Embed Size (px)
Citation preview

慈恵医大付属病院本院
研修医 久保 英祐

CONTENTS
➢INTRODUCTION
➢METHODOLOGY
➢GUIDELINE RECOMMENDATION FOR CDI
– Epidemiology
– Diagnosis
➢INFECTION PREVENTION AND CONTROL
– Isolation measure for patients with CDI
– Treatment
CONTENTS
➢INTRODUCTION
➢METHODOLOGY
➢GUIDELINE RECOMMENDATION FOR CDI
– Epidemiology
– Diagnosis
➢INFECTION PREVENTION AND CONTROL
– Isolation measure for patients with CDI
– Treatment
INTRODUCTION
• 2010年 IDSA/SHEA “CDIに関するガイドライン”
→疫学、予防、診断、治療を update
• 小児に関する記載も追加

INTRODUCTION
<CDI : Clostridium difficile infection とは>
• 症状がある(通常は下痢)
AND
• 検査が陽性
– CD毒素が陽性
–毒素を産生するCDの同定
–内視鏡的あるいは組織学的に偽膜性腸炎の診断

〈背景(アメリカでは)〉
• 欧州でCDIの感染はピークアウトしているが, アメリカではいまやっとプラトーに達した頃である
• 年間500,000人の感染, 15,000-30,000人以上の死亡に関連し, 入院患者への費用は$48億を超えるため問題となっている.
• 前回のガイドライン作成から7年もたち, 今回の改訂となった.
〈今後の展望〉
• 新規薬剤(Bezlotoxumab),PCRを用いた診断キットが次々と登場している.(Bezlotoxumabは再発リスクの高い患者への補助療法として)
• 技術革新は止まっておらず,近い未来にまた診療は進化するが, それは次回の改定で.
INTRODUCTION
CONTENTS
➢INTRODUCTION
➢METHODOLOGY
➢GUIDELINE RECOMMENDATION FOR CDI
– Epidemiology
– Diagnosis
➢INFECTION PREVENTION AND CONTROL
– Isolation measure for patients with CDI
– Treatment

METHODOLOGY
• 14人のパネルメンバーから構成
• GRADE system によるエビデンスレベル・推奨度
• 5つのデータベースを使用
– Medline, Embase, Cochrane Central Registry of Controlled trials, Health Technology Assessment, the Database of Abstracts of Reviews of Effects
• 成人:前回のガイドライン(2010年)に加え, 2016年までの文献を検索.
• 小児:今回から追加. 1977-2016年の文献を検索.

推奨度
• GRADE法:Grading of Recommendations Assessment, Development, an Evaluation methodologist
• 証拠となる試験のデザイン・質
• リスク&ベネフィット
• 患者の価値観
• 医療資源・コスト
を総合した推奨度を評価として用いている
CONTENTS
➢INTRODUCTION
➢METHODOLOGY
➢GUIDELINE RECOMMENDATION FOR CDI
– Epidemiology
– Diagnosis
➢INFECTION PREVENTION AND CONTROL
– Isolation measure for patients with CDI
– Treatment

Epidemiology
1. How are CDI cases best defined?
2. What is the minimal surveillance recommendation for institutions
3. What is the best way to express CDI incidence and rates?
4. How should CDI surveillance be approached in settings of high endemic rates or outbreaks?
5. What is the recommended CDI surveillance strategy for pediatric institutions?
(for children)
1. CDIの分類
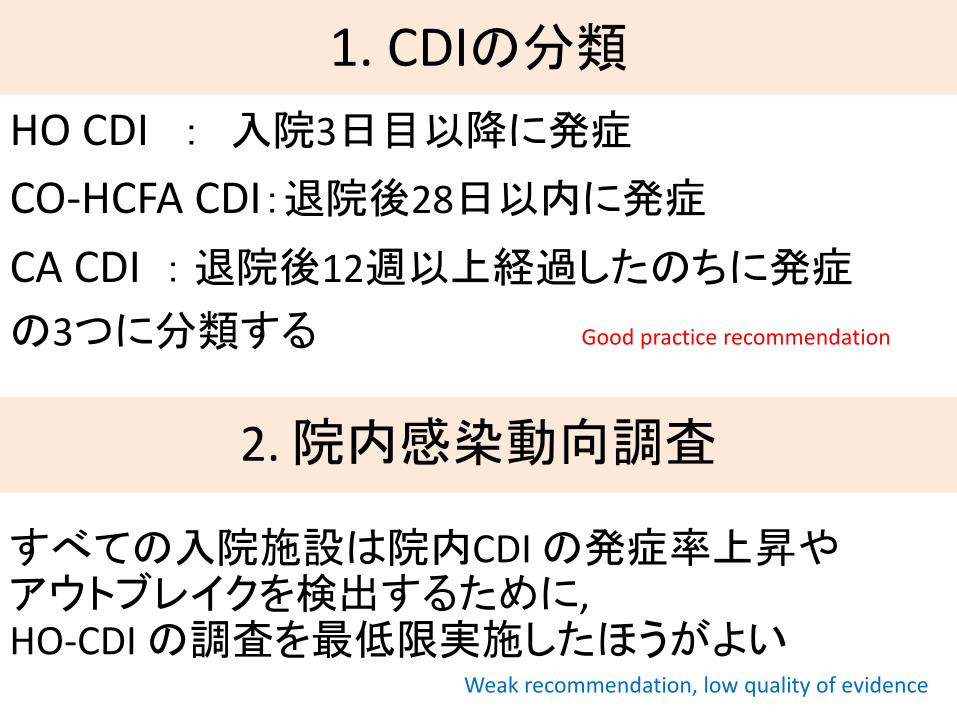
HO CDI : 入院3日目以降に発症
CO-HCFA CDI:退院後28日以内に発症
CA CDI : 退院後12週以上経過したのちに発症
の3つに分類する Good practice recommendation
2. 院内感染動向調査
すべての入院施設は院内CDI の発症率上昇やアウトブレイクを検出するために,HO-CDI の調査を最低限実施したほうがよい
Weak recommendation, low quality of evidence

Epidemiology
1. How are CDI cases best defined?2. What is the minimal surveillance recommendation for
institutions
3. What is the best way to express CDI incidence and rates?
4. How should CDI surveillance be approached in settings of high endemic rates or outbreaks?
5. What is the recommended CDI surveillance strategy for pediatric institutions?
(for children)
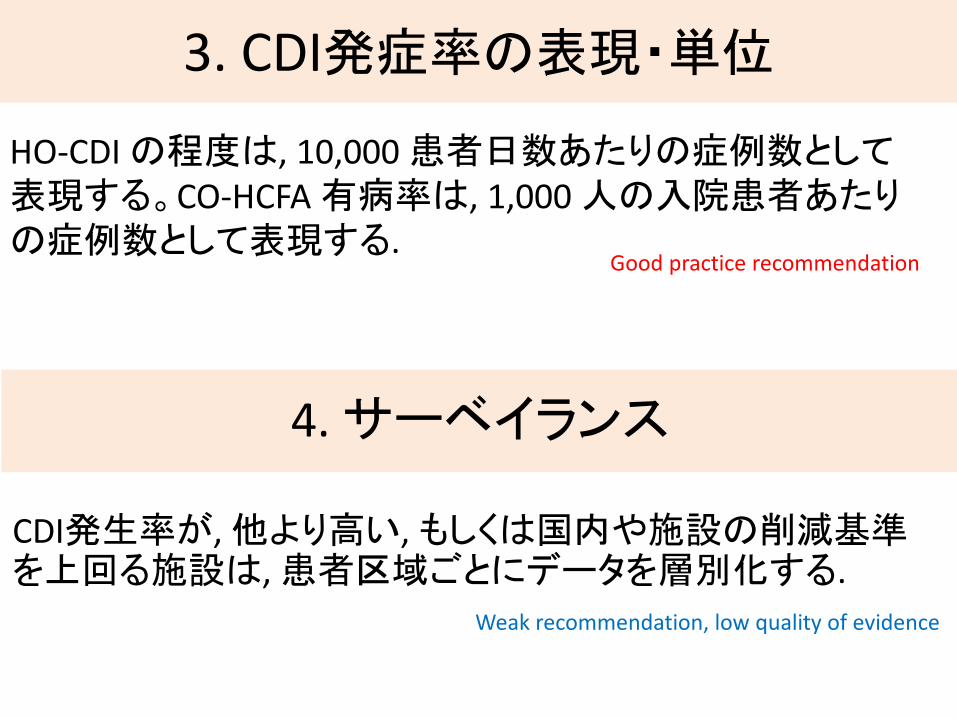
3. CDI発症率の表現・単位
HO-CDI の程度は, 10,000 患者日数あたりの症例数として表現する。CO-HCFA 有病率は, 1,000 人の入院患者あたりの症例数として表現する.
Good practice recommendation
4. サーベイランス
CDI発生率が, 他より高い, もしくは国内や施設の削減基準を上回る施設は, 患者区域ごとにデータを層別化する.
Weak recommendation, low quality of evidence

