Embed Size (px)
Citation preview

Upper GI Upper GI Hemorrhage:Hemorrhage:Emergency Emergency ManagementManagement
พญพญ. . ปิยะธดิา หาญสมบูรณ์ปิยะธดิา หาญสมบูรณ์หวัหน้างานโรคทางเดินอาหารหวัหน้างานโรคทางเดินอาหาร
กลุ่มงานอายุรศาสตร ์โรงพยาบาลกลุ่มงานอายุรศาสตร ์โรงพยาบาลราชวถีิราชวถีิ

Admission Rate 100/100,000Admission Rate 100/100,000 Incidence 50-100/100,000 per Incidence 50-100/100,000 per
yearyear

Clinical Clinical Manifestations:Manifestations: HematemesisHematemesis MelenaMelena HematocheziaHematochezia

Causes of acute upper Causes of acute upper gastrointestinal gastrointestinal harmorrhageharmorrhageDiagnosisDiagnosis Approx%Approx%
Peptic ulcerPeptic ulcer 35-5035-50Gastroduodenal erosions Gastroduodenal erosions 8-158-15OesophagitisOesophagitis 5-155-15VaricesVarices 5-105-10Mallory Weiss tearMallory Weiss tear 1515Upper gastrointestinal Upper gastrointestinal malignancymalignancy
11
Vascular malformations Vascular malformations 55RareRare 55

Acute Nonvariceal Acute Nonvariceal hemorrhagehemorrhage

Acute Variceal Acute Variceal hemorrhagehemorrhage

Portal Hypertensive Portal Hypertensive GastropathyGastropathy

Basic Principle in Basic Principle in ManagementManagement
Rapid AssessmentRapid Assessment Initial ResuscitationInitial Resuscitation

WhenWhen??
How manyHow many??

When to transfuse When to transfuse blood? blood? Changes in vital signsChanges in vital signs Continuous bleedingContinuous bleeding Signs of poor tissue oxygenationSigns of poor tissue oxygenation Low hematocrit (Hct 20-25%)Low hematocrit (Hct 20-25%)

TargetTarget Hemoglobin 10mg/dL Hemoglobin 10mg/dL ElderElder Hemoglobin 7-8 mg/dLHemoglobin 7-8 mg/dL normal adultnormal adult Hemoglobin 9 mg/dL patient with Hemoglobin 9 mg/dL patient with
portal hypertension portal hypertension Fresh Frozen Plasma 1 unit/ 4 units Fresh Frozen Plasma 1 unit/ 4 units
PRCPRC Platelet concentration if < 50,000Platelet concentration if < 50,000

AssessmentAssessment

ageage
prior gastrointestinal bleedingprior gastrointestinal bleeding
previous gastrointestinal diseaseprevious gastrointestinal diseaseprevious gastrointestinal previous gastrointestinal surgerysurgeryunderlying medical disorder (especially liver underlying medical disorder (especially liver disease)disease)use of nonsteroidal anti-inflammatory drugs including use of nonsteroidal anti-inflammatory drugs including aspirinaspirinuse of anticoagulation and/or antiplatelet use of anticoagulation and/or antiplatelet therapytherapy
abdominal painabdominal pain
change in bowel habitchange in bowel habit
weight lossweight loss
anemiaanemiahistory of oropharyngeal history of oropharyngeal diseasedisease
Important History

Vital SignsVital Signs Blood loss (% Blood loss (% of intravascular of intravascular vol)vol)
Severity of Severity of bleedbleed
Shock (resting Shock (resting hypotension)hypotension)
20-2520-25 MassiveMassive
Postural Postural (orthostatic (orthostatic hypotension hypotension and and tachycardia)tachycardia)
10-2010-20 ModerateModerate
NormalNormal <10<10 minorminor
Hemodynamic status and severity of GI bleeding

Characteristics of Characteristics of vomitusvomitus Bright red vomitusBright red vomitus Coffee groundCoffee ground

