Embed Size (px)
Citation preview

15.09.12 1 Forfatter Prosjektittel
FORSVARET Forsvarets logistikkorganisasjon
15.09.12 1
FORSVARET Forsvarets sanitet
Helse for stridsevne
Militære traumesystem, en forbedring av militær traumatologi
Bent-Åge Rolandsen Avdelingsoverlege Sykehusgruppen FFSS/FSAN

15.09.12 2 Helse for stridsevne
FORSVARET Forsvarets sanitet
Innledning
• Forskjell militær og sivil traumatologi
• Hva skal prehospitalt personell beherske • Hva skal militære kirurgiske team mestre • Traumesystem
– Sivile – Militære
15.09.12 3 Helse for stridsevne
FORSVARET Forsvarets sanitet
Militær traumatologi
• Skademekanisme – Penetrerende versus stump skademekanisme
• Militært traumesystem
– Betjene flere nivåer – 4R

15.09.12 4 Helse for stridsevne
FORSVARET Forsvarets sanitet
Militær traumatologi
• Medisinskfaglig kompetanse
– Spesialkompetanse på eksplosjons-‐ og prosjekElskader
– Bred generell kompetanse pga begrenset Elgang El spesialister

15.09.12 5 Helse for stridsevne
FORSVARET Forsvarets sanitet
Militær traumatologi • Militært miljø -‐ austere environment
– Behov for kunnskap utover det medisinske i skarpe operasjoner
– Beherske kommunikasjon med annet militært personell i grensesniGet mellom det rent operaEve og det fagmedisinske
– Beherske tjeneste som medisinsk fagpersonell i miljøer som krever stor krysskunnskap og robusthet.

15.09.12 6 Helse for stridsevne
FORSVARET Forsvarets sanitet
Hva skal prehospitalt personell beherske ?
Ulike krav for: • Vanlig soldat, Sanitetssoldat • Hjelpeplass • Evakuering (Bakke eller luN) • ABCDE / CABcDE/ MARCH
ABCDE/CABcDE/MARCH • LuNvegsproblemaEkk • Trykkpneumothorax • Ekstremitetsblødninger • Hindre hypotermi
• Dokumentasjon
15.09.12 7 Helse for stridsevne
FORSVARET Forsvarets sanitet
Hvilke kirurgiske/ortopediske
prosedyrer må beherskes av et norsk kirurgisk team?

