Embed Size (px)
Citation preview

Stéphane DAUGER
Nouvelle définition du SDRA
Réanimation et Surveillance Continue Pédiatriques
Hôpital Robert-Debré, Paris
JPP 2015 Institut des Cordeliers

Connaître l’histoire de la définition du SDRA
Comprendre les évolutions récentes
Appliquer la première définition pédiatrique
Cet exposé : on en fait quoi ?
1
2
3
S.Dauger 03/10/2015
HISTORIQUE DEFINITION PEDIATRIQUE MORBI-MORTALITE INTRODUCTION
2 / 26
CONCLUSION

Œdème alvéolaire hypoxémiant sub-aigu non
cardiogénique par augmentation de la
perméabilité capillaire
S.Dauger
DEFINITION PEDIATRIQUE MORBI-MORTALITE INTRODUCTION CONCLUSION HISTORIQUE
03/10/2015 3 / 26

S.Dauger
Ashbaugh Murray Berlin CCAE PALISI
1967 1988 1994 2012 2015
27 ans 18 ans
Description Traitement
Syndrome de Détresse Respiratoire de l’Adulte
Syndrome de Détresse Respiratoire Aigu
50 ans
DEFINITION PEDIATRIQUE MORBI-MORTALITE INTRODUCTION CONCLUSION HISTORIQUE
03/10/2015 4 / 26

