Embed Size (px)
DESCRIPTION
q
Citation preview

Tumor Kolorektal Author: Jaime Shalkow, MD; Chief Editor: Robert J Arceci, MD, PhD Pengarang:
Shalkow Jaime, MD; Pemimpin Redaksi: Arceci J Robert, MD, PhD
http://emedicine.medscape.com/article/993370-overview#a30
khtisar

At least 50% of the Western population develops a colorectal tumor by age 70 years. Setidaknya 50% dari populasi Barat mengembangkan tumor kolorektal pada usia 70 tahun. In 10% of these individuals, the tumor progresses to malignancy. Dalam 10% dari individu, tumor berkembang menjadi keganasan. In adults, colorectal cancer is the second leading cancer that causes death worldwide. [1] This article discusses the classification, etiology, genetics, clinical presentation, and management of colonic tumors seen in the children. Pada orang dewasa, kanker kolorektal merupakan kanker terkemuka kedua yang menyebabkan kematian di seluruh dunia. [1] Artikel ini membahas klasifikasi, etiologi, genetika, presentasi klinis, dan pengelolaan tumor kolon terlihat pada anak-anak. These include polyps, sporadic colorectal carcinoma (CRC) and familial colon cancer (familial adenomatous polyposis [FAP]), and hereditary nonpolyposis colorectal cancer (HNPCC). Ini termasuk polip, karsinoma kolorektal sporadis (CRC) dan kanker usus besar keluarga (keluarga adenomatosa poliposis [FAP]), dan kanker kolorektal herediter nonpolyposis (HNPCC).
See the images below. Lihat gambar di bawah.

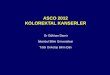
This picture depicts an abdominal CT scan of a 7 year-old boy with a mucinous adenocarcinoma of the ascending colon. Gambar ini melukiskan satu CT scan perut tahun anak laki-laki berusia 7 dengan adenocarcinoma mucinous dari usus besar naik. Note the thickness and increased vascularity of the colonic wall, as well as irregularities on the serosal surface. Perhatikan ketebalan dan peningkatan vaskularisasi dinding kolon, serta penyimpangan pada permukaan serosal. This cut also shows severe tumor infiltration of the colonic mesentery surrounding the mesenteric and retroperitoneal vessels. potong ini juga menunjukkan infiltrasi tumor parah dari mesenterium usus
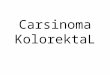
sekitarnya dan retroperitoneal kapal mesenterika. Coronal CT scan demonstrating the profuse tumoral infiltration of the ascending colonic mesentery surrounding mesenteric and portal vessels. CT scan koronal menunjukkan infiltrasi tumoral sebesar-besarnya dari mesenterium kolon ascending sekitarnya dan portal kapal mesenterika. Also note the thickness of the colonic hepatic flexure. Perhatikan juga ketebalan dari lentur hati kolon.
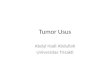
Surgical specimen after right hemicolectomy, including the terminal ileum up to the transverse colon. Bedah spesimen setelah hemicolectomy kanan, termasuk ileum terminal sampai ke kolon melintang. Mesenteric fat, vessels and lymph nodes were resected en block with the ascending colon. Mesenterika lemak, pembuluh dan kelenjar getah bening yang resected en blok dengan usus besar naik. The large intestine has been opened longitudinally. Usus besar telah dibuka longitudinal. Note the tumor on the right lower quadrant of the image, with severe thickness of the wall, areas of necrosis and hemorrhage, and some stippled calcifications. Catatan tumor pada

kuadran bawah kanan gambar, dengan ketebalan parah dinding, daerah nekrosis dan perdarahan, dan beberapa kalsifikasi dibintiki.
Polypoid Disease of the Gastrointestinal Tract Polypoid Penyakit Saluran gastrointestinal
Not all polyposis syndromes are familial. Tidak semua sindrom poliposis adalah keluarga. Familial polyposis syndromes are divided into 2 major groups based on the presence of adenomas or hamartomas. poliposis sindrom familial dibagi menjadi 2 kelompok utama berdasarkan adanya adenoma atau hamartomas. The inherited adenomatous polyposis syndromes include familial adenomatous polyposis (FAP) and Turcot syndrome; the familial hamartomatous polyposis syndromes include Peutz-Jeghers syndrome and juvenile polyposis. Sindrom mewarisi poliposis adenomatosa termasuk poliposis adenomatosa familial (FAP) dan sindrom Turcot, sindrom poliposis keluarga hamartomatous termasuk sindrom Peutz-Jeghers dan poliposis remaja.
Although juvenile polyps are common in children, adenomas are quite unusual. Walaupun polip remaja yang umum pada anak-anak, adenoma cukup tidak biasa. The latter are considered dysplastic precancerous lesions that are commonly seen in late adulthood. Yang terakhir dianggap lesi prakanker displastik yang biasanya terlihat pada usia dewasa akhir. When discovered in children, they suggest one of several types of inherited colorectal cancer. [2] Ketika ditemukan pada anak-anak, mereka menyarankan salah satu dari beberapa jenis kanker kolorektal diwariskan. [2]
Although the nomenclature is confusing, diffuse juvenile polyposis differs from juvenile polyposis coli. Meskipun tata nama yang membingungkan, poliposis remaja berdifusi berbeda dari coli poliposis remaja. Diffuse juvenile polyposis is a syndrome with multiple polyps spread throughout the GI tract and presents in younger children (aged 6 months to 5 years); in juvenile polyposis coli, the polyps are confined to the rectosigmoid area and are typically found in older patients (aged 5-15 y). poliposis Diffuse remaja adalah sindrom dengan polip yang tersebar di seluruh saluran GI dan hadiah pada anak-anak muda (usia 6 bulan sampai 5 tahun), di coli poliposis remaja, polip terbatas pada daerah rectosigmoid dan biasanya ditemukan pada pasien yang lebih tua (usia 5-15 y). Hamartomatous polyps may also be found in patients with Cowden disease, Cronkhite-Canada syndrome , Bannayan-Riley-Ruvalcaba syndrome, and basal cell nevus syndrome. [3] Hamartomatous polip juga dapat ditemukan pada pasien dengan penyakit Cowden, -Kanada sindrom Cronkhite ,-Riley-Ruvalcaba sindrom Bannayan, dan sindrom nevus sel basal. [3]
Colonic polyposis syndromes Sindrom kolon poliposis Nonfamilial polyposis - Isolated juvenile polyps (inflammatory polyps) Nonfamilial poliposis -
polip remaja Terpencil (polip inflamasi) Familial polyposis - Adenomas (FAP, Gardner syndrome, Turcot syndrome), hamartomas
(juvenile polyposis, Peutz-Jeghers syndrome, Cowden disease, Cronkhite-Canada syndrome) Keluarga poliposis - Adenoma (FAP, sindrom Gardner, sindrom Turcot), hamartomas (poliposis remaja, sindrom Peutz-Jeghers, penyakit Cowden, Cronkhite-Kanada sindrom)

The lesions can be isolated to the intestine (eg, juvenile, lymphoid, familial adenomatous) or can involve other areas of the body (eg, Peutz-Jeghers syndrome, Gardner syndrome, Turcot syndrome). Lesi dapat diisolasi pada usus (misalnya, remaja, limfoid, adenomatosa keluarga) atau dapat melibatkan area lain dari tubuh (misalnya, sindrom Peutz-Jeghers, sindrom Gardner, sindrom Turcot). Most polyps of the GI tract are benign and result from hamartomas of the mucosa or lymphoid hyperplasia of the submucosal layer. polip Sebagian besar saluran GI yang jinak dan hasil dari hamartomas dari hiperplasia limfoid mukosa atau lapisan submukosa. However, adenomatous polyps represent a genetic alteration in the mucosa and have substantial malignant potential. Namun, polip adenomatosa mewakili perubahan genetik pada mukosa dan memiliki potensi besar ganas.
For study purposes, only the hamartomatous lesions and other nonfamilial lesions are discussed in this section. Untuk tujuan studi, hanya lesi lesi hamartomatous dan nonfamilial lainnya dibahas dalam bagian ini. FAP is presented in detail below, with other cancer-predisposing entities. FAP disajikan secara rinci di bawah, dengan lain kanker-predisposisi entitas.
Polyps occur in 1% of preschool-aged and school-aged children [4] and are the most frequent cause of rectal bleeding in toddlers and infants aged 2-5 years. Polip terjadi pada 1% dari usia dan sekolah anak-anak usia pra sekolah [4] dan merupakan penyebab paling sering perdarahan dubur pada balita dan bayi berusia 2-5 tahun. Juvenile polyps are the most common (80%), followed by lymphoid polyps (15%). polip muda adalah yang paling umum (80%), diikuti oleh polip limfoid (15%).
Juvenile polyposis syndromes are classified as follows: [5] sindrom poliposis Juvenile diklasifikasikan sebagai berikut: [5]
Isolated juvenile polyps (nonmalignant) involves no family history of juvenile polyposis and fewer than 5 polyps confined to the colon. polip remaja Terpencil (nonmalignant) tidak melibatkan sejarah keluarga dari poliposis remaja dan kurang dari 5 polip terbatas pada usus besar.
Juvenile polyposis syndromes (malignant potential) are as follows: sindrom poliposis Juvenile (potensi ganas) adalah sebagai berikut:
Diffuse juvenile polyposis of infancy - Widespread polyposis of the entire GI tract in patients younger than 6 months. Diffuse poliposis remaja masa kanak-kanak - poliposis luas dari saluran GI seluruh pasien yang lebih muda dari 6 bulan.
Diffuse juvenile polyposis - Multiple polyps throughout the GI tract but concentrated in the stomach, distal colon, and rectum; usually occurs in patients aged 6 months to 5 years poliposis Diffuse remaja - polip Multiple sepanjang saluran pencernaan, tetapi terkonsentrasi di perut, usus distal, dan rektum, biasanya terjadi pada pasien berumur 6 bulan sampai 5 tahun
Juvenile polyposis coli - Multiple polyps confined to the distal colon and rectum in patients aged 5-15 years Juvenile poliposis coli - polip Multiple terbatas pada kolon distal dan rektum pada pasien usia 5-15 tahun

Lymphoid polyps (lymphoid nodular hyperplasia) Limfoid polip (hiperplasia limfoid nodular)
Lymphoid polyps (present in 15% of patients) are hyperplastic submucosal lymphoid aggregates, most likely due to a nonspecific infection (exposure to bacteria and viruses). polip limfoid (hadir di 15% dari pasien) adalah hiperplastik agregat limfoid submukosa, kemungkinan besar karena infeksi nonspesifik (paparan bakteri dan virus). Submucosal lymphoid tissue is prominent in children, particularly in the distal ileum (Peyer patches). jaringan limfoid submukosa yang menonjol pada anak-anak, khususnya di ileum distal (Peyer patch). These non-neoplastic polyps may occur in the rectum, colon, and terminal ileum. Polip ini non-neoplastik dapat terjadi pada rektum, usus besar, dan ileum terminal. Macroscopically, they appear as firm, round, submucosal nodules that are smooth or lobulated. Makroskopik, mereka muncul sebagai perusahaan, bulat, nodul submukosa yang halus atau lobulated. They are never pedunculated. Mereka tidak pernah pedunculated. They often have a volcano-like appearance with mucosal ulceration, which leads to occult blood loss. Mereka sering memiliki penampilan seperti gunung berapi dengan ulserasi mukosa, yang mengarah ke okultisme kehilangan darah. Histologically, they are hyperplastic lymphoid follicles with a large germinal center covered by colonic mucosa. Histologi, mereka folikel limfoid hiperplastik dengan pusat germinal besar ditutupi oleh mukosa kolon. They develop in young children, with a peak incidence at age 4 years. Mereka berkembang pada anak-anak, dengan kejadian puncak pada usia 4 tahun.
Patients present with anemia or, less frequently, with severe rectal bleeding. Pasien hadir dengan anemia atau, lebih jarang, dengan perdarahan rektum yang berat. Barium enema and colonoscopy findings are helpful (in 50% of patients), and biopsy findings confirm the diagnosis. Barium enema dan kolonoskopi temuan yang bermanfaat (dalam 50% dari pasien), dan temuan biopsi mengkonfirmasikan diagnosis.
Surgery is indicated only for uncontrolled bleeding and intussusception that does not respond to enema treatment. Operasi hanya diindikasikan untuk perdarahan yang tidak terkontrol dan intussusception yang tidak menanggapi pengobatan enema. Otherwise, expectant measures are adequate because these polyps are benign and spontaneously regress. Jika tidak, langkah-langkah hamil adalah cukup karena polip jinak dan regresi spontan.
Isolated juvenile polyps Isolated juvenile polip
Also known as retention, inflammatory, or cystic polyps, isolated juvenile polyps are the most common types of polyps found in children (80%) and represent one of the most common sources of lower GI bleeding in this population. Juga dikenal sebagai retensi, peradangan, kista atau polip, polip terisolasi remaja adalah jenis yang paling umum polip ditemukan pada anak-anak (80%) dan merupakan salah satu sumber yang paling umum dari perdarahan GI rendah pada populasi ini. They are considered hamartomas and lack malignant potential. [6, 7] Juvenile polyps occur in approximately 1% of preschool-aged children. Mereka dianggap hamartomas dan kurangnya potensi ganas. [6, 7] Juvenile polip terjadi pada sekitar 1% dari anak-anak usia prasekolah. The peak incidence is in children aged 3-5 years; boys seek medical attention twice as often as girls do. [7] The polyps are solitary in 50% of patients; the remaining patients have 2-5 polyps. Insiden puncak adalah pada anak usia 3-5 tahun, anak laki-laki mencari perhatian medis

dua kali lebih sering sebagai perempuan lakukan. [7] The polip soliter dalam 50% dari pasien; sisa pasien memiliki 2-5 polip. Approximately 40-60% of polyps are found in the rectosigmoid area; the remaining polyps are distributed throughout the proximal colon. [4] Isolated juvenile polyps are rarely seen after adolescence. Sekitar 40-60% dari polip ditemukan di daerah rectosigmoid, polip dan sisanya didistribusikan di seluruh kolon proksimal. [4] polip remaja Isolated jarang terlihat setelah remaja.
These polyps are smooth, reddish, and range from 2 mm to several centimeters in diameter. Ini polip yang halus, kemerahan, dan berkisar dari 2 mm sampai beberapa sentimeter dengan diameter. They often have an ulcerated surface, which accounts for the rectal bleeding. Mereka sering memiliki permukaan ulserasi, yang rekening untuk perdarahan dubur. On cross-section analysis, cystic spaces filled with mucus are revealed. Pada analisis penampang, ruang kistik diisi dengan lendir yang terungkap. Some data suggest that that these polyps may result from structural rearrangement of the mucosa secondary to an inflammatory process. [8] Beberapa data menunjukkan bahwa bahwa polip mungkin timbul dari penataan struktur dari mukosa sekunder untuk proses inflamasi. [8]
Patients most often present with hematochezia due to superficial ulceration of the polyp (93%), pain (10%), or rectal and/or polyp prolapse and encopresis. [4] Ten percent of juvenile polyps autoamputate with spontaneous cessation of rectal bleeding. [5, 7, 9] Colonoscopy of the entire colon is performed to eliminate juvenile polyposis (ie, >5 polyps). [10] The polyps can be endoscopically removed. Pasien paling sering hadir dengan hematochezia karena ulserasi superfisial dari polip (93%), sakit (10%), atau dubur dan / atau prolaps polip dan encopresis. [4] Sepuluh persen dari polip juvenil autoamputate dengan spontan penghentian pendarahan dubur. [5, 7, 9] Colonoscopy dari seluruh usus besar dilakukan untuk menghilangkan poliposis remaja (yaitu,> 5 polip). [10] yang dapat polip endoskopi dihapus. When managing a prolapsed polyp, controlling the polyp stalk prior to resection is mandatory. Ketika mengelola prolaps polip, mengendalikan tangkai polip sebelum reseksi adalah wajib. Failure to control the polyp stalk can result in retraction, which makes hemostatic control very difficult. [7] Kegagalan untuk mengontrol tangkai polip dapat mengakibatkan pencabutan, yang membuat kontrol hemostatik sangat sulit. [7]
Juvenile polyposis syndromes Juvenile poliposis sindrom
Diffuse juvenile polyposis of infancy Diffuse poliposis remaja masa kanak-kanak
This entity occurs within the first months of life and is not familial. [11] Patients may present with diarrhea, rectal bleeding, intussusception, prolapse, bowel obstruction, protein-losing enteropathy, macrocephaly, clubbing of fingers and toes, and hypotonia. [6] entitas ini terjadi dalam bulan pertama kehidupan dan tidak keluarga. [11] Pasien mungkin hadir dengan diare, perdarahan rektum, intussusception, prolaps, obstruksi usus,-kehilangan enteropati protein, macrocephaly, clubbing jari dan jari kaki, dan hypotonia. [ 6]
The entire GI tract is involved. Saluran GI seluruh yang terlibat. One third of these patients have other congenital abnormalities such as Meckel diverticulum , malrotation, and heart lesions. [5]

