Embed Size (px)
Citation preview

Übersichten
Notfall RettungsmedDOI 10.1007/s10049-017-0315-5
© Springer Medizin Verlag GmbH 2017
N. Hammer1,2 · D. Häske3 · A. Höch4 · C. Babian5 · B. Hossfeld6 · P. Voigt7 ·D. Winkler8 · M. Bernhard9
1 Department of Anatomy, University of Otago, Dunedin, New Zealand2 Institute of Anatomy, University of Leipzig, Leipzig, Germany3 Faculty of Medicine, Eberhard Karls University Tübingen, Tübingen, Germany4Department of Orthopaedics, Trauma and Reconstructive Surgery, University Clinic of Leipzig, Leipzig,Germany
5 Institute of Forensic Medicine, University of Leipzig, Leipzig, Germany6Department of Anesthesiology and Intensive Care Medicine, Section Emergency Medicine, FederalArmed Forces Medical Hospital, Ulm, Germany
7Division of Neuroradiology, University Clinic of Leipzig, Leipzig, Germany8Department of Neurosurgery, University Clinic of Leipzig, Leipzig, Germany9 Emergency Department, University Hospital of Leipzig, Leipzig, Germany
ThoracostomyA pictorial essay on approaches andpotential pitfalls
Introduction
Thoracic trauma is the secondmost com-mon traumatic cause of death [42, 43].About 20% of all major blunt traumacases are accompanied by a pneumo-thorax [26], underlining the need forout-of-hospital or in-hospital pleural de-compression [32]. Both needle decom-pression [2] and thoracostomy followedby chest tube drainage [11, 32] may wellserve to prevent injury-related complica-tions rather than causing iatrogenic dam-age. However, complication rates largelydepend on applying the correct and suit-able technique [9, 12, 17, 36]. Also,though technical complications may notalways hamper the effectiveness of tho-racotomy or cause persistent harm [36],one should be aware of potentially life-threatening conditions following an in-adequate insertion technique. A numberof complications have been described inthe literature, rangingbetween3and37%[4, 13, 18, 26, 36, 38, 40, 44]. Recently,Kaserer et al. [29] presented a retro-spective analysis over a 6-year period, inwhich 24 of 2261 trauma patients (1%)had undergone out-of-hospital chest de-compression. A successful out-of-hospi-tal releaseofa tensionpneumothoraxwasreported in83%ofpatientswith tube tho-
racostomy, whereas needle thoracocen-tesiswasonlyeffective in18%. Accordingto these results, needle decompression isassociated with failure rates higher than80%. In line with the current Germantrauma guidelines, tube thoracostomiesmay already be considered in the out-of-hospital setting to retain sufficientpleuraldecompression upon admission. Theseresults indicate that the technique of tho-racostomy appears to be complex.
Consequently, the given pictorialguide aims at summarising the two mostcommonly used techniques (Bülau andMonaldi) for thoracostomy and needledecompressionand to showpotential pit-falls caused by common but preventablehandling errors. For this purpose, bothpatient cases and clinical interventionsin human cadavers were used to give anencompassing insight.
Table 1 Clinical signs as indicators of pneumo- or haematothorax following blunt trauma.A one-sided diminished breath sound appears to be themost relevant sign.Adapted from [48]
>99% 98% 89% 61% 40% 12% 2% <1%
Auscultation + + + + – – – –
(90% sensitivity, 98% specificity)
Thoracic pain + – + – + – + –
(57% sensitivity, 79% specificity)
Breath shortness + + – – + + – –
(43% sensitivity, 98% specificity)
Procedure
According to the German level 3 guide-line for the management of severe injury,an evaluation of the chest and ventila-tion is recommended in patients suffer-ing from chest trauma [3]. Herein isincluded the respiratory rate and auscul-tation of the chest followed by a conse-quent re-evaluation if needed. Moreover,inspection, palpation and percussion aswell as the use of pulse oximetry shouldbe carried out. Lung sonography hasmeanwhile evolved as a reliable diagnos-tic tool for the evaluation of a pneumoth-orax, thereby combining the low costsand the ease of use in the clinical envi-ronment [27, 47]. If the patient is me-chanically ventilated, capnography andventilation pressure monitoring shouldbe used. Indicators of pneumothorax or
Notfall + Rettungsmedizin
Übersichten
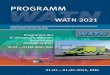
Fig. 18 Bülau thoracostomy. In a (ventral view) andb (dorsal view) a cross-section in the anterior axillary line and spatial re-lations is shown; theasterix shows thesiteof thepneumothorax inb, and thedashed line the internipple line. In candd (lateralview) two commonly usedmethods for excluding axillary fossa injury are summarised.The safe trianglemethod (c) uses thelateralmarginof thepectoralismajor, the anteriormarginof the latissimusdorsi andanextensionof the internipple line tode-lineate the regionof thoracostomy (dashed figure). Alternatively, as shown ind, a hand is placed cranially in the axilla to coverthemostvulnerable regionof theaxillary region.The solid line indicates theanterioraxillary line, thedashed line themiddleax-illar line. Ine (lateral view), the drainage isplaced in themiddle axillary line cranially in the fourth intercostal space, in f (dorsalview) in the anterior axillary line in the same intercostal space.1–7 first to seventh rib,Cl clavicle.Courtesy of the authors
Notfall + Rettungsmedizin

tension pneumothorax may include butare not limited to decreased or missingunilateral respiratory sounds, cutaneousemphysema, serial rib fractures, uppervenous congestion and high ventilationpressures [7, 8]. A suspected pneumo- orhaematothorax should be kept inmind iftheventilationsoundsarereducedunilat-erally (always check the tube position, ifthepatient is intubated). Arelevantpneu-mothorax is unlikely in the absence ofauscultation pathologies, thoracic pain,or dyspnoea (. Table 1; [48]). Moreover,it should be kept in mind that an unde-tected and initially small pneumothoraxcould develop into a life-threatening sit-uation in the following clinical course,especially under ventilation.
A tension pneumothorax will be sus-pected under clinical circumstances witha unilateral loss of ventilation sound byauscultation, and a typical syndrome in-cluding severe respiratory andanobviouscirculatory deterioration. One shouldkeep in mind that an unrecognised ten-sion pneumothorax is the most commonreason for trauma-associated cardiac ar-rest. A tension pneumothorax conse-quently has to be treated already duringthe out-of-hospital emergency medicalservice (EMS) treatment interval. Anassumed tension pneumothorax needsto be decompressed subsequently onceobserved. If a patient is intubated andventilated (positive pressure ventilation),a pneumothorax noticed during auscul-tation should likewise be decompressed.A detected pneumothorax in a sponta-neously breathing patient should be con-trolled and observed continuously.