Epidemiology
1. How are CDI cases best defined?
2. What is the minimal surveillance recommendation for institutions
3. What is the best way to express CDI incidence and rates?
4. How should CDI surveillance be approached in settings of high endemic rates or outbreaks?
5. What is the recommended CDI surveillance strategy for pediatric institutions?
(for children)
5. 小児の場合
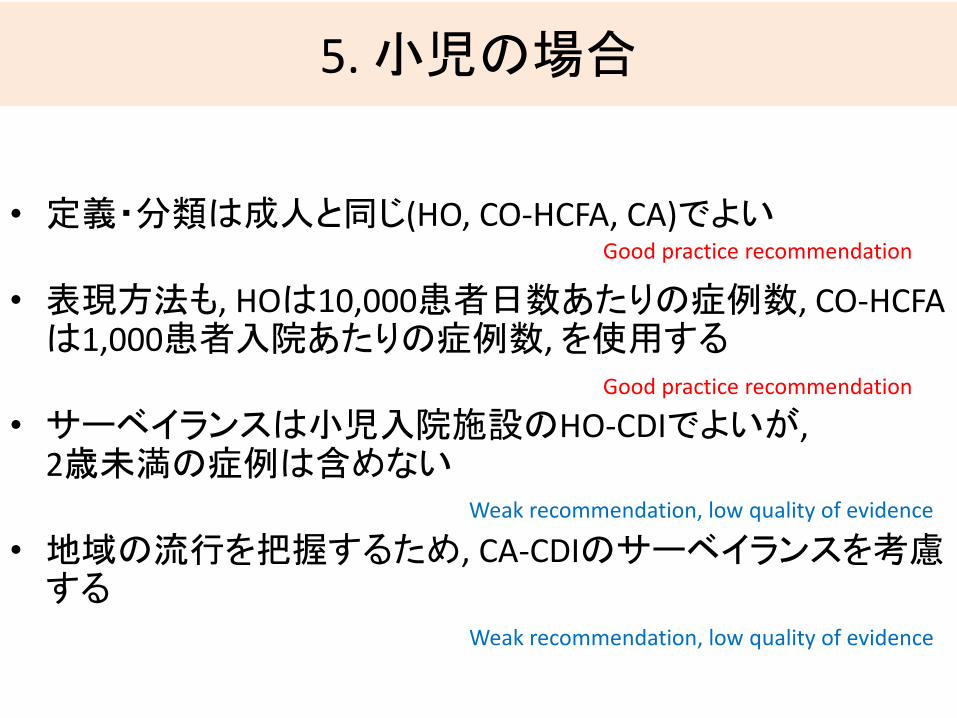
• 定義・分類は成人と同じ(HO, CO-HCFA, CA)でよい
• 表現方法も, HOは10,000患者日数あたりの症例数, CO-HCFAは1,000患者入院あたりの症例数, を使用する
• サーベイランスは小児入院施設のHO-CDIでよいが, 2歳未満の症例は含めない
• 地域の流行を把握するため, CA-CDIのサーベイランスを考慮する
Good practice recommendation
Good practice recommendation
Weak recommendation, low quality of evidence
Weak recommendation, low quality of evidence

CONTENTS
➢INTRODUCTION
➢METHODOLOGY
➢GUIDELINE RECOMMENDATION FOR CDI
– Epidemiology
– Diagnosis
➢INFECTION PREVENTION AND CONTROL
– Isolation measure for patients with CDI
– Treatment

Diagnosis
6. What is the preferred population for C. difficile testing, and should efforts be made to achieve this target?
7. What is the best-performing method (ie, in use positive and negative predictive value) for detecting patients at increased risk for clinically significant C. difficile infection in commonly submitted stool specimens?
8. What is the most sensitive method of diagnosis of CDI in stool specimens from patients likely to have CDI based on clinical symptoms?
9. What is the role of repeat testing, if any? Are there asymptomatic patients in whom repeat testing should be allowed, including test of cure?
10. Does detection of fecal lactoferrin or another biologic marker improve the diagnosis of CDI over and above the detection of toxigenic C. difficile Can such a subset predict a more ill cohort?
11. When should a neonate or infant be tested for C. difficile?
12. When should a toddler or older child be tested for C. difficile?
(for children)

6. CDI検査の対象
• 形をなさない便を
• 24 時間以内に3 回以上
• 新規に発症した患者で,
• 他に原因のない
症例は, CDI 検査をしたほうがよいWeak recommendation, low quality of evidence
Diagnosis6. What is the preferred population for C. difficile testing, and should efforts be made to achieve this target?
7. What is the best-performing method (ie, in use positive and negative predictive value) for detecting patients at increased risk for clinically significant C. difficile infection in commonly submitted stool specimens?
8. What is the most sensitive method of diagnosis of CDI in stool specimens from patients likely to have CDI based on clinical symptoms?
9. What is the role of repeat testing, if any? Are there asymptomatic patients in whom repeat testing should be allowed, including test of cure?
10. Does detection of fecal lactoferrin or another biologic marker improve the diagnosis of CDI over and above the detection of toxigenic C. difficile Can such a subset predict a more ill cohort?
11. When should a neonate or infant be tested for C. difficile?12. When should a toddler or older child be tested for C. difficile?
(for children)
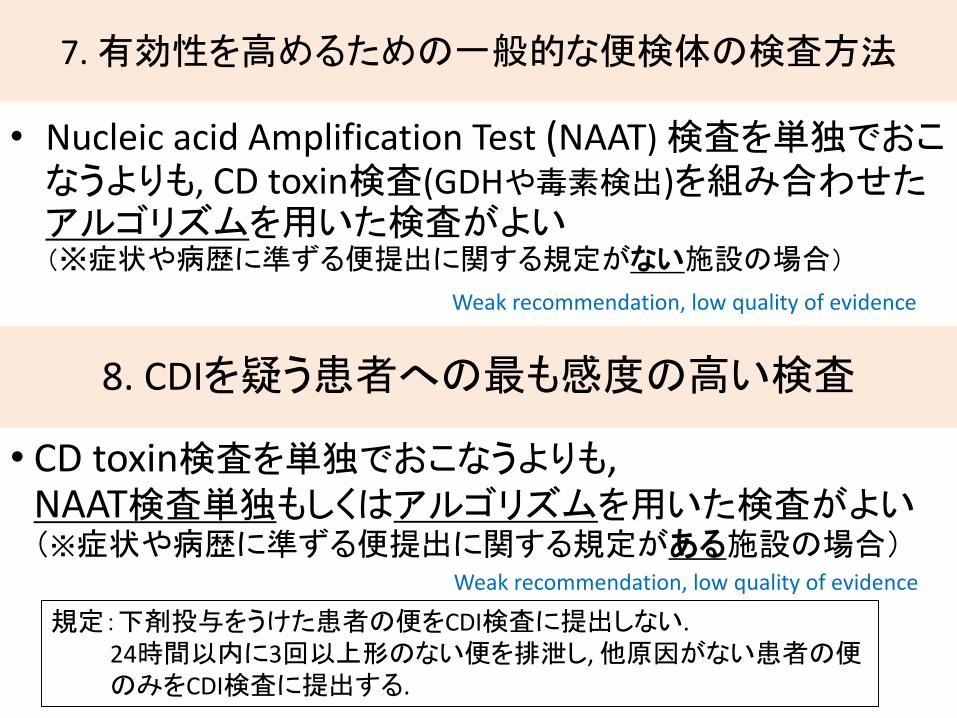
7. 有効性を高めるための一般的な便検体の検査方法
• Nucleic acid Amplification Test (NAAT) 検査を単独でおこなうよりも, CD toxin検査(GDHや毒素検出)を組み合わせたアルゴリズムを用いた検査がよい(※症状や病歴に準ずる便提出に関する規定がない施設の場合)
Weak recommendation, low quality of evidence
8. CDIを疑う患者への最も感度の高い検査
• CD toxin検査を単独でおこなうよりも, NAAT検査単独もしくはアルゴリズムを用いた検査がよい(※症状や病歴に準ずる便提出に関する規定がある施設の場合)
Weak recommendation, low quality of evidence
規定:下剤投与をうけた患者の便をCDI検査に提出しない.24時間以内に3回以上形のない便を排泄し, 他原因がない患者の便のみをCDI検査に提出する.

