Embed Size (px)
Citation preview
Shinya Goto, Masatsugu Hori, Norio Tanahashi,
Michael Hanna, Suzuko Oikawa, John Alexander
ARISTOTLE Japan investigators
Sponsored by Bristol-Myers Squibb and Pfizer
Apixaban versus Warfarin in Patients with Atrial Fibrillation -Sub-Analysis in Japanese Patients-
① Consultation fees: EISAI ② Stock ownership/profit: none ③ Patent fees: none ④ Remuneration for lecture: EISAI, Sanofi-Aventis, Otsuka ⑤ Manuscript fees: none ⑥ Trust research/joint research funds: Sanofi-Aventi, Eisai, Berlinger-Ingelheim, Otsuka ⑦ Scholarship fund: none ⑧ Affiliation with Endowed Department: none ⑨ Other remuneration such as gifts: none
The Japanese Circulation Society
COI Disclosure
Shinya Goto
Background - Japan sub-analysis -
• Warfarin is highly effective in stroke prevention with atrial fibrillation, but has several limitations.
• ARISTOTLE study demonstrated that….. Apixaban is Superior to warfarin at preventing Stroke/SE, Causes less Bleeding, and Results lower Mortality.
• Sub-analysis was performed for Japanese AF patients in
the ARISTOTLE study
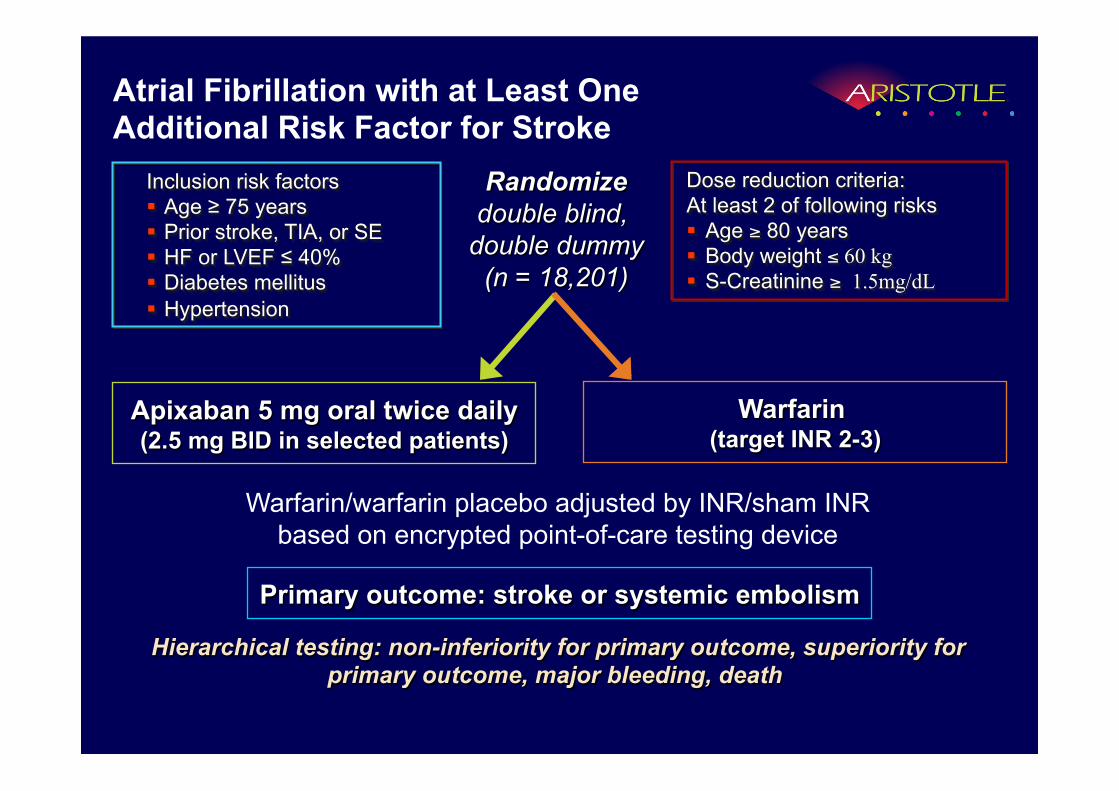
Warfarin (target INR 2-3)
Apixaban 5 mg oral twice daily (2.5 mg BID in selected patients)
Primary outcome: stroke or systemic embolism
Hierarchical testing: non-inferiority for primary outcome, superiority for primary outcome, major bleeding, death
Randomize double blind,
double dummy (n = 18,201)
Inclusion risk factors Age ≥ 75 years Prior stroke, TIA, or SE HF or LVEF ≤ 40% Diabetes mellitus Hypertension
Warfarin/warfarin placebo adjusted by INR/sham INR based on encrypted point-of-care testing device
Dose reduction criteria: At least 2 of following risks Age ≥ 80 years Body weight ≤ 60 kg S-Creatinine ≥ 1.5mg/dL
Atrial Fibrillation with at Least One Additional Risk Factor for Stroke
