-
7/25/2019 Pulp Revascularization in Immature Permanent Tooth
With Apical Periodontitis Using MTA
1/6
Case ReportPulp Revascularization in Immature Permanent Tooth
with
Apical Periodontitis Using Mineral Trioxide Aggregate
Katsura Saeki,1Yuko Fujita,1Yasuhiro Shiono,1 Yasuhiro
Morimoto,2 and Kenshi Maki1
Department of Pediatric Dentistry, Kyushu Dental University, --
Manazuru, Kokurakita-ku, Kitakyushu -, Japan Department of Oral
Diagnostic Science, Kyushu Dental University, Kitakyushu -,
Japan
Correspondence should be addressed to Kenshi Maki;
[email protected]
Received February ; Revised April ; Accepted April ; Published
May
Academic Editor: Jukka H. Meurman
Copyright Katsura Saeki et al. Tis is an open access article
distributed under the Creative Commons Attribution License,which
permits unrestricted use, distribution, and reproduction in any
medium, provided the original work is properly cited.
Mineral trioxide aggregate (MA) is a material that has been used
worldwide in several clinical applications, such as apical
barriersin teeth with immature apices, repair o root perorations,
root-end lling, pulp capping, and pulpotomy. Te purpose o thiscase
report was to describe successul revascularization treatment o an
immature mandibular right second premolar with apicalperiodontitis
in a -year-old emale patient. Afer preparing an access cavity
without anesthesia, the tooth was isolated using arubber dam and
accessed. Te canal was gently debrided using % sodium hypochlorite
(NaOCl) and % hydrogen peroxideirrigant. And then MA was packed
into the canal. X-ray photographic examination showed the dentin
bridge months aferthe revascularization procedure. Tickening o the
canal wall and complete apical closure were conrmed months afer
the
treatment. In this case, MA showed clinical and radiographic
success at revascularization treatment in immature permanenttooth.
Te successul outcome o this case suggests that MA is reliable and
effective or endodontic treatment in the pediatricdentistry.
1. Introduction
Immature permanent teeth with apical periodontitis or anabscess
are generally treated by apexication []. However,revascularization
procedures have recently been recom-mended to treat immature
permanent teeth with necroticpulp tissue and/or apical
periodontitis or an abscess.
Mineral trioxide aggregate (MA) is a material used
worldwide in a variety o clinical applications, such as anapical
barrier or teeth with immature apices, repair o rootperorations,
root-end lling, pulp capping, and pulpotomyprocedures []. In this
paper successul revascularizationtreatment o an immature mandibular
right second premolarwith apical periodontitis in a -year-old
patient using MAwas described.
2. Case Report
In June , a -year-old Japanese girl was reerred to privateclinic
by a general dentist or detailed examination o agingival abscess in
the mandibular right second premolar.
Te medical history o the patient was unremarkable, andthere was
no relevant amily history o medical or dentalabnormalities. An
extraoral examination revealed swelling inthe buccal region and the
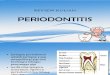
patient complained o spontaneouspain. Furthermore, an intraoral
examination revealed a gin-gival abscess in the region o the
mandibular right secondpremolar (Figure (a)). Te percussion test
was positive.
Radiographic ndings showed enlargement o the peri-
odontal ligament space, along with extensive radiolucencyin the
periradicular region in the area o the mandibularright second
premolar as compared with the mandibular lefsecond premolar
(Figures(b)and(c)). Te pulp vitality testwas negative. Te clinical
diagnosis was acute periradicularperiodontitis o the mandibular
right second premolar withpulpal necrosis.
