-
8/12/2019 Stroke 1994 D'Agostino 40 3
1/5
R B D'Agostino, P A Wolf, A J Belanger and W B KannelStroke risk
profile: adjustment for antihypertensive medication. The Framingham
Study.
Print ISSN: 0039-2499. Online ISSN: 1524-4628Copyright 1994
American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville
Avenue, Dallas, TX 75231Strokedoi: 10.1161/01.STR.25.1.40
1994;25:40-43Stroke.
http://stroke.ahajournals.org/content/25/1/40World Wide Web
at:
The online version of this article, along with updated
information and services, is located on the
http://stroke.ahajournals.org//subscriptions/
is online at:StrokeInformation about subscribi ng
toSubscriptions: http://www.lww.com/reprints
Information about r eprints can be found online at:Reprints:
document.Permissions and Rights Question and Answeravailable in
thePermissions in the middle column of the Web page under Serv
ices. Further information about this process isOnce the online
version of the published article for which permission is being
requested is located, click Request
can be obtained via RightsLink, a service of the Copyright
Clearance Center, not the Editorial Office.Stroke Requests for
permissions to reproduce figures, tables, or portions of articles
originally published inPermissions:
by guest on November 14, 2013http://stroke.ahajournals.org/
Downloaded from by guest on November 14,
2013http://stroke.ahajournals.org/ Downloaded from
http://stroke.ahajournals.org/content/25/1/40http://stroke.ahajournals.org//subscriptions/http://stroke.ahajournals.org//subscriptions/http://stroke.ahajournals.org//subscriptions/http://www.lww.com/reprintshttp://www.lww.com/reprintshttp://www.lww.com/reprintshttp://www.ahajournals.org/site/rights/http://www.ahajournals.org/site/rights/http://stroke.ahajournals.org/http://stroke.ahajournals.org/http://stroke.ahajournals.org/http://stroke.ahajournals.org/http://stroke.ahajournals.org/http://stroke.ahajournals.org/http://stroke.ahajournals.org/http://stroke.ahajournals.org/http://stroke.ahajournals.org/http://stroke.ahajournals.org//subscriptions/http://stroke.ahajournals.org//subscriptions/http://www.lww.com/reprintshttp://www.lww.com/reprintshttp://www.ahajournals.org/site/rights/http://www.ahajournals.org/site/rights/http://stroke.ahajournals.org/content/25/1/40
-
8/12/2019 Stroke 1994 D'Agostino 40 3
2/5
40
Stroke Risk Profile: Adjustmentfor Antihypertensive
MedicationThe Framingham Study
Ralph B. D Agostino, PhD ; Philip A. Wolf, MD ;
Albert J. Belanger MA; William B. Kannel, MD
Background and Purpose We sought to modify existingsex-specific
health risk appraisal functions (profile functions)for the
prediction of first stroke that bett er assess th e effects ofth e
use of antihypertensive medication.
Methods Hea lth risk appraisal functions were
previouslydeveloped from the Framingham Study cohort. These
func-tions were Cox proportional hazards regression models
relat-ing age, systolic blood p ressu re, dia betes mellitus,
cigarettesmoking, prior cardiovascular disease, atrial
fibrillation, leftventricular hypertrophy by electrocardiogram, and
the use ofantihypertensive medication to the occurrence of
stroke.Closer examination of the data indicated that
antihypertensivetherapy effect is present only for systolic blood
pressuresbetween 110 and 200 mm Hg. Adjustments to the
regressions
to better fit the observed data were developed and tested
forstatistical significance and goodness-of-fit of the
modelresiduals.
Results Modified functions more consistent with the datawere
developed, and, from these, tables to evaluate 10-yearrisk of first
stroke were computed.
Conclusions The stroke profile can be used for evaluationof the
risk of stroke and suggestion of risk factor modificationto reduce
risk. The effect of antihypertensive therapy in theevaluation of
stroke risk can now be better evaluated.
(Stroke.1994;25:40-43.)
Key Words antihypertensive agentsdisorders risk factors
cerebrovascular
Wolf et al 1 presented sex-specific health risk
appra isal functions (or profile functions)relating risk factors
including systolic blood
pressure and the use of antihypertensive medication tothe
probability of developing a stroke. Those functionswere Cox
proportional hazards regression models. Formen there was an
elevation of risk for those on antihy-pertensive medication. For
women there was an eleva-tion of risk and also an interaction of
systolic bloodpressure level and being on antihypertensive
medica-tion. In both sexes these effects were presented asapplying
to all levels of systolic blood pressures. Closerexamination of the
data indicated that an added effect ispresent only for systolic
blood pressures between 110and 200 mm Hg. Modifications to the h
ealth risk ap-praisal functions were developed to take this into
ac-count. These modifications are more consistent with thedata and
supply better statistical fits to the data. In thefollowing the
modified functions are presented alongwith tables that can be used
to estimate 10-year prob-abilities of first stroke.
