Embed Size (px)
Citation preview

Presented By:
Manali Baghel
Ph.D. Scholar
College of Biotechnology
DUVASU

Cervical cancer is a female-specific disease with ahigh incidence and mortality behind breast & lungcancer
A disease in which malignant cells form in thetissues of the cervix
It rises in 30–34 years of age and peaks at 55–65years
The worldwide incidence of cervical cancer is~510,000 new cases with ~288,000 deathsannually
Cervical cancer is a complex disease caused by theinteraction of viral, host, and environmental factors
Prevention, diagnosis, and treatment of female-specific diseases areincreasingly important issues due to lifestyle changes of women
Human pappilomavirus (HPV) has been detected in more than 90% ofcervical cancers and therefore implicated as the main cause of cervicalcancer
HPV infection alone is not sufficient to induce the malignanttransformation of HPV-infected cells
Other unidentified genetic alterations, such as microRNAs the masterswitches, are required.
MiRNAs are found to be associated in many cases of cervical cancer withchanged expressions.

Signs and Symptoms
The most common symptoms are:
Bleeding between periods
Bleeding after sexual intercourse
Bleeding in post-menopausal women
Discomfort during sexual intercourse
Smelly vaginal discharge
Vaginal discharge tinged with blood
Pelvic pain
Causes
Risk factors which are known to increase the risk ofdeveloping cervical cancer-
Human pappilomavirus (HPV)
Many sexual partners, becoming sexually active early
Smoking
Weakened immune system
Giving birth at a very young age
Several pregnancies
Contraceptive pill
Other sexually transmitted diseases (STD)
Chlamydia, gonorrhea
Genetic Alterations

Stages of Cervical Cancer
Mild Dysplasia
Moderate Dysplasia
Severe Dysplasia
Invasive Cervical Cancer
Stages of cervical cancer according to WHO classification-

Types of Cervical Cancer
Ectocervix-
Squamous Cell
Carcinoma
Endocervix-
Adenocarcinoma

Tests To diagnose Cervical Cancer
Phisical Exam & History
Pelvic Exam
Pap Test
HPV Test
Endocervical Curettage
Colposcopy
Biopsy

Cervical Cancer Vaccines
Two Vaccines are Licensed globally
which are also available in India:
A Quardivalent vaccine- Gardasil
(Merk)
HPV Serotypes 16, 18, 6 & 11
A bivalent vaccine- Cervarix
(Glaxo Smith Kline)
HPV serotypes HPV 16 & 18 Gardasil

Human Pappilomavirus (HPV)
One of the most common STIs
Papillomaviruses are small viruses approximately 52-55nm in size
HPVs are circular double stranded DNA viruses & belongs to family-Papillomaviridae
In 1981, Zur Hausen et al. reported the detection of HPV in cervicalneoplasia
In 1995 the WHO declared HPV as a known carcinogen for causingcervical cancer, because HPV DNA types could be detected in almost allcervical cancers
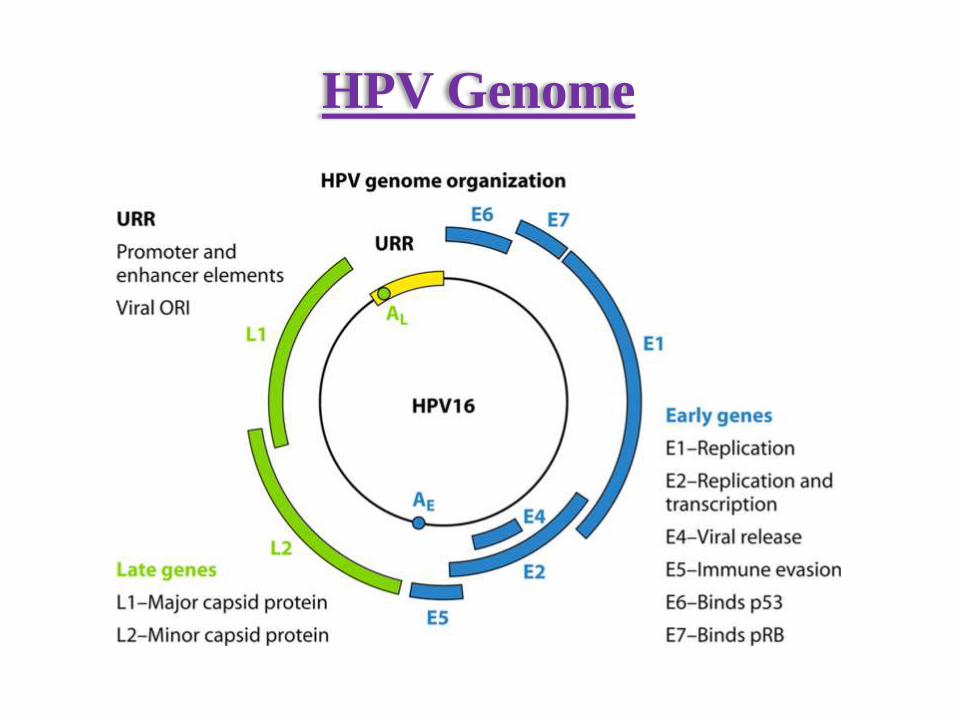
HPV Genome