Sepertiga dari pasien memiliki kelainan bawaan lain seperti divertikulum Meckel , malrotation, dan luka hati. [5]
Patients require total parenteral nutrition (TPN) and bowel rest, followed by selective resection. Pasien memerlukan nutrisi parenteral total (TPN) dan sisanya usus, diikuti dengan reseksi selektif.
Despite appropriate treatment, this disease is almost universally fatal; only 2 patients have been reported to survive after age 2 years. [6, 12] Meskipun pengobatan yang tepat, penyakit ini hampir secara universal fatal, hanya 2 pasien telah dilaporkan untuk bertahan hidup setelah usia 2 tahun. [6, 12]
Diffuse juvenile polyposis Diffuse remaja poliposis
Diffuse or familial juvenile polyposis was originally identified as isolated or multiple hamartomatous polyps that occur in the colon and rectum of children aged 6 months to 5 years. [13] Diffuse atau poliposis remaja keluarga pada awalnya diidentifikasi sebagai hamartomatous beberapa polip atau terisolasi yang terjadi dalam usus dan rektum anak usia 6 bulan sampai 5 tahun. [13]
Patients present with bright red blood per rectum, anemia, abdominal pain, and rectal prolapse. Pasien hadir dengan darah merah cerah per dubur, anemia, sakit perut, dan prolaps rektum. Diffuse juvenile polyposis is inherited as an autosomal dominant trait; [5] thus, if a parent has the condition, the chance of having an affected child is 50%. Diffuse poliposis remaja adalah diwariskan sebagai sifat dominan autosomal; [5] demikian, jika orang tua memiliki kondisi tersebut, peluang untuk memiliki anak yang terkena adalah 50%.
Hamartomas are malformed colonic mucosa arranged in a bizarre fashion. Hamartomas adalah mukosa kolon cacat diatur dalam mode aneh. Typically, these are not considered premalignant unless they are part of a polyposis syndrome. Biasanya, ini tidak dianggap premaligna kecuali mereka adalah bagian dari sebuah sindrom poliposis.
Patients with diffuse juvenile polyposis have a 50% lifetime risk of colorectal carcinoma (CRC). [14] This may be due to chronic inflammation that produces reactive hyperplasia, which then progresses to dysplasia or adenomatous changes. Pasien dengan poliposis remaja menyebar memiliki risiko seumur hidup 50% karsinoma kolorektal (CRC). [14] Hal ini mungkin disebabkan oleh peradangan kronis yang menghasilkan hiperplasia reaktif, yang kemudian berkembang menjadi displasia atau perubahan adenomatosa. These polyps often have an ulcerated surface and demonstrate more epithelium with a villous or papillary configuration. Polip ini sering memiliki permukaan ulserasi dan menunjukkan epitel lebih dengan konfigurasi vili atau papiler.
In addition to the aforementioned epithelial dysplasia occurring in juvenile polyps, adenomas are also often present. Selain displasia epitel tersebut terjadi di polip remaja, adenoma juga sering hadir. Thus, the approach to these patients is similar to that taken in patients with FAP. Dengan demikian, pendekatan pada pasien ini mirip dengan yang diambil pada pasien dengan TPI. Some authors recommend monitoring these patients with an annual CBC count (to detect anemia due to

GI bleeding), semiannual pancolonoscopy, and subsequent colectomy if severe dysplasia, bleeding, or rapid polyp formation occurs. Beberapa penulis merekomendasikan pemantauan pasien dengan jumlah CBC tahunan (untuk mendeteksi anemia karena pendarahan GI), pancolonoscopy semesteran, dan kolektomi berikutnya jika displasia parah, perdarahan, atau pembentukan polip cepat terjadi. Others advocate for prophylactic colectomy. Lain-lain advokasi untuk kolektomi profilaksis.
Associated congenital defects include cleft palate, malrotation, polydactyly, and cranial abnormalities. Asosiasi cacat bawaan termasuk langit-langit, malrotation, polydactyly, dan kelainan tengkorak.
Juvenile polyposis coli Juvenile poliposis coli
A child with at least 5 polyps, polyps throughout the GI tract, or one polyp and a family history of juvenile polyposis is considered to have the syndrome. Seorang anak dengan sedikitnya 5 polip, polip sepanjang saluran pencernaan, atau satu polip dan sejarah keluarga poliposis remaja dianggap memiliki sindrom tersebut.
Most patients have 50-100 colorectal polyps; they may also have gastric and small intestinal polyps. Kebanyakan pasien memiliki 50-100 polip kolorektal, mereka mungkin juga memiliki polip lambung dan usus kecil.
Identifying patients with this syndrome is fundamental because of the high risk for carcinoma (17%) at an early age; the mean age at diagnosis of carcinoma is 35.5 years. [11] Mengidentifikasi pasien dengan sindrom ini adalah fundamental karena risiko tinggi untuk karsinoma (17%) pada usia dini, usia rata-rata di diagnosis karsinoma adalah 35,5 tahun. [11]
Close long-term surveillance is important. surveilans Tutup jangka panjang adalah penting. The amount of polyps increases the risk of chronic bleeding, which subsequently leads to iron deficiency anemia, hypoproteinemia, and failure to thrive. [7, 12] Jumlah polip meningkatkan risiko perdarahan kronis, yang kemudian menyebabkan anemia defisiensi besi, hypoproteinemia, dan gagal tumbuh. [7, 12]
Macroscopically, these polyps resemble the isolated juvenile polyps; however, histologically, they have more epithelium with a villous or papillary configuration. Makroskopik, polip ini mirip dengan polip remaja terisolasi, namun, histologi, mereka memiliki lebih banyak epitel dengan konfigurasi vili atau papiler. Epithelial dysplasia can occur. displasia epitel dapat terjadi. Adenomas can also be found in conjunction with juvenile polyps. [6] Lobular polyps have a higher propensity for a more severe dysplasia (47%) than nonlobular polyps (10%). [15] Adenoma dapat juga ditemukan dalam hubungannya dengan polip remaja. [6] lobular polip memiliki kecenderungan yang lebih tinggi untuk displasia berat lebih (47%) daripada polip nonlobular (10%). [15]
According to the St. Mark's Polyposis Registry in London, the cumulative risk for cancer in patients with a juvenile polyposis syndrome is 68% by age 60 years. [16] Because the entity is transmitted in an autosomal dominant fashion, patients with a juvenile polyposis syndrome and

their families must receive long-term follow-up. [17] Menurut Mark St poliposis Registry di London, risiko kumulatif untuk kanker pada pasien dengan sindrom poliposis remaja adalah 68% dengan usia 60 tahun. [16] Karena entitas ditransmisikan dalam mode dominan autosomal, pasien dengan poliposis remaja sindrom dan keluarga mereka harus menerima jangka panjang tindak lanjut. [17]
Some authors advocate prophylactic total colectomy and rectal mucosectomy with an endorectal pull-through (ERPT), [15] whereas others recommend regular screening with colonoscopy and subsequent colectomy if severe dysplasia, rapid polyp formation, or bleeding occurs. [18] Beberapa penulis menganjurkan total kolektomi profilaksis dan mucosectomy dubur dengan tarik endorectal-melalui (ERPT), [15] sedangkan yang lain merekomendasikan skrining secara rutin dengan dan selanjutnya kolektomi kolonoskopi jika displasia parah, pembentukan polip cepat, atau perdarahan terjadi. [18]
When intussusception occurs in children older than 2 years, the discovery of a specific lead point is not uncommon (22%); however, lead points are only found in 2-8% of children within the usual age range (6-18 mo). Ketika intussusception terjadi pada anak yang lebih tua dari 2 tahun, penemuan titik timbal tertentu tidak jarang (22%), namun, poin memimpin hanya ditemukan pada 2-8% anak-anak dalam rentang usia yang biasa (6-18 bulan) . When a polyp is demonstrated as a lead point in a patient with intussusception, an evaluation may be indicated to identify polyposis syndromes. Ketika polip ditunjukkan sebagai titik utama dalam pasien dengan intussusception, evaluasi dapat diindikasikan untuk mengidentifikasi sindrom poliposis.
Some hamartomas do not appear to have any malignant potential. Beberapa hamartomas tampaknya tidak memiliki potensi ganas. However, germline mutations and somatic inactivation of STK11, SMAD4, BMPR1A, and PTEN genes in hamartomatous polyposis syndromes create an epithelial environment favorable for neoplastic transformation. [19] Namun, mutasi germline dan inaktivasi somatik dari STK11, SMAD4, BMPR1A, dan PTEN gen dalam sindrom poliposis hamartomatous menciptakan lingkungan epitel menguntungkan bagi transformasi neoplastik. [19]
Peutz-Jeghers syndrome Peutz-Jeghers sindrom
In 1921, Peutz reported on the association of intestinal polyps with mucocutaneous pigmented spots of the mouth, hands, and feet. [20] From 1944-1949, in a study of 20 patients, Jeghers defined the 2 main features of the syndrome as melanotic spots on the buccal mucosa and lips (with variable melanin pigmentation on the face and digits) and polyposis of the intestinal tract. [6] The melanotic spots range from brown to black and occur in the rectum, around the mouth, and on the lips, buccal mucosa, feet, nasal mucosa, and conjunctivae. Pada tahun 1921, Peutz melaporkan pada asosiasi dari polip usus dengan bercak berpigmen mukokutan mulut, tangan, dan kaki. [20] Dari 1944-1949, dalam studi dari 20 pasien, Jeghers mendefinisikan 2 fitur utama dari sindrom sebagai melanotic tempat pada mukosa bukal dan bibir (dengan pigmentasi melanin variabel pada wajah dan angka) dan poliposis dari saluran usus. [6] Rentang bintik melanotic dari coklat sampai hitam dan terjadi di rektum, sekitar mulut, dan di bibir , mukosa bukal, kaki, mukosa hidung, dan konjungtiva. These spots are typically present at puberty. [6] Bintik ini biasanya hadir saat pubertas. [6]

The polyps most commonly appear in the small intestine (55%), followed by stomach and duodenum (30%) and the colorectal area (15%). Polip paling sering muncul di usus kecil (55%), diikuti oleh lambung dan usus duabelas jari (30%) dan daerah kolorektal (15%). Dramatic advances have occurred in the understanding of the genetic and molecular basis of the disease that apply to these polyps. Drama kemajuan telah terjadi dalam memahami dasar molekuler genetik dan penyakit yang berlaku untuk polip. A germline mutation involving the genes LKB1 and STK11 (10-70% of cases) has been identified in this syndrome. [21, 22] Sebuah mutasi germline melibatkan gen LKB1 dan STK11 (10-70% dari kasus) telah diidentifikasi dalam sindrom ini. [21,
22]
Also, the ENG gene, which may play a role in the pathogenesis of the mucosal defects, has been identified in a subgroup of these patients, as well as in patients with hereditary hemorrhagic telangiectasia (HHT). [22] Although adenomas can occur concurrently in the syndrome, these polyps are mostly hamartomas of the muscularis mucosa. Juga, gen ENG, yang mungkin memainkan peran dalam patogenesis dari cacat mukosa, telah diidentifikasi dalam sebuah subkelompok pasien, serta pada pasien dengan telangiectasia hemoragik herediter (HHT). [22] Walaupun adenoma dapat terjadi bersamaan dalam sindrom, polip ini kebanyakan hamartomas dari mukosa muskularis. They appear as pedunculated lobulated lesions, measuring from a few millimeters to several centimeters. Mereka muncul sebagai lesi pedunculated lobulated, pengukuran dari beberapa milimeter sampai beberapa sentimeter. Peutz-Jeghers syndrome is inherited as an autosomal dominant trait, [20] but de novo cases can also develop. Peutz-Jeghers sindrom ini diwariskan sebagai sifat dominan autosomal, [20] tetapi de novo kasus juga dapat berkembang. It affects all ethnic groups with equal sex distribution; [6] however, symptoms appear earlier in males (5-10 y) than in females (10-15 y). [20] Ini mempengaruhi semua kelompok etnis dengan distribusi jenis kelamin yang sama; [6] , gejala muncul lebih awal pada laki-laki (5-10) y dari pada wanita (10-15 y). Namun [20]
GI disturbances become apparent later. gangguan GI menjadi jelas kemudian. Patients usually present during early adolescence. Pasien biasanya hadir selama masa remaja awal. Some patients present with an increased frequency of defecation, rectal bleeding, anemia, abdominal pain, vomiting, or recurrent episodes of intussusception. [20] Prolapse of rectal polyps in the first year of life, even in the absence of pigmentation, may indicate Peutz-Jeghers syndrome, at least in the familial cases. Beberapa. Pasien datang dengan suatu peningkatan frekuensi buang air besar dubur, perdarahan, anemia perut, nyeri, muntah, berulang atau episode dari intussusception [20] Keruntuhannya polip rektum pada tahun pertama kehidupan, bahkan tanpa adanya pigmentasi, dapat menunjukkan Peutz -Jeghers sindrom, setidaknya dalam kasus-kasus keluarga.
Compared with the general population, patients with Peutz-Jeghers syndrome have a 13-fold increased risk of death due to GI cancer and a 9-fold increased risk for all other cancers. [6] The risk of death due to cancer by age 60 years is 50%. Dibandingkan dengan populasi umum, pasien dengan sindrom Jeghers Peutz memiliki lipat peningkatan risiko-13 kematian akibat kanker GI dan lipat peningkatan risiko-9 untuk semua kanker lainnya. [6] Risiko kematian akibat kanker pada usia 60 tahun adalah 50%. Adenomatous and carcinomatous changes in the hamartomas have been reported. [23] Adenomatosa dan perubahan carcinomatous dalam hamartomas telah dilaporkan. [23]

Screening tests to detect all these forms of cancer are recommended in children who present with abdominal pain or occult anemia and melanotic-pigmented spots. Tes skrining untuk mendeteksi semua jenis kanker yang direkomendasikan pada anak-anak yang hadir dengan nyeri perut atau anemia gaib dan tempat melanotic-pigmen. An aggressive screening and biopsy program should be undertaken, including an annual examination with CBC count, breast and pelvic examinations (with cervical smears and pelvic ultrasonography) in females, mammography at age 25 years, testicular examination in males, pancreatic ultrasonography, and biennial upper and lower endoscopy. Sebuah skrining agresif dan program biopsi harus dilakukan, termasuk pemeriksaan tahunan dengan jumlah CBC, payudara dan pemeriksaan panggul (dengan pap serviks dan ultrasonografi panggul) pada wanita, mamografi pada usia 25 tahun, pemeriksaan testis pada laki-laki, ultrasonografi pankreas, dan dua tahunan atas dan bawah endoskopi.
Extensive intestinal resections are contraindicated because of the recurrent nature of the polyps and the ensuing short-bowel syndrome that may result. reseksi usus yang luas adalah kontraindikasi karena sifat berulang dari polip dan sindrom usus pendek berikutnya yang mungkin terjadi. Rapid growth, induration, severe dysplasia, villous changes, or polyps larger than 15 mm (which presents a much higher chance of having malignant transformation) suggest the need for a more aggressive intervention. [6] pertumbuhan yang cepat, indurasi, displasia parah, perubahan vili, atau polip yang lebih besar dari 15 mm (yang menyajikan banyak kesempatan yang lebih tinggi memiliki transformasi ganas) menyarankan perlunya intervensi lebih agresif. [6]
Gardner syndrome Sindrom Gardner
In 1962, Gardner and colleagues noticed extracolonic manifestations in some kindred with polyposis. Pada tahun 1962, Gardner dan koleganya melihat manifestasi extracolonic di beberapa sama dengan poliposis. In this syndrome, the polyps are adenomatous rather than hamartomas. Dalam sindrom ini, polip adenomatosa daripada hamartomas. The associated extraintestinal tumors include desmoid cysts, cysts of the mandible, fibromas, osteomas, and hypertrophy of the retinal pigmented epithelium. [24] Bone tumors are most common (80%), followed by inclusion cysts (35%) and desmoid tumors (18%). [7] The syndrome is inherited in an autosomal dominant pattern. Tumor ekstraintestinal terkait mencakup kista desmoid, kista para fibromas mandibula,, osteomas, dan hipertrofi epitel berpigmen retina. [24] Bone tumor adalah paling sering (80%) disusul kista inklusi (35%) dan tumor desmoid ( 18%). [7] Sindrom diturunkan dalam pola autosom dominan. The osteomas are most frequently found in the skull and facial bones. Yang osteomas adalah yang paling sering ditemukan di tengkorak dan tulang wajah. Abnormal dentition is common. [6] Periampullary malignancies may develop during the third or fourth decades of life at rates much more common than in the general population. [7] gigi abnormal adalah umum. [6] Periampullary keganasan dapat berkembang selama dekade ketiga atau keempat hidup dengan harga jauh lebih umum daripada di populasi umum. [7]
Gardner syndrome is considered a phenotypic variant of FAP, and different mutations on the adenomatous polyposis coli ( APC ) gene have been shown to be associated with this syndrome ( APC polymorphism in exons 13 and 15). [25] Intestinal polyps have a 100% likelihood of undergoing malignant transformation. [26] Sindrom Gardner dianggap sebagai varian fenotipik FAP, dan mutasi yang berbeda pada coli poliposis adenomatosa (APC) gen telah terbukti

berhubungan dengan sindrom (APC polimorfisme dalam ekson 13 dan 15). [25] polip usus memiliki 100% kemungkinan melakukan transformasi ganas. [26]
The natural history and treatment of patients with colonic polyps is the same as in those with FAP. Sejarah alam dan pengobatan pasien dengan polip kolon adalah sama seperti pada mereka dengan TPI. Desmoid tumors of the abdominal wall and mesentery occur in 20% of patients with Gardner syndrome, usually appear 6-30 months after surgery for intestinal manifestations, and are the leading cause of death in patients who have undergone colectomy. Desmoid tumor pada dinding perut dan mesenterium terjadi pada 20% pasien dengan sindrom Gardner, biasanya muncul 6-30 bulan setelah operasi untuk manifestasi usus, dan merupakan penyebab utama kematian pada pasien yang telah menjalani kolektomi. Desmoid tumors are dense fibroplastic proliferations but can present with dysplasia and even fibrosarcoma. tumor Desmoid adalah proliferations fibroplastic padat tetapi bisa hadir dengan fibrosarcoma dysplasia dan bahkan. Treatment is challenging. Pengobatan menantang. When these tumors are small and well defined, excision is feasible with a recurrence rate of 10%; however, some are not identified until they become unresectable. Bila tumor berukuran kecil dan didefinisikan dengan baik, eksisi layak dengan tingkat kekambuhan 10%, namun ada juga yang tidak teridentifikasi sampai mereka menjadi dioperasi. Desmoids that involve the small bowel mesentery should be treated according to their symptoms and growth rate. Desmoids yang melibatkan mesenterium usus kecil harus diperlakukan sesuai dengan gejala mereka dan tingkat pertumbuhan. Sulindac, tamoxifen, or vinblastine and methotrexate are adequate for slow-growing, mildly symptomatic tumors. Sulindac, tamoxifen, vinblastine dan methotrexate atau cukup untuk tumbuh lambat, tumor bergejala ringan. Aggressive tumors require high-dose tamoxifen, or antisarcoma chemotherapy (doxorubicin and dacarbazine), and possibly radiationtherapy. [22, 19] tumor agresif memerlukan dosis tamoxifen tinggi, atau kemoterapi antisarcoma (doxorubicin dan dacarbazine), dan mungkin radiationtherapy. [22, 19]
Turcot syndrome Turcot sindrom
This syndrome, also considered a variant of FAP, includes multiple pediatric brain tumors (eg, gliomas, ependymomas) in families that also have an increased risk for polyposis and colon cancer. Sindrom ini, juga dianggap sebagai varian dari FAP, termasuk tumor otak beberapa anak-anak (misalnya, glioma, ependymomas) dalam keluarga yang juga memiliki peningkatan risiko poliposis dan kanker usus besar. All patients with this syndrome develop carcinoma of the colon as young adults. [7] Colonic adenocarcinomas occur in the colonic polyps and in the mucosa between the polyps. Semua pasien dengan sindrom ini mengembangkan karsinoma usus besar sebagai orang dewasa muda. [7] adenocarcinoma kolon terjadi pada polip kolon dan di mukosa antara polip. Patients may present with chronic bloody diarrhea, hypoproteinemia, weight loss, anemia, malnutrition, bowel obstruction, and intussusception. Pasien mungkin hadir dengan diare berdarah kronis, hypoproteinemia, penurunan berat badan, anemia, kekurangan gizi, obstruksi usus, dan intussusception. Hamilton found that families with Turcot syndrome have mutations in APC or HNPCC genes. [27] The type of brain tumor correlates with the mutations, medulloblastomas in APC -related mutations, and microsatellite instability in families with glioblastoma multiforme. [6] In patients with a strong family history, begin diagnostic investigation during the second decade of life and continue annually. Hamilton menemukan bahwa keluarga dengan sindrom Turcot memiliki mutasi pada gen APC atau HNPCC. [27] Jenis