Technical aspects and themethod of decompression
A needle decompression of a tensionpneumothorax should be done only onetime, immediately followed by a surgicalthoracostomy with or without the inser-tion of a chest tube. A pneumothoraxwithout a tension component is com-monly decompressed applying the thora-costomy technique if indicated. Accord-ing to the recommendations of the Ger-manlevel3guideline for themanagementof severely injured patients [3], a thora-costomyshouldbeperformedusingadig-
Abstract · Zusammenfassung
Notfall Rettungsmed DOI 10.1007/s10049-017-0315-5© Springer Medizin Verlag GmbH 2017
N. Hammer · D. Häske · A. Höch · C. Babian · B. Hossfeld · P. Voigt · D. Winkler · M. Bernhard
Thoracostomy. A pictorial essay on approaches and potentialpitfalls
AbstractBackground. Thoracic trauma with consec-utive pneumothorax or haematothorax canbe accompanied by progressive respiratoryfailure. If untreated, this poses the riskof developing a life-threatening tensionpneumothorax and consecutive death.Needle decompression and thoracostomywith/without chest tube insertion aretherefore considered being among the finallife-saving measures.Objectives. The aim of the given work isto present the anatomical background ofthoracostomy and needle decompression,and to provide an image-based compilationof the procedure and potential pitfalls, basedon the new German level 3 guideline for themanagement of severely injured patients.Materials and methods. Literature review,clinical intervention in cadaveric specimens,subsequent dissection and imaging.Results and conclusions. Chest tubeinsertions are a suitable and effective but
technically challenging procedure to treata pneumothorax or haematothorax. Needledecompression is a simple but temporaryprocedure and is not considered as a measurefor definite care. In the given work, thetwo most commonly used techniques forthoracostomy for chest tube insertion orneedle decompression, namely Monaldi andBülau, are demonstrated using radiologicalimages, anatomical preparations andgraphical illustrations. This guide illustratesthoracic and abdominal surface anatomy andshows the corresponding internal topographyaccording to different levels, as well as theconsequences of potentialmisplacements.
KeywordsChest tubes · Hematothorax · Needledecompression · Respiratory failure · Tensionpneumothorax
Thorakotomie. Bebilderte Anleitung zur Anlage und potenzielleFehlerquellen
ZusammenfassungHintergrund. Das Thoraxtrauma mit konse-kutivem Pneumothorax oder Hämatothoraxgeht neben einem möglichen respiratori-schen Versagenmit dem Risiko einher, einenlebensbedrohlichen Spannungspneumo-thorax zu entwickeln, der unbehandelt zumTod führen kann. Die Nadeldekompressionund Thorakotomie mit/ohne Anlage einerThoraxdrainage gehören zu den endgültigenbzw. lebensrettendenMaßnahmen.Fragestellung. Ziel der Arbeit ist es, dieanatomischen und klinischen Hintergründezur Thorakotomie und Dekompressiondarzustellen und eine bildgestützteZusammenstellung der Vorgehensweiseund möglicher Fallstricke aufzuzeigen. DieBeschreibung und Darstellung berücksichtigtauch die aktuelle Version der deutschenS3-Leitlinie „Polytrauma/Schwerverletzten-Behandlung“.Material und Methoden. Literatur- undBildauswahl, Darstellung der klinischenIntervention an Körperspendern derAnatomie.
Ergebnisse und Diskussion. Die Anlageder Thoraxdrainage ist eine geeignete undwirksame, aber technisch schwierige unddaher komplikationsbehafteteMaßnahme.Die Nadeldekompression ist eine einfache,aber nur vorübergehende Maßnahme undstellt keine definitive Versorgungsoption dar.Diese Arbeit zeigt die beiden am häufigstenverwendeten Techniken (Monaldi- und Bülau-Drainage) zur Thorakotomie bei Anlage derThoraxdrainage oder Nadeldekompressionanhand von radiologischer Bildgebung,anatomischen Präparaten und Grafiken. DieAnleitung weist auf mögliche Fehlanlagenund die Zuordnung der entsprechendenOberflächenanatomie zur inneren Thorax-und Abdominaltopographie hin.
SchlüsselwörterHämatothorax · Nadeldekompression ·Respiratorisches Versagen · Spannungspneu-mothorax · Thoraxdrainage
Notfall + Rettungsmedizin

Übersichten
Fig. 18 Bülau thoracostomy. Ing andh (both ventral view) it is shownhow the index can beused to guide the drainage cra-nially or caudally in the fifth intercostal space,while i–l indicate the final tubeplacement following thoracostomywith theBülau technique (i [lateral view] the drain is secured by a suture, j and k ventral view and l the corresponding dorsal view).1–7 first to seventh rib,Cl clavicle.Courtesy of the authors. (Continued)
Notfall + Rettungsmedizin

ital insertion technique. Here the use ofthe trocars commonly supplied with thechest tubes shouldbe strictly avoided [35,40] to circumvent unintentional iatro-genic damage. Blunt widening of the in-tercostal space should be carried outwiththe finger tips. If the parietal pleura can-not beperforateddigitally, closed scissorsmay be applied to reinforce the examin-ing finger to facilitate this process, butwith extreme care not to harm the lungparenchyma. A catheter sized 28–36 Fris recommended in the case of traumatichaemato- or pneumothorax [19, 48] andan 8–14 Fr-sized catheter in the case ofnontraumatic haemato- or pneumotho-rax [48].
Bülau drainage
The patient is positioned supine with thearm of the respective side abducted andusing monitoring of the vital functions(e. g. ECG, blood pressure, pulse oxime-try). The fourth to sixth ribs and respec-tive intercostal spaces should be identi-fied (. Fig. 1a, b) before a potential entrypoint is identified cranially of the mam-millary line in the middle or anterioraxillary line (. Fig. 1c). Placing a handcranially into the patient’s axilla helpsidentifying the correct levels and is aneasy way to prevent neurovascular path-ways from being injured (. Fig. 1c). An-other approach is the so-called triangleof safety (. Fig. 1d). The anterior borderof the latissimus dorsi, the lateral borderof the pectoralis major form this triangleof safety, and the internipple line, withone of the apices located the axillary fossa[22, 35].
