Embed Size (px)
Citation preview

3155
□ CASE REPORT □
Organizing Pneumonia Complicated by Cyst andPneumothorax Formation
Tsukasa Kadota 1, Kenichiro Shimizu 1, Chikako Tsurushige 1, Makoto Kawaishi 1,
Jun Araya 1, Katsutoshi Nakayama 1, Kazuyoshi Kuwano 1 and Hiroshi Hano 2
Abstract
We present a case of organizing pneumonia complicated by pneumothorax in association with cyst forma-
tion that developed during corticosteroid treatment. Although it has been reported that the check-valve
mechanism is a plausible cause of cyst and pneumothorax formation in patients with organizing pneumonia,
the details of the corresponding pathological changes that occur in air-trapping have not been elucidated. A
pathological examination of lung specimens obtained with video-assisted thoracoscopic surgery suggested
that granulation tissues plugging the bronchiole lumens might be a potential cause of the check-valve mecha-
nism in this case. In this report, we also reviewed eight other cases of organizing pneumonia with pneumot-
horax or cyst formation.
Key words: organizing pneumonia, cyst, pneumothorax, check-valve mechanism
(Intern Med 51: 3155-3158, 2012)(DOI: 10.2169/internalmedicine.51.8319)
Introduction
Organizing pneumonia (OP) complicated by pneumotho-
rax formation concomitantly with cyst formation is rare.
Eight cases of OP complicated by cyst or pneumothorax for-
mation have been previously reported; however, the causal
mechanisms of the development of cyst and pneumothorax
formation related to OP have not been clarified (1-8). Al-
though air-trapping caused by the check-valve mechanism is
thought to be a plausible mechanism of cyst and pneumot-
horax formation, the details of the corresponding pathologi-
cal changes that occur in air-trapping have not been eluci-
dated. We herein report a case of OP complicated by cyst
and pneumothorax formation in which the pathological ex-
amination of lung specimens obtained with video-assisted
thoracoscopic surgery (VATS) suggested that granulation tis-
sues plugging the bronchiole lumens might be a potential
cause of the check-valve mechanism. We also reviewed
eight other reported cases of organizing pneumonia with
pneumothorax or cyst formation.
Case Report
A 37-year-old Japanese man was referred from another
hospital and was admitted to our hospital due to pneumonia
that was refractory to conventional antibiotic treatment. Four
weeks prior to admission, the patient presented with fever, a
dry cough and respiratory distress. Chest X-rays performed
at that time showed multiple areas of consolidation in the
right lung field, and a diagnosis of pneumonia was thus sus-
pected. The patient had been treated unsuccessfully with
several antibiotics (clarithromycin at a dose of 400 mg/day
for three days, then levofloxacin at a dose of 500 mg/day
for three days followed by meropenem at a dose of 1 g/day
for 14 days, garenoxacin at a dose of 400 mg/day for five
days and minocycline at a dose of 200 mg/day for nine
days). The patient also presented with arthralgia of multiple
joints; however, he denied morning stiffness or Raynaud’s
phenomenon. He had no medical history of allergies or pre-
vious medications and had smoked a half-pack of cigarettes
daily for 15 years.
