Embed Size (px)
Citation preview

10
간암과 감별이 필요한 양성 병변: 혈관성 병변
Benign Liver Mass Lesions: Vascular Lesions
경북대학교 의학전문대학원 내과학교실
탁 원 영
Focal lesions of the liver are commonly found in middle aged and older patients because of increasing usage and
improved sensitivity of imaging modalities. Focal lesions of the liver often have various imaging characteristics which
may be interpreted as either benign or malignant. Benign lesions include cystic lesions, vascular lesions, benign tumors,
pseudo lesions, and various infectious lesions. Hepatic hemangioma is known as the most common benign hepatic
tumor and other vascular lesions are not common. Clinical significance of these vascular lesions is differentiation from
other tumors. Understanding the underlying pathophysiology of these lesions may lead to characteristic imaging
manifestations, which direct the radiologist to the diagnosis. We reviewed the characteristic imaging features, clinical
symptoms, treatment and prognosis of the several hepatic vascular lesions based on the recent literatures.
Key words: Benign hepatic vascular lesions
서 론
최근 건강 검진의 증가와 초음파 및 컴퓨터 단층 촬영 기기 등의 영상 진단 기기의 발달로 간 내 공간
점유 병소의 발견이 늘고 있다. 간 내 공간 점유 병소는 간낭종, 상염색체우성성 다낭성간질환, 혈관종,
국소 결절성 과증식(focal nodular hyperplasia), 간선종(hepatic adenoma), 염증거짓종양(inflammatory pseudotumor),
간자색반병(peliosis hepatis), 국소지방침착, 과오종, 간농양 등 양성 병변에서 간세포암, 간 내 담관암 및
전이암 등 악성 종양까지 다양한 병변이 있을 수 있다.1-3 그 중 간 내 혈관성 병변은 혈관종(hemangioma)
이 대부분이고 나머지는 드물지만 종양과 감별을 해야 할 병변들이다. 이러한 드문 혈관성 병변의 정확한
진단은 영상 진단만으로는 충분치 않아 조직 검사를 시행하기 전에는 감별 진단이 어려운 경우가 많다.
간 내 대부분의 혈관성 병변은 혈관종이며 이외는 매우 드문 질환으로, 현재까지 발표된 자료를 바탕으로
간암과 감별해야 할 혈관성 병변의 진단 및 처치에 대해 정리해 보고자 한다.

탁원영❚Benign Liver Mass Lesions: Vascular Lesions
11
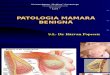
Figure 1. Dynamic contrast enhanced CT scan and contrast enhanced ultrasonography images of hepatic hemangioma. Both images shows peripheral nodular enhancement with centripetal progression of enhancement on the arterial phase (A) and the portal phase (B), and uniformly enhanced and brighter than the background liver on the delayed phase (C).
혈관종(Hemangioma)
혈관종은 간 내 가장 흔한 양성 종양으로 부검에서 관찰되는 빈도는 최대 20%까지 보고되고 있다.
여성에서 4:1에서 6:1의 비로 더 흔하며 모든 연령층에서 발견되나 건강 검진을 시행하기 시작하는 40
대에서 50대에 주로 발견된다.4 대부분의 혈관종은 4㎝미만으로 비교적 작은 혈관종이며 90% 이상에서
단발성이다. 건강검진에서 우연히 발견되는 무증상 결절이 대부분을 차지하며 혈관종은 크기의 변화는
없는 경우가 대부분이다. 일반적으로 4 cm 이상인 혈관종을 거대 혈관종으로 부른다. 혈관종으로 인한
증상은 매우 드물지만, 크기가 큰 경우이거나 또는 다발성일 경우 증상이 있을 수 있다. 주로 종괴에 의
한 주변 장기 압박으로 인해 상복부 불편감 또는 통증을 호소하는 경우가 있으며 조기 포만감, 오심, 구
역 등이 나타날 수 있다. 크기가 큰 혈관종의 경우 혈관종 내 혈전 형성으로 내부에 부분 경색, 괴사와
A B C
A B C

2012년 대한간학회 춘계 Single Topic Symposium
12
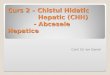
Figure 2. Dynamic contrast enhanced CT scan images before (A) and 2 years later (B) after radiofrequency ablation (RFA) shows markedly shrunked hemangioma after RFA.