アルゴリズム
日本臨床微生物学会

“Impact of Clinical Symptoms on Interpretation of Diagnostic Assays for Clostridium difficile Infections”
• 〈集合〉150人参加臨床症状として下痢をきたしていたのは96人 (64%)48時間以内に下剤を内服していたのは28人(19%)
• 〈方法〉各便検体についてtoxin EIA, GDH EIA, NAAT, toxigenic culture(TC)をおこない, それぞれの感度・特異度・陽性的中率・陰性的中率を算出した
• CDIの診断の定義を, 「TC陽性 + 症状あり」として解析した.
Erik R. Dubberke,et al. JOURNAL OF CLINICAL MICROBIOLOGY, Aug. 2011; 49, p. 2887–2893
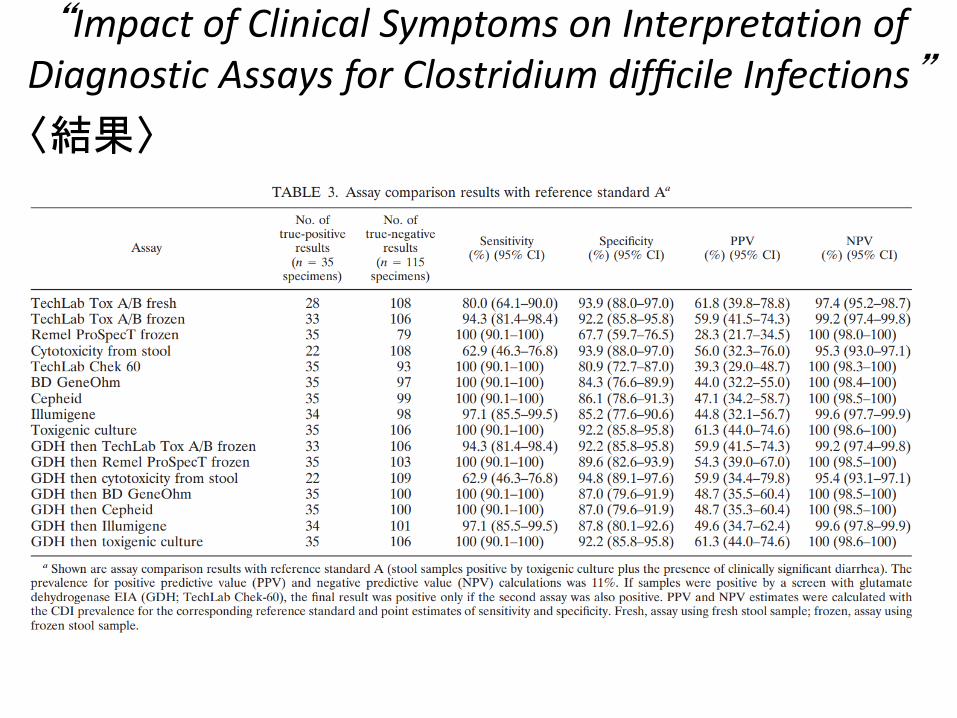
〈結果〉
“Impact of Clinical Symptoms on Interpretation of Diagnostic Assays for Clostridium difficile Infections”
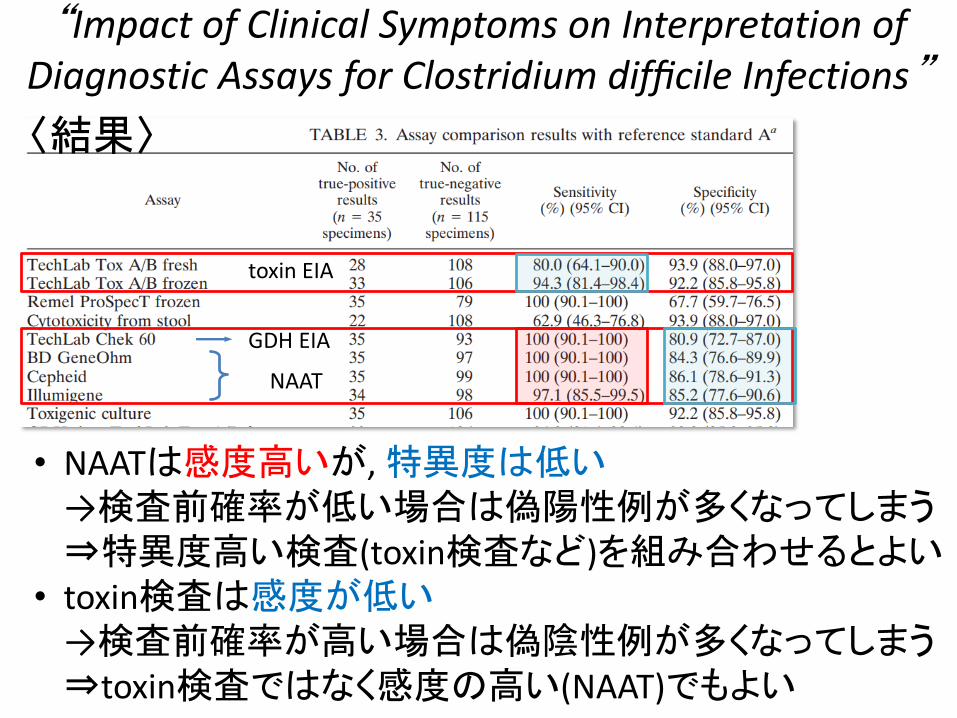
NAAT
GDH EIA
〈結果〉
“Impact of Clinical Symptoms on Interpretation of Diagnostic Assays for Clostridium difficile Infections”
toxin EIA
• NAATは感度高いが, 特異度は低い→検査前確率が低い場合は偽陽性例が多くなってしまう⇒特異度高い検査(toxin検査など)を組み合わせるとよい
• toxin検査は感度が低い→検査前確率が高い場合は偽陰性例が多くなってしまう⇒toxin検査ではなく感度の高い(NAAT)でもよい

“Detection of Toxigenic Clostridium difficile in Stool Samples by Real-Time Polymerase Chain Reaction for
the Diagnosis of C. difficile–Associated Diarrhea”
〈背景・方法〉
• アメリカのシカゴ
• 入院中の, CDIを疑った患者から得られた便のうち,
有形便を除いた下痢/軟便, 370検体
• EIA, NAAT, CCNA, TC の 4つの検査をそれぞれおこなった
• CDIの定義を,
「4つ中 2つ以上の検査で陽性, かつ下痢症状*を有する」
としたときの, EIA, NAAT, CCNA, TCそれぞれの感度 ・特異度 ・陽性的中率 ・陰性的中率を算出した.
(*下痢症状:1日3回以上の軟便/下痢便が, 少なくとも1日以上続く)
Lance R. Peterson, et al. Clin Infect Dis 2007; 45:1152–60

“Detection of Toxigenic Clostridium difficile in Stool Samples by Real-Time Polymerase Chain Reaction for
the Diagnosis of C. difficile–Associated Diarrhea”
〈結果〉
• CDIと診断されたのは30例
• Real-time PCR (NAAT)は EIAと比べて感度が高く, 特異度は変わらなかった. (NAAT 93.3% vs EIA 73,3%; P< 0.05)
Lance R. Peterson, et al. Clin Infect Dis 2007; 45:1152–60
NAATは EIA に替わる検査となりうるが,
PPVはやや低く,事前検査確率の低い例には物足りない

Diagnosis6. What is the preferred population for C. difficile testing, and should efforts be
made to achieve this target?
7. What is the best-performing method (ie, in use positive and negative predictive value) for detecting patients at increased risk for clinically significant C. difficile infection in commonly submitted stool specimens?
8. What is the most sensitive method of diagnosis of CDI in stool specimens from patients likely to have CDI based on clinical symptoms?
9. What is the role of repeat testing, if any? Are there asymptomatic patients in whom repeat testing should be allowed, including test of cure?
10. Does detection of fecal lactoferrin or another biologic marker improve the diagnosis of CDI over and above the detection of toxigenic C. difficile Can such a subset predict a more ill cohort?
11. When should a neonate or infant be tested for C. difficile?
12. When should a toddler or older child be tested for C. difficile?
(for children)
9. 繰り返しの検査の必要性
• 下痢症状の変化など明らかな臨床的根拠に欠ける場合, 同一の症状におこなう7日以内の再検査は推奨しない
• 7日以内の再検査(EIA, NAATs)で新たに見つかるのは2%
• むやみな再検査は偽陽性例を増やす危険性
• また、治療後に再検しても60%以上が陽性のままであるため、治療効果判定としての再検の意義もない
Strong recommendation, moderate quality of evidence

“Nonutility of repeat laboratory testing for detection of Clostridium difficile by use of PCR or enzyme
immunoassay.”
• EIA検査をした人は683人,PCRをしたのは443人
• 初回検査陰性と診断されたのち、7日以内に陽転化した例は、EIA法で1.9%, PCR法で1.7%しかいなかった.
J Clin Microbiol. 2008 Nov;46(11):3795-7Aichinger E. et al,

“Repeat Stool Testing to Diagnose Clostridium difficile Infection Using Enzyme Immunoassay
Does Not Increase Diagnostic Yield”
• 〈集団〉オハイオ州Cleveland Clinicに入院中の18歳以上の患者17,971人
• 〈CDIの定義〉下痢症状+EIA陽性かつ, 他に原因がない
• 〈検査方法〉EIA:CD toxinを検出するEIA(感度90%・特異度100%)
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2011;9:665– 669ABHISHEK DESHPANDE, et al.

EIA検査を繰り返した場合の陰性→陽性例
• 1回目陰性だった患者5,277人のうち, 2回目で陽性になったのは118人(2.2%)
• 1,2回目が陰性だった患者2,076人のうち, 3回目で陽性になったのは54人(2.6%)
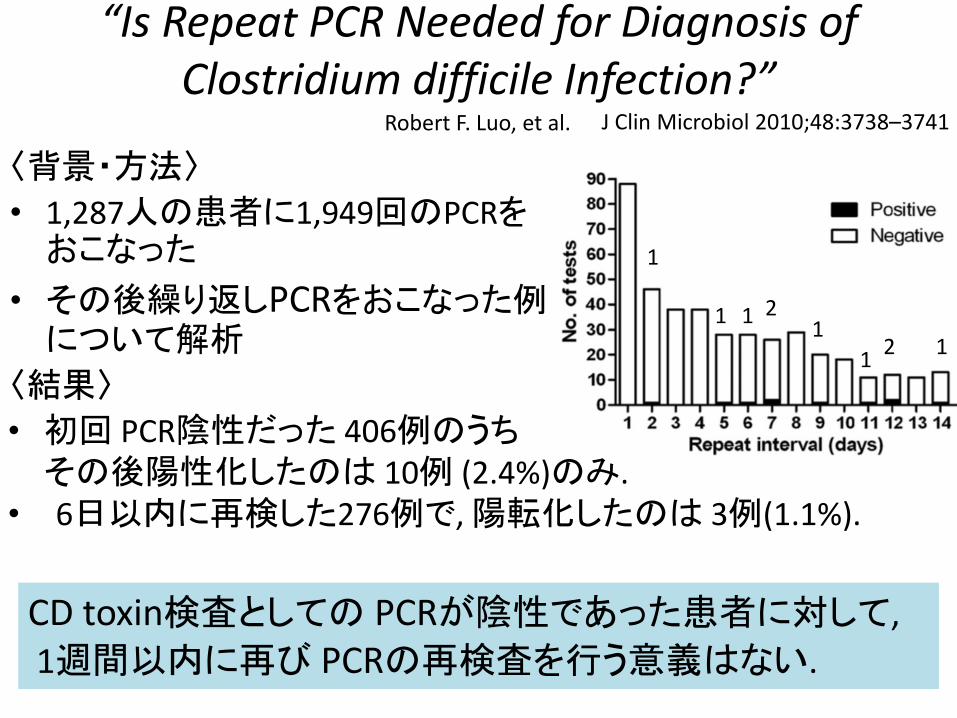
“Is Repeat PCR Needed for Diagnosis of Clostridium difficile Infection?”
〈背景・方法〉
• 1,287人の患者に1,949回のPCRをおこなった
• その後繰り返しPCRをおこなった例について解析
〈結果〉
J Clin Microbiol 2010;48:3738–3741Robert F. Luo, et al.
• 初回 PCR陰性だった 406例のうちその後陽性化したのは 10例 (2.4%)のみ.
• 6日以内に再検した276例で,陽転化したのは 3例(1.1%).
111
1
2
112
CD toxin検査としての PCRが陰性であった患者に対して,
1週間以内に再び PCRの再検査を行う意義はない.