ARDS definition task force. JAMA. 2012;307(23):2526-2533
these variables in one of the cohorts.There was no significant difference in thepredictive validity of the weight-adjusted criteria. The consensus panel re-viewed these results and considered thelack of evidence for predictive validity ofthese ancillary variables and their po-tential contribution to face validity andconstruct validity and decided to use thesimpler definition for severe ARDS thatrelied on oxygenation alone.
The Berlin Definition.The final Ber-lin Definition of ARDS is shown inTABLE 3. Twenty-two percent (95% CI,21%-24%) of patients met criteria formild ARDS (which is comparable withthe ALI non-ARDS category of theAECC definition; TABLE 4), 50% (95%CI, 48%-51%) of patients met criteriafor moderate ARDS, and 28% (95% CI,27%-30%) of patients met criteria forsevere ARDS. Mortality increased withstages of ARDS from mild (27%; 95%CI, 24%-30%) to moderate (32%; 95%CI, 29%-34%) to severe (45%; 95% CI,42%-48%). Median (IQR) ventilator-free days declined with stages of ARDSfrom mild (20 [1-25] days) to moder-ate (16 [0-23] days) to severe (1 [0-20] day). Median (IQR) duration of me-chanical ventilation in survivorsincreased with stages of ARDS frommild (5 [2-11] days) to moderate (7 [4-14] days) to severe (9 [5-17] days).
Using the Berlin Definition, 29% (95%CI, 26%-32%) of patients with mildARDS at baseline progressed to moder-
ate ARDS and 4% (95% CI, 3%-6%) pro-gressed to severe ARDS within 7 days;and 13% (95% CI, 11%-14%) of pa-tients with moderate ARDS at baselineprogressed to severe ARDS within 7 days.All differences between outcome vari-ables across categories of modified AECC(ALI non-ARDS and ARDS alone) andacross categories of Berlin Definition(mild, moderate, and severe) were sta-tistically significant (P! .001).
Compared with the AECC defini-tion, the final Berlin Definition had bet-ter predictive validity for mortality withan AUROC of 0.577 (95% CI, 0.561-0.593) vs 0.536 (95% CI, 0.520-0.553; P! .001), with the difference inAUROC of 0.041 (95% CI, 0.030-0.050). To ensure that missing PEEPdata in one of the cohorts did not bias
the results, the regression analysis wasrepeated without this cohort andyielded similar results.
The Berlin Definition performed simi-larly in the physiological database as inthe clinical database (TABLE 5, eFigure1, and eFigure 2). Twenty-five percent(95% CI, 20%-30%) of patients met cri-teria for mild ARDS, 59% (95% CI, 54%-66%) of patients met criteria for moder-ate ARDS, and 16% (95% CI, 11%-21%) of patients met criteria for severeARDS. Mortality increased with stages ofARDS from mild (20%; 95% CI, 11%-31%) to moderate (41%; 95% CI, 33%-49%) to severe (52%; 95% CI, 36%-68%), with P=.001 for differences inmortality across stages of ARDS. Me-dian (IQR) ventilator-free days de-clined with stages of ARDS from mild
Table 3. The Berlin Definition of Acute Respiratory Distress SyndromeAcute Respiratory Distress Syndrome
Timing Within 1 week of a known clinical insult or new or worsening respiratorysymptoms
Chest imaginga Bilateral opacities—not fully explained by effusions, lobar/lung collapse, ornodules
Origin of edema Respiratory failure not fully explained by cardiac failure or fluid overloadNeed objective assessment (eg, echocardiography) to exclude hydrostatic
edema if no risk factor presentOxygenationb
Mild 200 mm Hg ! PaO2/FIO2 " 300 mm Hg with PEEP or CPAP #5 cm H2Oc
Moderate 100 mm Hg ! PaO2/FIO2 " 200 mm Hg with PEEP #5 cm H2OSevere PaO2/FIO2 " 100 mm Hg with PEEP #5 cm H2O
Abbreviations: CPAP, continuous positive airway pressure; FIO2, fraction of inspired oxygen; PaO2, partial pressure ofarterial oxygen; PEEP, positive end-expiratory pressure.
aChest radiograph or computed tomography scan.b If altitude is higher than 1000 m, the correction factor should be calculated as follows: [PaO2/FIO2$ (barometric pressure/
760)].cThis may be delivered noninvasively in the mild acute respiratory distress syndrome group.
Table 4. Predictive Validity of ARDS Definitions in the Clinical DatabaseModified AECC Definitiona Berlin Definition ARDSa
ALI Non-ARDS ARDS Mild Moderate SevereNo. (%) [95% CI] of patients 1001 (24) [23-25] 3187 (76) [75-77] 819 (22) [21-24] 1820 (50) [48-51] 1031 (28) [27-30]Progression in 7 d from mild,
No. (%) [95% CI]336 (34) [31-37] 234 (29) [26-32] 33 (4) [3-6]
Progression in 7 d from moderate,No. (%) [95% CI]
230 (13) [11-14]
Mortality, No. (%) [95% CI]b 263 (26) [23-29] 1173 (37) [35-38] 220 (27) [24-30] 575 (32) [29-34] 461 (45) [42-48]Ventilator-free days, median (IQR)b 20 (2-25) 12 (0-22) 20 (1-25) 16 (0-23) 1 (0-20)Duration of mechanical ventilation in
survivors, median (IQR), db5 (2-10) 7 (4-14) 5 (2-11) 7 (4-14) 9 (5-17)
Abbreviations: AECC, American-European Consensus Conference; ALI, acute lung injury; ARDS, acute respiratory distress syndrome; FIO2, fraction of inspired oxygen; IQR, inter-quartile range; PaO2, arterial partial pressure of oxygen; PEEP, positive end-expiratory pressure.
aThe definitions are the following for ALI non-ARDS (200 mm Hg!PaO2/FIO2"300 mm Hg, regardless of PEEP), ARDS (PaO2/FIO2"200 mm Hg, regardless of PEEP), mild Ber-lin Definition (200 mm Hg!PaO2/FIO2"300 mm Hg with PEEP #5 cm H2O), moderate Berlin Definition (100 mm Hg!PaO2/FIO2"200 mm Hg with PEEP #5 cm H2O), andsevere Berlin Definition (PaO2/FIO2"100 mm Hg with PEEP #5 cm H2O).
bComparisons of mortality, ventilator-free days, and duration of mechanical ventilation in survivors across categories of modified AECC (ALI non-ARDS and ARDS) and acrosscategories of Berlin Definition (mild, moderate, and severe) are all statistically significant (P! .001).
THE BERLIN DEFINITION OF ACUTE RESPIRATORY DISTRESS SYNDROME
©2012 American Medical Association. All rights reserved. JAMA, Published online May 21, 2012 E5
Downloaded From: http://jama.jamanetwork.com/ on 06/05/2012
DEFINITION DITE DE BERLIN
02/10/2015! S.Dauger!
DEFINITION PEDIATRIQUE MORBI-MORTALITE INTRODUCTION CONCLUSION HISTORIQUE
5 / 26

• Age: 1 à 18 mois • Etude rétrospective / dossiers inform • 7 Réa Ped européennes - 2009 à 2011 • Patients avec ALI /ARDS selon AECC • Objectifs: IR : survie, survie sans ECMO - IIR : DMS Réa Ped
• 221 patients, Age=6 mois, DMS=10 jours • 38 décès, 4 ECMO (1 décès) • SDRA: PaO2/FiO2 au diagnostic: 133 (3-262)
AECC: ALI non-ARDS 16%, ARDS 84% BD: Mild 16%, Moderate 44%, Severe 40%
• Mortalité: HR [Severe vs Mild ARDS] = 3.8 (1.5-9.5) • ECMO + Mortalité: HR [Severe vs Mild ARDS] = 3.4 (1.4-8.4) • Pas de différence entre ALI (CCAE) et Moderate / Mild (BD)
S.Dauger
De Luca D. Intensive Care Med. 2013;39:2083-2091
DEFINITION PEDIATRIQUE MORBI-MORTALITE INTRODUCTION CONCLUSION HISTORIQUE
03/10/2015 6 / 26

