clinical features
There may be little swelling initially but this rapidchanges and fracture blisters are common. The ankmay be deformed or even dislocated; prompt approximate reduction is mandatory.
X-rays
This is a comminuted fracture of the distal end of thtibia, extending into the ankle joint. The fracture ma
F R A C T U R E S A N D
J O I N T I N
J U R I E S
916
31
(a) (b) (c)
(d) (e) (f)
31.9 Pilon fractures – imaging These are either(a) undisplaced (type 1), (b) minimally displaced (type 2);(c) markedly displaced (type 3). CT (d) shows that thereare usually five major tibial fragments: anterolateral (al),anterocentral (ac), anteromedial (am), the medial malleolu(mm) and the posterior fragment (p). These elements arebetter defined by three-dimensional CT reconstruction(e,f).

8/2/2019 Pé e tornozelo - Traumatologia
http://slidepdf.com/reader/full/pe-e-tornozelo-traumatologia 11/29
be classified according to the amount of displacementand comminution (Rüedi and Allgöwer, 1979),though this will usually require accurate definition by CT. Rüedi type 1 is an intra-articular fracture with lit-tle or no displacement of the fragments; in type 2 thereis more severe disruption of the articular surface but without very marked comminution. Type 3 is aseverely comminuted fracture with displacement of the fragments and gross articular irregularity.
In all cases, assessment is far better with CT scan-ning (preferably including three-dimensional recon-
struction) than with plain x-ray examination.
Treatment
The three points of early management of theseinjuries are: span , scan , plan . Staged treatment hasreduced the complication rate in these injuries.
Control of soft tissue swelling is a priority; this isbest achieved either by elevation and applying anexternal fixator across the ankle joint (the spanningexternal fixator, or travelling traction). It may take 2–3 weeks before the soft tissues improve, and fractureblisters can be actively managed rather than hidden
under plaster. Surgery can be planned, based on theCT scan.
Once the skin has recovered, an open reduction andfixation with plates and screws (usually with bonegrafting) may be possible. However, the more severeinjuries (types 2 and 3) do not readily tolerate largesurgical exposures for plating and significant woundbreakdown and infection rates have been reported.Better results have followed wider use of indirectreduction techniques (e.g. applying a bone distractoror utilizing the spanning fixator across the joint to
obtain as much reduction as possible through liga-mentotaxis) and plating through limited exposures.Recently, these injuries have been successfully treatedby using a combination of indirect reduction methodsand small screws to hold the articular fragments, cou-pled with axially stable locking plates. Circular framefixation has also been successful.
The soft-tissue swelling following these injuries issubstantial. After fixation, elevation and early move-ment help to reduce the oedema; arterio-venousimpulse devices applied to the sole of the foot are also
helpful.
(d)
(e)
(a) (b) (c)
31.10 Pilon fracture A 43-year old man suffered a high-energy com-minuted fracture of the distal end of the tibia. (a) Swelling and fractureblisters around the ankle. (b,c) X-rays showing disruption of the meta-physeal–diaphyseal junction in this pilon fracture. (d) Fracture held in anexternal fixator. (e) Fracture blisters were de-roofed and treated withFlamazine (silver sulfadiazine); the skin has re-epithelialized and is free ofinfection 5 days after injury.
(a) (b)
31.11 Same case as 31.10 – Outcome At 3 monthsafter minimal approach reduction and fixation with distallocking plates the fractures have healed and the joint iscongruent and normally aligned.

8/2/2019 Pé e tornozelo - Traumatologia
http://slidepdf.com/reader/full/pe-e-tornozelo-traumatologia 12/29
Outcome
Pilon fractures usually take several months to heal.Postoperatively, physiotherapy is focused on joint
movement and reduction of swelling. There remains,however, a challenging problem with poor functionalresults in these complex fractures, which represent asignificant soft tissue injury as well as bony jigsaw. Although bony union may be achieved, the fate of the joint is decided by the degree of cartilage injury – the‘invisible’ factor on x-rays. Secondary osteoarthritis,stiffness and pain are still frequent late complications.
ANKLE FRACTURES IN CHILDREN
Physeal injuries are quite common in children andalmost a third of these occur around the ankle.
Mechanism of injury
The foot is fixed to the ground or trapped in a creviceand the leg twists to one or the other side. The tibial(or fibular) physis is wrenched apart, usually resultingin a Salter –Harris type 1 or 2 fracture . With severeexternal rotation or abduction the fibula may alsofracture more proximally. The tibial metaphyseal spikemay come off posteriorly, laterally or posteromedially;
its position is determined by the mechanism of injury and suggests the method of reduction. With adduc-tion injuries the tip of the fibula may be avulsed.
Type 3 and 4 fractures are uncommon. They are dueto a supination–adduction force. The epiphysis is split vertically and one piece of the epiphysis (usually themedial part) may be displaced.
Two unusual injuries of the growing ankle are theTillaux fracture and the notorious triplane fracture .The Tillaux fracture is an avulsion of a fragment of tibia by the anterior tibiofibular ligament; in the child
or adolescent this fragment is the lateral part of thepiphysis and the injury is therefore a Salter–Harrtype 3 fracture.
The triplane fracture occurs on the medial side othe tibia and is a combination of Salter–Harris types
F R A C T U R E S A N D
J O I N T I N
J U R I E S
918
31
(a) (b) (c) (d)
31.12 Physeal injuries of the distal tibia The classification suggested by Dias and Tachdjian (1978) has the merit ofpointing to the required reduction manoeuvre – the reverse of the causal mechanism. (a) Supination–inversion: the fibulafracture is usually an avulsion (Salter–Harris type 1) whereas the medial malleolar fracture can be variable. (b) Pronation–eversion–external rotation: the fibular fracture is often high and transverse. (c) Supination–plantarflexion: a fracture of thdistal tibia only (Salter–Harris type 1 or 2) with posterior displacement. (d) Supination–external rotation: an oblique fibulafracture coupled with a fracture of the distal tibia.
31.13 Tillaux fracture Diagramillustrating the elements of thisunusual injury.
(a) (b)
(c) (d)
31.14 Ankle fractures in children (a) Salter–Harris type
2 injury; after reduction (b) growth has proceeded nor-mally. (c) Salter–Harris type 3 injury; (d) the medial side othe physis has fused prematurely, resulting in distortedgrowth.

8/2/2019 Pé e tornozelo - Traumatologia
http://slidepdf.com/reader/full/pe-e-tornozelo-traumatologia 13/29
and 3 injuries. Fracture lines appear in the coronal,sagittal and transverse planes. Injury to the physis may result in either asymmetrical growth or arrestedgrowth.
Clinical features
Following a sprain the ankle is painful, swollen,bruised and acutely tender. There may be an obviousdeformity, but sometimes the injury looks deceptively mild.
Imaging
Undisplaced physeal fractures – especially those in thedistal fibula – are easily missed. Even a hint of physeal widening should be regarded with great suspicion andthe child x-rayed again after 1 week. In an infant thestate of the physis can sometimes only be guessed at,but a few weeks after injury there may be extensiveperiosteal new bone formation.
In triplane fractures the tibial epiphysis may be splitin one plane and the metaphysis in another, thus
making it difficult to see both fractures in the same x-ray. CT scans are particularly helpful in these andother type 3 injuries.
Treatment
Salter–Harris types 1 and 2 injuries are treated closed.If it is displaced, the fracture is gently reduced undergeneral anaesthesia; the limb is immobilized in a full-length cast for 3 weeks and then in a below-knee walking cast for a further 3 weeks. Occasionally, sur-gery is needed to extract a periosteal flap, which pre-
vents an adequate reduction.Type 3 or 4 fractures, if undisplaced, can be treated
in the same manner, but the ankle must be re-x-rayed after 5 days to ensure that the fragments have not slipped. Displaced fractures can sometimes be reducedclosed by reversing the forces that produced theinjury. However, unless reduction is near-perfect, thefracture should be reduced open and fixed with inter-fragmentary screws, which are inserted parallel to thephysis. Postoperatively the leg is immobilized in abelow-knee cast for 6 weeks.
(a) (b) (c) (d)
31.15 Tillaux fracture (a,b) This avulsion fracture of the lateral part of the physis was reduced and fixed percutaneously(c,d).
(a) (b) (c)
31.16 Triplane fracture The three fractureplanes may not be seen in a single x-ray, butcan be visualized from a combination ofimages. In this case the epiphyseal fracture isclearly seen only in the coronal plane CT scan(c).