Diagnosis
6. What is the preferred population for C. difficile testing, and should efforts be made to achieve this target?
7. What is the best-performing method (ie, in use positive and negative predictive value) for detecting patients at increased risk for clinically significant C. difficile infection in commonly submitted stool specimens?
8. What is the most sensitive method of diagnosis of CDI in stool specimens from patients likely to have CDI based on clinical symptoms?
9. What is the role of repeat testing, if any? Are there asymptomatic patients in whom repeat testing should be allowed, including test of cure?
10.Does detection of fecal lactoferrin or another biologic marker improve the diagnosis of CDI over and above the detection of toxigenic C. difficile Can such a subset predict a more ill cohort?
11. When should a neonate or infant be tested for C. difficile?12. When should a toddler or older child be tested for C. difficile?
(for children)

10. バイオマーカー検査は有効か
• 診断を補助する目的として, 便中ラクトフェリンや
その他のバイオマーカーの使用を推奨するデータは不十分である.
No recommendation

Diagnosis
6. What is the preferred population for C. difficile testing, and should efforts be made to achieve this target?
7. What is the best-performing method (ie, in use positive and negative predictive value) for detecting patients at increased risk for clinically significant C. difficile infection in commonly submitted stool specimens?
8. What is the most sensitive method of diagnosis of CDI in stool specimens from patients likely to have CDI based on clinical symptoms?
9. What is the role of repeat testing, if any? Are there asymptomatic patients in whom repeat testing should be allowed, including test of cure?
10. Does detection of fecal lactoferrin or another biologic marker improve the diagnosis of CDI over and above the detection of toxigenic C. difficile Can such a subset predict a more ill cohort?
11.When should a neonate or infant be tested for C. difficile?
12.When should a toddler or older child be tested for C. difficile?
(for children)
11-12. 小児に対するC. difficile検査
• 乳児毒素産生性C.difficileの無症候性の有病率が高いため, 下痢症状の12 ヶ月以下の新生児または乳児にCDIの検査は日常的におこなうべきでない
• 幼児他の感染性または非感染性の原因が除外されていない限り, 1 ~2 歳の下痢の子どもに日常的にC. difficile検査をおこなうべきではない.
2歳以上の小児では, 長引く下痢やその悪化, そしてリスク因子(例:基礎に炎症性腸疾患や免疫不全状態など), または関連する曝露(例:医療との接触または最近の抗菌薬)をもつ患者には C. difficile 検査は勧められる
Strong recommendation, moderate quality of evidence
Weak recommendation, modarate quality of evidence
Weak recommendation, low quality of evidence

CONTENTS
➢INTRODUCTION
➢METHODOLOGY
➢GUIDELINE RECOMMENDATION FOR CDI
– Epidemiology
– Diagnosis
➢INFECTION PREVENTION AND CONTROL
– Isolation measure for patients with CDI
– Treatment

Isolation measures for patients with CDI (1)
13.Should private rooms and/or dedicated toilet facilities be used for isolated patients with CDI?
14. Should gloves and gowns be worn while caring for isolated CDI patients?
15. When should isolation be implemented?
16. How long should isolation be continued?
17. What is the recommended hand hygiene method (assuming glove use) when caring for patients in isolation for CDI?
18. Should patient bathing interventions be implemented to prevent CDI?
19. Should noncritical devices or equipment be dedicated to or specially cleaned after being used on the isolated patient with CDI?

13. 入院ベッド・トイレ
1. 他の患者への感染を減らすため専用トイレを備えた個室に CDI 患者を収容する.個室の数に限りがある場合, 個室には便失禁患者を優先する.
2. 患者同士をまとめることが必要な場合, 同じ病原体に感染,または保菌している患者をまとめることが推奨される.-すなわち, MRSA または VRE などの他の多剤耐性病原体と CDI 患者を同部屋としない.
Strong recommendation, moderate quality of evidence
Strong recommendation, moderate quality of evidence
Isolation measures for patients with CDI (1)
13. Should private rooms and/or dedicated toilet facilities be used for isolated patients with CDI?
14.Should gloves and gowns be worn while caring for isolated CDI patients?
15. When should isolation be implemented?
16. How long should isolation be continued?
17. What is the recommended hand hygiene method (assuming glove use) when caring for patients in isolation for CDI?
18. Should patient bathing interventions be implemented to prevent CDI?
19. Should noncritical devices or equipment be dedicated to or specially cleaned after being used on the isolated patient with CDI?
14. 手袋・ガウンの着用
• 医療従事者は, CDI 患者の部屋への入室時と CDI 患者のケアのときは, 手袋をつけるべきである.
• 医療従事者は, CDI 患者の部屋への入室時と CDI 患者のケアのときは,ガウンを使用する必要がある.
Strong recommendation, moderate quality of evidence
Strong recommendation, high quality of evidence

Isolation measures for patients with CDI (1)
13. Should private rooms and/or dedicated toilet facilities be used for isolated patients with CDI?
14. Should gloves and gowns be worn while caring for isolated CDI patients?
15.When should isolation be implemented?
16.How long should isolation be continued?
17. What is the recommended hand hygiene method (assuming glove use) when caring for patients in isolation for CDI?
18. Should patient bathing interventions be implemented to prevent CDI?
19. Should noncritical devices or equipment be dedicated to or specially cleaned after being used on the isolated patient with CDI?

15-16. 隔離の期間
• CDIが疑われ, すぐに検査結果を得ることができない場合, C. difficile 検査の結果が出るまで, 先行的に接触予防策を行う
• 下痢が改善してからも少なくとも48 時間は, 接触予防策を継続する.
• CDI に対する標準的な感染対策を実施しているにもかかわらず, CDI 発生率が高いままであれば, 退院まで接触予防策を延長する.
weak recommendation, low quality of evidence
Strong recommendation, moderate quality of evidence
weak recommendation, low quality of evidence

Isolation measures for patients with CDI (1)
13. Should private rooms and/or dedicated toilet facilities be used for isolated patients with CDI?
14. Should gloves and gowns be worn while caring for isolated CDI patients?
15. When should isolation be implemented?
16. How long should isolation be continued?
17.What is the recommended hand hygiene method (assuming glove use) when caring for patients in isolation for CDI?
18. Should patient bathing interventions be implemented to prevent CDI?
19. Should noncritical devices or equipment be dedicated to or specially cleaned after being used on the isolated patient with CDI?
17. 手指衛生
• 日常的には, CDI 患者との接触の前後, および手袋を脱いだ後に, 流水と石けん, あるいは擦式アルコール製剤で手指衛生を実施する.
• CDI アウトブレイクや流行状況下では, 流水と石けんが芽胞を除去する効果が高いため, CDI患者のケアの前後ではアルコールではなく流水と石けんで手指衛生をおこなう
• 便あるいは便汚染の可能性が高い場所(例:会陰領域)に直接接触する場合は, 流水と石けんでの手洗いが好ましい.
weak recommendation, low quality of evidence
Strong recommendation, moderate quality of evidence
Good practice recommendation
• 理論的には芽胞に対してアルコールは無効とされている
• アルコール消毒の効果を試した実験で, MRSAやVRE感染症は減ったが, CDI感染率は変化しなかった との結果.=アルコール消毒はCDI感染を拡大はさせない.
• 一方, 流水手洗いによりCDI発生率が減った
“Reduction in nosocomial transmission of drug-resistant bacteria after introduction of an alcohol-based handrub.”
• 6年の間, 入院・外来患者への診療に 62.5% エチルアルコールによる手指衛生で対応した• C.difficileの発生率は前3年間と後3年間で変わらなかった
“Evaluation of the national Cleanyourhands campaign to reduce Staphylococcus aureus bacteraemia and Clostridium difficile infection in hospitals in England and Wales by improved hand hygiene: four year, prospective, ecological, interrupted time series study”
17. 手指衛生
Isolation measures for patients with CDI (1)13. Should private rooms and/or dedicated toilet facilities be used for isolated patients
with CDI?
14. Should gloves and gowns be worn while caring for isolated CDI patients?
15. When should isolation be implemented?
16. How long should isolation be continued?
17. What is the recommended hand hygiene method (assuming glove use) when caring for patients in isolation for CDI?
18.Should patient bathing interventions be implemented to prevent CDI?
19.Should noncritical devices or equipment be dedicated to or specially cleaned after being used on the isolated patient with CDI?

