Embed Size (px)
Citation preview

CASE REPORT
Primary pulmonary Ewing’s sarcoma: report of a case
Yoshinobu Ichiki • Akira Nagashima •
Yasuhiro Chikaishi • Manabu Yasuda •
Ichiro Yamamoto • Satoshi Toyoshima
Received: 16 May 2011 / Accepted: 25 July 2011 / Published online: 7 April 2012
� Springer 2012
Abstract The Ewing’s sarcoma family of tumors has
been reported to originate in a variety of sites, most com-
monly in the extremities. We herein describe a rare case of
primary pulmonary Ewing’s sarcoma in a patient with a
family history of sarcoma. The patient was a 42-year-old
male, who presented with hemoptysis. Chest radiographs
revealed a pulmonary mass in the right lower lobe. Clinical
and radiological examinations (computed tomography and
positron emission tomography) revealed that the lesion was
a primary lesion. The lesion was resected by right lower
lobectomy. The tumor was located in the pulmonary
parenchyma, and there was no evidence of an extrapul-
monary involvement by the tumor. Histologically, the
tumor was composed of uniform cells with round nuclei
and scant cytoplasm which were arranged in cohesive
lobules with rare pseudorosette formation. Immunohisto-
chemically, the tumor cells were positive for CD99, and
negative for epithelial markers, neuroendocrine markers,
myogenic markers and lymphoma markers. This diagnosis
was further supported by the cytogenic and reverse trans-
criptase-polymerase chain reaction findings of EWS/FLI-1
fusion transcripts. This demonstrated the presence of a very
rare primary pulmonary Ewing’s sarcoma. The patient was
treated with chemotherapy after the operation because
Ewing’s sarcoma is an aggressive neoplasm. The patient
has had no recurrent disease for 6 months after the
operation.
Keywords Lung cancer � Ewing’s sarcoma
Abbreviations
ESFT Ewing’s sarcoma family of tumors
PNET Primitive neuroectodermal tumors
PET Positron emission tomography
CT Computed tomography,
FDG 8F-fluorodeoxyglucose
CEA Carcinoembryonic antigen,
SCC Squamous cell carcinoma related antigen
TBLB Transbronchial lung biopsy
RT-PCR Reverse transcriptase-polymerase chain reaction
SUV Standard uptake value
Introduction
The Ewing’s sarcoma family of tumors (ESFT) incorpo-
rates both the well-recognized primary bone and the
extraskeletal soft tissue sarcomas. Primitive neuroectoder-
mal tumors (PNET) and ESFT have a similar neural phe-
notype and can, therefore, be considered the same entity. A
common genetic translocation involving chromosome 22
links these tumors with the most prevalent being t(11; 22)
(q24; q12), which occurs in approximately 85 % of cases
[1]. First described in 1921 by American pathologist James
Ewing, Ewing’s sarcomas are neuroectodermal tumors
characterized by monotonous small round cells that are
arranged in sheets on histological examination. Although
Ewing’s sarcoma presenting with a lytic bone lesion is, in
itself, uncommon, it is recognized as the second most
prevalent primary bone tumor worldwide [1].
Cases of primary pulmonary ESFT have been reported
in recent years, but there are still only a few reports in the
literature. To date, only 10 cases of primary pulmonary
Y. Ichiki (&) � A. Nagashima � Y. Chikaishi � M. Yasuda �I. Yamamoto � S. Toyoshima
Department of Chest Surgery and Pathology,
Kitakyushu Municipal Medical Center,
2-1-1 Bashaku, Kokurakita-ku, Kitakyushu 802-0077, Japan
e-mail: [email protected]
123
Surg Today (2012) 42:812–815
DOI 10.1007/s00595-012-0170-4

ESFT have been reported. We herein discuss both the
clinical course and the therapeutic management of this
disease and the associated family history.