Classification Of HPV
More than 100 types of human papilloma viruses (HPVs)
are known today, and they are generally classified according
to their potential to induce malignant transformation-

HPV Life Cycle and Infection
The HPV life cycle consists of initial infection, uncoating, genome
maintenance, genome amplification, and packaging to form new viral
particles
HPV Induced Dysregulation
Once viral DNA is incorporated into host DNA, oncogenic transformationis induced
Oncoproteins E6 & E7 inactivate tumor suppressor genes p53 & pRB.
E6 protein binds to E6-associated protein (E6-AP), a ubiquitin proteinligase , & forms E6/E6-AP complex & targets p53
E6 degrades p53, inhibits p53 binding to DNA & binds to p53 enhancers &suppressed p53 function
E6/E6-AP complex also activates telomerase & contributes to cellimmortalization
E7 protein contributes to carcinogenesis by degrading Rb family proteinsnecessary for cell cycle progression

HPV Determition
PCR-based methods are commonly used for HPV Detection
after DNA isolation
Most PCR assays utilize consensus primers, directed to a
conserved L1 gene, and hence are able to amplify most of the
mucosal HPV types
The other PCR type used to detect specific HPV is HPV type
specific PCR such as HPV 16 or 18

MicroRNA
MicroRNAs are small (~18-24 nt), non-coding RNAs that regulategene expression & associated with cancer
First miRNA, lin-4, was discovered in C. elegans in 1993, is foundin most eukaryotes, including humans
It is predicted that miRNA account for 1-5% of the human genomeand regulate at least 30% of protein-coding genes
To date, more than 17,000 miRNAs have been annotated in 142species, including over 1900 human miRNAs

MiRNA Biogenesis & Function
Classification of MiRNAs
MicroRNAs are classified in two group depending on their
origin-
Intergenic or Exonic miRNAs: located between the introns of
genes & transcribed by RNA pol II or pol III as a stem loop structure called
pri-miRNA
Interagenic or Intronic miRNAs: miRNAs located within an
intron of a protein coding gene & transcribed by RNA pol II as part of pre-
mRNA

MiRNA Time Line
(Lindow et al., 2012)

MiRNA Expression Profiling
Initially it was conducted on samples extracted from tissues, now stable
miRNAs are found in readily available body fluids including, serum ,
plasma, urine and saliva
MiRNA expressions are generally analyzed by microarray & qRT-PCR
using microRNA specific primers
U6 RNA, RNU44, and RNU48 is usually used as reference control & A.
thaliana miRNA as negative control
Quantification is done using the 2 delta Ct method, where fold change in
expression of a gene in an experimental sample is quantified relative to the
same gene in a reference sample

MiRNAs In Cervical Cancer
MiRNAs play a vital role in cancer regulating pathways, like controlling
cell proliferation, differentiation and survival
MiRNAs involved in carcinogenesis are classified into oncogenic miRNAs
(oncomiRs) and tumor suppressor miRNAs(TSG)
Involved in cancer pathogenesis by posttranscriptional regulation of gene
expression
50% of miRNA genes are localized in cancer-associated genomic regions
or in fragile sites or integration sites of high-risk HPVs
Expression patterns of miRNAs suggested that beyond HPV, microRNAs
play a major role in cervical cancer

Altered Expressions of MiRNAs in
Cervical Cancer
MicroRNAs expressions were analyzed for normal cervix and cervical
cancer tissues, by microarray in combination with RT-PCR verification &
found to be deregulated
On comparision, many miRNAs with cancer-specific upregulation or
downregulation have been found-
MiR-21 is overexpressed in cervical cancer and is a negative regulator of
expression of the tumor suppressor gene programmed cell death 4
(PDCD4)

MiR Let-7a was found to be downregulated by HPV & this
downregulation of miR let-7a leads to the aberrant expression of STAT3
(validate target of let-7a) developing CC
MiR- 218 is found to be underexpressed in CC tissues compared to the
normal cervix & leads to the decreased expression of LAMB3, which is
involved in cell migration and tumorigenicity
MiR-34a was identified as a direct transcriptional target of cellular
transcription factor p53, since HPV E6 oncoprotein destabilizes p53 during
virus infection, it causes down-regulation of miR-34a expression in most
CC tissues
Cont..

