Embed Size (px)
Citation preview
ステロイド・免疫抑制剤の使い方2015 update
帝京大学ちば総合医療センター
血液・リウマチ内科
萩野 昇

治療薬の分類
• 「症状を緩和させるが、疾患そのものの修飾作用がないもの(A)」– 「痛みをごまかす・熱を下げる薬」
• 「疾患修飾作用があるもの(B-1 csDMARD, B-2 bDMARD/tsDMARD)」– 「病気を治す薬」
• 「併存病態の治療(C:骨粗鬆症、脂質代謝異常症など)」– 「合併症の治療薬」
番外: 医師と患者の心の平穏を保つために処方される薬
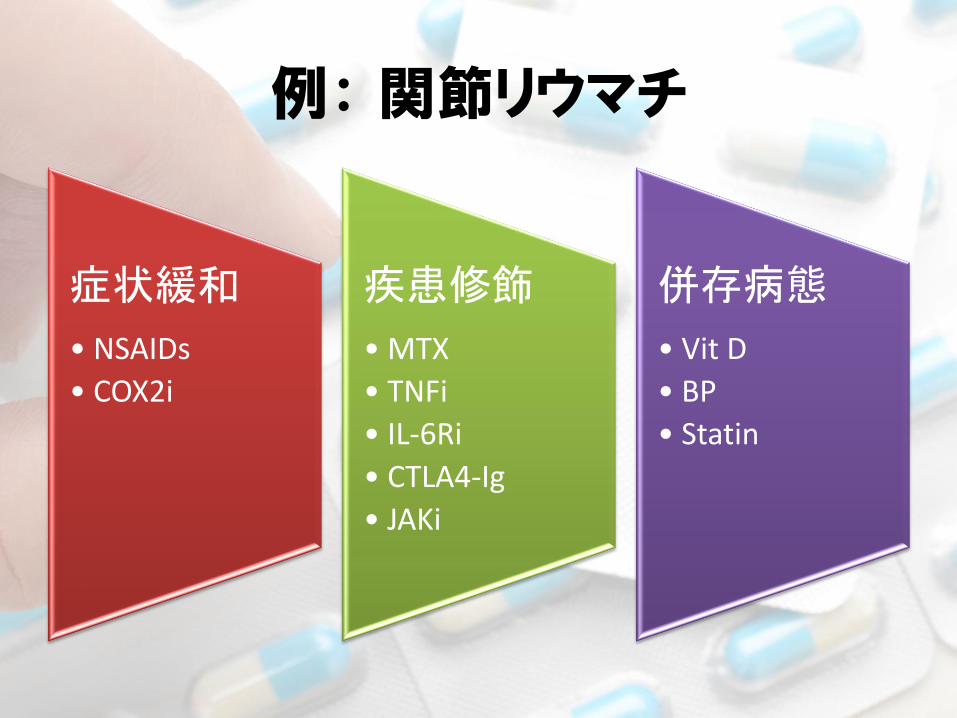
例: 関節リウマチ
症状緩和
• NSAIDs
• COX2i
疾患修飾
• MTX
• TNFi
• IL-6Ri
• CTLA4-Ig
• JAKi
併存病態
• Vit D
• BP
• Statin
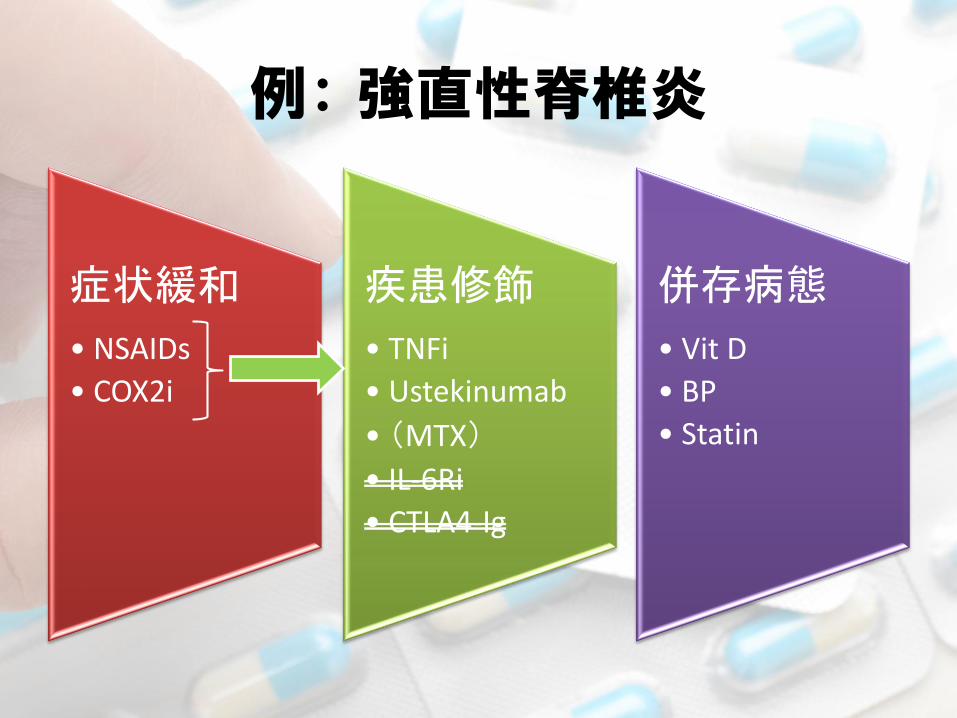
例: 強直性脊椎炎
症状緩和
• NSAIDs
• COX2i
疾患修飾
• TNFi
• Ustekinumab
• (MTX)
• IL-6Ri
• CTLA4-Ig
併存病態
• Vit D
• BP
• Statin

Ann Rheum Dis 2013;72:1280–1286
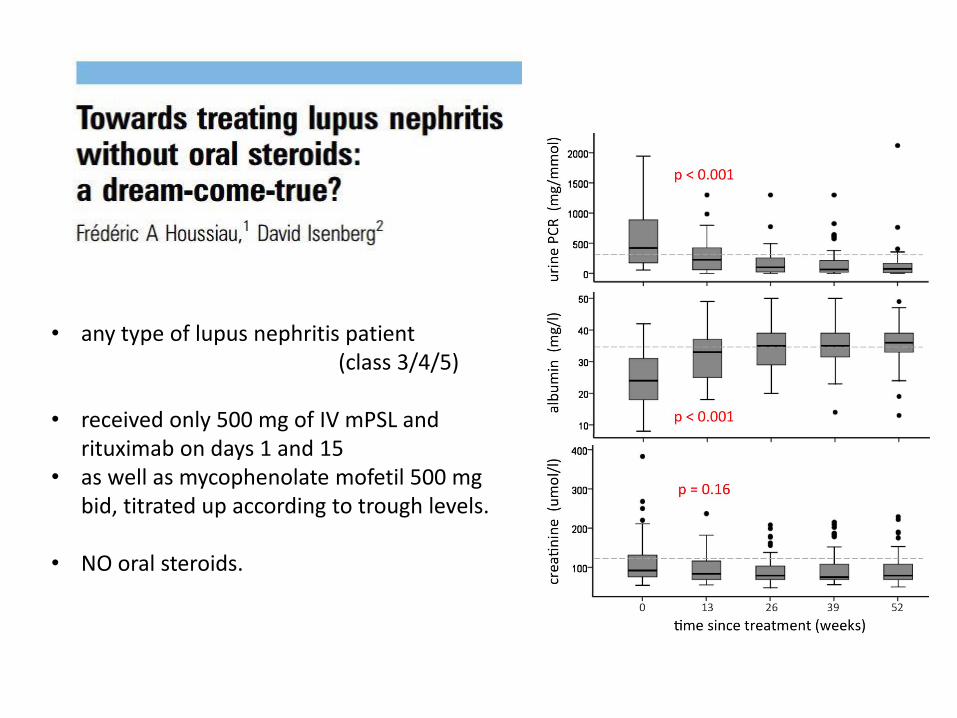
• any type of lupus nephritis patient (class 3/4/5)
• received only 500 mg of IV mPSL and rituximab on days 1 and 15
• as well as mycophenolate mofetil 500 mg bid, titrated up according to trough levels.
• NO oral steroids.
1. Glucocorticoid mecanisms of action overview
2. Adverse reaction
– Infection
– Osteoporosis
3. Clinical use overview
– Lupus and Vasculitis
– Inflammatory Arthritis
– Others
Mayo Clin Proc. 1949 Apr 13;24(8):181-97.
【 病歴 】
• 29歳女性、罹病期間4.5年の関節リウマチ
• 右股関節の破壊性病変が著しい
• ESR 最大で108 mm/時
• 100 mgの”Compound E”連日投与開始
–投与当日・翌日には著変なし
–投与開始3日目:ベッドでの寝返りが可能に
–投与開始4日目:朝のこわばりが消失
–投与開始後 1週間:全ての関節痛が消失

Question 1
• HenchらがこのRA患者に使用したCompound-Eは、副腎皮質ホルモンとしての力価でPrednisoloneに換算して何mg相当であったと推測されるか?
1. 10 mg
2. 15 mg
3. 20 mg
4. 25 mg
Answer 1
• Compound E:
17-Hydroxy-11-Dehydrocorticosterone
• 100mgのハイドロコルチゾン
→ プレドニゾロン 25mg相当の糖質コルチコイド作用
その後間もなく、Compound Eの
「鉱質コルチコイド作用」による副作用が出現…
ステロイドの臨床免疫学:OS
• 「抗炎症作用」 + 「免疫抑制作用」
• 抗炎症作用: anti-inflammatory effect
• 免疫抑制作用:immunosuppressive effect

