-
子宮頸癌Cervical Cancer
三 軍 總 醫 院
余 慕 賢
-
96 台灣女性 10 大癌症 (發生率排序) 乳癌 7,502 66.10
結腸癌 4,471 39.39
肺癌 3,161 27.85
肝癌 2,900 25.55
子宮頸癌 1,749 15.41
甲狀腺癌 1,407 12.40
胃癌 1,301 11.46
子宮體癌 1,165 10.26
皮膚癌 1,113 9.81
卵巢癌 1,047 9.23
-
87/98 台灣女性主要癌症死亡原因
肺癌 1708/2615 16.06/22.8
肝癌 1377/2292 12.95/20.0
直腸結腸癌 1227/1969 11.54/17.2
乳癌 995/1588 9.4/13.9
胃癌 812/825 7.6/7.2
子宮頸癌 1017/657 9.6/5.7
卵巢癌 273/435 2.6/3.8
-
Human Papillomavirus▪ >200 types identified
▪ 30-40 anogenital▪ 15-20 oncogenic types,
including 16, 18, 31, 33, 35,39, 45, 51, 52, 58-HPV 16 (54%) and
HPV 18(13%) account for the majorityof worldwide cervical
cancers
▪ Nononcogenic types include:6, 11, 40, 42, 43, 44, 54-HPV 6 and
11 are most often associated with external genital warts
-
Risk Factors for HPV Infection
Women▪ Young age(peak age
group 20-24 y/o)▪ Lifetime number of sex
partners▪ Early age of first sexual
intercourse▪ Male partner sexual
behavior▪ Smoking▪ Oral contraceptive use▪ Uncircumcised
male
partners
Men▪ Young age(peak age
group 25-29 y/o)▪ Lifetime unmber of sex
partners▪ Being uncircumcised
-
Natural History of HPV Infectionin Young Women
Rotgers University, New Jersey Study
• The cumulative 24/36-month incidence: 34/43%
• The median duration of HPV infection: 8 months
• Only 9% remained infected by 24 months after the incident
infection
• Probability of acquiring a subsequent infection with a
different HPV type within 24 months of the initial infection:
70%
Ho et al., 1998 (N Engl J Med 338:423-428)
Ho et al., 2002 (J Infect Dis 186:737-742)
-
HPV Clearance▪ In women 15-25 years of age, ~80% of HPV
infections are transientGradual development of cell-mediated
immune
response presumed mechanism
▪ In a study of 608 college women, 70% of new HPV infection
cleared within 1 year and 91 % within 2 years
Median duation of infection = 8 months
Certain HPV types are more likely to persist
(eg, HPV 16 and HPV 18)
-
HPV Persistence
▪ Persistent infection: Detection of same HPV type two or more
times over several months to 1 year
▪ Widely accepted that persistence of high-risk types of HPV is
crucial for development of cervical precancer and cancer
▪ Infection with multiple HPV types▪ Immune suppression▪
Currently, there are no antiviral available to
treat the underlying HPV infection
-
HPV Disease Progression
▪ In a study of women(N=899) 13-22 years of age positive for HPV
DNA
▪ 260(29%) were diagnosed with LSIL by cytology
▪ Probability of LSIL regression61% at 12 months’ follow up
91% at 36 months’ follow up
▪ Probability of progression to HSIL = 3%
Moscicki 2004
-
人類乳突病毒( HPV)
超過 200 型的 HPV,96 種確定會感染人類
HPV 可分為高危險性及低危險性兩大類型
性行為是 HPV 感染主要的傳染途徑
61% 於一年內清除; 91% 三年內清除