18.入浴
• 皮膚の芽胞を減らすために, 患者には手を洗い, シャワーを浴びるよう奨励する.
Good practice recommendation
19.患者用備品・診療具の管理
•患者備品はディスポーザブル製品を可能な限り使用し, 再利用可能備品は殺芽胞消毒剤での消毒をおこなう.
strong recommendation, moderate quality of evidence

20.What is the role of manual, terminal disinfection using a C. difficile sporicidal agent for patients in isolation for CDI?
21.Should cleaning adequacy be evaluated?
22.What is the role of automated terminal disinfection using a method that is sporicidal against C. difficile?
23.What is the role of daily sporicidal disinfection?24. Should asymptomatic carriers of C. difficile be identified and isolated if positive?
25. What is the role of antibiotic stewardship in controlling CDI rates?
26. What is the role of proton pump inhibitor restriction in controlling CDI rates?
27. What is the role of probiotics in primary prevention of CDI?
Isolation measures for patients with CDI (2)
20-23. 室内・周囲環境の管理, 清掃
• 殺芽胞剤を使用した最終病室清掃・毎日の清掃は, 高度流行地域, 院内アウトブレイク期間, あるいは同室で CDI 症例が繰り返し発生している場合には考慮される.
• 環境のクリーニングの質を保証するために清掃効果の評価をおこなう
• 現時点では, CDI 予防ための非接触式消毒システムによる機械的な自動の殺芽胞消毒を推奨するデータは限られている.
Weak recommendation, low quality of evidence
Good practice recommendation
No recommendation

20. What is the role of manual, terminal disinfection using a C. difficile sporicidal agent for patients in isolation for CDI?
21. Should cleaning adequacy be evaluated?
22. What is the role of automated terminal disinfection using a method that is sporicidal against C. difficile?
23. What is the role of daily sporicidal disinfection?
24.Should asymptomatic carriers of C. difficile be identified and isolated if positive?
25. What is the role of antibiotic stewardship in controlling CDI rates?
26. What is the role of proton pump inhibitor restriction in controlling CDI rates?
27. What is the role of probiotics in primary prevention of CDI?
Isolation measures for patients with CDI (2)
24. 無症候性保菌者への対応
• 無症候性保菌者のスクリーニングし, 接触予防策をとることを推奨するデータは不十分である.
No recommendation
20. What is the role of manual, terminal disinfection using a C. difficile sporicidal agent for patients in isolation for CDI?
21. Should cleaning adequacy be evaluated?
22. What is the role of automated terminal disinfection using a method that is sporicidal against C. difficile?
23. What is the role of daily sporicidal disinfection?
24. Should asymptomatic carriers of C. difficile be identified and isolated if positive?
25.What is the role of antibiotic stewardship in controlling CDI rates?
26. What is the role of proton pump inhibitor restriction in controlling CDI rates?
27. What is the role of probiotics in primary prevention of CDI?
Isolation measures for patients with CDI (2)

25. CDI予防のための抗菌薬の適正使用
• CDI リスクを下げるために, 高リスクの抗菌薬療法の頻度と期間, および処方される抗菌薬の数を最小限に抑える.
• 抗菌薬スチュワードシップ・プログラムを実施する.
• 標的とされる抗菌薬は, 地域の疫学と C. difficile 菌株に基づいているべきである. ニューキノロン, クリンダマイシンとセファロスポリンの制限が考慮される(手術時抗菌薬予防を除く).
Strong recommendation, moderate quality of evidence
Good practice recommendation
Strong recommendation, moderate quality of evidence

20. What is the role of manual, terminal disinfection using a C. difficile sporicidal agent for patients in isolation for CDI?
21. Should cleaning adequacy be evaluated?
22. What is the role of automated terminal disinfection using a method that is sporicidal against C. difficile?
23. What is the role of daily sporicidal disinfection?
24. Should asymptomatic carriers of C. difficile be identified and isolated if positive?
25. What is the role of antibiotic stewardship in controlling CDI rates?
26.What is the role of proton pump inhibitor restriction in controlling CDI rates?
27.What is the role of probiotics in primary prevention of CDI?
Isolation measures for patients with CDI (2)

26. PPIとCDI
• プロトンポンプ阻害薬(PPI)の使用と CDI との間には疫学的関連があり, 不要な PPI は中止すべきであるが, CDI 予防のための対策として PPI を中止するというエビデンスは不十分である
27. プロバイオティクス
•現時点では, 臨床治験外のCDIの一次予防のためのプロバイオティクスの投与を推奨するにはデータが不十分である.
No recommendation
No recommendation
CONTENTS
➢INTRODUCTION
➢METHODOLOGY
➢GUIDELINE RECOMMENDATION FOR CDI
– Epidemiology
– Diagnosis
➢INFECTION PREVENTION AND CONTROL
– Isolation measure for patients with CDI
– Treatment

Treatment
28.What are important ancillary treatment strategies for CDI?
29. What are the best treatments of an initial CDI episode to ensure resolution of symptoms and sustained resolution 1 month after treatment?
30. What are the best treatments of fulminant CDI?
31. What are the best treatments for recurrent CDI?
32. What is the best treatment of an initial episode or first recurrence of non-severe CDI in children?
33. What is the best treatment of an initial episode of severe CDI in children?
34. What are the best treatments for a second or greater episode of recurrent CDI in children?
35. Is there a role for fecal microbiota transplantation in children with recurrent CDI?
(for children)
28. 補助的治療戦略
• CDI 再発のリスクに影響する可能性があるため, できるだけ早く原因と思われる抗菌薬を中止する
• CDI のための抗菌薬治療は, 検査所見の結果判明に大幅な遅延が予想される状況, または, 劇症型CDI の場合には, 経験的に開始されるべきである(第 30 章に記載)
Strong recommendation, moderate quality of evidence
Weak recommendation, low quality of evidence

Treatment
28. What are important ancillary treatment strategies for CDI?
29.What are the best treatments of an initial CDI episode to ensure resolution of symptoms and sustained resolution 1 month after treatment?
30. What are the best treatments of fulminant CDI?
31. What are the best treatments for recurrent CDI?
32. What is the best treatment of an initial episode or first recurrence of non-severe CDI in children?
33. What is the best treatment of an initial episode of severe CDI in children?
34. What are the best treatments for a second or greater episode of recurrent CDI in children?
35. Is there a role for fecal microbiota transplantation in children with recurrent CDI?
(for children)
29. CDIの標準的な初回治療
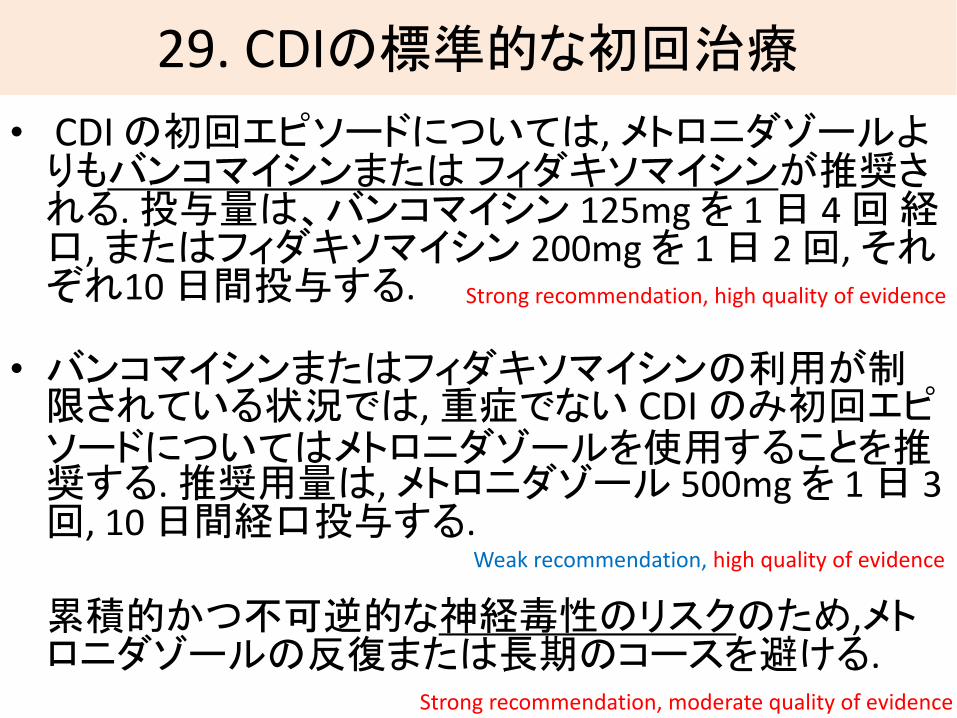
• CDIの初回エピソードについては, メトロニダゾールよりもバンコマイシンまたはフィダキソマイシンが推奨される. 投与量は、バンコマイシン 125mg を 1 日 4 回経口, またはフィダキソマイシン 200mg を 1 日 2 回, それぞれ10 日間投与する.
• バンコマイシンまたはフィダキソマイシンの利用が制限されている状況では, 重症でない CDI のみ初回エピソードについてはメトロニダゾールを使用することを推奨する. 推奨用量は, メトロニダゾール 500mg を 1 日 3 回, 10 日間経口投与する.
累積的かつ不可逆的な神経毒性のリスクのため,メトロニダゾールの反復または長期のコースを避ける.
Strong recommendation, high quality of evidence
Strong recommendation, moderate quality of evidence
Weak recommendation, high quality of evidence

“Vancomycin, metronidazole, or tolevamer for Clostridium difficile infection:
results from two multinational, randomized, controlled trials.”
• (Tolevamer vs) MNZ(278人) vs VCM(259人)
• 治療法:MNZ 375mg x4, VCM 125mg x4 (x 各10日間)
• 治療成功率 (Tolevamer 44.2%), MNZ 72.7%, VCM 81.1%
Clin Infect Dis. 2014 Aug 1;59(3):345-54Johnson S, et al.
P= 0.02