S.Dauger
Copyright © 2015 by the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies.Unauthorized reproduction of this article is prohibited
Pediatric Critical Care Medicine www.pccmjournal.org 1
Objective: To describe the final recommendations of the Pediatric
Acute Lung Injury Consensus Conference.
Design: Consensus conference of experts in pediatric acute lung
injury.
Setting: Not applicable.
Subjects: PICU patients with evidence of acute lung injury or
acute respiratory distress syndrome.
Interventions: None.
Methods: A panel of 27 experts met over the course of 2 years
to develop a taxonomy to define pediatric acute respiratory dis-
tress syndrome and to make recommendations regarding treat-
ment and research priorities. When published, data were lacking
a modified Delphi approach emphasizing strong professional
agreement was used.
Measurements and Main Results: A panel of 27 experts met over
the course of 2 years to develop a taxonomy to define pediatric
acute respiratory distress syndrome and to make recommenda-
tions regarding treatment and research priorities. When published
data were lacking a modified Delphi approach emphasizing strong
professional agreement was used. The Pediatric Acute Lung Injury
Consensus Conference experts developed and voted on a total
of 151 recommendations addressing the following topics related
to pediatric acute respiratory distress syndrome: 1) Definition,
prevalence, and epidemiology; 2) Pathophysiology, comorbidities,
and severity; 3) Ventilatory support; 4) Pulmonary-specific ancillary
treatment; 5) Nonpulmonary treatment; 6) Monitoring; 7) Nonin-
vasive support and ventilation; 8) Extracorporeal support; and 9)
Morbidity and long-term outcomes. There were 132 recommenda-
tions with strong agreement and 19 recommendations with weak
agreement. Once restated, the final iteration of the recommenda-
tions had none with equipoise or disagreement.
Conclusions: The Consensus Conference developed pediatric-
specific definitions for acute respiratory distress syndrome and
recommendations regarding treatment and future research priori-
ties. These are intended to promote optimization and consistency
of care for children with pediatric acute respiratory distress syn-
drome and identify areas of uncertainty requiring further investiga-
tion. (Pediatr Crit Care Med 2015; XX:00–00)
Key Words: acute lung injury; acute respiratory distress syndrome;
consensus development conference; guidelines; pediatrics
Since the first description of the “acute respiratory distress syndrome” (ARDS) by Ashbaugh et al (1) in 1967, pediat-ric intensivists have recognized that ARDS in children is
different from ARDS in adults. In the absence of identification of these differences, however, children have been characterized
Copyright © 2015 by the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies
DOI: 10.1097/PCC.0000000000000350
Supported, in part, by the Department of Pediatrics, The Pennsylvania State University College of Medicine; Health Outcome Axis–Ste Justine Research Center, Montreal, Canada; Respiratory Research Network of Fonds de Recherche du Québec-Santé, QC, Canada; Mother and Children French-Speaking Network; French-Speaking Group in Pediatric Emergency and Intensive Care, French-Speaking Intensive Care Society (SRLF); European Society for Pediatric and Neonatal Intensive Care Society (travel support for European experts); Australian and New Zealand Intensive Care Society (travel support for Australian expert); Children’s Hospital of Richmond of Virginia Commonwealth University; Division of Critical Care Medicine, CS Mott Children’s Hospital at the University of Michigan; and Department of Anesthesia and Critical Care, Children’s Hospital of Philadelphia.
Dr. Jouvet received grants from the respiratory research network of Fonds de Recherche du Québec-Santé, Réseau mère enfant de la francophonie, and Research Center of Ste-Justine Hospital related to the submitted work; and received equipment on loan from Philips and Maquet outside the submit-ted work. Dr. Thomas served on the Advisory Board for Discovery Labora-tories and Ikaria outside the submitted work; received a grant from United States Food and Drug Administration Office of Orphan Product Development outside the submitted work. Dr. Willson served on the Advisory Board for Discovery Laboratories outside the submitted work. Drs. Khemani, Smith, Dahmer, and Watson received grants from the National Institutes of Health (NIH) outside the submitted work. Dr. Zimmerman received research grants from the NIH, Seattle Children's Research Institute, and ImmuneXpress out-side the submitted work. Drs. Flori and Sapru received grants from the NIH related to the submitted work. Dr. Cheifetz served as a consultant with Philips and Hill-Rom outside the submitted work; and received grants from Philips, Care Fusion, Covidien, Teleflex, and Ikaria outside the submitted work. Drs. Rimensberger and Kneyber received travel support from the European Soci-etiy of Pediatric and Neonatal Intensive Care (ESPNIC) related to this work. Dr. Tamburro received a grant from United States Food and Drug Administra-tion Office of Orphan Product Development outside the submitted work. Dr. Emeriaud received a grant from Respiratory Health Network of the Fonds de la Recherche du Québec – Santé outside the submitted work. Dr. Newth served as a consultant for Philips Medical outside the submitted work. Drs. Erickson, Quasney, Curley, Nadkarni, Valentine, Carroll, Essouri, Dalton, Mac-rae, Lopez-Cruces, Santschi, and Bembea have disclosed that they do not have any potential conflicts of interest.
For information regarding this article, E-mail: [email protected]
Pediatric Acute Respiratory Distress Syndrome: Consensus Recommendations From the Pediatric Acute Lung Injury Consensus Conference
The Pediatric Acute Lung Injury Consensus Conference Group
• SDRA pédiatrique différent de SDRA adulte !
• Pourtant même définition depuis la CCAE de 1994.
• Définition revue en 2010 = définition de Berlin:
• Plusieurs limites quand appliquées aux nourrissons/enfants: - Oxygénation mesurée en artériel - Grande variabilité des techniques de ventilation - Physiopath, étiologies, traitements, devenir…
MORBI-MORTALITE INTRODUCTION CONCLUSION HISTORIQUE DEFINITION PEDIATRIQUE
03/10/2015
PALICC Pediatr Crit Care Med. 2015;16(5):428-439
7 / 26