ステロイドの臨床免疫学:OS
• 「抗炎症作用」 + 「免疫抑制作用」
• 抗炎症作用: anti-inflammatory effect
「いま起きている異常な免疫反応を抑える」
例:気管支喘息発作(好酸球性気道炎症による
可逆性気管支収縮)
短期・比較的大量のステロイド
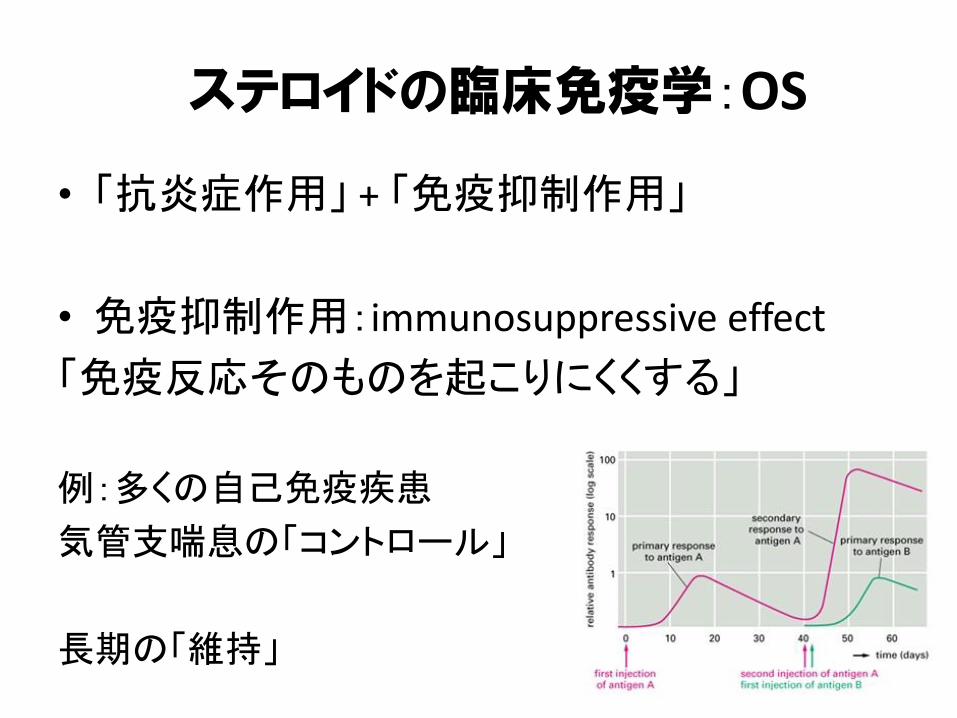
ステロイドの臨床免疫学:OS
• 「抗炎症作用」 + 「免疫抑制作用」
• 免疫抑制作用:immunosuppressive effect
「免疫反応そのものを起こりにくくする」
例:多くの自己免疫疾患
気管支喘息の「コントロール」
長期の「維持」
「ステロイド治療」に関する臨床上の疑問
• ステロイドで治療するべき病態か?• どのくらいの初期量で?
– 「パルス」は必要か?
• 初期量をどのくらいの期間継続するか?• 投与経路は? (PO vs IV)• どのようなペースで減量するか?• 少量で「維持」するのか?中止可能か?
• 免疫抑制剤の併用を行うべきか?