8/2/2019 Pé e tornozelo - Traumatologia
http://slidepdf.com/reader/full/pe-e-tornozelo-traumatologia 14/29
Tillaux fractures are treated in the same way as type3 fractures. Triplane fractures, if undisplaced, can bemanaged closed but require vigilant monitoring forlate displacement. Displaced fractures must bereduced and fixed.
Complications
Malunion Imperfect reduction may result in angular
deformity of the ankle – usually valgus. In childrenunder 10 years old, mild deformities may beaccommodated by further growth and modelling. Inolder children the deformity should be corrected by asupramalleolar closing-wedge osteotomy.
Asymmetrical growth Fractures through the epiphysis(Salter–Harris type 3 or 4) may result in localizedfusion of the physis. The bony bridge is usually in themedial half of the growth plate; the lateral half goes ongrowing and the distal tibia gradually veers into varus.MRI and CT are helpful in showing precisely wherephyseal arrest has occurred. If the bony bridge is small
(less than 30 per cent of the physeal width) it can beexcised and replaced by a pad of fat in the hope thatphyseal growth may be restored. If more than half of the physis is involved, or the child is near the end of the growth period, a supramalleolar closing-wedgeosteotomy is indicated.
Shortening Early physeal closure occurs in about 2 percent of children with distal tibial injuries. Fortunately the resulting limb length discrepancy is usually mild.If it promises to be more than 2 cm and the child is young enough, proximal tibial epiphysiodesis in theopposite limb may restore equality. If the discrepancy is marked, or the child near the end of the growthperiod, leg lengthening is indicated.
PRINCIPLES IN MANAGING INJURIESOF THE FOOT
Injuries of the foot are apt to be followed by residualsymptoms and loss of function, which seem out of proportion to the initial trauma. Severe injuries affectthe foot as a whole, whatever the particular bone that
might be fractured. A global approach is thereforeessential in dealing with these injuries, the objectivebeing a return to full weightbearing without pain, with an appropriate propulsive gait.
Identification of these injuries is particularly chal-lenging in the patient with multiple trauma, where themore subtle foot injuries might be missed as the life-threatening truncal injuries and limb-threatening longbone injuries distract attention from the more subtleinjuries to the foot, which may nonetheless impaireventual function.
Clinical assessment
The entire foot should be examined systematically, nmatter that the injury may appear to be localized tone spot. Multiple fractures, or combinations of fractures and dislocations, are easily missed. The circulation and nerve supply must be carefully assessed; well-reduced fracture is a useless achievement if thfoot becomes ischaemic or insensitive. Similarly, atten
tion must be paid to the soft tissues and functionmovement of the foot; the stiff, painful foot impaired for propulsion, and maybe even for stance
Fractures and dislocations may cause tenting of thskin; this is always a bad sign because there is a risk oskin necrosis if reduction is delayed.
Imaging
Imaging routinely begins with anteroposterior, laterand oblique x-rays of the foot. If a fracture of the taluor calcaneum, or fracture–dislocation of the midtars joints is suspected then special views may be helpfubut a more rewarding approach is to carry out a Cscan of the foot.
CT is especially useful for evaluating fractures of thcalcaneum, and MRI is helpful in diagnosing osteochondral fractures of the talus. Familiarity with ttalocalcaneal anatomy is essential if fractures of thhindfoot are to be diagnosed properly.
Treatment
Swelling is always a problem. Not only does it makclinical examination difficult, but more importantly
may lead to definitive treatment being delayed; fratures and dislocations are more difficult to reduce inswollen foot. The principles are:
• realign and splint the foot, keep it elevated anapply Cryo-Cuff or ice-packs and intermittenpneumatic compression foot pumps;
F R A C T U R E S A N D
J O I N T I N
J U R I E S
920
31
31.17 Talus and calcaneum The main features of thesetwo bones, and their relationship to each other, are showhere.

8/2/2019 Pé e tornozelo - Traumatologia
http://slidepdf.com/reader/full/pe-e-tornozelo-traumatologia 15/29
• make the diagnosis, defining the extent of injury;• start definitive treatment as soon as the fracture pat-
tern is properly defined and swelling permits.
In the rehabilitation phase, if the foot has to beimmobilized, exercise those joints that can be left free.Start weightbearing as soon as the patient will tolerateit, provided this will not jeopardize the reduction. If aremovable splint will fit the purpose, use it so that
non-weightbearing exercises can be started as soon aspossible. Prolonged immobilization predisposes tostiffness, impaired function, localized osteoporosisand complex regional pain syndrome.
INJURIES OF THE TALUS
Talar fractures and dislocations are relatively uncom-mon. They usually involve considerable violence – caraccidents in which the occupants are thrown against
the resistant frame of the vehicle, falls from a height,or severe wrenching of the ankle. The injuries includefractures of the neck, body, head or bony processes of the talus, dislocations of the talus or the joints aroundthe talus, osteochondral fractures of the superior articular surface, and a variety of chip or avulsion frac-tures.
The significance of the more serious injuries isenhanced by two important facts: (1) the talus is amajor weightbearing structure (the superior articularsurface carries a greater load per unit area than any other bone in the body); (2) it has a vulnerable blood
supply and is a relatively common site for post-trau-matic ischaemic necrosis.
Blood vessels enter the bone from the anterior tib-ial, posterior tibial and peroneal arteries, as well asanastomotic vessels from the surrounding capsule andligaments. The head of the talus is richly supplied by intraosseous vessels. However, the body of the talus issupplied mainly by vessels that enter the talar neck from the tarsal canal and then run retrograde fromdistal to proximal. In fractures of the talar neck these vessels are divided; if the fracture is displaced, the
extraosseous plexus too may be damaged and thebody of the talus is at risk of ischaemia.
Mechanism of injury
Fracture of the talar neck is produced by violenthyperextension of the ankle. The neck of the talus isforced against the anterior edge of the tibia, whichacts like a cleaver. If the force continues, the fractureis displaced and the surrounding joints may sublux ordislocate.
Fracture of the body is usually a compression injury
due to a fall from a height, or an everting force acrossthe body, fracturing the lateral process (the snow-boarders’ fracture). Avulsion fractures are associated with ligament strains around the ankle and hindfoot.
Clinical features
The patient has most commonly been involved in amotor vehicle accident or has fallen from a height.The foot and ankle are painful and swollen; if the frac-ture is displaced, there may be an obvious deformity,or the skin may be tented or split. Tenting is a dan-
gerous sign; if the fracture or dislocation is notpromptly reduced, the skin may slough and become
(a) (b) (c)
(d) (e) (f)
31.18 Injuries of the talus–x-rays (a)Talocalcaneal fracture–dislocation.(b) Undisplaced fracture of the talar neck.(c) Type III fracture of the neck. (d) Displacedfracture of the body of the talus. (e) This fractureof the body was thought to be well reduced;however, in the AP view (f) it is possible to seetwo overlapping outlines, indicating that thefragments are malrotated.

8/2/2019 Pé e tornozelo - Traumatologia
http://slidepdf.com/reader/full/pe-e-tornozelo-traumatologia 16/29
infected. The pulses should be checked and compared with those in the opposite foot.
X-ray
Anteroposterior, lateral and oblique views are essen-tial; CT scanning helps to identify associated injuriesof the ankle and foot. Both malleoli, the ankle mor-tise, the talus and all the adjacent tarsal bones shouldbe carefully assessed. Undisplaced fractures are notalways easy to see, and sometimes even severely dis-placed fractures are missed in the initial assessmentbecause of unfamiliarity with the normal appearance –sad but true.
Classification
Fractures of the neck of the talus These fractures areclassified according to the system devised by Hawkins(1970) and modified by Canale (1978):
• Group I – undisplaced• Group II – displaced (however little) and associated with subluxation or dislocation of the subtalar joint
• Group III – displaced, with dislocation of the body of the talus from the ankle joint
• Type IV – displaced vertical talar neck fracture withassociated talonavicular joint disruption.
Fractures of the head of the talus This is a rare injury;the fracture usually involves the talonavicular joint.
Fractures of the body of the talus These are alsouncommon. The fracture is often displaced and may cause distortion of the talocalcaneal joint. Rotationalmalalignment of the fragments is difficult to diagnoseon plain x-ray examination; the deformity is best visualized by three-dimensional CT reconstruction.
Fractures of the lateral and posterior processes These areusually associated with ankle ligament strains. It is some-times difficult to distinguish between a fracture of theposterior process and a normal os trigonum. A simple ruleis ‘if it’s not causing symptoms it doesn’t really matter’.
Osteochondral fractures Osteochondral fracturesfollowing acute trauma usually occur on the lateral partof the dome of the talus. The diagnosis is often missed
when the patient is first seen and may come to lightonly after CT or MRI scan.
Treatment
The general principles set out on page 920 should beobserved.
UNDISPLACED FRACTURES A split below-knee plaster is applied and, when theswelling has subsided, is replaced by a complete cast
with the foot plantarflexed. Weightbearing is not pemitted for the first 4 weeks; thereafter, the plaster removed, the fracture position is checked by x-ray,new cast is applied and weightbearing is gradualintroduced. Further plaster changes or use of aadjustable splintage boot will allow the foot to bbrought up, slowly, to plantigrade; physiotherapy commenced. At 8–12 weeks the splintage is discardeand function is regained by normal use.
DISPLACED FRACTURES OF THE NECKEven the slightest displacement makes it a type II frature, which needs to be reduced. If the skin is tighreduction becomes urgent because of the risk of sknecrosis. Reduction must be perfect : (1) in order tensure that the subtalar joint is mechanically soun(2) to lessen the chance – or at any rate lessen theffects – of avascular necrosis.
With type II fractures , closed manipulation undgeneral anaesthesia can be tried first. Traction
applied with the ankle in plantarflexion; the foot then steered into inversion or eversion to correct thdisplacement shown on the x-ray. The reduction checked by x-ray; nothing short of ‘anatomic’ acceptable. A below-knee cast is applied (with the foostill in equinus) and this is retained, non-weightbeaing, for 4 weeks. Cast changes after that will allow thfoot to be gradually brought up to plantigrade; however, weightbearing is not permitted until there is evdence of union (8–12 weeks).
F R A C T U R E S A N D
J O I N T I N
J U R I E S
922
31
(a) (b)
(c) (d)
31.19 Fractures of the talus – treatment (a) Thisdisplaced fracture of the body was reduced and fixed witha countersunk screw (b), giving a perfect result. Fracturesof the neck, even if well reduced (c) are still at risk of developing ischaemic necrosis (d).