Case report
The patient was a 42-year-old male who was admitted to
our hospital because of hemoptysis. His past history was
noncontributory, but his family history was notable. His
brother had undergone amputation of the right wrist
because of synovial sarcoma. Chest radiographs of the
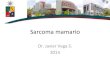
patient revealed a right lower lobe mass. Computed
tomography (CT) disclosed a well-circumscribed and
homogeneous mass measuring 3.9 9 2.6 cm with slight
lobulation in segment 9 of the right lower lobe of the lung
(Fig. 1). A positron emission tomography (PET) with 18F-
fluorodeoxyglucose (FDG) scan showed increased FDG
uptake (maximal standard uptake value 3.2) without any
other abnormal uptake. As a result, the lesion seemed to be
a primary malignant tumor of the lung. None of the serum
tumor markers, including carcinoembryonic antigen
(CEA), squamous cell carcinoma related antigen (SCC),
Cyfra, NSE and proGRP, was elevated.
The patient underwent the bronchoscopy, then a trans-
bronchial lung biopsy (TBLB) and washing cytology were
performed. However, no malignant cells were detected.
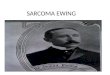
The lesion was resected by a right lower lobectomy. The
tumor was 3.6 9 3.0 9 2.5 cm in size. The tumor was
located in the pulmonary parenchyma, and there was no
evidence of an extrapulmonary involvement by the tumor
(Fig. 2). The cut surface was well-demarcated, and showed
a lobulated configuration with a yellowish area remaining
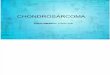
in the periphery of the tumor. Histologically, the tumor was
composed of uniform cells with round nuclei and scant
cytoplasm which were arranged in cohesive lobules with
rare pseudorosette formation (Fig. 3a). Immunohistoche-
mially, the tumor was positive for CD99 (Fig. 3b), but
negative for epithelial markers (cytokeratin AE1/AE2,
EMA), neuroendocrine markers (chromogranin A, synap-
tophysin), myogenic markers (desmin, a-SMA) and lym-
phoma markers (LCA, CD3, CD20, CD79a, CD30). This
diagnosis was further supported by the cytogenic and
reverse transcriptase-polymerase chain reaction (RT-PCR)
to detect ESFT-associated chimeric mRNA (data not
shown). After the operation, the patient was treated with
adjuvant chemotherapy including doxorubicin, vincristine,
ifosfamide, etoposide and cyclophosphamide. The courses
of adjuvant chemotherapy have been and will be admin-
istered every 3 weeks for a total of 17 courses. The planned
duration of adjuvant chemotherapy is 49 weeks. The
patient has demonstrated no recurrent disease for 6 months
after the operation.
Comment
A ESFT is an uncommon malignant neoplasm. The tumors
in this family share a common histological feature of clo-
sely packed small primitive round cells. ESFT most fre-
quently arises in the bones, followed by the soft tissue, but
they have also rarely been reported at other sites [2, 3]. The
pathological diagnosis of ESFT used to require standard
light and electron microscopy, looking for small, round,
blue cells with abundant glycogen and absent cytoplasmic
filaments [4]. Because of the lack of any specific mor-
phological features, the misdiagnosis rate was high due to
the lack of a diagnostic histopathology. Now, with the
advent of specific staining and genomic techniques, we are
able to confidently identify ESFT that displays the
same immunohistochemical and molecular features. CD99
Fig. 1 A chest computed tomography scan of the patient revealed a
solitary intrapulmonary mass in the right lower lobe
Fig. 2 The cut surface of the lobectomy specimen revealed a
medullary tumor with necrotic or hemorrhagic foci confined to the
pulmonary parenchyma
Surg Today (2012) 42:812–815 813
123

staining reveals the MIC2 gene product, which presents a
cell-surface glycoprotein p30/32mic2, and has recently been
used in the evaluation of the EWS family, although it is not
entirely specific for this family [5–7].