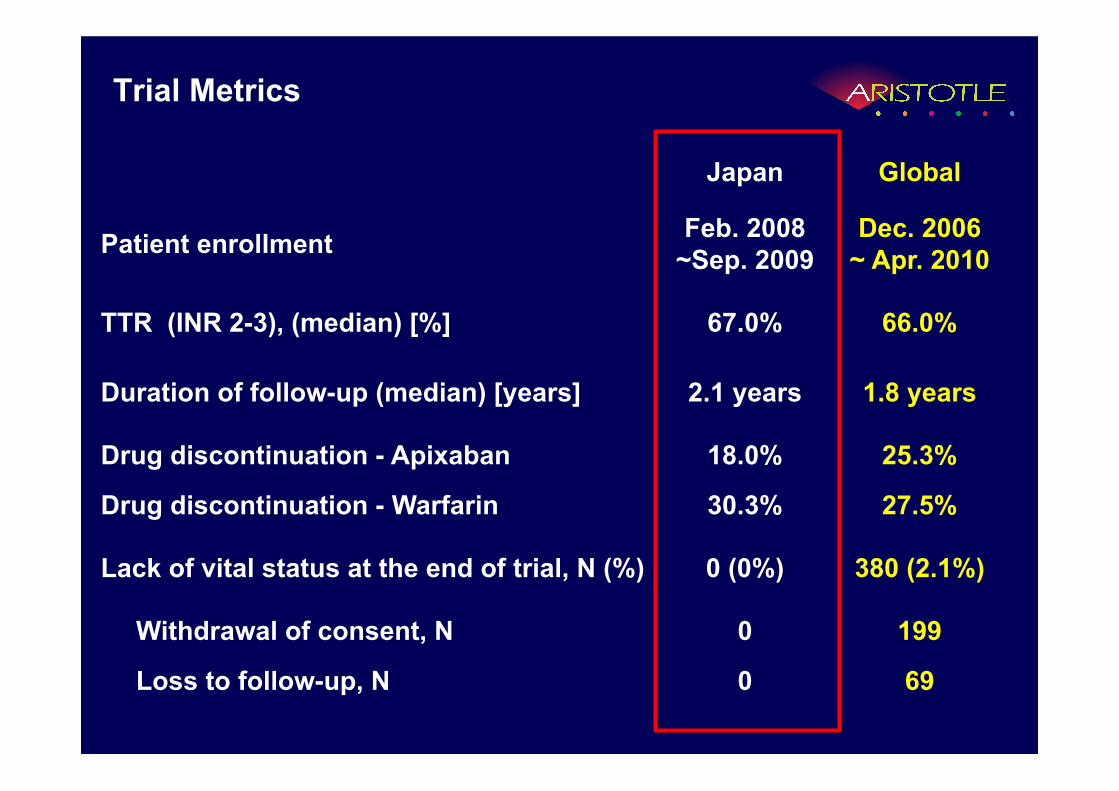
Japan Global
Patient enrollment Feb. 2008 ~Sep. 2009
Dec. 2006 ~ Apr. 2010
TTR (INR 2-3), (median) [%] 67.0% 66.0%
Duration of follow-up (median) [years] 2.1 years 1.8 years
Drug discontinuation - Apixaban 18.0% 25.3%
Drug discontinuation - Warfarin 30.3% 27.5%
Lack of vital status at the end of trial, N (%) 0 (0%) 380 (2.1%)
Withdrawal of consent, N 0 199
Loss to follow-up, N 0 69
Trial Metrics
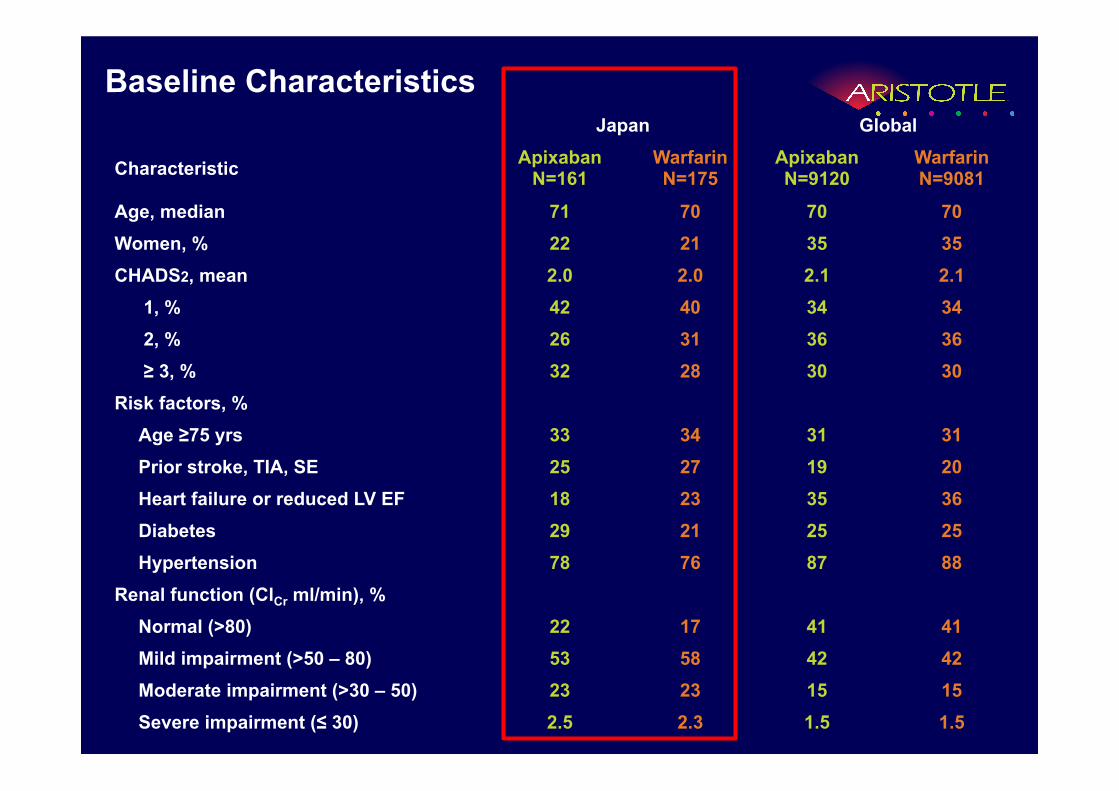
Baseline Characteristics Japan Global
Characteristic Apixaban N=161
Warfarin N=175
Apixaban N=9120
Warfarin N=9081
Age, median 71 70 70 70 Women, % 22 21 35 35 CHADS2, mean 2.0 2.0 2.1 2.1
1, % 42 40 34 34 2, % 26 31 36 36 ≥ 3, % 32 28 30 30
Risk factors, % Age ≥75 yrs 33 34 31 31 Prior stroke, TIA, SE 25 27 19 20 Heart failure or reduced LV EF 18 23 35 36 Diabetes 29 21 25 25 Hypertension 78 76 87 88
