Embed Size (px)
Citation preview

BENIGN PROSTATIC HYPERPLASIANODULAR HYPERPLASIA
BY : KHALED H. N. ALKHODARISUPERVISOR : DR. BELAL DABOUR

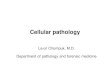
PROSTATEANATOMY

PROSTATEANATOMY

PROSTATEANATOMY

The prostate gland secretes a thin, milky fluid that contains calcium, citrate ion, phosphate ion, a clotting enzyme, and a profibrinolysin.
During emission, the capsule of the prostate gland contracts simultaneously with the contractions of the vas deferens.
30% of semen volume.
A slightly alkaline prostatic fluid successful fertilization of the ovum.
PROSTATEPHYSIOLOGY

Extremely common abnormality.
It is present in: 20% men >= 40 year. increases to 70% by age 60 and to 90% by age 80.
Characterized by : Proliferation of both stromal and epithelial elements. With resultant enlargement of the gland may urinary
obstruction.
PATHOLOGY BENIGN PROSTATIC HYPERPLASIA - BPH

The cause remains incompletely understood But excessive androgen-dependent growth of stromal and glandular elements has a central role .(DHT).
DHT is 10 times more potent than testosterone.
Does not occur in males: Castrated before the onset of puberty. In men with genetic diseases that block androgen
activity.
PATHOLOGY BENIGN PROSTATIC HYPERPLASIA - BPH

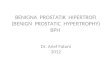
MORPHOLOGY
Always occurs in the inner, transitional zone of the prostate.
Affected prostate is enlarged 60 - 100 g Vs. normal 7 and 16 g.
Contains many well-circumscribed nodules that bulge from the cut surface. Solid Contain cystic spaces = dilated glandular elements.
The urethra is usually compressed.

MORPHOLOGY In some cases, hyperplastic glandular and stromal
elements may project into the bladder lumen as a pedunculated mass a ball-valve type of urethral obstruction.

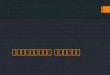
Microscopically the hyperplastic nodules are composed of Variable proportions of proliferating glandular elements. Fibromuscular stroma.
The hyperplastic glands are lined by Tall, columnar epithelial cells. Peripheral layer of flattened basal cells.
The glandular lumina often contain inspissated, proteinaceous secretory material = corpora amylacea.
MORPHOLOGY

CLINICAL FEATURES Appears in only about 10% of men with pathologic
evidence of BPH. There is no direct correlation between histologic changes and
clinical symptoms. The most common manifestations are related to
lower urinary tract obstruction: Difficulty in starting the stream of urine (hesitancy) Intermittent interruption of the urinary stream while
voiding. Later urinary tract infections , hydronephrosis.
These symptoms frequently are accompanied by: Urinary urgency, frequency, and nocturia.

TREATMENT
Initial pharmacological Inhibit DHT formation (Finestride). Relax smooth muscle by blocking alpha adrenergic
blockers (Flomax).
Various surgical techniques are reserved for severely symptomatic cases recalcitrant to medical therapy.