Received July 28, 1993; final revision received September
29,1993; accepted September 29, 1993.
From the Department of Mathematics (R .B.D., A.J.B.), Collegeof
Liberal Arts, and the Department of Neurology (P.A.W.),School of
Medicine, Boston University; and the Section of Pre-ventive
Medicine and Epidemiology (P.A.W., W.B.K.), EvansMemorial
Department of Clinical Research and Department ofMedicine,
University Hospital, Boston, Mass.
Reprint requests to Ralph B. D'Agostino, PhD, Boston
Univer-sity, Mathematics Department, 111 Cummington St, Boston,
MA02215.
Subjects nd M ethodsThe data used were the same as those used to
develop the first
functions.1 Health risk appraisal functions were developed
usingsubjects aged 55 to 84 years, free of stroke at the time of
twoexamination cycles (examinations 9 and 14), and followed for
10years from each of these examinations. Stroke risk
factorsincluded age, systolic blood press ure, use of
antihypertensivetherapy, diabetes mellitus, cigarette smoking,
prior cardiovascu-lar disease (coronary heart disease, cardiac
failure, or intermit-tent claudication), atrial fibrillation, and
left ventricular hyper-trophy by electrocardiogram. All these
factors are the same aspreviously u sed and are defined elsewhere
.12
The Cox proportional hazards regression model was used asthe
model for the stroke profile.3 In the analysis of Wolf et al, 1
use of antihypertension medication was entered into theanalysis
as a dummy variable, and the interaction of it withsystolic blood
pressure was investigated as the product of thedummy variable for
the antihypertensive medication and sys-
tolic blood pressure. More consistent with the data is
thereplacement of the latter two variables w ith a variable of
theform
NEWHRXSBP=HRX {SBP- 110)*(200-S5/>)
for systolic blood pressures between 110 and 200 mm Hg. HereHRX
is a dummy variable defined as 1 if the individual is
onantihypertensive medication and 0 if not, and SBP is
theindividual's systolic blood pressure. Th e variable NE-WHRXSBP
equals 0 for systolic blood pressures below 110 orgreater than 200
mm Hg.
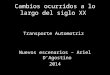
The effect of this variable on the stroke profile is illustrated
inthe F igure. For women the regression coefficient for SBP in
thenew stroke profile is 0.0161, and for NEWHRXSBP it is
0.00026.For systolic blood pressures below 110 mm Hg or above
200
mm Hg, the stroke profile function gives the same weight
toindividuals whether they are on or off antihypertensive
medica-tion, and it is 0.0\6\*SBP. For those with systolic blood
pres-
by guest on November 14, 2013http://stroke.ahajournals.org/
Downloaded from
http://stroke.ahajournals.org/http://stroke.ahajournals.org/http://stroke.ahajournals.org/http://stroke.ahajournals.org/http://stroke.ahajournals.org/
-
8/12/2019 Stroke 1994 D'Agostino 40 3
3/5
3 T
ontri ution
* not on iretf cation
- on media t ion
- m ediati on has no effect
80 90 100 110 120 130 140 150 160 170 180 190 200 210 220 230
240
Systolic Blood Pressure (SBP)
D Agostino et al S troke Risk Profile 41
Graph shows contribution of systolic blood pressure(SBP) on
female stroke profile function. The contri-bution is 0.0161 SBP for
wom en w ith SBP below
110 mm Hg or above 200 mm Hg regardless of theirantihypertensive
medication use and for those withSBP between 110 and 200 mm Hg if
they are not onantihypertensive m edication. The contribution
is0.0161 *SBP+0.000 26*(SBP-11 0)*(200-SBP) forthose with SBP
between 110 and 200 mm Hg andalso on antihypertensive medica
tion.
sures between 110 mm Hg and 200 mm Hg and not on medica-tion,
the contribution of the blood pressure to the s troke profileis
0.0161*55/*, while for those with systolic blood pressuresbetween
110 mm Hg and 200 mm Hg and on medication thecontribution is
0.0161*SBP+0.00026*(SBP-110)*(200-SBP).
