Embed Size (px)
Citation preview

Enfermedad Vascular Periférica
MARGARITA GARCÍA
´TÉCNICA HEMODINAMIA

Enfermedad de miembros inferiores:
Aorto-iliac
Femoro-popliteal
Tibio-peroneal
Enfermedad Renal
Enfermdedad Carotídea
Enfermedad Periferica Vascular Manifestaciones Sistémicas de Aterosclerosis
Enfermedad Aorto Femoral
Pacientes con aterosclerosis sintomáticos ó asintomáticos en las extremidades inferiores tienen alto potencial de desarrollar aterosclerosis in otros vasos
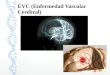
Enfermedad relacionada con el flujo de sangre dentro de las arterias.
La causa más común del estrechamiento o bloqueo de las arterias son
los depósitos de grasa llamados aterosclerosis.
Cambios ateroscleroticos
EVP Definición
Arteria Normal Arteria con aterosclerosis
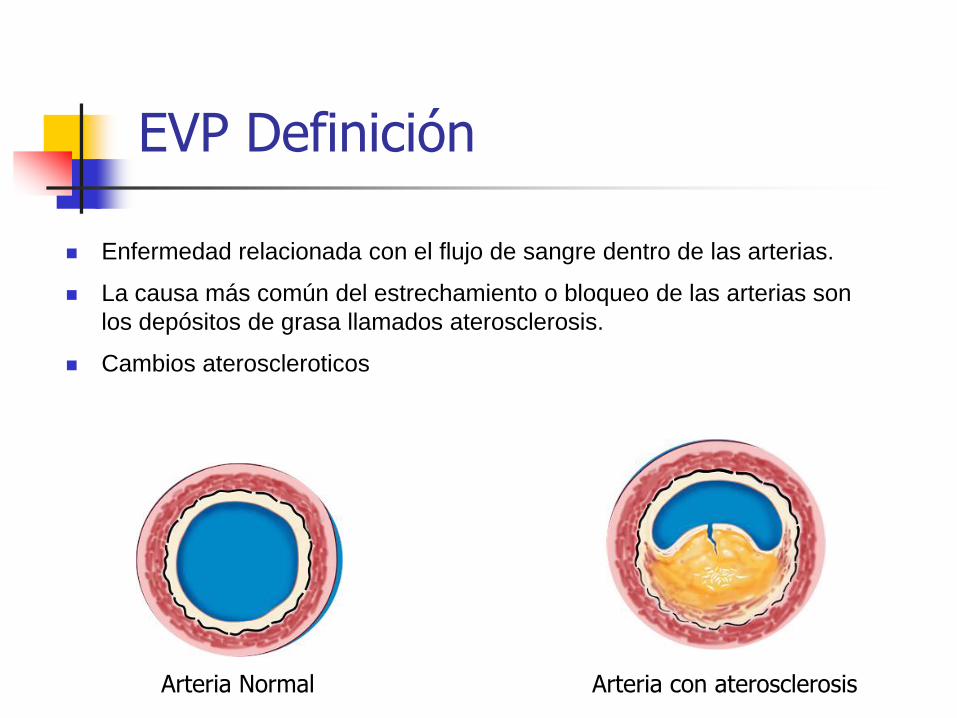
Ateroesclerosis
Definición
Combinación variable de cambios en la íntima de las arterias.
Coronarias, aorta, ilíacas, femorales, renales, subclavía, carotidas, etc.
Estrechamiento de las arterias causada por:
la proliferación de células
acumulación de lípidos
tejido fibroso
depósitos de calcio
Placa aterosclerotica en
una arteria
Corte transversal de una arteria

Evolución de la Aterosclerosis

Evolución de la Aterosclerosis
La placa aterosclerotica puede complicarse con:
Calcificaciones
Trombus
Ulceración

Riesgo de Embolización distal

Factores de Riesgo Asociados
Tabaquismo
Hipertensión Arterial
Diabetes Mellitus
30-50% de Pt con diabetes tienen PVD y la frecuencia de amputación aumenta hasta 4 veces más
Hiperlipidemia
Sedentismo
Obesidad
Mayor del 30% del peso ideal
Edad
Hombres >45 años
Mujeres > 55 años
Historia familiar de Enfermerdad Coronaria
Modificables No Modificables