tumor otak berkorelasi dengan mutasi, medulloblastomas di-terkait mutasi APC, dan ketidakstabilan mikrosatelit dalam keluarga dengan glioblastoma. [6] Pada pasien dengan sejarah keluarga yang kuat, mulai penyelidikan diagnostik selama dekade kedua kehidupan dan terus setiap tahun.
Cronkhite-Canada syndrome Cronkhite-Kanada sindrom
This is a variant of juvenile polyposis in which the GI polyps are associated with skin hyperpigmentation, alopecia, and nail changes (Cronkhite, 1955). Ini adalah varian dari poliposis remaja di mana GI polip berhubungan dengan hiperpigmentasi kulit, alopecia, dan perubahan kuku (Cronkhite, 1955). Hair loss and skin and nail changes may be evident long before GI symptoms appear. Rambut rontok dan kulit dan perubahan mungkin kuku jelas jauh sebelum GI gejala muncul. The hamartomatous polyps appear in the stomach and colon. Polip hamartomatous muncul dalam perut dan usus besar. Chronic diarrhea results in malabsorption, hypovitaminosis, hypoproteinemia, and fluid and electrolyte imbalance. Diare kronis mengakibatkan malabsorpsi, hypovitaminosis, hypoproteinemia, dan ketidakseimbangan cairan dan elektrolit. Because patients with Cronkhite-Canada syndrome may develop colonic malignancy, close follow-up is recommended (see Syndromes associated with CRC). [7] Karena pasien dengan sindrom Cronkhite-Kanada dapat mengembangkan keganasan kolon, dekat tindak-up yang direkomendasikan (lihat Syndromes terkait dengan CRC). [7]
Typically, in all syndromes with increased risk of cancer, the author recommends following a screening schedule like the one used for patients with Peutz-Jeghers syndrome to identify malignancies at an earlier stage. Biasanya, dalam semua sindrom dengan meningkatnya risiko kanker, penulis merekomendasikan mengikuti jadwal pemutaran seperti yang digunakan untuk pasien dengan sindrom Peutz-Jeghers untuk mengidentifikasi kanker pada tahap awal.
Bloom syndrome Sindrom Bloom
This is a rare, recessively inherited disease in which growth retardation, accelerated aging, immunodeficiency, susceptibility to chromosome breaks, and a high frequency of malignant tumors are observed. [28] Patients with Bloom syndrome appear hypersensitive to various different DNA-damaging agents, such as UV light and irradiation. Ini adalah recessively, mewarisi penyakit langka di mana keterbelakangan pertumbuhan, dipercepat, imunodefisiensi penuaan, kerentanan terhadap istirahat kromosom, dan frekuensi tinggi tumor ganas diamati. [28] Pasien dengan sindrom Bloom muncul hipersensitif terhadap berbagai agen yang merusak DNA yang berbeda, seperti sinar UV dan iradiasi. A generalized DNA repair defect is present, likely a defect in DNA ligation; thus, this process has been encompassed in diseases of DNA repair defects such as xeroderma pigmentosum, ataxia-telangiectasia, and Fanconi anemia. Cacat DNA umum perbaikan hadir, kemungkinan cacat dalam ligasi DNA, dengan demikian, proses ini telah dicakup dalam penyakit cacat perbaikan DNA seperti pigmentosum xeroderma, ataksia-telangiectasia, dan anemia Fanconi.
The Bloom syndrome gene has been cloned and has been found to code for a putative helicase on chromosome 15. Gen Sindrom Bloom telah diklon dan telah ditemukan kode untuk sebuah helikase putative pada kromosom 15. In this regard, genes involved in DNA repair may be

considered tumor suppressor genes. [29] Only 0.8% of individuals with Bloom syndrome and colorectal neoplasia carry the BLM(Ash) mutation, [30] and this appears to have little clinical effect on the number of neoplasms, patient age at detection, or tumor location within the colon. [31] No specific incidence of colorectal cancer in patients with Bloom syndrome has been described in the literature. Dalam hal ini, gen yang terlibat dalam reparasi DNA dapat dianggap gen supresor tumor. [29] Hanya 0,8% dari individu dengan sindrom Bloom dan neoplasia kolorektal membawa BLM (Ash) mutasi, [30] dan ini tampaknya memiliki efek klinis yang kecil pada jumlah neoplasma, umur pasien di deteksi, atau lokasi tumor dalam usus besar. [31] Tidak ada kejadian khusus kanker kolorektal pada pasien dengan sindrom Bloom telah dijelaskan dalam literatur.
Cowden syndrome Cowden sindrom
This is an autosomal dominant transmitted disease with hamartomas of all 3 embryonal layers. Ini adalah penyakit menular autosomal dominan dengan hamartomas dari semua 3 lapisan embrional. Facial tricholemmomas, oral papillomas, multinodular goiter, and GI polyps with occasional GI cancer may also be found in patients with this syndrome. tricholemmomas Facial, papillomas lisan, gondok multinodular, dan polip dengan kanker GI GI sesekali juga dapat ditemukan pada pasien dengan sindrom ini. Fibrocystic breast disease and esophageal glycogenic acanthosis have been described. [19] These patients have a higher breast and thyroid cancer risk. penyakit fibrokistik payudara dan acanthosis glycogenic esofagus telah diuraikan. [19] Pasien ini memiliki payudara yang lebih tinggi dan risiko kanker tiroid. Germline mutations have been identified in the PTEN gene. mutasi germline telah diidentifikasi dalam gen PTEN.
Treatment is directed toward alleviating symptoms of pain, bleeding, or obstruction. Perawatan diarahkan untuk mengurangi gejala nyeri, perdarahan, atau obstruksi. Polyps should be removed when symptomatic, and screening to detect subsequent development of more polyps is warranted. Polip harus dihapus bila gejala, dan penyaringan untuk mendeteksi perkembangan selanjutnya lebih polip dibenarkan.
Ruvalcaba-Myhre-Smith syndrome Ruvalcaba-Myhre-Smith sindrom
This syndrome includes developmental abnormalities, microcephaly, and juvenile polyposis. Sindrom ini meliputi kelainan perkembangan, microcephaly, dan poliposis remaja. It is a rare disease that occurs in males. Ini adalah penyakit langka yang terjadi pada laki-laki. No cancer has been reported in these patients. Tidak kanker telah dilaporkan pada pasien ini. The polyps are removed when symptomatic, and family screening is advised. Polip dihapus ketika gejala, dan penyaringan keluarga disarankan.
Osler-Weber-Rendu syndrome Osler-Weber-Rendu syndrome
Also termed HHT, Osler-Weber-Rendu syndrome is an autosomal dominant familial disorder characterized by telangiectases and vascular malformations of the skin and mucous membranes and recurrent GI bleeding. HHT Juga disebut, Osler-Weber-Rendu syndrome adalah gangguan keluarga autosomal dominan dicirikan oleh telangiectases dan kelainan vaskular pada kulit dan selaput lendir dan berulang perdarahan GI. It may also affect the brain, lungs, and liver. [32] The

lesions are typically noticed in the first few years of life, and 50% of patients aged 10 years have had a GI bleed. Hal ini juga dapat mempengaruhi otak, paru-paru, dan hati. [32] Lesi biasanya melihat dalam beberapa tahun pertama kehidupan, dan 50% pasien berusia 10 tahun telah memiliki GI berdarah. A family history of the disease is reported in 80% of patients. Riwayat keluarga penyakit ini dilaporkan dalam 80% pasien.
The pathogenesis may relate to mutations of the ENG and ALK1 genes, which play an important role in determining the properties of endothelial cells during angiogenesis. [33] Telangiectases are usually present on the lips, oral and nasopharyngeal membranes, tongue, and perlingual areas. patogenesis mungkin berhubungan dengan mutasi dari IND dan ALK1 gen, yang memainkan peranan penting dalam menentukan sifat-sifat sel endotel selama angiogenesis. [33] Telangiectases biasanya terdapat pada bibir, oral dan nasofaring membran, lidah, dan daerah perlingual. They also occur in the colon but are more common in the stomach and small bowel, where they tend to cause significant bleeding. [34] Mereka juga terjadi di usus besar tetapi lebih sering terjadi di usus kecil dan perut, di mana mereka cenderung menyebabkan perdarahan yang signifikan. [34]
In one study, 6 of 24 patients (25%) evaluated with HHT developed a colonic neoplasia, 3 had adenocarcinoma of the colon, and 3 more had multiple colonic polyps. [35] Elinav et al recommend lower GI tract evaluation for all patients with new-onset anemia or GI bleeding, even if blood loss may be a manifestation of GI HHT. Dalam sebuah penelitian, 6 dari 24 pasien (25%) dievaluasi dengan HHT mengembangkan neoplasia kolon, 3 telah adenocarcinoma dari usus besar, dan 3 lebih memiliki polip kolon berganda. [35] Elinav et merekomendasikan rendah GI saluran evaluasi al untuk semua pasien dengan onset baru anemia atau perdarahan GI, bahkan jika kehilangan darah mungkin merupakan manifestasi dari GI HHT.
Oldfield syndrome Sindrom Oldfield
This syndrome refers to the association between sebaceous cysts and FAP. Sindrom ini mengacu pada hubungan antara kista sebasea dan TPI. Patients present during adolescence with subcutaneous lesions typically located on the extremities, scalp, and face; they develop during adolescence. [36] These patients share the same chromosomal derangements as those with FAP (ie, germline mutations of the APC gene on band 5q21). Pasien hadir selama masa remaja dengan lesi subkutan biasanya terletak di kaki, kulit kepala, dan wajah, mereka berkembang selama masa remaja. [36] berbagi ini pasien yang derangements kromosom yang sama seperti yang dengan FAP (misalnya, germline mutasi gen APC pada 5q21 band) .
The most recently described adenomatous polyposis syndrome, MutYH-associated polyposis, is autosomal recessive and requires an inherited mutation from each parent for the development of the disease. [2] Yang dijelaskan adenomatosa poliposis sindrom yang paling baru, terkait poliposis MutYH, adalah autosom resesif dan memerlukan mutasi warisan dari orang tua masing-masing untuk perkembangan penyakit. [2]
Colorectal carcinoma Karsinoma Kolorektal
Syndromes associated with CRC include the following: Sindrom yang berhubungan dengan CRC adalah sebagai berikut:

Gardner syndrome - Polyposis, osteomas, and multiple sebaceous cysts Gardner syndrome - poliposis, osteomas, dan kista beberapa sebaceous
Turcot syndrome - Polyposis and brain tumors (gliomas, ependymomas) Turcot sindrom - poliposis dan tumor otak (glioma, ependymomas)
Peutz-Jeghers syndrome - Colonic polyposis, ovarian tumors, and mucocutaneous pigmentation of lips, oral mucosa, and perioral region Peutz-Jeghers sindrom - kolon poliposis, tumor ovarium, dan pigmentasi mukokutan bibir, mukosa mulut, dan wilayah perioral
Cronkhite-Canada syndrome - GI polyposis, skin hyperpigmentation, alopecia, and nail changes Cronkhite sindrom-Kanada - GI poliposis, hiperpigmentasi kulit, alopecia, dan perubahan kuku
Osler-Weber-Rendu syndrome - Juvenile polyps and hepatic telangiectasia Osler-Weber-Rendu syndrome - polip muda dan telangiectasia hati
Oldfield syndrome - Polyposis and multiple sebaceous cysts Sindrom Oldfield - poliposis dan kista beberapa sebaceous
Bloom syndrome - Growth retardation, accelerated aging, immune deficiency, and malignant tumors sindrom Bloom - keterbelakangan Pertumbuhan, mempercepat penuaan, defisiensi imun, dan tumor ganas
Cowden syndrome - Hamartomas, GI polyps, breast, thyroid, and GI cancer Cowden sindrom - Hamartomas, GI polip, payudara, tiroid, dan GI kanker
Ruvalcaba-Myhre-Smith syndrome - Microcephaly and juvenile polyposis in males; no cancer Ruvalcaba-Myhre-Smith sindrom - poliposis Microcephaly dan remaja dalam laki-laki; kanker tidak
The screening schedule for patients with polyposis syndromes and increased risk of malignancy is as follows: Jadwal screening untuk pasien dengan sindrom poliposis dan peningkatan risiko keganasan adalah sebagai berikut:
Symptoms related to polyps - Annually Gejala yang berhubungan dengan polip - Tahunan Blood count to detect anemia - Annually menghitung Darah untuk mendeteksi anemia -
Tahunan
Breast and pelvic examinations with cervical smears and pelvic ultrasonography in girls - Annually Payudara dan panggul pemeriksaan dengan pap leher dan ultrasonografi panggul pada anak perempuan - Tahunan
Testicular examination with ultrasonography in boys - Annually Testis pemeriksaan dengan ultrasonografi pada anak laki-laki - Tahunan
Pancreatic ultrasonography - Annually Pankreas ultrasonografi - Tahunan
Esophagogastroduodenoscopy and colonoscopy - Biennially Esophagogastroduodenoscopy dan kolonoskopi - setiap dua

Mammography - Recommended at ages 25, 30, 35, and 38 years; biennially until age 50 years; annually thereafter Mamografi - Fitur pada usia 25, 30, 35, dan 38 tahun; dua tahun sekali sampai usia 50 tahun; setiap tahun
Familial colon cancer Keluarga kanker usus
Familial colon cancer syndromes are divided into those associated with polyposis (familial polyposis coli) and HNPCC. sindrom kanker familial usus besar dibagi ke dalam yang terkait dengan poliposis (coli poliposis kekeluargaan) dan HNPCC. To provide a better description of the genesis of these 2 entities and their differences, their genetic principles are briefly discussed below. Untuk memberikan gambaran yang lebih baik dari kejadian ini 2 entitas dan perbedaan mereka, prinsip-prinsip genetik mereka secara singkat dibahas di bawah ini.
Colorectal Carcinoma Genetics (Defects in Mismatch Recognition and Repair) Karsinoma Kolorektal Genetika (Cacat dalam Pengakuan Ketidaksesuaian dan Perbaikan)
The unwinding and copying enzymes that replicate DNA form a highly efficient and accurate replicative complex; however, this process is not perfect. Pembalikan enzim dan penyalinan yang meniru DNA membentuk kompleks replikatif sangat efisien dan akurat, namun proses ini tidak sempurna. Mistakes in base pairing occasionally occur, depending on the organism, the accuracy of DNA polymerases, and the peculiarities of the local environment, which may make such mistakes more or less likely. Kesalahan dalam basis pasangan kadang-kadang terjadi, tergantung pada organisme, keakuratan polimerase DNA, dan kekhususan lingkungan lokal, yang mungkin melakukan kesalahan seperti itu lebih atau kurang mungkin. Some stretches of DNA are more likely to accumulate errors than others, particularly stretches of DNA that consist of tandem-repeat units. Beberapa ruas DNA lebih cenderung untuk mengakumulasi kesalahan daripada yang lain, khususnya ruas DNA yang terdiri dari unit-repeat tandem. These areas are termed microsatellite regions. Daerah ini disebut daerah mikrosatelit. Certain patients have marked instability in the microsatellite repeats throughout their genomes; this instability leads to a failure to recognize and repair these nucleotide mismatches. pasien tertentu telah ditandai ketidakstabilan mikrosatelit mengulangi seluruh genom mereka; ketidakstabilan ini mengarah ke kegagalan untuk mengenali dan memperbaiki ketidaksesuaian tersebut nukleotida. Mismatch repair defects are an early step in the process leading to malignant transformation in some cancers. perbaikan cacat Ketidaksesuaian merupakan langkah awal dalam proses menuju transformasi ganas di beberapa kanker.
The progression from normal colon epithelium to dysplastic epithelium begins with hyperplasia, followed by the development of adenomas and, finally, invasive carcinomas. Perkembangan dari epitel usus normal epitel displastik dimulai dengan hiperplasia, diikuti dengan pengembangan adenoma dan, akhirnya, karsinoma invasif. Most mutations that occur in colon cancer develop after birth in single cells as a result of exposures to environmental influences or perhaps as a result of mistakes that cells make when they copy their DNA during cell division. Kebanyakan mutasi yang terjadi pada kanker usus besar berkembang setelah kelahiran pada sel tunggal sebagai akibat dari eksposur terhadap pengaruh lingkungan atau mungkin sebagai akibat dari kesalahan yang membuat sel-sel ketika mereka salinan DNA mereka selama pembelahan sel.