Regulation of miRNAs by HPV
Oncoproteins
Deletions or mutations in miRNA genes, as well as
aberrant expression of oncogenic or tumor-
suppressive miRNAs, are common in human
cancers
Deregulation of oncogenic and tumor suppressive
miRNAs in human cervical cancer is associated
with HR-HPV integration
Cervical cancer represents a unique tumor model
for understanding how viral E6 and E7
oncoproteins deregulate the expression of the
microRNA
MiRNAs
HPV

HPV-oncoproteins regulated miRNAs and factors
involved in malignant transformation.

miRNA Chromosome Putative Function
hsa-miR-210 11 Oncogenic (og)
hsa-miR-182 07 Og/tumeor suppressor(tsg)
hsa-miR-183 08 Og/tsg
hsa-miR-200c 12 Tumor suppressor
hsa-miR-203 14 Og/tsg
hsa-miR-193b 16 oncogenic
hsa-miR-34a 01 tsg
hsa-miR-31 11 og/tsg
hsa-miR-210 11 Og/tsg
hsa-miR-27a 19 Og/tsg
hsa-miR-503 X Og/tsg
hsa-miR-27b 09 Og/tsg
hsa-miR-127 14 og/tsg

MiRNAs Underxpressed in Cervical
Cancer Cell Lines
MiRNA Chromosome Putative Function
hsa-miR-126 09 Og/tsg
hsa-miR-145 05 Og/tsg
hsa-miR-451 17 Og/tsg
hsa-miR-195 19 Og/tsg
hsa-miR-143 05 Og/tsg
hsa-miR-199b 09 Og/tsg
hsa-miR-1 01 Og/tsg
hsa-miR-495 14 Og/tsg
hsa-miR-497 17 Og/tsg
hsa-miR-133b 06 Og/tsg
hsa-miR-223 X Og/tsg
hsa-miR-149 02 Og/tsg

HPV-Oncoproteins are able to regulate the
expression of miRNAs
HPV Proteins MiRNAs Up/Downregulated Target Gene
E5 mir-146a Up-regulated ZNF813
E5 mir-324-5p Down-regulated CDH2, CTNNB1
E5 mir-203 Down-regulated p63
E6 mir-34a Down-regulated p18Ink4c, CDK4,CDK6, Cyclin E2
E6 mir-218 Down-regulated LAMB3
E6 mir-23b Down-regulated uPA
E6/E7 mir-29 Down-regulated YY1 and CDK6
E7 mir-15b Down-regulated CCNA2, CCNB1,CCNB2 MSH6
E7miR-15a/miR-16-1 andmiR-203
Down-regulated c-Myc, c-Myb, PPAR

Diagnosis & Treatment of Cervical Cancer
Using miRNAs
Many studies have examined the use ofmiRNAs as cancer diagnostic marker and asanticancer therapy.
Diagnosis of Cervical Cancer Using
miRNAs in Serum
MiRNAs with expression changes in cancer have the potential to be
diagnostic biomarkers based on plasma & serum tests
miR-21 and miR-126 are found to be overexpressed in serum and are
associated with cervical cancer.
Overexpression of other miRs including miR-27a, miR-34, miR-34a, miR-
146a, miR-155, miR-196a, miR-203, and miR-221 was detected in the
serum of CC samples
These results indicate that miRNA levels in serum can be used for
diagnosis of cervical cancer

Diagnosis of Lymph Node Metastasis
Using miRNAs in Serum
Several miRNAs in serum have been identified as candidate markers for
lymph node metastasis in CC
Zhao et al. analyzed expression of miR-20a and miR-203 in serum
collected before surgery and treatment in 80 patients:
The miR-20a level in serum of patients with CC was markedly higher than
that in healthy volunteers and was overexpressed in patients with lymph
node metastasis
The expression level of miR-203 in patients with CC was higher in
comparison with healthy volunteers, however, lymph node metastasis was
found only when miR-203 expression was suppressed