A physical examination revealed hypoxemia with an oxy-
gen saturation of 95% (nasal O2 at 1 L/min). Auscultation of
1Department of Respiratory Medicine, Jikei University Hospital, Japan and 2Department of Pathology, Jikei University Hospital, Japan
Received for publication June 19, 2012; Accepted for publication August 16, 2012
Correspondence to Dr. Tsukasa Kadota, [email protected]
Intern Med 51: 3155-3158, 2012 DOI: 10.2169/internalmedicine.51.8319
3156
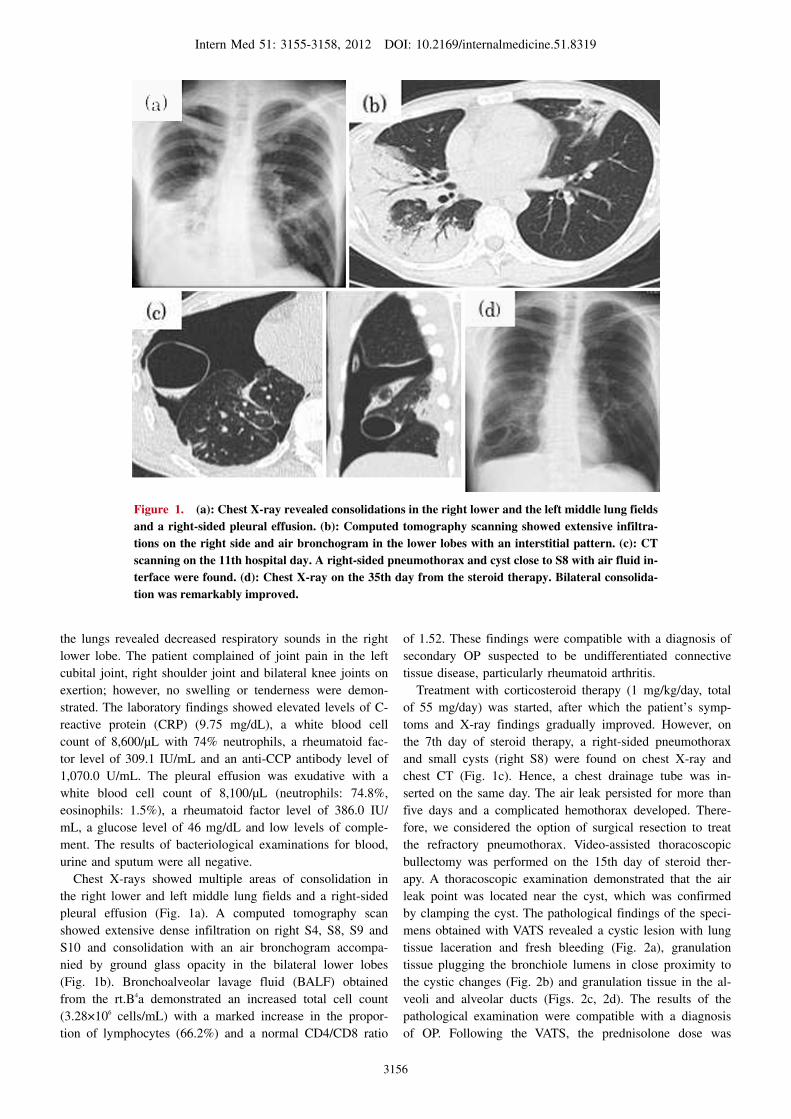
Figure 1. (a): Chest X-ray revealed consolidations in the right lower and the left middle lung fields and a right-sided pleural effusion. (b): Computed tomography scanning showed extensive infiltra-tions on the right side and air bronchogram in the lower lobes with an interstitial pattern. (c): CT scanning on the 11th hospital day. A right-sided pneumothorax and cyst close to S8 with air fluid in-terface were found. (d): Chest X-ray on the 35th day from the steroid therapy. Bilateral consolida-tion was remarkably improved.
the lungs revealed decreased respiratory sounds in the right
lower lobe. The patient complained of joint pain in the left
cubital joint, right shoulder joint and bilateral knee joints on
exertion; however, no swelling or tenderness were demon-
strated. The laboratory findings showed elevated levels of C-
reactive protein (CRP) (9.75 mg/dL), a white blood cell
count of 8,600/μL with 74% neutrophils, a rheumatoid fac-
tor level of 309.1 IU/mL and an anti-CCP antibody level of
1,070.0 U/mL. The pleural effusion was exudative with a
white blood cell count of 8,100/μL (neutrophils: 74.8%,
eosinophils: 1.5%), a rheumatoid factor level of 386.0 IU/
mL, a glucose level of 46 mg/dL and low levels of comple-
ment. The results of bacteriological examinations for blood,
urine and sputum were all negative.