8/2/2019 Pé e tornozelo - Traumatologia
http://slidepdf.com/reader/full/pe-e-tornozelo-traumatologia 17/29
If closed reduction fails (which it often does), openreduction is essential; indeed, some would say that all type II fractures should be managed by open reduc-tion and internal fixation without attempting closedtreatment. Through an anteromedial incision the frac-ture is exposed and manipulated into position. Wideraccess can be obtained by pre-drilling and thenosteotomizing the medial malleolus; after the talarfracture has been reduced, the malleolar fragment is
fixed back in position with a screw. The position ischecked by x-ray and the fracture is then fixed withtwo K-wires or a lag screw. Postoperatively a below-knee cast is applied; weightbearing is not permitteduntil there are signs of union (8–12 weeks).
Type III fracture–dislocations need urgent openreduction and internal fixation. The approach willdepend on the fracture pattern and position of dis-placed fragments. Osteotomy of the medial malleolusmight help; the malleolus is pre-drilled for screw fixa-tion and osteotomized and retracted distally withoutinjuring the deltoid ligament. This wide exposure is
essential to permit removal of small fragments fromthe ankle joint and perfect reduction of the displacedtalar body under direct vision; even then, it is difficult!The position is checked by x-ray and the fracture isthen fixed securely with screws. If there is the slight-est doubt about the condition of the skin, the woundis left open and delayed primary closure carried out 5days later. Postoperatively the foot is splinted and ele- vated until the swelling subsides; a below-knee cast orsplintage boot is then applied, following the sameroutine as for type II injuries.
DISPLACED FRACTURES OF THE BODYFractures through the body of the talus are usually displaced or comminuted and involve the ankleand/or the talocalcaneal joint; occasionally the frag-ments are completely dislocated.
Minimal displacement can be accepted; a below-knee non-weightbearing cast is applied for 6–8 weeks;this is then replaced by a weightbearing cast foranother 4 weeks.
Horizontal fractures that do not involve the ankleor subtalar joint are treated by closed reduction andcast immobilization (as earlier).
Displaced fractures with dislocation of the adjacent joints should be accurately reduced. In almost all casesopen reduction and internal fixation will be needed. An osteotomy of the medial malleolus is useful foradequate exposure of the talus; the malleolus is pre-drilled before the osteotomy and fixed back into posi-tion after the talar fracture has been dealt with. Theprognosis for these fractures is poor: there is a consid-erable incidence of malunion, joint incongruity, avas-cular necrosis and secondary osteoarthritis of theankle or talocalcaneal joint.
DISPLACED FRACTURES OF THE HEADThe main problem is injury to the talonavicular joint.If the fragments are large enough, open reduction andinternal fixation with screws is the recommendedtreatment. If there is much comminution, it may bebetter simply to excise the smaller fragments. Postop-erative immobilization is the same as for other talarfractures.
FRACTURES OF THE TALAR PROCESSESIf the fragment is large enough, open reduction andfixation with K-wires or small screws is advisable. Tiny fragments are left but can be removed later if they become symptomatic.
OSTEOCHONDRAL FRACTURESThese small surface fractures of the dome of the talususually occur with severe ankle sprains or subtalar dis-locations. Most acute lesions can be treated by castimmobilization for 4–6 weeks. Occasionally a dis-placed fragment is large enough to warrant operative
replacement and internal fixation – easier said thandone! More often it is separated from its bed and isexcised: the exposed bone is then drilled to encouragerepair by fibrocartilage.
OPEN FRACTURESFractures of the talus are often associated with burstskin wounds. In some cases the fracture becomes‘open’ when stretched or tented skin starts sloughing.There is a high risk of infection in these wounds andprophylactic antibiotics are advisable.
The injury is treated as an emergency. Under gen-
eral anaesthesia, the wound is cleaned and debridedand all necrotic tissue is removed. The fracture is thendealt with as for closed injuries, except that the woundis left open and closed by delayed primary suture orskin grafting 5–7 days later, when swelling has sub-sided and it is certain that there is no infection.
Sometimes, in open injuries, the talus is completely detached and lying in the wound. After adequate debridement and cleansing, the talus should be replacedin the mortise and stabilized, if necessary with crossedK-wires. Later definitive fixation is then performed.
Complications
Malunion The importance of accurate reduction hasbeen stressed. Malunion may lead to distortion of the joint surface, limitation of movement and pain on weightbearing. If early follow-up x-rays show re-displacement of the fragments, a further attempt atreduction is justified. Persistent malunion predisposesto osteoarthritis.
Avascular necrosis Avascular necrosis of the body of thetalus occurs in displaced fractures of the talar neck. The

8/2/2019 Pé e tornozelo - Traumatologia
http://slidepdf.com/reader/full/pe-e-tornozelo-traumatologia 18/29
incidence varies with the severity of displacement: intype 1 fractures it is less than 10 per cent; in type 2about 30–40 per cent; and in type 3 more than 90 percent. The earliest x-ray sign (often present by the sixth week) is apparent increased density of the avascularsegment; in reality it is the rest of the tarsus that hasbecome slightly porotic with disuse, but the avascularportion remains unaffected and therefore looks more‘dense’. The opposite is also true: if the dome of the
talus becomes osteoporotic, this means that it has ablood supply and it will not develop osteonecrosis.This is the basis of Hawkins’ sign, which should belooked for 6–8 weeks after injury.
If osteonecrosis does occur, the body of the talus willeventually appear on x-ray to be more dense than thesurrounding bones. Despite necrosis, the fracture may heal, so treatment should not be interrupted by thisevent; if anything, weightbearing should be delayed inthe hope that the bone is not unduly flattened. Func-tion may yet be reasonable. However, if the talus becomes flattened or fragmented, or pain and disabil-
ity are marked, the ankle may need to be arthrodesed.Secondary osteoarthritis Osteoarthritis of the ankleand/or subtalar joints occurs some years after injury inover 50 per cent of patients with talar neck fractures.There are a number of causes: (1) articular damage dueto the initial trauma; (2) malunion and distortion of the articular surface; (3) avascular necrosis of the talus.Pain and stiffness may be managed by judiciousanalgesic medication and orthotic adjustments, but insome cases the painful hindfoot will simply not allow areturn to function; arthrodesis of the affected jointscan help to relieve symptoms. Operative fusion of one
joint may predispose to overload of the associated foot joints, and hence to later arthritis, but this should beaccepted.
FRACTURES OF THE CALCANEUM
The calcaneum is the most commonly fractured tarsalbone, and in 5–10 per cent of cases both heels areinjured simultaneously. Crush injuries, although they always heal in the biological sense, are likely to be fol-lowed by long-term disability. The general attitude tothese injuries at the beginning of the twentieth cen-tury (at least from an industrial point of view) was that“the man who breaks his heel-bone is finished”. This was followed by attempts, throughout the latter partof that century, to modify the outcome through openreduction and internal fixation of these fractures.
Mechanism of injury
In most cases the patient falls from a height, oftenfrom a ladder, onto one or both heels. The calcaneum
is driven up against the talus and is split or crushedOver 20 per cent of these patients suffer associateinjuries of the spine, pelvis or hip.
Avulsion fractures sometimes follow tractinjuries of the tendo Achillis or the ankle ligamentOccasionally the bone is shattered by a direct blow.
Pathological anatomy
Based largely on the work of Palmer (1948) anEssex-Lopresti (1952), it has been customary tdivide calcaneal fractures into extra-articular fractur(those involving the various calcaneal processes or thbody posterior to the talocalcaneal joint) and intrarticular fractures (those that split the talocalcanearticular facet).
EXTRA-ARTICULAR FRACTURESThese account for 25 per cent of calcaneal injurieThey usually follow fairly simple patterns, with sheaing or avulsion of the anterior process, the sustentac
ulum tali, the tuberosity or the inferomedial procesFractures of the posterior (extra-articular) part of thbody are caused by compression. Extra-articular fratures are usually easy to manage and have a gooprognosis.
INTRA-ARTICULAR FRACTURESThese injuries are much more complex and unpredictable in their outcome. They are best understooby imagining the impact of the talus cleaving the bonfrom above to produce a primary fracture line thruns obliquely across the posterior articular facet an
the body from posteromedial to anterolateral. Wherit splits, the posterior articular facet depends upon thposition of the foot at impact: if the heel is in valgu(abducted), the fracture is in the lateral part of thfacet; if the heel is in varus (adducted), the fracture more medial.
The upward displacement of the body of the calca
F R A C T U R E S A N D
J O I N T I N
J U R I E S
924
31
(a) (b)
31.20 Extra-articular fractures of the calcaneum Fractures may occur through (A) the anterior process, (B) thebody, (C) the tuberosity, (D) the sustentaculum tali or (E)the medial tubercle. Treatment is closed unless the frag-ment is large and badly displaced, in which case it willneed to be fixed back in position.