1 - Définir le SDRA pédiatrique 2 - Proposer une prise en charge thérapeutique 3 - Identifier les priorités des futures recherches
PALISI : Amérique du Nord ANZIC : Australie - Nouvelle Zélande CCCTG : Canada WFPIC : Société mondiale de soins intensifs pédiatriques ESPNIC : Europe GFRUP : France
En pratique très proches des objectifs de la CCAE de 1994 chez l’adulte !
S.Dauger
MORBI-MORTALITE INTRODUCTION CONCLUSION HISTORIQUE DEFINITION PEDIATRIQUE
8 / 26 03/10/2015
PALICC Pediatr Crit Care Med. 2015;16(5):428-439

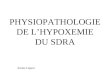
3 membres organisateurs - Début en mars 2012
Méthode: - Delphi: consensus - RAND/UCLA: évaluation reco après textes longs - Graduation: Consensus fort: >7 / 9 Consensus faible: <7 ou 1 expert <7 - 2°tour après nouvelle reco à consensus faible - % experts avec avis <7 Consensus fort: >95% ou 1 expert <7 max
27 experts / 21 institutions / 8 pays
Europe : P. Riemensberger (Suisse) D. Macrae (Angleterre) S. Essourri (France) M. Kneyber (Pays-bas)
S.Dauger
MORBI-MORTALITE INTRODUCTION CONCLUSION HISTORIQUE DEFINITION PEDIATRIQUE
03/10/2015
PALICC Pediatr Crit Care Med. 2015;16(5):428-439
9 / 26