Objectives of NG Objectives of NG LavageLavage Appearance of gastric contentAppearance of gastric content Clear the stomach for the Clear the stomach for the
endoscopyendoscopy Prevent pulmonary aspirationPrevent pulmonary aspiration

NG aspirate colorNG aspirate color Stool colorStool color Mortality %Mortality %
ClearClear Brown or RedBrown or Red 66
Coffee groundCoffee ground Brown or blackBrown or black 8.28.2
RedRed 19.119.1
Red BloodRed Blood BlackBlack 12.312.3
BrownBrown 19.419.4
RedRed 28.728.7
Cappelli MS, et al. High risk gastrointestinal bleeding. Cappelli MS, et al. High risk gastrointestinal bleeding. Gastroenterol Clin N AmGastroenterol Clin N Am. 2000;29(2). 2000;29(2)
Aljabreen AM, Fallone CA, Barkun AN. Nasogastric aspirate predicts high risk endoscopic lesions in Aljabreen AM, Fallone CA, Barkun AN. Nasogastric aspirate predicts high risk endoscopic lesions in patients with acute upper GI bleeding. patients with acute upper GI bleeding. Gastrointest EndoscGastrointest Endosc. 2004;59:172.. 2004;59:172.

Risk Risk StratificationStratification

The Rockall risk score The Rockall risk score schemeschemeValueValue ScoreScore
00 11 22 33Age Age (years)(years)
<60<60 60-7960-79 >80>80 --ShockShock No shock No shock
(systolic (systolic BPBP100, 100, pulse<100)pulse<100)
TachycardiTachycardia (systolic a (systolic BPBP100, 100, pulse>100pulse>100))
HypotensioHypotension (systolic n (systolic BP<100)BP<100)
--
ComorbiditComorbidityy
No major No major comorbiditcomorbidityy
-- Cardiac Cardiac failure, failure, ischemic ischemic heart heart disease, disease, any major any major comorbiditcomorbidityy
Renal Renal failure, failure, liver liver failure, failure, disseminatdisseminated ed malignancmalignancyy
DiagnosisDiagnosis Mallory-Mallory-Weiss tear, Weiss tear, no lesion no lesion identified identified and no and no SRHSRH
All other All other diagnosesdiagnoses
Malignancy Malignancy of upper of upper gastrointegastrointestinal tractstinal tract
--
Major Major stigmata stigmata of recent of recent hemorrhaghemorrhagee
None or None or dark spot dark spot onlyonly
-- Blood in Blood in upper upper gastrointegastrointestinal stinal tract, tract, adherent adherent clot, clot, visible or visible or spurting spurting vesselvessel
--
Maximum additive score prior to diagnosis=7, maximum additive score following Maximum additive score prior to diagnosis=7, maximum additive score following diagnosis=11. BP, blood pressure; SRH, stigmata of recent hemorrhagediagnosis=11. BP, blood pressure; SRH, stigmata of recent hemorrhage
Rockall Score > 2 High Risk

Rockall score Rockall score <<2 could be safely 2 could be safely managed in OPD setting managed in OPD setting
Rockall T, Logan R, Devlin H, et al. Selection of patients for early discharged or Rockall T, Logan R, Devlin H, et al. Selection of patients for early discharged or outpatient care after acute gastrointestinal hemorrhage.outpatient care after acute gastrointestinal hemorrhage. Lancet Lancet. 1996;347:1138-. 1996;347:1138-
40.40.