8/2/2019 Pé e tornozelo - Traumatologia
http://slidepdf.com/reader/full/pe-e-tornozelo-traumatologia 19/29
neum produces one of the classic x-ray signs of a ‘de-pressed’ fracture: flattening of the angle subtended by the posterior articular surface and the upper surface of the body posterior to the joint (Böhler’s angle).
The advent of CT, and the trend towards operativereduction and fixation of displaced calcaneal fractures,have sharpened our understanding of these complexinjuries. There are two important ways of assessing orclassifying these injuries that are of relevance to the
treating surgeon (and the patient). The work of Sanders and Gregory (1995) has helped to define theintra-articular fracture pattern and the associated out-come and prognosis. Knowledge of the variations infracture pattern, particularly in relation to the lateral wall of the calcaneum (Eastwood et al., 1993) hasimproved our understanding of the anatomy that islikely to be encountered at operation, approachingfrom an extended L-shaped incision; the lateral jointfragment may sometimes be trapped within the body
of the calcaneum and can only be reduced if the lat-eral wall of the body is osteotomized so as to gainaccess to it (Eastwood et al., 1993).
Clinical features
There is usually a history of a fall from a height, or a roadtraffic accident; in elderly osteoporotic people even acomparatively minor injury may fracture the calcaneum.
The foot is painful and swollen and a large bruiseappears on the lateral aspect of the heel. The heel may look broad and squat. The surrounding tissues arethick and tender, and the normal concavity below thelateral malleolus is lacking. The subtalar joint cannotbe moved but ankle movement is possible.
Always check for signs of a compartment syndromeof the foot (intense pain, very extensive bruising anddiminished sensation, with pain on passive toe move-ment).
(a) (b) (c) (d)
31.21 Intra-articular fractures of the calcaneum The primary fracture line (a,b) is created by the impact of the taluson the calcaneum – it runs from posteromedial to anterolateral. Secondary fracture lines may create ‘tongue’ (c) or ‘joint depression’ (d) variants to the fracture pattern.
(a) (b) (c)
31.22 Intra-articular fractures of the calcaneum CT scans have allowed a better understanding of the fractureanatomy. A coronal CT scan enables the identification of three major fragments in most intra-articular fractures: the lateral joint fragment (L), the sustentaculum tali (S) and the body fragment (B). In type 1 fractures (a) the lateral joint fragment isin valgus whereas the body is in varus. In type 2 fractures (b), the sustentaculum tali is in varus and the lateral joint is elevated in relation to it. In type 3 fractures (c) the lateral joint fragment is impacted and buried within the body fragment(Eastwood et al., 1993).

8/2/2019 Pé e tornozelo - Traumatologia
http://slidepdf.com/reader/full/pe-e-tornozelo-traumatologia 20/29
X-ray
Plain x-rays should include lateral, oblique and axial views. Extra-articular fractures are usually fairly obvious. Intra-articular fractures, also, can often beidentified in the plain films and if there is displacementof the fragments the lateral view may show flattening
of the tuber-joint angle (Böhler’s angle).For accurate definition of intra-articular fractures,CT is essential and three-dimensional reconstruction views even better. Coronal sections will show the frac-ture ‘geometry’ clearly enough to permit accuratediagnosis of most intra-articular fractures (Lowrie etal., 1988).
With severe injuries – and especially with bilateralfractures or in the unconscious patient – it is essential to assess the knees, spine and pelvis as well.
Treatment
For all except the most minor injuries, the patient isadmitted to hospital so that the leg and foot can beelevated and treated with cold (ice or Cryo-Cuff) andcompression until swelling subsides. This also givestime to obtain the necessary CT scans.
EXTRA-ARTICULAR FRACTURESThe byword for the management of extra-articulafractures is ‘mobility and function are more importanthan anatomical repositioning’. The vast majority artreated closed: (1) compression bandaging, ice packand elevation until the swelling subsides; (2) exercisas soon as pain permits; (3) no weightbearing for
weeks and partial weightbearing for another 4 week Variations from this routine relate to specific injurie
Fractures of the anterior process Most of these aavulsion fractures and many are mistaken for an anksprain. Oblique x-rays will show the fracture, whicalmost always involves the calcaneocuboid joint. there is a large displaced fragment, internal fixatiomay be needed; this is followed by the usual ‘closedroutine.
Fractures of the tuberosity These are usually due tavulsion by the tendo Achillis; clinical signs are simil
to those of a torn Achilles tendon. If the fragment displaced, it should be reduced and fixed witcancellous screws; the foot is then immobilized slight equinus to relieve tension on the tendo Achilli Weightbearing can be permitted after 4 weeks.
F R A C T U R E S A N D
J O I N T I N
J U R I E S
926
31
(a) (b) (c)
31.24 Calcaneal fractures –imaging Bilateral calcanealfractures (a,b) are caused by a faon the heels from a height or byan explosion from below. In eithecase the spine also may be
fractured, as it was in this patient(c). With bilateral heel fractures,always x-ray the spine.
(a) (b) (c) (d)
31.23 Fracture of the calcaneum – imaging (a,b) Measurement of Böhler’s angle and the x-ray appearance in a normfoot. (c) Flattening of Böhler’s angle in a fractured calcaneum. (d) The CT scan in this case shows how the articular fragments have been split apart.