“A Comparison of Vancomycin and Metronidazole for the Treatment of Clostridium difficile
–Associated Diarrhea, Stratified by Disease Severity”
〈背景・方法〉• Saint Francis Hp. に入院中のCDI患者172人のうち, 最後まで治療をおこなった150人で比較.
• 経口バンコマイシン vs経口メトロニダゾールVCM: 125mg x 4 x 10days, MNZ: 250mg x 4 x 10days
〈結果〉
• Mild CDI : 81人, severe CDI : 69人
• Mild CDI → 治癒率 VCM 98% vs MNZ 90% (P= 0.36)Severe CDI →治癒率 VCM 97% vs MNZ 76% (P= 0.02)
• 再発率に差は認めなかった
Fred A. Zar, et al. Clin Infect Dis 2007; 45:302–7
Severe CDI には, VCMがより有効
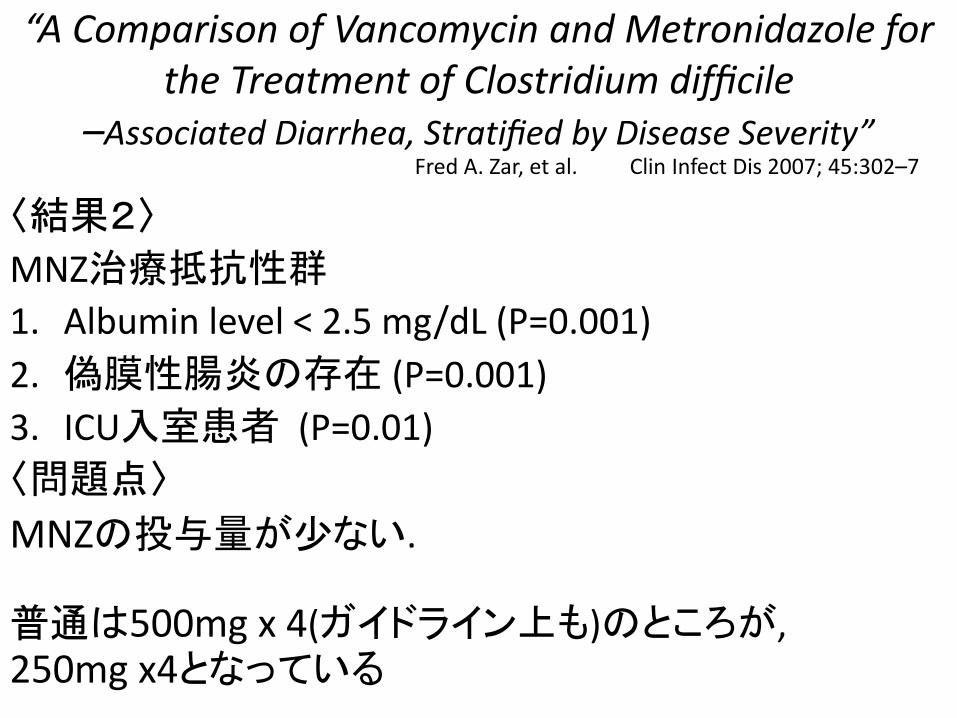
“A Comparison of Vancomycin and Metronidazole for the Treatment of Clostridium difficile
–Associated Diarrhea, Stratified by Disease Severity”
〈結果2〉
MNZ治療抵抗性群
1. Albumin level < 2.5 mg/dL (P=0.001)
2. 偽膜性腸炎の存在 (P=0.001)
3. ICU入室患者 (P=0.01)
〈問題点〉
MNZの投与量が少ない.
普通は500mg x 4(ガイドライン上も)のところが, 250mg x4となっている
Fred A. Zar, et al. Clin Infect Dis 2007; 45:302–7
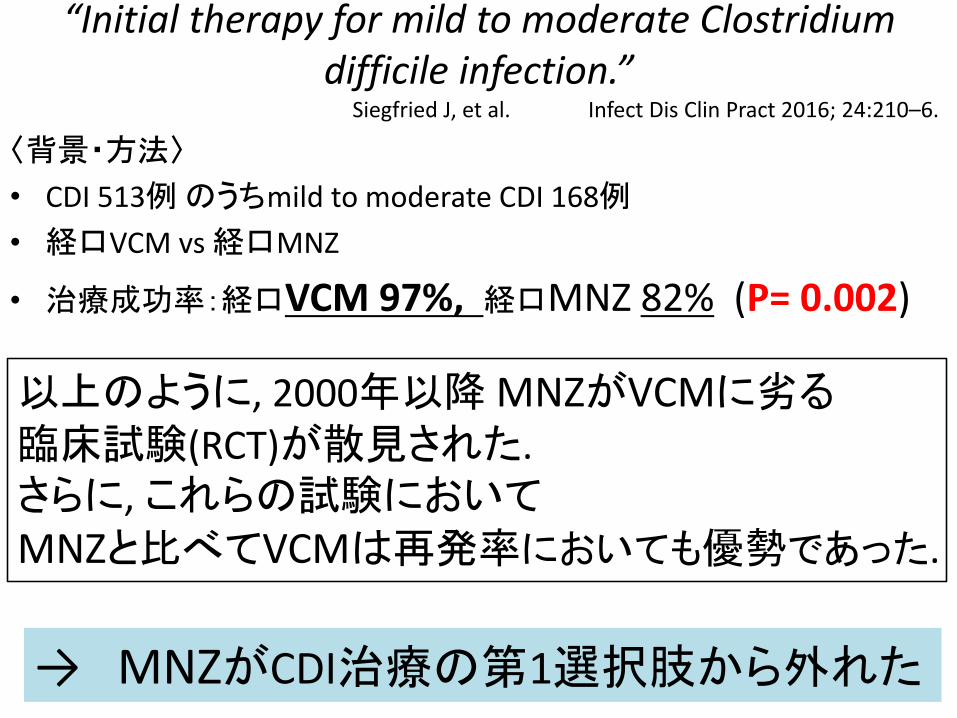
“Initial therapy for mild to moderate Clostridium difficile infection.”
〈背景・方法〉
• CDI 513例のうちmild to moderate CDI 168例
• 経口VCM vs 経口MNZ
• 治療成功率:経口VCM 97%, 経口MNZ 82% (P= 0.002)
Siegfried J, et al. Infect Dis Clin Pract 2016; 24:210–6.
以上のように, 2000年以降MNZがVCMに劣る臨床試験(RCT)が散見された.さらに,これらの試験においてMNZと比べてVCMは再発率においても優勢であった.
→ MNZがCDI治療の第1選択肢から外れた

治療の延期
10日たっても症状が減少しない場合には, 投与期間を10日から14日まで延ばすことも考慮される.
本文より
メトロニダゾールと脳症
経口メトロニダゾールの反復・延長投与は神経毒性が出現したとのレポートがあり, できるだけ控える.

fidaxomicin
治療成績はVCMと同等再発率に関してはむしろ好成績
• RNA合成阻害• 消化管からはほとんど吸収されず• 便中への排出率は92%と高い• 2018/5/23 ダフクリアを承認• アステラス製薬が販売

“Fidaxomicin versus Vancomycin for Clostridium difficile Infection”
〈背景・方法〉
• アメリカとカナダの病院• CDI (fulminant CDIを除く)629人• うち596人を解析(fidaxomicin 287人, VCM 309人)• 投与方法:fidaxomicin200mg x2,
VCM 125mg x4, 各10日間
〈結果〉• 臨床症状改善率 : fidaxomicin 88.2%, VCM 85.8%
• 完治率 : fidaxomicin 74.6%, VCM 64.1% (P= 0.006)• 再発率 : fidaxomicin 15.4%, VCM 25.3% (P= 0.005)
N Engl J Med 2011; 364:422–31. Louie TJ, et al.
FidaxomicinはVCMに非劣勢であり, 再発率や完治率ではむしろ好成績
fidaxomicin vancomycin
28. What are important ancillary treatment strategies for CDI?
29. What are the best treatments of an initial CDI episode to ensure resolution of symptoms and sustained resolution 1 month after treatment?
30.What are the best treatments of fulminant CDI?
31. What are the best treatments for recurrent CDI?
32. What is the best treatment of an initial episode or first recurrence of non-severe CDI in children?
33. What is the best treatment of an initial episode of severe CDI in children?
34. What are the best treatments for a second or greater episode of recurrent CDI in children?
35. Is there a role for fecal microbiota transplantation in children with recurrent CDI?
(for children)
Treatment
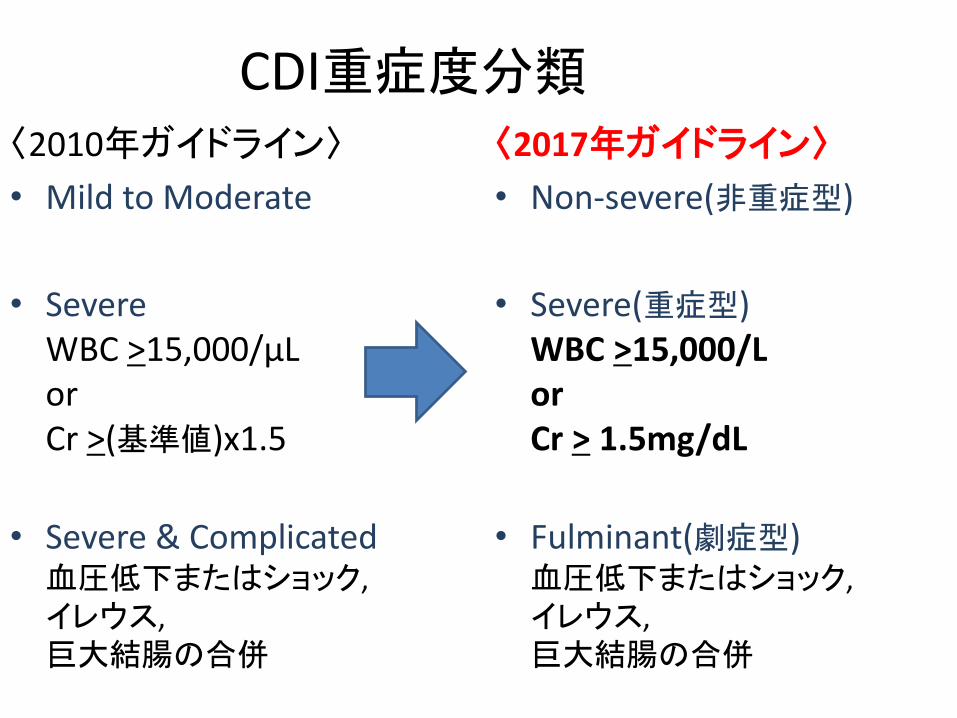
CDI重症度分類〈2010年ガイドライン〉
• Mild to Moderate
• SevereWBC >15,000/μLor Cr >(基準値)x1.5
• Severe & Complicated血圧低下またはショック,イレウス, 巨大結腸の合併
〈2017年ガイドライン〉
• Non-severe(非重症型)
• Severe(重症型)WBC >15,000/Lor Cr > 1.5mg/dL
• Fulminant(劇症型)血圧低下またはショック,イレウス, 巨大結腸の合併
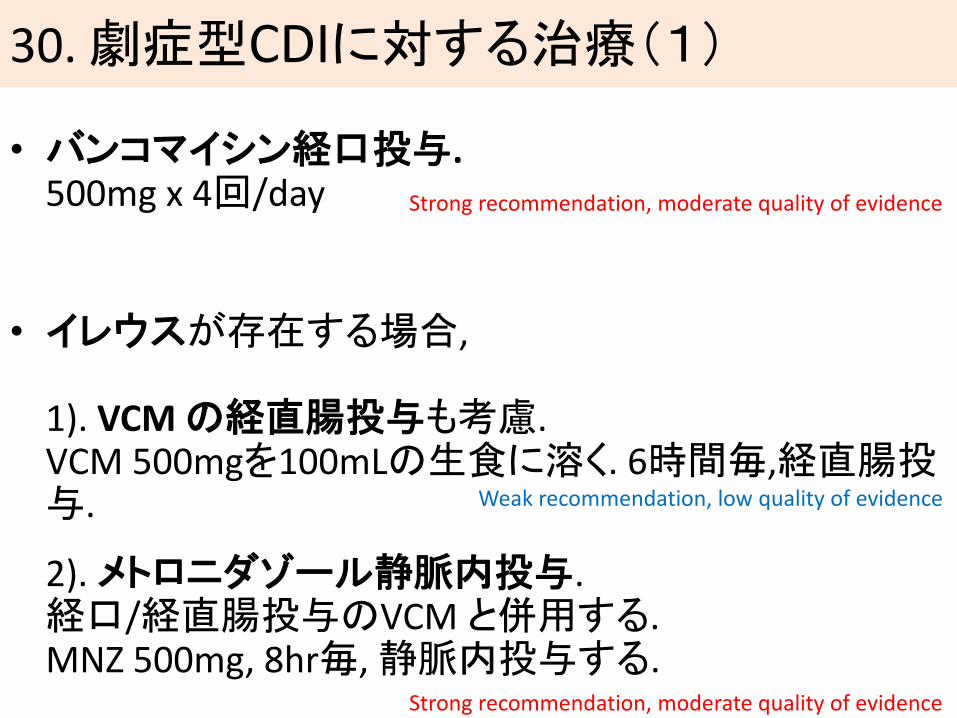
30. 劇症型CDIに対する治療(1)
• バンコマイシン経口投与.500mg x 4回/day
• イレウスが存在する場合,
1). VCM の経直腸投与も考慮.VCM 500mgを100mLの生食に溶く. 6時間毎,経直腸投与.
2). メトロニダゾール静脈内投与.経口/経直腸投与のVCMと併用する.MNZ 500mg, 8hr毎, 静脈内投与する.
Strong recommendation, moderate quality of evidence
Weak recommendation, low quality of evidence
Strong recommendation, moderate quality of evidence