Chest X-rays showed multiple areas of consolidation in
the right lower and left middle lung fields and a right-sided
pleural effusion (Fig. 1a). A computed tomography scan
showed extensive dense infiltration on right S4, S8, S9 and
S10 and consolidation with an air bronchogram accompa-
nied by ground glass opacity in the bilateral lower lobes
(Fig. 1b). Bronchoalveolar lavage fluid (BALF) obtained
from the rt.B4a demonstrated an increased total cell count
(3.28×106 cells/mL) with a marked increase in the propor-
tion of lymphocytes (66.2%) and a normal CD4/CD8 ratio
of 1.52. These findings were compatible with a diagnosis of
secondary OP suspected to be undifferentiated connective
tissue disease, particularly rheumatoid arthritis.
Treatment with corticosteroid therapy (1 mg/kg/day, total
of 55 mg/day) was started, after which the patient’s symp-
toms and X-ray findings gradually improved. However, on
the 7th day of steroid therapy, a right-sided pneumothorax
and small cysts (right S8) were found on chest X-ray and
chest CT (Fig. 1c). Hence, a chest drainage tube was in-
serted on the same day. The air leak persisted for more than
five days and a complicated hemothorax developed. There-
fore, we considered the option of surgical resection to treat
the refractory pneumothorax. Video-assisted thoracoscopic
bullectomy was performed on the 15th day of steroid ther-
apy. A thoracoscopic examination demonstrated that the air
leak point was located near the cyst, which was confirmed
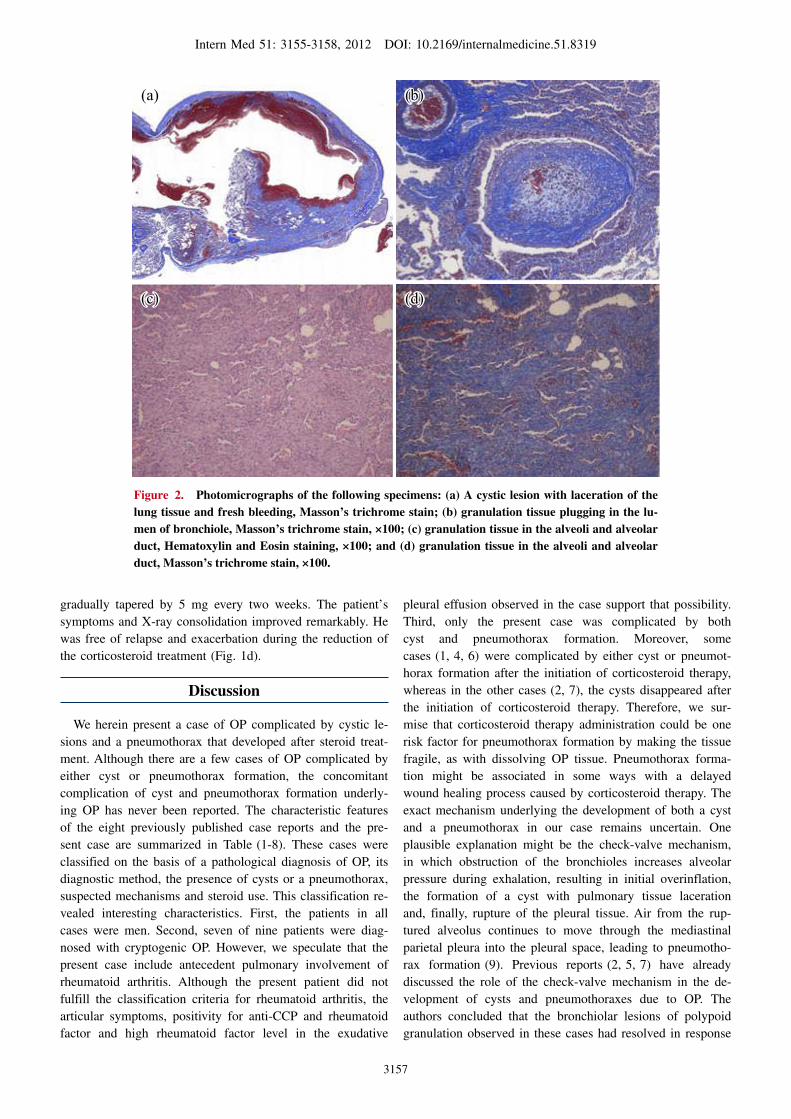
by clamping the cyst. The pathological findings of the speci-
mens obtained with VATS revealed a cystic lesion with lung
tissue laceration and fresh bleeding (Fig. 2a), granulation
tissue plugging the bronchiole lumens in close proximity to
the cystic changes (Fig. 2b) and granulation tissue in the al-
veoli and alveolar ducts (Figs. 2c, 2d). The results of the
pathological examination were compatible with a diagnosis
of OP. Following the VATS, the prednisolone dose was
Intern Med 51: 3155-3158, 2012 DOI: 10.2169/internalmedicine.51.8319
3157