Copyright © 2015 by the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies.Unauthorized reproduction of this article is prohibited
Feature Article
Pediatric Critical Care Medicine www.pccmjournal.org 3
of calculation, a strong agreement corresponded to a percent-age of agreement more than 95% (no more than one expert rated below 7 on the RAND/UCLA scale).
The third and final meeting took place on October 9, 2013, in Paris, France. Each group presented their final recommen-dations, and a third round of voting was conducted for several specific but unresolved recommendations related to the defi-nitions. The organizers believed it was vital to achieve strong agreement regarding definitions, and this was accomplished after much dialog and debate. Additionally, each group of experts presented their consensus regarding key areas of con-troversy and future research.
RESULTSThe nine topics studied by PALICC resulted in 151 total rec-ommendations, including 132 recommendations with strong agreement and 19 with weak agreement. Once restated, the final iteration of the recommendations had none with equi-poise or disagreement, according to the predefined definitions by the RAND/UCLA appropriateness methodology. The rec-ommendations for each topic are listed below, with the justifi-cation for these recommendations detailed in the supplement in this issue of Pediatric Critical Care Medicine.
Section 1: Definition, Prevalence, and Epidemiology1.1 Age. 1.1.1 We recommend that there should not be age criteria for the definition of PARDS. However, exclusion cri-teria for PARDS should include causes of acute hypoxemia that are unique to the perinatal period, such as prematurity-related lung disease, perinatal lung injury (e.g., Meconium
Aspiration Syndrome, and pneumonia and sepsis acquired during delivery), or other congenital abnormalities (e.g., con-genital diaphragmatic hernia or alveolar capillary dysplasia). Strong agreement
1.1.2 We recommend that in the absence of a compel-ling rationale related to physiology or feasibility, studies of PARDS should not include age limits. In order to better understand the pathobiology of PARDS across the spectrum of age, and in the absence of a clear break point in the epide-miology of PARDS, adult and pediatric investigators should engage in collaborative studies targeting adolescents and young adults. Future studies are needed to evaluate potential age-dependent differences in the pathophysiology of PARDS across the entire pediatric age spectrum. Strong agreement
1.2 Timing and Triggers for PARDS. 1.2.1 We recommend that symptoms of hypoxemia and radiographic changes must occur within 7 days of a known clinical insult to qualify for PARDS. Strong agreement
1.3 Defining PARDS in Children With Left Ventricular Dysfunction. 1.3.1 We recommend that children with left ven-tricular heart dysfunction that fulfill all other PARDS criteria have PARDS if the acute hypoxemia and new chest imaging changes cannot be explained by acute left ventricular heart fail-ure or fluid overload. Strong agreement
1.4 Radiographic Findings. 1.4.1 We recommend that chest imaging findings of new infiltrate(s) consistent with acute pulmonary parenchymal disease are necessary to diagnose PARDS. Strong agreement
1.4.2 We recommend that future clinical trials for PARDS should stratify patients by the presence or absence of bilateral
Figure 1. Plan for the three meetings of the Pediatric Acute Lung Injury Consensus Conference (PALICC). The timeline, including the tasks, that has been completed by the PALICC experts. PALISI = Pediatric Acute Lung Injury and Sepsis Investigators.
S.Dauger
MORBI-MORTALITE INTRODUCTION CONCLUSION HISTORIQUE DEFINITION PEDIATRIQUE
03/10/2015
PALICC Pediatr Crit Care Med. 2015;16(5):428-439
10 / 26

9 chapitres = 151 recommandations = 132 « fortes »
1 - Définition, prévalence, épidémiologie
2 - Physiopathologie, comorbidités, sévérité
3 - Supports ventilatoires
4 - Traitements complémentaires à visée pulmonaire
5 - Traitements non pulmonaires
6 - Monitorage
7 - Ventilation et support non invasif
8 - Support extracorporel
9 - Morbidité et devenir à long terme
S.Dauger
MORBI-MORTALITE INTRODUCTION CONCLUSION HISTORIQUE DEFINITION PEDIATRIQUE
03/10/2015
PALICC Pediatr Crit Care Med. 2015;16(5):428-439
11 / 26

