-
7/30/2019 Vein diseases
1/10
Vein diseases: Thrombosis. Embolia of magistral vessels. PTPhS.
Pulmonary embolism
Difinition:
Inflammation of a thrombus in a vein is called
thrombophlebitis.
The acute inflammatory response makes the developing thrombus
firmly adherent to the
intima of the vessel wall, making embolization uncommon.
Venous thrombosis may involve the superficial or deep venous
systems of the leg. When
both systems are affected, thrombus formation usually begins in
the deep veins and extends to thesuperficial system.
Anatomy:
Vein refluxe.
Anatomy of the venous system in the limbs: In communicating
system are responsible for unidirectional blood flow toward the
heart.
In lower limb, communicating veins are most prominent along the
medial aspect of the calf,where they are called perforating veins.
The names of these veins come from their course from the
superficial to the deep venous system in which they perforate
the deep fascia of the leg.The perforating veins: Hunterian
Dodd
Boyd
Cockett
Bassi
Near the ankle are the Cockett perfopating veins, near the knee
the Boyd perforators and
the thigh the Hunterian perforating vein.
All veins in the upper and lower limbs contain valves every few
centimeters which ensure
that blood flows towards the heart.
Venous pathophysiology:
Blood from the skin and superficial tissues, external to the
deep fascia, drains via the long
and short saphenous veins SFJ (saphenofemoral junction) and SPJ
(saphenopopliteal junction)
and communicating veins into the deep veins. Valves prevent the
flow of blood from the deep to the superficial system.
Normally the pressure in the superficial veins of the foot and
ankle falls from a resting levelof 80-100 mmHg to about 20
mmHg.
This ability to reduce the pressure in the superficial venous
system is crucial to the health of
the lower limb. Patients with damage to the veins in whom the
superficial venous pressure does notfall during exercise may
develop varicose eczema, skin damage and leg ulceration.
Pathological features leading to deep vein thrombosis include
Virchow's triad:
reduced blood flow in the systemic veins,
injury to the veins,
a state of hypercoagulability (Trousseaus triad).
These factors remain important in the pathogenesis of pulmonary
embolism.
Etiology and pathogenesis of thrombosis:
-
7/30/2019 Vein diseases
2/10
Pregnancy increases the risk of pulmonary embolism because
pressure from the gravid
uterus retards venous flow from the legs and pelvis.
Risk factors of the profound veins thrombosis/pulmonary
embolism:
Pulmonary embolism/profound veins thrombosis in anamnesis,
Varicose veins, Oncological diseases,
Character and duration of the surgery (prolonged surgery, pelvic
surgery), Postoperative complications,
General anesthesia,
Age over 40,
Obesity (profound obesity),
Diabetes,
Dehydratation/polycythemia,
Infection/sepsis,
Treatment with estrogens (pills),
Blood circulation insufficiency,
Respiratory insufficiency, Bed regime (prolonged bed rest for
more then 4-6 days),
Immobilization, Trauma,
Postoperative period, Pelvic masses, Pregnancy. Prolonged
steroid therapy.
Classic triad of profound veins thrombosis of the lower
extremities:
Pain.
Edema.
Increased skin temperature of the extremity.
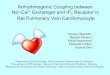
Varicose veins:
Vein diseases: edema
Symptoms and Sings: Deep vein thrombosis is often
symptomless.
Earliest sing of deep vein thrombosis is rise in
temperature.
Deep venous thrombosis is serious since the thrombus is much
more likely to embolize to the
lungs: when the thrombosis is proximal to the calf, there is a
50 per cent likelihood of pulmonaryembolism, and up to 30 per cent
of thrombi isolated to the calf veins embolize to the lungs. As
many
as 40 to 50 per cent of patients with deep venous thrombosis who
develop pulmonary embolism
-
7/30/2019 Vein diseases
3/10
have no symptoms of deep venous disease, causing a delay in the
administration of appropriate
prophylactic and therapeutic measures.
In patients who develop symptoms, mild oedema, superficial
venous dilatation, and pain inthe calf are present. Palpation of
the calf may disclose tenderness and occasionally a thrombosed vein
can be felt
at any site from the plantar aspect of the foot to the femoral
triangle in the groin.
A thrombosed vein is usually identified by palpation in the
popliteal space. Homans' sign - tenderness and tightness in the
calf with hyperextension of the foot.