Cipoletta criteriaCipoletta criteria Endoscopic absence of varices, other signs Endoscopic absence of varices, other signs
of portal hypertension, or high risk stigmata of portal hypertension, or high risk stigmata of recent hemorrhageof recent hemorrhage
Absence of hypovolemic shock or orthostasisAbsence of hypovolemic shock or orthostasis Hb > 8mg/dL and no blood transfusionHb > 8mg/dL and no blood transfusion Normal coagulation studiesNormal coagulation studies Absence of serious medical illnessAbsence of serious medical illness Easy accessibility to hospital and adequate Easy accessibility to hospital and adequate
social/family supportsocial/family support
Capoletta L, BiancoM, Rotondana G, et al. Outpatient management for low risk nonvariceal upper GI Capoletta L, BiancoM, Rotondana G, et al. Outpatient management for low risk nonvariceal upper GI bleeding; a randomized controlled trial. bleeding; a randomized controlled trial. Gastrointest EndoscGastrointest Endosc.2002;55:1-5.2002;55:1-5

Longstreth Guidelines for Longstreth Guidelines for selecting Patient with acute UGIH selecting Patient with acute UGIH for OPD carefor OPD careAbsoluteAbsolute
No high risk endoscopic features, varices,or No high risk endoscopic features, varices,or portal hypertensive gastropathyportal hypertensive gastropathy
Not absoluteNot absolute No debilitationNo debilitation No orthostatic vital sigh changesNo orthostatic vital sigh changes No severe liver diseaseNo severe liver disease No anticoagulation therapy or coagulopathyNo anticoagulation therapy or coagulopathy No fresh, voluminous hematemesis or multiple No fresh, voluminous hematemesis or multiple
episodes of melena on the day of presentationepisodes of melena on the day of presentation No severe anemia (hemoglobin 8 g/dL)No severe anemia (hemoglobin 8 g/dL)Adequate support at homeAdequate support at home
Longstreth G, Feitelberg S. Successful outpatient management of acute upper gastrointestinal hemorrhage: use of practice guidelines in a large patient series.
Gastrointest Endosc. 1998;47:219-222.

University of California,San Francisco (UCSF) Triage
Very Low Risk
• age < 60
• Absence of major cormorbid
• No Hx of red hematemesis, hematochezia or bright red nasogastric aspirate
• No Hemodynamic instability
• No significant coagulopathy and profound anemia
D/C from ER
Outpatient workup
Elmunzer BJ, Inadomi JM, Elta GH. Risk Stratification in Upper Elmunzer BJ, Inadomi JM, Elta GH. Risk Stratification in Upper Gastrointestinal Bleeding. Gastrointestinal Bleeding. J Clin GastroenterolJ Clin Gastroenterol 2007;41:559-563. 2007;41:559-563.

LOW RiskLOW Risk• Hemodynamic stable within 1 hour Hemodynamic stable within 1 hour of resuscitationof resuscitation
• No recent red hematemesis, No recent red hematemesis, hematochezia, or bright red hematochezia, or bright red nasogastric aspiratenasogastric aspirate
• No active cardiopulmonary or liver No active cardiopulmonary or liver diseasedisease
• No significant coagulopathy or No significant coagulopathy or profound anemiaprofound anemia
Allow:Allow:Age> 60,coffee ground in NG aspirate, presence of Age> 60,coffee ground in NG aspirate, presence of compensated comorbidities,and initial compensated comorbidities,and initial hemodynamic compromisehemodynamic compromise
EGD
Low risk
D/C from ER
Outpatient workup
Elmunzer BJ, Inadomi JM, Elta GH. Risk Stratification in Upper Elmunzer BJ, Inadomi JM, Elta GH. Risk Stratification in Upper Gastrointestinal Bleeding. Gastrointestinal Bleeding. J Clin GastroenterolJ Clin Gastroenterol 2007;41:559- 2007;41:559-563563.

