Pearls and Pitfalls In the Management of Dengue Hemorrhagic
Fever
1
Pearls and pitfalls in DHF management
Dr. Aung Kyi WynnSenior consultant pediatrician
DENGUE2DefinitionAcute illness caused by four serotypes of
dengue virus and characterized by a hemorrhagic diathesis and a
tendency to develop a shock syndrome (dengue shock syndrome DSS)
that may be fatal.Thrombocytopenia with concurrent
haemoconcentration is a constant findings.3Causal Agent Dengue
virus = Serotype 1- 4Infection with one type gives lifelong
immunity for this type, but partial immunity for other types45
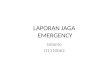
VectorTransmitted by Aedes aegypti.Bite during daytimeGrow in
clear water
6
Countries/areas at risk of dengue transmission, 2008
7
(8-12daysvirus replicates)(3-14days avr 4-6 daysvirus
replicates)Principal reservoir hostVirus multiplies in midgut,
brain, body fat, salivary glandsMan-Mosquitoe-Man cycle(about 5
days)(about 5 days)9Awareness of DHFPearls - Aware and Recognize
DHF
Pitfall Failure to get diagnosis of DHFCRITERIA FOR
DENGUEProbable dengue-live in /travel to dengue endemic area.-Fever
and 2 of the following criteria:Nausea, vomitingRashAches and
painsTourniquet test positiveLeukopeniaAny warning sign
Laboratory-confirmed dengue(important when no sign of plasma
leakage)
10Use of NS 1 AntigenNS 1 rapid tests (eg. SD BIOLINE) had
similar diagnostic sensitivities ( 61.6% ) compared to RT PCR (
62.4%) in confirmed casesBoth tests have 100% specificSensitivity
become significantly improved (83.7%)when NS 1 and/or Ig G and/or
IgM was positive.
Use of NS 1 Antigensignificantly more sensitive for Primary than
secondary Dengue.Associated with underlying viraemia
(Vianney Tricou et,al at Oxford University Clinical Research
Unit)
1314
USG findingsHepatomegaly 87.5 %Pericholecystic
oedema83%Gallbladder wall thickening80%Ascites74%Pleural effusion
(Rt) 44%Splenomegaly3.4%Pleural effusion (Bilateral)2%(on third and
fourth day of fever)
15CRITERIA FOR SEVERE DENGUE
Severe plasma leakageleading to:Shock (DSS)Fluid accumulation
with respiratory distress
Severe bleedingas evaluated by clinician
Severe organ involvementLiver: AST or ALT 1000CNS: Impaired
consciousnessHeart and other organs
1617
Bleeding in mesentry and intestinal wall18Many faces of DHFDHF
with GEDHF with Asthmatic Bronchitis DHF with Appendicitis DHF with
extreme drowsiness DHF with Hepatitis DHF with acute intravascular
hemolysis 19&moDwkdif;wGif ? zsm;emvQif
aoG;vGefwkyfauG;rSwf/20HESS TEST Pearls Proper doing and
interpretation
Pitfall Wrong methods and interpretation21HESS TESTAppropriate
cuff Exact 5 minutes Proper method Wait till the bluish
discoloration gone 1 square inch square at maximum area
22HESS TEST - InterpretationNot any spot is positive > 20
positive 10-20 Equivocal < 10 Negative Be aware of false (+)
23Positive tourniquet test
Febrile, critical and recovery phases in dengue
24
25Dengue case classification and level of severity
27
A stepwise approach to the management of dengue
2829DETECTION OF SHOCK Pearls Predict or Detect in Time
Pitfall Failure to recognize shock 30DETECTION OF SHOCKWarn
parents that fall in temperature is more important than fever
Afebrile with improvement or deterioration
Proper written instruction 31DETECTION OF SHOCKAt the time when
the temperature drops i.e., from day 3 onwards with worsening of
general condition In other diseases, with the drop in temperature,
the child feels better, eats better, is alert, up and go about and
can play wherelse in DSS, it is reversed32
WHY DETECTION OF SHOCK IS IMPORTANTStagnant acidemia promote
occurrence and enhanced severity of DIC33tzsm;uspOf? rvef;vQif
tpOfowdcsyf/34WHEN TO ADMITPearls Proper admission
Pitfall Too early or late admission
WHEN TO ADMITDangerous mistake DHF patients need admission only
when develop shock
Admission Criteria Patients with warning signs Those with
co-exisitng conditions that may make dengue or its management more
complicated (infancy, obesity, diabetes mellitus, renal failure,
chronic haemolytic diseases)
Admission criteriaSigns and symptoms related to hypotension
(possible plasma leakage)
Dehydrated patient, unable to tolerate oral fluidsGiddiness or
postural hypotensionProfuse perspiration, fainting, prostration
during defervescenceHypotension or cold extremities
37Admission criteriaBleeding spontaneous bleeding independent of
the platelet count