• 唯一の「正解」はない
• 臨床試験のプロトコルは参考になる
• 明らかに「不適切」ということはある
–治療対象
–副作用モニタリング・治療
–投与量

• Genomic Effect
–転写抑制 (Transrepression)
–転写促進 (Transactivation)
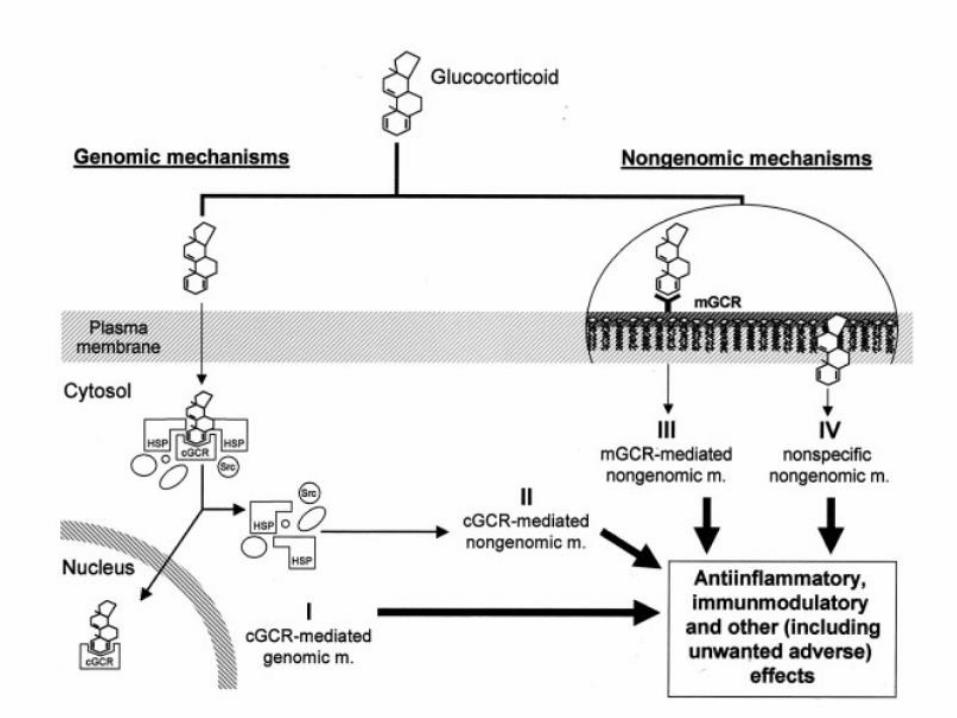
• Non-Genomic Effect
–細胞膜上のGCRに結合
– GC-細胞質内GCR(cGCR)によるNon-Genomic Effect
–細胞膜への直接作用(膜安定化?)
GCの薬理作用Arthritis Rheumatism 2011;63;1-9
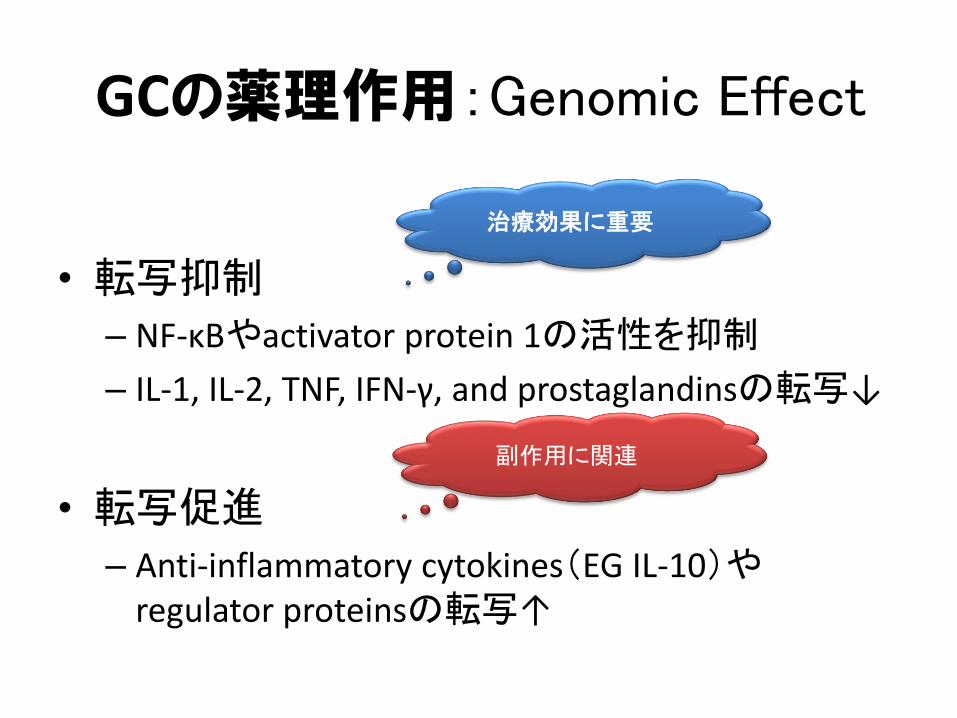
GCの薬理作用:Genomic Effect
• 転写抑制
– NF-κBやactivator protein 1の活性を抑制
– IL-1, IL-2, TNF, IFN-γ, and prostaglandinsの転写↓
• 転写促進
– Anti-inflammatory cytokines(EG IL-10)やregulator proteinsの転写↑
治療効果に重要
副作用に関連
Question 2
• GC投与からGenomic effectを介した制御タン
パクの濃度変化が起きるまで、どのぐらいの時間が必要でしょうか?
1. 5秒
2. 30秒
3. 3分
4. 30分
Answer 2
• 少なくとも30分は必要
• 組織や臓器レベルでGenomic Effectを介したGC投与の効果が観察されるまでには、それよりも長時間を要する。
GCの薬理作用:
Non-Genomic Effect
GC投与後、秒のorderで作用発現
• 細胞膜上のGCRに結合
• GC-細胞質内GCR(cGCR)によるNon-Genomic Effect
• 細胞膜への直接作用(nonspecific)
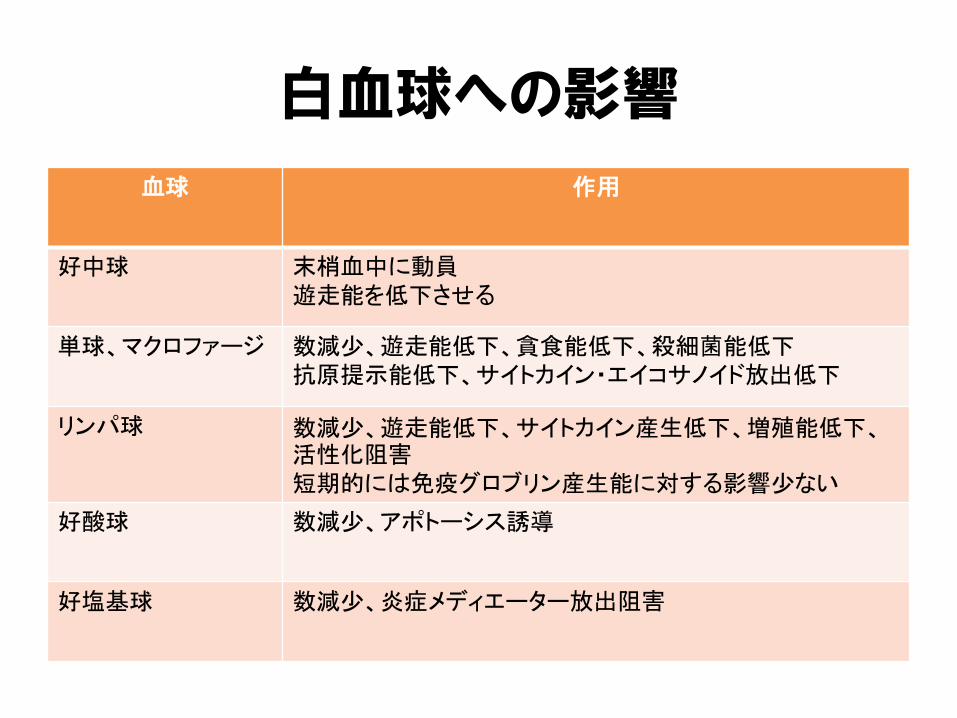
白血球への影響
血球 作用
好中球 末梢血中に動員遊走能を低下させる
単球、マクロファージ 数減少、遊走能低下、貪食能低下、殺細菌能低下抗原提示能低下、サイトカイン・エイコサノイド放出低下
リンパ球 数減少、遊走能低下、サイトカイン産生低下、増殖能低下、活性化阻害短期的には免疫グロブリン産生能に対する影響少ない
好酸球 数減少、アポトーシス誘導
好塩基球 数減少、炎症メディエーター放出阻害
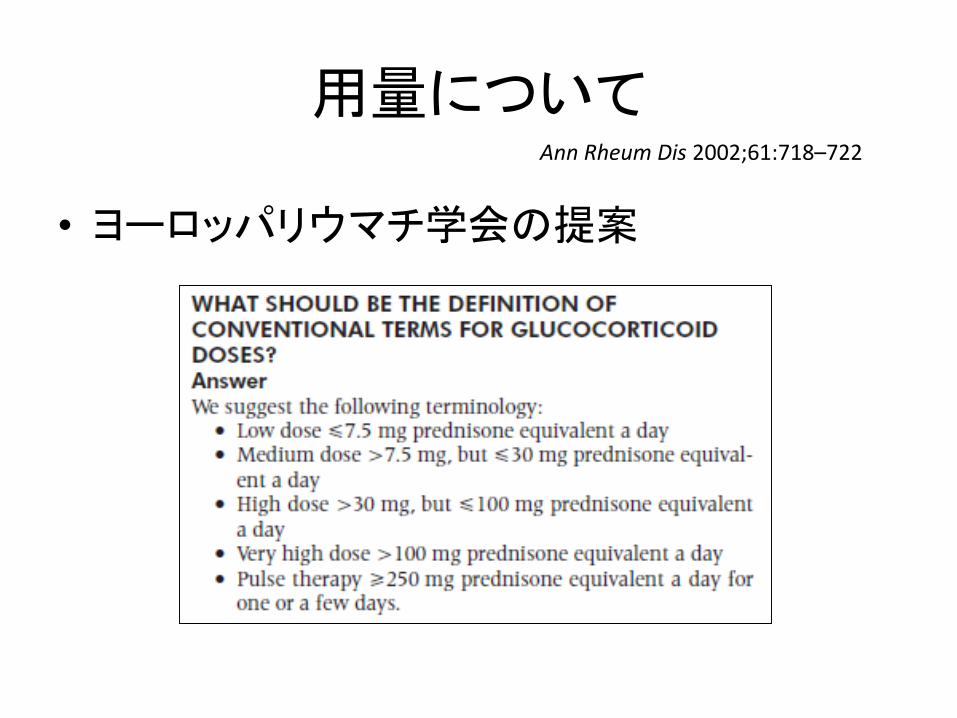
用量について
• ヨーロッパリウマチ学会の提案
Ann Rheum Dis 2002;61:718–722
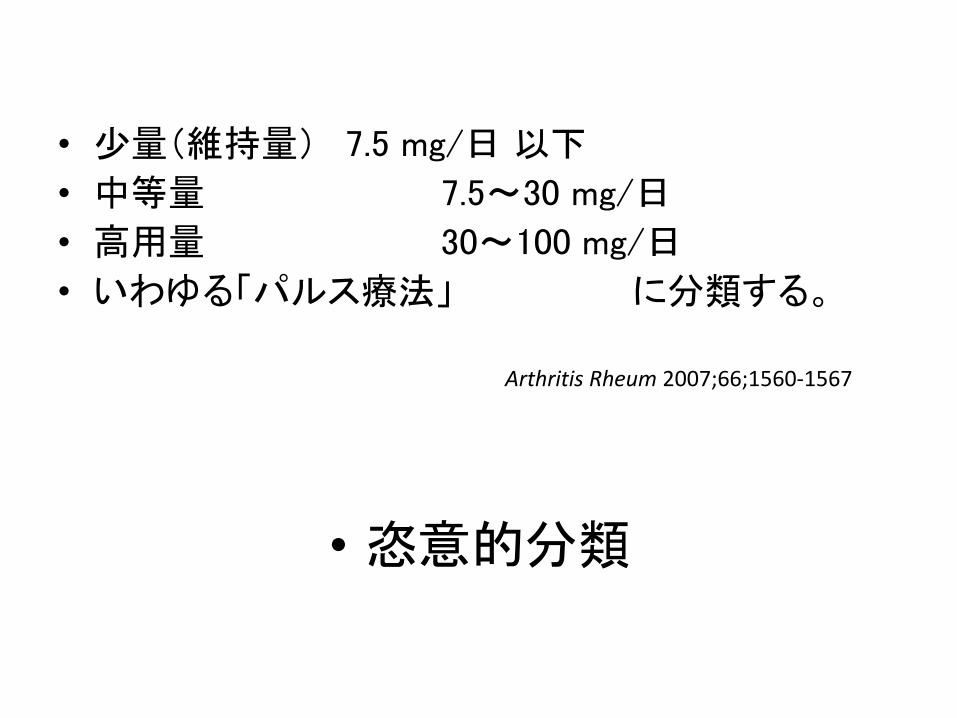
• 少量(維持量) 7.5 mg/日 以下
• 中等量 7.5~30 mg/日
• 高用量 30~100 mg/日
• いわゆる「パルス療法」 に分類する。
Arthritis Rheum 2007;66;1560-1567
• 恣意的分類
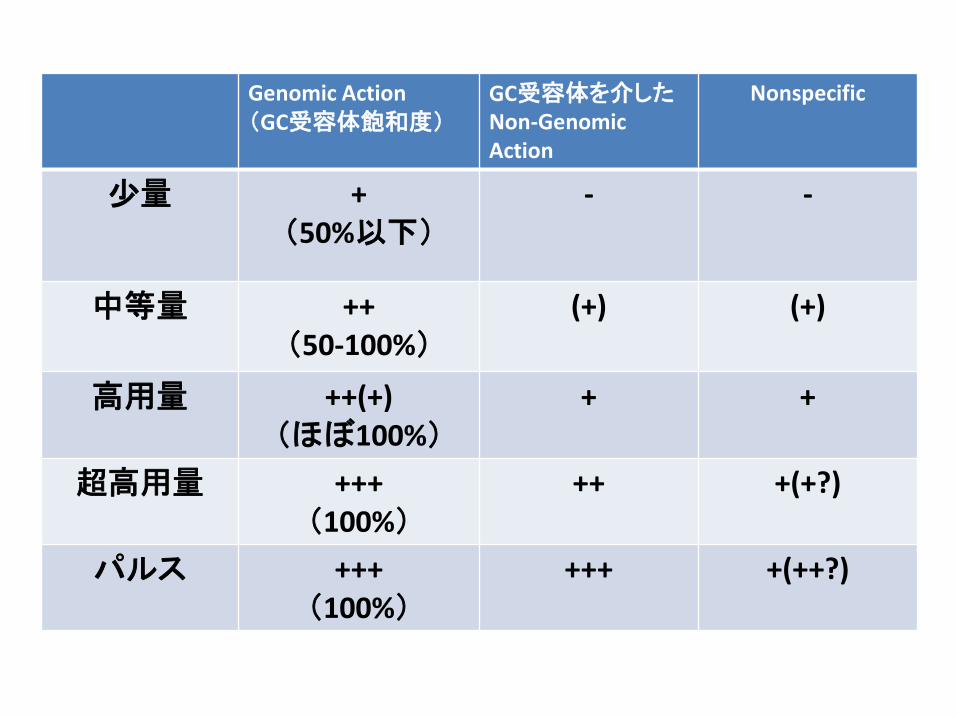
Genomic Action(GC受容体飽和度)
GC受容体を介したNon-Genomic Action
Nonspecific
少量 + (50%以下)
- -
中等量 ++(50-100%)
(+) (+)
高用量 ++(+)(ほぼ100%)
+ +
超高用量 +++(100%)
++ +(+?)
パルス +++(100%)
+++ +(++?)
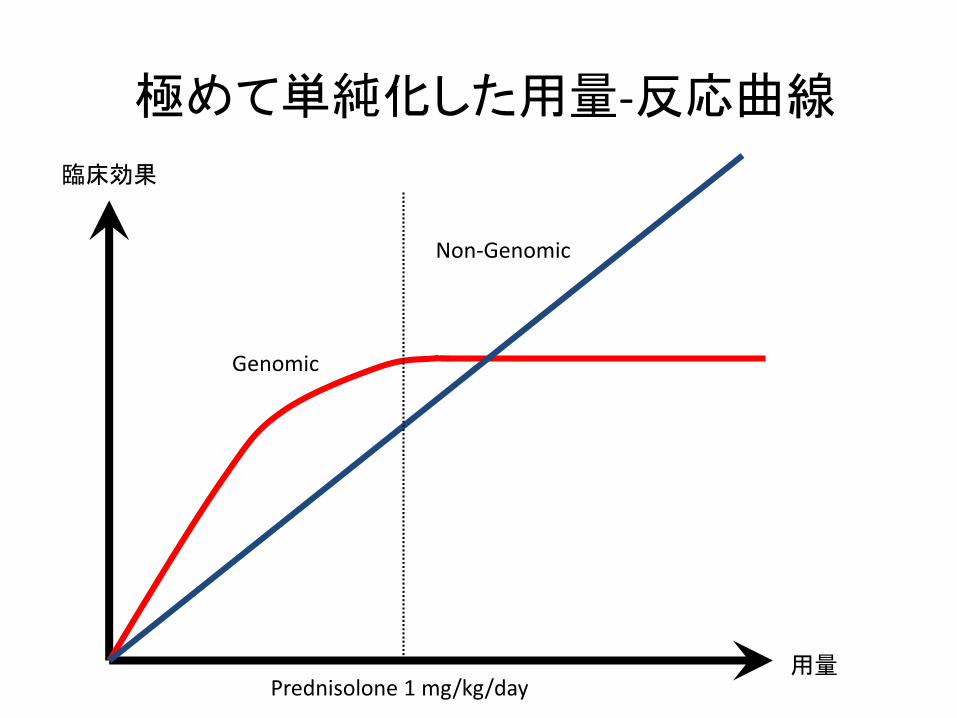
Non-Genomic
Genomic
臨床効果
用量Prednisolone 1 mg/kg/day
極めて単純化した用量-反応曲線
• mPSL 500 mg vs 1000 mg–臨床効果同じ–感染:500 mgの方が少なかった。(Lupus 2002; 11: 508-13)
• mPSL 100 mg vs 1000 mgの投与–効果・副作用とも同じ。(Ann Rheum Dis 1987; 46: 773-6)
いずれも対象疾患はSLE(臓器病変は統一されていない)
Autoimmun Rev. 2006 ;5(2):111-3