MiRNA Therapeutic Approaches
MiRNA
Inhibition therapy
when the target miRNA
is overexpressed
MiRNA
Supplementation
therapy when the
miRNA is repressed

Treatment with miRNA
Supplementation
Anticancer treatment may be achieved by regulating the expression
level of miRNAs
The function of tumor suppressor miRs with reduced levels may be
recovered by supplementation of the miRNA itself
Atelocollagen, is being examined as a potential delivery system for
nucleic-acid-based drugs
This protein is extracted from calf dermis and then digested with
protease to reduce antigenicity & can be transferred in to tissues or
cells
Supplementary agents can be classified as:
o Hairpin single-stranded pre-miRNA
o Double-stranded RNA
Liu et al. introduced miR-143 into HeLa CC cells and showed that cell
growth was inhibited and apoptosis was enhanced with increased miR-143
expression & maintained Bcl2 (oncogene) expression
o Therefore, miR-143 has an association with Bcl2 and treatment targeting
this pathway may be possible
Similarly, supplementing anti-let7a miR in HPV16 positive CC cases can
increase the expression of down-regulated let-7a miR & maintain the
expression of STAT3
Cont..

Treatment by Inhibition of
miRNA Function
One strategy for overexpressed miRNA in cancer is to inhibit the miRNA
function using agents with complementary binding to the miRNA
Antisense miRNA oligonucleotides (AMOs) or ‘antagomirs’ are the most
common miRNA inhibitors based on Antisense technology
• For miR-21, an oncomiR in cervical cancer, anti-miR-21 was developed as
a modified 2’-O-methoxyethyl (2’-O-MOE) phosphorothioate antisense
agent
• Wang et al. found, miR-21 expression was downregulated and tumor
growth was markedly suppressed by the AMO in comparison with a control
group

• MiR-21 inhibition may be achieved with other approaches,
including miRNA sponges, miRNA erasers, and tough decoys
• Tough decoys may have particularly potent inhibitory activity
• Haraguchi et al. inhibited miR-21 using a tough decoy and
recovered expression of PDCD4, a target gene of miR-21
Cont..

Difference MiRNA Based Drug &
Traditional Drug
Miravirsen, first miR based drug, made for silencing
miR-122 in HCV infected patients.

Anti-miR Treatment In Other Deseases

miRNAs Associated with Therapeutic
Resistance for Cervical Cancer
Expression of various miRNAs is up- or downregulated in cervical cancer
and these expression levels can increase or decrease sensitivity to
chemotherapy and radiotherapy
Phuah et al. showed that the expression patterns of 25 miRNAs, including
miR-138, miR-210, and miR-744, altered the sensitivity to 1’S-1’-
acetoxychavicol (ACA) and cisplatin
Lei et al. found that miR-155 negatively regulates the EGF-induced
epithelial-mesenchymal transition(EMT), inhibits proliferation, metastasis,
invasion, and increases sensitivity to cisplatin
Thus, miRNAs may have an important role in the response to
chemotherapy

Summary & Conclusion
HPV
Cervical
Cancer
Progression
Cervical cancer remains as a leading cause of
morbidity and mortality for women worldwide
HPV Integration may alter miRNA expression via
deletion, amplification, or genomic rearrangement
which may have implications for their expression in
cervical cancer
Depending on the nature of their targets, miRNAs
can function as either tumor suppressor miRs or
oncogenic miRs.
These findings suggest many approaches to miRNA-
specific personalized treatment and molecular targeted
therapy
Therefore, miRNAs are likely to be important in
diagnosis and treatment of cervical cancer.
Target
MiRNA

References
• Walboomers JM, Jacobs MV, Manos MM, Bosch FX, Kummer JA, et al.(1999) Human papillomavirus is a necessary cause of invasive cervicalcancer worldwide. J Pathol 189: 12-19.
• de Villiers EM, Fauquet C, Broker TR, Bernard HU, zur Hausen H (2004)Classification of papillomaviruses. Virology 324: 17-27.
• Ho GY, Bierman R, Beardsley L, Chang CJ, Burk RD (1998) Natural history ofcervicovaginal papillomavirus infection in young women. N Engl J Med338: 423-428.
• zur Hausen H (2002) Papillomaviruses and cancer: from basic studies toclinical application. Nat Rev Cancer 2: 342-350.
• Klingelhutz AJ, Foster SA, McDougall JK (1996) Telomerase activation bythe E6 gene product of human papillomavirus type 16. Nature 380: 79-82.
• Scheffner M, Werness BA, Huibregtse JM, Levine AJ, Howley PM (1990)The E6 oncoprotein encoded by human papillomavirus types 16 and 18promotes the degradation of p53. Cell 63: 1129-1136.