Figure 2. Photomicrographs of the following specimens: (a) A cystic lesion with laceration of the lung tissue and fresh bleeding, Masson’s trichrome stain; (b) granulation tissue plugging in the lu-men of bronchiole, Masson’s trichrome stain, ×100; (c) granulation tissue in the alveoli and alveolar duct, Hematoxylin and Eosin staining, ×100; and (d) granulation tissue in the alveoli and alveolar duct, Masson’s trichrome stain, ×100.
(a)
(c) (d)
(b)(a)
(c) (d)
(b)
gradually tapered by 5 mg every two weeks. The patient’s
symptoms and X-ray consolidation improved remarkably. He
was free of relapse and exacerbation during the reduction of
the corticosteroid treatment (Fig. 1d).
Discussion
We herein present a case of OP complicated by cystic le-
sions and a pneumothorax that developed after steroid treat-
ment. Although there are a few cases of OP complicated by
either cyst or pneumothorax formation, the concomitant
complication of cyst and pneumothorax formation underly-
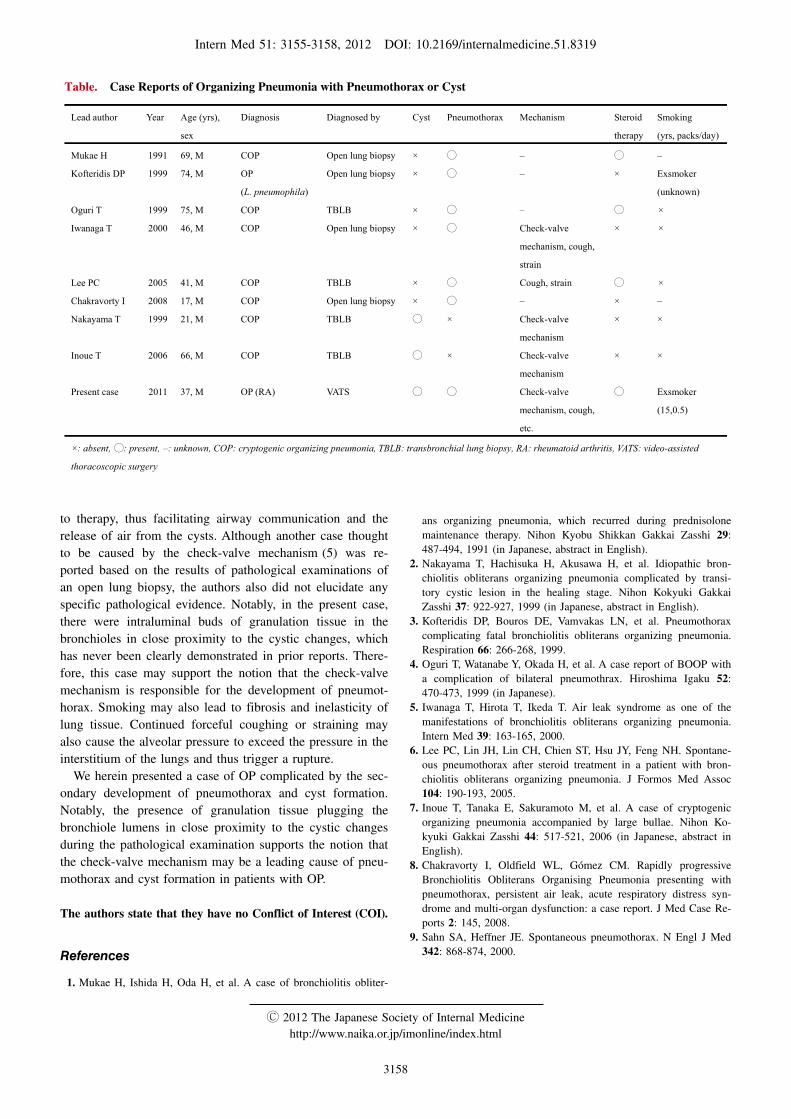
ing OP has never been reported. The characteristic features
of the eight previously published case reports and the pre-
sent case are summarized in Table (1-8). These cases were
classified on the basis of a pathological diagnosis of OP, its
diagnostic method, the presence of cysts or a pneumothorax,
suspected mechanisms and steroid use. This classification re-
vealed interesting characteristics. First, the patients in all
cases were men. Second, seven of nine patients were diag-
nosed with cryptogenic OP. However, we speculate that the
present case include antecedent pulmonary involvement of
rheumatoid arthritis. Although the present patient did not
fulfill the classification criteria for rheumatoid arthritis, the
articular symptoms, positivity for anti-CCP and rheumatoid
factor and high rheumatoid factor level in the exudative
pleural effusion observed in the case support that possibility.
Third, only the present case was complicated by both
cyst and pneumothorax formation. Moreover, some
cases (1, 4, 6) were complicated by either cyst or pneumot-