80% 的感染是短暫的
平均感染期間為 8 個月
HPV 16,18 較易持續感染
-
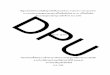
Cervical Intraepithelial Neoplasia
Normal LSIL HSIL Invasion
Metastasis
CIN1 CIN2 CIN3
-
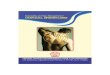
0–1 Year 0–5 Years 1–20 Years
子宮頸癌
HPV 感染清除YU2009
持續感染
人類乳突病毒與子宮頸癌
CIN1
CIN2/3
HPV
子宮頸癌
-
篩檢-1 首次抹片結果為難以判讀者,於6個月內再次接受抹片檢查的比率。
篩檢-2a 首次抹片結果為4(ASCUS)者,於6個月內已追蹤的比率。
篩檢-2b 首次抹片結果為6,7(CIN 1) 者,於6個月內已追蹤的比率。
篩檢-3a1 首次抹片檢查結果為8-11(CIN2,3),16(ASC-HSIL),17(HSIL)者,於2
個月內接受陰道鏡檢查的比率。
篩檢-3a2 首次抹片檢查結果為8-11(CIN2,3),16(ASC-HSIL),17(HSIL)者,於2
個月內接受切片檢查的比率。
篩檢-3b1 首次抹片檢查結果為5(AGCUS),15AGC-N),18(AIS)者,於2 個月內接受陰道鏡檢查的比率。
篩檢3-b2 首次抹片檢查結果為5(AGCUS),15AGC-N),18(AIS)者,於2 個月內接受切片檢查的比率。
篩檢-4a
首次抹片結果為16(ASC-HSIL)者,於2個月內其組織病理檢查結果亦為03,04,05,07-10,12的比率。
篩檢-4b
首次抹片結果為8-11(CIN2,3)者,於2個月內其組織病理檢查結果亦為03,04,05,07-10,12的比率。
篩檢-5 首次抹片結果為首次8-13及5者,於6個月內於陰道鏡下實施切片的比率。
-
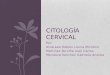
子宮頸癌前病變
正 常
低危險病變CIN1
高危險病變CIN2/3
-
治療-a 切片結果為04,05,07-10,12者,於2個月內接受治療的比率。
前驅病灶-1 子宮頸手術標本之組織病理檢查結果為HSIL的個案,在確定診斷時曾接受陰道鏡檢查的比率。
前驅病灶-2 診斷性子宮頸手術標本之組織病理檢查結果為HSIL之個案,於6個月內已接受適當處置的比率。
前驅病灶-3 診斷性子宮頸手術標本之組織病理檢查結果為HSIL之個案,於1年內未接受適當處置的比率。
前驅病灶-4 診斷性子宮頸手術標本之組織病理檢查結果為HSIL且接受治療之個案中,接受子宮全切除手術所占的比率。
前驅病灶-5
診斷性子宮頸手術標本之組織病理檢查結果為HSIL之50歲(含)以上個案,進行子宮頸錐狀手術時,同時接受子宮內頸搔刮取樣(ECC)人數的比率。
前驅病灶-6
診斷性子宮頸手術標本之組織病理檢查結果為HSIL之個案,以子宮頸錐狀手術為完整治療後,6個月內抹片追蹤的比率。
前驅病灶-7
診斷性子宮頸手術標本之組織病理檢查結果為HSIL之個案,以子宮全切除手術為完整治療後,6個月內抹片追蹤的比率。
前驅病灶-8
診斷性子宮頸手術標本之組織病理檢查結果為HSIL,且接受子宮全切除手術之個案中,術前曾接受子宮頸錐狀手術所占的比率。
-
0–1 Year 0–5 Years 1–20 Years
子宮頸癌
HPV 感染清除YU2009
持續感染
子宮頸癌疫苗預防癌前病變
CIN1
CIN2/3
HPV
子宮頸癌
-
子宮頸癌疫苗
誘出體內抗體以保護身體免於病毒感染
能夠在接種者體內,有效產生疫苗所涵蓋之HPV病毒型的抗體
對持續感染的預防效益可以達到100%
對由HPV病毒型所引起的子宮頸癌前病變產生100%的預防效果
後續追蹤已經確定效益至少可維持 8 年以上
治療性疫苗還處於人體試驗及前臨床試驗中。
-
Cervical cancer
• Early age at first intercourse
• Intercourse with multiple sexual partners
• HPV types: low risk(6, 11) vs high risk(16,
18, 45, 56 in 84% cervical cancer tissue; 31,
33, 35, 51, 52, 58 in 10% cervical cancer
tissue)
-
子宮頸侵襲癌
-
Radical hysterectomy
Bladder dysfunctions
Sensory loss, storing and voiding dysfunctions, urinary
incontinence, and detrusor instability
Anorectal mobidity dysorders
Constipation and related symptoms including dyschezia,
tenesmus, and the sensation of incomplete evacuation
Sexual dissatisfactionReduced sexual interest, and diminished
arousal
-
Surgical Endpoints1900-2000
Removal of tumor
and the area of
possible extension
(en bloc resection)
Reduce the
operative mortality
>2000
Reduce mortality
Balancing
prognosis and
morbidity
Improve
therapeutic efficacy
The shortest survival is operative death
-
Reducing surgery-related
pelvic nerve damage
Less radical surgery by reducing the extent of the
resected parametrial tissues.