• Werness BA, Levine AJ, Howley PM (1990) Association of humanpapillomavirus types 16 and 18 E6 proteins with p53. Science 248: 76-79.
• Huibregtse JM, Scheffner M, Howley PM (1991) A cellular proteinmediates association of p53 with the E6 oncoprotein of humanpapillomavirus types 16 or 18. EMBO J 10: 4129-4135.
• Dyson N, Howley PM, Munger K, Harlow E (1989) The human papillomavirus-16 E7 oncoprotein is able to bind to the retinoblastoma geneproduct. Science 243: 934-937.
• Munger K, Werness BA, Dyson N, Phelps WC, Harlow E, et al. (1989)Complex formation of human papillomavirus E7 proteins with theretinoblastoma tumor suppressor gene product. EMBO J 8: 4099-4105.
• Farh KK, Grimson A, Jan C, Lewis BP, Johnston WK, et al. (2005) Thewidespread impact of mammalian MicroRNAs on mRNA repression andevolution. Science 310: 1817-1821.
• Volinia S, Calin GA, Liu CG, Ambs S, Cimmino A, et al. (2006) AmicroRNA expression signature of human solid tumors defines cancer genetargets. Proc Natl Acad Sci U S A 103: 2257-2261.

• He, L., He X., Lim, L.P. et al., (2007). A microRNA component of the p53tumour suppressor network. Nature. 447, 1130–1134.
• H. L. Howie, R. A. Katzenellenbogen, and D. A. Galloway, “PapillomavirusE6 proteins,” Virology, vol. 384, no. 2, pp. 324–334, 2009.
• T. Kiyono, A. Hiraiwa,M. Fujita, Y. Hayashi, T. Akiyama, and M. Ishibashi,“Binding of high-risk human papillomavirus E6 oncoproteins to the humanhomologue of the Drosophila discs large tumor suppressor protein,”Proceedings of the National Academy of Sciences of the United States ofAmerica, vol. 94, no.21, pp. 11612–11616, 1997.
• Kozomara A, Griffiths-Jones S. MiRBase: integrating microRNA annotation and deep-sequencing data. Nucleic Acids Res 2011;39:D152–7.
• Q. Yao, H. Xu, Q.-Q. Zhang, H. Zhou, and L.-H. Qu, “MicroRNA-21 promotescell proliferation and down-regulates the expression of programmed celldeath 4 (PDCD4) in HeLa cervical carcinoma cells,” Biochemical andBiophysical Research Communications, vol. 388, no. 3, pp. 539–542, 2009.

• S. Gilad, E. Meiri, Y. Yogev et al., “Serum microRNAs are promising novelbiomarkers,” PLoS One, vol. 3, no. 9,Article ID e3148, 2008.
• P. S. Mitchell, R. K. Parkin, E. M. Kroh et al., “Circulating microRNAs as stableblood-based markers for cancer detection,” Proceedings of the NationalAcademy of Sciences of the United States of America, vol. 105, no. 30, pp.10513–10518, 2008.
• C. H. Lawrie, S. Gal, H. M. Dunlop et al., “Detection of elevated levels oftumour-associated microRNAs in serum of patients with diffuse large B-celllymphoma,” British Journal of Haematology, vol. 141, no. 5, pp. 672–675,2008.
• S. M. Wilting, R. A. van Boerdonk, F. E. Henken et al., “Methylation-mediatedsilencing and tumour suppressive function of hsa-miR-124 in cervical cancer,”Molecular Cancer, vol. 9, article 167, 2010.
• X. M. Wang, J. Xu, Z. Q. Cheng et al., “Study on effects of microRNA-21antisense oligonucleotide in vivo and in vitro on bionomics of human cervicalsquamous carcinoma cell lines SiHa,” Chinese Journal of Pathology, vol. 41, no.4, pp. 254–259, 2012.
• T. Haraguchi, Y. Ozaki, and H. Iba, “Vectors expressing efficient RNA decoysachieve the long-term suppression of specific microRNAactivity inmammaliancells,”Nucleic Acids Research, vol. 37, no. 6, article e43, 2009.