Embed Size (px)
Citation preview

Estrategias de optimización de la profilaxis quirúrgica: una sola dosis basta
Josep M Badia
Servicio de Cirugía General, Hospital General de Granollers
Universitat Internacional de Catalunya
GEIRAS 2019

Errores de administración de PA
Evidencia y guías
Propuestas de mejora
GEIRAS 2019

Auditoría de Profilaxis en Cirugía Duración
Bratzler DW y cols. Arch Surg 2005;140:174
60%
GEIRAS 2019

Auditoría de Profilaxis en Cirugía Duración
Bratzler DW y cols. Arch Surg 2005;140:174
GEIRAS 2019

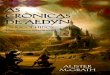
Audit profilaxis %
Incorrecta 43 %
ATB incorrecto 24 %
Dosis incorrecta 19 %
Timing incorrecto 28 %
Duración incorrecta 38 %
McGrath K et al. Crit Care 2014
GEIRAS 2019

Prolongación de PA y mR
Estudio de cohorte, 2641 operaciones de by-pass coronario
PA > 24 horas no disminuye ILQ, puede aumentarla e incrementa el riesgo de mR
PA > 48 h no se asoció a menor ILQ (OR 1,2; CI 0,8-1,6)
PA > 48 h se asoció a mayor riesgo de resistencia bacteriana (OR 1,6; CI 1,1-2,6)
Harbath S y cols. Circulation 2000
GEIRAS 2019

GEIRAS 2019

Moderate quality of evidence. Postoperative continuation has neither benefit nor harm in reducing SSI rates when compared
to a single dose of antibiotic prophylaxis.
GEIRAS 2019

Cardíaca
Vascular
GEIRAS 2019

OrtognáticaGEIRAS 2019

Guías – OMS 2016
GEIRAS 2019

Guías – CDC 2017
GEIRAS 2019

Guías – SEIMC-AEC 2019
¿Cuál es la duración más adecuada? Para la mayoría de procedimientos quirúrgicos, una dosis única de un
antibiótico cuya semivida asegure niveles de fármaco en suero y tejido suficientes mientras dura la intervención quirúrgica es adecuada (A-I).
¿Es necesario repetir la dosis durante la cirugía? Se recomienda una dosis adicional intraoperatoria cuando el procedimiento
quirúrgico exceda dos veces la semivida del antibiótico (B-II). Con cefazolina u otro antibiótico con semivida similar se debe administrar una
segunda dosis intraoperatoria a las 3 horas (B-II). Se recomienda una dosis adicional cuando la semivida del antibiótico está
disminuida (quemados, elevadas tasas de filtración glomerular), o sangrado significativo (> 1.500 mL en adultos ó 25 mL/kg en niños) (B-II).
GEIRAS 2019

Ortognática
Tort S et al. Cochrane 2016
GEIRAS 2019

Artroplastia
Siddiqi A et al. J Bone Jont Surg 2019
GEIRAS 2019

Estrategias de optimización de la profilaxis quirúrgica: una sola dosis basta
GEIRAS 2019

Evidencia científica
Guidelines
GEIRAS 2019

Evidencia científica
Guidelines Cumplimiento
GEIRAS 2019

Online surveys to members of:
AEC: 835 responses
AECP: 355 responses
AEEQ and 9 Spanish Societies of
Surgical Specialties: 1,105 responses
Aim: to know the level of implementation of the “core” measures
Questions to determine which measures were used in their hospital and the personal preferences of surgeons.
Comparison of results with recommendations of national and international organizations.
GEIRAS 2019

45,7%42,8%
52,8%
33,1%
53,4%
39,1%
31,8%
27,0%
18,2%
29,6%
33,4%
30,0%
34,1%
73,3%70,5%
49,7%
67,8%
27,7%
60,6%
57,5%
12,6%
37,4%
51,0%
19,9%
0,0%
10,0%
20,0%
30,0%
40,0%
50,0%
60,0%
70,0%
80,0%
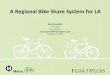
No eliminaciónvello
Rasurado conmaquinillaeléctrica
Antisepsia consolución
alcohólica
Protecciónmárgenes conanillo plástico
Normotermiaintra o
perioperatoria
Hiperoxiaperioperatoria
FiO2 0,8
Lavados decavidades
Lavados delsubcutáneo
Suturasantisépticas
Cambio dematerial
quirúrgico
Cambio deguantes
Terapia depresiónnegativa
Hay evidencia Lo utilizo
Brecha evidencia - práctica 1.105 enfermerasquirúrgicas y cirujanosde 9 especialidades
Badia JM et al. Congress of the Surgical Infection Society-Europe - Dublin,2019
GEIRAS 2019

GEIRAS 2019

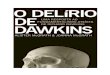
Translationof evidenceinto practice
33,9%
79,0%
49,9%
75,5%
50,6%
71,1%
62,5%
51,7%
73,0%
79,6%
78,9%
81,60%
56,7%
61,2%
30,0%
59,2%
35,6%
44,3%
58,2%
31,8%
23,6%
26,4%
WHO check-list
Bundle for SSI prevention
Hospital policy for SSI prevention
Fast-track protocol
SSI surveillance program
Provider-specific feedback
Computerized decision program
SSI surveillance hospital team
Surgical Unit SSI coordinator
Educational program
Educative materials in theatre
0% 10% 20% 30% 40% 50% 60% 70% 80% 90%
Currently in place Should be implemented24
1,105 responses10 Societies (nurses and surgeons)
GEIRAS 2019

Estrategias para la prevención de la ILQ
Vigilancia y feed-back
Trabajo en equipo
Bundles - Checklist
GEIRAS 2019

Estrategias para la prevención de la ILQ
Vigilancia y feed-back
Trabajo en equipo
BundleCheklist
Feed-back, Circuito
Informatización
GEIRAS 2019

Estrategias para la prevención de la ILQ
“we engaged an interdisciplinary team,
including surgery, anesthesia, nursing,
and hospital epidemiology and infection
control leaders, to support development
of a colorectal CUSP team.”
“Front-line personnel”
Vigilancia y feed-back
Trabajo en equipo
BundleCheklist
GEIRAS 2019

GEIRAS 2019

GEIRAS 2019

Odom-Forren J. Nursing 2006;36:59–63
Greene LR. Am Nurse Today 2015;10:9
GEIRAS 2019

Mauermann WJ et al.
Anesthesiology
2006;105:413-21
GEIRAS 2019

GEIRAS 2019

Estrategias para la prevención de la ILQ
Vigilancia y feed-back
Trabajo en equipo
BundleCheklist
GEIRAS 2019

GEIRAS 2019

GEIRAS 2019

Protocolización
Formación
Team-work
Circuitos – work flow
Prescripción automatizada 2.0
Check-list 2.0
Audit informatizado 2.0
Feed-back
GEIRAS 2019

Muchas gracias!GEIRAS 2019

GEIRAS 2019

Prescripción automatizada
Timely discontinuation from 38.8% to 55.7% (p<0.001)
Absolute increase of 16.9% (95% CI 10.1% to 23.7%)
Greater in cardiac surgeries: 33.6% (95% CI 23.9% to 43.2%)
Evidence of infection in only 14% of surgeries where the prescriber indicated treatment as the reason for ordering
GEIRAS 2019











![Ich heiße Sie herzlich willkommen. Steve McGrath Direktor HM Revenue & Customs [Amt für Steuern und Zölle]](https://img.pdfslide.tips/doc/110x75/570491cd1a28ab14218df493/ich-heisse-sie-herzlich-willkommen-steve-mcgrath-direktor-hm-revenue-customs.jpg)