The Figure depicts the contribution to the stroke profile
forsystolic blood pressures between 80 mm Hg and 240 mm Hg.
The values 110 mm Hg and 200 mm Hg were selected foruse in the
NEWHRXSBP variable because most systolic bloodpressures of those on
antihypertensive medication fell in thatinterval (96 ) and because
they repres ented discontinuities inthe frequency distributions.
The selection of other values didnot improve the fit to the
data.
The Statistical Analysis System's Cox proportional hazardsmodel
procedure, PROC PHREG,4 was used for analysis. Modelsusing the
antihypertensive therapy variable and the interaction ofit with
systolic blood pressure levels were contrasted with modelsusing the
NEWHRXSBP variable, for both statistical significanceand
goodness-of-fit as judged by analyses of the m
odels'residuals.4
ResultsDuring 10 y ears of follow-up from examinations 9 and
14, 472 stroke events occurred in 2372 men and 3362women.
Descriptive statistics of these are given in theprevious article.1
The new variable NEWHRXSBP wasstatistically significant for both
sexes in Cox regressionmodels that included all the risk factors
listed aboveexcept for antihypertensive medication (/'=.0006
forwomen and />=.O5 for men).
For both the female and male models the addition ofthe dummy
variables for antihypertensive medication andthe interaction of
this with systolic blood pressure did notadd significantly to the
regressions that already included
NEWHRXSBP. This latter variable was sufficient to re -place
them. Further, analysis of the residuals indicatedthat the use of
NEWHRXSBP provided the best mod el fitto the data. F inally,
selection of v lues other than 110 and200 mm Hg for NEWHRXSBP did
not improve statisticalsignificance and model fit. Table 1 presents
the Coxregression coefficients and their standard errors,
relativerisks, and 95 confidence intervals for the risk factors
ofthe new hea lth risk appraisal functions. Tables 2 and 3 givethe
probabilities of stroke within 10 years for men andwomen aged 55 to
84 years and free of previous stroke,respectively, com puted from
these functions. Table 4 givesthe average 10-year probabilities of
first stroke by agegroups for each sex. Table 4 can be used for
comparison
with probabilities computed from Tables 2 and 3. Thesetables
replace tab les of the previous article1 as follows: th enew Table
1 here replaces the previous Table 3, Table 2
replaces the previous Table 5, Table 3 replaces the previ-ous
Table 6, and th e present Table 4 replaces the previousTable 4.
As an illustration, say a 70-year-old woman presentsherself to a
physician with the following profile: systolicblood pressure of 135
mm Hg, on antihypertensivetherapy, nondiabetic, cigarette smoker,
previous history
TABLE 1 . Regress ion Coefficients, Relative Risk s,
andConfidence Intervals for Risk Factors in CoxProportional Haza
rds Regres sions for Stroke Profile inSubjec ts Aged 55-84 Years
and Free of S t roke a tExaminations 9 and 14
Variable
Me n
Age, y*
SBP, mm Hg*
NEWHRXSBPCVD
LVH
Cigs
AF
Diabetes
Women
Age, y*
SBP, mm Hg*
NEWHRXSBP
CVD
LVH
Cigs
AF
Diabetes
0.0488
0.0152
0.00019
0.5460
0.7864
0.5224
0.5998
0.3429
0.0699
0.0161
0.00026
0.4404
0.8055
0.5419
1.1173
0.5604
SE
0.0103
0.0031
0.00010
0.0151
0.2846
0.1429
0.3011
0.1894
0.0089
0.0024
0.00007
0.1462
0.2429
0.1453
0.2302
0.1706
RR
1.63
1.16
N/A1.73
2.20
1.69
1.82
1.41
2.01
1.17
N/A
1.55
2.24
1.72
3.06
1.75
95 Cl
1.33-1.99
1.10-1.24
1.68-1.78
1.26-3.84
1.27-2.23
1.01-3.29
0.97-2.04
1.69-2.40
1.12-1.23
1.17-2.07
1.39-3.60
1.29-2.29
1.95-4.80
1.25-2.45
RR indicates relative risk; Cl, confidenc e interval; and N/A,
notapplicable. Variables were defined as follows: SBP,
systolicblood pressure; NEWHRXSBP =0 if SBP 20 0,else, =HR X*(SB
P-11 0)*(200 -SBP ) where HRX=1 if on medi-catio n, 0 if not; CVD
(cardiovascular disea se), history of myoca r-dial infarction,
angina pecto ris, corona ry insufficiency, intermit-tent
claudication, or congestive he art failure (yes =1 , no =0 );LVH,
left ventricular hypertrophy o n electrocardiogram (ye s= 1,no=0);
Cigs, smokes cigarettes (yes=1, no=0); AF, history ofatrial
fibrillation (yes=1, no=0); Diabetes, history of diabetes(yes=1,
no=0) .