「あなたにとってのステロイドパルス」
• 施設A:– ソル・メドロールⓇ 1000mgの点滴を3日間、その後、500mgを3日間、250mgを3日間…
• 施設B:– ソル・メドロールⓇ 1000mgの点滴を3日間の後、約1 mg/kg/dayのソル・メドロール点滴に移行
• 施設C:– ソル・メドロールⓇ 250mg×1日4回の点滴を
3-5日間施行
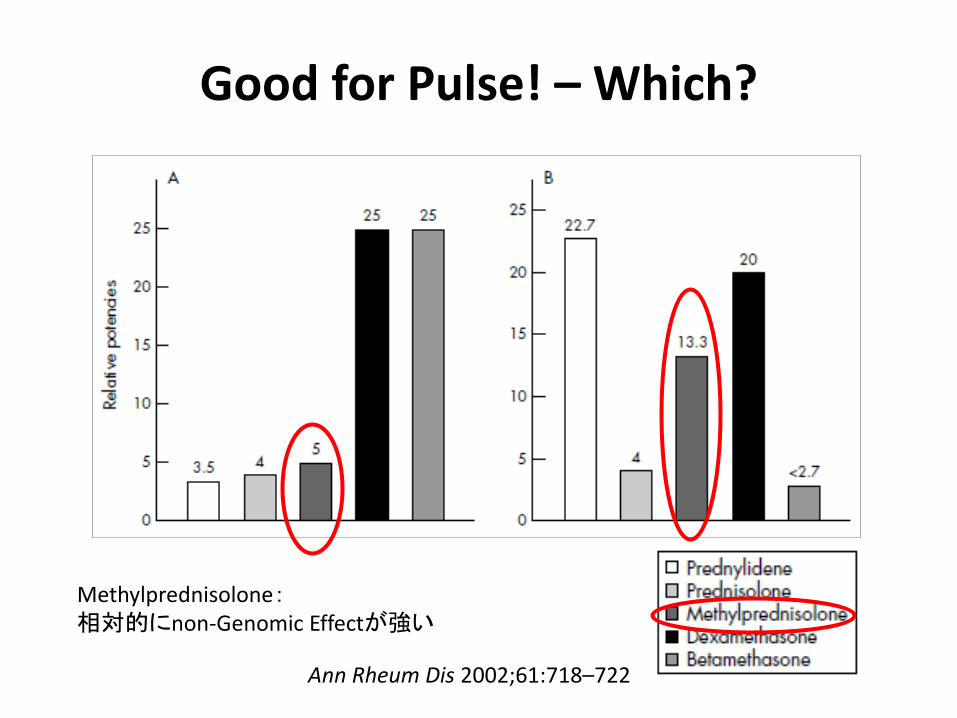
Good for Pulse! – Which?
Methylprednisolone:相対的にnon-Genomic Effectが強い
Ann Rheum Dis 2002;61:718–722
1. Glucocorticoid mecanisms of action overview
2. Adverse reaction
– Infection
– Osteoporosis
3. Clinical use overview
– Lupus and Vasculitis
– Inflammatory Arthritis
– Others
免疫不全の分類
• 好中球減少症
• 細胞性免疫不全
• 液性免疫不全
• 非常にClassicだが、”Works well so far”
Otto Jirovec.
Mackowiak P A et al. Clin Infect Dis. 2004;39:270-271
© 2004 by the Infectious Diseases Society of America
Pneumocystis jirovecii
– “One of the greatest errors in using CYC and prednisone is the failure to use Pneumocystis carinii (jiroveci) pneumonia (PCP) prophylaxis”
Rheum Dis Clin N Am 33 (2007) 691-739

Pneumocystis jirovecii
PLoS Pathog 2012; 8(11): e1003025
PcPと炎症(Inflammation)
免疫抑制(Immunosuppression)
• PcP: (細胞性)免疫の抑制をバックグラウンドとして発症する感染症
• 病原体そのものの急速な増殖やtoxinによる
臓器障害ではなく、何らかの機序による肺の重篤な炎症が臓器障害の主体
–菌体量 ≠ 臨床的な重症度
–抗炎症治療が抗病原体治療に併用される
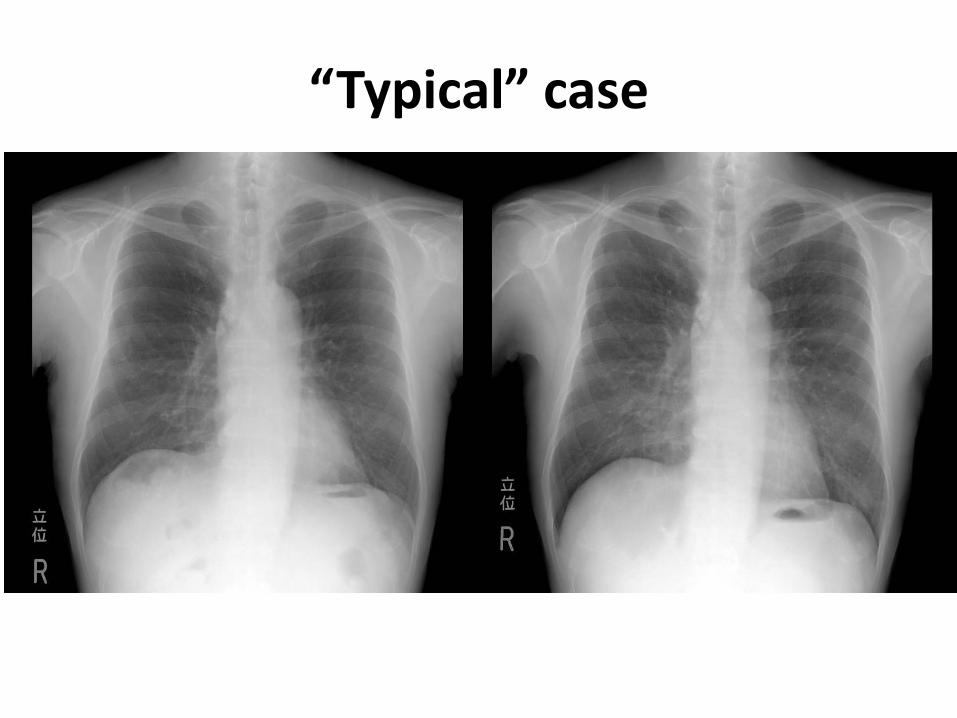
“Typical” case
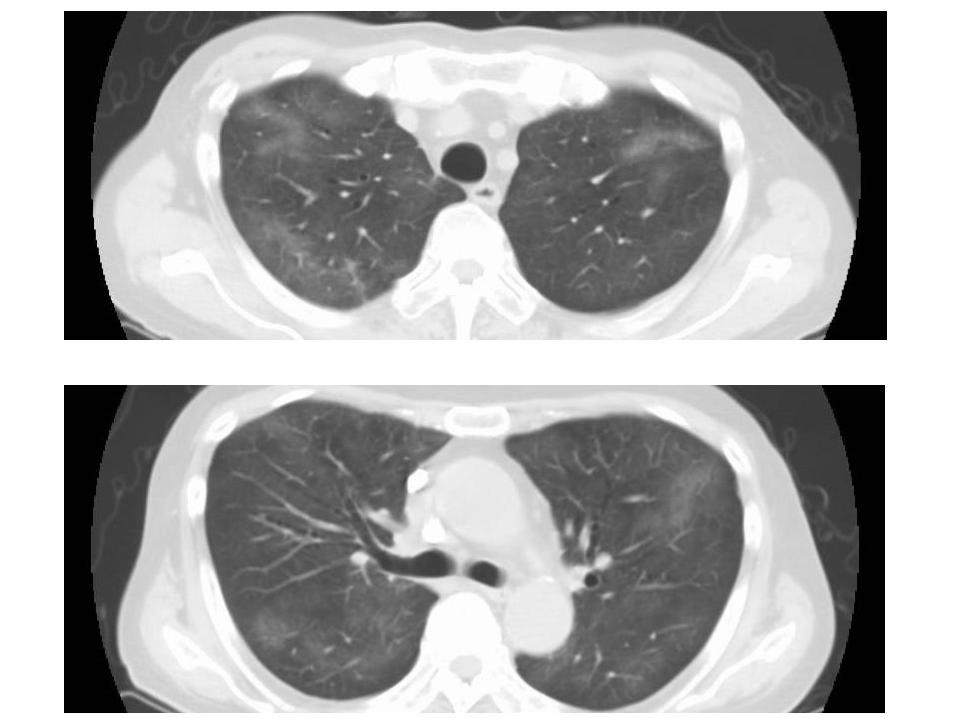

MTX肺臓炎とPcP~ CT画像では区別できない~
• MTX肺臓炎 alone
– MTXを中止
– 必要ならばステロイド
• PcP
– ST合剤+ステロイド
• 疑わしきはPcPとして治療する。
Intern Med 2011: 50; 305-313
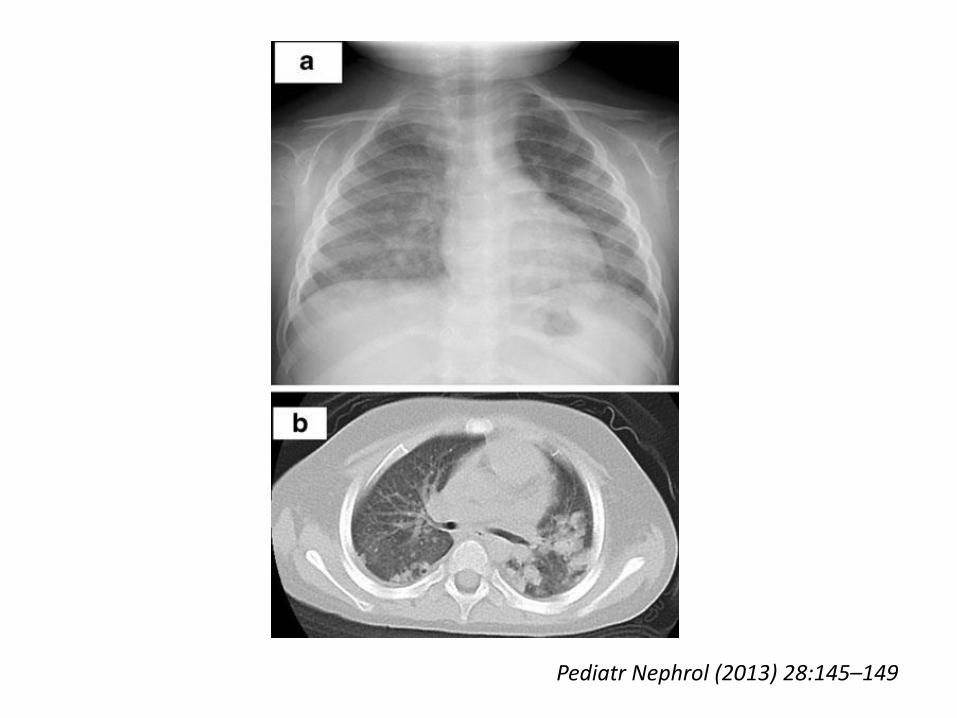
Pediatr Nephrol (2013) 28:145–149