Renal function (ClCr ml/min), % Normal (>80) 22 17 41 41 Mild impairment (>50 – 80) 53 58 42 42 Moderate impairment (>30 – 50) 23 23 15 15 Severe impairment (≤ 30) 2.5 2.3 1.5 1.5
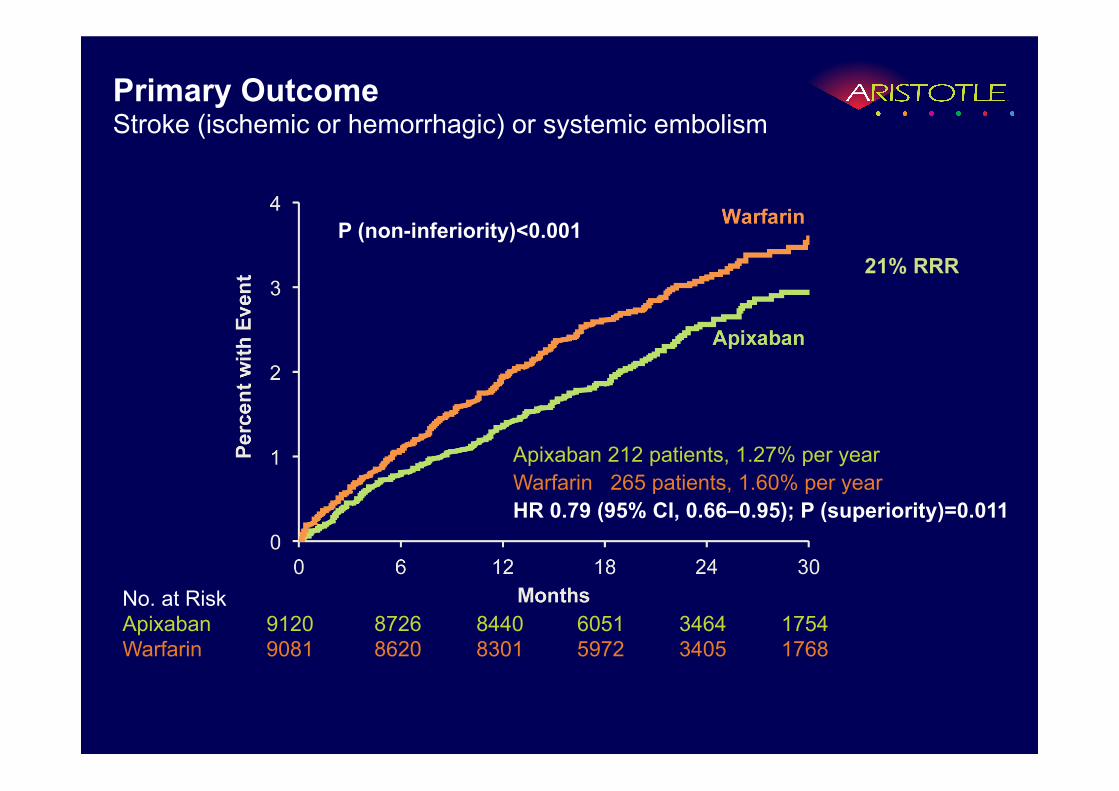
Primary Outcome Stroke (ischemic or hemorrhagic) or systemic embolism
Apixaban 212 patients, 1.27% per year Warfarin 265 patients, 1.60% per year HR 0.79 (95% CI, 0.66–0.95); P (superiority)=0.011
No. at Risk Apixaban 9120 8726 8440 6051 3464 1754 Warfarin 9081 8620 8301 5972 3405 1768
P (non-inferiority)<0.001 21% RRR
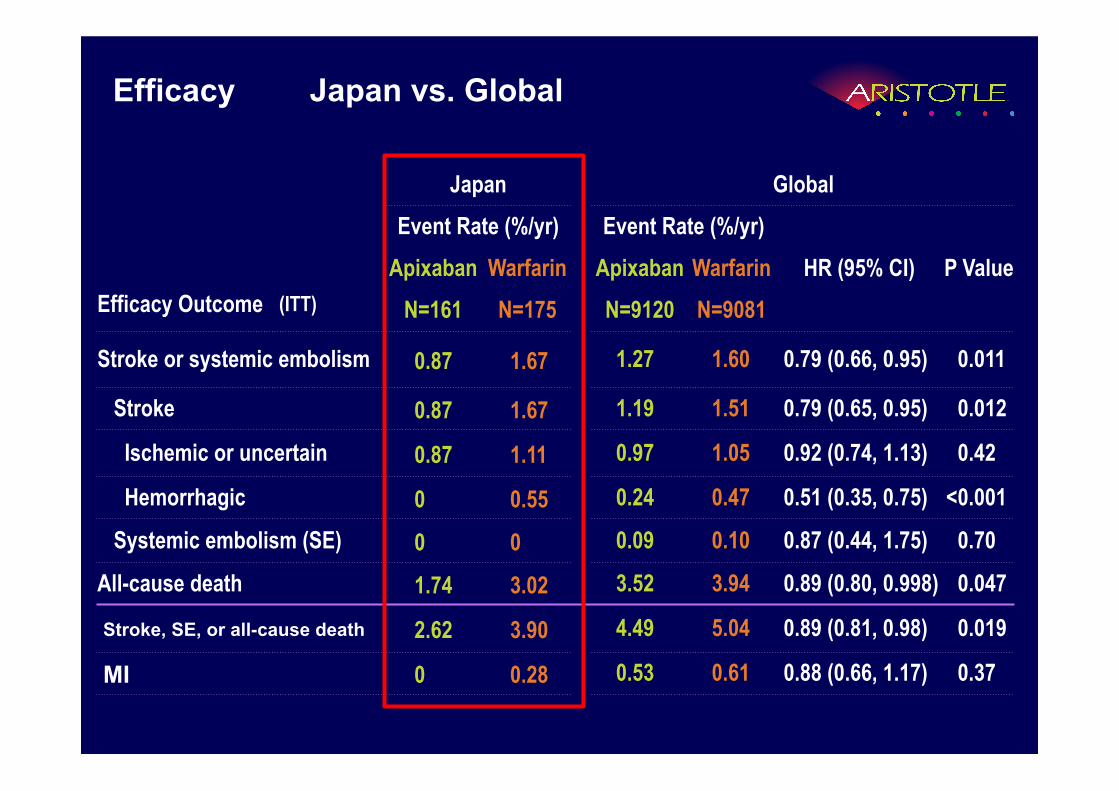
Efficacy Japan vs. Global
Efficacy Outcome (ITT)
Japan Global Event Rate (%/yr) Event Rate (%/yr)
HR (95% CI) P Value Apixaban Warfarin Apixaban Warfarin N=161 N=175 N=9120 N=9081
Stroke or systemic embolism 0.87 1.67 1.27 1.60 0.79 (0.66, 0.95) 0.011
Stroke 0.87 1.67 1.19 1.51 0.79 (0.65, 0.95) 0.012
Ischemic or uncertain 0.87 1.11 0.97 1.05 0.92 (0.74, 1.13) 0.42