Te patient underwent oral surgery at Kyushu Den-tal University
Hospital. Te reason or hospitalization wasbecause she was not able
to eat orgingival swelling andspon-taneous pain. During
hospitalization, she received an intra-
venous drip containing an antibiotic. She lef the hospital days
later andwas reerred to our clinic. Postsurgery intraoral
Hindawi Publishing CorporationCase Reports in MedicineVolume
2014, Article ID 564908, 5
pageshttp://dx.doi.org/10.1155/2014/564908
http://dx.doi.org/10.1155/2014/564908http://dx.doi.org/10.1155/2014/564908
-
7/25/2019 Pulp Revascularization in Immature Permanent Tooth
With Apical Periodontitis Using MTA
2/6
Case Reports in Medicine
(a) (b)
(c)
F : (a) Preoperative intraoral photograph showing a gingival
abscess in the mandibular right second premolar. (b) Panoramic
X-rayshowing extensive radiolucency in the periradicular region in
the mandibular right second premolar compared with the mandibular
lefsecond premolar. (c) X-ray showing an immature open apex and
enlargement o the periodontal ligament space and extensive
radiolucencyin the periradicular region in the mandibular right
second premolar.
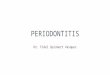
examination showed no abnormalities on the gingiva o
themandibular right second premolar (Figure (a)). However,the talon
cusp o the mandibular right second premolar wasractured (Figure
(b)). Without using anesthetic, the toothwas isolated with a rubber
dam and accessed. Upon enteringthe coronal aspect o the root canal,
hemorrhaging into thepulp chamber was observed (Figure (c)). A le o
K sizewas inserted into the canal. Te length o le is mm.And the
patient reported discomort, indicating potentialsurvival o residual
vital pulp tissue. Te hemorrhaging inthe coronal portion o the
canal was gently irrigated; thenthe area was debrided using . mL o
% sodium hypochlo-rite (NaOCl) and . mL o % hydrogen peroxide [,
].No instrumentation was perormed. Next, MA (Pro-RootMA, Dentsply
Sankin, ochigi, Japan) was packed into the
canal using MAP system (Dentsply Sankin, ochigi, Japan)(Figure
(d)) and the access cavity was closed with glass-ionomer cement
(Fuji IX GP, GC, okyo, Japan). An X-rayobtained afer the procedure
conrmed MA placement inthe canal (Figure (e)).
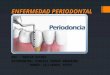
Six months later, an intraoral examination showed
noabnormalities in the gingiva o the mandibular right sec-ond
premolar (Figure (a)), while an X-ray photographicevaluation showed
ormation o a dentin bridge in themandibular right second premolar
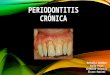
(Figures(b)and (c)).en months later, an intraoral examination
showed noabnormalities o the gingiva in the mandibular right
secondpremolar (Figure (a)), and X-ray images revealed ormation
o a dentin bridge and thickening o the canal walls in
themandibular right second premolar (Figures(b)and(c)).
We think it is important to ollow up this tooth, but shehad
moved. It is too ar or her to reer to our clinic. So wecould not
ollow up her.
3. Discussion
Apexogenesis is done is in immature teeth when part o thepulp
tissue inside the root canal remains vital and apparentlyhealthy.
Tis procedure allows continued physiological devel-opment and
ormation o the root end.
In cases with an immature root with a large apicaloramen, pulp
inection associated with an apical lesion does
not always indicate pulp necrosis, as seen in our patient,likely
because the pulp at this stage is vital enough andhas extremely
high healing ability. Tose procedures havebeen shown to result in
increased thickening o the canalwalls by deposition o hard tissue
and encourage continuedroot development in affected immature
permanent teeth[]. Continued root development o revascularizationo
immature permanent necrotic teeth depends on whetherHertwigs
epithelial sheath survives in cases o apical
peri-odontitis/abscess. Hertwigs epithelial sheath has
importantrole in root development and shape and may be involved
inregulation o the differentiation o periodontal ligament stemcells
with the ormation o cementum.
-
7/25/2019 Pulp Revascularization in Immature Permanent Tooth
With Apical Periodontitis Using MTA
3/6
Case Reports in Medicine
(a) (b)
(c) (d) (e)
F : (a) Intraoral photograph showing no abnormalities o gingiva.
(b) Te central cusp o the mandibular right second premolar had
been ractured. (c) Afer controlling hemorrhage, viable tissue
was obser ved in the canal because insertion o a K-le evoked a
sensation. (d)Placement o MA in the canal. (e) Postoperative X-ray
photograph showing MA placement in canal.