Following thorough disinfection andsterile draping, using sterile gloves,a sharp incision (2–4 cm) will be carriedout by means of a scalpel, ideally in thefourth or fifth intercostal space in case ofusing the middle axillary line (. Fig. 1e)or the fourth intercostal space in caseof the anterior axillary line (. Fig. 1f).Incisions 1 cm anterior of the middleaxillary line appear to save neural struc-tures such as the long thoracic nerve[9]. The incision should be extendedmanually by blunt preparation at theinferior rib of the respective intercostalspace, pushing aside both intercostal
muscles and the parietal pleura to accessthe pleural cavity. Furthermore, usingthe finger allows for palpation of theintercostal space. Danger of injury ofthe provider should be considered incase of bony fragments.
A finger can be used to guide the tipof the drainage either cranially (pneu-mothorax; . Fig. 1g) or caudally (e. g.haematothorax, serothorax; . Fig. 1h).In adults, a drainage insertion length of15–20 cm may serve as a reference valuebut depends on the patients’ length ratio.Care should be taken that some man-ufacturers do not give the total lengthof the drainage rather than the distanceto the most proximal drainage hole –for these types the maximum insertiondistance given by the scale should be5–10 cm less. Following the insertion,the drainage should be secured by 1.0silk suturing (. Fig. 1i) before the in-cision is covered by wound dressings.If applied, a Heimlich valve may beutilised to maintain suction pressuresof 20–30 cm H2O [16, 35, 49]. How-ever, if the Heimlich system is mountedincorrectly, this may even result in a de-terioration of the pneumothorax [10].Moreover, a vacuum of this extent maynot be generated in the common out-of-hospital setting. Here, Heimlich systemsmay only help to decrease the air influxonto the pleural cavity. Therefore, theuse of Heimlich systems during routineuse may not be recommended. Twopotential final positions of the drainagetip following thoracostomy accordingto the Bülau technique are depicted in. Fig. 1j–l.
Monaldi drainage
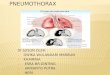
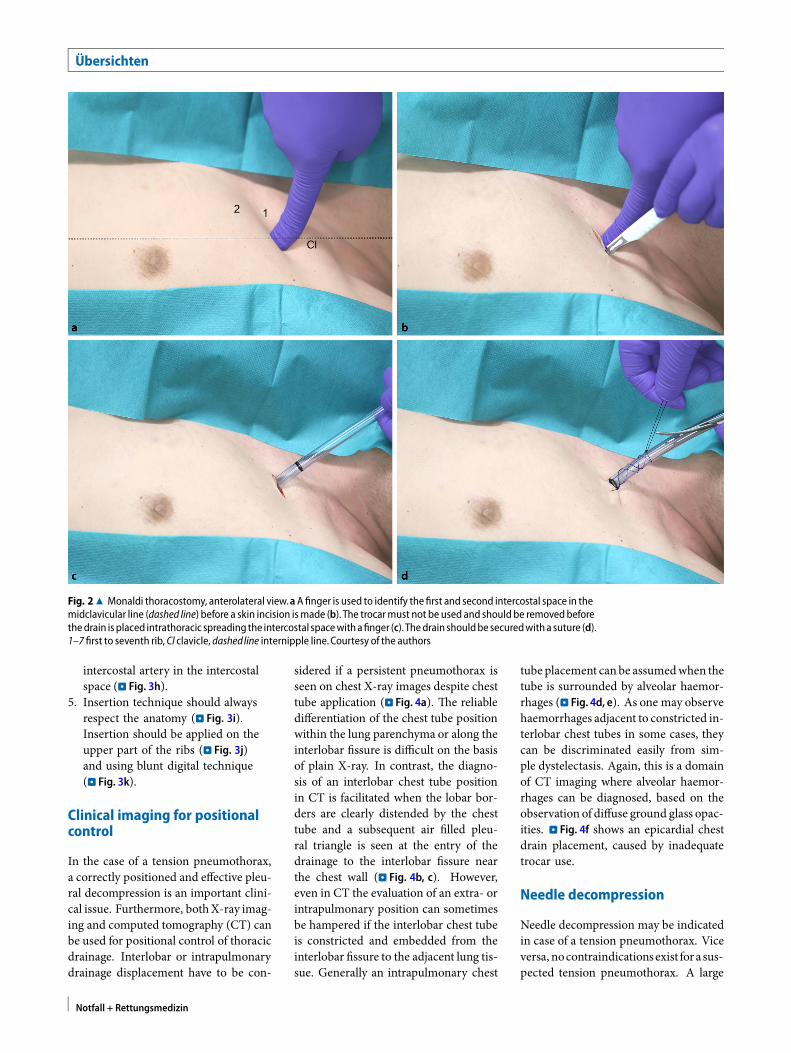
The patient is positioned supine with thearmof the respective side adducted alongthe chest and using monitoring of thevital functions (e. g. ECG, blood pres-sure, pulse oximetry; . Fig. 2a). The firstand second rib and respective intercostalspaces should be identified before a po-tential entry point is identified in themedial clavicular line. To identify thesecond rib, it might be helpful to palpatethe sternal angle between manubriumand corpus of the sternum. Followingthorough disinfection and sterile drap-
ing, using sterile gloves, a sharp incision(2–4 cm) should be carried out by meansof a scalpel, ideally in the second in-tercostal space (. Fig. 2b). The incisionshould be extended manually by bluntdigital preparation at the inferior rib ofthe respective intercostal space, pushingaside both intercostal muscles and theparietalpleura toaccess thepleural cavity.Furthermore, using the finger allows forpalpation of the intercostal space and forplacing the drainage. The danger of self-injury of the provider should be consid-ered in case of bony fragments. . Fig. 2cshows the drainage in a potential end po-sition; 1.0 silk suturing should be doneto secure the drainage (. Fig. 2d).