S.Dauger
Copyright © 2015 by the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies.Unauthorized reproduction of this article is prohibited
Feature Article
Pediatric Critical Care Medicine www.pccmjournal.org 5
2.2.2 For disease severity measures that can be made at the bedside, we recommend that future research studies evaluating both trajectory of illness and recovery should use standardized, minimal datasets with adequately explicit defi-nitions. Strong agreement
2.2.3 Recent adult studies evaluating the effect of dead-space ventilation, thereby reflecting lung perfusion, have been highly predictive of outcome. We recommend that future mul-ticenter studies should examine the association of dead space and outcome of PARDS. Strong agreement
2.2.4 Studies examining the relationship between tidal vol-ume, peak airway pressures, PEEP, or mean airway pressure with
mortality or length of mechanical ventilation have resulted in con-flicting results; some studies exhibit associations with outcomes while others do not. We recommend that future studies incorporat-ing variables such as tidal volume, peak and plateau airway pressures, PEEP, or Paw use explicit proto-cols and definitions such that these measures can be more robustly evaluated. Strong agreement
2.2.5 Among measures requir-ing more in-depth calculation, we recommend that the use of an estimate of multiple organ system failure should be included in any studies of clinical risk factors asso-ciated with outcome in patients with PARDS. Strong agreement
2.2.6 With respect to evaluating risk factors related to organ failure in a research related to PARDS, caution should be exercised in the use of organ failure scoring sys-
tems that include indices of respiratory failure. We recommend the development of a validated, nonpulmonary organ failure definition for use in PARDS research. Strong agreement
2.2.7 We recommend further research into the potential use of combinations of biomarker levels in providing a stronger prediction of outcome. Strong agreement
2.2.8 We recommend that early response to therapy should not be used as a primary outcome measure in phase III clinical research trials. Future research should explore the relationship of early response to therapy as an intermediate process vari-able linked to more clinically relevant, long-term outcomes (e.g., ventilator-free days and mortality). Strong agreement
Section 3: Ventilatory Support3.1 Modes of Conventional Ven-tilation. 3.1.1 There are no out-come data on the influence of mode (control or assisted) during conventional mechanical ventila-tion. Therefore, no recommenda-tion can be made on the ventilator mode to be used in patients with PARDS. Future clinical studies should be designed to assess con-trol and assisted modes of ventila-tion on outcome. Strong agreement
3.2 Tidal Volume/Plateau Pressure Limitations. 3.2.1 In any mechanically ventilated pedi-atric patient, we recommend in
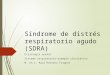
Figure 2. Pediatric acute respiratory distress syndrome definition. OI = oxygenation index, OSI = oxygen saturation index. aUse PaO
2-based metric when available. If PaO
2 not available, wean FIO
2 to maintain
SpO2 ≤ 97% to calculate OSI or oxygen saturation/FIO
2 ratio. bFor nonintubated patients treated with
supplemental oxygen or nasal modes of noninvasive ventilation, see Figure 3 for at-risk criteria. cAcute respiratory distress syndrome severity groups stratified by OI or OSI should not be applied to children with chronic lung disease who normally receive invasive mechanical ventilation or children with cyanotic congenital heart disease. OI = (FIO
2 × mean airway pressure × 100)/PaO
2. OSI = (FIO
2 × mean airway
pressure × 100)/SpO2.
Figure 3. At risk of pediatric acute respiratory distress syndrome definition. aGiven lack of available data, for patients on an oxygen blender, flow for at-risk calculation = FiO
2 × flow rate (L/min) (e.g., 6 L/min flow at 0.35
FiO2 = 2.1 L/min). bIf PaO
2 not available, wean FiO
2 to maintain SpO
2 d 97% to calculate oxygen saturation index.
PF=PaO2/FiO2
OI=(PM x FiO2 x 100)/PaO2
SF=SpO2/FiO2
OSI=(PM x FiO2 x 100)/SpO2
MORBI-MORTALITE INTRODUCTION CONCLUSION HISTORIQUE DEFINITION PEDIATRIQUE
03/10/2015
PALICC Pediatr Crit Care Med. 2015;16(5):428-439
12 / 26

S.Dauger
• Pas de mesure de l’espace mort.
• Pas de mesure de la compliance pulmonaire.
• Si étude, penser à standardiser la lecture des RP voire à les automatiser.
• Objectifs d’oxygénation : 88% < SpO2TC < 97%.
• Pour les patients IRC et cardiaques : diagnostic avec tous les critères et dégradation franche de l’oxygénation.
• Rien sur la prévalence et l’épidémiologie.
MORBI-MORTALITE INTRODUCTION CONCLUSION HISTORIQUE DEFINITION PEDIATRIQUE
03/10/2015
PALICC Pediatr Crit Care Med. 2015;16(5):428-439
13 / 26

S.Dauger
• Il y a des différences avec l’adulte … il n’y a pas d’étude.
• Mesure de la sévérité du SDRA dans les premières 24 h.
• La mesure de l’espace mort devrait être testée chez l’enfant comme facteur prédictif de mortalité.
• Résultats pédiatriques discordants chez l’enfant entre paramètres de ventilation et survie : à tester.
• Intégrer la mesure de la défaillance d’organes dans les futures études.
• Utiliser des critères de jugement robustes à moyen et long termes
MORBI-MORTALITE INTRODUCTION CONCLUSION HISTORIQUE DEFINITION PEDIATRIQUE
03/10/2015
PALICC Pediatr Crit Care Med. 2015;16(5):428-439
14 / 26