Hemorrhagic 0 0.55 0.24 0.47 0.51 (0.35, 0.75) < 0.001
Systemic embolism (SE) 0 0 0.09 0.10 0.87 (0.44, 1.75) 0.70
All-cause death 1.74 3.02 3.52 3.94 0.89 (0.80, 0.998) 0.047
Stroke, SE, or all-cause death 2.62 3.90 4.49 5.04 0.89 (0.81, 0.98) 0.019
MI 0 0.28 0.53 0.61 0.88 (0.66, 1.17) 0.37
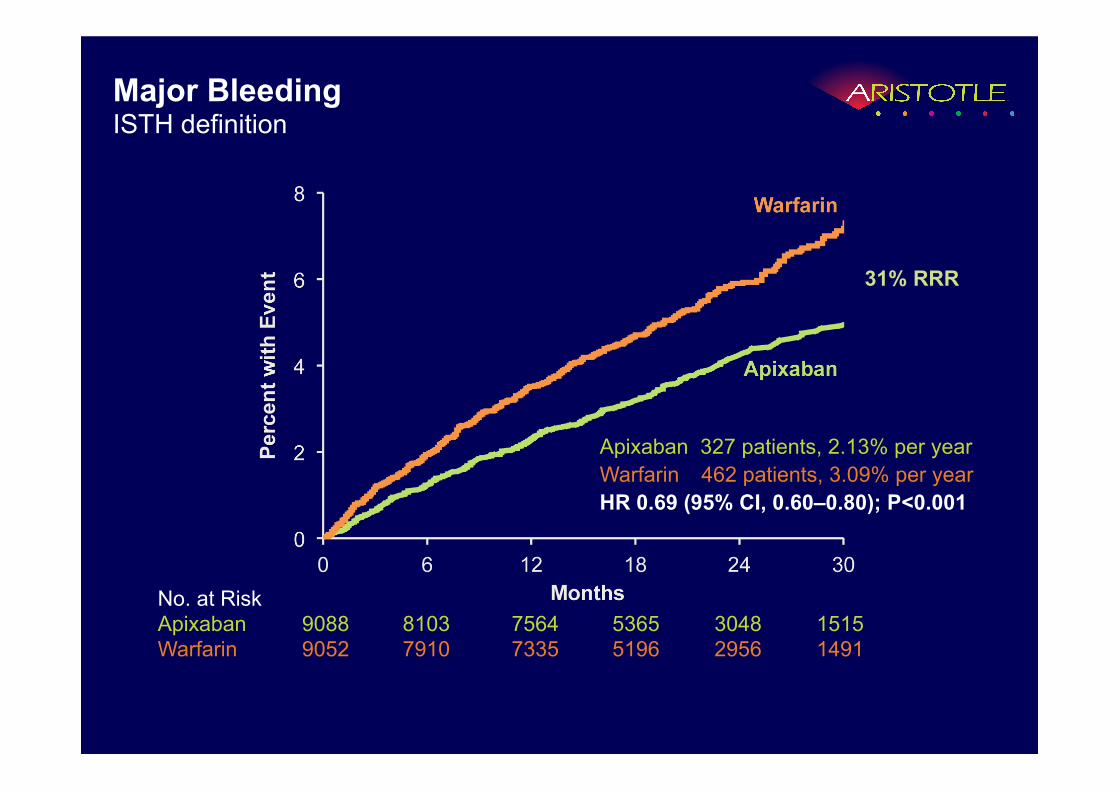
Major Bleeding ISTH definition
Apixaban 327 patients, 2.13% per year Warfarin 462 patients, 3.09% per year HR 0.69 (95% CI, 0.60–0.80); P<0.001
No. at Risk Apixaban 9088 8103 7564 5365 3048 1515 Warfarin 9052 7910 7335 5196 2956 1491
31% RRR
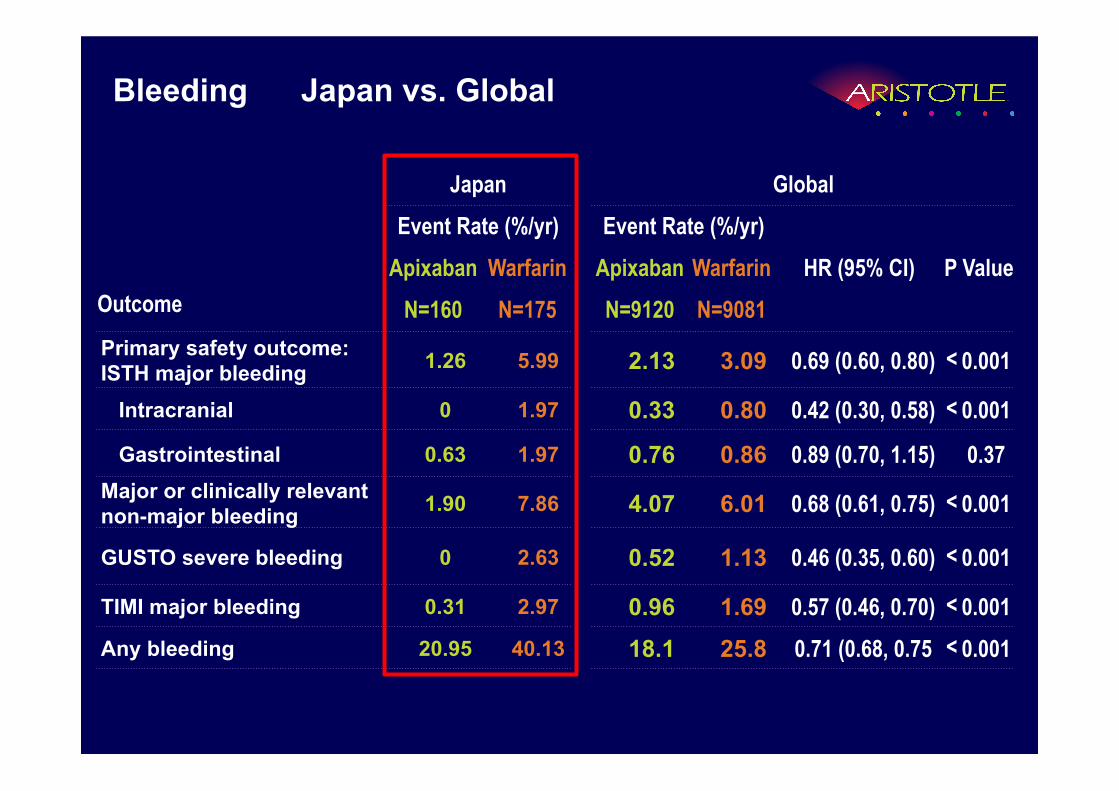
Bleeding Japan vs. Global
Outcome
Japan Global Event Rate (%/yr) Event Rate (%/yr)
HR (95% CI) P Value Apixaban Warfarin Apixaban Warfarin N=160 N=175 N=9120 N=9081
Primary safety outcome: ISTH major bleeding 1.26 5.99 2.13 3.09 0.69 (0.60, 0.80) < 0.001
Intracranial 0 1.97 0.33 0.80 0.42 (0.30, 0.58) < 0.001