Evolución de la Enfermedad
Claudicación Interminente
dolor en la pantorrilla o músculo del muslo que
ocurre después de haber caminado una cierta
distancia, como una o dos cuadras. El dolor para al
descanso.
Dolor al descanso
Ulceración
Cambios Isquémicos
Ulceración
Frialdad
Cianosis Gangrena
Perdida de extremidad

Progresión de Enfermedad Perífero Vascular (PVD)
‘Silent’ Intermittent
claudication
Pain at rest,
gangrene,
ulceration
Life-threatening
infection
Clinical presentation
Critical Limb Ischemia (CLI) Symptomatic Disease
Peripheral Vascular Disease (PVD)
Mild claudication
Moderate claudication
Severe claudication
Difficulty walking >½ km Difficulty walking >¼ km Difficulty walking around the home
Hiatt WR. N Engl J Med, 2001; 344: 1608-1621. American Diabetes Association. Diabetes Care 2003; 26: 3333-3341. Weitz JI et al. Circulation. 1996; 94: 3026-3049.

Advanced Symptoms of Lower Limb PVD
This intense paleness of the foot represents severe peripheral vascular disease
Elevation Pallor

Advanced Symptoms of Lower Limb PVD
This intense red/purple colour, along with the ulcer on the tip of the left great toe, represents advanced PVD and critical limb ischaemia
Dependent Rubor
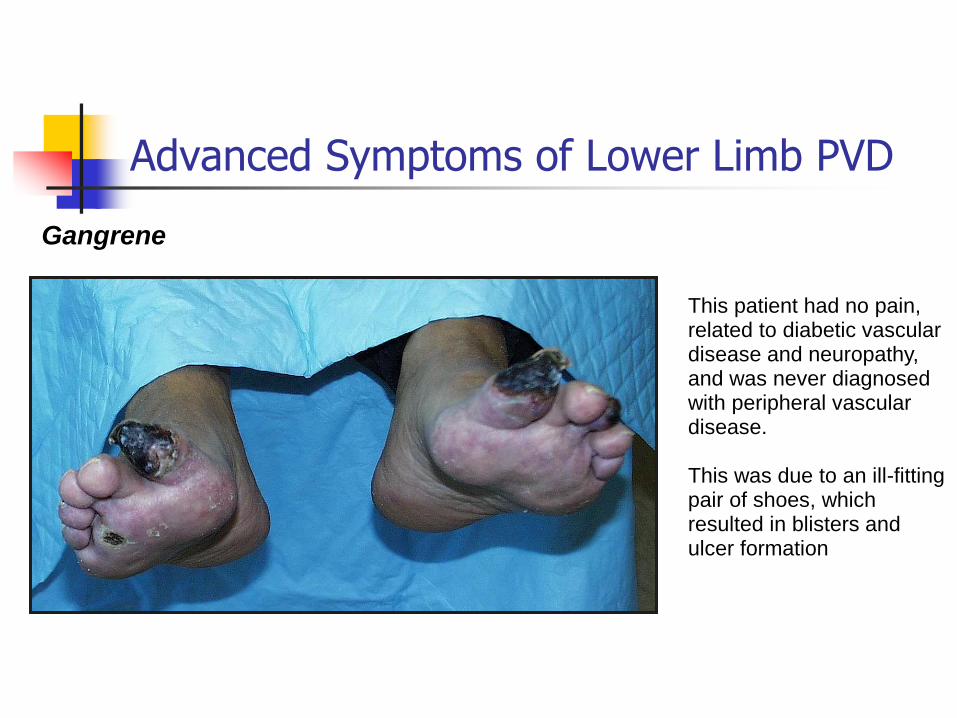
Advanced Symptoms of Lower Limb PVD
This patient had no pain, related to diabetic vascular disease and neuropathy, and was never diagnosed with peripheral vascular disease. This was due to an ill-fitting pair of shoes, which resulted in blisters and ulcer formation
Gangrene

Evaluación no Invasiva
Ankle-brachial Index
Prueba de esfuerzo ( treadmill ) Incluye caminar de (10º-12º) a 1.5-2.0 milas por hora por 5
minutos
Doppler US Angio MRI Pulsos perifericos
Doppler
Angiografia ó RM

Pruebas de Diagnóstico para PVD
The Ankle-Brachial Index (ABI)
Peripheral vascular disease can be easily diagnosed by measuring the ankle-brachial index (ABI)
Sacks D et al. J Vasc Interv Radiol 2003; 14: S389.