통증도 발생 가능하다4. 혈관종의 크기가 갑자기 커지거나 크기가 큰 경우 자발 출혈이나 파열이 발생
할 수 있으며 혈복강이나 혈담 등의 양상으로 나타날 수 있다. 매우 드물지만 혈관종 내에서 혈소판의
응고 및 파괴로 인한 혈소판 감소증 및 파종성 혈관내 응고(Disseminated Intravascular Coagulation)을 동
반한 Kasabach-Merritt syndrome이 보고 되어 있다.5,6 혈관종은 편평한 내피세포로 이루어진 다양한 크기
의 혈관들로 구성되어 있고 내부에 섬유기질로 이루어진 실 같은 조직으로 분리되어 있다. 혈전이 흔히
관찰되며 주변조직과는 경계가 분명하나 일반적으로 캡슐은 관찰되지 않는다.
초음파에서 우연히 발견되는 경우가 대부분이며, 초음파상의 전형적인 소견은 경계가 분명한 고에코를
나타내며 내부는 균일한 영상을 나타낸다. 다른 소견으로는 간혹 후방음향증강(posterior acoustic enhancement)
을 보이는 경우가 있다. 주변의 저에코성 달무리는 나타나지 않는다. 초음파상 소견이 분명하지 않
을 때는 조영증강 컴퓨터 단층촬영, 조영증강 자기공명촬영 등을 시행할 수 있으며 최근에는 조영증강
초음파를 이용하여 진단을 내리고 있다.8 대부분의 전형적인 경우는 진단이 어렵지 않으나, 유경성
(pedunculated)의 양상이나, 미만성인 경우나 혈관션트와 동반되어 있는 비전형적인 경우는 진단이 쉽지
않으며, 특히 경화증(sclerosis) 변화가 동반된 경우는 다른 종양과 감별이 쉽지 않다. 경화증 변화는
섬유화에 의하여 혈관내부가 막히는 상태를 의미하며, 완전히 진행된 경우에는 조직 검사로도 진단이
쉽지 않아 주변의 작은 혈관들을 확인 가능한 경우에만 진단이 가능하다.7
혈관종의 치료는 아직 정립되어 있지 않다. 대부분의 무증상 혈관종은 경과 관찰 외 별다른 처치가
필요하지 않다. 증상이 있거나 크기가 증가하는 경우, 악성 종양과 감별이 되지 않는 경우 치료를 고려
할 수 있다. 고식적으로 개복 수술을 통한 간절제가 간혈관종의 기본 치료 방법으로 알려져 있다. 이외
에 스테로이드를 이용한 약물적 치료부터 방사선 치료, 색전술 등의 치료가 보고 되었으나 불완전한
치료 효과 및 합병증으로 인해 채택되지 않고 있다.9 최근 혈관종의 파열 및 다장기 부전을 동반한
A B

탁원영❚Benign Liver Mass Lesions: Vascular Lesions
13
Kasabach-Merritt syndrome 환자에서 간 이식술을 시행하여 성공적으로 치료한 경우도 보고 되어 있다.10
최근 비침습적 치료로서 간세포암의 국소 치료로 널리 시행되고 있는 고주파 열소작술에 의한 혈관종
의 치료가 소개되어 4 cm 이상의 증상이 있거나 크기가 증가하는 혈관종을 고주파열 소작술로 효과적
으로 치료한 결과가 보고 되었다. 향후 침습적인 개복수술의 부담감, 합병증, 안정성 등을 고려할 때 일
부 환자에서 비침습적이고 안전한 고주파 열소작술을 개복 수술의 대안으로 고려할 수 있다.11,12
Budd-Chiari 증후군
Budd-Chiari 증후군은 결절성 재생증식(nodular regenerative hyperplasia), 거대 재생결절(macroregenerative
nodule)이 흔하게 관찰되는데 간세포암과 감별이 필요하다.13 Budd-Chiari 증후군은 간세정맥과 하대정맥
사이에 발생한 간정맥 혈류의 폐쇄로 발생하며 원발성인 경우와 이차적인 경우를 모두 포함한다. 임상
양상은 폐쇄 정도 및 발생 기간에 따라 무증상에서부터 드물지만 전격성 간염의 형태까지 다양하다. 간
정맥 혈류가 폐쇄되면 굴모양혈관(sinusoid) 내압의 증가, 문맥혈류의 감소, 중심소엽의 울혈, 간종대가
나타나며, 간정맥 혈류 폐쇄의 급성도에 따라 간세포의 괴사가 발생하고 복수, 통증, 황달을 나타낸다.