Tzu Chi Medical Journal 24 (2012) 88e89
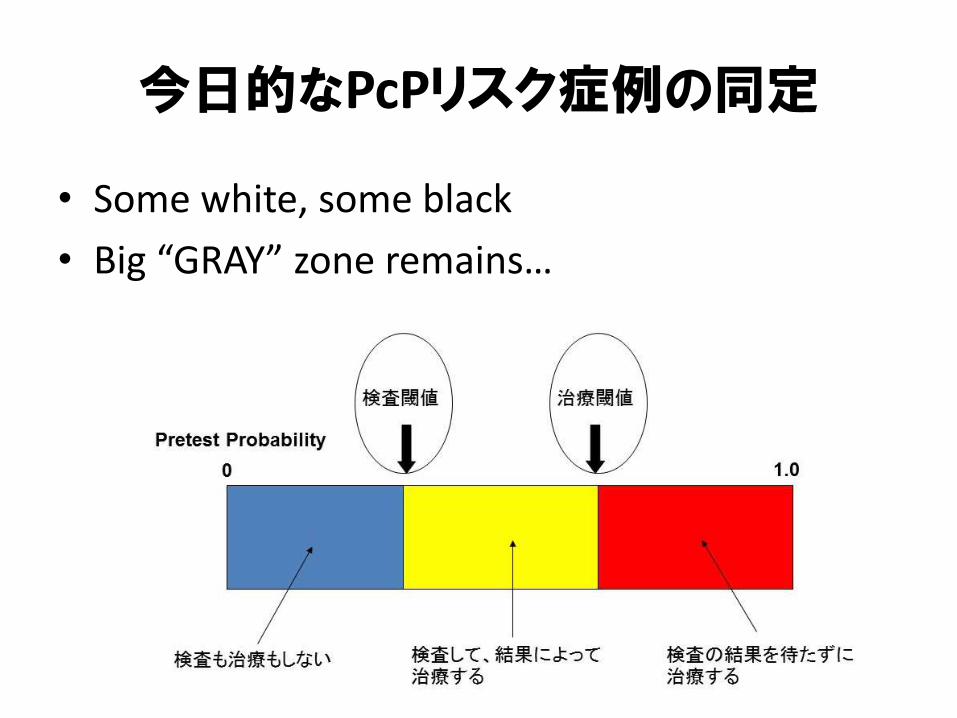
今日的なPcPリスク症例の同定
• Some white, some black
• Big “GRAY” zone remains…
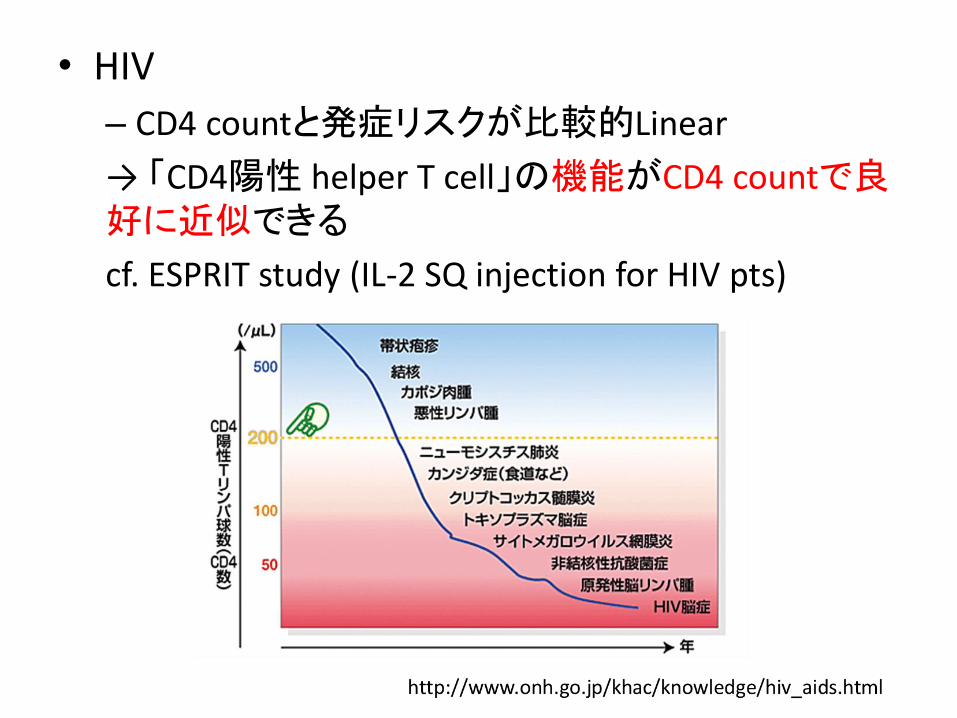
• HIV
– CD4 countと発症リスクが比較的Linear
→ 「CD4陽性 helper T cell」の機能がCD4 countで良好に近似できる
cf. ESPRIT study (IL-2 SQ injection for HIV pts)
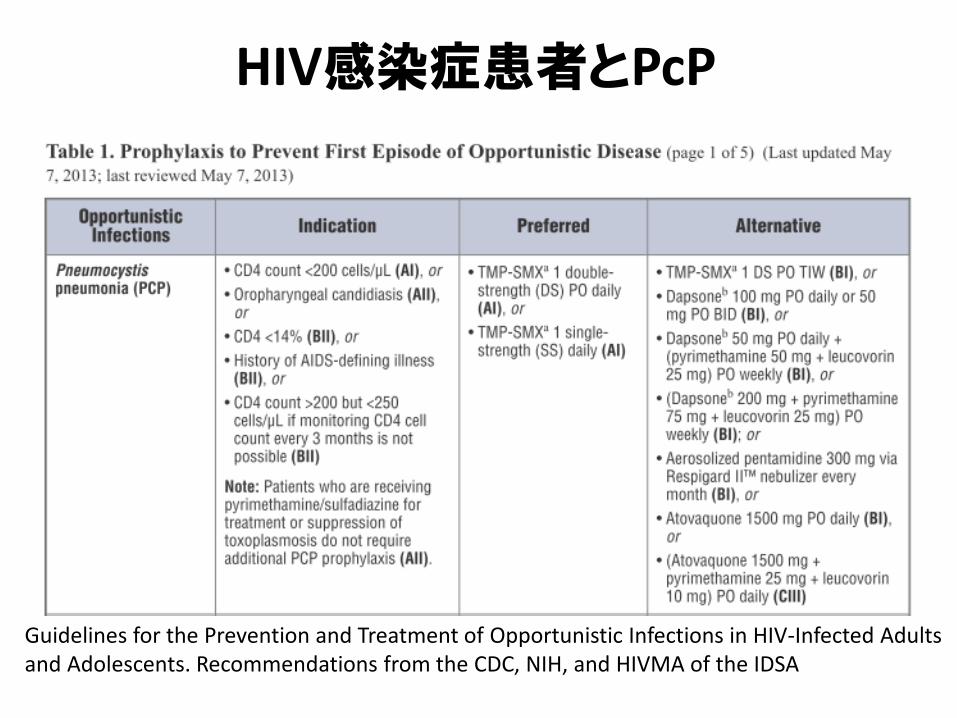
HIV感染症患者とPcP
Guidelines for the Prevention and Treatment of Opportunistic Infections in HIV-Infected Adults and Adolescents. Recommendations from the CDC, NIH, and HIVMA of the IDSA

• HIV– CD4 countと発症リスクが比較的Linear
• “Non-HIV PcP”と一括されるが…–膠原病・自己免疫性疾患
– HSCT
– SOT
– Lymphoma
–その他担がん患者
– Others…
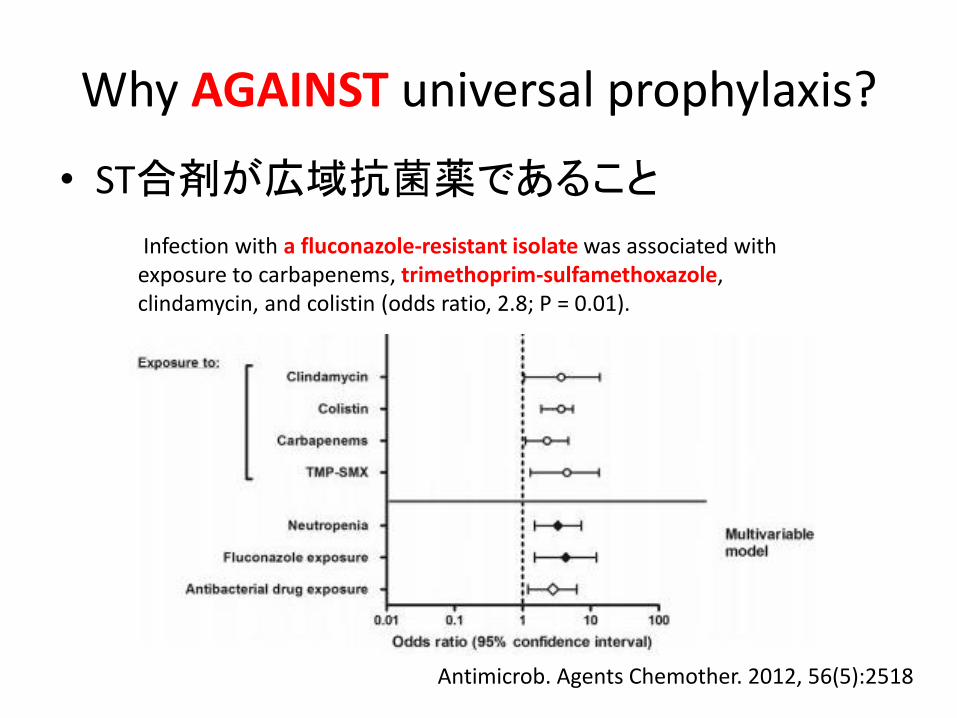
Why AGAINST universal prophylaxis?
• ST合剤が広域抗菌薬であること
Infection with a fluconazole-resistant isolate was associated with exposure to carbapenems, trimethoprim-sulfamethoxazole, clindamycin, and colistin (odds ratio, 2.8; P = 0.01).
Antimicrob. Agents Chemother. 2012, 56(5):2518