Blantchford ScoreBlantchford ScoreAdmission risk markerAdmission risk marker ScoreScore
Blood urea nitrogen level Blood urea nitrogen level ((mgmg//dLdL))
>> 18.2 – 22.418.2 – 22.4 22>> 22.4 - 28 22.4 - 28 33>> 2828 - 70- 70 44
>> 7070 66Hemoglobin level for men Hemoglobin level for men ((gg//dLdL))
1212 - - 13 g13 g//dLdL 11
1010 - - 11 g11 g//dLdL 33
< 10< 10 66
Hemoglobin level for women Hemoglobin level for women ((gg//dLdL))
1010 - - 12 g12 g//dLdL 11
< 10< 10 66
Admission risk markerAdmission risk marker ScoreScore
Systolic blood pressures Systolic blood pressures ((mm Hgmm Hg))
100100 -109-109 11
9090 - - 9999 22
<90<90 33
Other markersOther markers
Pulse > 100 per minPulse > 100 per min 11
Presentation with melenaPresentation with melena 11
Presentation with syncopePresentation with syncope 22
Hepatic diseaseHepatic disease 22
Cardiac failureCardiac failure 22
Blantchford score > 0 High RiskBlantchford score > 0 High Risk

The Rockall risk score The Rockall risk score schemeschemeValueValue ScoreScore
00 11 22 33Age Age (years)(years)
<60<60 60-7960-79 >80>80 --ShockShock No shock No shock
(systolic (systolic BPBP100, 100, pulse<100)pulse<100)
TachycardiTachycardia (systolic a (systolic BPBP100, 100, pulse>100pulse>100))
HypotensioHypotension (systolic n (systolic BP<100)BP<100)
--
ComorbiditComorbidityy
No major No major comorbiditcomorbidityy
-- Cardiac Cardiac failure, failure, ischemic ischemic heart heart disease, disease, any major any major comorbiditcomorbidityy
Renal Renal failure, failure, liver liver failure, failure, disseminatdisseminated ed malignancmalignancyy
DiagnosisDiagnosis Mallory-Mallory-Weiss tear, Weiss tear, no lesion no lesion identified identified and no and no SRHSRH
All other All other diagnosesdiagnoses
Malignancy Malignancy of upper of upper gastrointegastrointestinal tractstinal tract
--
Major Major stigmata stigmata of recent of recent hemorrhaghemorrhagee
None or None or dark spot dark spot onlyonly
-- Blood in Blood in upper upper gastrointegastrointestinal stinal tract, tract, adherent adherent clot, clot, visible or visible or spurting spurting vesselvessel
--
Maximum additive score prior to diagnosis=7, maximum additive score following Maximum additive score prior to diagnosis=7, maximum additive score following diagnosis=11. BP, blood pressure; SRH, stigmata of recent hemorrhagediagnosis=11. BP, blood pressure; SRH, stigmata of recent hemorrhage
Clinical Rockall ScoreClinical Rockall Score

Clinical Rockall score 0, no adverse Clinical Rockall score 0, no adverse outcomesoutcomes
1-3,no adverse outcomes, 29% need 1-3,no adverse outcomes, 29% need transfusiontransfusion
>3>3 ,21% rebleeding, 5%surgery, 10% death,21% rebleeding, 5%surgery, 10% death
OPD workup
ThamTham TCK, James C, Kelly M. Predicting outcome of acute non variceal upper TCK, James C, Kelly M. Predicting outcome of acute non variceal upper gastrointestinal hemorrhage without endoscopy using clinical Rockall score. gastrointestinal hemorrhage without endoscopy using clinical Rockall score.
Postgrad MedPostgrad Med J J 2006;82:757-759.2006;82:757-759.
Clinical Rockall < 3

ธนัวาคม 2547

High Risk factorsHost factors:Age> 60 yrsCormorbid conditionsHemostatic instability,orthostatic hypotension, PR> 100,BP < 100CoagulopathyBleeding character:
Continuous red blood from NGRed blood per rectum
Patient course:Need blood transfusionHemodynamic instability