Approximately 80% of annual cases of colorectal carcinoma (CRC) are not associated with hereditary factors. Sekitar 80% kasus tahunan karsinoma kolorektal (CRC) tidak berhubungan dengan faktor keturunan.
The pathological progression of adenoma to carcinoma depends on reproducible genetic alterations such as APC gene inactivation, K-ras oncogene activation, and p53 mutation. Perkembangan patologis adenoma untuk karsinoma tergantung pada perubahan genetik direproduksi seperti inaktivasi gen APC, ras onkogen aktivasi-K, dan mutasi p53.
Mutations in the APC gene, a tumor suppressor gene that controls tumor initiation, are present in 80-90% of patients with familial adenomatous polyposis (FAP). [22] When the APC gene is mutated, the function of both APC alleles is lost. Mutasi pada gen APC, penekan tumor gen yang mengontrol inisiasi tumor, hadir dalam 80-90% pasien dengan poliposis adenomatosa familial (TPI). [22] Ketika gen APC termutasi, fungsi dari kedua alel APC hilang . One allele is defective at birth in all cells, having been inherited from one parent; the other APC gene allele is mutated in individual colon cells during early childhood, supporting the 2-hit hypothesis by Knudson. [37] Satu alel rusak pada saat lahir di semua sel, yang telah diwarisi dari satu induk; alel gen APC lainnya bermutasi dalam sel-sel usus individu selama anak usia dini, mendukung hipotesis 2 dilanda oleh Knudson. [37]
Malignant progression from the development of hyperplasia takes 20-30 years. perkembangan ganas dari perkembangan hiperplasia membutuhkan 20-30 tahun. This is because the tumors have to accumulate other mutations in oncogenes and other tumor suppressor genes that convert the benign adenoma into a malignant tumor. Hal ini karena tumor harus mengumpulkan mutasi lainnya di onkogen dan gen supresor tumor lainnya yang mengkonversi adenoma jinak menjadi tumor ganas. Recently, inactivation of the APC gene has been found to result in activation of the WNT signaling pathway and uncontrolled cell growth. Baru-baru ini, inaktivasi gen APC telah ditemukan untuk mengakibatkan aktivasi dari jalur signaling NTB dan pertumbuhan sel yang tidak terkendali. The location of the mutation in the APC gene correlates with the phenotype expressed in the patient, creating classic FAP (central mutation) or attenuated FAP (with peripheral gene mutations). Lokasi mutasi pada gen APC berkorelasi dengan fenotip disajikan dalam pasien, menciptakan klasik FAP (mutasi pusat) atau dilemahkan FAP (dengan mutasi gen perifer).
In contrast, defects in DNA repair, particularly a DNA repair system termed DNA mismatch repair, cause hereditary nonpolyposis colon cancer (HNPCC). Sebaliknya, cacat pada perbaikan DNA, khususnya sistem perbaikan DNA disebut mismatch perbaikan DNA, menyebabkan kanker nonpolyposis usus turun temurun (HNPCC). The enzymes that copy DNA are not perfect and often make mistakes. Enzim-enzim bahwa DNA copy tidak sempurna dan sering melakukan kesalahan. This mismatch must be repaired in order to avoid mutations. ketidaksesuaian ini harus diperbaiki untuk menghindari mutasi. The DNA mismatch repair system recognizes the DNA mismatch and repairs it. Ketidakcocokan sistem perbaikan DNA mengakui ketidakcocokan DNA dan perbaikan itu. Some human genes ( MSH2, MLH1, PMS1, PMS2, and GTBP) have been identified as involved in nucleotide mismatch recognition and repair. [38] Beberapa gen manusia (MSH2, MLH1, PMS1, PMS2, dan GTBP) telah diidentifikasi sebagai terlibat dalam pengakuan mismatch nukleotida dan perbaikan. [38]

Patients with HNPCC do not have defects in the APC gene inherited from their parents. Pasien dengan HNPCC tidak memiliki cacat pada gen APC warisan dari orang tua mereka. Benign tumors (ie, adenomas) develop at the same rate in these patients as in the general population; however, once a patient with HNPCC has an adenoma, it rapidly progresses because of the inherited DNA repair defect. tumor jinak (yaitu, adenoma) mengembangkan pada tingkat yang sama pada pasien seperti dalam populasi umum, namun, sekali seorang pasien dengan HNPCC memiliki adenoma, itu dengan cepat berkembang karena cacat DNA diwariskan perbaikan. Mutations involving tumor suppressor genes and oncogenes rapidly accumulate, and, as a result, only 3-5 years are needed for a benign tumor to progress to cancer. Mutasi yang melibatkan gen supresor tumor dan onkogen cepat menumpuk, dan, sebagai akibatnya, hanya 3-5 tahun yang dibutuhkan untuk tumor jinak untuk berkembang menjadi kanker. FAP may be considered a disease of tumor initiation, whereas HNPCC may be considered a disease of tumor progression. [39] FAP dapat dianggap sebagai penyakit inisiasi tumor, sedangkan HNPCC dapat dianggap sebagai penyakit perkembangan tumor. [39]
Familial Adenomatous Polyposis Keluarga adenomatous poliposis
As mentioned, adenomatous polyps represent a disturbing alteration in the mucosa and have substantial malignant potential. Seperti disebutkan, polip adenomatosa mewakili perubahan mengganggu di mukosa dan memiliki potensi besar ganas. Adenomatous polyps occur in less than 3% of children with polyps. [6] However, familial adenomatous polyposis (FAP) accounts for less than 1% of all colorectal cancer. [19] The criteria for a diagnosis of FAP and, thus, for an increased risk of cancer in children with polyps include the following: polip adenomatosa terjadi dalam waktu kurang dari 3% anak-anak dengan polip. [6] Namun, kekeluargaan adenomatosa poliposis (TPI) menyumbang kurang dari 1% dari semua kanker kolorektal. [19] Kriteria untuk diagnosis FAP dan, dengan demikian, untuk peningkatan risiko kanker pada anak-anak dengan polip adalah sebagai berikut:
More than 5 polyps in the colon Lebih dari 5 polip di usus besar Polyps throughout the GI tract Polip di seluruh saluran pencernaan
Any number of polyps associated with a family history of juvenile polyposis Setiap jumlah polip yang terkait dengan sejarah keluarga poliposis remaja
FAP occurs in approximately 1 per 7000 individuals. [37] The major feature of the syndrome is extensive polyposis, which is defined by at least 100 visible adenomatous polyps in the large intestine. [6] Some patients have thousands of polyps. FAP terjadi pada sekitar 1 per 7000 individu. [37] Ciri utama dari sindrom ini adalah poliposis luas, yang didefinisikan oleh sedikitnya 100 polip adenomatosa terlihat di usus besar. [6] Beberapa pasien memiliki ribuan polip. The rate of development of colorectal carcinoma (CRC) in the third decade of life and after is nearly 90%. [38] Tingkat pengembangan karsinoma kolorektal (CRC) pada dekade ketiga kehidupan dan setelah hampir 90%. [38]
These patients also have a greatly increased risk of upper GI malignancies (eg, duodenal and periampullary adenocarcinomas), thyroid cancer (occurring in 1% of patients with FAP), [40] and hepatoblastoma (occurring in 1 case per 250 persons with FAP, compared with 1 case per

100,000 persons in the general population). [41, 42] Pasien ini juga memiliki peningkatan risiko keganasan sangat GI atas (misalnya, duodenum dan adenocarcinoma periampullary), kanker tiroid (terjadi pada 1% pasien dengan FAP), [40] dan hepatoblastoma (terjadi dalam 1 kasus per 250 orang dengan FAP, dibandingkan dengan 1 kasus per 100.000 orang dalam populasi umum). [41, 42]
FAP has been divided into 2 types: the sparse type and the profuse type. FAP telah dibagi menjadi 2 jenis: jenis jarang dan jenis berlimpah. A relationship between the location of mutations in the gene and the phenotypic expression of FAP has been established. [43] The sparse type of FAP is characterized by hundreds of polyps; the profuse type is characterized by thousands of polyps. Hubungan antara lokasi mutasi pada gen dan ekspresi fenotipik FAP telah didirikan. [43] Jenis jarang dari FAP ini ditandai dengan ratusan polip, tipe berlimpah ditandai oleh ribuan polip. Patients with the profuse type tend to have adenocarcinoma at an earlier age. [6]
In addition, depending on the codons that are mutated within the gene, patients may develop desmoid tumors or congenital hypertrophy of retinal pigment epithelium (CHRPE). [43] Environmental factors may affect manifestations of FAP; identical mutations may result in different phenotypes in different patients. [43] Pasien dengan tipe sebesar-besarnya cenderung memiliki adenokarsinoma pada usia lebih dini. [6] Selain itu, tergantung pada kodon yang bermutasi di dalam gen, pasien dapat mengembangkan tumor bawaan desmoid atau hipertrofi epitel pigmen retina (CHRPE). [43] Faktor lingkungan dapat mempengaruhi manifestasi dari FAP; dapat mengakibatkan mutasi yang berbeda dalam fenotipe yang berbeda. pasien identik [43]
Adenomatous polyps progress through dysplasia to complete transformation. Adenomatosa polip kemajuan melalui displasia untuk menyelesaikan transformasi. Extension of the neoplastic cells into the basement membrane of the colonic epithelium represents carcinoma in situ. Perpanjangan sel-sel neoplastik ke dalam membran basal epitel kolon merupakan karsinoma in situ. Because the colonic mucosa does not contain lymphatics, metastasis does not occur until the tumor invades the submucosa through the muscularis mucosa. Karena mukosa kolon tidak mengandung limfatik, metastasis tidak terjadi sampai tumor menyerang submucosa melalui mukosa muskularis. The duodenal mucosa may also be involved with adenomatous polyps; periampullary adenocarcinoma develops in the duodenal mucosa in 2.9% of patients with FAP. [44] Although gastric polyps may occur in patients with FAP, the polyps are usually benign hamartomas, and no evidence of neoplastic transformation has been reported. [6] The use of capsule endoscopy may play a role in the screening for small intestinal polyps. Mukosa duodenum juga mungkin terlibat dengan polip adenomatosa; adenokarsinoma periampullary berkembang di dalam mukosa duodenum dalam 2.9% dari pasien dengan TPI. [44] Walaupun polip lambung dapat terjadi pada pasien dengan FAP, polip biasanya hamartomas jinak, dan tidak ada bukti transformasi neoplastik telah dilaporkan. [6] Penggunaan endoskopi kapsul mungkin memainkan peran dalam seleksi untuk polip usus kecil.
FAP is inherited as an autosomal dominant trait; a 10% incidence of new mutations is reported. FAP ini diwariskan sebagai sifat dominan autosomal, sebuah kejadian 10% dari mutasi baru dilaporkan. FAP is caused by a deletion in the APC gene on the long arm of chromosome 5. FAP disebabkan oleh delesi pada gen APC di lengan panjang kromosom 5. The APC gene codes for a protein product that acts as a tumor suppressor. [39] Specific genetic alterations have been identified in most of the 30% of patients who do not test positive for mutations in the APC gene

with routine testing. [22] Recent studies indicate the presence of mosaicism in approximately 15% of such cases. [45] Kode gen APC untuk produk protein yang bertindak sebagai penekan tumor. [39]
perubahan genetik tertentu telah diidentifikasi di sebagian besar 30% pasien yang tidak tes positif untuk mutasi pada gen APC dengan pengujian rutin. [22] Studi terbaru menunjukkan adanya mosaicism pada sekitar 15% dari kasus tersebut. [45]
All untreated patients with FAP develop colon cancer. Semua pasien yang tidak diobati dengan FAP mengembangkan kanker usus besar. The average age at which these patients develop cancer is 39 years; malignant transformation occurs by age 20 years in 7% of patients and by age 25 years in 15% of patients. [6] Rata-rata usia di mana pasien tersebut mengembangkan kanker adalah 39 tahun, terjadi transformasi dengan usia 20 tahun di 7% pasien dan pada usia 25 tahun di 15% dari pasien. Ganas [6]
Patients usually present during early adolescence. Pasien biasanya hadir selama masa remaja awal. Approximately 90% are asymptomatic but are identified during routine surveillance because of a family history of FAP. Sekitar 90% tidak menunjukkan gejala tetapi diidentifikasi selama pengawasan rutin karena sejarah keluarga TPI. Some patients present with an increased frequency of defecation, rectal bleeding, anemia, and abdominal pain. Beberapa pasien datang dengan peningkatan frekuensi buang air besar, perdarahan rektum, anemia, dan sakit perut. The diagnosis is confirmed by endoscopic biopsy findings. Diagnosis dikonfirmasi oleh temuan biopsi endoskopik. Most who present with symptoms already have a malignant condition. [6] Because many FAP carriers have few polyps but still develop early colorectal cancer, surgery is indicated even if polyposis does not develop. Kebanyakan yang hadir dengan gejala sudah memiliki kondisi ganas. [6] Karena banyak operator FAP beberapa polip tapi masih mengembangkan kanker kolorektal dini, operasi diindikasikan bahkan jika poliposis tidak berkembang. After prophylactic surgery, carriers require screening of their upper GI tracts and rectums (if rectal mucosa is left in place) to evaluate for malignancy. [38] Surgical removal of the entire colonic mucosa prevents the development of CRC. [9] Setelah operasi profilaksis, pembawa memerlukan penyaringan saluran cerna atas dan rectums (jika mukosa rektum yang tersisa di tempat) untuk mengevaluasi untuk keganasan. [38] Operasi pengangkatan seluruh mukosa kolon mencegah perkembangan CRC. [9]
Total proctocolectomy with permanent ileostomy is not advocated because of the physiologic and psychologic impact of a permanent stoma in a young patient and because of the risk of bladder atony, impotence, and retrograde ejaculation due to destruction of nervi erigentes during the pelvic dissection. [38] Total abdominal colectomy with ileorectal anastomosis is also not ideal because 44% of patients require subsequent treatment for rectal polyps that develop in the remaining mucosa and because the cumulative risk of developing rectal cancer is 10% at age 50 years and 29% by age 60 years. [6] proktokolektomi Total dengan ileostomy permanen tidak dianjurkan karena dampak fisiologis dan psikologis dari stoma permanen pada pasien muda dan karena risiko atoni kandung kemih, impotensi, dan ejakulasi retrograde karena rusaknya erigentes Nervi selama pembedahan panggul. [38 ] kolektomi perut Total dengan anastomosis ileorectal juga tidak ideal karena 44% dari pasien yang memerlukan pengobatan selanjutnya untuk polip dubur yang berkembang di mukosa yang tersisa dan karena risiko kumulatif mengembangkan kanker dubur adalah 10% pada usia 50 tahun dan 29% pada usia 60 tahun. [6]

In a 30-year review of FAP, Nikitin et al found that coloproctectomy with preservation of the anal sphincter and coloproctectomy with ileoanal pull-through resulted in the development of anal canal cancer in 4.1% of patients, whereas 10.7% of patients developed cancer after colectomy with preservation of various colonic segments. [46] They found that occurrence of cancer is not related to sex, age, length of preserved colonic segment, presence of cancer in the removed colonic segment, or postoperative follow-up period. Dalam review 30-tahun FAP, Nikitin et al menemukan bahwa coloproctectomy dengan pelestarian sfingter anal dan coloproctectomy dengan ileoanal pull-melalui menghasilkan perkembangan kanker anal kanal di 4.1% pasien, sedangkan 10,7% pasien kanker dikembangkan setelah kolektomi dengan pelestarian berbagai segmen kolon. [46] Mereka menemukan bahwa terjadinya kanker tidak berhubungan dengan jenis kelamin, umur, panjang segmen kolon diawetkan, kehadiran kanker di segmen kolon dihapus, atau tindak lanjut pasca operasi periode. Presence of polyps in the colonic segments preserved during surgery significantly increased the risk of cancer at a later time. Kehadiran polip di segmen kolon diawetkan selama operasi secara signifikan meningkatkan risiko kanker di lain waktu.
Total colectomy with a rectal mucosectomy and endorectal pull-through (ERPT) is the procedure of choice. [7] Some authors suggest that an ileal reservoir is not absolutely necessary because it increases the risk of pouchitis (23%) and that patients who undergo straight (nonreservoir) pull-through develop a neoreservoir within 24 months, which decreases the frequency of stools. [6] Total kolektomi dengan mucosectomy dubur dan endorectal pull-through (ERPT) adalah prosedur pilihan. [7] Beberapa penulis menyarankan bahwa reservoir ileum tidak mutlak diperlukan karena meningkatkan risiko pouchitis (23%) dan bahwa pasien yang menjalani lurus (nonreservoir) pull-melalui mengembangkan neoreservoir dalam waktu 24 bulan, yang mengurangi frekuensi tinja. [6]
Laparoscopic techniques for total abdominal colectomy with ileorectal anastomosis have been described as safe and effective. [47] Gastroduodenoscopy and flexible endoscopic surveillance of the pelvic pouch must be performed annually in these patients. [19] Rapid growth, induration, severe dysplasia, villous changes, or polyps larger than 1 cm (which presents a much higher chance of having malignant transformation) suggest the need for more aggressive intervention. teknik Laparoskopi untuk perut kolektomi total dengan anastomosis ileorectal telah digambarkan sebagai aman dan efektif. [47] Gastroduodenoscopy dan pengawasan endoskopi fleksibel kantong panggul harus dilakukan setiap tahun pada pasien ini. [19] pertumbuhan yang cepat, indurasi, displasia parah, perubahan vili , atau polip lebih besar dari 1 cm (yang menyajikan kesempatan yang jauh lebih tinggi memiliki transformasi ganas) menyarankan kebutuhan untuk intervensi lebih agresif.
Sulindac (Clinoril), a nonsteroidal anti-inflammatory drug (NSAID), was found to reduce the number of polyps in patients with FAP. [48] However, later studies demonstrated that the effect was only partial and that CRC may still develop. Sulindac (Clinoril), obat anti-inflammatory drugs (NSAID), telah ditemukan untuk mengurangi jumlah polip pada pasien dengan TPI. [48] Namun, kemudian penelitian menunjukkan bahwa efek tersebut hanya parsial dan CRC masih bisa terjadi. Apparently, the mechanism of action is induction of apoptosis in the abnormally proliferating colony of epithelial cells. Rupanya, mekanisme tindakan adalah induksi apoptosis di koloni abnormal berkembang biak sel-sel epitel. Studies with the more specific