Why AGAINST universal prophylaxis?
• ST合剤が広域抗菌薬であること
• 副作用が時として重篤であること
– 3.1%で中止が必要なADR
– Retrospective cohort study:
SLEのminor flareと関連?
• “Non-HIV”と概括すると、稀な事象であること
Why STILL CONSIDER PcP prophylaxis?
– Mortalityが高いから
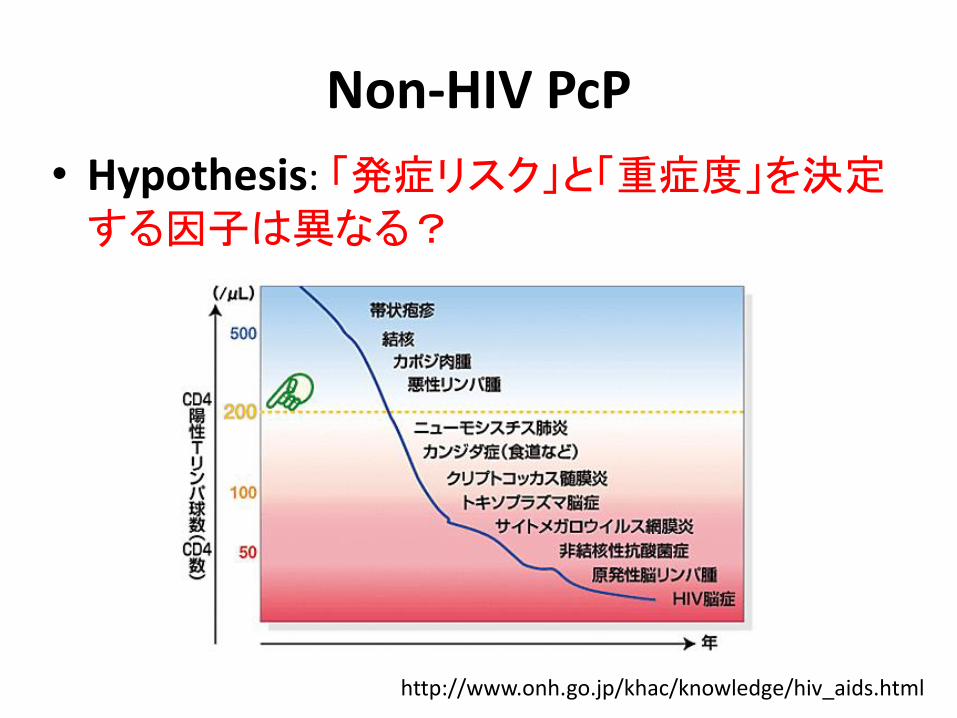
Non-HIV PcP
• Hypothesis: 「発症リスク」と「重症度」を決定
する因子は異なる?
http://www.onh.go.jp/khac/knowledge/hiv_aids.html

Non-HIV PcP
• Hypothesis: 「発症リスク」と「重症度」を決定
する因子は異なる?
• ”Non-HIV”で一括されている
–その中の疾患や治療強度を比較したstudyはない
発症リスク: Classic
• 疾患
–膠原病の種類によっても発症リスク異なる
• 治療強度
–ステロイド
• ある時点での内服量
• 積算量
–免疫抑制剤の併用の有無
A Survey of Rheumatologists’ Practice for Prescribing Pneumocystis Prophylaxis
• 女性のリウマチ科医 (OR 1.47, p = 0.03)
• 米国でプラクティス (OR 1.77, p = 0.004)
• 大学病院ベースの診療 (OR 2.75, p < 0.001)
• 臨床経験が10年未満 (OR 4.08, p < 0.001)
• PCP症例の経験がある (OR 2.62, p < 0.001)
• 長期ステロイド内服 (OR 2.04, p < 0.001) や、
免疫抑制剤併用が必要な患者を診療 (OR 3.19, p = 0.003).
J Rheumatol. 2010 Apr;37(4):792-9
A Survey of Rheumatologists’ Practice for Prescribing Pneumocystis Prophylaxis
• 予防を考慮するにあたって最も重要な事項
– treatment regimen (68.6%)
– rheumatologic diagnosis (9.3%)
– medication dosage (8.3%).
J Rheumatol. 2010 Apr;37(4):792-9
発症リスク: Hidden agenda
• 地域差 and/or 人種差
– リウマチ・膠原病領域での多国籍研究
• その他
–肺障害 (間質性肺炎、気道病変)
–低栄養?

ADVISORY COMMITTEE MEETINGTOFACITINIB FOR THE TREATMENT OF
RHEUMATOID ARTHRITISNDA 203214
BRIEFING DOCUMENTMay 9, 2012
• Two of the 3 Pneumocystis jiroveciipneumonia cases occurred in Japan, a country where pneumocystis is diagnosed 10 times more frequently than in the United States.
http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/ArthritisAdvisoryCommittee/UCM302960.pdf
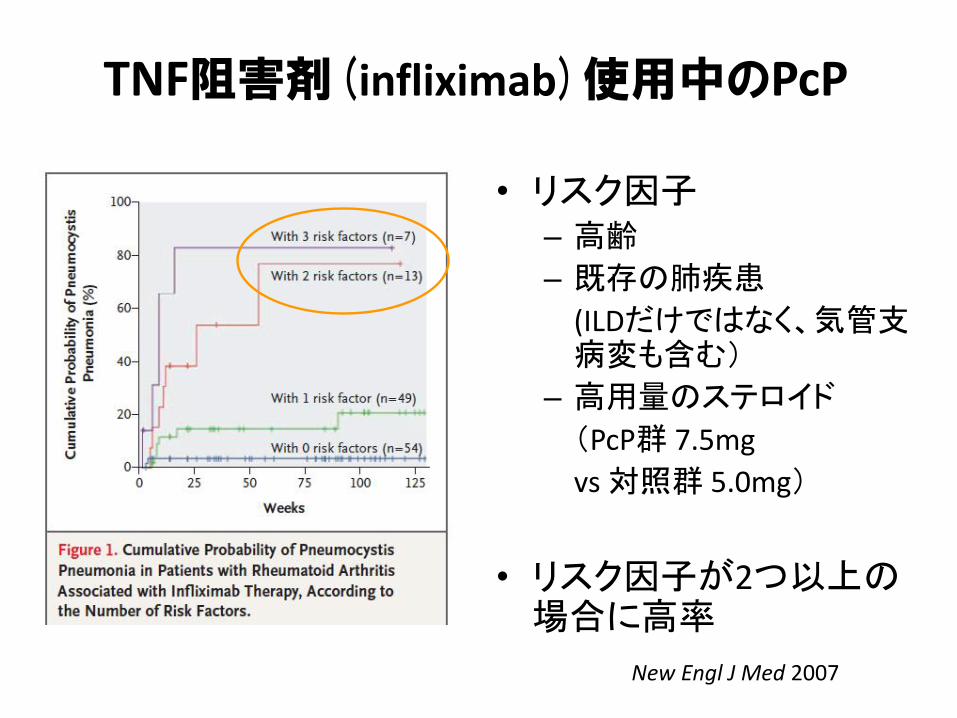
TNF阻害剤(infliximab)使用中のPcP
• リスク因子– 高齢
– 既存の肺疾患
(ILDだけではなく、気管支病変も含む)
– 高用量のステロイド
(PcP群 7.5mg
vs 対照群 5.0mg)
• リスク因子が2つ以上の場合に高率
New Engl J Med 2007
TNF阻害剤(infliximab)使用中のPcP本邦からのcase series