The biological role of the MIC2 gene product is
unknown so far, and the structural analysis of the MIC2
gene and protein has not yet provided any clues as to its
molecular function. However, it seems dangerous to rely
solely on immunopositivity for MIC2, and a complete
absence of positive staining for both epithelial and neuro-
endocrine makers made the diagnosis of EWS likely, since
tumors positive for MIC2 are usually negative for those
markers. A characteristic reciprocal cytogenetic transloca-
tion t(11; 22)(q24;q12) is also shared with members of the
ESFT. This translocation results in a hybrid gene product
between the EWS gene located on the long arm of
chromosome 22 and the FL-1 gene on the long arm of
chromosome 11, which can be detected by RT-PCR.
The first case of primary ESFT of the lung was reported
in 1989 by Hammer and colleagues and was described by
Takahashi et al. [8]. Eleven cases, including this case, have
been reported in total since then. A review of the literature
revealed a male preponderance with a mean subject age of
30.4 (ranging from 8 to 67) [8, 9]. Combinations of ther-
apy, including surgery with chemotherapy, with or without
radiotherapy, have been performed. Out of the patients
with available data, five patients survived without recurrent
disease for eight to twenty-four months after the surgery.
All five patients had undergone surgery and chemotherapy.
Four patients died, all within 2 years after the surgery, and
two of these had undergone surgery alone [10].
Extraskeletal Ewing’s sarcoma is potentially curable.
The disease-free survival rates have been increased sig-
nificantly by management with aggressive surgical resec-
tion in combination with multi-agent chemotherapy, with
or without radiotherapy [9]. The treatment of choice is an
early surgical removal, with intensive chemotherapy and
radiation therapy to ablate any residual microscopic dis-
ease. The 5-year disease-free survival rate is estimated to
be 60–70 % for localized disease managed with multi-
agent chemotherapy and surgical resection [10]. Unfortu-
nately, the outcomes have not yet improved for patients
with metastasis or recurrent disease; the 5-year survival
rates remain less than 25 % [11].
We have herein presented a rare example of primary
pulmonary Ewing’s sarcoma, which was suggested by a
combination of microscopic and immunohistochemical
studies, and was confirmed by a genetic analysis, disclosing
the existence of EWS/FLI-1 fusion transcripts. In 85 % of
cases, the gene fusion is a result of a translocation between
EWS and FLI1 (11q24), and in 5–10 % of cases it is a
result of a translocation between EWS and ERG (21q22)
[12]. We, therefore, used primers for EWS–FLI1 and
EWS-ERG. EWS–FLI1 was detected by RT-PCR, but
EWS-ERG was not. It is important to note that extraskel-
etal Ewing’s sarcoma is recognized as a potential cause of a
pulmonary mass. The optimal treatment of primary pul-
monary ESFT has not yet been clearly established. How-
ever, adjuvant and/or neoadjuvant chemotherapy may thus
be able to improve the treatment outcome.
In this case, the maximal standard uptake value (SUV)
of FDG PET was 3.2. The value of the delayed phase of
SUV was not measured. This value might indicate the
possibility that it was due to inflammatory changes, but
malignancy was nevertheless suspected. Therefore, a sur-
gical resection was performed. The value is compatible
with that of a previous study of Ewing’s sarcoma (SUV of
4.5 ± 2.79). In the diagnosis of Ewing’s sarcoma, a FDG
PET scan is not diagnostic, but the sensitivity and speci-
ficity of the examination are quite high, with values of 96
and 78 %, respectively [13].
Fig. 3 a The histopathological findings of hematoxylin–eosin stained
sections revealed small round neoplastic cells with rare pseudorosette
formation. b Immunostaining for CD99 revealed tumor cells q
strongly linear surface staining
814 Surg Today (2012) 42:812–815
123

Interestingly, the brother of this patient had a synovial
sarcoma of the right wrist. A detailed family history of
malignant disease for patients with sarcoma including
ESFT is particularly important because an array of many
types of malignant diseases may be present. Hereditary
syndromes associated with ESFT were reported and a large
number of different transcriptions were identified [14].
Although germline mutations have been identified as cau-
sal for the expression of malignant disease in only a limited
number of these disorders, when such a mutation is present,
it provides the essential requirement for integrating the
sarcoma into a hereditary cancer syndrome of concern.