8/2/2019 Pé e tornozelo - Traumatologia
http://slidepdf.com/reader/full/pe-e-tornozelo-traumatologia 21/29
Fractures of the body If it is certain that the subtalar joint is not involved, the prognosis is good and thefracture can be treated by the usual ‘closed’ routine.However, if there is much sideways displacement and widening of the heel, closed reduction by manualcompression should be attempted. Weightbearing isavoided for 6–8 weeks; however, cast immobilization isunnecessary except if both heels are fractured or if thepatient simply cannot manage a one-legged gait withcrutches (e.g. those who are elderly or frail).
INTRA-ARTICULAR FRACTURESUndisplaced fractures are treated in much the same way as extra-articular fractures: compression bandag-ing, ice-packs and elevation followed by exercises and
non-weightbearing for 6–8 weeks. As long as verticalstress is avoided, the fracture will not become dis-placed; cast immobilization is therefore unnecessary and it may even be harmful in that it increases the risk of stiffness and algodystrophy. Good or excellentresults can be expected in most patients with undis-placed intra-articular fractures.
Displaced intra-articular fractures are best treatedby open reduction and internal fixation as soon as theswelling subsides. CT has greatly facilitated this
approach; the medial and lateral fragments can beclearly defined and, with suitable drawings or models,the surgical procedure can be carefully planned andrehearsed.
The operation is usually performed through a sin-gle, wide lateral approach; access to the posterior facetand medial fragment is achieved by taking down thelateral aspect of the calcaneum, performing the reduc-tion, and then rebuilding this wall. The various frag-ments are held with interfragmentary screws – bonegrafts are sometimes added to fill in defects. The ante-rior part of the calcaneum and the calcaneocuboid
joint also need attention; the fragments are similarly reduced and fixed. Finally a contoured plate is placedon the lateral aspect of the calcaneum to buttress theentire assembly. The wound is then closed anddrained.
Postoperatively the foot is lightly splinted and ele- vated. Exercises are begun as soon as pain subsidesand after about 2 weeks the patient can be allowed upnon-weightbearing on crutches. Partial weightbearingis permitted only when the fracture has healed (sel-dom before 8 weeks) and full weightbearing about 4 weeks after that. Restoration of function may take 6–12 months.
Outcome
Extra-articular fractures and undisplaced intra-artic- ular fractures , if properly treated, usually have a goodresult. However, the patient should be warned that itmay take 6–12 months before full function isregained, and in about 10 per cent of cases there willbe residual symptoms that might preclude a return totheir previous job if this involved walking on unevensurfaces or balancing on ladders.
(a) (b)
31.25 Extra-articular calcaneal fractures –treatment (a) Avulsion fracture of posterosupe-rior corner (b) fixed by a screw.
(a) (b)
(c) (d)
31.26 Intra-articular calcaneal fracture – treatment(a) X-ray gives limited information, but the CT (b) showsthe severe depression of the posterior calcaneal facet. Thiswas treated operatively with a calcaneal locking plate, toreconstitute the posterior facet (arrow) and restore theheight of the calcaneum (c,d).

8/2/2019 Pé e tornozelo - Traumatologia
http://slidepdf.com/reader/full/pe-e-tornozelo-traumatologia 22/29
The outcome for displaced intra-articular fractures is much less predictable. The results of operative treat-ment are heavily dependent on the severity of the frac-ture and the experience of the surgeon (Buckley et al.,1992; Sanders et al., 1995). The Canadian multi- centre study showed a shorter time off work andlower requirement for subtalar arthrodesis in thosemanaged operatively. Results were particularly favourable with internal fixation in younger men and
those not working with heavy loads or receiving work-men’s compensation. In experienced hands, forselected fractures, this is a rational treatment. How-ever, it is not an enterprise for the tyro and unless theappropriate skills and facilities are available the patientshould be referred to a specializing centre.
Closed treatment, though it may be the only alter-native, has a bad reputation. Crosby and Fitzgibbons(1990), in a follow up of 30 patients who had under-gone closed treatment, found that 50 per cent of those with uncomplicated displaced intra-articularfractures were contemplating having an arthrodesis
within 4 years of injury; only two out of 10 patientshad a ‘good’ result. Those with comminuted fracturesfared even worse: all of them were assessed as havinga poor result.
The fact remains that the heel fracture is a seriousand disabling injury in many patients with heavy orphysically demanding jobs; mechanical reconstructionof the bony anatomy does not necessarily improve thefunctional outcome.
Complications
EARLYSwelling and blistering Intense swelling and blisteringmay jeopardize operative treatment. The limb shouldbe elevated with the minimum of delay.
Compartment syndrome About 10 per cent of patientsdevelop intense pressure symptoms. The risk of a full-blown compartment syndrome can be minimized by starting treatment early. If operative decompression iscarried out, this will delay any definitive procedure forthe fracture.
LATE
Malunion Closed treatment of displaced fractures, orinjudicious weightbearing after open reduction, may result in malunion. The heel is broad and squat , and thepatient has a problem fitting shoes. Usually the foot isin valgus and walking may be impaired.
Peroneal tendon impingement Lateral displacement of the body of the calcaneum may cause painfulcompression of the peroneal tendons against the lateralmalleolus. Treatment consists of operative paring downof protuberant bone on the lateral wall of thecalcaneum.
Insufficiency of the tendo Achillis The loss of heel heighmay result in diminished tendo Achillis action. If thinterferes markedly with walking, subtalar arthrodes with insertion of a bone block may alleviate tproblem.
Talocalcaneal stiffness and osteoarthritis Displaced intrarticular fractures may lead to joint stiffness andeventually, osteoarthritis. This can usually be manage
conservatively but persistent or severe pain manecessitate subtalar arthrodesis. If the calcaneocubo joint is also involved, a triple arthrodesis is better.
MIDTARSAL INJURIES
Injuries in this area vary from minor sprains, ofteincorrectly labelled as ‘ankle’ sprains, to severe frature–dislocations that can threaten the survival of thfoot. The mechanism differs accordingly, from benig
twisting injuries to crushing forces that producsevere soft tissue damage; bleeding into the fascicompartments of the foot may cause a typical compartment syndrome.
Isolated injuries of the navicular, cuneiform ocuboid bones are rare. Fractures in this region shoube assumed to be ‘combination’ fractures or fracturesubluxations, until proved otherwise.
Remember that small flakes of bone on x-ray oftehave large ligaments attached to them, and that ‘midfoot sprain’ (like ‘partial Achilles tendon rupture’) isdangerous diagnosis to make.
Pathological anatomy
The most useful classification is that of Main and Jowe(1975), which is based on the mechanism of injury.
Medial stress injuries are caused by violent inversioof the foot and vary in severity from sprains of thmidtarsal joint to subluxation or fracture–subluxatioof the talonavicular or midtarsal joints.
Longitudinal stress injuries are the most commonThey are caused by a severe longitudinal force witthe foot in plantarflexion. The navicular is compressebetween the cuneiforms and the talus, resulting i
fracture of the navicular and subluxation of the midtarsal joint.
Lateral stress injuries are usually due to falls which the foot is forced into valgus. Injuries includfractures and fracture–subluxations of the cuboid anthe anterior end of the calcaneum as well as avulsioinjuries on the medial side of the foot.
Plantar stress injuries result from falls in which thfoot is twisted and trapped under the body; the usually present as dorsal avulsion injuries or fracturesubluxation of the calcaneocuboid joint.
F R A C T U R E S A N D
J O I N T I N
J U R I E S
928
31

8/2/2019 Pé e tornozelo - Traumatologia
http://slidepdf.com/reader/full/pe-e-tornozelo-traumatologia 23/29
Crush injuries usually cause open comminuted frac-tures of the midtarsal region.
Clinical features
The foot is bruised and swollen. Tenderness is usually diffuse across the midfoot. A medial midtarsal disloca-tion looks like an ‘acute club-foot’ and a lateral dislo-cation produces a valgus deformity; with longitudinalstress injuries there is often no obvious deformity. Any attempt at movement is painful. It is important toexclude distal ischaemia or a compartment syndrome.
X-ray
Multiple views are necessary to determine the extentof the injury; be sure that all the tarsal bones areclearly shown. Tarso-metatarsal dislocation may bemissed if the forefoot falls back into place; fractures of the tarsal bones or bases of the metatarsals shouldalert the surgeon to this possibility. Abnormality of alignment, or fracture, on any view should lead to CTscanning to better assess the extent of injury.
Treatment
Ligamentous strains The foot may be bandaged untilacute pain subsides. Thereafter, movement isencouraged. Be prepared to re-examine and re-x-ray the foot that does not settle within a few weeks.
Undisplaced fractures The foot is elevated to counteractswelling. After 3 or 4 days a below-knee cast or
removeable splintage boot is applied and the patient isallowed up on crutches with limited weightbearing.The plaster is retained for 4–6 weeks.
Displaced fractures An isolated navicular or cuboidfracture is sometimes displaced and, if so, may needopen reduction and screw fixation.
Fracture–dislocation These are severe injuries. Undergeneral anaesthesia, the dislocation can usually bereduced by closed manipulation but holding it is aproblem. If there is the least tendency toredisplacement, percutaneous K-wires are run acrossthe joints to fix them in position.
The foot is immobilized in a below-knee cast for 6–8 weeks. Exercises are then begun and should be prac-tised assiduously; it may be 6–8 months beforefunction is regained.
If accurate reduction cannot be achieved by closed
manipulation, then open reduction and screw fixationis necessary; the importance of anatomical reductioncannot be overemphasized. However, missed fracturesare a lost cause and open reduction will seldomimprove the situation in those who present late (morethan 3 weeks after injury).
Comminuted fractures Severely comminuted fracturesdefy accurate reduction. Attention should be paid tothe soft tissues; there is a risk of ischaemia. The foot issplinted in the best possible position and elevated untilswelling subsides. Early arthrodesis, with restoration of the longitudinal arch, is advisable, with stable fixation
and interpositional bone graft block.
OUTCOME A major problem with midtarsal injuries is the fre-quency with which fractures and dislocations are missedat the first examination, resulting in undertreatmentand a poor outcome. Even with accurate reduction of midtarsal fracture–dislocations, post-traumatic os-teoarthritis may develop and about 50 per cent of pa-tients fail to regain normal function. If symptoms arepersistent and intrusive, arthrodesis may be indicated.
31.28 Midtarsal injuries Reconstructed CT after reduc-tion of a severe tarso-metatarsal injury reveals associatedinjuries of the cuboid and the lateral cuneiform.
(a) (b)
31.27 Midtarsal injuries (a) X-ray showing dislocation ofthe talonaviclar joint. (b) X-ray on another patient show-ing longitudinal compression fracture of the navicularbone and subluxation of the head of the talus. This injuryis often difficult to demonstrate accurately on plain x-ray.