*For age and SBP, the RR is computed for an increase of 10units.
All other variables compare presence vs absence.
by guest on November 14, 2013http://stroke.ahajournals.org/
Downloaded from
http://stroke.ahajournals.org/http://stroke.ahajournals.org/http://stroke.ahajournals.org/http://stroke.ahajournals.org/http://stroke.ahajournals.org/
-
8/12/2019 Stroke 1994 D'Agostino 40 3
4/5
42 Stroke Vol 2 5, No 1 January 1994
TABLE 2. Probability of Stroke Within 10 Years for Men Aged 5
5-8 5 Years and Free of Previous Stroke in theFramingham Heart
Study
Age, yUntreated SBP,mm Hg
Treated SBP,mm Hg
Diabetes
Cigs
CVD
AF
LVH
Points
1
2
3
4
5
6
7
8
9
10
0 + 1
54-56 57-59
97-105 106-115
97-105 106-112
No
No
No
No
No
10-YearProbability,
3
3
4
4
5
5
6
7
8
10
+2
60-62
116-125
113-117
Yes
Points
11
12
13
14
15
16
17
18
19
20
+3
63-65
126-135
118-123
Yes
10-YearProbability,
11
13
15
17
20
22
26
29
33
37
Points
+ 4 + 5
66-68 69-72
136-145 146-155
124-129 130-135
Yes
Ye s
Yes
Points
21
22
23
24
25
26
27
28
29
30
+6 +7 +8 +9 + 1 0
73-75 76-78 79-81 82-84 85
156-165 166-175 176-185 186-195 196-205
136-142 143-150 151-161 162-176 177-205
10-YearProbability,
42
47
52
57
63
68
74
79
84
88Variables were defined as follows: SBP, systolic blood
pressure; Diabetes, history of diabetes; Cigs, smokes cigarettes;
CVD
(cardiovascular disea se), history of myoca rdiai infarction,
angina p ectoris, coronary insufficiency, intermittent ciaud
ication, or con gestiveheart failure; AF, history of atrial
fibrillation; LVH, left ventricular hypertrophy on
electrocardiogram.
of cardiovascular disease, no atrial fibrillation present,and no
left ventricular hypertrophy. Using Table 3, thiswoman receives 5
points for being aged 70, 6 points forhaving a systolic blood press
ure of 135 mm H g while onantihypertensive therapy, no points for
diabetes, 3points for smoking, 2 points for history of
cardiovasculardisease, no points for the presence of atrial
fibrillation,and no points for left ventricular hypertrophy.
Thisperson therefore receives a total of 16 poin ts. A score of
16 points yields a 10-year stroke probab ility of 19 .Relatin g
this 19 to the average probability for awomen this age provides
perspective; the average 10-year probability of stroke for a
70-year-old women is10.9 (Table 4). Thus, this hypothetical woman
has astroke risk that is 1.7 times the average. Her physiciancan
urge her to stop smoking, which would result in atotal of 13 points
and a probability of 11 for a strokerisk of 1.0 relative to the
average risk.
Computation of the risk for the aforementioned70-year-old woman
by the previous function1 produceda probability of 23 , which is a
difference of 4 fromthe new estimate. Part of this difference is
due torounding in generating Table 3 but also reflects a slight
overestimate by the previous function for women
onantihypertensive medication. The exact estimates pro-duced
directly by the Cox regressions are 20.2 for the
new function and 23.2 for the old function, accountingfor 3 of
the 4 difference. Ro und ing prod uced bygenerating the tables
accounts for 1 of the difference.