S.Dauger
Copyright © 2015 by the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies.Unauthorized reproduction of this article is prohibited
Feature Article
Pediatric Critical Care Medicine www.pccmjournal.org 5
2.2.2 For disease severity measures that can be made at the bedside, we recommend that future research studies evaluating both trajectory of illness and recovery should use standardized, minimal datasets with adequately explicit defi-nitions. Strong agreement
2.2.3 Recent adult studies evaluating the effect of dead-space ventilation, thereby reflecting lung perfusion, have been highly predictive of outcome. We recommend that future mul-ticenter studies should examine the association of dead space and outcome of PARDS. Strong agreement
2.2.4 Studies examining the relationship between tidal vol-ume, peak airway pressures, PEEP, or mean airway pressure with
mortality or length of mechanical ventilation have resulted in con-flicting results; some studies exhibit associations with outcomes while others do not. We recommend that future studies incorporat-ing variables such as tidal volume, peak and plateau airway pressures, PEEP, or Paw use explicit proto-cols and definitions such that these measures can be more robustly evaluated. Strong agreement
2.2.5 Among measures requir-ing more in-depth calculation, we recommend that the use of an estimate of multiple organ system failure should be included in any studies of clinical risk factors asso-ciated with outcome in patients with PARDS. Strong agreement
2.2.6 With respect to evaluating risk factors related to organ failure in a research related to PARDS, caution should be exercised in the use of organ failure scoring sys-
tems that include indices of respiratory failure. We recommend the development of a validated, nonpulmonary organ failure definition for use in PARDS research. Strong agreement
2.2.7 We recommend further research into the potential use of combinations of biomarker levels in providing a stronger prediction of outcome. Strong agreement
2.2.8 We recommend that early response to therapy should not be used as a primary outcome measure in phase III clinical research trials. Future research should explore the relationship of early response to therapy as an intermediate process vari-able linked to more clinically relevant, long-term outcomes (e.g., ventilator-free days and mortality). Strong agreement
Section 3: Ventilatory Support3.1 Modes of Conventional Ven-tilation. 3.1.1 There are no out-come data on the influence of mode (control or assisted) during conventional mechanical ventila-tion. Therefore, no recommenda-tion can be made on the ventilator mode to be used in patients with PARDS. Future clinical studies should be designed to assess con-trol and assisted modes of ventila-tion on outcome. Strong agreement
3.2 Tidal Volume/Plateau Pressure Limitations. 3.2.1 In any mechanically ventilated pedi-atric patient, we recommend in
Figure 2. Pediatric acute respiratory distress syndrome definition. OI = oxygenation index, OSI = oxygen saturation index. aUse PaO
2-based metric when available. If PaO
2 not available, wean FIO
2 to maintain
SpO2 ≤ 97% to calculate OSI or oxygen saturation/FIO
2 ratio. bFor nonintubated patients treated with
supplemental oxygen or nasal modes of noninvasive ventilation, see Figure 3 for at-risk criteria. cAcute respiratory distress syndrome severity groups stratified by OI or OSI should not be applied to children with chronic lung disease who normally receive invasive mechanical ventilation or children with cyanotic congenital heart disease. OI = (FIO
2 × mean airway pressure × 100)/PaO
2. OSI = (FIO
2 × mean airway
pressure × 100)/SpO2.
Figure 3. At risk of pediatric acute respiratory distress syndrome definition. aGiven lack of available data, for patients on an oxygen blender, flow for at-risk calculation = FiO
2 × flow rate (L/min) (e.g., 6 L/min flow at 0.35
FiO2 = 2.1 L/min). bIf PaO
2 not available, wean FiO
2 to maintain SpO
2 d 97% to calculate oxygen saturation index.
PALICC Pediatr Crit Care Med. 2015;16(5):428-439
PF=PaO2/FiO2 - OI=(PM x FiO2 x 100)/PaO2
SF=SpO2 / FiO2 - OSI=(PM x FiO2 x 100)/SpO2
03/10/2015
MORBI-MORTALITE INTRODUCTION CONCLUSION HISTORIQUE DEFINITION PEDIATRIQUE
15 / 26

SUPPORT VENTILATOIRE INVASIF (1)
• Sondes à ballonnet. Tolérer les fuites si OHF.
• Pas de différences selon le mode ventilatoire.
• Vt expiré = 5 à 8 ml/kg selon poids attendu. Plutôt 3 à 6 ml/kg pour les plus sévères.
• Pplat = 28 cm H2O et 29–32 cm H2O pour les plus sévères.
• PEEP = 10 à 15 cm H2O selon oxygénation/hémoD.
• > 15 cm H2O pour les plus sévères en surveillant Pplat.
• Manœuvres de recrutement par augmentation et décroissance progressive de la PEEP, pas du Vt.
02/10/2015! S.Dauger!
MORBI-MORTALITE INTRODUCTION CONCLUSION HISTORIQUE DEFINITION PEDIATRIQUE
16 / 26

• HFO à envisager si Pplat > 28 cm H2O avec manœuvre de recrutement selon O2, CO2, hémodynamique.
• Pas de jet ventilation à haute fréquence, sauf en plus de l’OHF si barotraumatisme massif documenté.
• Pas de percussion à haute fréquence, sauf en cas d’encombrement gênant la ventilation.
• Pas de ventilation liquide.
• PEEP<10: SpO2TC=92 à 97% - PEEP>10: SpO2TC=88 à 92%
• Si SpO2TC<92% : monitorage SvCO2 et délivrance d’O2
• Hypercapnie permissive : pH=7,15-7,30
02/10/2015! S.Dauger!
MORBI-MORTALITE INTRODUCTION CONCLUSION HISTORIQUE DEFINITION PEDIATRIQUE
17 / 26
SUPPORT VENTILATOIRE INVASIF (2)