이러한 질병의 심한 정도와 유병기간에 따라 전격형, 급성형, 아급성형, 만성형으로 분류한다. 전격성은
황달 발생 8주 이내 간성뇌증이 나타나며 복수와 신부전을 동반한다. 급성형은 짧은 기간에 상복부 통
증, 간종대, 복수, 황달, 신부전이 나타나며,14 아급성형은 곁맥관의 발달로 급성형에 비해 점진적으로
발생하며, 복수와 간괴사가 경하다. 만성형은 2개월 이상에 걸쳐 서서히 복수가 발생하고 혈청 ALT치
는 정상이거나 경하게 증가하고 황달은 없는 경우가 많다.15
Budd-Chiari 증후군의 영상학적 소견은 질병의 단계에 따라 다양하게 나타날 수 있다. 급성형의 경우
CT의 비조영 사진에서 넓은 저음영의 간을 보이지만 간의 형태는 유지하고 있으며 하대정맥과 간정
맥이 좁아져 있는 것을 볼 수 있다. 만성형의 경우는 간의 울혈과 비대, 특히 미상엽을 중심으로 부채모
양의 영역에 조영증강과 비대가 나타나고 주변부는 오히려 위축되는 등의 모양의 변형이 일어난다. 그
리고 간정맥과 하대정맥은 혈류가 감소하여 비조영 CT에서는 나타나지 않는 경우가 많다. 조영증강 CT
및 혈관조영술에서는 하대정맥과 간정맥의 미세한 곁순환의 형성으로 거미줄 모양을 보이는 것이 특징
이다. 그리고 간의 비균질 조영을 보이는데 만성형에서 잘 더 나타나는 소견이다.16 큰 재생성 결절이
생기기도 하는데 이는 간의 관류가 감소하여 간의 비정상적, 국소적 위축이 발생하는데 이에 대한 보상
으로 혈액공급이 원활한 부위가 증식하여 국소 재생결절이 발생하는 것으로 생각된다. 이는 간세포
암과 감별이 필요하다. 크기는 대개 1-4 cm이다. 거대재생결절은 영상검사나 병리학적으로 국소결절과
형성(focal nodular hyperplasia)과 유사한 소견을 보인다. 이 결절은 조영증강 CT에서 동맥기에 균질하게

2012년 대한간학회 춘계 Single Topic Symposium
14
조영증강 되며 간문맥기에도 약간 조영증강 되어있어 간문맥기에 washout되는 간세포암과 감별이 가능
하다. CT로 구별이 어려울 경우는 조직검사를 시행하여 감별 진단 할 수 있다.17
치료는 내과적 치료와 간세포 괴사를 방지하기 위해 간정맥 혈류의 폐쇄를 완화시키는 조치, 간이식
등이 있다. 간정맥이 완전히 폐쇄되지 않았으면 진행을 막기 위해 항응고제를 사용하고 원인요소를 교
정한다. 위장관 출혈이나 복수 등에 대한 예방과 치료가 필요하다. 간괴사가 진행하지 않고 협착부위가
짧을 때는 경피 혈관 성형술을 실시 할 수 있으며 스텐트를 삽입하기도 한다. 그리고 심한 문맥압항진
증을 치료하기 위해 경정맥경유간내문맥전신순환션트(transjugular intrahepatic portosystemic shunt)이나 수
술적 치료로 문맥과 대정맥 사이를 우회 연결하는 션트술을 시행한다. 심한 간부전이 있으면 간이식을
고려한다.
간동맥-문맥 단락(Arterioportal Shunt)
간동맥가지와 간문맥 사이에 단락이 생기면 굴모양혈관이나 주변 담도주위 세정맥에서 동맥혈류가
문맥으로 흐르는 국소이상으로 나타나게 된다. 작은 비종양성 간동맥-문맥 단락이 간실질에 국소적으로
형성되면 간암과 구분하기 어려운 경우가 있으며 종양이 문맥과 간정맥의 혈류장애를 유발하면 병변의
범위를 과대평가 할 수 있으므로 이에 대한 이해가 중요하다.18,19 간동맥-문맥 단락은 외상 후 발생하며
이러한 이상은 조직손상, 간조직 검사, PTBD 같은 기구를 이용한 시술 이후에 주로 발생한다.20 이외에
도 간경변에서 작은 간동맥 문맥 단락이 저절로 생기기도 하고 사라지기도 하나 발생원인이 명확하지
않다. 혈관이 풍부한 간세포암, 혈관종이 관련이 있고 드물지만 간동맥의 동맥류가 간문맥내로 파열로
도 발생할 수 있다.