Pruebas de Diagnóstico para PVD
La medida del Ankle Brachial Indices (ABI) es por comparación de presiones de la extremidad superior e inferior.
Este representa el método más básico de diagnostico de enfermedad periférica.
Indice
braquial del
tobillo Severidad de la enfermedad Síntomas
0.95 Ninguna Ninguna
0.7-0.95 Media Single Segment
Disease
No-Claudicación
0.5-0.75 Moderado aumento
Claudicación
0.3-0.5 Moderately severe
Usually multisegment
disease unless acute
Severe
Claudication
<0.3 Critica
Severe multisegment
disease and/or acute
Rest pain,
tissue
loss
Indice braquial del tobillo versus la severidad de la enfermedad
Indice Braquial del Tobillo (ABI)

Doppler
El Doppler es método no invasivo que recolecta información anatómica funcional.
Categoria
de
Estenosis
Pico
velocidad sistólica
(PSV)
Turbulencia
Post-estenotica
Normal No elevación de PSV Ninguna
<50% <2X segmento normal Mínimo
50-75% 2-4 X segmento normal Presente
75-99% >4X segmento normal Severo
Ocluido No flujo No flujo
Criteria Duplex Arterial Periférico
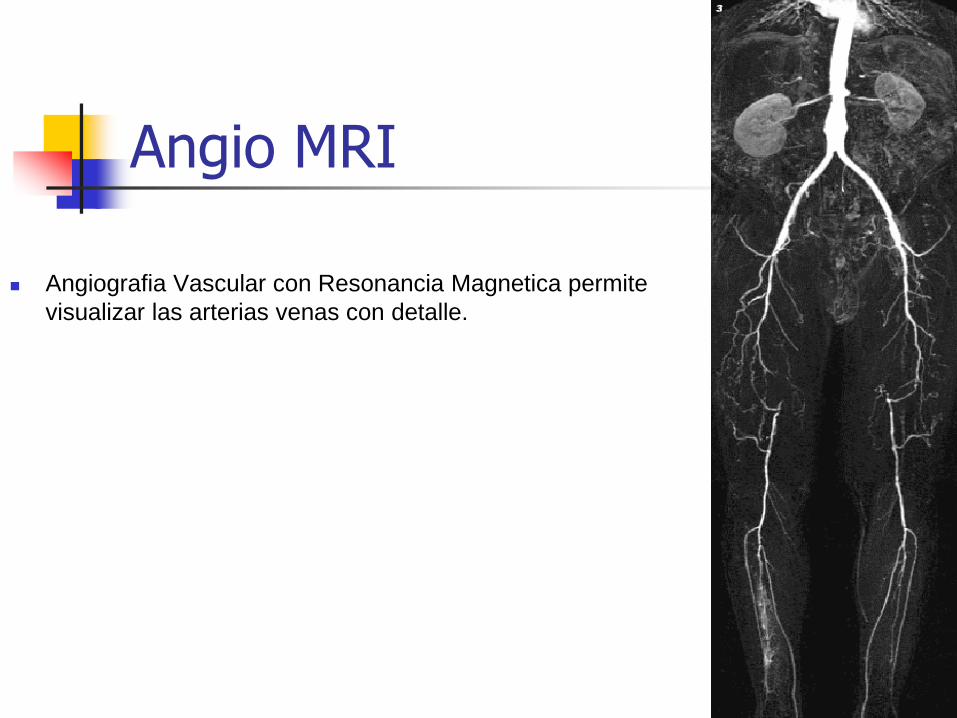
Angio MRI
Angiografia Vascular con Resonancia Magnetica permite
visualizar las arterias venas con detalle.

Tratamiento

SFA Treatment Options
Bypass Surgery Endarterectomy Medication
Angioplasty Stenting
Amputation
Lifestyle modification

Manejo Conservador

Ventajas y Desventajas Tx Endovascular

Enfermedad Vascular Periférica
Tratamiento – Técnicas Minimamente Invasiva
Angioplastia
Stenting
Trombolysis

CONCLUSIONES
Toda enfermedad vascular periferica Es preventiva . Eliminando factores de riesgo como el fumado.