• A diagnosis of PcP was deemed definitive…– if P jiroveci was found on microscopic analysis of respiratory samples with
concurrent clinical manifestations (fever, dry cough, or dyspnea), hypoxemia, and radiologic findings indicative of PcP.
• The diagnosis of PcP was considered presumptive…– if a patient fulfilled these conditions in the absence of evidence of bacterial
pneumonia and presence of either a positive polymerase chain reaction (PCR) test for P jiroveci DNA or increased serum 1,3-D-glucan levels with response to standard treatments for PcP .
• PcP確実例:PcPの臨床症状に加えてP.jiroveci菌体を同定• PcP疑い例:PcPの臨床症状に加えてPneumocystis-PCR陽性、あるいは β-Dグルカンの上昇を認め、通常治療に反応
• 「確実例 2例+疑い例 19例」の検討であることに留意
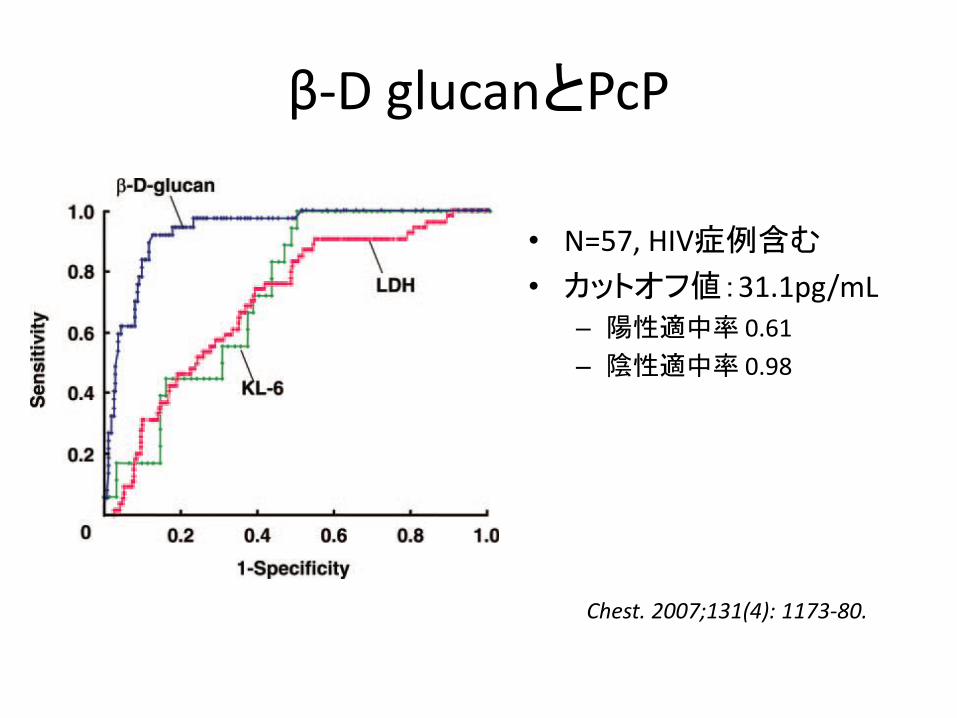
β-D glucanとPcP
• N=57, HIV症例含む
• カットオフ値:31.1pg/mL– 陽性適中率 0.61
– 陰性適中率 0.98
Chest. 2007;131(4): 1173-80.
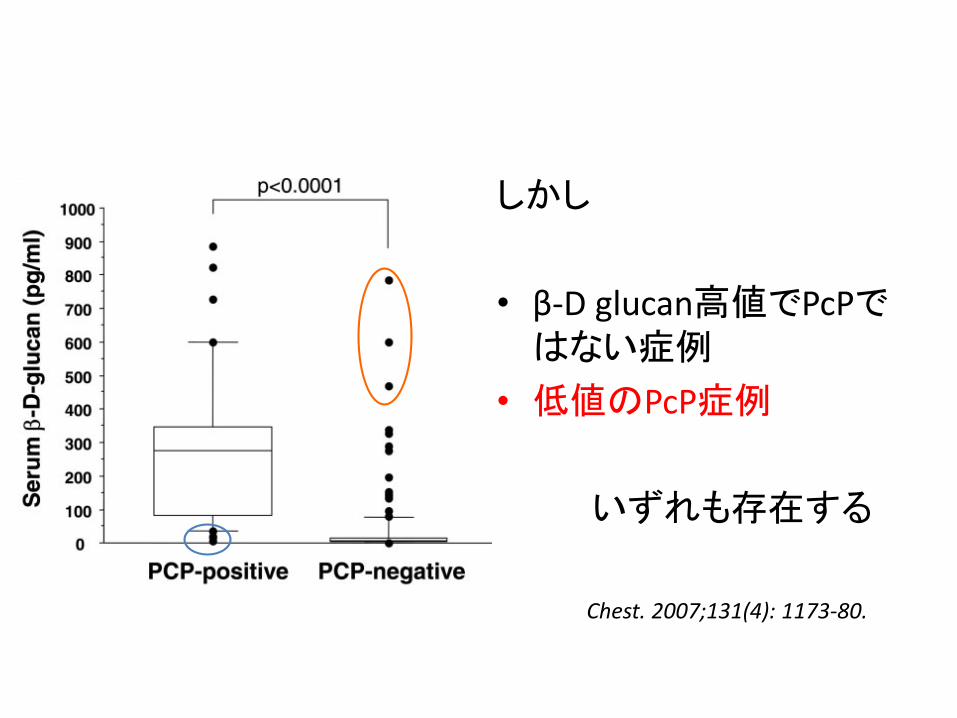
しかし
• β-D glucan高値でPcPではない症例
• 低値のPcP症例
いずれも存在する
Chest. 2007;131(4): 1173-80.
発症リスク: Hidden agenda
• 地域差 and/or 人種差
– リウマチ・膠原病領域での多国籍研究
• その他
–肺障害 (間質性肺炎、気道病変)
–低栄養?

GIO pathophysiology
Nat. Rev. Rheumatol. doi:10.1038/nrrheum.2014.188
• 1st line: Bisphosphonate
• High-risk: Teriparatide
– Only 2-yrs.
• ??? Denosumab
–低エストロゲン性骨粗鬆症からのデータ
–閉経前の若年女性、男性
• データの欠如
–多くの臨床試験の一次評価項目が「骨密度」
1. Glucocorticoid mecanisms of action overview
2. Adverse reaction
– Infection
– Osteoporosis
3. Clinical use overview
– Lupus and Vasculitis
– Inflammatory Arthritis
– Others
ARTHRITIS & RHEUMATOLOGYVol. 66, No. 2, February 2014, pp 379–389
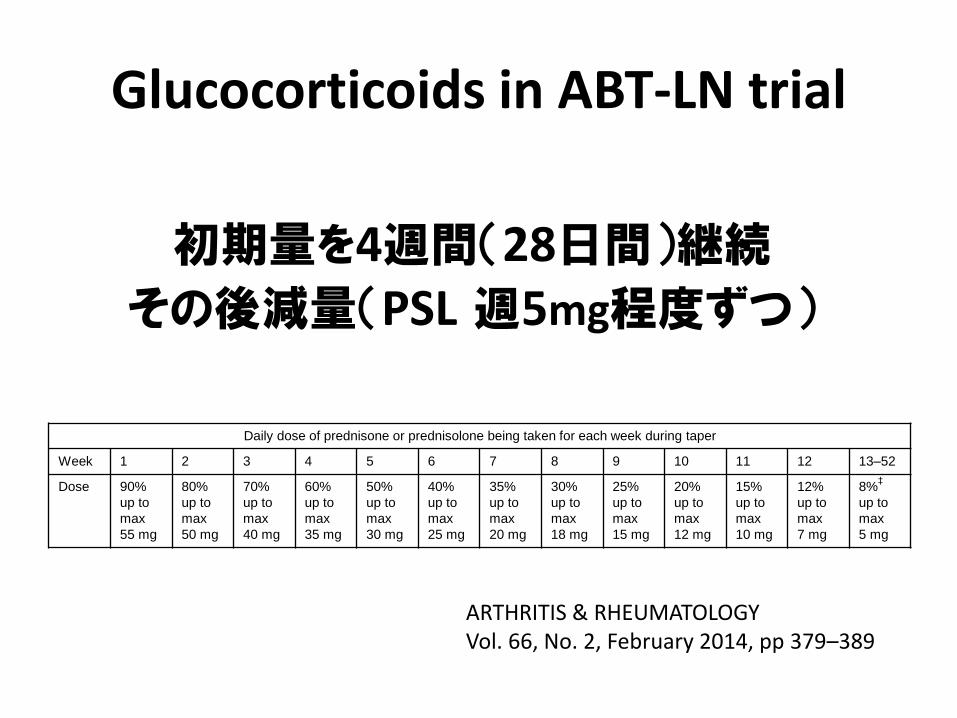
Glucocorticoids in ABT-LN trial
Daily dose of prednisone or prednisolone being taken for each week during taper
Week 1 2 3 4 5 6 7 8 9 10 11 12 13–52
Dose 90%
up to
max
55 mg
80%
up to
max
50 mg
70%
up to
max
40 mg
60%
up to
max
35 mg
50%
up to
max
30 mg
40%
up to
max
25 mg
35%
up to
max
20 mg
30%
up to
max
18 mg
25%
up to
max
15 mg
20%
up to
max
12 mg
15%
up to
max
10 mg
12%
up to
max
7 mg
8%‡
up to
max
5 mg
ARTHRITIS & RHEUMATOLOGYVol. 66, No. 2, February 2014, pp 379–389
初期量を4週間(28日間)継続その後減量(PSL 週5mg程度ずつ)
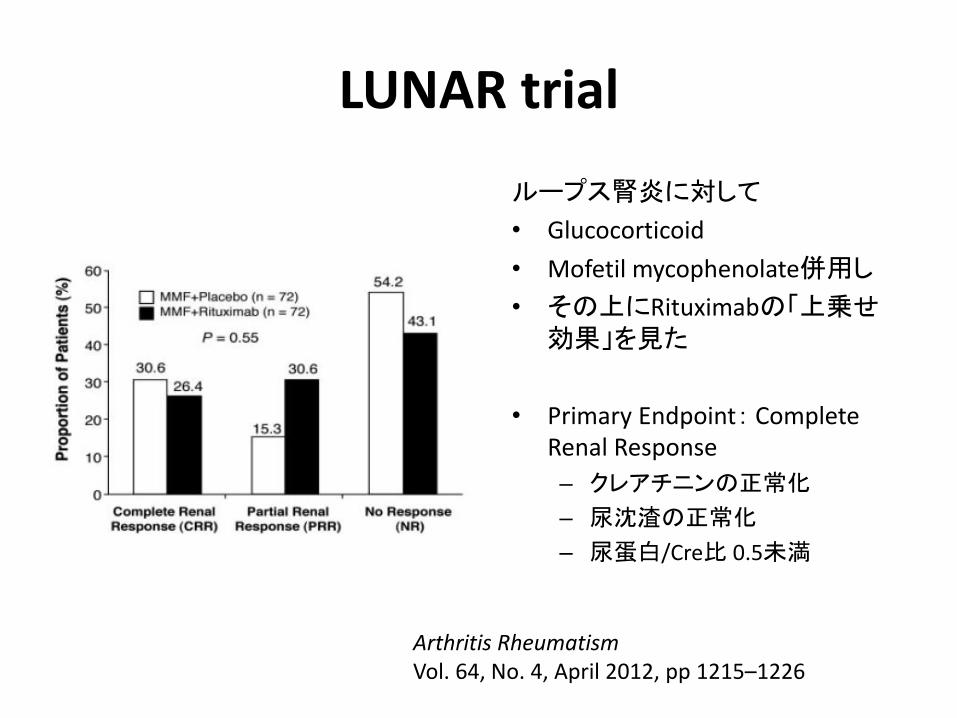
LUNAR trial
ループス腎炎に対して
• Glucocorticoid
• Mofetil mycophenolate併用し
• その上にRituximabの「上乗せ効果」を見た
• Primary Endpoint: Complete Renal Response
– クレアチニンの正常化
– 尿沈渣の正常化
– 尿蛋白/Cre比 0.5未満
Arthritis RheumatismVol. 64, No. 4, April 2012, pp 1215–1226
Ann Rheum Dis 2013;72:1280–1286
• Another problem with LUNAR and other observational studies is the continued reliance on long-term oral steroids.
•
• In the LUNAR study the data suggest that patients were failing to have their steroids cut according to planned taper, highlighting how difficult it is to wean steroids once started.
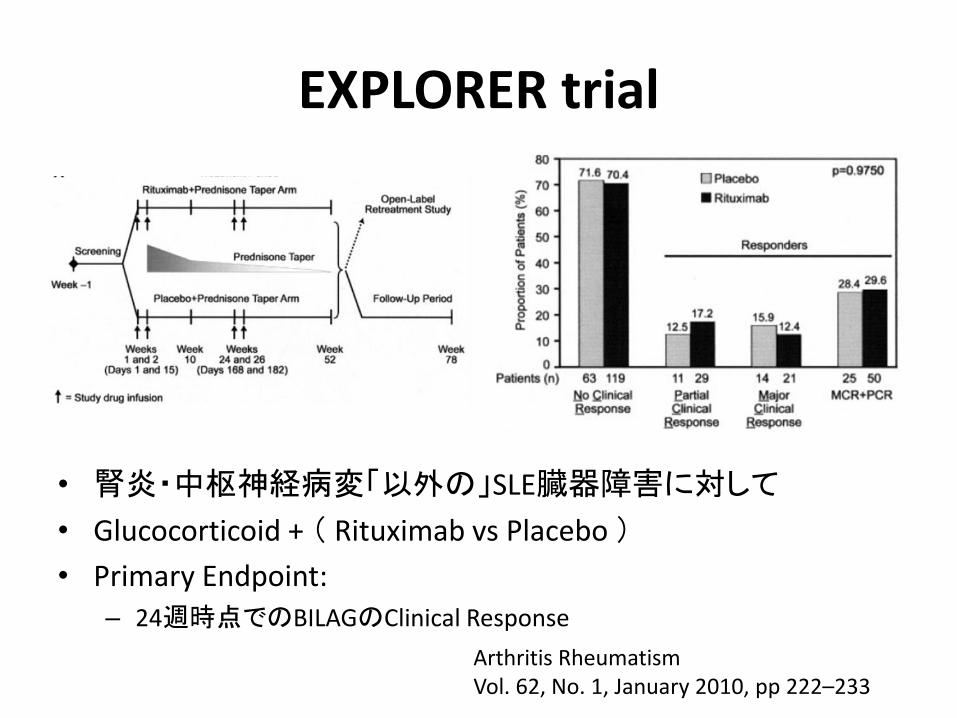
EXPLORER trial
• 腎炎・中枢神経病変「以外の」SLE臓器障害に対して
• Glucocorticoid + ( Rituximab vs Placebo )
• Primary Endpoint:
– 24週時点でのBILAGのClinical Response
Arthritis RheumatismVol. 62, No. 1, January 2010, pp 222–233