이 병변은 임상적으로 의미는 간세포암과의 감별진단이다. 진단은 조영증강 CT를 통하여 진단 할 수
있다. 동맥기에는 가장자리에 위치한 작고, 비구형으로 조영되는 병변으로 나타나며 문맥초기부터 지연
기까지 주변 간실질과 같은 조영정도를 보이게 된다. 쐐기 모양이 많으며 일시적으로 조영되어 나타
나는 특징이 있으나 작은 간세포암과 감별이 어려운 경우는 시간 간격을 두고 CT를 반복해볼 수도
있다.21
유전성출혈모세혈관확장증(Hereditary Hemorrhagic Telangiectasia)
유전성출혈모세혈관확장증은 transforming growth factor에 결합하는 단백의 이상으로 혈관이형성이 생겨
말초 혈관확장과 같은 이상형태를 나타내는 질환이다. 유병율은 인구 10만명당 10명에서 20명 정도로

탁원영❚Benign Liver Mass Lesions: Vascular Lesions
15
발생하는 것으로 알려져 있으며 상염색체 우성 유전으로 남녀간의 발생율의 차이는 없다. 임상양상은
코피, 객혈 등이 주로 흔한 증상이나 간내 병변은 환자의 74%정도에서 가지고 있고, 간내 병변은 진단
되고 10년에서 20년 정도 지난 이후 발생한다. 간내 병변을 가진 환자에서 동맥과 정맥, 문맥션트 등으
로 인한 과혈류로 high output 심부전이 발생한다. 다른 합병증으로는 간외 단락, 문맥고혈압, 간성뇌병
증, 담도허혈, 담도염, 간부전 등이 발생할 수 있다. 확장되고 삐뚤어진 간내외 혈관상으로 인하여 CT
소견은 동맥기에 모자이크처럼 지저분한 조영을 보여준다. 그리고 문맥기와 정맥기에는 조기에 조영되
는 양상을 보여준다. 그리고 혈관덩어리로 인한 담도의 확장이 생기기도 한다.22,23
이 질환을 다른 병변과 감별하는데 가장 중요한 요인은 정확하고 자세한 병력청취이다. 가족력을 대
부분 갖고 있으며 잦은 코피 등의 증상을 자세히 확인하여야 한다. 치료는 환자의 증상에 따라 다르며
대부분은 수혈과 철분공급만으로 충분하지만 드문 경우에 coil을 이용한 간동맥 색전술이나 수술적 결
찰 그리고 간이식이 필요한 경우도 있다.24,25
간자색반병(Peliosis hepatis)
간자색반병은 간굴모양혈관의 확장과 1mm부터 수 센티미터에 이르는 다양한 크기의 다수의 소강
(lacuna)을 형성하는 드문 질환이다. 소강내에는 혈액이 풍부하다. 원인은 정확히 알려져 있지 않으며,
결핵, 나병과 같은 만성 소모성 질환, 간세포암과 같은 다양한 암, AIDS, 경구용피임약, tamoxifen,
azathioprine 과 같은 약제들, 신이식, 심장이식, 독소노출 등에 의해 2차적으로 발생할 수 있다.26 발생율
과 유병율은 잘 알려져 있지 않고 우연히 발견되는 경우가 대부분이다. 자연 경과에 대해서도 잘 알려
져 있지 않으나 대개 무증상이며 원인 약제를 중단하거나 감염에서 회복되면 자연적으로 퇴행할 수 있
다. 합병증으로 간부전, 담즙 정체, 간문맥 항진증을 유발할 수 있으며, 간표면에서 파열되어 복강내 출
혈을 야기하면 즉각적인 색전술 및 수술적 치료가 필요하다.27
비조영증강 CT에서 병변은 전형적으로 음영감소 소견으로 나타나며 조영증강 CT에서는 다양한 형
태의 조영증강으로 나타난다. 동맥기에서의 병변은 주변 간실질에 비교하여 음영이 점차 증가되며, 구
심성으로 조영이 되며, 전체적으로 조영이 되거나 초기에 구모양의 혈관으로 조영되거나 문맥기에 원
심성의 조영을 보인다. 지연기에는 미만성으로 증가된 음영증가를 보일 수 있다. 1cm 미만의 작은 병변
의 경우 비조영 영상 및 조영증강 영상에서 나타나지 않을 수 있고 혈전이 생기면 전이암이나 농양과
같은 조영이 되지 않는 소견을 보인다.27,28
간자색반병은 혈관종과 과다혈관 전이암(hypervascular metastasis)과 감별을 하여야 하며 과다혈관 전
이암은 전형적으로 문맥기에 간실질에 비해 조영감소나 비슷한 조영정도를 보이며 혈관종은 특징적으

2012년 대한간학회 춘계 Single Topic Symposium
16
로 동맥기에서 부터 구형의 조영증강이 구심성으로 진행하는 양상을 보이고 주위 혈관들에 종괴효과를
보인다. 간자색반병은 천자를 피하여야 하며, 간농양과 구별이 중요한데 간농양은 전형적으로 여러 중
격으로 구성되어 있으며, 조영증강 없이 포도송이 모양을 보이는 것이 특징이다.28
참고문헌
1. Porayko MK, Choudhary C. Benign Neoplasms of the Liver. Current treatment options in gastroenterology.
2001;4(6):479-91.