Pitfalls
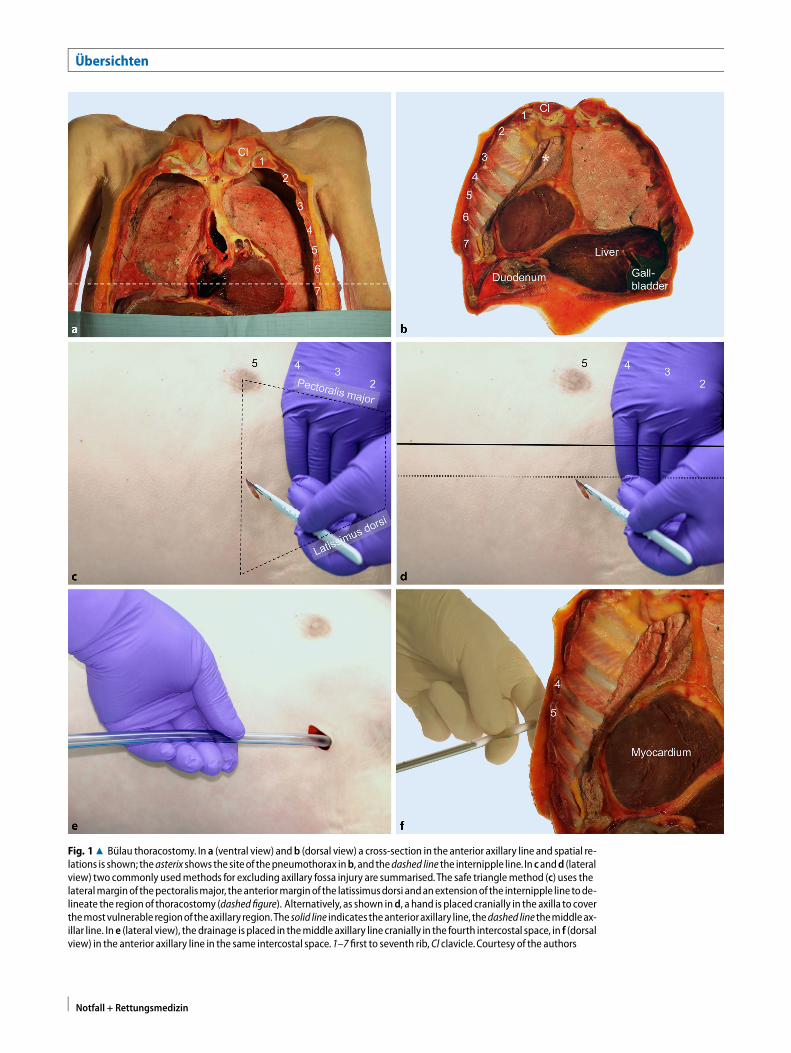
1. The use of scissors to expand theincision (. Fig. 3a) may cause damageto the lung parenchyma (. Fig. 3b).Manual digital techniques should bepreferred.
2. Trocars offer a high risk of iatrogenicinjury (. Fig. 3c Monaldi, 3d Bülau),e. g. parenchymal damage of thelungs (. Fig. 3e) or cardiac injury(. Fig. 3f), and should therefore beavoided in any stage of thoracostomyand drainage [35, 40].
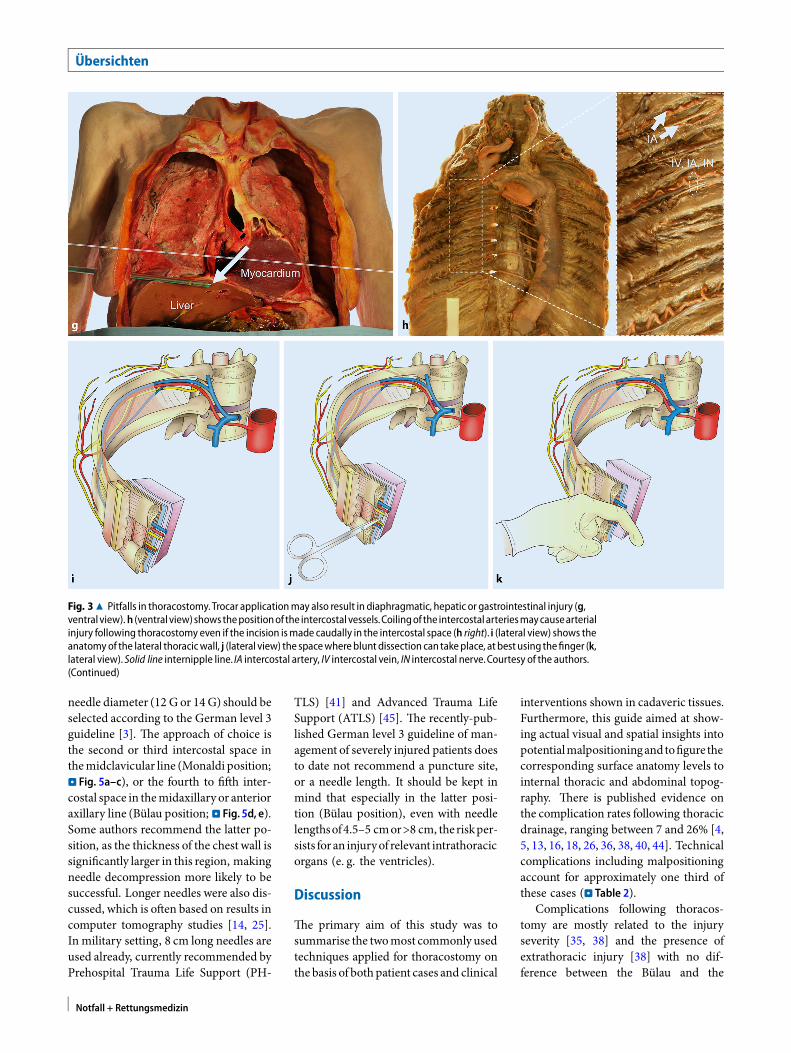
3. Placement caudal of the fifth in-tercostal space may result in di-aphragmatic, hepatic, splenic and/orintestinal lesions (. Fig. 3g). A suf-ficient identification of the insertionpoint is essential.
4. The posterior intercostal vessels andnerve usually run cranially in theintercostal space, merging with thetwo (anterior) intercostal branchesfor each segment originating fromthe internal thoracic artery, onerunning cranially and one caudally.The anastomosis of the posteriorintercostal artery with the anteriorintercostal branches is usually foundin the middle or anterior axillaryline, but can also be located moredorsally (. Fig. 3h). This anatomicalvariation may then cause arterialbleeding if thoracostomy is carriedout according to the existing guide-lines. Moreover, hypertension-relatedcoiling may cause displacement of the
Notfall + Rettungsmedizin
Übersichten
Fig. 28 Monaldi thoracostomy, anterolateral view.aA finger is used to identify the first and second intercostal space in themidclavicular line (dashed line) before a skin incision ismade (b). The trocarmust not be used and should be removedbeforethedrain is placed intrathoracic spreading the intercostal spacewithafinger (c). Thedrain shouldbe securedwitha suture (d).1–7 first to seventh rib,Cl clavicle, dashedline internipple line.Courtesy of the authors
intercostal artery in the intercostalspace (. Fig. 3h).