Gracias

Cirugía

Enfermedad Aorto Ilíaca

Patrones de la enfermedad

Oclusiones Totales

Oclusiones Totales

Chronic Total Occlusions
Morphology
A chronic total occlusion (CTO) is a complete or nearly complete obstruction of an artery typically defined as > 3 months old1
Consists of fibro-atheromatous plaque with a fibrous cap at the proximal and distal margins1
Arteries can form their own bypass collateral system around the CTO to provide blood flow to the distal artery2
Collateral flow may not fully compensate for the flow provided by a native vessel2
1Aziz S., Heart 2005; 91(Suppl III):iii42-48. 2©Cordis Corporation, Internal Document 060124.

Every 3 minutes…
Up to 160,000 PAD-related amputations are performed every year
In 60-70% of those cases, the amputation is the first intervention
Source: The Sage Group, 2005

CTO Technologies Help Save Limbs
David Kandzari MD - Duke University
Failed surgery twice-
Patient Recommended
for Amputation
9 month follow up
Critical Limb Ischemia
Revascularized
with
FRONTRUNNER™ XP
CTO Catheter

Staggering Morbidity and Mortality
Morbidity *
At 2 years 15% of patients with initially successful BKA will convert to AKA
An additional 15% of patients will suffer a major contralateral amputation
Mortality at 3 years** 43% for below the knee
61% for above the knee
*Dormandy J, Heeck L, Vig S: Major amputations: Clinical patterns and predictors. Semin Vasc Surg 12: 154-161, 1999.
**Feinglass J, Pearce WH, Martin GJ, et al: Postoperative and late survival outcomes after major amputation: Findings from the
Department of Veterans Affairs National Surgical Quality Improvement Program. Surgery 130:21-29, 2001.

CTO Technology Landscape
Guidewire Successful Cross Successful Re-
Entry
Crossing Technology Re-Entry Technology
Failure to stay
true lumen, or
extended
crossing period
Subintimal

FRONTRUNNER® XP CTO Catheter
Facilitates placement of a conventional guide wire across stenotic lesions or chronic total occlusions in the
peripheral vasculature by creating a pathway through the occluded vessel via blunt micro-dissection.

FRONTRUNNER® XP CTO Catheter Indications For Use
INDICATIONS
The FRONTRUNNER XP CTO Catheter is intended to facilitate the intraluminal
placement of conventional guide wires beyond stenotic lesions (including chronic total
occlusions) in the peripheral vasculature prior to further percutaneous intervention.
CONTRAINDICATIONS
The device is not intended for use in the cerebral vasculature.
WARNINGS*
•Do not use this device to cross a lesion within a stent.
•Do not use this device in the coronary vasculature.

OUTBACK® LTDTM Re-Entry Catheter
The OUTBACK® LTDTM Re-Entry Catheter is a single lumen catheter designed to facilitate placement
and positioning of guidewires and catheters within the peripheral vasculature.

OUTBACK® LTDTM Re-Entry Catheter
Indications for Use INDICATIONS FOR USE
The OUTBACK® LTDTM Re-Entry Catheter is intended to facilitate
placement and positioning of guidewires and catheters within the
peripheral vasculature.
CONTRAINDICATIONS*
The OUTBACK® LTDTM Re-Entry Catheter is not intended for use in
the coronary or cerebral vasculature.
*For more details on Indications, Contraindications, Warning and instructions for use, please see
the IFU. Please read the IFU prior to use.

David Kandzari MD - Duke University
CLI Patient
Recommended for
Amputation
9 month follow up-
Patient revascularized
with FRONTRUNNER®XP
CTO Catheter
Crossing Complex Chronic Total Occlusions = Saving Limbs

Gracias

Procedimientos Ilíaco – Femoral (SFA)

Objetivos Presentación
Entender la historia natural de la enfermedad Periférica
Reconocer signos y síntomas de la enfermedad

Anatomía Iliaca – Femoral

Ilíaca Interna
Origen
A nivel de la sínfisis sacroilíaca
Trayecto
Verticalemnte a la pelvis menor por delante del sacro y detrás de la iliíaca externa.
Longitud aprox. 2 a 4 cm
Ramas
Intrapélvicas parietales
Intrapélvicas viscerales
Extrapélvicas

Arteria Femoral Común
Es la continuación de la arteria Iliaca Externa.