Organ impairment Renal, hepatic, neurological or cardiac
enlarged, tender liver, although not yet in shock chest pain or
respiratory distress, cyanosis
38Admission criteriaFindings through further investigations
Rising haematocritPleural effusion, ascites or asymptomatic
gall-bladder thickening
39Admission criteriaCo-existing conditionsPregnancyCo-morbid
conditions, such as diabetes mellitus, hypertension, peptic ulcer,
haemolytic anemias and othersOverweight or obese (rapid venous
access difficult in emergency)Infancy or old age
40Admission criteriaSocial circumstancesLiving aloneLiving far
from health facilityWithout reliable means of transport
4142WHERE TO ADMIT Pearls Close monitoring and Titration
Pitfall Inadequate monitoring & Inadequate experience
Management according to groups AC
Group A patients who may be sent homeGroup B patients who should
be referred for in-hospital managementGroup C patients who require
emergency treatment and urgent referral when they have severe
dengue
43Group A (who may be sent home)Patients who do not have warning
signs ORwho are able to tolerate adequate volumes of oral fluids
and pass urine at least once every six hours do not have any of the
warning signs particularly when fever subsides
44
Group B(Referred for in-hospital care)
Patients with any of the following features:co-existing
conditions such as pregnancy, infancy, old age, diabetes mellitus,
renal failuresocial circumstances such as living alone, living far
from hospital OR Existing warning signs
45
Group C(Require emergency treatment)
Patients with any of the following features:severe plasma
leakage with shock and/or fluid accumulation with respiratory
distresssevere bleedingsevere organ impairment
46Group A patientTreatment
Advice for:adequate bed restadequate fluid intakeParacetamol,
3gram maximum per day in adults and accordingly in
children.(10mg/dose)
Patients with stable HCT can be sent home
47Group A patientMonitoring
Daily review for disease progression:decreasing white blood cell
countdefervescencewarning signs (until out of critical period).
Advice for immediate return to hospital if development of any
warning signs, andwritten advice for management (e.g. home care
card for dengue)4849Use of Drugs Pearls Use of appropriate Drugs
and avoidance of unnecessary and dangerous drugs
Pitfalls Use of unnecessary and dangerous drugs50Use of DrugsUse
Paracetamol only as antipyretic
Not need to have food
Avoid all others NSAID No Nimuslide, No Ibuprofen 51OTHER DRUGS
ORS or Any fluid and Salt
Avoid unusual large amount especially in older children
? Antacids & Ranitidine
Group B(with co-existing conditions or social circumstances)
Treatment
Encouragement for oral fluidsIf not tolerated, start intravenous
fluid therapy 0.9% saline or Ringers Lactate at maintenance
rate
52Group B(with co-existing conditions or social
circumstances)Monitor:temperature patternvolume of fluid intake and
lossesurine output (volume and frequency)warning signsHCT, white
blood cell and platelet counts
53Group B(with existing warning signs)Treatment
Obtain reference HCT before fluid therapyGive isotonic solutions
such as 0.9 % saline, Ringers LactateStart with 57 ml/kg/hr for 12
hours, then reduce to 35 ml/kg/hr for 24 hr, and then reduce to 23
ml/kg/hr or less according to clinical response
54Group B(with existing warning signs)Reassess clinical status
and repeat HCT:
if HCT remains the same or rises only minimally -> continue
with 23 ml/kg/ hr for another 24 hours; if worsening of vital signs
and rapidly rising HCT -> increase rate to 510 ml/kg/hr for 12
hours
5556
49 & 50
Group B(with existing warning signs)Reassess clinical status,
repeat HCT and review fluid infusion rates accordingly:
reduce intravenous fluids gradually when the rate of plasma
leakage decreases towards the end of the critical phase
This is indicated by:adequate urine output and/or fluid
intakeHCT decreases below the baseline value in a stable
patient
57Group B (with existing warning signs)Monitor
vital signs and peripheral perfusion (14 hourly) until patient
is out of critical phaseurine output (46 hourly)HCT (before and
after fluid replacement, then 612 hourly)blood glucoseother organ
functions (renal profile, liver profile, coagulation profile, as
indicated)
58Pearls and Pitfalls In the Management of ShockDSS is
hypovolemic shock due to plasma leakage:Volume replacement with