2. Mathieu D, Zafrani ES, Anglade MC, Dhumeaux D. Association of focal nodular hyperplasia and hepatic
hemangioma. Gastroenterology. 1989;97(1):154-7.
3. Bahirwani R, Reddy KR. Review article: the evaluation of solitary liver masses. Alimentary pharmacology &
therapeutics. 2008;28(8):953-65.
4. Jhaveri KS, Vlachou PA, Guindi M, Fischer S, Khalili K, Cleary SP, et al. Association of hepatic
hemangiomatosis with giant cavernous hemangioma in the adult population: prevalence, imaging appearance,
and relevance. AJR American journal of roentgenology. 2011;196(4):809-15.
5. Concejero AM, Chen CL, Chen TY, Eng HL, Kuo FY. Giant cavernous hemangioma of the liver with
coagulopathy: adult Kasabach-Merritt syndrome. Surgery. 2009;145(2):245-7.
6. Aslan A, Meyer Zu Vilsendorf A, Kleine M, Bredt M, Bektas H. Adult Kasabach-Merritt Syndrome due to
Hepatic Giant Hemangioma. Case reports in gastroenterology. 2009;3(3):306-12.
7. Aibe H, Hondo H, Kuroiwa T, Yoshimitsu K, Irie H, Tajima T, et al. Sclerosed hemangioma of the liver.
Abdominal imaging. 2001;26(5):496-9.
8. Bartolotta TV, Midiri M, Quaia E, Bertolotto M, Galia M, Cademartiri F, et al. Benign focal liver lesions:
spectrum of findings on SonoVue-enhanced pulse-inversion ultrasonography. European radiology.
2005;15(8):1643-9.
9. Aksenov IV, Fedorchenko AN. [Hepatic hemangioma: the choice of treatment]. Khirurgiia. 2010;(6):40-2.
10. Kumashiro Y, Kasahara M, Nomoto K, Kawai M, Sasaki K, Kiuchi T, et al. Living donor liver transplantation
for giant hepatic hemangioma with Kasabach-Merritt syndrome with a posterior segment graft. Liver
transplantation : official publication of the American Association for the Study of Liver Diseases and the
International Liver Transplantation Society. 2002;8(8):721-4.
11. Park SY, Tak WY, Jung MK, Jeon SW, Cho CM, Kweon YO, et al. Symptomatic-enlarging hepatic hemangiomas
are effectively treated by percutaneous ultrasonography-guided radiofrequency ablation. Journal of hepatology.
2011;54(3):559-65.
12. Tak WY, Park SY, Jeon SW, Cho CM, Kweon YO, Kim SK, et al. Ultrasonography-guided percutaneous
radiofrequency ablation for treatment of a huge symptomatic hepatic cavernous hemangioma. Journal of
clinical gastroenterology. 2006;40(2):167-70.