DiscussionIn a previous article1 we discussed in detail the
importance of control and intervention of the riskfactors of
stroke and described in detail how to use thestroke profiles or
health risk appraisal functions. The
focus of this article has been the adjustm ent for
antihy-pertensive medication. It involved determining the re-gion
of blood pressures attained by those on antihyper-tensive
medication and then approximating the riskprofiles for these
subjects. While the adjustments madefor antihypertensive medication
in this article do notdiffer appreciably from those generated by
the previousfunction, they are more consistent with the data
andreflect a substantive advancement in the generation ofhealth
risk appraisal functions. These functions havetraditionally ignored
the effects of treatments, assumingthat, for example, blood
pressures attained on medica-tion are equivalent to uncontrolled
blood pressures.This is not the case with our data. Further health
risk
appraisal functions will have to explore and
investigatetreatments not only for blood pressure but for
otherimportant risk factors such as cholesterol and glucose.
by guest on November 14, 2013http://stroke.ahajournals.org/
Downloaded from
http://stroke.ahajournals.org/http://stroke.ahajournals.org/http://stroke.ahajournals.org/http://stroke.ahajournals.org/http://stroke.ahajournals.org/
-
8/12/2019 Stroke 1994 D'Agostino 40 3
5/5
D Agostino et al Stroke Risk Profile 43
TABLE 3. Probability of Stroke Within 10 Years for Wom en Aged 5
5-8 4 Years and Free of Previous Stroke in theFramingham Heart
Study
Age, yUntreated SBP,m m H g
Treated SBP,m m H g
Diabetes
Cigs
CVD
AF
LVH
Points
1
2
3
4
5
6
7
8
9
10
0 + 1
54-56 57-59
95-106
95-106
No
No
No
No
No
10-YearProbability,
1
1
2
2
2
3
4
4
5
6
+2
60-62
107-118
107-113
Ye s
Points
11
12
13
14
15
16
17
18
19
20
+3
63-64
119-130
114-119
Yes
Yes
10-YearProbability,
8
9
11
13
16
19
23
27
32
37
Points
+ 4 + 5
65-67 68-70
131-143 144-155
120-125 126-131
Ye s
Points
21
22
23
24
25
26
27
+6 +7 +8 +9 +10
71-73 74-76 77-78 79-81 82-84
156-167 168-180 181-192 193-204 205-216
132-139 140-148 149-160 161-204 205-216
Yes
10-YearProbability,
43
50
57
64
71
78
84
Variables were defined as follows: SBP, systolic blood pressure;
Diabetes, history of diabetes; Cigs, Smokes cigarettes;
CVD(cardiovascular disease), history of myocardial infarction,
angina pectoris, coronary insufficiency, intermittent ciaudication,
or congestiveheart failure; AF, history of atrial fibrillation;
LVH, left ventricular hypertrophy on electrocardiogram.
Finally, in our previous article we discussed in detailhow to
use the health risk appraisal functions forestimates different than
10 years. The instructions giventhere are appropriate here except
that the antihyper-tension variable and the interaction of this
with systolic
TABLE 4. Average 10-Year Probability of StrokeAccording to Age
in Men and Women
Age Group, y Men Women
4.7
7.2
10 9
15.5
23.9
6.5
Values are percentages.
55-59
60-64
65-69
70-74
75-79
80-84
Age-adjusted
5.9
7.8
11.0
13.7
18.0
22.3
9.6
blood pressure level are replaced by the new variableNEWHRXSBP
described above.
AcknowledgmentsThis study was supported in part by National
Institute of
Neurological Disorders and Stroke grant 2-RO1-NS-17950-09(Dr
Wolf), National Heart, Lung, and Blood Institute
grantRO1-H140423-04 (Dr D'Agostino), and National Heart, Lung,and
Blood Institute contract NIH-NO1-HC-38038 (Dr Wolf).
References1. Wolf PA, D'Agostino R B, Belanger AJ, Kannel WB.
Probability of
stroke: a risk profile from the Framingham Study. Stroke.
1991;22:312-318.
2. Cupples LA, D'Agostino RB. Some risk factors related to
theannual incidence of cardiovascular disease and death using
pooledrepeated biennial measurements: Framingham Heart
Study,30-year follow-up. In: Kannel WB, Wolf PA, Garrison RJ, eds.
Th eFramingh am Study: An Epidemiologica l Investigation of
Cardio-vascular Disease, Section 34. Bethesda, Md: National Heart,
Lung,and Blood Institute publication NIH 87-2703; 1987.
3. Kalbfleisch JD, Prentice RL. T he Statistical Analysis of
Failure TimeData. New York, NY: John Wiley & Sons, Inc;
1980.
4. SAS Institute Inc. SA S Supplemental Library User s Guide,
Version 5Edition. Cary, NC: SAS Institute Inc; 1986.
by guest on November 14, 2013http://stroke.ahajournals.org/
Downloaded from
http://stroke.ahajournals.org/http://stroke.ahajournals.org/http://stroke.ahajournals.org/http://stroke.ahajournals.org/http://stroke.ahajournals.org/