Preserving the nerves without reducing the
radicality of surgery.
-
Radical Hysterectomy
-
RH after Neoadjuvant C/T
-
診療-1 原發子宮頸癌病人以同步化放療(CCRT)為主要治療時,病患有接受化療次數至少2次以上的比率。
診療-2 子宮頸癌病人接受體外放射治療,於治療期間有再度確認放療位置的比率。
診療-3 子宮頸癌病人治療後1年內充分追蹤的比率。
診療-4 非第 IV B期(FIGO期別)之子宮頸癌病人3個月內死亡的比率。
診療-5
子宮頸鱗狀上皮細胞癌,接受子宮切除手術(包括任一型的子宮切除手術及次全子宮切除手術),於365天內再接受骨盆放射線治療的比率。
-
Treatment of
Recurrent Cervical Cancer
Extent of disease
Site of recurrence
Disease free interval
Performance status
Comorbidities
-
EBRT(external bean)
Interstitial implant
Brachytherapy
CCRT in recurrent disease
IORT(intraoperative)
Salvage Treatment after Previous
Surgery: RT or CCRT
Monk BJ, et al Gyneco Oncol, 1994
Ijaz T, et al Gynecol Oncol 1998
Grigsby PW, et al IJGO 2004
-
Salvage Treatment after Definitive
Radiation Therapy: Radical Surgery
Radical hysterectomy
Pelvic exenteration
High acute and late complications
Recurrent central pelvic disease
Pelvic reconstruction
Berek JS , et al Gynecol Oncol 2005
Marnitz S, et al Gynecol Oncol 2006
-
Chemotherapy in advanced &
recurrent cervical cancer
Bonomi F et al, JCO 1985
Thigpen JT et al, Gynecol Oncol 1989
McGure III WP et al, JCO 1989
5 randomized trials in 1980 and 1990s
Platinum-based therapies most effective
Cisplatin more active than carboplatin
3 ways to increase response without prolonging survival
– Increase platinum dose
– Add ifosfamide to cisplatin
– Add paclitaxel to cisplatin
Single agent cisplatin 50 mg/m2 became the best choice
-
GOG 169
Cisplatin (50 mg/m2)
Day 1 of a 21-day cycle
6 cycles total
N = 134
Cisplatin (50 mg/m2)/Paclitaxel (135 mg/m2) **
Day 1 of a 21-day cycle
6 cycles total
N = 130
Patients with stage IVB,
recurrent, or persistent
squamous cell cervical
cancer
(N = 264*)
Quality of life (QoL) and tumor
measured after each cycle
*280 patients enrolled; 16 ineligible (8 from each arm) N = 264
for intent-to-treat analysis
**Paclitaxel given as a 24-hour infusion followed immediately by
cisplatin.
Moore DH, et al. J Clin Oncol. 2004;22:3113-3119.