cyclooxygenase-2 (COX-2) inhibitors (eg, celecoxib [Celebrex]) have also shown some efficacy. [49] Studi dengan lebih spesifik siklooksigenase-2 (COX-2) inhibitor (misalnya, celecoxib [Celebrex]) juga menunjukkan beberapa keberhasilan miliki. [49]
The American Society of Colon and Rectal Surgeons have published management guidelines and practice parameters for patients with FAP. American Society of Colon dan rektal Bedah telah menerbitkan pedoman pengelolaan dan parameter latihan untuk pasien dengan TPI. Patients with FAP or people with personal or family risk factors for FAP should be referred to center registries and genetic counselors with experience in the multidisciplinary management of these individuals. [50] Pasien dengan FAP atau orang-orang dengan faktor risiko keluarga atau pribadi untuk FAP harus dirujuk ke pusat pendaftar dan konselor genetik dengan pengalaman dalam pengelolaan multidisiplin dari individu-individu. [50]
Hereditary Nonpolyposis Colon Cancer (Lynch Syndrome) Herediter Nonpolyposis Colon Cancer (Lynch Syndrome)
Hereditary nonpolyposis colon cancer (HNPCC) describes a clinical syndrome of colorectal cancer that occurs with early onset and in multiple family members. nonpolyposis kanker usus besar keturunan (HNPCC) menggambarkan suatu sindrom klinis dari kanker kolorektal yang terjadi dengan onset dini dan di beberapa anggota keluarga. In contrast to familial adenomatous polyposis (FAP), HNPCC does not have a specific phenotype, and malignancy develops in the absence of adenomatosis of the colon and rectum. Berbeda dengan poliposis adenomatosa familial (TPI), HNPCC tidak memiliki fenotip tertentu, dan keganasan berkembang dalam ketiadaan adenomatosis dari usus besar dan rektum. Lynch syndrome is the most common hereditary colon cancer syndrome and accounts for about 2-3% of all colorectal cancer cases. [45] The lifetime risk of developing colorectal cancer for patients with Lynch syndrome is 60-80%. [45] sindrom Lynch adalah yang paling umum herediter sindrom kanker usus besar dan menyumbang sekitar 2-3% dari semua kasus kanker kolorektal. [45] Risiko seumur hidup mengembangkan kanker kolorektal pada pasien dengan sindrom Lynch adalah 60-80%. [45]
The expression of the disease may be limited to the colon (Lynch syndrome I) or mat coexist with extracolonic tumors (Lynch syndrome II). [51] These other tumors include endometrial (the second most common after colorectal carcinoma [CRC]), uterine, ovarian, stomach, pancreatic, and genitourinary cancers. [52] They usually manifest in the second decade of life. [38] Patients with Lynch syndrome have a 50% lifetime risk of developing cancer and a 3-fold increased incidence of CRC compared with the general population. Ekspresi penyakit mungkin terbatas pada usus besar (Lynch saya sindrom) atau tikar hidup berdampingan dengan tumor extracolonic (sindroma Lynch II). [51] Tumor lainnya termasuk endometrium (yang kedua yang paling umum setelah karsinoma kolorektal [CRC]), uterus , ovarium, perut, pankreas, dan Genitourinary kanker. [52] Mereka biasanya terwujud dalam dekade kedua kehidupan. [38] Pasien dengan sindrom Lynch memiliki risiko seumur hidup 50% kanker berkembang dan lipat peningkatan kejadian-3 CRC dibandingkan dengan populasi umum. Female patients with Lynch II syndrome should also undergo vaginal ultrasonography, endometrial aspiration, and serum CA-125 assessment annually beginning at age 30 years. [19] pasien wanita dengan sindrom II Lynch juga harus menjalani ultrasonografi vagina, aspirasi endometrium, dan serum CA-125 penilaian setiap tahun dimulai pada usia 30 tahun. [19]

Most CRCs in patients with HNPCC demonstrate microsatellite instability. CRC Sebagian besar pada pasien dengan HNPCC menunjukkan ketidakstabilan mikrosatelit. Lynch used the term replication error positive to describe such tumors. [43, 19] The first genetic cause of the syndrome was identified in chromosome 2; since then, additional loci have been described. Lynch menggunakan istilah kesalahan replikasi positif untuk menggambarkan tumor tersebut. [43, 19] Penyebab genetik pertama dari sindrom itu diidentifikasi pada kromosom 2, sejak itu, lokus tambahan yang telah dijelaskan. More than 90% of these mutations are in 2 genes, MSH2 and MLH1 , which are located on chromosome arms 2p and 3p, respectively. Lebih dari 90% dari mutasi ini berada di 2 gen, MSH2 MLH1, dan yang terletak di lengan kromosom 2p dan 3p, masing-masing. These genes are inherited in a dominant fashion, with 90% penetrance. [51] Patients suspected of carrying the mutation may be tested for mismatch repair gene mutations in commercial laboratories. Gen ini diwariskan secara dominan, dengan penetrasi 90%. [51] Pasien dicurigai melakukan mutasi dapat dites untuk mutasi gen perbaikan mismatch di laboratorium komersial.
HNPCC accounts for approximately 2-5% of all colorectal cancer cases, [43, 19] but these patients reportedly have a better prognosis than those with sporadic CRC. [53] The average age of colorectal cancer onset among HNPCC gene carriers was reported to be 45 years, but recent studies have shown that it appears to be at age 69 years. [54] Synchronous and metachronous tumors are frequent. HNPCC menyumbang sekitar 2-5% dari semua kasus kanker kolorektal, [43,
19] tetapi pasien ini dilaporkan memiliki prognosis lebih baik dibandingkan dengan CRC sporadis. [53] Rata-rata usia onset kanker kolorektal antara pembawa gen HNPCC dilaporkan menjadi 45 tahun, tetapi studi terbaru menunjukkan bahwa tampaknya pada usia 69 tahun. [54] Synchronous dan tumor metachronous sering terjadi.
Patients present with lower stage disease at diagnosis than patients with sporadic CRC, and distant metastases at diagnosis are also less frequent. Pasien datang dengan stadium penyakit saat diagnosis lebih rendah daripada pasien dengan CRC sporadis, dan metastasis jauh di diagnosa juga kurang sering. One possible explanation is that the large number of mutations that accumulate in these cells results in production of abnormal products recognized as foreign by the host. Satu penjelasan yang mungkin adalah bahwa sejumlah besar mutasi yang terakumulasi dalam sel hasil produksi produk abnormal diakui sebagai asing oleh tuan rumah. Alternatively, a high mutation rate may actually hinder tumor dissemination through derangement of functions critical to that process. [53] Atau, tingkat mutasi yang tinggi sebenarnya dapat menghalangi penyebaran tumor melalui kekacauan fungsi penting untuk proses itu. [53]
The Amsterdam criteria for defining HNPCC include the following: [55] Kriteria Amsterdam untuk mendefinisikan HNPCC meliputi: [55]
Onset of colorectal cancer in at least 3 individuals spanning 2 generations Timbulnya kanker kolorektal dalam setidaknya 3 individu yang mencakup 2 generasi
At least one of these individuals is a first-degree relative of the other two Setidaknya satu dari individu-individu ini adalah relatif tingkat pertama dari dua lainnya
At least one of these individuals must have a diagnosis prior to age 50 years Setidaknya satu dari individu-individu ini harus memiliki diagnosis sebelum usia 50 tahun

The stringency of the Amsterdam criteria likely excludes a number of individuals with an inherited predisposition to colorectal cancer. Yang ketat dari kriteria Amsterdam kemungkinan tidak termasuk sejumlah individu dengan predisposisi diwariskan kepada kanker kolorektal. FAP must be excluded. FAP harus dikecualikan. Some patients with this syndrome satisfy the Amsterdam criteria for HNPCC, but their cancer cells do not display MSI-2. Beberapa pasien dengan sindrom ini memenuhi kriteria Amsterdam untuk HNPCC, tetapi sel-sel kanker mereka tidak menampilkan MSI-2. These patients seem to have a distinct form of the syndrome recently referred to as "familial colorectal cancer type X." Pasien ini tampaknya memiliki bentuk yang berbeda dari sindrom baru-baru ini disebut sebagai "jenis kanker familial kolorektal X." They have a lesser risk for colorectal cancer and a later onset. Mereka memiliki resiko yang lebih rendah untuk kanker kolorektal dan onset kemudian. They do not carry the risk for extracolonic malignancies. [56, 19] Mereka tidak membawa risiko keganasan extracolonic. [56, 19]
HNPCC malignancies occur in the cecum and ascending colon more often than in other colorectal sites (70%); they have a higher incidence of poorly differentiated and mucin-producing tumors (signet cell). HNPCC keganasan terjadi pada sekum dan usus ascending lebih sering daripada di situs kolorektal lain (70%), mereka memiliki insiden yang lebih tinggi tumor diferensiasi buruk dan musin-memproduksi (sel meterai). Full colonoscopic screening is recommended biannually, beginning at age 25 years. [57, 19, 58, 59] Lynch proposed treatment with subtotal colectomy rather than hemicolectomy or a segmental resection because the risk of a second or third primary cancer of the colon is 45% over 10 years. skrining colonoscopic Full dianjurkan dua kali setahun, dimulai pada usia 25 tahun. [57, 19, 58, 59] mengusulkan pengobatan Lynch dengan kolektomi subtotal daripada hemicolectomy atau reseksi segmental karena risiko sepertiga primer atau kedua kanker usus besar adalah 45 % lebih dari 10 tahun. Patients who are poorly compliant with colonoscopic surveillance may be candidates for prophylactic colectomy. Pasien yang kurang sesuai dengan surveilans colonoscopic mungkin menjadi kandidat untuk kolektomi profilaksis. Patients who have undergone subtotal colectomy must be informed that they require lifelong endoscopic evaluation of their remaining rectal segment. [43] They also still face the risk of extracolonic cancers. Pasien yang telah mengalami kolektomi subtotal harus diberitahu bahwa mereka memerlukan evaluasi endoskopik seumur hidup segmen yang tersisa dubur mereka. [43] Mereka juga masih menghadapi risiko kanker extracolonic.
Lynch reported that colonic polyps can be identified in as many as 17% of first-degree relatives during colonoscopic screening. Lynch melaporkan bahwa polip kolon dapat diidentifikasi dalam sebanyak 17% dari saudara-saudara tingkat selama pemutaran colonoscopic. Adenomas are more likely to grow and progress to invasive cancer in this patient population than in the general population. Adenoma lebih mungkin untuk tumbuh dan berkembang menjadi kanker invasif pada populasi pasien dibandingkan pada masyarakat umum.
The optimal management strategy for HNPCC gene carriers has yet to be established. Strategi pengelolaan yang optimal untuk pembawa gen HNPCC belum ditetapkan. Evidence suggests that surveillance colonoscopy and polypectomy are effective in reducing the risk of invasive cancer in these patients. [45] It seems wise to advise biannual colonoscopy starting at age 25-30 years and annually after age 40 years. Bukti menunjukkan bahwa colonoscopy pengawasan dan polypectomy efektif dalam mengurangi risiko kanker invasif pada pasien ini. [45] Tampaknya bijak untuk menasihati colonoscopy setiap semester dimulai pada usia 25-30 tahun dan setiap

tahun setelah usia 40 tahun. Currently, experts have not reached consensus regarding the role of prophylactic subtotal colectomy for patients with HNPCC. Saat ini, para ahli belum mencapai konsensus mengenai peran kolektomi subtotal profilaksis untuk pasien dengan HNPCC. Given the high penetrance of the disorder and the high rate of synchronous and metachronous disease among mutation carriers, a strong case may be made for prophylactic colectomy in these patients. Mengingat penetrasi tinggi dari gangguan dan tingkat tinggi penyakit sinkron dan metachronous diantara perusahaan mutasi, kasus yang kuat dapat dibuat untuk kolektomi profilaksis pada pasien ini.
Subtotal colectomy with a rectal mucosectomy and endorectal pull-through (ERPT) has not been studied in this population. Subtotal kolektomi dengan mucosectomy dubur dan endorectal pull-through (ERPT) belum diteliti pada populasi ini. Patients who elect to undergo a subtotal colectomy require colonoscopic surveillance of the remaining rectum. Pasien yang memilih untuk menjalani kolektomi subtotal memerlukan pengawasan colonoscopic dari rektum yang tersisa. Patients who elect not to consider prophylactic surgery must commit to lifelong surveillance. Pasien yang memilih untuk tidak mempertimbangkan operasi profilaksis harus berkomitmen untuk pengawasan seumur hidup. At present, both of these are reasonable management strategies. Saat ini, kedua adalah strategi manajemen yang wajar.
Sporadic Colorectal Carcinoma Sporadis Karsinoma Kolorektal
Adenocarcinoma of the colon and rectum is the most common cancer of the GI tract [60] and has the second highest mortality rate. [1] Approximately 150,000 new cases are diagnosed annually in the United States; less than 1% of which (approximately 80 per year) occur in patients younger than 20 years. [38, 9, 61] Adenokarsinoma dari usus besar dan rektum merupakan kanker yang paling umum pada saluran GI [60] dan memiliki angka kematian tertinggi kedua. [1] Sekitar 150.000 kasus baru didiagnosa setiap tahun di Amerika Serikat; kurang dari 1% di antaranya (sekitar 80 per tahun) terjadi pada pasien yang lebih muda dari 20 tahun. [38, 9, 61]
In children, colorectal cancer is the second most common cancer of the alimentary tract after liver tumors; the incidence of colorectal cancer is 1.3-2 cases per million population. [60, 62] Most patients present during the second decade of life. [60, 63, 64] The youngest patient ever reported was aged 9 months. [65] Children are more likely than adults to have advanced-stage at presentation, as well as unfavorable tumor histology (mucinous), which confers them a poor outcome. [66, 65] Pada anak-anak, kanker kolorektal merupakan kanker yang paling umum kedua saluran pencernaan setelah tumor hati; insiden kanker kolorektal adalah 1,3-2 kasus per juta penduduk. [60, 62] Kebanyakan pasien hadir selama dekade kedua kehidupan. [60 , 63, 64] Pasien termuda dilaporkan berusia 9 bulan. [65] Anak-anak lebih mungkin dibandingkan orang dewasa untuk memiliki stadium lanjut pada presentasi, serta histologi tumor tidak menguntungkan (mucinous), yang memberikan mereka hasil yang buruk. [ 66, 65]
The development of carcinoma of the colon appears to be associated with several predisposing factors, as follows: Perkembangan karsinoma usus besar tampaknya dikaitkan dengan beberapa faktor predisposisi, sebagai berikut:
Familial polyposis syndromes poliposis sindrom familial

Hereditary nonpolyposis syndromes nonpolyposis herediter sindrom
Inflammatory bowel disease(ulcerative colitis) Radang usus (kolitis ulserativa)
Previous ureterosigmoidostomy Sebelumnya ureterosigmoidostomy
Previous radiation therapy Sebelumnya terapi radiasi
Possible exposure to environmental chemicals and radiation Kemungkinan paparan bahan kimia lingkungan dan radiasi
Another predisposing factor may be a diet high in fat and cholesterol and low in fiber because fecal material in the bowel of patients consuming low-fiber diets has a long transit time; however, this association has not been supported in children. Faktor lain mungkin predisposisi diet tinggi lemak dan kolesterol dan rendah serat karena bahan tinja dalam usus pasien mengkonsumsi diet rendah serat memiliki waktu transit yang lama, namun asosiasi ini belum didukung pada anak-anak.
Approximately 75% of patients present with sporadic cases, 10-20% of patients have familial colon cancer without a defined genetic pattern, and 1% of patients have a genetic polyposis syndrome. [39] The oncogene β-catenin has been identified in 15% of colorectal adenocarcinomas. Sekitar 75% dari pasien datang dengan kasus sporadis, 10-20% dari pasien kanker usus besar keluarga tanpa pola genetik didefinisikan, dan 1% pasien memiliki sindrom poliposis genetik. [39] The β onkogen-catenin telah diidentifikasi di 15 % dari adenokarsinoma kolorektal. β-catenin creates a dedifferentiated stem cell–like phenotype of cell that remains in a state of constant proliferation, which is an important contributor of cancer invasion and metastasis. β-catenin menciptakan fenotipe induk dedifferentiated seperti sel-sel yang masih dalam keadaan proliferasi konstan, yang merupakan kontributor penting dari invasi kanker dan metastasis. The serum protease, urokinase plasminogen activator (uPA) initiates a cascade of proteolytic steps that degrade the extracellular matrix, playing a role in adhesion, migration, invasion, and intravasation. The protease serum, urokinase plasminogen aktivator (UPA) memulai langkah proteolitik riam yang mendegradasi matriks ekstraselular, memainkan peran dalam adhesi, migrasi, invasi, dan intravasation. It is a coordinator of cell growth and, when found in the tumor cells, indicates aggressive tumor growth and poor patient survival. Ini adalah koordinator pertumbuhan sel dan, saat ditemui di sel-sel tumor, menunjukkan pertumbuhan tumor agresif dan kelangsungan hidup pasien miskin.
In patients with sporadic colorectal carcinoma (CRC), 1% are secondary to inflammatory bowel disease, and 5-6% present with hereditary nonpolyposis syndromes. Pada pasien dengan karsinoma kolorektal sporadis (CRC), 1% adalah sekunder terhadap penyakit radang usus, dan 5-6% hadir dengan sindrom nonpolyposis turun temurun. A clear-cut association and progressively increasing likelihood of colon cancer is observed in patients with ulcerative colitis (UC); the risk is 20-fold higher than in the general population and is related to the length of time with UC, [67, 68]
increasing 1-2% per year after 10 years. A-potong asosiasi jelas dan semakin meningkatkan kemungkinan kanker usus besar yang diamati pada pasien dengan radang borok usus besar (UC), risikonya adalah 20 kali lipat lebih tinggi dari pada populasi umum dan berhubungan dengan panjang waktu dengan UC, [67, 68 ] meningkat 1-2% per tahun setelah 10 tahun. The patient's age and the extent of disease at diagnosis are strong independent risk factors for colorectal cancer in