La Arteria Femoral Común empieza al nivel del ligamento inguinal como la continuación de la arteria iliaca externa.
Baja vertical recto sobre la cabeza femoral, y después de subir de la Arteria Femoral Profunda la arteria femoral común continúa como la Arteria Femoral Superficial siendo el eje arterial principal de la rama inferior.
Anatomía

Arteria Femoral Profunda
Nace a nivel del cuello femoral
Ramas perforantes
Usualmente son 4
Las ramas terminales de las perforantes se anastomosan con ramas misculares de la Femoral Superficial.
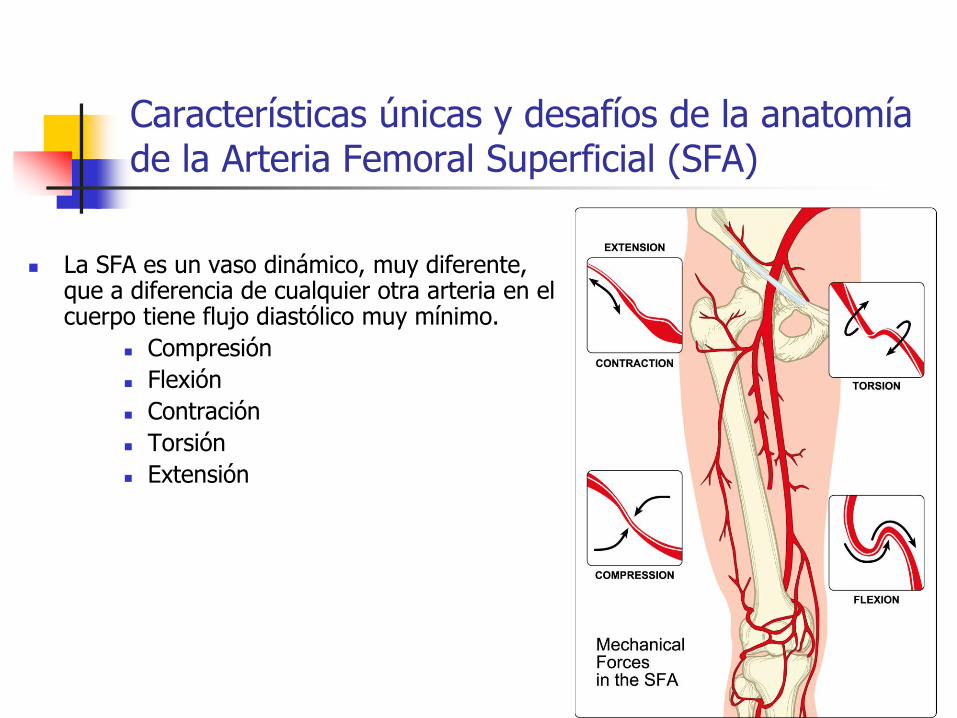
Características únicas y desafíos de la anatomía de la Arteria Femoral Superficial (SFA)
La SFA es un vaso dinámico, muy diferente, que a diferencia de cualquier otra arteria en el cuerpo tiene flujo diastólico muy mínimo.
Compresión
Flexión
Contración
Torsión
Extensión

La Arteria Femoral Superficial
está afectada en más del 50% de
las veces, por Enfermedad
Arterial Periférica.
Johnsrude and Jackson.Litttle A practical approach to angiography., Brown ed,1982
Sitios comunes de Enfermedad Arterial Periférica

2- 5 mm
3 - 10 mm 5 - 12 mm
6 - 10 mm
6 - 10 mm
30 - 40 mm
1.5 - 5 mm
20 - 30 mm
5 -8 mm
2 -3 mm
7 - 15 mm
5 - 10 mm
5 - 10 mm
3 - 10 mm
Superficial 4 -6 mm
3 - 6 mm
2 - 4 mm
2 - 4 mm
2 - 4 mm