8/2/2019 Pé e tornozelo - Traumatologia
http://slidepdf.com/reader/full/pe-e-tornozelo-traumatologia 24/29
TARSO-METATARSAL INJURIES
The five tarso-metatarsal (TMT) joints form a struc-tural complex that is held intact partly by the inter-digitating joints and partly by the strong ligamentsthat bind the metatarsal bones to each other and tothe tarsal bones of the midfoot.
An appreciation of the anatomy across the TMT
joints is important in understanding these injuries.The second metatarsal base is set into a recess formedby the medial, intermediate and lateral cuneiforms.There is no ligament between the first and secondmetatarsal bases, but the plantar ligament betweensecond metatarsal base and medial cuneiform is shortand thick. In the coronal plane, the second metatarsalbase forms the apex or keystone in the arch.
Dislocation is rare, but important not to miss;twisting and crushing injuries are the usual causes, with the foot buckling or twisting at the midfoot–forefoot junction. The term Lisfranc injury is oftenused for the disruptions that occur at the midfoot–forefoot junction. Classifying these by direction of forefoot dislocation is, however, pointless – it is nei-ther a guide to treatment nor an indication of out-come. These are often high-energy injuries withextensive damage to the whole region of the foot, andsimply to assess the direction of metatarsal displace-ment is to miss the complexity of the injury pattern.
Clinical features
TMT dislocation or fracture–dislocation should
always be suspected in patients with pain and swellingof the foot after high-velocity car accidents and falls.Unfortunately about 20–30 per cent of these injuriesare initially missed. Only with severe injury is there anobvious deformity.
X-rays may be difficult to interpret; somethinlooks wrong but it is often difficult to tell what. A sytematic method for examining the foot x-rays can helto improve the pick-up rate for these injuries. Concentrate on the second and fourth metatarsals in thoblique views: the medial edge of the second shoulbe in line with the medial edge of the seconcuneiform, and the medial edge of the fourth shouline up with the medial side of the cuboid. A true la
eral may show the dorsal displacement of the seconmetatarsal base. If a fracture–dislocation is suspecte(the displacement may reduce spontaneously and nobe immediately detectable), stress views may revethe abnormality, but a CT scan is a more efficient waof showing the extent of injury.
Treatment
The method of treatment depends on the severity othe injury. Undisplaced sprains require cast immoblization for 4–6 weeks. Subluxation or dislocation cal
for accurate reduction. This can often be achieved btraction and manipulation under anaesthesia; the postion is then held with percutaneous K-wires or screwand cast immobilization. The cast is changed after few days when swelling has subsided; the new cast retained, non-weightbearing, for 6–8 weeks. The K wires are then removed and rehabilitation exercisbegun.
If closed reduction fails, open reduction is essentiaThe key to success is the second TMT joint. Througa longitudinal incision, the base of the seconmetatarsal is exposed and the joint manipulated int
position. Reduction of the remaining parts of thtarso-metatarsal articulation will not be too difficulThe bones are fixed with percutaneous K-wires oscrews and the foot is immobilized as describe earlier.
F R A C T U R E S A N D
J O I N T I N
J U R I E S
930
31
(a) (b) (c) (d)
31.29 TMT injuries (a) Dislocation of the TMT joints. (b) X-ray after reduction and stabilization with K-wires. (c) X-rayshowing a high-energy fracture–dislocation involving the TMT joints. These are serious injuries that may be complicated b(d) compartment syndrome of the foot.

8/2/2019 Pé e tornozelo - Traumatologia
http://slidepdf.com/reader/full/pe-e-tornozelo-traumatologia 25/29
Complications
Compartment syndrome A tensely swollen foot may hide a serious compartment syndrome that could resultin ischaemic contractures. If this is suspected, intra-compartmental pressures should be measured (seeChapter 23). Treatment should be prompt and effec-tive: through a medial longitudinal incision, or two well-spaced dorsal incisions, all the compartments can
be decompressed; the wound is left open until swellingsubsides and the skin can be closed without tension.
INJURIES OF METATARSAL BONES
Metatarsal fractures are relatively common and are of four types: (1) crush fractures due to a direct blow;(2) a spiral fracture of the shaft due to a twistinginjury; (3) avulsion fractures due to ligament strains;(4) insufficiency fractures due to repetitive stress.
Clinical features
In acute injuries pain, swelling and bruising of thefoot are usually quite marked; with stress fractures,the symptoms and signs are more insidious.
X-rays should include routine anteroposterior, lat-eral and oblique views of the entire foot; multipleinjuries are not uncommon. Undisplaced fracturesmay be difficult to detect and stress fractures usually show nothing at all until several weeks later.
TreatmentTreatment will depend on the type of fracture, the siteof injury and the degree of displacement.
UNDISPLACED AND MINIMALLY DISPLACEDFRACTURESThese can be treated by support in a below-knee castor removable boot splint; the foot is elevated and
active movements are started immediately, partial weightbearing for about 4–6 weeks. At the end of thatperiod, exercise is very important and the patient isencouraged to resume normal activity. Slight malu-nion rarely results in disability once mobility has beenregained.
DISPLACED FRACTURESDisplaced fractures can usually be treated closed. The
foot is elevated until swelling subsides. The fracturemay be reduced by traction under anaesthesia and theleg immobilized in a cast – non-weightbearing – for 4 weeks. Alternatively the fracture position might beaccepted, depending on the degree of displacement.For the second to fifth metatarsals, displacement inthe coronal plane can be accepted and closed treat-ment, as above, is satisfactory. However, for the firstmetatarsal and for all fractures with significant dis-placement in the sagittal plane (i.e. depression or ele- vation of the displaced fragment) open reduction andinternal fixation with K-wires, or better with stable
fixation using a plate and small screws, is advisable. A below-knee cast is applied and weightbearing isavoided for 3 weeks; this is then replaced by a weight-bearing cast for another 4 weeks.
Fractures of the metatarsal neck have a tendency todisplace, or re-displace, with closed immobilization. Itis therefore important to check the position repeat-edly if closed treatment is used. If the fracture isunstable, it may be possible to maintain the positionby percutaneous K-wire or screw fixation. The wire isremoved after 4 weeks; cast immobilization is retainedfor 4–6 weeks.
FRACTURES OF THE FIFTH METATARSAL
BASE
Forced inversion of the foot (the ‘pot-hole injury’)may cause avulsion of the base of the fifth metatarsal, with pull-off by the peroneus brevis tendon or the
(a) (b) (c) (d)
31.30 Metatarsal injuries(a) Transverse fractures of threemetatarsal shafts. (b) Avulsionfracture of the base of the fifth
metatarsal – the pot-hole injury,or Robert Jones fracture.(c) Florid callus in a stressfracture of the secondmetatarsal. (d) Jones’ fractureof the fifth metatarsal.