Gastrointestinal 0.63 1.97 0.76 0.86 0.89 (0.70, 1.15) 0.37 Major or clinically relevant non-major bleeding 1.90 7.86 4.07 6.01 0.68 (0.61, 0.75) < 0.001
GUSTO severe bleeding 0 2.63 0.52 1.13 0.46 (0.35, 0.60) < 0.001
TIMI major bleeding 0.31 2.97 0.96 1.69 0.57 (0.46, 0.70) < 0.001 Any bleeding 20.95 40.13 18.1 25.8 0.71 (0.68, 0.75 < 0.001
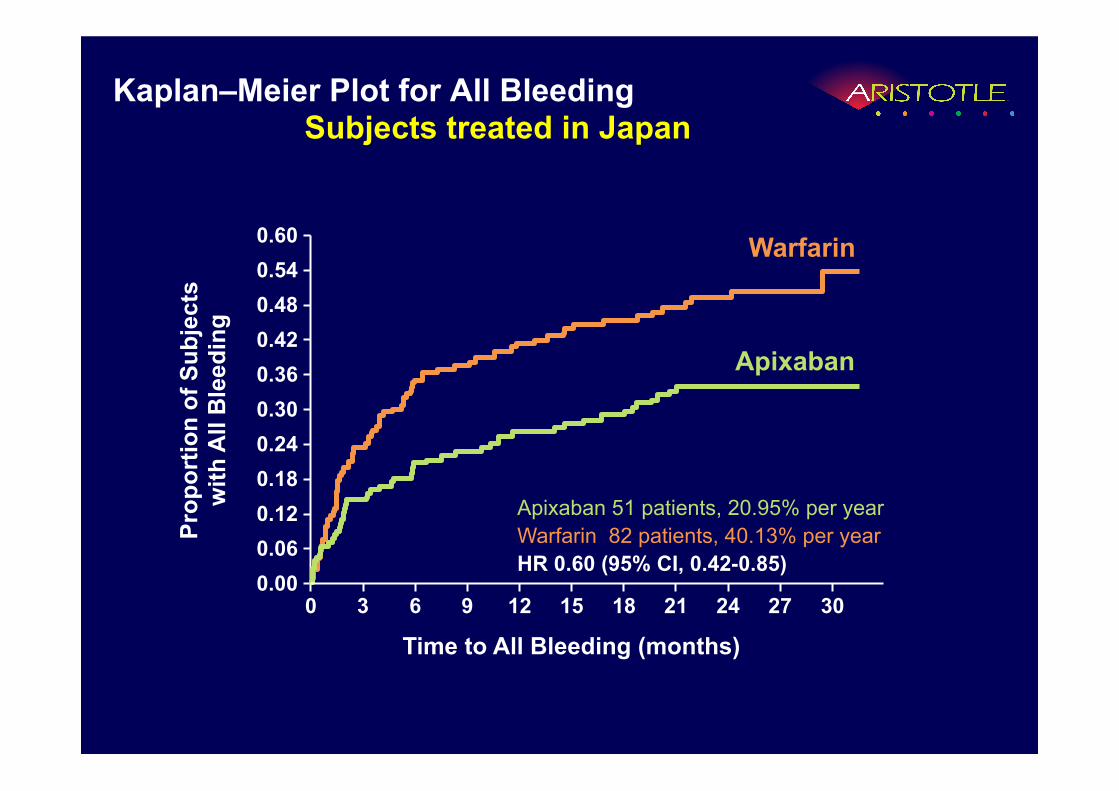
Kaplan–Meier Plot for All Bleeding Subjects treated in Japan
Apixaban 51 patients, 20.95% per year Warfarin 82 patients, 40.13% per year HR 0.60 (95% CI, 0.42-0.85)
0.00
0.60
0.24
0.12
0.36
Prop
ortio
n of
Sub
ject
s
with
All
Ble
edin
g
0.48 0.54
0.18
0.06
0.30
0.42
0
Time to All Bleeding (months) 6 9 12 18 24 3 30 27 21 15
Apixaban
Warfarin
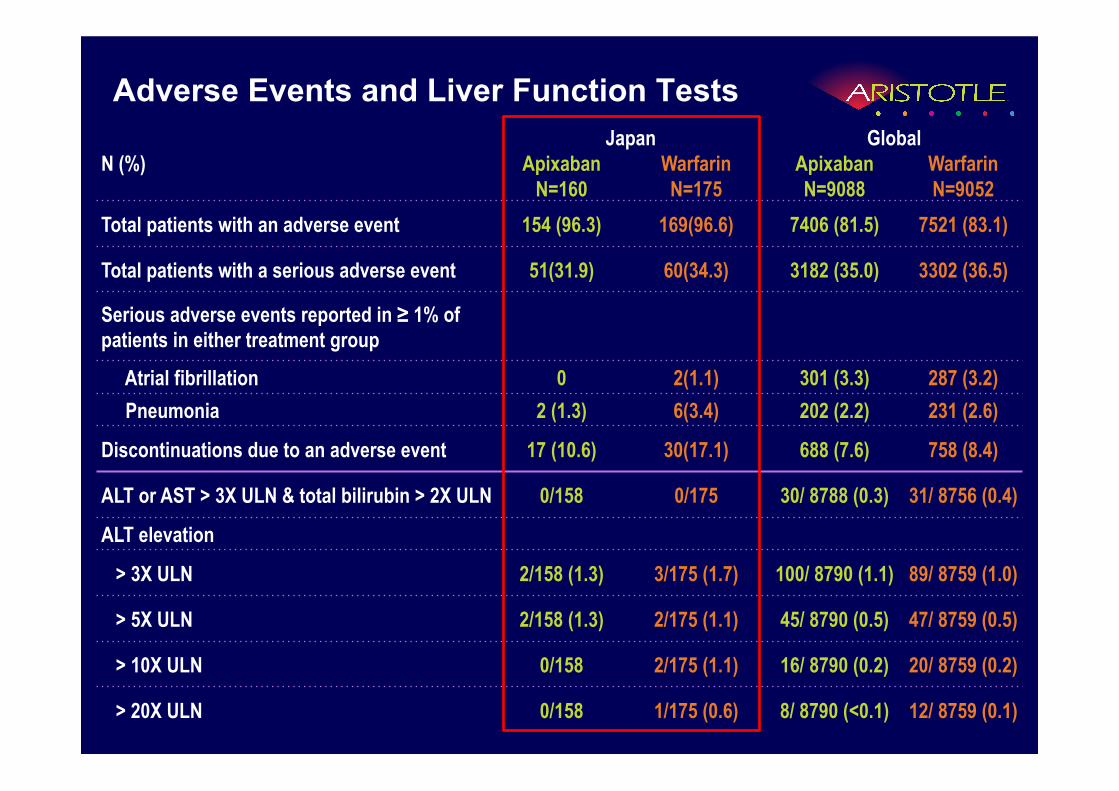
Adverse Events and Liver Function Tests
N (%) Japan Global
Apixaban Warfarin Apixaban Warfarin N=160 N=175 N=9088 N=9052