13. Fox MA, Fox JA, Davies MH. Budd-Chiari syndrome-a review of the diagnosis and management. Acute
medicine. 2011;10(1):5-9.
14. Loomes DE, Chang A, Webber D, Scudamore CH, Yoshida EM. Acute Budd-Chiari syndrome. Canadian journal
of gastroenterology = Journal canadien de gastroenterologie. 2011;25(6):302-3.
15. Mukund A, Gamanagatti S. Imaging and interventions in Budd-Chiari syndrome. World journal of radiology.
2011;3(7):169-77.

탁원영❚Benign Liver Mass Lesions: Vascular Lesions
17
16. Kikuchi Y, Yoshida H, Mamada Y, Taniai N, Mineta S, Yoshioka M, et al. Huge caudate lobe of the liver due to
Budd-Chiari syndrome. Journal of Nihon Medical School = Nihon Ika Daigaku zasshi. 2010;77(6):328-32.
17. Luo YK, Li JL, Wang YX, Wang ZL, Xu JH, Tang J, et al. [Clinical value of contrast-enhanced ultrasound in the
diagnosis of Budd-Chiari syndrome with inferior vena cava obstruction]. Zhongguo yi xue ke xue yuan xue bao
Acta Academiae Medicinae Sinicae. 2010;32(4):470-2.
18. Han JK, Kim SH. [Arterioportal shunt mimicking hepatocellular carcinoma]. The Korean journal of hepatology.
2004;10(1):78-80.
19. Byun JH, Kim TK, Lee CW, Lee JK, Kim AY, Kim PN, et al. Arterioportal shunt: prevalence in small
hemangiomas versus that in hepatocellular carcinomas 3 cm or smaller at two-phase helical CT. Radiology.
2004;232(2):354-60.
20. Maes J, D'Archambeau O, Snoeckx A, Op de Beeck B, Voormolen M, Parizel PM. Post-traumatic hepatic arterial
pseudoaneurysm and arterioportal shunt. JBR-BTR. 2010;93(4):189-92.
21. Luo MY, Shan H, Jiang ZB, Liang WW, Zhang JS, Li LF. Capability of multidetector CT to diagnose
hepatocellular carcinoma-associated arterioportal shunt. World journal of gastroenterology : WJG.
2005;11(17):2666-9.
22. Piskorz MM, Waldbaum C, Volpacchio M, Sorda J. [Liver involvement in hereditary hemorrhagic
telangiectasia]. Acta gastroenterologica Latinoamericana. 2011;41(3):225-9.
23. Senzolo M, Riggio O, Primignani M. Vascular disorders of the liver: recommendations from the Italian
Association for the Study of the Liver (AISF) ad hoc committee. Digestive and liver disease : official journal of
the Italian Society of Gastroenterology and the Italian Association for the Study of the Liver. 2011;43(7):503-14.
24. Olitsky SE. Hereditary hemorrhagic telangiectasia: diagnosis and management. American family physician.
2010;82(7):785-90.
25. McDonald J, Bayrak-Toydemir P, Pyeritz RE. Hereditary hemorrhagic telangiectasia: an overview of diagnosis,
management, and pathogenesis. Genetics in medicine : official journal of the American College of Medical
Genetics. 2011;13(7):607-16.
26. Nougaret S, Aufort S, Ramos J, Pierredon MA, Delhom E, Colleau J, et al. [Hepatic peliosis: an entity to
remember]. Journal de radiologie. 2009;90(11 Pt 1):1745-9.
27. Lee WJ. [Peliosis hepatis]. The Korean journal of hepatology. 2009;15(3):379-82.
28. Verswijvel G, Janssens F, Colla P, Mampaey S, Verhelst H, Van Eycken P, et al. Peliosis hepatis presenting as a
multifocal hepatic pseudotumor: MR findings in two cases. European radiology. 2003;13 Suppl 4:L40-4.


![Hepatic angiosarcoma with an associated focal nodular ... · vascular channels [1,2]. Focal nodular hyperplasia (FNH), on the other hand, is a benign hepatic lesion displaying hepatocytic](https://img.pdfslide.tips/doc/110x75/5f05ab797e708231d4141d25/hepatic-angiosarcoma-with-an-associated-focal-nodular-vascular-channels-12.jpg)