“The Addition of Intravenous Metronidazole to Oral Vancomycin is Associated With Improved Mortality in
Critically Ill Patients With Clostridium difficile Infection”
〈背景・方法〉
• アメリカの単施設, ICU入室しているCDI患者187人のうち,重篤な(設定基準を満たした)88人.
• 経口VCM群(44人)と, 経口VCM+静注MNZ群(44人)の比較
〈結果〉
• 院内死亡率: VCM 36.4%, VCM+ iv-MNZ 15.9% (P= 0.03)
• 治療成功率: VCM 20.5%, VCM+ iv-MNZ 13.6% (P= 0.57)
• 入院日数, ICU入室日数にも違いはみとめなかった.
Kristina E. et al. Clin Infect Dis 2015; 61:934–41
メトロニダゾール静注併用群が, 院内死亡率においては優れた結果となった

“The Addition of Intravenous Metronidazole to Oral Vancomycin is Associated With Improved Mortality in
Critically Ill Patients With Clostridium difficile Infection”〈問題点〉
投薬量(/day)がまちまち
• VCM単独群:79.5% がVCM 125mg x 4 (残りは250mg x 4 か 500mg x 4)18.2% は治療期間に用量が変更された.
• VCM + iv-MNZ併用群:59.0% がVCM 125mg x 4 (残りは250mg x 4 か 500mg x 4)25.0% は治療期間にVCMの用量が変更された.MNZ投与量は, 500mg x 4 (25.0%), 500mg x3 (72.7%), 250mg x4 (2.3%)(平均投与日数12.5日;3-33日)
• 治療期間に関しては両群間に差はなかった.
重症度がガイドラインとずれている
• 7つの基準のうち, 3つ以上を満たすものを “critically ill” と設定した.Alb < 2.5g/dL, HR > 90bpm, MAP <60mmHg, WBC >15,000/μL, age >60, sCr > baselinex1.5, BT > 38℃
Kristina E. et al. Clin Infect Dis 2015; 61:934–41
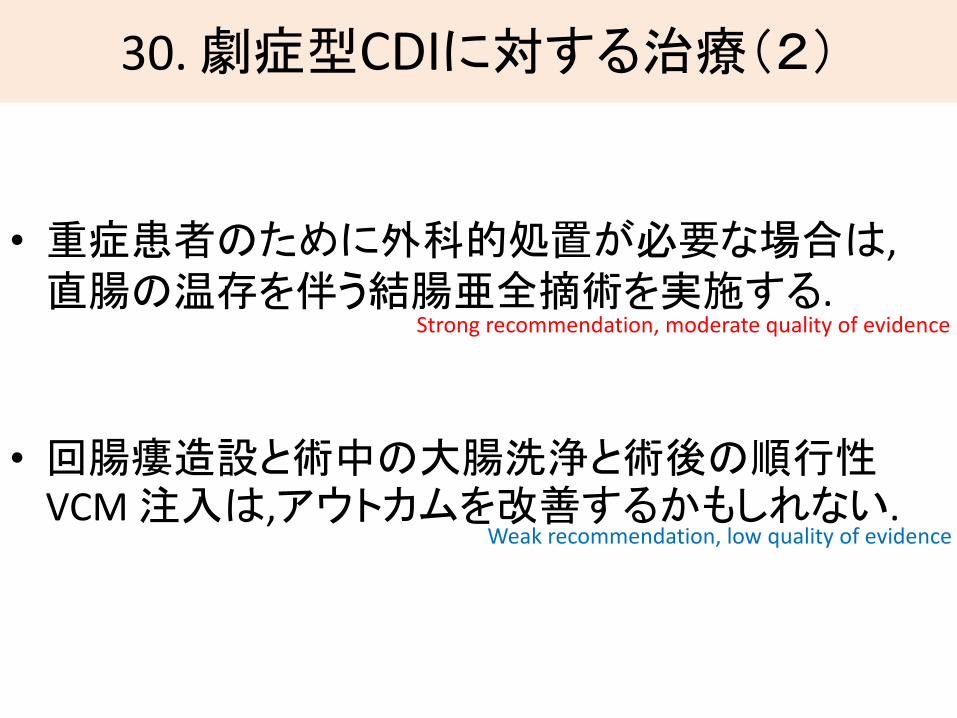
30. 劇症型CDIに対する治療(2)
• 重症患者のために外科的処置が必要な場合は, 直腸の温存を伴う結腸亜全摘術を実施する.
• 回腸瘻造設と術中の大腸洗浄と術後の順行性VCM 注入は,アウトカムを改善するかもしれない.
Strong recommendation, moderate quality of evidence
Weak recommendation, low quality of evidence
過去のICU勉強会, 井澤先生より