UC. Usia pasien dan sejauh mana penyakit pada diagnosis merupakan faktor risiko yang kuat independen untuk kanker kolorektal di UC. Cancer risk is higher for patients with childhood-onset inflammatory bowel disease than patients who develop the disease during adulthood. Kanker risiko lebih tinggi untuk pasien dengan anak-onset penyakit radang usus dibandingkan pasien yang mengalami penyakit ini selama dewasa. Reports give a cumulative incidence of 5-10% at age 20 years and 12-20% at age 30 years. [69] Laporan memberikan kejadian kumulatif dari% 5-10 pada usia 20 tahun dan 12-20% pada usia 30 tahun. [69]
Ulcerative proctitis likely does not increase the risk of colonic or rectal cancer. [69] The current practice of surveillance and early surgery may have and impact on prognosis. [70] Ulcerative proctitis kemungkinan tidak meningkatkan risiko kanker kolon atau dubur. [69] Praktek saat surveilans dan operasi dini mungkin memiliki dan berdampak pada prognosis. [70]
In patients with ulcerative colitis who develop colon cancer, the cancer usually occurs at a young age, and synchronous tumors are prevalent. Pada pasien dengan radang borok usus besar yang mengembangkan kanker usus besar, kanker biasanya terjadi pada usia muda, dan tumor sinkron yang lazim. Furthermore, patients with colitis involving the entire colon are more likely to develop cancer than those with left-sided colitis only; in these patients, the risk of cancer begins to increase 15-20 years after the onset of symptoms. [71] Patients with ulcerative colitis who develop colonic strictures should be considered to have carcinomas until proven otherwise, and a stricture in these patients is an indication for surgical intervention. [7] In a report by Lashner, 11 of 15 patients with strictures were found to have carcinomas on biopsy findings. [68] Lebih lanjut, pasien dengan kolitis yang melibatkan seluruh usus besar lebih mungkin mengembangkan kanker dibanding mereka dengan kolitis sisi kiri saja; pada pasien, risiko kanker mulai meningkat 15-20 tahun setelah timbulnya gejala. [71] Pasien dengan radang borok usus besar yang mengalami penyempitan kolon harus dipertimbangkan untuk memiliki karsinoma sampai terbukti sebaliknya, dan striktur pada pasien ini merupakan indikasi untuk intervensi bedah. [7] Dalam sebuah laporan oleh Lashner, 11 dari 15 pasien dengan penyempitan ditemukan memiliki karsinoma pada biopsi temuan. [68]
Patients who have had the disease for a minimum of 7 years should undergo surveillance endoscopy at least every other year. [7] Colectomy is indicated for the following reasons: [69] Pasien yang memiliki penyakit ini selama minimal 7 tahun harus menjalani endoskopi surveilans paling tidak setiap tahun lainnya. [7] colectomy diindikasikan untuk alasan berikut: [69]
A macroscopic lesion with overlying low-grade dysplasia Sebuah lesi makroskopik dengan atasnya dysplasia tingkat rendah
A low-grade dysplasia in multiple foci Sebuah dysplasia tingkat rendah di beberapa foci
Persistent unifocal low-grade dysplasia found on repeated examinations Persistent displasia ringan unifocal ditemukan pada pemeriksaan ulang
High-grade dysplasia High-grade displasia
In patients with Crohn disease, the risk for colon cancer is 20 times greater than that in the general population; this risk is also related to the amount of bowel involved. Pada pasien dengan penyakit Crohn, risiko untuk kanker usus besar adalah 20 kali lebih besar daripada dalam

populasi umum, risiko ini juga terkait dengan jumlah usus yang terlibat. These patients are also at increased risk to develop lymphoma and small intestinal tumors. [70] Their colorectal cancer risk probably results from chronic inflammation or dysplastic rectal mucosa (left after surgery), and surveillance is important in such cases. [6] Contrast enemas and colonoscopy are the mainstays of surveillance. Pasien-pasien ini juga pada peningkatan risiko untuk mengembangkan limfoma dan tumor usus kecil. [70] mereka kolorektal resiko kanker mungkin hasil dari peradangan kronis atau mukosa dubur displastik (kiri setelah operasi), dan pengawasan adalah penting dalam kasus tersebut. [6] Kontras enema dan kolonoskopi adalah andalan surveilans. Biopsies should be performed on suspicious areas and should also be performed randomly during the colonoscopy. Biopsi harus dilakukan pada daerah yang mencurigakan dan juga harus dilakukan secara acak selama colonoscopy tersebut. The risk for cancer in patients with Crohn disease is less frequent than in patients with chronic ulcerative colitis. [72] Some malignancies related to inflammatory bowel disease might be secondary to immunomodulation therapy used to treat the latter. Risiko kanker pada pasien dengan penyakit Crohn kurang sering dibandingkan pada pasien dengan radang borok usus besar kronis. [72] Beberapa penyakit berbahaya yang berhubungan dengan penyakit radang usus mungkin sekunder terhadap terapi immunomodulation digunakan untuk mengobati kedua.
Patients who undergo urinary diversion with ureterosigmoidostomy are at risk for the development of colon cancer (5% of patients), likely because of chronic inflammation caused by the mixture of feces and urine at the implant site. [73] Although many types of urinary diversion have been described, almost all of them include an intestinal segment as a reservoir. Pasien yang menjalani diversi urin dengan ureterosigmoidostomy beresiko untuk perkembangan kanker usus besar (5% dari pasien), mungkin karena peradangan kronis yang disebabkan oleh campuran kotoran dan air seni di lokasi implan. [73] Meskipun banyak jenis diversi urin telah dijelaskan, hampir semua dari mereka termasuk segmen usus sebagai reservoir. An exception is ureterostomy, in which the ureters open directly on the skin; however, these are not continent, are difficult to care for, and tend to stenose frequently. Kekecualian adalah ureterostomy, di mana ureter terbuka langsung pada kulit, namun, ini tidak benua, sulit untuk merawat, dan cenderung stenose sering. The Bricker diversion includes an ileal conduit as a reservoir and has been used worldwide after cystectomy for cancer. Pengalihan Bricker mencakup saluran ileum sebagai reservoir dan telah digunakan di seluruh dunia setelah kistektomi untuk kanker.
Another option for diversion is the Mainz 2 pouch, which uses a sigmoid pouch as a reservoir, in which the ureters are implanted with an antireflux mechanism. Pilihan lain untuk pengalihan adalah Mainz 2 kantong, yang menggunakan kantong sigmoid sebagai reservoir, di mana ureter yang tertanam dengan mekanisme antireflux. This seems to decrease the incidence of cancer in the colonic segment, which always presents at the site of the ureteral implant and is believed to be secondary to the carcinogenic effect of nitrosamines present in the infected urine secondary to reflux. Hal ini tampaknya untuk menurunkan kejadian kanker di segmen kolon, yang selalu menyajikan di lokasi implan saluran kemih dan diyakini menjadi sekunder untuk efek karsinogenik nitrosamin hadir dalam urin yang terinfeksi sekunder refluks.
Children with other abdominal malignancies who have received radiation therapy also have an increased risk for early development of colorectal cancer in the radiation field as a second malignant condition. Anak-anak dengan keganasan perut lain yang telah menerima terapi radiasi

juga memiliki peningkatan risiko untuk pengembangan awal kanker kolorektal di medan radiasi sebagai kondisi ganas kedua. This is likely because of a mutation in the P53 gene caused by radiation, which, in turn, leads to the neoplasm. [63, 74] The Children's Oncology Group screening guidelines recommend that children and adolescents who receive 30 Gy or more of pelvic radiotherapy be screened for colorectal cancer after 10 years or at age 35 years, whichever is later. Hal ini mungkin karena mutasi pada gen P53 yang disebabkan oleh radiasi, yang, pada gilirannya, menyebabkan neoplasma tersebut. [63, 74] Anak-anak Oncology Group pedoman skrining merekomendasikan bahwa anak-anak dan remaja yang menerima Gy atau lebih dari panggul radioterapi 30 diputar untuk kanker kolorektal setelah 10 tahun atau pada usia 35 tahun, mana yang kemudian. Some authors recommend shortening this screening period for certain patients. [66] Beberapa penulis menyarankan memperpendek periode ini penyaringan untuk pasien tertentu. [66]
Several case reports have come from the central Mississippi Valley, where some patients had been exposed to pesticides and herbicides; however, a clear-cut relationship between the exposure and the development of colorectal cancer could not be established because the levels of pesticide residues were no higher in these patients and their families than in control subjects. [75] Familial multiple cancer syndromes and Bloom syndrome are also predisposing pathologies that increase the risk of colorectal cancer in the pediatric population. [76] Beberapa laporan kasus berasal dari Mississippi Valley pusat, di mana beberapa pasien telah terpapar dengan pestisida dan herbisida, namun hubungan yang jelas antara eksposur dan perkembangan kanker kolorektal tidak dapat ditentukan karena tingkat residu pestisida ada lebih tinggi pada pasien dan keluarga mereka dibanding subyek kontrol. [75] beberapa sindrom kanker familial dan sindrom Bloom juga predisposisi patologi yang meningkatkan risiko kanker kolorektal pada populasi anak-anak. [76]
Colorectal cancer in pediatric patients is associated with a significantly worse survival rate than in adults; this is likely because of delayed diagnosis, advanced clinical stage at presentation, and increased incidence of high-grade tumors. Kanker kolorektal pada pasien pediatrik dikaitkan dengan tingkat kelangsungan hidup secara signifikan lebih buruk dari pada orang dewasa, ini mungkin karena diagnosis tertunda, lanjut stadium klinis pada presentasi, dan peningkatan kejadian tumor grade tinggi. Approximately 60-86% of pediatric and adolescent patients have Dukes stage C or D. [66] The increased frequency of mucinous variety and the preponderance of right-sided lesions contribute to the advanced stage at diagnosis. [60, 77] Sekitar 60-86% dari pasien anak-anak dan remaja memiliki tahap Dukes C atau D. [66] Frekuensi meningkat varietas mucinous dan dominan sisi lesi hak berkontribusi pada stadium lanjut saat diagnosis. [60, 77]
Epidemiology Epidemiologi
In adults, colorectal cancer is the second leading cause of cancer death in the Western world. [78] It is rare in populations with limited meat intake; therefore, it is less common in Africa and Asia. [38, 79] In children and adolescents, these tumors may occur in any site in the large bowel and are not usually associated with a family history of colon cancer. [60, 75, 80, 81, 79] No sex predilection is reported. Pada orang dewasa, kanker kolorektal merupakan penyebab kedua kematian kanker di dunia Barat. [78] Hal ini jarang terjadi di populasi dengan konsumsi daging terbatas, karena itu, kurang umum di Afrika dan Asia. [38, 79] Pada anak-anak dan remaja, tumor ini dapat terjadi dalam

setiap situs dalam usus besar dan tidak biasanya berhubungan dengan riwayat keluarga kanker usus besar. [60, 75, 80, 81, 79] Tidak ada predileksi seks dilaporkan.
Pathology Patologi
Colon cancer is triggered by a series of point mutations and genetic alterations that progressively cause normal cells to transform into adenomas that could become progressively dysplastic, resulting in carcinoma foci. [82] These mutations occur in a certain sequence that can determine the clinical characteristics of the tumor. Kanker usus besar dipicu oleh serangkaian mutasi titik dan perubahan genetik yang semakin menyebabkan sel normal berubah menjadi adenoma yang dapat menjadi semakin displastik, mengakibatkan karsinoma fokus. [82] Mutasi ini terjadi dalam urutan tertentu yang dapat menentukan karakteristik klinis tumor.
Colorectal cancer arises from the mucosal surface of the bowel, generally at the site of an adenomatous overgrowth or polyp. Kanker usus besar muncul dari permukaan mukosa usus, umumnya di lokasi pertumbuhan berlebih adenomatosa atau polip. The tumor may penetrate the bowel wall and may even perforate the serosa into the omental fat, lymph nodes, liver, ovaries, and other loops of bowel. Tumor dapat menembus dinding usus dan bahkan mungkin perforasi yang serosa ke dalam lemak omentum, kelenjar getah bening, hati, ovarium, dan loop lainnya dari usus. Some lesions may obstruct the bowel lumen. Beberapa lesi dapat menghambat lumen usus. More than one cancer may be present. Lebih dari satu kanker mungkin ada. Multiple lesions may have the same or different histology and may have the same or different stages of development. Beberapa lesi mungkin memiliki histologi yang sama atau berbeda dan mungkin memiliki tahap yang sama atau berbeda pembangunan. Carcinoma in situ may occur in one or more polyps. Karsinoma in situ dapat terjadi dalam satu atau lebih polip. Patients with synchronous primary tumors have the same prognosis as patients with single colon cancers. [83] Pasien dengan tumor primer sinkron memiliki prognosis yang sama dengan pasien dengan kanker usus besar tunggal. [83]
The epidermal growth factor receptor (EGFR), is a tyrosine kinase receptor abnormally expressed and activated in colorectal cancer cells (72-82%). Reseptor faktor pertumbuhan epidermal (EGFR), adalah reseptor tirosin kinase diungkapkan dan diaktifkan abnormal pada sel-sel kanker kolorektal (72-82%). It initiates signal transduction cascades promoting cell division, migration, angiogenesis, and inhibiting apoptosis. [78] Thus, EGFR plays an important role in the pathogenesis of colorectal cancer. Ini memulai kaskade transduksi sinyal mempromosikan pembelahan sel, migrasi, angiogenesis, dan menghambat apoptosis. [78] Dengan demikian, EGFR memainkan peran penting dalam patogenesis kanker kolorektal. Its expression is associated with poor survival and increased risk of invasion metastasis. ekspresi adalah dikaitkan dengan ketahanan hidup miskin dan meningkatkan risiko metastasis invasi. Italiano et al demonstrated EGFR expression by immunohistochemistry in colorectal cancer metastatic cells. [78] Monoclonal antibodies and low molecular weight tyrosine kinase inhibitors may become important in the therapeutic armamentarium for patients with colorectal cancer. Italiano et al menunjukkan EGFR ekspresi oleh imunohistokimia dalam sel-sel kanker kolorektal metastatik. [78] antibodi monoklonal dan berat molekul rendah tirosin kinase inhibitor dapat menjadi penting dalam armamentarium terapi untuk pasien dengan kanker kolorektal.

A rare morphological form or "flat-type" colorectal tumor has been reported; this form tends to be more aggressive, and, despite the small size of the tumor, it shows high-grade dysplasia and progresses rapidly to invasive cancer. Bentuk morfologi langka atau "flat-type" tumor kolorektal telah dilaporkan; formulir ini cenderung lebih agresif, dan, meskipun ukuran kecil tumor, hal itu menunjukkan displasia bermutu tinggi dan berkembang dengan cepat untuk kanker invasif. Inactivation of p53 and 17p-LOH have been described in this tumor. [84] Because these tumors are derived from endoderm, all cytologic characteristics are those of carcinomas. Inaktivasi p53 dan 17p-LOH telah dijelaskan dalam tumor ini. [84] Karena tumor ini berasal dari endoderm, semua karakteristik sitologi adalah dari karsinoma. They may be well or poorly differentiated and contain pools of mucin. Mereka mungkin baik atau buruk dibedakan dan berisi genangan musin. Mucin-producing or signet ring adenocarcinoma is the predominant cell type; it occurs in 50% of pediatric cases compared with a 5% occurrence reported in adults. [85] These tumors may become huge. memproduksi atau cincin cap adenocarcinoma-musin adalah jenis sel yang dominan, melainkan terjadi pada 50% kasus pediatrik dibandingkan dengan 5% kejadian dilaporkan pada orang dewasa. [85] Tumor ini dapat menjadi besar. The differential diagnosis includes malignant carcinoid, leiomyosarcoma, malignant fibrous histiocytoma, and metastatic tumor from other sites. Diagnosis diferensial meliputi karsinoid ganas, leiomyosarcoma, histiocytoma berserat ganas, dan tumor metastasis dari situs lain.
In a series reported by LaQuaglia, the interval from symptom onset to diagnosis was not a significant predictor of mortality; however, tumor grade was a predictor. [63] Signet ring tumors behave more aggressively and are associated with earlier penetration of the bowel wall and extension along peritoneal surfaces, which suggests more aggressive tumor biology. Dalam seri yang dilaporkan oleh LaQuaglia, interval dari munculnya gejala untuk diagnosis tidak merupakan prediktor yang signifikan dari kematian, namun grade tumor adalah prediktor. [63] tumor cincin meterai bersikap lebih agresif dan berkaitan dengan penetrasi sebelumnya dinding usus dan ekstensi sepanjang permukaan peritoneal, yang menunjukkan biologi tumor lebih agresif. The mucin absorbs water, swells, and invades tissues, thus promoting spread of malignant cells. musin menyerap air, membengkak, dan menyerang jaringan, sehingga mempromosikan penyebaran sel-sel ganas. Mucin also interferes with the mucopolysaccharide-coating immune recognition of carcinoma cells. [76] Children have a worse prognosis when compared with adult patients who are at the same disease stage. [66] Musin juga mengganggu lapisan-mucopolysaccharide pengakuan kekebalan sel karsinoma. [76] Anak-anak memiliki prognosis yang lebih buruk bila dibandingkan dengan pasien dewasa yang berada pada tahap penyakit yang sama. [66]
Clinical presentation Presentasi klinis
Signs and symptoms may be absent or innocuous. Tanda dan gejala mungkin tidak ada atau tidak berbahaya. However, almost all children present with abdominal pain, and 40-70% have nausea and vomiting. Namun, hampir semua anak hadir dengan sakit perut, dan 40-70% mengalami mual dan muntah. Most (76%) [66] also have altered bowel habits and weight loss. Sebagian besar (76%) [66] juga telah mengubah kebiasaan buang air besar dan penurunan berat badan. Due to its rarity, colorectal cancer is frequently overlooked in the differential diagnosis of these symptoms in children. [86] Unlike in adults, colorectal cancer in children is evenly distributed throughout the colon, with a third of the lesions located in the ascending colon. [60, 63] Karena kelangkaannya,