isotonic salt solutions, plasma, plasma substitute, for the period
of plasma leakage(24 - 48hrs)is life-saving5960Pearls and Pitfalls
in the Management of ShockVolume replacement should be monitored
according to the rate of plasma leakage (PCV, vital signs, urine
output) to avoid fluid over loadThe rate of leakage is more rapid
in 1st 6 12 hrs Group C(Require emergency treatment)
Treatment of compensated shock
Start IV fluid resuscitation with isotonic crystalloid solutions
at 510 ml/kg/hr over 1 hourReassess patients condition
61Group C(Require emergency treatment)
Treatment of compensated shock
If patient improves:IV fluids should be reduced gradually to 57
ml/kg/hr for 12 hours, then to 35 ml/kg/hr for 24 hours,then to 2-3
ml/kg/hr for 24 hours and then reduced further depending on
haemodynamic status;IV fluids can be maintained for up to 2448
hours
62Group C(Require emergency treatment)Treatment of compensated
shock
If patient is still unstable:
check HCT after 1st bolus; if HCT increases/still high
(>50%), repeat a 2nd bolus of crystalloid solution at 1020
ml/kg/hr for 1hr if there is improvement after 2nd bolus, reduce
rate to 710 ml/kg/hr for 12 hrs and continue to reduce as aboveif
HCT decreases, this indicates bleeding and need to cross-match and
transfuse blood as soon as possible
63Group C(Require emergency treatment)Treatment of hypotensive
shock
Initiate IV fluid resuscitation with crystalloid or colloid
solution at 20 ml/kg as a bolus for 15 minutes
-If patient improves:give a crystalloid/colloid solution of 10
ml/kg/hr for 1 hr, then reduce gradually as above
64Group CTreatment of hypotensive shock
-If patient is still unstable:review the HCT taken before the
1st bolus;if HCT was low (50%), continue colloid infusion at 1020
ml/kg as a 3rd bolus over 1 hr,then reduce to 710 ml/kg/h 12 hr,
then change back to crystalloid solution and reduce rate as
above
66Group C(Require emergency treatment)Treatment of haemorrhagic
complicationsGive 510 ml/kg of fresh packed red cells or 1020 ml/kg
of fresh whole blood
6768
69Stagnant acidemia promote occurrence and enchanced severity of
DIC
PRP transfusion as prophylaxis for bleeding in all shock cases
is not recommended
Pearls and Pitfalls In the Management of Shock ( contd)Pearls
and Pitfalls In the Management of Shock ( contd)There are abnormal
haemostatic changes that potentiate bleeding in DHF/DSSSevere
bleeding ( may be concealed ) often occurs in cases with prolonged
shock and further perpetuates shock
7071Refractory shock despite adequate volume replacement and a
drop in PCV ( at any rate e.g. from 50 % to 40 % ) indicates
significant bleeding and a need for FWB transfusion ( 10 ml/kg/dose
)Pearls and Pitfalls In the Management of Shock ( contd)72Major
contributory factor to the high mortality ratefailure to recognize
internal bleedingover transfusion with crystalloid and/or plasma
fluid instead of bloodPearls and Pitfalls In the Management of
Shock ( contd)73Pitfall------------ Too much rely on platelet count
and PCVPearl------------ In conjunction with hemodynamic Status
Pearls and Pitfalls In the Management of Shock ( contd)Key
decisionsWhen to give blood?
When to stop IV fluid or give diuretics?IV fluid therapyNarrow
therapeutic indexTimelyAppropriate volumeRateAppropriate
typeAppropriate duration(Fluid replacement-
40-60ml/kg)7576PREVENTION Pearls - Correct prioritization
Pitfall Just for show 77PREVENTIONLarva control more important
than killing adult mosquitoes
School, Tuition, Nursery, Day care centre
Whole wards or villages
Health more important than Education
DHF more important than lung diseases 78Prevention (contd)Key
Container should not be in the vicinity where 3 -8 yrs old children
are aggregatede.g. primary school, private tuition, day- care
centreControl measures should be emphasized in these
areasaoG;vGefwkyfauG;tE&m,fuif;*gxm&moDwkdif;wGif ?
zsm;emvQif aoG;vGefwkyfauG;rSwf/tzsm;uspOf? rvef;vQif
tpOfowdcsyf/
7980CONCLUSIONSIt is a preventable and treatable disease
Awareness of clinical features, early and effective treatment of
shock, appropriate management with close monitoring can save the
lives of patients
Effective preventative measures will reduce the burden of DHF
FAQSSecondary dengue infection Vs virulence theoryRole of
corticosteroidTwo attacks of dengue in the same season?Importance
of D/C diagnosis81FAQS cont.Role of OPD MORole of ward MORole of
abateDengue vaccine
82
83Thank you