15.09.12 8 Helse for stridsevne
FORSVARET Forsvarets sanitet
Kirurgisk team • Spesialist i generell kirurgi • Spesialist i ortopedisk kirurgi • Spesialist i anestesiologi • Anestesisykepleier • To operasjonssykepleiere
15.09.12 9 Helse for stridsevne
FORSVARET Forsvarets sanitet
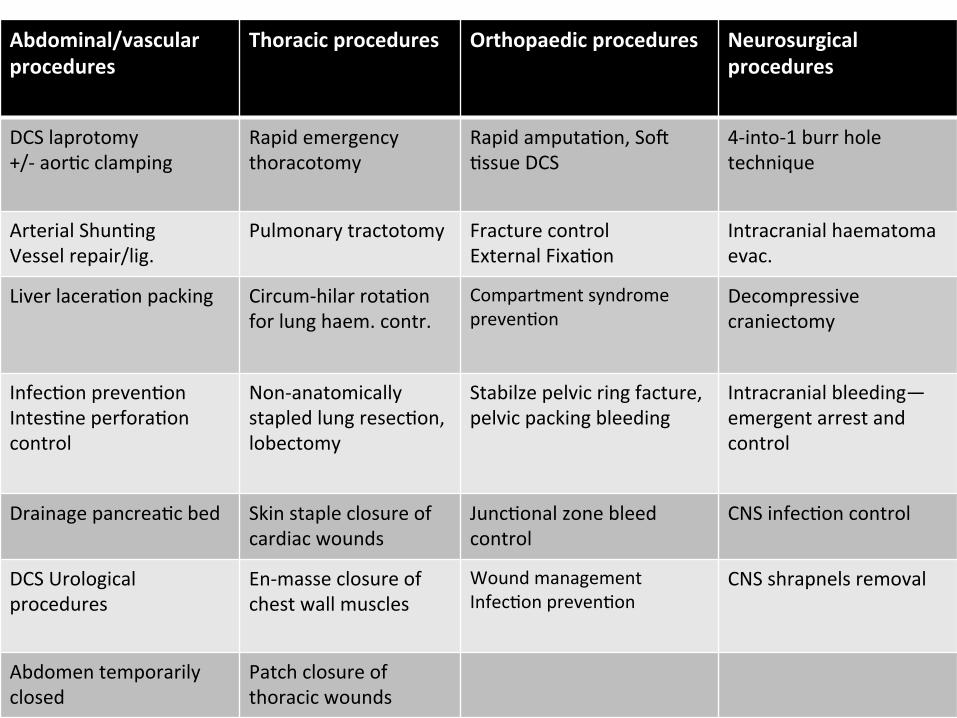
Abdominal/vascular procedures
Thoracic procedures Orthopaedic procedures Neurosurgical procedures
DCS laprotomy +/-‐ aorEc clamping
Rapid emergency thoracotomy
Rapid amputaEon, SoN Essue DCS
4-‐into-‐1 burr hole technique
Arterial ShunEng Vessel repair/lig.
Pulmonary tractotomy Fracture control External FixaEon
Intracranial haematoma evac.
Liver laceraEon packing Circum-‐hilar rotaEon for lung haem. contr.
Compartment syndrome prevenEon
Decompressive craniectomy
InfecEon prevenEon IntesEne perforaEon control
Non-‐anatomically stapled lung resecEon, lobectomy
Stabilze pelvic ring facture, pelvic packing bleeding
Intracranial bleeding—emergent arrest and control
Drainage pancreaEc bed Skin staple closure of cardiac wounds
JuncEonal zone bleed control
CNS infecEon control
DCS Urological procedures
En-‐masse closure of chest wall muscles
Wound management InfecEon prevenEon
CNS shrapnels removal
Abdomen temporarily closed
Patch closure of thoracic wounds

15.09.12 10 Helse for stridsevne
FORSVARET Forsvarets sanitet
Anestesiologisk kompetanse
• Vanskelig luNvei • Plan for ”vascular access” • Traumeanestesi • Intensiv behandling • Damage control resuscitaEon • Indikasjon og gjennomføring av fullblodstransfusjon

15.09.12 11 Helse for stridsevne
FORSVARET Forsvarets sanitet
Traumesystem
Wars have always promoted advances in trauma care because of the concentrated exposure of military hospitals to large numbers of injured people during a relaEvely short span of Eme. Dr Michael Debakey (Basert på erfaringer fra 2. verdenskrig)

15.09.12 12 Helse for stridsevne
FORSVARET Forsvarets sanitet
Hva er et traumesystem?
Organisert plan for behandling av akuG skadde pasienter i en definert region eller populasjon
MÅL:
• OpEmal sjanse for overlevelse • Minimalt funksjonstap

15.09.12 13 Helse for stridsevne
FORSVARET Forsvarets sanitet
Sivile traumesystem • Erkjennelse i USA at skader og ulykker var et folkehelse problem
• Kombinert med erfaringer fra saniteten i Vietnamkrigen
• Innføring av traumesystem i USA – Redusert mortalitet 15-‐20 %

15.09.12 14 Helse for stridsevne
FORSVARET Forsvarets sanitet
Hva er et traumesystem?
• Fundamentet er:
– Prehospital tjeneste – Sykehus – Rehabilitering
• I en fungerende behandlingskjede.