5. Insertion technique should alwaysrespect the anatomy (. Fig. 3i).Insertion should be applied on theupper part of the ribs (. Fig. 3j)and using blunt digital technique(. Fig. 3k).
Clinical imaging for positionalcontrol
In the case of a tension pneumothorax,a correctly positioned and effective pleu-ral decompression is an important clini-cal issue. Furthermore, bothX-ray imag-ing and computed tomography (CT) canbe used for positional control of thoracicdrainage. Interlobar or intrapulmonarydrainage displacement have to be con-
sidered if a persistent pneumothorax isseen on chest X-ray images despite chesttube application (. Fig. 4a). The reliabledifferentiation of the chest tube positionwithin the lung parenchyma or along theinterlobar fissure is difficult on the basisof plain X-ray. In contrast, the diagno-sis of an interlobar chest tube positionin CT is facilitated when the lobar bor-ders are clearly distended by the chesttube and a subsequent air filled pleu-ral triangle is seen at the entry of thedrainage to the interlobar fissure nearthe chest wall (. Fig. 4b, c). However,even in CT the evaluation of an extra- orintrapulmonary position can sometimesbe hampered if the interlobar chest tubeis constricted and embedded from theinterlobar fissure to the adjacent lung tis-sue. Generally an intrapulmonary chest
tube placement canbe assumedwhen thetube is surrounded by alveolar haemor-rhages (. Fig. 4d, e). As one may observehaemorrhages adjacent to constricted in-terlobar chest tubes in some cases, theycan be discriminated easily from sim-ple dystelectasis. Again, this is a domainof CT imaging where alveolar haemor-rhages can be diagnosed, based on theobservation of diffuse ground glass opac-ities. . Fig. 4f shows an epicardial chestdrain placement, caused by inadequatetrocar use.
Needle decompression
Needle decompression may be indicatedin case of a tension pneumothorax. Viceversa, nocontraindicationsexist forasus-pected tension pneumothorax. A large
Notfall + Rettungsmedizin

Fig. 38 Pitfalls in thoracostomy.Usingscissors forcuttingtissues (a, lateralview)may likely result inparenchymaldamage(b,ventral view). Trocarapplication (c,d, anterolateral and lateralview)mayresult in intralobar (e, ventral view)andcardiac injury(f, dorsal view). Courtesy of the authors
Notfall + Rettungsmedizin
Übersichten
Fig. 38 Pitfalls in thoracostomy.Trocar applicationmay also result in diaphragmatic, hepatic or gastrointestinal injury (g,ventral view).h (ventral view)showsthepositionof the intercostal vessels.Coilingof the intercostal arteriesmaycausearterialinjury following thoracostomy even if the incision ismade caudally in the intercostal space (h right). i (lateral view) shows theanatomyof the lateral thoracicwall, j (lateral view) the spacewhereblunt dissection can takeplace, at best using thefinger (k,lateral view). Solid line internipple line. IA intercostal artery, IV intercostal vein, IN intercostal nerve.Courtesy of the authors.(Continued)
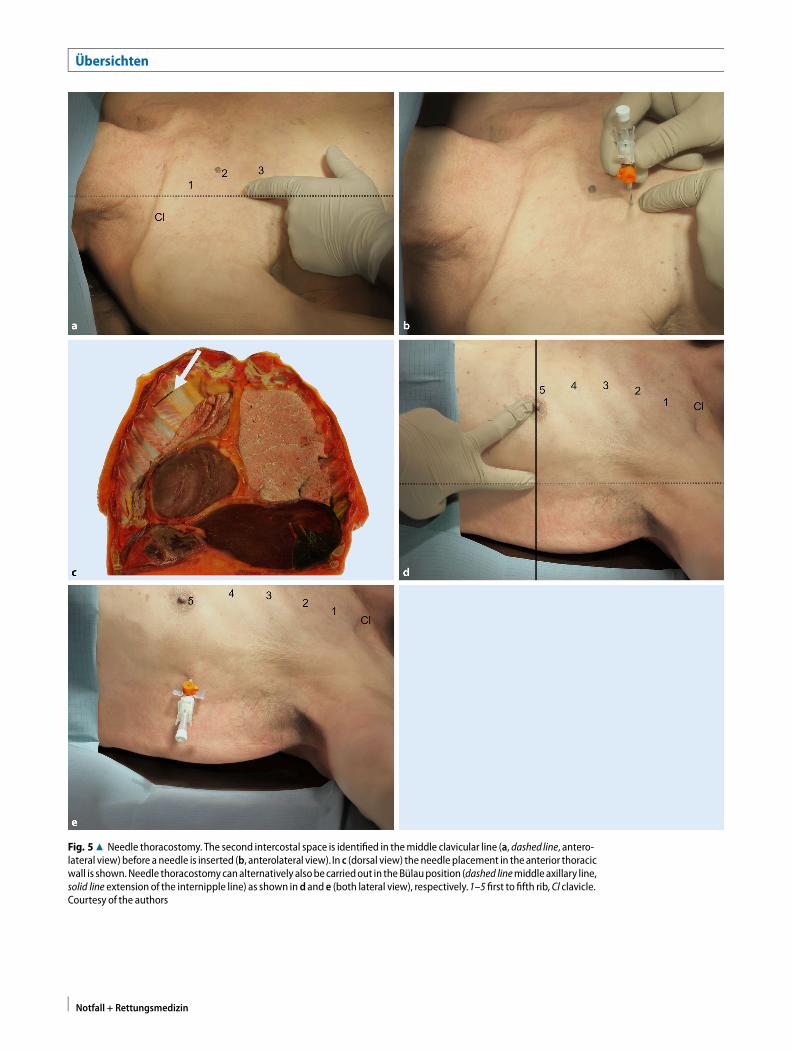
needle diameter (12 G or 14G) should beselected according to the German level 3guideline [3]. The approach of choice isthe second or third intercostal space inthemidclavicular line (Monaldi position;. Fig. 5a–c), or the fourth to fifth inter-costal space in themidaxillary or anterioraxillary line (Bülau position; . Fig. 5d, e).Some authors recommend the latter po-sition, as the thickness of the chest wall issignificantly larger in this region, makingneedle decompression more likely to besuccessful. Longer needles were also dis-cussed, which is often based on results incomputer tomography studies [14, 25].In military setting, 8 cm long needles areused already, currently recommended byPrehospital Trauma Life Support (PH-
TLS) [41] and Advanced Trauma LifeSupport (ATLS) [45]. The recently-pub-lished German level 3 guideline of man-agement of severely injured patients doesto date not recommend a puncture site,or a needle length. It should be kept inmind that especially in the latter posi-tion (Bülau position), even with needlelengthsof4.5–5 cmor>8 cm, theriskper-sists foran injuryof relevant intrathoracicorgans (e. g. the ventricles).