SUPPORT VENTILATOIRE NON INVASIF
• A mettre en place tôt, plutôt immunodéprimés.
• Intubation si pas d’amélioration rapide.
• Masque naso buccal ou facial.
• Humidification active.
• Sédation possible.
• Plutôt VS PEEP + AI, rarement CPAP seule sauf intolérance.
• Pas d’indication à ce jour de l’O2 à haut débit
02/10/2015! S.Dauger!
MORBI-MORTALITE INTRODUCTION CONCLUSION HISTORIQUE DEFINITION PEDIATRIQUE
18 / 26

TRAITEMENT COMPLEMENTAIRE
• NO: pas systématique. HTAP, défaillance VD, attente ECMO. Evaluer/patient.
• Surfactant: non recommandé.
• DV: non recommandé. Résultats adultes ???
• Aspirations: système clos pas recommandé à ce jour. Attention au dérecrutement. Pas de sérum physiologique.
• Kiné respi: non recommandé à ce jour.
• Corticoïdes: non recommandé à ce jour. • Autres: hélium, prostaglandines, activateurs du
plasminogène, fibrinolytiques, b-2, n acétylcystéïne, almitrine, cough-assist : non recommandés
02/10/2015! S.Dauger!
MORBI-MORTALITE INTRODUCTION CONCLUSION HISTORIQUE DEFINITION PEDIATRIQUE
19 / 26

MONITORAGE
• Scope et alarmes: individuelles spécifiques.
• Poids prédit: sexe, taille, longueur de l’ulna.
• Monitorage ventilatoire: Vt expiré continu, Pmax (PC-VAC), Pplat (VC-VAC), pression/volume et débit/volume, spirométrie à pièce en T chez petits (ou compensés)
• Oxygénation: FIO2, SpO2TC, PaO2, Pmoy, GDS à une fréquence à adapter à chaque patient, PCO2TC ou CO2ET.
• Sevrage: épreuves de VS ou de sevrage.
• Radio: pour le diagnostic, réquence à adapter à chaque patient, pas de TDM systématique.
• Hémodynamique: échocardiographie, KTA 02/10/2015! S.Dauger!
MORBI-MORTALITE INTRODUCTION CONCLUSION HISTORIQUE DEFINITION PEDIATRIQUE
20 / 26

SUPPORT EXTRA-CORPOREL
• Si étiologie réversible ou greffe pulmonaire possible.
• Evaluation précise.
• Qualité de vie au décours.
• Equipe entrainée.
• Techniques partielles ?
02/10/2015! S.Dauger!
MORBIDITE - DEVENIR A LONG TERME
• SpO2TC, questionnaire des symptomes, EFR +/- pneumopédiatre dans l’année suivante.
• Evaluation neurolo-psychologique à 3 mois.
MORBI-MORTALITE INTRODUCTION CONCLUSION HISTORIQUE DEFINITION PEDIATRIQUE
21 / 26

S.Dauger
Yehya N. Crit Care Med. 2015;43(5):937-946
INTRODUCTION CONCLUSION HISTORIQUE DEFINITION PEDIATRIQUE MORBI-MORTALITE
03/10/2015 22 / 26

Gestel JPJ. Bone Marrow Transplant. 2014;49:1287-1292 02/10/2015! S.Dauger!
INTRODUCTION CONCLUSION HISTORIQUE DEFINITION PEDIATRIQUE MORBI-MORTALITE
23 / 26

Etude multicentrique française
Lille
Robert Debré , Paris
Necker, Paris
Trousseau, Paris
Reine Fabiola, Bruxelles
Investigateur principal : Pr Francis Leclerc, Lille
• Patients revus à 1 an +/- 2 mois
• 3 ans au moins à la reconvocation
TDM thoracique
EFR complète
Examen clinique + interrogatoire
Test de marche de 6 min
S.Dauger
INTRODUCTION CONCLUSION HISTORIQUE DEFINITION PEDIATRIQUE MORBI-MORTALITE
03/10/2015 24 / 26

Mieux décrire le SDRA chez le nourrisson et l’enfant
Etudier les particularités physiopathologiques
Repérer précocement les patients à risque
Cette nouvelle définition : on en fait quoi ?
1
2
3
S.Dauger
HISTORIQUE DEFINITION PEDIATRIQUE MORBI-MORTALITE INTRODUCTION CONCLUSION
Optimiser la réalisation d’études multicentriques 4
Décrire la morbidité - Réduire la mortalité 5
03/10/2015 25 / 26