-
293 patients
Cervical cancer
Stage IV
Recurrent
Persistent
R
A
N
D
O
M
I
Z
E
GOG 179
•1º endpoint : Survival
•2º endpoints: PFS,ORR, QOL, toxicity
Cisplatin 50 mg/m2. Day 1, q21d
Topotecan 0.75 mg/m2/d1-3 plus
Cisplatin 50 mg/m2 d1
Long HJ III et al, JCO 2005
-
Adverse Events
-
GOG 204: Schema
Regimen II
Topotecan/Cisplatintopotecan 0.75 mg/m2 days 1, 2,
and 3 + CIS 50 mg/m2 day 1,Q3W
Regimen III
Navelbine/Cisplatinvinorelbine 30 mg/m2 day 1 and 8 +
CIS 50 mg/m2 day 1 every 3 wks
Regimen I
Paclitaxel/Cisplatinpaclitaxel 135 mg/m2 over 24 hrs +
CIS 50 mg/m2 day 2 every 3 wks
Regimen IV
Gemcitabine/Cisplatingemcitabine 1,000mg/m2 day 1 and
8 + CIS 50 mg/m2 day 1 Q 3 wks
R
• Patients with stage IVB,
recurrent or persistent cancer
not amenable to cure
• GOG PS 0,1
• No CNS meta
• Measurable disease
• Planned: max 600 patients
• Between May 2003 and April
2007, 513 patients were
enrolled
1. Cisplatin/Paclitaxel was reference arm
2. Primary endpoint: Overall survival
-
癌細胞餓死理論
Folkman 博士認為「無血液供應則癌不能生長」
腫瘤細胞增長分裂至0.1-0.2 公分左右會誘導血管的新生,以提供其養分和氧氣
癌細胞的成長和轉移都和血管新生有密切的關係
腫瘤血管新生的程度、惡性度和臨床的預後息息相關
新生的血管會幫助癌細胞的轉移
-
腫瘤生長需要血管新生
Modified from Folkman J. N Engl J Med 1971;285:11826
TAF(Tumour
angiogenic factor)
(擴散)
(佈滿;灌注)
腫瘤血管生成因子(Tumor angiogenesis factors,TAFs)
-
http://www.businessweek.com/magazine/content/03_40/b3852088.htm
OCTOBER 6, 2003SCIENCE & TECHNOLOGY
-
GOG 204-R: 2x2 Factorial Design
Cervical cancer stage IVB, recurrent, persistent
RA
ND
OM
IZA
TIO
N
• Paclitaxel 175mg/m2 for 3
hrs day 1
• Cisplatin 50mg/m2 day 2,
q3wks x 6
• Paclitaxel 175mg/m2 for 3
hrs day 1
• Topotecan 0.75mg/m2 day
1-3, q3wks x 6
RA
ND
OM
IZA
TIO
NR
AN
DO
MIZ
AT
ION
Bevacizumab
Bevacizumab
Placebo
Placebo
GOG; on-going study
GOG 204 Replacement Protocol
-
Chemotherapy for advanced, recurrent, and
metastatic cervical cancer.
Moore DH. Journal of the National Comprehensive Cancer
Network.
6(1):53-7, 2008 Jan.
When cervical cancer is beyond curative treatment with
surgery
or radiation therapy, the prognosis is poor and palliation is
the
primary objective.
Early prospective studies identified cisplatin as an active drug
for
advanced, metastatic, or recurrent cervical cancer, and
results
with other platinum analogs seemed inferior to cisplatin.
-
Chemotherapy for advanced, recurrent, and
metastatic cervical cancer. (2)
Moore DH. Journal of the National Comprehensive Cancer
Network.
6(1):53-7, 2008 Jan.
Several phase III trials have established the combination of
cisplatin plus paclitaxel as standard therapy for
comparison.
Using pooled data from 3 Gynecologic Oncology Group (GOG)
phase III studies, a predictive model was developed to
better
identify patients who are unlikely to respond to cisplatin-
containing chemotherapy.
The GOG is currently developing a phase III trial to
investigate
the impact of bevacizumab and a regimen containing topotecan
instead of cisplatin in combination with paclitaxel
chemotherapy
This study has the potential to radically change standard
care
for cervical cancer chemotherapy.
-
存活分析-2a 子宮頸癌病患(FIGO)II期,1年存活率。
存活分析-2b 子宮頸癌病患(FIGO)II期,3年存活率。
存活分析-2c 子宮頸癌病患(FIGO)II期,5年存活率。
存活分析-3a 子宮頸癌病患(FIGO)III 期,1年存活率。
存活分析-3b 子宮頸癌病患(FIGO)III 期,3年存活率。
存活分析-3c 子宮頸癌病患(FIGO)III 期,5年存活率。
存活分析-4a 子宮頸癌病患(FIGO)IV期,1年存活率。
存活分析-4b 子宮頸癌病患(FIGO)IV期,3年存活率。
存活分析-4c 子宮頸癌病患(FIGO)IV期,5年存活率。
-
敬 請 指 教
謝 謝 聆 聽