Discussion
The primary aim of this study was tosummarise the twomost commonly usedtechniques applied for thoracostomy onthe basis of bothpatient cases and clinical
interventions shown in cadaveric tissues.Furthermore, this guide aimed at show-ing actual visual and spatial insights intopotentialmalpositioningandtofigure thecorresponding surface anatomy levels tointernal thoracic and abdominal topog-raphy. There is published evidence onthe complication rates following thoracicdrainage, ranging between 7 and 26% [4,5, 13, 16, 18, 26, 36, 38, 40, 44]. Technicalcomplications including malpositioningaccount for approximately one third ofthese cases (. Table 2).
Complications following thoracos-tomy are mostly related to the injuryseverity [35, 38] and the presence ofextrathoracic injury [38] with no dif-ference between the Bülau and the
Notfall + Rettungsmedizin

Fig. 48 Radiological evaluationofchestdrains. Ina (anteriorview)anX-raywithcorrect tubeplacementonthe rightsideanda subcutaneous tube placement on the left side is shown. Inb (transverse) and c (axial) the chest drain is placed inter lobar asseen in computed tomography,d,e (transverse) confirm the suspecteddiagnosis of intrapulmonal placementwith surround-ing haemorrhage. In f (transverse), an epicardial placement is seen in computed tomography.Courtesy of the authors
Notfall + Rettungsmedizin
Übersichten
Fig. 58 Needle thoracostomy. The second intercostal space is identified in themiddle clavicular line (a, dashed line, antero-lateral view)before a needle is inserted (b, anterolateral view). In c (dorsal view) the needle placement in theanterior thoracicwall is shown.Needle thoracostomycanalternatively alsobecarriedout in theBülauposition (dashed linemiddle axillary line,solid line extension of the internipple line) as shown ind and e (both lateral view), respectively.1–5 first to fifth rib, Cl clavicle.Courtesy of the authors
Notfall + Rettungsmedizin
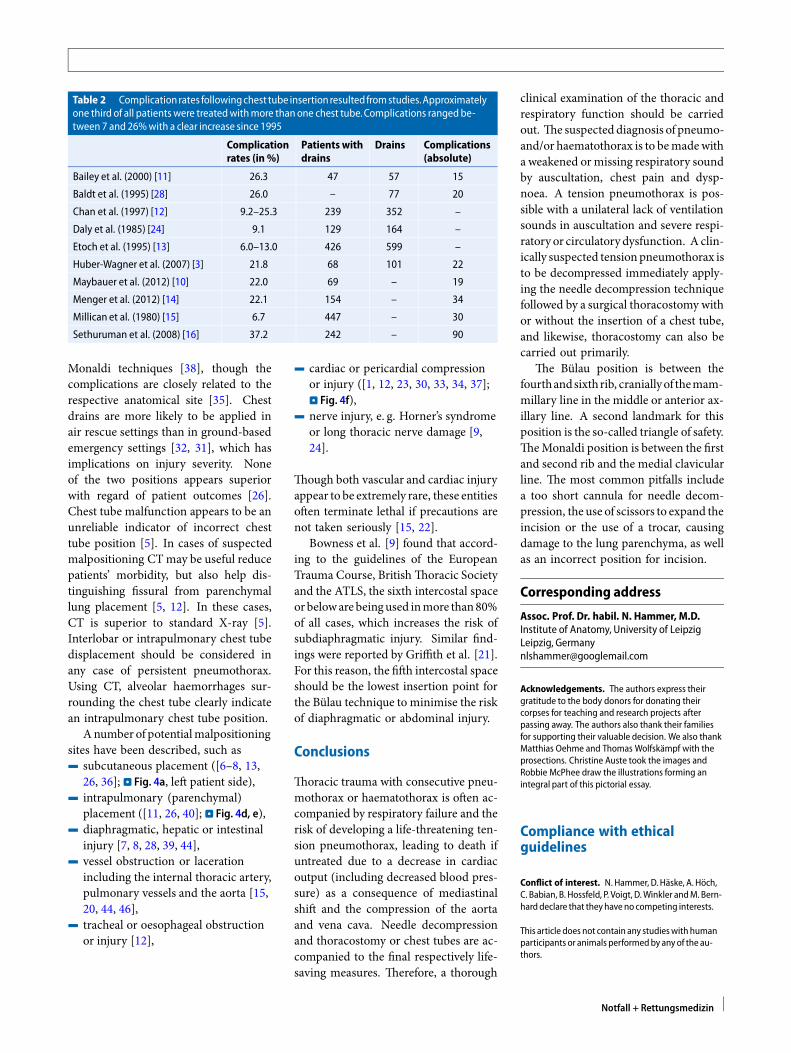
Table 2 Complicationrates followingchest tube insertionresultedfromstudies.Approximatelyone third of all patients were treatedwithmore thanone chest tube.Complications rangedbe-tween 7 and 26%with a clear increase since 1995
Complicationrates (in %)
Patients withdrains
Drains Complications(absolute)
Bailey et al. (2000) [11] 26.3 47 57 15
Baldt et al. (1995) [28] 26.0 – 77 20
Chan et al. (1997) [12] 9.2–25.3 239 352 –
Daly et al. (1985) [24] 9.1 129 164 –
Etoch et al. (1995) [13] 6.0–13.0 426 599 –
Huber-Wagner et al. (2007) [3] 21.8 68 101 22
Maybauer et al. (2012) [10] 22.0 69 – 19
Menger et al. (2012) [14] 22.1 154 – 34
Millican et al. (1980) [15] 6.7 447 – 30
Sethuruman et al. (2008) [16] 37.2 242 – 90
Monaldi techniques [38], though thecomplications are closely related to therespective anatomical site [35]. Chestdrains are more likely to be applied inair rescue settings than in ground-basedemergency settings [32, 31], which hasimplications on injury severity. Noneof the two positions appears superiorwith regard of patient outcomes [26].Chest tube malfunction appears to be anunreliable indicator of incorrect chesttube position [5]. In cases of suspectedmalpositioning CTmay be useful reducepatients’ morbidity, but also help dis-tinguishing fissural from parenchymallung placement [5, 12]. In these cases,CT is superior to standard X-ray [5].Interlobar or intrapulmonary chest tubedisplacement should be considered inany case of persistent pneumothorax.Using CT, alveolar haemorrhages sur-rounding the chest tube clearly indicatean intrapulmonary chest tube position.