Glucocorticoids in RAVE trial
ステロイドパルス(1000mgを1-3日)、その後1mg/kg(最大 80mg/day)で最大4週間その後 40mgで2週間
30mgで2週間15mgで2週間10mgで2週間7.5mgで2週間5mgで2週間2.5mgで2週間→ 中止
N Engl J Med 2013;369:417-27.
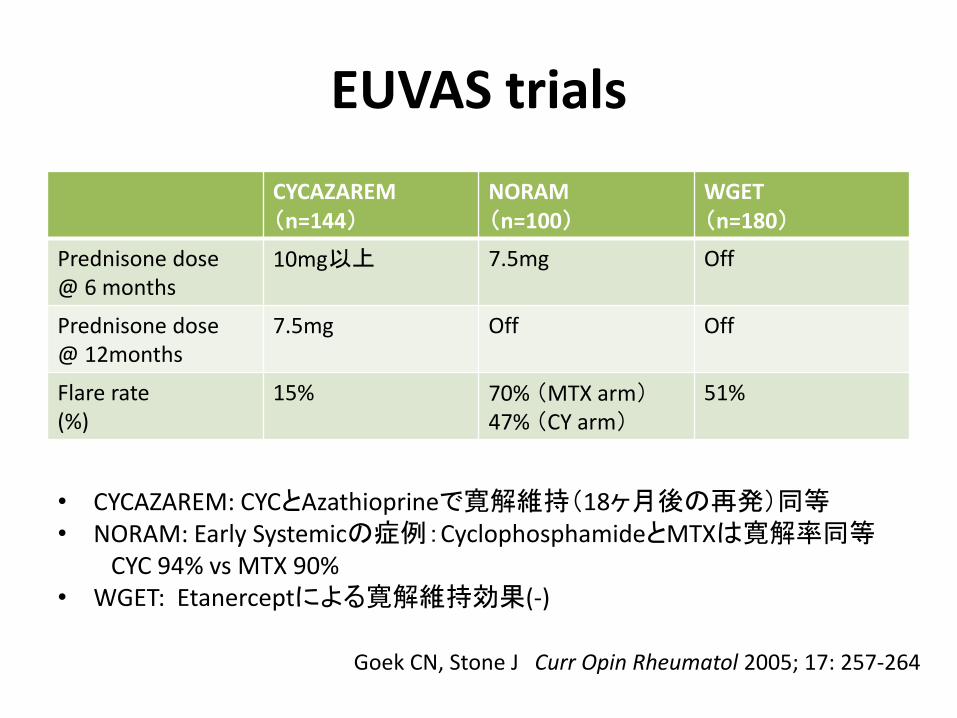
EUVAS trials
CYCAZAREM(n=144)
NORAM(n=100)
WGET(n=180)
Prednisone dose@ 6 months
10mg以上 7.5mg Off
Prednisone dose@ 12months
7.5mg Off Off
Flare rate(%)
15% 70% (MTX arm)47% (CY arm)
51%
• CYCAZAREM: CYCとAzathioprineで寛解維持(18ヶ月後の再発)同等• NORAM: Early Systemicの症例:CyclophosphamideとMTXは寛解率同等
CYC 94% vs MTX 90%• WGET: Etanerceptによる寛解維持効果(-)
Goek CN, Stone J Curr Opin Rheumatol 2005; 17: 257-264
Glucocorticoid in AAV – pearl?
• Pearl: A little bit of prednisone goes a long way toward sustaining disease remissions in AAV.
• 少量ステロイドによる「維持療法」で、
ANCA関連血管炎の再燃率が大幅に低下する。
Stone J “A Clinician’s Pearls and Myths in Rheumatology” p262Springer 2009

関節リウマチ診療におけるGC
• 抗リウマチ(疾患修飾)作用: あり
• 副作用:あり

• リウマチ性多発筋痛症・巨細胞性動脈炎
ステロイドが治療の中心
• SLE・ANCA関連血管炎などの膠原病• 関節リウマチなど破壊性/末梢関節炎
ステロイドは「必要最小限」
• 強皮症
• 強直性脊椎炎など体軸関節炎
ステロイド全身投与は使わない
Behçet病、高安動脈炎、IgG4-RDなど位置付け未
ステロイド投与そのものの工夫
• As much as necessary, as little as possible.
• 隔日投与
Annals of Internal Medicine 1975: 82; 613-8

• biopsy-proven GCA(n=60)
• 60例とも「プレドニゾン 20mgを8時間間隔」で5日間治療
• その後以下の3群にランダムに振り分けた。
1. Group A: prednisone 15mg q8hr
2. Group B: prednisone 45mg q24hr (朝8時に内服)
3. Group C: prednisone 90mg q48hr (朝8時に内服)
• エンドポイントとして、同regimenで1ヶ月治療した場合の「効果」と「副作用」を検討した。
Annals of Internal Medicine 1975: 82; 613-8
• Group Aのうち18例は1ヶ月後にGCAに関連したすべての症状が消失した。– 消失しなかった2例については、そもそもステロイド治療に反応性ではなかった可能性はある。
• Group Bのうち16例で上記と同様の反応が得られた。
• Group C 20例のうち、4週間継続して動脈炎のコントロール良好であったのは、6例のみであった。
• "Hypercortisonism"に関連した副作用が認められたのはGroup Aで9名、Bで7名、Cで0名であった
Annals of Internal Medicine 1975: 82; 613-8
ステロイド・免疫抑制剤以外の工夫
• ACE阻害薬
• ARB
• Spironolactone
• Statin
• ? 尿酸降下剤
Kidney Int 2000: 57; 274-81Am J Med 2006: 119; 912-919Rheumatology 2008: 47; 1093-96
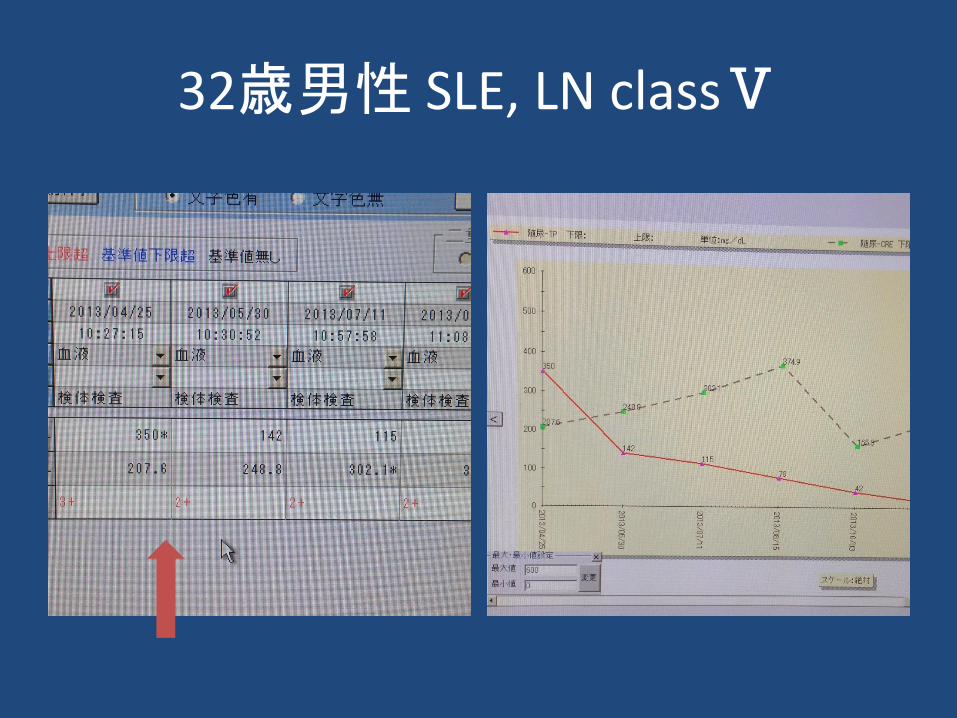
32歳男性 SLE, LN classⅤ

65歳男性結節性多発動脈炎左下肢amputation後CRPのchronicな陽性
• 多くのリウマチ性疾患で「ステロイド中心」の治療はout-of-dateになりつつある
• しかし、全くの”Glucocorticoid-free therapy”が困難なリウマチ性疾患も多い。
ステロイドは添えるだけAs of 2015.