Acute Non Variceal Acute Non Variceal HemorrhageHemorrhage

Bleeding Peptic UlcerBleeding Peptic Ulcer-- EpidemiologyEpidemiology -- More than 300,000 hospital admissions More than 300,000 hospital admissions
annually in the USannually in the US11
Incidence: 103 cases/100,000 adults/yearIncidence: 103 cases/100,000 adults/year22
Mortality: 5~14%Mortality: 5~14%33, unchanged for the past , unchanged for the past two decades, exclusively among elderly two decades, exclusively among elderly patients with significant comorbiditiespatients with significant comorbidities
11Yavorski RT et al. Am J Gastroenterol 1995; 90:568-73Yavorski RT et al. Am J Gastroenterol 1995; 90:568-7322Longstreth GF. Am J Gastroenterol 1995; 90:206-10Longstreth GF. Am J Gastroenterol 1995; 90:206-10
33Rockall TA et al. BMJ 1995; 38:222-6Rockall TA et al. BMJ 1995; 38:222-6

Bleeding Peptic UlcerBleeding Peptic Ulcer-- Natural HistoryNatural History --
Approximately 80-85% bleeding Approximately 80-85% bleeding stops spontaneouslystops spontaneously
Remaining 15-20% recurrent or Remaining 15-20% recurrent or continuous bleedingcontinuous bleeding
Early risk- stratification facilitates Early risk- stratification facilitates appropriate level of careappropriate level of care
Multidisciplinary approachMultidisciplinary approach

RebleRebleedingeding
55 1010 2222 4343 5555
MortaMortalitylity
22 33 77 1111 1111
CleaClean-n-BaseBase
Flat Flat spotspot
AdheAdherentrentClotClot
NBVNBVVV
ActivActive e BleeBleedd
Laine et al. Laine et al. NEJMNEJM 1994; 331:717 1994; 331:717
Risk of rebleeding correlated with endoscopic bleeding stigmaRisk of rebleeding correlated with endoscopic bleeding stigma

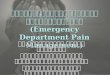
Role of PPIRole of PPI

Keep gastric Keep gastric pH>6pH>6
Platelet Platelet aggregatioaggregation and clot n and clot formationformation
PrinciplePrinciple

Omeprazole before endoscopy in Omeprazole before endoscopy in patients with gastrointestinal patients with gastrointestinal bleedingsbleedings
LauLau JY, Leung WK, Wu JY, Leung WK, Wu JC, et al.JC, et al.
New Engl J MedNew Engl J Med. 2007 . 2007 Apr 19;356(16): 1631-Apr 19;356(16): 1631-
40.40.
N 638N 638
319319319319OmeprazoleOmeprazole
80mgIV bolus,80mgIV bolus,8mg/hr8mg/hr
placeboplacebo
19.1%19.1% 28.4%28.4%Endoscopic RxEndoscopic Rx

Reduced the need for endoscopic therapy
Infusion of high dose Omeprazole before endoscopy acclerated the resolution of signs of bleeding in ulcers
LauLau JY, Leung WK, Wu JC, JY, Leung WK, Wu JC, et al.et al.
New Engl J MedNew Engl J Med. 2007 . 2007 Apr 19;356(16): 1631-40Apr 19;356(16): 1631-40..

High dose PPI after High dose PPI after endoscopic therapyendoscopic therapy Decreased RebleedingDecreased Rebleeding Decreased SurgeryDecreased Surgery
Cochrane systematic review 2005Lau JY, Sung JJ, Lee KK, et al. Effect of intravenous omeprazole on
recurrent bleeding after endoscopic treatment of bleeding peptic ulcers. N Engl J Med. 2000;343: 310-16.

Endoscopic Management Endoscopic Management of Non variceal of Non variceal HemorrhageHemorrhage Injection TherapyInjection Therapy Thermal DevicesThermal Devices Mechanical DevicesMechanical Devices

Acute Variceal Acute Variceal BleedingBleeding

Esophageal VaricesEsophageal Varices 50% in cirrhosis50% in cirrhosis 20% varices – large at presentation20% varices – large at presentation Developing rate 10-15% per yearDeveloping rate 10-15% per year 1/3 varices bleed1/3 varices bleed Mortality rate ~20-30% /bleeding Mortality rate ~20-30% /bleeding
episodeepisode 50% stop spontaneously50% stop spontaneously