horax formation after the initiation of corticosteroid therapy,
whereas in the other cases (2, 7), the cysts disappeared after
the initiation of corticosteroid therapy. Therefore, we sur-
mise that corticosteroid therapy administration could be one
risk factor for pneumothorax formation by making the tissue
fragile, as with dissolving OP tissue. Pneumothorax forma-
tion might be associated in some ways with a delayed
wound healing process caused by corticosteroid therapy. The
exact mechanism underlying the development of both a cyst
and a pneumothorax in our case remains uncertain. One
plausible explanation might be the check-valve mechanism,
in which obstruction of the bronchioles increases alveolar
pressure during exhalation, resulting in initial overinflation,
the formation of a cyst with pulmonary tissue laceration
and, finally, rupture of the pleural tissue. Air from the rup-
tured alveolus continues to move through the mediastinal
parietal pleura into the pleural space, leading to pneumotho-
rax formation (9). Previous reports (2, 5, 7) have already
discussed the role of the check-valve mechanism in the de-
velopment of cysts and pneumothoraxes due to OP. The
authors concluded that the bronchiolar lesions of polypoid
granulation observed in these cases had resolved in response
Intern Med 51: 3155-3158, 2012 DOI: 10.2169/internalmedicine.51.8319
3158
Table. Case Reports of Organizing Pneumonia with Pneumothorax or Cyst
Lead author Year Age (yrs),
sex
Diagnosis Diagnosed by Cyst Pneumothorax Mechanism Steroid
therapy
Smoking
(yrs, packs/day)
Mukae H 1991 69, M COP Open lung biopsy × ◯ – ◯ –
Kofteridis DP 1999 74, M OP
(L. pneumophila)
Open lung biopsy × ◯ – × Exsmoker
(unknown)
Oguri T 1999 75, M COP TBLB × ◯ – ◯ ×
Iwanaga T 2000 46, M COP Open lung biopsy × ◯ Check-valve
mechanism, cough,
strain
× ×
Lee PC 2005 41, M COP TBLB × ◯ Cough, strain ◯ ×
Chakravorty I 2008 17, M COP Open lung biopsy × ◯ – × –
Nakayama T 1999 21, M COP TBLB ◯ × Check-valve
mechanism
× ×
Inoue T 2006 66, M COP TBLB ◯ × Check-valve
mechanism
× ×
Present case 2011 37, M OP (RA) VATS ◯ ◯ Check-valve
mechanism, cough,
etc.