But it may be present with any type of calf muscle irritation
and is not pathognomonic for
thrombotic disease.
Phlegmasia alba dolens (White leg) is a condition of deep
femoral vein thrombosis
associated with lymphangitis. Here, the limb is grossly swollen,
painful and white.
Phlegmasia caerulea dolens is the condition found when
ileofemoral thrombosis is
associated with massive swelling of the entire extremity to the
inguinal ligament, severe pain,
tenderness, and cyanosis.
Ileofemoral arterial thrombosis with spasm is frequently present
and is characterized by a
pale cool extremity with diminished or absent pulses. Disease
confined to the popliteal vein and its tributaries may be occult or
confused with other
conditions such as rupture of the gastrocnemius muscle or
disorders involving the knee, particularly
a ruptured Baker's cyst. It is therefore important to confirm
objectively the presence of suspected
deep venous thrombosis.
Diagnostic tests:
The most specific test for confirmation of the diagnosis of deep
venous thrombosis is
venography (contrast medium is injected into a vein on the
dorsum of the foot to demonstrate the
venous drainage through the popliteal, femoral, and iliac
veins).
Palpation of the perforating vein
Diagnostic tests:
Venography.
Diagnostic tests:
Real-time B-mode ultrasonic imaging combined with Doppler
ultrasound (duplex
scanning) is a practical, non-invasive method of assessment of
blood flow in veins and valve cuspmovement, and can differentiate
between acute and chronic thrombosis.
Doppler ultrasound (Duplex scanning): Te perforating vein
insufficiency.
Plethysmography and Intravenous administration of radioactive
fibrinogen are anothersensitive non-invasive techniques used to
diagnose deep venous thrombosis.
Diagnostic tests:
-
7/30/2019 Vein diseases
4/10
Magnetic resonance imaging (MRI) is a reliable method of
diagnosing venous thrombosis
and can demonstrate thrombi in the pelvic veins.
The differential diagnosis includes:
ruptured Baker,s cyst,
superficial thrombophlebitis, calf muscle haematomas,
ruptured plantaris tendon. All of these diagnoses can be
demonstrated on ultrasonography, which has the advantageofallowing
the examination of the soft tissues, something which venography is
unable to do.
Treatment:
Anticoagulation prevents the propagation of the original
thrombus and the development of
new thrombi while the existing thrombus is lysed by naturally
occurring fibrinolysis.
Classification of the antithrombotic medications:
1. Antiaggregants (antithrombotic drugs):
Acetylsalicylic acid (Aspirin).
Dipiridamol (Curantyl).
Indobuphen (Ibustrin).
Tiklopdin (Ticlid).
Clopidogrel (Plavinix).
Inhibitors of glycoprotein receptors (GP) II b/III a:
Abximab (Rheo-pro).
Lamifiban.
Integrilin.
1. Anticoagulants:
Direct:
Heparin . Low-molecular heparins (LMN):
Dalteparin (Fragmin).
Nadroparin (Fraksiparin). Parnoparin (Fluxum).
Reviparin (Clivarin).
Enoxaparin (Cleksan).
Sulodeksid (Vessel due F)
Indirect inhibitors of prothrombine:
Girudin (Lepirudin).
Indirect:
Acenocoumarol (Syncumar).
Caumarin (Varfarin).
-
7/30/2019 Vein diseases
5/10
Phenindione (Phenilin).
3.Thrombolytic medications: Streptokinase (Cabikinase,
Streptase).
Streptodekase. Urokinase.
Anisoisolated plasminogen-streptokinase activated complex
(Anistreplase). Tissue plasminogen activator (Alteplase, TPA).
Indication for prescription of heparin:
Treatment of acute arterial thrombosis. Treatment of acute
thrombosis and superficial veins.
Prevention and treatment of acute thrombosis in patients, which
are in shock
(nonhemorrhagical). Prevention of reocclusion after
angioplasty.
Prevention of thrombosis and embolism during valves prosthesis
in cardio-vascular surgery Decrease of the risk of thrombosis of
profound veins and pulmonary embolism after
surgeries, during prolonged immobilization or other risk
factors.
Prevention of reocclusion in patients receiving Thrombolytic
therapy with the help of tissue-
type plasminogen activator.