Total patients with an adverse event 154 (96.3) 169(96.6) 7406 (81.5) 7521 (83.1)
Total patients with a serious adverse event 51(31.9) 60(34.3) 3182 (35.0) 3302 (36.5)
Serious adverse events reported in ≥ 1% of patients in either treatment group
Atrial fibrillation 0 2(1.1) 301 (3.3) 287 (3.2) Pneumonia 2 (1.3) 6(3.4) 202 (2.2) 231 (2.6)
Discontinuations due to an adverse event 17 (10.6) 30(17.1) 688 (7.6) 758 (8.4)
ALT or AST > 3X ULN & total bilirubin > 2X ULN 0/158 0/175 30/ 8788 (0.3) 31/ 8756 (0.4)
ALT elevation
> 3X ULN 2/158 (1.3) 3/175 (1.7) 100/ 8790 (1.1) 89/ 8759 (1.0)
> 5X ULN 2/158 (1.3) 2/175 (1.1) 45/ 8790 (0.5) 47/ 8759 (0.5)
> 10X ULN 0/158 2/175 (1.1) 16/ 8790 (0.2) 20/ 8759 (0.2)
> 20X ULN 0/158 1/175 (0.6) 8/ 8790 (<0.1) 12/ 8759 (0.1)
Conclusion
In patients with atrial fibrillation, apixaban is
superior to warfarin at preventing stroke or
systemic embolism, causes less bleeding, and
results in lower mortality.