However, a major problem is that sarcomas are exceed-
ingly rare, and this problem is coupled with the fact that the
compilation of a sufficiently detailed family history of
malignant disease has often been ignored. Consequently, it
is exceedingly difficult to discern which patients/families
may be candidates for germline testing.
Acknowledgments We would like to thank Professor Hiroshi
Hashimoto and his colleagues in the Department of Pathology, School
of Medicine, University of Occupational and Environmental Health
for their detailed genetic analysis.
Conflict of interest Yoshinobu Ichiki and co-authors have no
conflict of interest to report.
References
1. Bernstein M, Kovar H, Paulussen M, Randall RL, Schuck A, Teot
LA, et al. Ewing’s sarcoma family of tumors: current manage-
ment. Oncologist. 2006;11:503–11.
2. Tsuji S, Hisaoka M, Morimitsu Y, Hashimoto H, Jimi A,
Watanabe J, et al. Peripheral primitive neuroectodermal tumour
of the lung: report of two cases. Histopathology. 1998;33:369–74.
3. Rud NP, Reiman HM, Pritchard DJ, Frassica FJ, Smithson WA.
Extraosseous Ewing’s sarcoma. A study of 42 cases. Cancer. 1989;
64:1548–53.
4. Triche TJ, Askin FB. Neuroblastoma and the differential diagnosis
of small-round-, blue-cell tumors. Hum Pathol. 1983;14:569–95.
5. Dei Tos AP, Wadden C, Calonje E, Sciot R, Pauwels P, Knight
JC, et al. Immunohistochemical demonstration of glycoprotein
p30/32 MIC (CD99) in synovial sarcoma. A potential cause of
diagnostic confusion. Appl. Immunohistochem. 1995;3:168–73.
6. Fellinger EJ, Garin-Chesa P, Triche TJ, Huvos AG, Retting WJ.
Immunohistochemical analysis of Ewing’s sarcoma cell surface
antigen p30/32 MIC2. Am J Pathol. 1991;139:317–25.
7. Lumadue JA, Askin FB, Perlman EJ. MIC2 analysis of small cell
carcinoma. Am J Clin Pathol. 1994;102:692–4.
8. Takahashi D, Nagayama J, Nagatoshi Y, Inagaki J, Nishiyama K,
Yokoyama R, et al. Primary Ewing’s sarcoma family tumors of
the lung—a case report and review of the literature. Jpn J Clin
Oncol. 2007;37:874–7.
9. Hancom K, Sharma A, Shackcloth M. Case report-thoracic on-
cologic Primary extraskeletal Ewing’s sarcoma of the lung.
Interact Cardiovasc Thorac Surg. 2010;10:803–4.
10. Raney RB, Asmar L, Newton WA Jr, Bagwell C, Breneman JC,
Crist W, et al. Ewing’s sarcoma of soft tissues in childhood: a
report from the Intergroup Rhabdomyosarcoma Study, 1972 to
1991. J Clin Oncol. 1997;15:574–82.
11. Cotterill SJ, Ahrens S, Paulussen M, Jurgens HF, Voute PA, Gadner
H, et al. Prognostic factors in Ewing’s tumor of bone: analysis of
975 patients from the European Intergroup Cooperative Ewing’s
Sarcoma Study Group. J Clin Oncol. 2000;18:3108–14.
12. Zucman J, Melot T, Desmaze C, Ghysdael J, Plougastel B, Peter
M, et al. Combinatorial generation of variable fusion protein in
the Ewing family of tumours. EMBOJ. 1993;12:4481–7.
13. Gyorke T, Zajic T, Lange A, Schafer O, Moser E, Mako E, et al.
Impact of FDG PET for staging of Ewing sarcoma and primitive
neuroectodermal tumours. Nucl Med Commun. 2006;27:17–24.
14. Arvand A, Denny CT. Biology of EWS/ETS fusions in Ewing’s
family tumors. Oncogene. 2001;20:5747–54.
Surg Today (2012) 42:812–815 815
123