Anumber of potentialmalpositioningsites have been described, such as4 subcutaneous placement ([6–8, 13,
26, 36]; . Fig. 4a, left patient side),4 intrapulmonary (parenchymal)
placement ([11, 26, 40]; . Fig. 4d, e),4 diaphragmatic, hepatic or intestinal
injury [7, 8, 28, 39, 44],4 vessel obstruction or laceration
including the internal thoracic artery,pulmonary vessels and the aorta [15,20, 44, 46],
4 tracheal or oesophageal obstructionor injury [12],
4 cardiac or pericardial compressionor injury ([1, 12, 23, 30, 33, 34, 37];. Fig. 4f),
4 nerve injury, e. g. Horner’s syndromeor long thoracic nerve damage [9,24].
Though both vascular and cardiac injuryappear to be extremely rare, these entitiesoften terminate lethal if precautions arenot taken seriously [15, 22].
Bowness et al. [9] found that accord-ing to the guidelines of the EuropeanTrauma Course, BritishThoracic Societyand the ATLS, the sixth intercostal spaceorbeloware beingused inmore than80%of all cases, which increases the risk ofsubdiaphragmatic injury. Similar find-ings were reported by Griffith et al. [21].For this reason, the fifth intercostal spaceshould be the lowest insertion point forthe Bülau technique to minimise the riskof diaphragmatic or abdominal injury.
Conclusions
Thoracic trauma with consecutive pneu-mothorax or haematothorax is often ac-companied by respiratory failure and therisk of developing a life-threatening ten-sion pneumothorax, leading to death ifuntreated due to a decrease in cardiacoutput (including decreased blood pres-sure) as a consequence of mediastinalshift and the compression of the aortaand vena cava. Needle decompressionand thoracostomy or chest tubes are ac-companied to the final respectively life-saving measures. Therefore, a thorough
clinical examination of the thoracic andrespiratory function should be carriedout. The suspected diagnosis of pneumo-and/or haematothorax is to bemadewitha weakened ormissing respiratory soundby auscultation, chest pain and dysp-noea. A tension pneumothorax is pos-sible with a unilateral lack of ventilationsounds in auscultation and severe respi-ratory or circulatory dysfunction. A clin-ically suspected tensionpneumothorax isto be decompressed immediately apply-ing the needle decompression techniquefollowed by a surgical thoracostomy withor without the insertion of a chest tube,and likewise, thoracostomy can also becarried out primarily.
The Bülau position is between thefourthandsixthrib, craniallyof themam-millary line in the middle or anterior ax-illary line. A second landmark for thisposition is the so-called triangle of safety.TheMonaldi position is between the firstand second rib and the medial clavicularline. The most common pitfalls includea too short cannula for needle decom-pression, the use of scissors to expand theincision or the use of a trocar, causingdamage to the lung parenchyma, as wellas an incorrect position for incision.
Corresponding address
Assoc. Prof. Dr. habil. N. Hammer, M.D.Institute of Anatomy, University of LeipzigLeipzig, [email protected]
Acknowledgements. The authors express theirgratitude to the body donors for donating theircorpses for teaching and research projects afterpassing away. The authors also thank their familiesfor supporting their valuable decision. We also thankMatthias Oehme and Thomas Wolfskämpf with theprosections. Christine Auste took the images andRobbie McPhee draw the illustrations forming anintegral part of this pictorial essay.
Compliance with ethicalguidelines
Conflict of interest. N.Hammer, D. Häske, A. Höch,C. Babian, B. Hossfeld, P. Voigt, D.Winkler andM. Bern-harddeclare that theyhave no competing interests.
This article does not contain any studieswith humanparticipants or animals performedby anyof the au-thors.
Notfall + Rettungsmedizin
Übersichten
References
1. Abad C, Padron A (2002) Accidental perforation ofthe left ventriclewith a chest draintube. TexHeartInst J29:143
2. Aho JM, Thiels CA, El KhatibMMetal (2016)Needlethoracostomy: clinical effectiveness is improvedusing a longer angiocatheter. J TraumaAcute CareSurg80:272–277
3. Arbeitsgemeinschaft Der WissenschaftlichenMedizinischen Fachgesellschaften EV (2016)S3 – Leitlinie Polytrauma/Schwerverletzten-Behandlung. AWMFRegister-Nr. 012/019:446
4. Bailey RC (2000) Complications of tube thoracos-tomyin trauma. JAccidEmergMed17:111–114
5. Baldt MM, Bankier AA, Germann PS et al(1995) Complications after emergency tubethoracostomy: assessment with CT. Radiology195:539–543
6. Bergaminelli C, De Angelis P, Gauthier P et al(1999) Thoracic drainage in trauma emergencies.MinervaChir54:697–702
7. Bernhard M, Helm M, Mutzbauer T et al (2010)Invasive Notfalltechniken: Intraossäre Punk-tion, Notfallkoniotomie und Thoraxdrainage.NotfallmedUp2date5:41–59
8. Bernhard M, Helm M, Mutzbauer TS et al (2010)Invasive Notfalltechniken. Notf Rettungsmed13:399–414
9. Bowness J, Kilgour PM, Whiten S et al (2015)Guidelines for chest drain insertion may notprevent damage to abdominal viscera. EmergMedJ32:620–625
10. BroderJS,FoxJW,MilneJetal (2016)Heimlichvalveorientation error leading to radiographic tensionpneumothorax: analysis of an error and a call foreducation, device redesign and regulatory action.EmergMedJ33:260–267
11. BuschmannCT, Kleber C, Schulz T et al (2012)Not-fallmedizinup2date. Rechtsmedizin22:197–216