Japan:
The results in Japan are consistent with those of the
global.

THANKS to all Japan Collaborators National Coordinator — Shinya Goto :Tokai University School of Medicine
Japan Safety Review Group — Masatsugu Hori :Osaka Medical Center for Cancer & Cardiovascular Diseases Norio Tanahashi : Saitama Medical University International Medical Center John Alexander : Duke University Medical Center
Investigator — Fukui General Clinic Kazuo Satake, Mayumi Taniguchi, Kihara Cardiovascular Clinic Hajime Kihara, Azusa Kitano, National Hospital Organization Takasaki General Medical Center Toyoshi Sakaki,Yoshiko Murayama, Takagi Hospital Takeshi Yoshihiro, Akiko Tsubakihara, Hokusetsu General Hospital Michihiro Suwa, Yukiko Ohara, Izumi General Hospital Hiroshi Yoshii, Yukie Nakama, Oita Red Closs Hospital Tetsu Iwao, Sayumi Sakaguchi, Shuwa General Hospital Susumu Adachi, Takahiro Tojo, Nagasaki University Hospital Kouji Maemura, Yayoi Yoshioka, Saga University Hospital Kouichi Node, Mayumi tomiyasu, Medical Corp. Sakura-kai Takahashi Hospital Akihiko Takahashi, Toshiomi Kunihiro, Toyama Prefectural Central Hospital Kazuo Usuda, Naomi Tamura, Otofuke Koumeikan Hospital Kouichi Fujii, Mika Ohshima, Sapporo Yuushokan Hospital Hiroyuki Takagi, Minori Matsuo, National Hospital Organization Osaka National Hospital Yukihiro Koretsune, Tomoko Kitagawa, Tomakomai
Nisshou Hospital Shigeki Yura, Masato Fujimori, Osaka Saiseikai Izuo Hospital Satoshi Yamamoto, Yukako
Sawada, Izumi Municipal Hospital Yoshio Kawase Hatsumi Watanabe, Nakamura Cardiovascular Clinic Yuuichiro Nakamura, Kazumi Yamamoto, Nara City Hospital Akihiko Matsushima, Mayumi Hyakken, Toho University Ohashi Medical Center Kaoru Sugi, Etsuko Nagumo, Saga Prefectural Hospital KOSEIKAN Kiyoshi Hayashida, Rie Yamaguchi, Osaka General Medical Center Takahisa Yamada, Noriko Oyama, Showa University Hospital Youichi Kobayashi, Fumiyo Hibino, Tokyo Metropolitan Geriatric Hospital Yuusuke Tsubokou, Kaoru Fujinami, National Hospital Organization Yokohama Medical Center Kazunori Iwade, Yuuko Sakuma, Showa University Fujigaoka Hospital Yuukei Higashi, Kanae Iwata, Yubari Medial Center Tomohiko Murakami, Aya Kumagai, National Cerebral and Cardiovascular Center Shirou Kamakura, Fujiko Nakahara, National Hospital Oraniztion Sendai Medical Center Tsuyoshi Shinozaki, Mitsuo Yata, Kurume University Medical Center Hisao Ikeda, Kiyoko Tanaka, Tokai University Hospital Shinya Goto, Michiyo Iwamoto, Medical Corporation Tenyokai Central Clinic Yoshihiko Atsuchi, Narumi Otsuka, Ishinkaii Yao General Clinic Syouzo Tanaka, Yukari Toyama, Iwakuni Medical Center Takayuki Hisaoka, Kunihiro Toshiomi, Uzumasa Hospital Masashi Yamashita, Yukako Sawada, Saga Memorial Hospital Kenichi Yamamoto, Rie Yamaguchi, Yokosuka General Hospital Uwamachi Takamasa Iwasawa, Yuka Motegi, Iseikai Hospital Hirotaka Murata, Yasunori Yamaguchi, Shirakawa Kosei General Hospital Tomiyoshi Saito, Mieko Ishii