Positive moments of heparin prescription:
Accessibility.
Treatment with heparin is physiological (substitution
therapy).
Effectiveness and relative safety of heparin (proved by multiple
randomized studies).
Successive clinical use of heparin.
Disadvantages of ungraded heparin in prevention and treatment of
thrombosis:
Relatively low bioavailability.
Rapid elimination from the organism.
Multiple introduction of heparin.
Significant number of hemorrhagic complications (up to 10%).
Necessity of thorough laboratory monitoring of the system of
coagulation.
No reliable direct correlation between the quantity and effect
expression. No clinically valuable effect on thrombin, connected
with thrombi.
Increased sensitivity reaction, where heparin is an
allergen.
Model of heparin indication due to the initial time of blood
coagulation:
Indirect anticoagulants:
Neodicumarin 0,1 (N. 30). 1pill 2-3 times a day, controlling
prothrombin time (PT).
Tab. Phepromaron 0,01 (N. 20). Tab. Nitropharini 0,005 (N.
30).
Tab. Syncumari 0,004 (N. 50) /syncoumar or acenocoumarol/ from
the 2-nd day of
treatment the medicine is prescribed in the supporting dose of 2
mg/daily once a day in the morning.
-
7/30/2019 Vein diseases
6/10
Tab. Phenylini 0,03 (N. 30) /phenylin, or phenindione/. Tab.
Omephini 0,05 (N. 30).
Advantages of low-molecular heparins over upgraded heparin:
Prolong effect.
Introduced 1-2 times a day.
No need for the frequent laboratory control.
Less expressed influence on thrombocytes.
Less frequency of the side effects and complications
development.
Surgical treatment:
The surgical extraction of venous thrombi has been almost
completely discontinued since the
recurrence rate is high. Venous thrombectomy still has a role in
the management of patients with
extensive iliofemoral disease in which limb loss is imminent,
such as in phlegmasia alba dolens.
Prophylactic. General measures are:
adequate hydration,
avoiding calf pressure,
early postoperative mobilization,
stop oral contraceptives at least 6 weeks prior to
operation.
PTPhS:
Valvular incompetence of the deep veins develop in the same way
as in the superficial
venous system, with the degeneration of the valve cusps
resulting in reverse flow in these veins.
PTPhS:
When the deep veins fill with thrombus a new channel appears
(recanalisation) after a
number of weeks or months (6 months). However, the deep vein
valves are destroyed by this
process and, although the veins carry blood, the valves no
longer work and reverse flow is
allowed. Some veins are severely scarred by the recanalisation
process so that they also
become very narrow and ineffective at carryng blood.
PTPhS:
Under these conditions the blood must find an alternative way
round the blockage and
collateral veins develop. In the leg the long and short
saphenous veins may act as collateral channels
and may double in size to accommodate the additional blood flow.
In patients with chronic iliac veinocclusion large suprapubic or
abdominal varices may be seen carrying the collateral flow.
PTPhS: PTPhS with edema and lipodermatosclerosis
Ischaemic venous ulceration
Clinical features of deep vein incompetence:
A number of patients with severe deep vein damage has little to
show for their
problems.
-
7/30/2019 Vein diseases
7/10
In patients with venous valvular incompetence the calf muscle
increases in size,
apparently in response to the greater work in returning blood
from the leg.
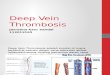
PTPhS:
Necrotic ulceration
Clinical features of deep vein incompetence:
ankle oedema (especially in those patients who have persistent
venous obstruction).
skin complications.
mild eczema.
severe ulcerations.
PTPhS:
An early sing of sing injury is brown pigmentation in the skin
(this occurs because the high
venous pressures which result from damage to the muscle pumping
mechanism cause red blood cells
to be forced out of capillaries in the skin where their
haemoglobin breaks down to form
haemosiderin).
A later and more serious stage is lipodermatosclerosis in which
palpable induration develops
in the skin and subcutaneous tissues. This particularly affects
the gaiter area of the leg, just above the malleoli, and may be
theprecursor of the leg ulceration. Atrophie blanche may also
develop. In this condition the superficial
blood vessels are lost from the skin and white patches
develop.
These indicate that the skin has been severely damaged by the
venous valvular
incompetence.
Venous ulceration may develop in these areas.