(a) (b) (c)
F : (a) Intraoral photograph showing no abnormalities o gingiva.
(b) Panoramic X-ray photograph showing the ormation o a
dentinbridge in the mandibular right second premolar. (c) X-ray
shows that radiolucency became less radiolucent in the
periradicular region andthe ormation o a dentin bridge in the
mandibular right second premolar.
-
7/25/2019 Pulp Revascularization in Immature Permanent Tooth
With Apical Periodontitis Using MTA
4/6
Case Reports in Medicine
(a) (b) (c)
F : (a) Intraoral photograph showing no abnormalities o gingiva.
(b) Panoramic X-ray showing the ormation o a dentin bridge
andthickening o the canal walls in the mandibular right second
premolar. (c) Panoramic X-ray showing the ormation o a dentin
bridge andthickening o the canal walls and establishment o the
periodontal ligament space and lamina dura in the mandibular right
second premolar.
MA is a cement material with excellent biocompatibilityand good
sealing capacity that is able to produce hardtissues such as dentin
and cementum []. It is used orapexication and sealing o
communication between the rootandperiodontal tissue, such as in
reverse root canal lling andperoration repair []. However, there
are ew reports o itsuse or pulp revascularization using MA [, ].
Calciumhydroxide ormulations are typically used or apexogenesisand
poor sealing capacity []. Furthermore, ormation o anecrotic layer
immediately beneath the pulp can occur andthe procedure must be
changed to a pulpectomy in somecases due to spreading inammation,
as it does not providean adequate biodeense mechanism against even
a limitedbacterial invasion []. Accordingly, we used MA in
thiscase. Generally, the root o a tooth with pulp
revascularizationis smaller than a mature tooth and is
characterized bymore rapid calcication o the pulp than that seen
afer aconventional apexogenesis procedure, as noted in the
presentcase []. Chen et al. [] demonstrated ve types o responseo
these immature teeth withinected necrotic pulp tissueandapical
periodontitis/abscess to revascularization procedures:type ,
ormation o a hard tissue barrier in the canal betweenthe coronal
cement plug and root apex using MA. Te
present case was consistent with type . In cases with animmature
root with a large apical oramen, pulp inectionassociated with an
apical lesion does not always indicate pulpnecrosis, as seen in our
patient, likely because the pulp at thisstage is vital enough and
has extremely high healing ability.It has been reported that pulp
revascularization was inducedby removing inective material rom the
root canal andapply-ing calcium hydroxide past MA [, ].
raditionally, inthe clinical protocol or revascularization
treatment, severalkinds o antibacterial medicine were used. But,
recently, itreported that a single-visit pulp revascularization
protocolcan be a avorable treatment or partially necrotic
immaturepermanent teeth using MA as a pulpal seal [].
Accordingly, or immature tooth with a pulp inectionand open
apical oramen, treatment should start with pulprevascularization
and then shif to apexication i incurable,while considering the
inection to be reversible.
4. Conclusion
In the present case, clinical and radiographic evidenceshowed
successul use o MA or revascularization treat-
ment o an immature permanent tooth. More studies arenecessary to
understand the mechanisms o pulp revascular-ization comparing
different protocols.
Conflict of Interests
No potential conict o interests was disclosed.
Acknowledgments
Tis study was supported in part by grants-in-aid or scien-tic
research rom the Ministry o Education, Science, Sports,and Culture
o Japan and rom Kitakyushu to Kenshi Maki.
References
[] M. Rafer, Apexication: a review, Dental Traumatology, vol.,
no. , pp. , .
[] S.-I. Iwaya, M. Ikawa, and M. Kubota, Revascularization o
animmature permanent tooth with apical periodontitis and
sinustract,Dental Traumatology, vol. , no. , pp. , .
[] F. Banchs and M. rope, Revascularization o immature
per-manent teeth with apical periodontitis: new treatment
proto-col?Journal of Endodontics, vol. , no. , pp. , .
[] P. Becerra, D.Ricucci,S. Loghin, J.L. Gibbs,and L. M.