8/2/2019 Pé e tornozelo - Traumatologia
http://slidepdf.com/reader/full/pe-e-tornozelo-traumatologia 26/29
lateral band of the plantar fascia. Pain due to asprained ankle may overshadow pain in the foot.Examination will disclose a point of tendernessdirectly over the prominence at the base of the fifthmetatarsal bone.
A careful assessment of the fracture pattern will pro- vide a guide to prognosis and treatment. Again, an ap-preciation of the patho-anatomy explains these factors.
The fifth metatarsal base extends much more prox-
imal into the midfoot region, compared to the othermetatarsal bases. It articulates with the cuboid and with the fourth metatarsal. The peroneus brevis ten-don and lateral band of the plantar fascia insert ontothe base of the fifth metatarsal. There is a relative watershed in the blood supply to the fifth metatarsalat the junction between the diaphysis and metaphysis.
Robert Jones, a founding father and doyen of orthopaedics, described his own fracture (sustained whilst dancing), as a fracture of the fifth metatarsalabout three-fourths of an inch from its base. Unfor-tunately, as observed above with Pott’s fractures, what
has passed into history as this eponymous fracture isoften not what was actually described, and the term‘Jones fracture’ is now sometimes used for any frac-ture of the proximal fifth metatarsal. A more usefulclassification system takes account of the fracture line,and whether it is proximal, affecting the tuberosity, inthe region of articulation with the fourth metatarsal,or at the metaphyseal/diaphyseal junction – the latterhas a higher rate of non-union, probably as a conse-quence of the relatively poor blood supply in thatregion.
Occasionally a normal peroneal ossicle in this area
may be mistaken for a fracture; there is also anapophyseal ossification centre in the tuberosity.
Treatment
The proximal avulsion fractures can usually be treatedsymptomatically, with initial rest and support, but with early mobilization and return to function.
The intra-articular injuries and those at the meta-physeal–diaphyseal junction may also be treated non-operatively, but there is a greater risk of non-unionand slower return to function. The role of fixation with an interfragmentary screw or screws and plate is
therefore an issue for discussion between the surgeonand the patient, depending to a large extent on thepatient’s functional demands and expectations withrespect to sport, activity, and time away from these.
STRESS INJURY (MARCH FRACTURE)
In a young adult (often a military recruit or a nurse)the foot may become painful and slightly swollen afteroveruse. A tender lump is palpable just distal to the
midshaft of a metatarsal bone. Usually the seconmetatarsal is affected, especially if it is much longethan an ‘atavistic’ first metatarsal. The x-ray appeaance may at first be normal but a radioisotope sca will show an area of intense activity in the bone. Latea hairline crack may be visible and later still (4– weeks) a mass of callus is seen.
Unaccountable pain in elderly osteoporotic peopmay be due to the same lesion; x-ray diagnosis is mor
difficult because callus is minimal and there may be nmore than a fine linear periosteal reaction along thmetatarsal. If osteoporosis has not already been diagnosed, then this should be considered and assesse with bone densitometry.
Metatarsal pain after forefoot surgery may also bdue to stress fractures of the adjacent metatarsals, consequence of redistributed stresses in the foot.
No displacement occurs and neither reduction nosplintage is necessary. The forefoot may be supporte with an elastic bandage and normal walking is encouaged.
INJURIES OFMETATARSOPHALANGEAL JOINTS
Sprains and dislocations of the metatarsophalange(MTP) joints are common in dancers and athletes. simple sprain requires no more than light splintinstrapping a lesser toe (second to fifth) to its neighboufor a week or two is the easiest way. If the toe is di
located, it should be reduced by traction and manipulation; the foot is then protected in a short walkincast for a few weeks.
FRACTURED TOES
A heavy object falling on the toes may fracture phlanges. If the skin is broken it must be covered withsterile dressing, and antibiotics are given; a contamnated wound will require formal surgical washout anexploration. The fracture is disregarded and th
patient encouraged to walk in a supportive boot oshoe. If pain is marked, the toe may be splinted bstrapping it to its neighbour for 2–3 weeks.
FRACTURED SESAMOIDS
One of the sesamoids (usually the medial) may frature from either a direct injury (landing from a heighon the ball of the foot) or sudden traction; chroni
F R A C T U R E S A N D
J O I N T I N
J U R I E S
932
31

8/2/2019 Pé e tornozelo - Traumatologia
http://slidepdf.com/reader/full/pe-e-tornozelo-traumatologia 27/29
repetitive stress is more often seen in dancers and runners.
The patient complains of pain directly over thesesamoid. There is a tender spot in the same area andsometimes pain can be exacerbated by passively hyper-extending the big toe. X-rays will usually show thefracture (which must be distinguished from a smooth-edged bipartite sesamoid).
Treatment is often unnecessary, though a local
injection of lignocaine helps for pain. If discomfort ismarked, the foot can be supported in a removableboot/splint for 2–3 weeks. An insole with differentialpadding or cut-out under the sesamoid might alsospeed a return to sporting activities. Occasionally,intractable symptoms call for excision of the offendingossicle; care should be taken not to disrupt the flexorattachment to the proximal phalanx as this may resultin great toe deformity.
REFERENCES AND FURTHER READING
Ajis A, Younger AS, Maffulli N. Anatomic repair for
chronic lateral ankle instability. Foot Ankle Clin 2006; 11:
539–45.
Bajammal S, Tornetta P 3rd, Sanders D, Bhandari M.
Displaced intra-articular calcaneal fractures. J Orthop
Trauma 2005; 19: 360–4.
Blauth M, Bastian L, Krettek C, Knop C, Evans S. Surgical
options for the treatment of severe tibial pilon fractures: a
study of three techniques. J Orthop Trauma 2001; 15:
153–60.
Bosse MJ, McCarthy ML, Jones AL et al . Lower Extrem-
ity Assessment Project (LEAP) Study Group. The insen-
sate foot following severe lower extremity trauma: an
indication for amputation? J Bone Joint Surg 2005; 87A:
2601–8.
Broström L. Sprained ankles. Surgical treatment of
‘chronic’ ligament ruptures. Acta Chir Scand 1966; 132:
551–65.
Buckley R, Tough S, McCormack R et al . Operative com-
pared with nonoperative treatment of displaced intra-
articular calcaneal fractures: a prospective, randomized,
controlled multicenter trial. J Bone Joint Surg 2002; 84A:
1733–44.
Canale ST, Kelly FB Jr. Fractures of the neck of the talus.
Long-term evaluation of seventy-one cases. J Bone Joint
Surg 1978; 60A: 143–56.
Chrisman OD, Snook GA. Reconstruction of lateral liga-
ment tears of the ankle: an experimental study and clini-
cal evaluation of seven patients treated by a new
modification of the Elmslie procedure. J Bone Joint Surg
1969; 51A: 904–12.
Clare MP, Sanders RW. Preoperative considerations in ankle
replacement surgery. Foot Ankle Clin 2002; 7: 709–20.
Coetzee JC, Ly TV. Treatment of primarily ligamentous Lis-
franc joint injuries: primary arthrodesis compared with
open reduction and internal fixation. Surgical technique.
J Bone Joint Surg 2007; 89A(Suppl 2 Pt 1): 122–7.
Coetzee JC. Making sense of Lisfranc injuries. Foot Ankle
Clin 2008; 13: 695–704.
Colville MR. Reconstruction of the lateral ankle ligaments.
J Bone Joint Surg 1994; 76A: 1092–102.
Crosby LA, Fitzgibbons T. Intra-articular calcaneal frac-
tures: Results of closed treatment. Clin Orthop 1993;
290: 46–54.
Das De S, Balasubramaniam P. A repair operation forrecurrent dislocation of the peroneal tendons. J Bone
Joint Surg 1985; 67B: 585–7.
Dattani R, Patnaik S, Kantak A, Srikanth B, Selvan TP.
Injuries to the tibiofibular syndesmosis. J Bone Joint Surg
2008; 90B: 405–10.
Dias LS, Tachdjian MO. Physeal injuries of the ankle in
children. Clinical Orthopaedics and Related Research
1978; 136: 230.
Eastwood DM, Gregg PJ, Atkins RM. Intra-articular frac-
tures of the calcaneum. Part 1: Pathological anatomy and
classification. J Bone Joint Surg 1993; 75B: 183–8.
Eastwood DM, Langkamer VG, Atkins RM. Intra- articular fractures of the calcaneum. Part 2: Open reduc-
tion and internal fixation by the extended lateral
transcalcaneal approach. J Bone Joint Surg 1993; 75B:
189–95.
Egol KA, Wolinsky P, Koval KJ. Open reduction and inter-
nal fixation of tibial pilon fractures. Foot Ankle Clin 2000;
5: 873–85.
Eiff M, Smith A, Smith G. Early mobilization versus immo-
bilization in the treatment of lateral ankle sprains. Am J
Sports Med 1994; 22: 83–8.
Espinosa N, Smerek JP, Myerson MS. Acute and chronic
syndesmosis injuries: pathomechanisms, diagnosis and
management. Foot Ankle Clin 2006; 11: 639–57.
Essex-Lopresti P. The mechanism, reduction technique and
results in fractures of the os calcis. Br J Surg 1952; 39:
395–419.
Goel DP, Buckley R, deVries G, Abelseth G, Ni A, Gray R.
Prophylaxis of deep-vein thrombosis in fractures below
the knee: a prospective randomised controlled trial.
J Bone Joint Surg 2009; 91B: 388–94.
Harris AM, Patterson BM, Sontich JK, Vallier HA. Results
and outcomes after operative treatment of high-
energy tibial plafond fractures. Foot Ankle Int 2006; 27:
256–65.
Hawkins LG. Fractures of the neck of the talus. J Bone Joint Surg 1970; 52A: 991–1002.
Helfet DL, Koval K, Pappas J, Sanders RW, DiPasquale
T. Intraarticular ‘pilon’ fracture of the tibia. Clin Orthop
Relat Res 1994; 298: 221–8.
Hopkinson WJ, St Pierre P, Ryan JB et al . Syndesmosis
sprains of the ankle. Foot Ankle 1990; 10: 325.
Karlsson J, Bergsten T, Lansinger O, Peterson L.
Reconstruction of the lateral ligaments of the ankle for
chronic-lateral instability. J Bone Joint Surg 1988; 70A:
581–588.