PULMONARY EMBOLISM:
Pulmonary embolism is a common and sometimes fatal complication
of deep venous
thrombosis. Although it is recognized in the postoperative
period, most patients develop pulmonary
embolism secondary to non-surgical disorders, including
congestive heart failure, cerebrovascularaccidents, chronic
pulmonary disease, systemic infections, carcinomatosis, and many
chronic
disorders.
Emboli that prove fatal are generally 1.5 cm or more in diameter
and 50 cm or more in
length, and are often fragmented. The right pulmonary artery is
more commonly affected than theleft, and the lower lobes more often
than the upper lobes.
Emboli originate primarily in the systemic venous circulation;
most arise in the iliac and
femoral veins, but up to 20 per cent originate from other
sources, including the inferior vena cava,
the subclavian, axillary, and internal jugular veins. Emboli due
to neoplasms should also be
considered in the differential diagnosis.
Physiological changes following pulmonary embolism are related
to the size of the emboli
and can be divided into those that produce microembolism
(obstruction of terminal small arteries
and arterioles) and those that produce macroembolism (occlusion
of the large pulmonary vessels).
-
7/30/2019 Vein diseases
8/10
-
7/30/2019 Vein diseases
9/10
The presence of phlegmasia caerulea dolens with secondary
arterial spasm is a rare
indication for thrombectomy. Although thrombosis may recur in
such patients, the venous lumen may remain patent forlong enough to
relieve the arterial spasm and prevent gangrene developing.
Pulmonary embolectomy:
In 1908, Trendelenburg performed the first pulmonary
embolectomy. In 1924, Kirschner performed the first successful
pulmonary embolectomy.
The first successful pulmonary embolectomy performed using
extracorporeal circulation was
reported in 1961.
Pulmonary embolectomy:
A median sternotomy is made for exposure of the pulmonary
artery. The main pulmonary
artery is usually found to be free of emboli, although partial
obstruction may be present. The emboli
are removed from the right and left pulmonary arteries and from
their major branches.
Pulmonary embolectomy:
Smaller emboli may be removed by passage of a Fogarty catheter
and irrigation with saline.
The pulmonary artery is closed and cardiopulmonary bypass is
gradually discontinued, allowing the
heart and lungs to resume normal function.
Pulmonary embolectomy:
A serious complication which may follow pulmonary embolectomy is
massive
endobronchial haemorrhage.
Vena caval interruption:
was previously recommended for selected patients with pulmonary
embolism, it is seldom
performed today. A stainless steel umbrella designed by
Greenfield, Michna, Amplatz, Gunther and
Birds nest can be inserted under local anaesthesia through the
femoral or jugular vein. With thisdevice a filter is fixed to the
wall of the inferior vena cava by hooks.
Complications: include distal migration to the bifurcation of
the inferior vena cava,
protrusion of the struts through the caval wall, formation of
thrombus on the filter, misplacement of the device,
retroperitoneal haemorrhage,
perforation of the duodenum or ureter,
development of a thrombus proximal to the umbrella, producing
emboli.
The filter may also migrate into the iliac vein, renal vein,
right atrium, right ventricle, or
pulmonary artery, and such migration is occasionally fatal.
The filter may also stimulate distal thrombosis in the vena cava
and late occlusion may
occur.
Methods of embolectomy in patients with pulmonary embolism:
Trendelenburgs position with extrapleural approach,
cross-clamping of aorta and pulmonary
artery (it is nor used nowadays).
Embolectomy through the branches of pulmonary artery (Marion P.,
Estanove K., 1956 . ).
Embolectomy from the pulmonary artery in conditions of temporary
(more then 3 min)cross-clamping of veins cava (Vosschulte K.,
1959). It is advised to perform a surgery in conditions
of artificial lung ventilation. It is rather well spread method
of surgery.
-
7/30/2019 Vein diseases
10/10
Transvenous embolectomy is the most perspective.
Prevention of pulmonary embolism:
No method or combination of methods completely prevents
thromboembolism.
Factors which reduce the risk include physical activity and
elevation of the lower extremities for
gravity drainage of venous return.Some consider compression of
the legs by stockings or mechanical devices and prophylactic
anticoagulation to be useful. Early ambulation and resumption of
physical activity after operation orbed rest for any reason has
long been recommended.