Lin,His-tologic study o a human immature permanent premolar
with
-
7/25/2019 Pulp Revascularization in Immature Permanent Tooth
With Apical Periodontitis Using MTA
5/6
Case Reports in Medicine
chronic apical abscess afer
revascularization/revitalization,Journal of Endodontics, vol. , no.
, pp. , .
[] H. W. Roberts, J. M. oth, D. W. Berzins, and D. G.
Charlton,Mineral trioxide aggregate material use in endodontic
treat-ment: a review o the literature,Dental Materials, vol. , no.
,pp. , .
[] A. Rao, A. Rao, and R. Shenoy, Mineral trioxide
aggregateareview,Journal of Clinical Pediatric Dentistry, vol. ,
no. , pp., .
[] S. Simon, F. Rilliard, A. Berdal, and P. Machtou, Te use
omineral trioxide aggregate in one-visit apexication treatment:a
prospective study, International Endodontic Journal, vol. ,no. ,
pp. , .
[] I. H. Barngkgei, E. S. Halboub, and R. S. lboni, Pulpotomyo
symptomatic permanent teeth with carious exposure usingmineral
trioxide aggregate,Iranian Endodontic Journal, vol. ,no. , pp. ,
.
[] A. Harandi, M. Forghani, and J. Ghoddusi, pulp therapy
withthree different pulpotomy agents in immature molars: a
casereport, Iranian Endodontic Journal, vol. , no. , pp. ,
.[] Y. Fujita and K. Maki, Single-visit revascularization
treatment
o an immature permanent tooth with apical periodontitis: acase
report,Pediatric Dental Journal, vol. , pp. , .
[] M. Y.-H. Chen, K.-L. Chen, C.-A. Chen, F. ayebaty, P.
A.Rosenberg, and L. M. Lin, Responses o immature permanentteeth
with inected necrotic pulp tissue and apical periodon-titis/abscess
to revascularization procedures, InternationalEndodontic Journal,
vol. , no. , pp. , .
[] S. I. Iwaya, M. Ikawa, and M. Kubota, Revascularization oan
immature permanent tooth with periradicular abscess
aferluxation,Dental Traumatology, vol. , no. , pp. , .
[] K. Neha, R. Kansal, P. Garg, R. Joshi, D. Garg, and H.-S.
Grover,Management o immature teeth by dentin-pulp regeneration:
a
recent approach,Medicina Oral, Patologia Oral y Cirugia
Bucal,vol. , no. , pp. ee, .
[] R. K. Subay, B. Ilhan, and H. Ulukapi, Mineral trioxide
aggre-gate as a pulpotomy agent in immature teeth: long-term
casereport,European Journal of Dentistry, vol. , pp. , .
[] J. A. H. Lindeboom, J. W. F. H. Frenken, F. H. M. Kroon,
andH. P. van den Akker, A comparative prospective
randomizedclinical study o MA and IRM as root-end lling materials
insingle-rooted teeth in endodontic surgery, Oral Surgery,
OralMedicine, Oral Pathology, Oral Radiology, and Endodontics,
vol., no. , pp. , .
[] S. Y. Shin, J. S. Albert, and R. E. Mortman, Onesteppulp
revas-cularization treatment o an immature permanent tooth
withchronic apical abscess: a case report,International
EndodonticJournal, vol. , no. , pp. , .
[] D. M. Ferris and J. C. Baumgartner, Peroration repair
com-paring two types o mineral trioxide aggregate, Journal
ofEndodontics, vol. , no. , pp. , .
[] P. E. Murray, A. A. Haez, A. J.Smith, and C. F. Cox,
Identica-tion o hierarchical actors to guide clinical decision
making orsuccessul long-term pulp capping,Quintessence
International,vol. , no. , pp. , .
-
7/25/2019 Pulp Revascularization in Immature Permanent Tooth
With Apical Periodontitis Using MTA
6/6
Submit your manuscripts at
http://www.hindawi.com
















![Periodontitis [autosaved]](https://img.pdfslide.tips/doc/110x75/587d75871a28ab634b8b5185/periodontitis-autosaved.jpg)