kanker kolorektal sering diabaikan dalam diagnosis diferensial dari gejala-gejala pada anak-anak. [86] Tidak seperti pada orang dewasa, kanker kolorektal pada anak-anak secara merata di seluruh usus besar, dengan sepertiga dari lesi terletak di usus besar naik. [60, 63]
The signs and symptoms of colorectal cancer are related to its primary site within the large bowel. Tanda-tanda dan gejala kanker kolorektal berhubungan dengan situs utama di dalam usus besar. Tumors involving the cecum and ascending colon, which may be associated with familial colon carcinoma, may develop large masses before symptoms appear. Tumor yang melibatkan sekum dan kolon ascending, yang mungkin berhubungan dengan kanker usus besar keluarga, dapat mengembangkan massa yang besar sebelum gejala muncul.
Constipation or diarrhea and change in the caliber of stools are more common with left-sided lesions and may present before the development of tarry stools or rectal bleeding, which is observed in a third of the patients. Sembelit atau diare dan perubahan kaliber tinja yang lebih umum dengan lesi sisi kiri dan mungkin ada sebelum perkembangan tinja tinggal atau perdarahan dubur, yang diamati dalam sepertiga dari pasien. Patients with tumors of the rectum and sigmoid may present with changes in the caliber of stools or hematochezia. Pasien dengan tumor rektum dan sigmoid dapat hadir dengan perubahan kaliber kotoran atau hematochezia. Approximately 20-30% of patients have anorexia and weight loss. [6] Sekitar 20-30% dari pasien memiliki berat badan dan anoreksia. [6]
Clinical and laboratory investigation Klinis dan pemeriksaan laboratorium
In the absence of rectorrhagia or hematochezia, patients may test positive for occult blood in the stool; however, screening for fecal occult blood has not proven to be of significant value for the treatment of pediatric patients. [38] Hepatic function abnormalities may be related to metastatic involvement of the liver. Dalam ketiadaan rectorrhagia atau hematochezia, pasien mungkin tes positif untuk darah yang tersembunyi dalam tinja, namun screening untuk darah yang tersembunyi tinja tidak terbukti dari nilai yang signifikan untuk pengobatan pasien anak. [38] kelainan fungsi hati mungkin terkait keterlibatan metastatis hati. Anemia is due to blood loss or malnutrition. Anemia karena kehilangan darah atau gizi buruk. Although fewer than 75% of the colon carcinomas in children produce carcinoembryonic antigen (CEA), levels of this protein should be determined. Meskipun kurang dari 75% dari karsinoma usus besar pada anak-anak menghasilkan antigen Carcinoembryonic (CEA), kadar protein ini harus ditentukan. CEA may be a useful tool in identifying recurrent disease after resection. [7] CEA dapat menjadi alat yang berguna dalam mengidentifikasi penyakit berulang setelah reseksi. [7]
Imaging studies Studi-studi imaging
Conventional radiographic studies include barium enema with air contrast to define the tumor and the remainder of the colon. studi radiografi konvensional termasuk barium enema dengan kontras udara untuk menentukan tumor dan sisa dari usus besar. Abdominal and chest CT scanning may define areas of spread to the liver, lungs, or enlarged lymph nodes, as well as pelvic metastases, especially to the ovaries. Perut dan dada CT scan dapat menentukan area menyebar ke hati, paru-paru, atau pembesaran kelenjar getah bening, serta metastasis panggul, khususnya ovarium. colorectal cancer has the ability to metastasize through various routes,

including transmural invasion and spread by continuity, intraluminal extension, and hematogenous, lymphatic, and transperitoneal routes. kanker kolorektal memiliki kemampuan untuk bermetastasis melalui berbagai rute, termasuk invasi transmural dan disebarkan oleh kontinuitas, ekstensi intraluminal, dan rute hematogenous, limfatik, dan transperitoneal. Kaste et al analyzed 32 patients with peritoneal metastatic implants from different primary tumors and found that 22% of these patients had colorectal cancer. [87] Kaste dkk dianalisis 32 pasien dengan implan peritoneal metastasis dari tumor primer yang berbeda dan menemukan bahwa 22% dari pasien kanker kolorektal. [87]
CT scanning may be unable to detect intra-abdominal metastases because of lesion size, paucity of intra-abdominal fat, contiguity with the primary tumor, ascites, implant location, and adequacy of bowel opacification. CT scan mungkin tidak dapat mendeteksi metastase intra-abdomen karena ukuran lesi, kekurangan lemak intra-abdominal, kedekatan dengan tumor primer, asites, lokasi implan, dan kecukupan kekeruhan usus. Current CT scanners are able to detect implants as small as 5 mm in diameter. Lancar CT scanner mampu mendeteksi implan sekecil diameter 5 mm. MRI may further improve detection. MRI lebih lanjut dapat meningkatkan deteksi.
Colonoscopy is useful in locating the site of lesions within the large bowel. Colonoscopy berguna dalam mencari lokasi lesi dalam usus besar. The entire length of the colon should be evaluated. Seluruh panjang usus besar harus dievaluasi. Transrectal ultrasonography may help determine the extent of invasion and resectability of rectosigmoid cancer. ultrasonografi transrectal dapat membantu menentukan tingkat invasi dan resectability kanker rectosigmoid. Intraoperative ultrasonography of the liver may reveal metastasis not observed with other imaging studies. [7] Radioisotope studies should include a bone scan; if results are positive, bone marrow aspiration and biopsy are indicated to determine spread to the marrow. Intrabedah ultrasonografi hati dapat mengungkapkan metastasis tidak diamati dengan studi pencitraan lain. [7] Radioisotop studi harus mencakup tulang scan, jika hasilnya positif, aspirasi sumsum tulang dan biopsi yang ditunjukkan untuk menentukan menyebar ke sumsum.
Staging Pementasan
In 1932, Cuthbert Esquire Dukes, the Director of the Research Laboratory at St. Mark's Hospital in London, indicated that growth of colorectal cancers followed an orderly and predictable fashion. [88] He created a staging classification system that was later modified in 1954 by Astler and Coller. [89] The extent of the disease is determined using the modified Dukes staging scheme. Pada tahun 1932, Cuthbert Esquire Dukes, Direktur Laboratorium Penelitian di St Mark's Hospital di London, menunjukkan bahwa pertumbuhan kanker kolorektal menyusul dan diprediksi secara teratur. [88] Dia menciptakan sebuah sistem klasifikasi pementasan yang kemudian diubah pada tahun 1954 oleh Astler dan Coller. [89] Luasnya penyakit ditentukan dengan menggunakan skema Dukes staging dimodifikasi. According to this classification, in stage A, only the mucosa and submucosa are affected; in stage B, the disease is limited to the bowel wall; in stage C, the disease is limited to the lymph nodes; and in stage D, the patient has distant metastases, peritoneal implants, direct invasion of other viscera, or surgically unresectable tumors. Menurut klasifikasi ini, pada tahap A, hanya mukosa dan submucosa terpengaruh, dalam tahap B, penyakit ini terbatas pada dinding usus, dalam tahap C, penyakit ini

terbatas pada kelenjar getah bening, dan dalam tahap D, pasien telah metastasis jauh, implan peritoneal, invasi langsung dari jeroan lain, atau operasi tumor dioperasi.
Tumor, node, metastases (TNM) staging of colorectal cancer is as follows: Tumor, node, metastasis (TNM) stadium dari kanker kolorektal adalah sebagai berikut:
Primary tumor Tumor primer
TX: Primary tumor cannot be assessed. TX: tumor primer tidak dapat dinilai. T0: No evidence of primary tumor is present. T0: Tidak ada bukti tumor primer hadir.
Tis: Carcinoma in situ is present. Tis: Carcinoma in situ hadir.
T1: Tumor cells invade the submucosa. T1: Tumor menginvasi sel submucosa tersebut.
T2: Tumor cells invade the muscularis propria. T2: Tumor menginvasi sel propria muskularis.
T3: Tumor cells invade the muscularis propria and penetrate into subserosa or into nonperitonealized pericolic or perirectal tissues. T3: Tumor menginvasi sel propria muskularis dan menembus ke subserosa atau ke jaringan pericolic atau perirectal nonperitonealized.
T4: Tumor cells perforate the visceral peritoneum or directly invade other organs or structures. T4: Tumor sel perforasi peritoneum viseral atau langsung menyerang organ lain atau bangunan.
Nodal involvement Nodal keterlibatan
NX: Regional lymph nodes cannot be assessed. NX: Daerah kelenjar getah bening tidak dapat dinilai.
N0: No evidence of regional lymph node metastasis is present. N0: Tidak ada bukti dari metastasis kelenjar getah bening regional hadir.
N1: Metastasis in 1-3 pericolic or perirectal lymph nodes is present. N1: Metastasis pada 1-3 kelenjar getah bening pericolic atau perirectal hadir.
N2: Metastasis in 4 or more pericolic or perirectal lymph nodes is observed. N2: Metastasis dalam 4 atau lebih kelenjar getah bening pericolic atau perirectal diamati.
N3: Metastasis in any lymph node along the course of a named vascular trunk is present. N3: Metastasis dalam kelenjar getah bening di sepanjang perjalanan batang vaskular bernama hadir.
Distant metastasis Jauh metastasis
MX: Presence of distant metastasis cannot be assessed. MX: Kehadiran metastasis jauh tidak dapat dinilai.
M0: No evidence of distant metastasis is observed. M0: Tidak ada bukti dari metastasis jauh yang diamati.
M1: Distant metastasis is present. M1: metastasis Jauh hadir.

Modified duke staging is as follows: pementasan duke Modified adalah sebagai berikut:
Stage 0 Tahap 0
Tis Tis N0 N0
M0 M0
A A
Stage 1 Tahap 1
T1 T1 N0 N0
M0 M0
A A
T2 T2
N0 N0
M0 M0
B1 B1
Stage 2 Tahap 2
B2 B2 T4 T4
N0 N0
M0 M0
B3 B3
Stage 3 Tahap 3
Any T Setiap T N1 N1
M0 M0
C C
Any T Setiap T
N2,N3 N2, N3

M0 M0
C C
Stage 4 Tahap 4
Any T Setiap T Any N Setiap N
M1 M1
D D
Treatment Pengobatan
General surgical principles apply. Prinsip umum bedah berlaku. Biopsy findings are required to confirm the diagnosis of colorectal cancer. Temuan Biopsi diperlukan untuk mengkonfirmasi diagnosis kanker kolorektal. A biopsy sample can be obtained with colonoscopy, laparoscopy, or laparotomy. [90] Staging procedures include performing a biopsy of known enlarged lymph nodes, a biopsy of the ovaries in female patients, a resection of the omentum, and a biopsy of the liver. Contoh biopsi dapat diperoleh dengan colonoscopy, laparoskopi, atau laparotomi. [90] Staging prosedur termasuk melakukan biopsi yang diketahui pembesaran kelenjar getah bening, biopsi dari ovarium pada pasien wanita, sebuah reseksi omentum, dan biopsi hati . Ligating the mesenteric vein that drains the tumor area early during surgery before manipulating the tumor is important to avoid cellular dissemination. Ligating vena mesenterika yang mengalir daerah tumor awal selama operasi sebelum memanipulasi tumor ini penting untuk menghindari penyebaran selular.
When the tumor is confined to the cecal area or right colon, a right hemicolectomy is performed; if the lesions are located from the splenic flexure to the sigmoid colon, a left hemicolectomy is performed. Ketika tumor terbatas pada daerah cecal atau usus besar kanan, hemicolectomy hak dilakukan, jika lesi terletak dari lentur lienalis ke kolon sigmoid, sebuah hemicolectomy kiri dilakukan. Low anterior resections may be performed in patients with tumors located 5 cm above the anal verge. reseksi anterior rendah dapat dilakukan pada pasien dengan tumor terletak 5 cm di atas ambang dubur. If present, liver metastases may be resected at the time of intestinal resection or at a later time. Jika ada, metastasis hati mungkin resected pada saat reseksi usus atau di lain waktu. Lobectomy is not necessary if margins can be preserved, with a lesser resection if 1.5 cm of normal liver parenchyma margin is preserved. [7] Lobektomi tidak diperlukan jika margin dapat dilestarikan, dengan reseksi yang lebih rendah jika 1,5 cm margin parenkim hati normal adalah diawetkan. [7]
Because it has shown to be of prognostic significance, complete surgical resection with aggressive lymph node dissection is essential for cure; [65] thus, it is the goal of surgery. Karena telah menunjukkan untuk menjadi penting prognostik, reseksi bedah lengkap dengan diseksi kelenjar getah bening yang agresif sangat penting untuk penyembuhan; [65] dengan demikian, adalah tujuan dari operasi. Adequate retroperitoneal lymph node biopsies cannot be overemphasized. [66] However, only 40-69% of pediatric patients are candidates for curative

resection, a much lower number than in adults. [6, 38, 60, 63] Debulking is of little use in patients with extensive metastatic disease. biopsi kelenjar getah bening retroperitoneal yang memadai tidak dapat terlalu menekankan. [66] Namun, hanya 40-69% dari pasien anak-anak adalah kandidat untuk reseksi kuratif, nomor jauh lebih rendah dibandingkan orang dewasa. [6, 38, 60, 63] Debulking adalah menggunakan sedikit pada pasien dengan penyakit metastasis luas. Occasionally, resections of bulky tumors or metastases offer palliation. Kadang-kadang, reseksi dari tumor besar atau paliatif metastasis ditawarkan.
Surgery is the only modality known to be effective in providing cures, although adjuvant chemotherapy extends life. Pembedahan adalah modalitas hanya diketahui efektif dalam memberikan pengobatan, meskipun kemoterapi adjuvan memperpanjang hidup. Few patients with extensive metastatic disease are cured. Beberapa pasien dengan penyakit metastasis luas disembuhkan.
Chemotherapy and radiation therapy Kemoterapi dan terapi radiasi
Patients who have tumors that are considered unresectable at diagnosis should undergo only biopsy and neoadjuvant chemotherapy, with or without radiation therapy. Pasien yang memiliki tumor yang dianggap dioperasi di diagnosa harus menjalani biopsi hanya kemoterapi dan neoadjuvant, dengan atau tanpa terapi radiasi. Intraoperative radiation therapy (IORT) is advocated for diseases that are known to have metastasized to the mesentery or mesenteric lymph nodes. Intraoperatif terapi radiasi (IORT) adalah menganjurkan untuk penyakit yang diketahui telah menjalar ke mesenterium atau kelenjar getah bening mesenterika. IORT is performed while the bowel is displaced from the peritoneal cavity. [38] Several chemotherapeutic regimens have been used, including 5-fluorouracil, [81] irinotecan, and folinic acid (leucovorin) rescue. [91] Other active agents in adults with colorectal cancer include oxaliplatin, and irinotecan. IORT dilakukan ketika usus dipindahkan dari rongga peritoneal. [38] Beberapa rejimen kemoterapi yang telah digunakan, termasuk 5-fluorouracil, [81] irinotecan, dan folinic asam (leucovorin) penyelamatan. [91] bahan aktif lainnya pada orang dewasa dengan kanker kolorektal termasuk oxaliplatin, dan irinotecan. Newer targeted therapeutic agents, such as bevacizumab and cetuximab, have increased the efficacy to the standard chemotherapy treatment. [65] Agen terapi baru yang ditargetkan, seperti bevacizumab dan cetuximab, telah meningkatkan khasiat untuk pengobatan kemoterapi standar. [65]
Survivors of colorectal cancer may have an increased risk for secondary leukemias or other secondary malignancies. [92, 93, 42, 94] Boice reported a 2-6% risk of acquiring a leukemic disorder after treatment with semustine (nitrosoureas). [93] Alkylating agents also increase the risk of secondary leukemias. [93] In addition, pediatric patients with cancer treated with radiotherapy for solid tumors have a 3% incidence of secondary malignant neoplasms. [58] Survival for children with colorectal cancer is dismal; the 5-year survival rate in different series is 5-28%. [63, 95] Selamat dari kanker kolorektal mungkin memiliki peningkatan risiko leukemia sekunder atau keganasan sekunder lainnya. [92, 93, 42, 94] Boice melaporkan 2-6% risiko tertular gangguan leukemia setelah pengobatan dengan semustine (nitrosoureas). [93] agen juga meningkatkan risiko sekunder. leukemia alkylating [93] Selain itu, anak dengan pasien kanker diobati dengan radioterapi untuk tumor yang solid memiliki 3 kejadian% sekunder. neoplasma ganas Dalam [58] Survival untuk

anak-anak dengan kanker kolorektal adalah buruk, sedangkan 5 tahun kesintasan dalam seri berbeda 5-28%. [63, 95]
Genetic testing and chemopreventive agents Genetik pengujian dan agen chemopreventive
Genetic testing for cancer susceptibility has positive attributes. pengujian Genetika untuk kerentanan kanker memiliki atribut positif. Family members who have tested negative for the particular APC or MMR gene are spared the repeated medical and endoscopic examinations that otherwise would have to be performed in every member of each family. Anggota keluarga yang telah diuji negatif bagi APC tertentu atau gen MMR terhindar dari pemeriksaan medis dan endoskopi berulang yang seharusnya harus dilakukan setiap anggota keluarga masing-masing. They are also spared the anxiety associated with not knowing whether they are affected. Mereka juga terhindar dari kecemasan yang terkait dengan tidak mengetahui apakah mereka terpengaruh. Surveillance can then be concentrated on those who have inherited a mutant gene. Surveilans kemudian dapat berkonsentrasi pada mereka yang telah mewarisi gen mutan.
Future prospective studies should include a systematic family history and testing for potentially relevant genetic conditions if indicated. studi prospektif masa depan harus meliputi riwayat keluarga yang sistematis dan pengujian untuk kondisi genetik berpotensi relevan jika diindikasikan. They should also address the risk of colorectal cancer in family members and promote sensible family screening guidelines. [66] Mereka juga harus mengatasi risiko kanker kolorektal pada anggota keluarga dan meningkatkan pedoman skrining keluarga yang masuk akal. [66]
Most cancers have an increased glycolytic pathway (Warburg effect). Sebagian besar kanker memiliki jalur glikolitik meningkat (Warburg efek). Proteomic studies have demonstrated this pathway enhancement in colorectal cancer culture cells. proteomika studi telah menunjukkan peningkatan jalur ini dalam sel-sel kanker kolorektal budaya. Xhuezhi et al also reported on decreased gluconeogenesis, suppressed glucuronic acid pathway, and an impaired tricarboxylic acid cycle. [1] This provides an insight to the tumorigenesis of colorectal cancer and possible specific target therapies to be developed. Xhuezhi dkk juga melaporkan pada glukoneogenesis menurun, ditekan jalur asam glukuronat, dan siklus asam tricarboxylic terganggu. [1] ini memberikan wawasan ke tumorigenesis kanker kolorektal dan kemungkinan terapi target yang spesifik untuk dikembangkan. The author is currently running a clinical trial in pediatric cancer patients, using citric acid to block the glycolytic pathway, and starve tumor cells by obliging them to go into alternative energy producing pathways.
The authors believe that cancer cells are unable to survive through these alternative pathways because they are unable to produce enough energy through them. It is well known that citric acid blocks the glycolytic pathway, [96] and that this effect might be an adjuvant in cancer treatment. [86] Another mechanism of action we have hypothesized for this, is that citric acid binds to the inner mitochondrial membrane, releasing Caspase 8 (among other enzymes), which, in turn, induce apoptosis in cancer cells.
Chemopreventive agents may one day inhibit the development of adenomas. NSAIDs have well documented effect on shrinking existing adenomas in patients with FAP and potentially inhibit