8/2/2019 Pé e tornozelo - Traumatologia
http://slidepdf.com/reader/full/pe-e-tornozelo-traumatologia 28/29
Konradsen L, Homer P, Sondergaard L. Early mobiliza-
tion treatment for grade III ankle ligament injuries. Foot
Ankle 1992; 12: 69–73.
Kuo RS, Tejwani NC, Digiovanni CW et al . Outcome after
open reduction and internal fixation of Lisfranc joint
injuries. J Bone Joint Surg Am 2000; 82A: 1609–18.
Langdon IJ, Kerr PS, Atkins RM. Fractures of the calca-
neum: the anterolateral fragment. J Bone Joint Surg 1994;
76B: 303–5.
Lauge-Hansen N. Fractures of the ankle. II. Combinedexperimental-surgical and experimental-roentgenologic
investigations. Arch Surg 1950; 60: 957–85.
Li X, Killie H, Guerrero P, Busconi BD. Anatomical recon-
struction for chronic lateral ankle instability in the high-
demand athlete: functional outcomes after the modified
Broström repair using suture anchors. Am J Sports Med
2009; 37: 488–94.
Lowrie IG, Finlay DB, Brenkel IJ, Gregg PJ. Computerised
tomographic assessment of the subtalar joint in calcaneal
fractures. J Bone Joint Surg Am 1988; 70B: 247–50.
Main BJ, Jowett RL. Injuries of the midtarsal joint. J Bone
Joint Surg 1975; 57B: 89–97.Michelson JD. Ankle fractures resulting from rotational
injuries. J Am Acad Orthop Surg 2003; 11: 403–12.
Muller ME, Allgöwer M, Schneider R, Willeneger H.
Manual of Internal Fixation . (3rd edition) Springer,
Berlin, 1991, pp 598–600.
Nunn T, Baird C, Robertson D, Gray I, Gregori A. Fitness
to drive in a below knee plaster? An evidence based
response. Injury 2007; 38: 1305–07.
Palmer I. The mechanism and treatment of fractures of the
calcaneus. J Bone Joint Surg 1948; 30A: 2–8.
Papadokostakis G, Kontakis G, Giannoudis P, Hadji-
pavlou A. External fixation devices in the treatment of
fractures of the tibial plafond: a systematic review of the
literature. J Bone Joint Surg Br 2008; 90: 1–6.
Pearse EO, Klass B, Bendall SP. The ‘ABC’ of examining
foot radiographs. Ann R Coll Surg Engl 2005; 87: 449–51.
Philbin T, Rosenberg G, Sferra JJ. Complications of
missed or untreated Lisfranc injuries. Foot Ankle Clin
2003; 8: 61–71.
Porter DA. Evaluation and treatment of ankle syndesmosis
injuries. Instr Course Lect 2009; 58: 575–81.
Quill GE Jr. Fractures of the proximal fifth metatarsa
Orthop Clin North Am 1995; 26: 353–61.
Rammelt S, Heineck J, Zwipp H. Metatarsal fracture
Injury 2004; 35(Suppl 2): SB77–86.
Ruedi TP, Allgöwer M. The operative treatment of intr
articular fractures of the lower end of the tibia. Cl
Orthop 1979; 138: 105–10.
Sanders R, Gregory P. Operative treatment of intra-artic
lar fractures of the calcaneus. Orthop Clin N Am 199
26: 203–14.Schnetzler KA, Hoernschemeyer D. The pediatric triplan
ankle fracture. J Am Acad Orthop Surg 2007; 15: 738
47.
Sirkin M, Sanders R, DiPasquale T, Herscovici D Jr.
staged protocol for soft tissue management in the trea
ment of complex pilon fractures. J Orthop Trauma 199
13: 78–84.
Sirkin MS. Plating of tibial pilon fractures. Am J Orth
2007; 36(Suppl 2): 13–17.
SooHoo NF, Krenek L, Eagan MJ, Gurbani B, Ko CY
Zingmond DS. Complication rates following ope
reduction and internal fixation of ankle fractures. J Bo Joint Surg 2009; 91A: 1042–9.
Tarkin IS, Clare MP, Marcantonio A, Pape HC. An upda
on the management of high-energy pilon fracture
Injury 2008; 39: 142–54.
Teeny SM, Wiss DA. Open reduction and internal fixatio
of tibial plafond fractures. Clin Orthop 1993; 292: 108
17.
Tezval M, Dumont C, Stürmer KM. Prognostic reliabili
of the Hawkins sign in fractures of the talus. J Orth
Trauma 2007; 21: 538–43.
Thordarson DB. Complications after treatment of tibi
pilon fractures: prevention and management strategie
J Am Acad Orthop Surg 2000; 8: 253–65.
Vallier HA, Nork SE, Barei DP, Benirschke SK, Sang
orzan BJ. Talar neck fractures: results and outcome
J Bone Joint Surg 2004; 86A: 1616–24.
Vander Griend R, Michelson JD, Bone LB. Fractures
the ankle and distal part of the tibia. J Bone Joint Su
1996; 78A: 1772–83.
Weinfeld SB, Haddad SL, Myerson MS. Metatarsal stre
fractures. Clin Sports Med 1997; 16: 319–38.
F R A C T U R E S A N D
J O I N T I N
J U R I E S
934
31

8/2/2019 Pé e tornozelo - Traumatologia
http://slidepdf.com/reader/full/pe-e-tornozelo-traumatologia 29/29
Textbooks tend to project an idealised version of themedical world: they assume, for a start, that there is adoctor, or at least a qualified medical attendant, and ahospital or clinic where patients can be examined andtreated as prescribed on the printed page; that basicequipment such as x-ray machines and CT scannersare accessible; that there are facilities for essential lab-oratory investigations; that the recommended drugs
and surgical implants are available; that the environ-ment is clean if not actually sterile; that a variety of operations can be performed and that an appropriatelevel of postoperative care will be applied.
It is right that a book such as this should teach whatis considered to be ‘best practice’ at the time of writ-ing. However, we should also recognise that for themajority of people in the world these high standardsare out of reach and compromises have to be made atevery level of healthcare provision.
It is beyond the scope of this book to discuss waysof improving conditions in disadvantaged countries.
Here we simply offer a brief reminder of what exists inthe wider world.
GLOBAL DISTRIBUTION OF RESOURCESModern orthopaedic surgery is expensive by virtue of the equipment and hospital facilities required and thetraining of surgeons and allied medical staff. Table 1shows the disparities among a number of representa-tive countries in terms of per capita expenditure onhealth per year, the number of doctors per hundredthousand population and Gross Domestic Product(GDP). The situation in poorer countries threatens tobe made even worse by the migration of doctors to
relatively richer countries that offer better workingfacilities, economic benefits and living conditions.
GENERAL EFFECTS OF POVERTY ANDMALNUTRITIONPoverty is linked to malnutrition, which contributesto reduced immune function and increased suscepti-bility to infection – including osteomyelitis, septicarthritis and tuberculosis of bones and joints The
Cases such as the one shown in Figure 1 are rarely seen in affluent countries.
Specific nutritional deficiencies also take their tolland conditions such as calcium deficiency rickets andscurvy, seldom seen in affluent countries, are notuncommon in Africa.
EFFECTS OF THE HIV PANDEMICHIV infection rates are unusually high in some parts of the world, particularly in Africa. The virus causes a de-
Epilogue –Global Orthopaedics
GDP per Per capita Doctors/ capita in total 1000US$ expenditure population
on health inUS$
Malawi 10,600 2, 58 0.02
Egypt 4,200 2,258 0.54
China 7,800 2,277 1.06
Thailand 9,200 2,293 0.37
Mexico 10,700 2,655 1.98
Mauritius 13,700 2,516 1.06
Latvia 16,000 2,852 3.01
Kuwait 23,100 2,538 1.53
New Zealand 26,200 2,081 2.37
UK 31,800 2,560 2.30
USA 43,800 6,096 2.56
Table 1 Variation in health expenditure and numberof doctors compared to GDP
Christopher Lavy, Felicity Briggs