◯ Exsmoker
(15,0.5)
×: absent, ◯: present, –: unknown, COP: cryptogenic organizing pneumonia, TBLB: transbronchial lung biopsy, RA: rheumatoid arthritis, VATS: video-assisted
thoracoscopic surgery
to therapy, thus facilitating airway communication and the
release of air from the cysts. Although another case thought
to be caused by the check-valve mechanism (5) was re-
ported based on the results of pathological examinations of
an open lung biopsy, the authors also did not elucidate any
specific pathological evidence. Notably, in the present case,
there were intraluminal buds of granulation tissue in the
bronchioles in close proximity to the cystic changes, which
has never been clearly demonstrated in prior reports. There-
fore, this case may support the notion that the check-valve
mechanism is responsible for the development of pneumot-
horax. Smoking may also lead to fibrosis and inelasticity of
lung tissue. Continued forceful coughing or straining may
also cause the alveolar pressure to exceed the pressure in the
interstitium of the lungs and thus trigger a rupture.
We herein presented a case of OP complicated by the sec-
ondary development of pneumothorax and cyst formation.
Notably, the presence of granulation tissue plugging the
bronchiole lumens in close proximity to the cystic changes
during the pathological examination supports the notion that
the check-valve mechanism may be a leading cause of pneu-
mothorax and cyst formation in patients with OP.
The authors state that they have no Conflict of Interest (COI).
References
1. Mukae H, Ishida H, Oda H, et al. A case of bronchiolitis obliter-
ans organizing pneumonia, which recurred during prednisolone
maintenance therapy. Nihon Kyobu Shikkan Gakkai Zasshi 29:
487-494, 1991 (in Japanese, abstract in English).
2. Nakayama T, Hachisuka H, Akusawa H, et al. Idiopathic bron-
chiolitis obliterans organizing pneumonia complicated by transi-
tory cystic lesion in the healing stage. Nihon Kokyuki Gakkai
Zasshi 37: 922-927, 1999 (in Japanese, abstract in English).
3. Kofteridis DP, Bouros DE, Vamvakas LN, et al. Pneumothorax
complicating fatal bronchiolitis obliterans organizing pneumonia.
Respiration 66: 266-268, 1999.
4. Oguri T, Watanabe Y, Okada H, et al. A case report of BOOP with
a complication of bilateral pneumothrax. Hiroshima Igaku 52:
470-473, 1999 (in Japanese).
5. Iwanaga T, Hirota T, Ikeda T. Air leak syndrome as one of the
manifestations of bronchiolitis obliterans organizing pneumonia.
Intern Med 39: 163-165, 2000.
6. Lee PC, Lin JH, Lin CH, Chien ST, Hsu JY, Feng NH. Spontane-
ous pneumothorax after steroid treatment in a patient with bron-
chiolitis obliterans organizing pneumonia. J Formos Med Assoc
104: 190-193, 2005.
7. Inoue T, Tanaka E, Sakuramoto M, et al. A case of cryptogenic
organizing pneumonia accompanied by large bullae. Nihon Ko-
kyuki Gakkai Zasshi 44: 517-521, 2006 (in Japanese, abstract in
English).
8. Chakravorty I, Oldfield WL, Gómez CM. Rapidly progressive
Bronchiolitis Obliterans Organising Pneumonia presenting with
pneumothorax, persistent air leak, acute respiratory distress syn-
drome and multi-organ dysfunction: a case report. J Med Case Re-
ports 2: 145, 2008.
9. Sahn SA, Heffner JE. Spontaneous pneumothorax. N Engl J Med
342: 868-874, 2000.
Ⓒ 2012 The Japanese Society of Internal Medicine
http://www.naika.or.jp/imonline/index.html





