Variceal Pressure Variceal Pressure mm Hgmm Hg
Incidence of Incidence of bleeding %bleeding %
< 13< 13 00>13-14>13-14 99>14-15>14-15 1717>15-16>15-16 5050>16>16 7272


Predicting Variceal Predicting Variceal HemorrhageHemorrhageChild ClassChild ClassRedRedWalWalee
AA BB CCF1F1 F2F2 F3F3 F1F1 F2F2 F3F3 F1F1 F2F2 F3F3
-- 66 1010 1515 1010 1616 2626 2020 3030 4242++ 88 1212 1919 1515 2323 3333 2828 3838 5454++++++
1616 2323 3434 2828 4040 5252 4444 6060 7272

Risk Factors for recurrent Risk Factors for recurrent hemorrhagehemorrhageEarly Rebleeding Early Rebleeding <6wk<6wk
Late Rebleeding Late Rebleeding >6wk>6wk
Age > 60Age > 60 Severity of liver Severity of liver failurefailure
Severity of initial Severity of initial bleedbleed
AscitesAscites
Renal failureRenal failure HepatomaHepatomaAscitesAscites Active alcoholismActive alcoholismActive Bleeding on Active Bleeding on scopescope
Red signsRed signs
Platelet clot on Platelet clot on varicevariceRed signsRed signs

Sherry red spot (red Sherry red spot (red color sign)color sign)
Red SpotRed Spot Red Wale sign (varices Red Wale sign (varices on varix)on varix)

Esophageal VaricesEsophageal Varices
Platelet clot

Initial Management:Initial Management: Resuscitation and Blood TransfusionResuscitation and Blood Transfusion
(Keep hemoglobin 8gm/dl) (Keep hemoglobin 8gm/dl) Class I Level BClass I Level B Antibiotic prophylaxis for 7 daysAntibiotic prophylaxis for 7 days
Norfloxacin 400 mg bid or IV Ciprofloxacin Norfloxacin 400 mg bid or IV Ciprofloxacin Class I Level AClass I Level A
Ceftriazone 1 gm/day Ceftriazone 1 gm/day Class I Level BClass I Level B Pharmacologic Therapy 3-5 days Pharmacologic Therapy 3-5 days Class I Class I
Level ALevel ASomatostatin and analogsSomatostatin and analogsTerlipressinTerlipressin
EGD within 12EGD within 12 hourshours++EVL or EVL or sclerotherapy sclerotherapy Class I Level AClass I Level A
BalloonBalloon tamponade used as temporary tamponade used as temporary measure (max 24 hours) measure (max 24 hours) Class I Level BClass I Level B
ACG Practice Guideline 2007ACG Practice Guideline 2007

N-2 butyl-cyanoacrylate for N-2 butyl-cyanoacrylate for bleeding gastric varices: A bleeding gastric varices: A United states pilot study and United states pilot study and cost analysiscost analysis
RebleediRebleedingng72 hour72 hour 2/37 2/37
(5.5%)(5.5%)6 week6 week 1/30 1/30
(3%)(3%)1 year1 year 5/28 5/28
(18%)(18%)
survivalsurvival3 3 monthsmonths
30/34 30/34 (88%)(88%)
1 year1 year 24/31 24/31 (29%)(29%)
Greenwald BD, Caldwell SH, Hespenheide EE, et alAm J Gastroenterol 2003 Sep;98(9):1982-8.
Odd of Death > 7 fold non Odd of Death > 7 fold non cyanoacrylate groupcyanoacrylate group

Role of SurgeryRole of Surgery Severe hemorrhage unresponsive Severe hemorrhage unresponsive
to initial resuscitationto initial resuscitation Unavailable or failure of Unavailable or failure of
endoscopic therapyendoscopic therapy Coexisting 2Coexisting 2ndnd indication to indication to
operations such as perforation, operations such as perforation, obstruction or suspicious of obstruction or suspicious of malignancymalignancy