“Impact of Emergency Colectomy on Survival of Patients With Fulminant Clostridium difficile Colitis
During an Epidemic Caused by a Hypervirulent Strain”〈背景・方法〉• ICU入室となったCDI患者165例
• 手術施行群と手術非施行群それぞれの死亡率を, 年齢・免疫不全・(昇圧剤の必要な)ショック・WBCのピーク値・乳酸ピーク値それぞれでsub group解析した.
〈結果〉①65歳以上, ②免疫不全でない, ③WBC >20,000μL, ④Lac 2.2-4.9mmol/Lのとき,
手術による利益があると考えられる.
Franc¸ois Lamontagne, et al. Ann Surg 2007; 245:267–72
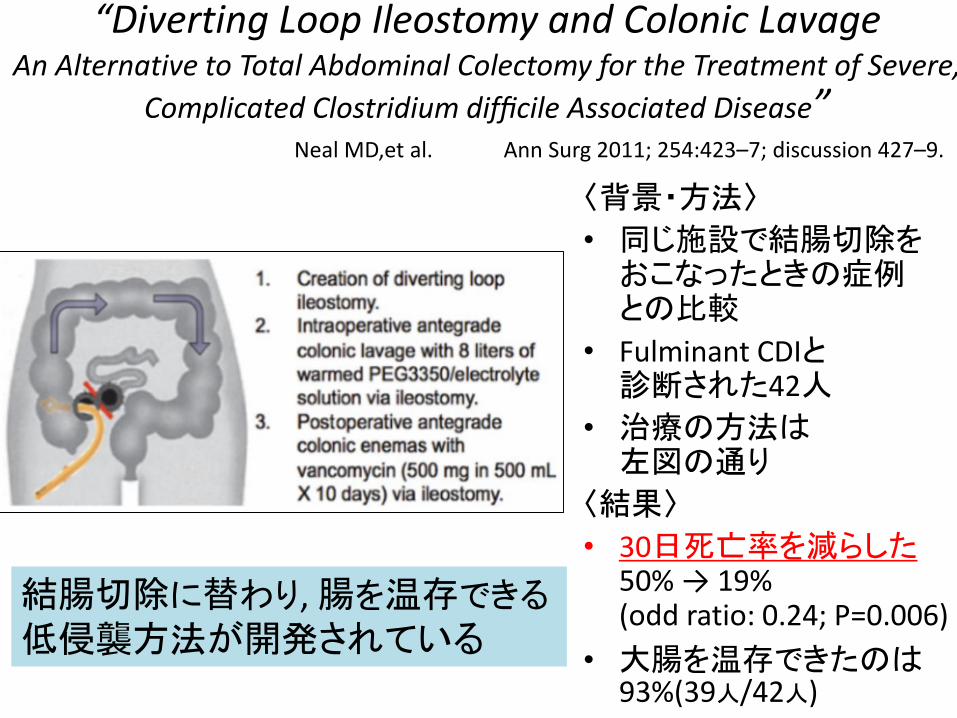
“Diverting Loop Ileostomy and Colonic Lavage An Alternative to Total Abdominal Colectomy for the Treatment of Severe,
Complicated Clostridium difficile Associated Disease”
〈背景・方法〉
• 同じ施設で結腸切除をおこなったときの症例との比較
• Fulminant CDIと診断された42人
• 治療の方法は左図の通り
〈結果〉
• 30日死亡率を減らした50% → 19%(odd ratio: 0.24; P=0.006)
• 大腸を温存できたのは93%(39人/42人)
結腸切除に替わり, 腸を温存できる低侵襲方法が開発されている
Ann Surg 2011; 254:423–7; discussion 427–9. Neal MD,et al.
Treatment
28. What are important ancillary treatment strategies for CDI?
29. What are the best treatments of an initial CDI episode to ensure resolution of symptoms and sustained resolution 1 month after treatment?
30. What are the best treatments of fulminant CDI?
31.What are the best treatments for recurrent CDI?
32. What is the best treatment of an initial episode or first recurrence of non-severe CDI in children?
33. What is the best treatment of an initial episode of severe CDI in children?
34. What are the best treatments for a second or greater episode of recurrent CDI in children?
35. Is there a role for fecal microbiota transplantation in children with recurrent CDI?
(for children)
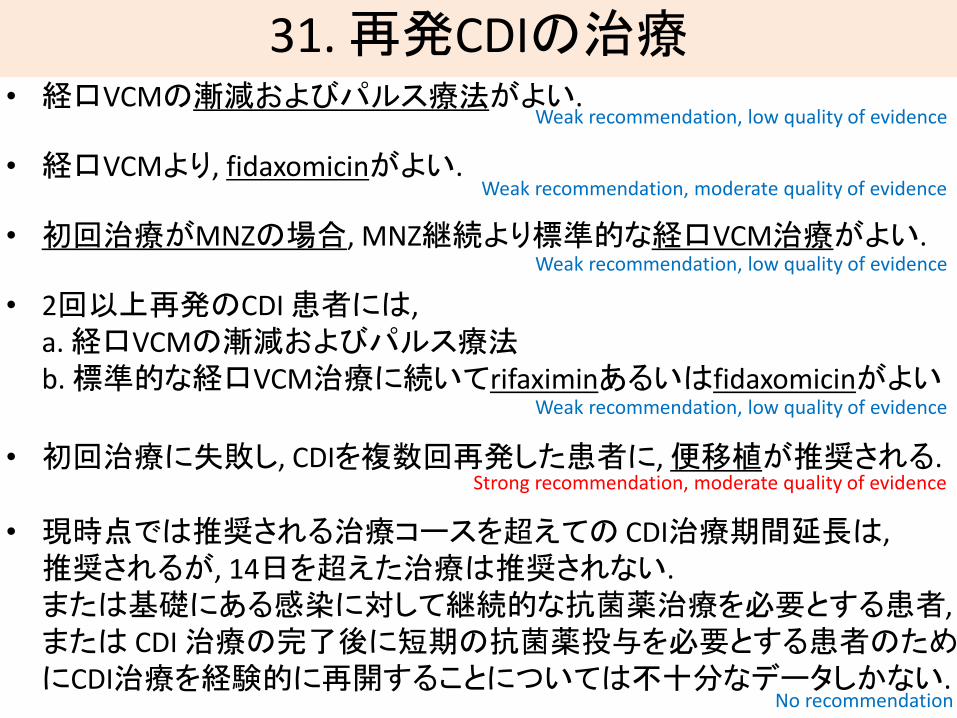
31. 再発CDIの治療• 経口VCMの漸減およびパルス療法がよい.
• 経口VCMより, fidaxomicinがよい.
• 初回治療がMNZの場合, MNZ継続より標準的な経口VCM治療がよい.
• 2回以上再発のCDI 患者には, a. 経口VCMの漸減およびパルス療法b. 標準的な経口VCM治療に続いてrifaximinあるいはfidaxomicinがよい
• 初回治療に失敗し, CDIを複数回再発した患者に, 便移植が推奨される.
• 現時点では推奨される治療コースを超えての CDI治療期間延長は, 推奨されるが, 14日を超えた治療は推奨されない. または基礎にある感染に対して継続的な抗菌薬治療を必要とする患者,または CDI 治療の完了後に短期の抗菌薬投与を必要とする患者のためにCDI治療を経験的に再開することについては不十分なデータしかない.
Weak recommendation, low quality of evidence
Weak recommendation, moderate quality of evidence
Weak recommendation, low quality of evidence
Weak recommendation, low quality of evidence
Strong recommendation, moderate quality of evidence
No recommendation

Treatment
28. What are important ancillary treatment strategies for CDI?
29. What are the best treatments of an initial CDI episode to ensure resolution of symptoms and sustained resolution 1 month after treatment?
30. What are the best treatments of fulminant CDI?
31. What are the best treatments for recurrent CDI?
32.What is the best treatment of an initial episode or first recurrence of non-severe CDI in children?
33.What is the best treatment of an initial episode of severe CDI in children?
34. What are the best treatments for a second or greater episode of recurrent CDI in children?
35. Is there a role for fecal microbiota transplantation in children with recurrent CDI?
(for children)

32-33. 小児のCDI治療(非重症・重症例)
• 初回エピソードまたは非重症CDIの初回再発の小児の治療には, メトロニダゾールかバンコマイシンのいずれかが推奨される.
• 重症CDI 初回エピソードの小児には, 経口バンコ
マイシンがメトロニダゾールよりも推奨される.
Weak recommendation, low quality of evidence
Strong recommendation, moderate quality of evidence

Treatment
28. What are important ancillary treatment strategies for CDI?
29. What are the best treatments of an initial CDI episode to ensure resolution of symptoms and sustained resolution 1 month after treatment?
30. What are the best treatments of fulminant CDI?
31. What are the best treatments for recurrent CDI?
32. What is the best treatment of an initial episode or first recurrence of non-severe CDI in children?
33. What is the best treatment of an initial episode of severe CDI in children?
34.What are the best treatments for a second or greater episode of recurrent CDI in children?
35.Is there a role for fecal microbiota transplantation in children with recurrent CDI?
(for children)
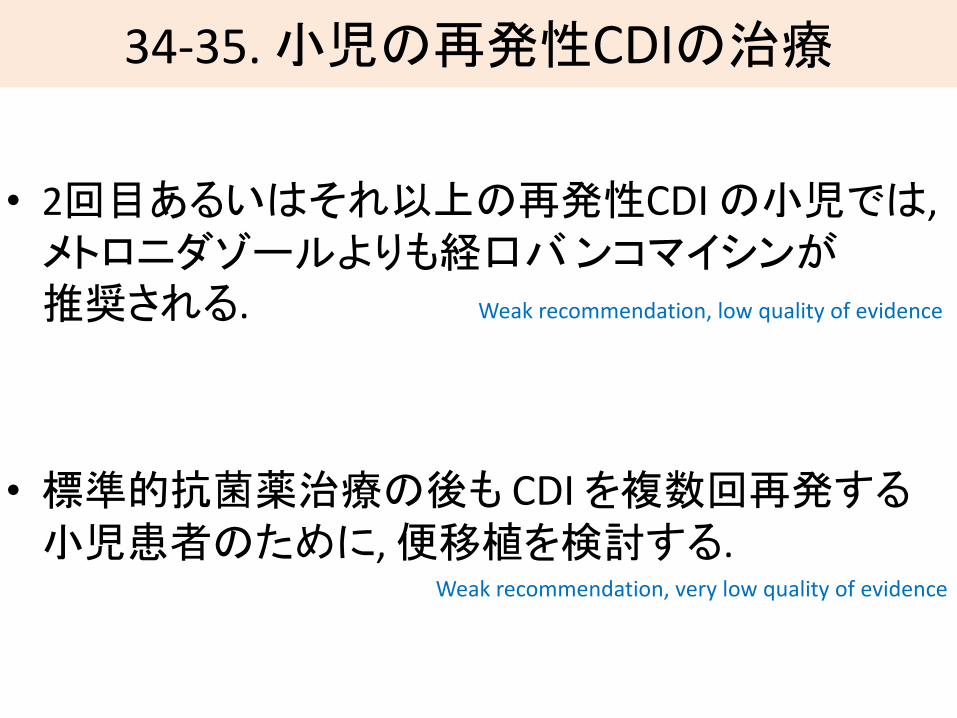
34-35. 小児の再発性CDIの治療
• 2回目あるいはそれ以上の再発性CDIの小児では, メトロニダゾールよりも経口バンコマイシンが推奨される.
• 標準的抗菌薬治療の後も CDIを複数回再発する小児患者のために,便移植を検討する.
Weak recommendation, low quality of evidence
Weak recommendation, very low quality of evidence
私見
• CDIは職場で最もよく見る感染症の一つ
• 検査も治療も進化しており, 今後も発展が期待されている.
• 臨床の現場で検査前確率を意識する重要性.
• MNZは安価であり, non-severe CDI症例にはまだまだ使える余地がある.
• Fidaxomicinの可能性
終





