12. Cameron EW, Mirvis SE, Shanmuganathan K et al(1997) Computed tomography of malpositionedthoracostomy drains: a pictorial essay. Clin Radiol52:187–193
13. Chan L, Reilly KM, Henderson C et al (1997)Complication rates of tube thoracostomy. Am JEmergMed15:368–370
14. ChangSJ, Ross SW,KieferDJet al (2014) Evaluationof 8.0-cm needle at the fourth anterior axillaryline for needle chest decompression of tensionpneumothorax. J Trauma Acute Care Surg76:1029–1034
15. Covelli V, Cavallo P (2008) Unusual late compli-cation of chest tube thoracostomy. Inj Extra39:335–336
16. Daly RC, Mucha P, Pairolero PC et al (1985) The riskofpercutaneouschesttubethoracostomyforbluntthoracic trauma. AnnEmergMed14:865–870
17. De Lesquen H, Avaro JP, Gust L et al (2015)Surgical management for the first 48h followingblunt chest trauma: state of the art (excludingvascular injuries). Interact Cardiovasc Thorac Surg20:399–408
18. EtochSW,Bar-NatanMF,Miller FBetal (1995) Tubethoracostomy. Factors related to complications.ArchSurg130:521–526
19. Fitzgerald M, Mackenzie CF, Marasco S et al(2008)Pleuraldecompressionanddrainageduringtraumareceptionandresuscitation. Injury39:9–20
20. GoodingCA, Kerlan RK Jr., Brasch RC (1981) Partialaortic obstruction produced by a thoracostomytube. JPediatr98:471–473
21. Griffiths JR, Roberts N (2005) Do junior doctorsknowwhere to insert chestdrains safely?PostgradMedJ81:456–458
22. Haron H, Rashid NA, Dimon MZ et al (2010) Chesttube injury to left ventricle: complication ornegligence? AnnThoracSurg90:308–309
23. Harris T,MasudS, LamondAet al (2015) Traumaticcardiacarrest: auniqueapproach. Eur JEmergMed22:72–78
24. Havelock T, Teoh R, Laws D et al (2010) Pleuralprocedures and thoracic ultrasound: BritishThoracic Society pleural disease guideline 2010.Thorax65(Suppl2):ii61–ii76
25. Hecker M, Hegenscheid K, Volzke H et al (2016)Needle decompression of tensionpneumothorax:population-based epidemiologic approach toadequate needle length in healthy volunteers inNortheast Germany. J Trauma Acute Care Surg80:119–124
26. Huber-Wagner S, Korner M, Ehrt A et al (2007)Emergency chest tube placement in trauma care– which approach is preferable? Resuscitation72:226–233
27. Husain LF, Hagopian L, Wayman D et al (2012)Sonographicdiagnosis ofpneumothorax. J EmergTraumaShock5:76–81
28. Icoz G, Kara E, Ilkgul O et al (2003) Perforation ofthe stomach due to chest tube complication ina patient with iatrogenic diaphragmatic rupture.ActaChirBelg103:423–424
29. Kaserer A, Stein P, Simmen HP et al (2016) Failurerate of prehospital chest decompression aftersevere thoracic trauma. Am J EmergMed. doi:10.1016/j.ajem.2016.11.057
30. Kerger H, Blaettner T, Froehlich C et al (2007)Perforation of the left atrium by a chest tubein a patient with cardiomegaly: managementof a rare, but life-threatening complication.Resuscitation74:178–182
31. Kleber C, Giesecke MT, Tsokos M et al (2013)Trauma-related preventable deaths in Berlin2010: need to change prehospital managementstrategies and trauma management education.WorldJSurg37:1154–1161
32. Kleber C, Giesecke MT, Lindner T et al (2014)Requirement for a structured algorithm in cardiacarrest following major trauma: epidemiology,management errors, and preventability of trau-maticdeaths inBerlin. Resuscitation85:405–410
33. Kollef MH, Dothager DW (1991) Reversiblecardiogenic shock due to chest tube compressionof the rightventricle. Chest99:976–980
34. KopecSE,ConlanAA, IrwinRS(1998)Perforationofthe right ventricle: a complication of blind place-mentofachesttubeintothepostpneumonectomyspace. Chest114:1213–1215
35. KuhajdaI,ZarogoulidisK,Kougioumtzi Ietal (2014)Tube thoracostomy; chest tube implantation andfollowup. JThoracDis6:S470–S479
36. Maybauer MO, Geisser W, Wolff H et al (2012)Incidence and outcome of tube thoracostomypositioning in trauma patients. Prehosp EmergCare16:237–241
37. Meisel S, Ram Z, Priel I et al (1990) Anothercomplicationof thoracostomy–perforationof therightatrium. Chest98:772–773
38. Menger R, Telford G, Kim P et al (2012) Compli-cations following thoracic traumamanaged withtubethoracostomy. Injury43:46–50
39. Miller KS, Sahn SA (1987) Chest tubes. Indications,technique,managementandcomplications. Chest91:258–264
40. Millikan JS, Moore EE, Steiner E et al (1980)Complications of tube thoracostomy for acutetrauma. AmJSurg140:738–741
41. Naemt (ed) (2016) Präklinisches Traumamanage-ment. Prehospital Trauma Life Support (PHTLS),Deutsche Bearbeitung durch PHTLS Deutschlandund Schweiz. Urban & Fischer in Elsevier, München
42. Schulz-Drost S, Matthes G, Ekkernkamp A (2015)Erstversorgung des Patienten mit schweremThoraxtrauma. NotfRettungsmed18:421–437
43. Schulz-Drost S, Matthes G, Ekkernkamp A (2015)Thoraxtrauma. NotfallmedUp2date10:17–32
44. Sethuraman KN, Duong D, Mehta S et al (2011)Complications of tube thoracostomy placementin the emergency department. J Emerg Med40:14–20
45. Surgeons ACO (2012) ATLS manual. AmericanCollegeofSurgeons,Chicago
46. Takanami I (2005)Pulmonaryarteryperforationbya tube thoracostomy. Interact Cardiovasc ThoracSurg4:473–474
47. Volpicelli G (2011) Sonographic diagnosis ofpneumothorax. IntensiveCareMed37:224–232
48. WaydhasC,SauerlandS(2007)Pre-hospitalpleuraldecompression and chest tube placement afterblunt trauma: a systematic review. Resuscitation72:11–25
49. Zardo P, Busk H, Kutschka I (2015) Chest tubemanagement: state of the art. Curr OpinAnaesthesiol28:45–49
Notfall + Rettungsmedizin