their formation. [37] Although NSAIDs may have non-COX-mediated pathways, aspirin inhibits COX enzymes in the conversion of arachidonic acid to prostaglandins. Although COX-1 is thought to produce cytoprotective prostaglandins in the GI tract, COX-2 is expressed in response to growth factors, mitogens, and cytokines and is found in 50% of colorectal adenomas and in 85% of cancers. [19] COX-2-specific NSAIDs inhibition is believed to be protective against epithelial transformation. NF-kB transcription factor translocation producing apoptosis is another mechanism of aspirin.
Specific COX-2 inhibitors are no longer used because of their cardiovascular side effects. Bevacizumab is a monoclonal antibody that targets vascular endothelial growth factor-A (VEGF-A), which is believed critical in cancer angiogenesis. Cetuximab is another monoclonal antibody that targets the EGFR, which is involved in cancer cell proliferation, degradation of the extracellular matrix (invasiveness), tumor migration, and endothelial proliferation. It may well become a good genetic target treatment for colorectal cancer. Collaborative multi-institutional pediatric clinical trials are needed to evaluate the prognosis, optimal treatment response, and the basic biology of childhood-onset colorectal cancer.
Removal of the tumor and surrounding lymph nodes is the primary treatment for stage III colon cancer. Before surgery, you will have had a CT scan to detect any cancer that may have spread outside of the colon. During the surgery, the surgeons will also explore the abdomen and liver for tumor that may have spread from the colon to other sites such as the liver or abdominal cavity. The surgeon will also attempt to remove lymph nodes around the site of the colon where the cancer sits to see if the cancer has spread to the lymph nodes.
The type of surgery depends on a variety of factors, including: the location of the tumor, the presence of other associated cancers or polyps, the stage of the cancer; the risk of development of other colon cancer in the future; the patient’s preference. The method of reconstruction of the colon can vary. Some surgeons use manual suturing either in one or two layers, others prefer one of various stapling techniques.
A variety of types of colorectal surgeries are possible depending on where the cancer occurs. The surgical techniques for colon cancer differs signficantly from the surgical techniques for rectal cancer. At Johns Hopkins we have a team of surgeons who specialize in colon and rectal cancer surgery. By coordinating your care with experts in medical and radiation oncology, patients at Johns Hopkins receive the full benefits of a multidisciplinary team approach. Clinical trials are options for all stages of colorectal cancer patients at Johns Hopkins and may be fully explored with your team of experts. The strength of our cancer program ensures that patients receive the most advanced, effective, and safe treatments.

To make a surgical appointment at Johns Hopkins please call (410) 933-1233
Please choose the location of your cancer to view the corresponding surgical techniques:
Colon Resection
Rectal Resection
Colorectal resection, including regional lymph nodes, is based on the blood supply to the bowel (Figure 20).
Figure 20. Arterial blood supply to the colon.
The mainstay for the treatment of Stage I colorectal cancer is surgery. The goals of surgery are to:
Remove the cancer completely with clear margins. Remove adjacent draining lymph node.

Avoid excessive disruption or spillage of tumor cells.
Reconstruct the bowel, if possible, in order to achieve intestinal continuity and normal or near normal bowel function postoperatively.
The type of surgery depends on a variety of factors, including: the location of the tumor, the presence of other associated cancers or polyps, the stage of the cancer; the risk of development of other colon cancer in the future; the patient’s preference. The method of reconstruction of the colon can vary. Some surgeons use manual suturing either in one or two layers, others prefer one of various stapling techniques.
A variety of types of colorectal surgeries are possible depending on where the cancer occurs. The surgical techniques for colon cancer differs signficantly from the surgical techniques for rectal cancer. At Johns Hopkins we have a team of surgeons who specialize in colon and rectal cancer surgery ensuring that patients get the most advanced, effective, and safe treatments.
To make a surgical appointment at Johns Hopkins please call (410) 933-1233
Please choose the location of your cancer to view the corresponding surgical techniques:
Colon Resection
Rectal Resection
Colorectal resection, including regional lymph nodes, is based on the blood supply to the bowel (Figure 20).

Figure 20. Arterial blood supply to the colon.
Surgical Treatment of Stage I Colon Cancer
A right hemicolectomy (Figure 21) is the surgical procedure performed for patients with cancer between the cecum and ascending colon.

Figure 21. Right hemicolectomy with ileocolic anastomosis.
A transverse colectomy (Figure 22) is performed for tumors in the transverse colon. The middle colic artery is ligated and the ascending and descending colon are anastomosed.
Figure 22. Transverse colectomy with anastomosis of ascending and descending colon.
Extended right colectomy is performed in cases in which the cancer is located in the proximal or mid transverse colon (Figure 23). This resection requires removal of the terminal ileum, cecum, ascending colon, hepatic flexure and a portion of the transverse colon.

Figure 23. Extended right colectomy with ileocolic anastomosis.
Left hemicolectomy (Figure 24) is the procedure for tumors of the descending colon. The left colic artery is ligated, the splenic flexure and descending colon removed and the transverse and upper sigmoid colon joined (anastomosed).
Figure 24. Left hemicolectomy with transverse and sigmoid colon anastomosis.

Sigmoid colectomy removes tumors of the sigmoid colon (Figure 25). The upper rectum and descending colon are joined (anastomosed).
Figure 25. Sigmoid colectomy with anastomosis of descending colon and upper rectum.
Surgical Treatment of Stage I Rectal Cancer
The surgical management of rectal cancer can be particularly complicated, depending on the location of the tumor. There are a variety of surgical procedures that are available to patients with rectal cancer ranging from local excision to radical abdominoperineal resection. Accurate preoperative staging determining depth of invasion and lymph node involvement is essential in selection of the appropriate operative procedure. CT or MRI and endorectal ultrasound are diagnostic tests used for staging of the tumor.
The three options for management of rectal cancers include:
Local excision Restorative anterior or low anterior resection

Abdominal perineal resection with permanent colostomy
Local excision also known as transanal excision for rectal cancer is reserved for selected early lesions of the rectum. In this case, the surgeon removes full thickness of the rectum only without harvesting any lymph nodes. In general, local excision may be offered for T1 rectal cancers (i.e. cancer has only spread to submucosa), small tumors (less than 3–4 cm in diameter) within 6–8 cm of the anal verge, and with limited circumferential involvement (less than one third of rectal circumference). Tumors should be moderately- to well-differentiated and be T1 on transrectal ultrasound. A 1-cm margin of grossly normal mucosa beyond the edge of the tumor is ideal, although 5-mm is acceptable. A full thickness rectal wall excision to the perirectal fat layer is performed. Local excision reduces perioperative complications and preserves anorectal, bladder, and sexual function. Studies have demonstrated about a 90% recurrence-free survival rate in patients with T1 well–to–moderately differentiated rectal tumors without venous or lymph vessel invasion.
Local excision may not be recommended for cancers that have worrisome features such as poorly differentiated or lymphovascular invasion since such features suggest a higher likelihood of nodes involvement and more extensive procedures such as a low anterior resection or an abdomino-perineal resection may be needed.
The low anterior resection is suitable for lesions located in the upper two-thirds of the rectum. This sphincter-sparing operation can be performed for cancers in the middle and lower third of the rectum with low coloanal anastomosis at the level of the pelvic floor (Figure 26).

Figure 26. Low anterior resection for tumors in the upper two thirds of the rectum. A, Temporary colostomy; B, subsequent colorectal anastomosis; C, restoration of GI tract continuity.
Colorectal anastomosis or coloanal reconstructions are alternatives to permanent colostomy. Construction of a colon J-pouch creates a neorectal reservoir that can reduce frequency and urgency of bowel movements and nocturnal bowel movements in selected cases (Figure 27).

Figure 27. A, Low anterior resection; B,C, coloanal anastomosis; D, j pouch construction creating a reservoir.
These radical “transabdominal” resections are recommended for most cancers at risk for recurrence (higher than stage T1 or poorly differentiated with lymphatic or vascular involvement). The selection of surgical procedure should be guided toward the prevention of pelvic recurrence. Total mesorectal excision with a low anterior resection or an abdominoperineal resection is the optimal surgical procedure for rectal cancer. Total mesorectal excision removes the rectal mesentery as an intact unit. This reduces local recurrence along with preserving sexual function, urinary function, and continency.
Abdominoperineal resection is used when the lesion is in the lowest part of the rectum (Figure 28) typically involving the anal musculature. A colostomy allows for drainage of waste through an opening in the abdominal wall.

Figure 28. Abdominoperineal resection with colostomy.
Treatment for Advanced (Unresectable) Rectal Cancer
Endoscopic Therapy For patients with obstructive unresectable rectal cancer, endoscopic therapy using the neodymium-yttrium-aluminum-garnet (Nd:YAG) laser is an alternative to recanalize the rectal lumen. Electrofulguration using a heater probe has also been used for palliative therapy.
Another approach for patients who are poor surgical candidates is photodynamic therapy(PDT). In this procedure, patients are sensitized with a hematoporphyrin derivative, which is taken up preferentially by the tumor cells. At this point, phototherapy is performed using a laser beam applied through a flexible optical fiber directed at the tumor. The laser sensitizes the protoporphyrin ultimately inducing apoptosis (programmed cell death) essential killing the tumor cells. This technique is still considered experimental.
Complications associated to endoscopic therapy with Nd:YAG laser are bleeding and perforation.
Surgical Treatment of Stage II Rectal Cancer
The surgical management of rectal cancer can be particularly complicated, depending on the location of the tumor. There are a variety of surgical procedures that are available to patients with rectal cancer ranging from local excision to radical abdominoperineal resection. Accurate

preoperative staging determining depth of invasion and lymph node involvement is essential in selection of the appropriate operative procedure. CT or MRI and endorectal ultrasound are diagnostic tests used for staging of the tumor. Stage II rectal cancers are staged as T3NOM0 or T4N0M0, generally based on endorectal ultrasound or MRI staging.
The three options for management of Stage II rectal cancers include: Local excision Restorative anterior or low anterior resection
Abdominal perineal resection with permanent colostomy
In general, local excision is rarely offered for stage II rectal cancers except in the context of a clinical trial since the lymph nodes need to be sampled to make sure that there is no cancer in them. Nodal sampling can be performed by either a restorative procedure which salvages the sphincter muscles such as a low anterior resection or an abdominoperineal resection which would result in a permanent colostomy. The low anterior resection is suitable for lesions located in the upper two-thirds of the rectum. This sphincter-sparing operation can also be performed for cancers in the middle and lower third of the rectum with low coloanal anastomosis at the level of the pelvic floor (Figure 25).
These radical “transabdominal” resections are recommended for most cancers at risk for recurrence (higher than stage T1 or poorly differentiated with lymphatic or vascular involvement). The selection of surgical procedure should be guided toward the prevention of pelvic recurrence. Total mesorectal excision with a low anterior resection or an abdominoperineal resection is the optimal surgical procedure for rectal cancer. Total mesorectal excision removes the rectal mesentery as an intact unit. This reduces local recurrence along with preserving sexual function, urinary function, and continency.
Abdominoperineal resection is used when the lesion is in the lowest part of the rectum (Figure 28) typically involving the anal musculature. A colostomy allows for drainage of waste through an opening
in the abdominal wall. Surgery and Radiation Therapy for Stage II Rectal Cancer
Patients with presumed preoperative stage II rectal cancers also benefit from radiation therapy to minimize the risk of future local recurrence. Along with total mesorectal excision, both these modalities have been shown to decrease the risk of local recurrence from historic highs of 40% to now less than 5%. Radiation therapy can be given before surgery, termed neoadjuvant therapy or after surgery, termed adjuvant therapy. The timing and need for radiation therapy is best done within a multidisciplinary team and should be discussed with your surgeon.
Treatment for Advanced (Unresectable) Rectal Cancer

Endoscopic Therapy For patients with obstructive unresectable rectal cancer, endoscopic therapy using the neodymium-yttrium-aluminum-garnet (Nd:YAG) laser is an alternative to recanalize the rectal lumen. Electrofulguration using a heater probe has also been used for palliative therapy.
Another approach for patients who are poor surgical candidates is photodynamic therapy(PDT). In this procedure, patients are sensitized with a hematoporphyrin derivative, which is taken up preferentially by the tumor cells. At this point, phototherapy is performed using a laser beam applied through a flexible optical fiber directed at the tumor. The laser sensitizes the protoporphyrin ultimately inducing apoptosis (programmed cell death) essentially killing the tumor cells. This technique is still considered experimental.
Complications associated to endoscopic therapy with Nd:YAG laser are bleeding and perforation.
Surgical Treatment of Stage III Colon Cancer
A right hemicolectomy (Figure 21) is the surgical procedure performed for patients with cancer between the cecum and ascending colon.
Figure 21. Right hemicolectomy with ileocolic anastomosis.

A transverse colectomy (Figure 22) is performed for tumors in the transverse colon. The middle colic artery is ligated and the ascending and descending colon are anastomosed.
Figure 22. Transverse colectomy with anastomosis of ascending and descending colon.
Extended right colectomy is performed in cases in which the cancer is located in the proximal or mid transverse colon (Figure 23). This resection requires removal of the terminal ileum, cecum, ascending colon, hepatic flexure and a portion of the transverse colon.

Figure 23. Extended right colectomy with ileocolic anastomosis.
Left hemicolectomy (Figure 24) is the procedure for tumors of the descending colon. The left colic artery is ligated, the splenic flexure and descending colon removed and the transverse and upper sigmoid colon joined (anastomosed).
Figure 24. Left hemicolectomy with transverse and sigmoid colon anastomosis.
Sigmoid colectomy removes tumors of the sigmoid colon (Figure 25). The upper rectum and descending colon are joined (anastomosed).

Figure 25. Sigmoid colectomy with anastomosis of descending colon and upper rectum.
Surgical Treatment of Stage III Rectal Cancer
The surgical management of rectal cancer can be particularly complicated, depending on the location of the tumor. There are a variety of surgical procedures that are available to patients with rectal cancer ranging from local excision to radical abdominoperineal resection. Accurate preoperative staging determining depth of invasion and lymph node involvement is essential in selection of the appropriate operative procedure. CT or MRI and endorectal ultrasound are diagnostic tests used for staging of the tumor. Stage II rectal cancers are staged as T3NOM0 or T4N0M0, generally based on endorectal ultrasound or MRI staging.
The three options for management of Stage III rectal cancers include:
Local excision Restorative anterior or low anterior resection
Abdominal perineal resection with permanent colostomy
In general, local excision is rarely offered for stage II rectal cancers except in the context of a clinical trial since the lymph nodes need to be sampled to make sure that there is no cancer in them. Nodal sampling can be performed by either a restorative procedure which salvages the sphincter muscles such as a low anterior resection or an abdominoperineal resection which would result in a permanent colostomy. The low anterior resection is suitable for lesions located in the upper two-thirds of the rectum. This sphincter-sparing operation can also be performed for cancers in the middle and lower third of the rectum with low coloanal anastomosis at the level of the pelvic floor (Figure 25).

Figure 26. Low anterior resection for tumors in the upper two thirds of the rectum. A, Temporary colostomy; B, subsequent colorectal anastomosis; C, restoration of GI tract continuity.
Colorectal anastomosis or coloanal reconstructions are alternatives to permanent colostomy. Construction of a colon J-pouch creates a neorectal reservoir that can reduce frequency and urgency of bowel movements and nocturnal bowel movements in selected cases (Figure 27).

Figure 27. A, Low anterior resection; B,C, coloanal anastomosis; D, j pouch construction creating a reservoir.
These radical “transabdominal” resections are recommended for most cancers at risk for recurrence (higher than stage T1 or poorly differentiated with lymphatic or vascular involvement). The selection of surgical procedure should be guided toward the prevention of pelvic recurrence. Total mesorectal excision with a low anterior resection or an abdominoperineal resection is the optimal surgical procedure for rectal cancer. Total mesorectal excision removes the rectal mesentery as an intact unit. This reduces local recurrence along with preserving sexual function, urinary function, and continency.
Abdominoperineal resection is used when the lesion is in the lowest part of the rectum (Figure 28) typically involving the anal musculature. A colostomy allows for drainage of waste through an opening in the abdominal wall.

Figure 28. Abdominoperineal resection with colostomy.
Treatment for Advanced (Unresectable) Rectal Cancer
Endoscopic Therapy For patients with obstructive unresectable rectal cancer, endoscopic therapy using the neodymium-yttrium-aluminum-garnet (Nd:YAG) laser is an alternative to recanalize the rectal lumen. Electrofulguration using a heater probe has also been used for palliative therapy.
Another approach for patients who are poor surgical candidates is photodynamic therapy(PDT). In this procedure, patients are sensitized with a hematoporphyrin derivative, which is taken up preferentially by the tumor cells. At this point, phototherapy is performed using a laser beam applied through a flexible optical fiber directed at the tumor. The laser sensitizes the protoporphyrin ultimately inducing apoptosis (programmed cell death) essentially killing the tumor cells. This technique is still considered experimental.
Complications associated to endoscopic therapy with Nd:YAG laser are bleeding and perforation.