15.09.12 15 Helse for stridsevne
FORSVARET Forsvarets sanitet
Hva er et traumesystem?
• Traumeregister • Overføringskriterier • Kliniske retningslinjer • Trening/opplæring • Traumemøter/M&M møter

15.09.12 16 Helse for stridsevne
FORSVARET Forsvarets sanitet
Norway87 concluded that for trauma patients, advanced airwaymanagement and thoracic drainage performed by a physicianincreased survival. A Danish series of studies on endotrachealintubation performed on-scene, concluded that while the proce-dure is widespread it requires skills that are restricted to speciallytrained physicians.25,26,54 The presence of an anaesthesiologistprolonged median on-scene time by 1 min, and in cases in whichendotracheal intubation was performed, by 7.5 min.63 A survey ofNorwegian pre-hospital anaesthesiologists128 also confirmed theneed for training to maintain airway management skills. Recentlythe Scandinavian Society of Anaesthesiology and Intensive Careproposed a flow chart for airway management in the field,stratified by the provider’s level of skill.12
The northernmost areas of Scandinavia face special chal-lenges.126,163 A survey from northern Norway describes theoperational and medical characteristics of 147 missions in theBarents Sea,46 with one-third of the search and rescue missions
carried out in darkness, transport times of up to 425 min, andpatients often severely injured; a scenario not unlike the‘‘tyranny of distance’’ describing rural trauma management inAustralia.29
For decades, pre-hospital fluid therapy has been aimed at theimmediate restoration of normovolaemia.139 More recent experi-mental and clinical research has questioned this approach.107,139
Scandinavian researchers have contributed to this debate,69,70,108–
113,130,164 and treatment protocols have been called for.107,129 InStockholm a study of 102 hypotensive trauma patients found thatthe initiation and form of fluid therapy was irrespective of the typeand severity of the injury.148 Further, they demonstrated a lack ofemployment of treatment protocol, and that on-scene timeexceeded recommendations.148 Scandinavian guidelines for mana-ging trauma patients with massive bleeding were recentlypublished42 based on the existing literature and consensus amongthe experts in the field. The guidelines include a step-wiseframework and differential approach for pre-hospital triage andmanagement of the haemorrhaging trauma patient.42
Fig. 1. The inclusive trauma system. The components and their interactions in an inclusive trauma system. The core operational components constitute an organised systemfrom the site of injury to rehabilitation. All levels of resources are employed according to the clinical requirements. The outer administrative framework represents funding,assessment and continual development of the system. Adapted with permission from the Health Resources and Service Administration, US Department of Health and HumanServices.152
Fig. 2. Mechanism of injury in severe and fatal trauma. Typical distribution ofmechanism of injury extrapolated from Søreide et al.145 and Hansen et al.51
Fig. 3. Distribution of TBI mortality rates in Scandinavia. Data were obtained fromreferences.5,32,35,133
T. Kristiansen et al. / Injury, Int. J. Care Injured 41 (2010) 444–452446

15.09.12 17 Helse for stridsevne
FORSVARET Forsvarets sanitet
6 http://www.cs.amedd.army.mil/dasqaDocuments.aspx?type=1
Transforming US Army Trauma Care: An Evidence-Based Review of the Trauma Literature
Table 1. Evidence-based lessons about trauma care derived from the literature.
Civilian Trauma Systems 1. Trauma systems improve mortality.4-7 2. Integration of designated trauma centers within a state improves outcomes.4-7 3. Initial treatment by ATLS-trained physicians at rural level III trauma centers decreases preventable deaths.8-10 4. Initial transport to a rural level III trauma center with only an ATLS physician does not increase mortality and may
decrease mortality in rural areas even with delays of up to 4 hours to reach the level I trauma center.6,11-13 5. RTS <6.00 and hypotension in patients with chest or abdominal injury predicts a need for DCS prior to transfer to a
level I center.14
Military Trauma Systems 1. Battlefields and tactics change over time and modern battlefields may contain multiple types of conflict
simultaneously within the same battle-space.15-18 2. Combat trauma system contingency planning is important to remain prepared for future complex battlefields.1 3. Proper utilization of surgical resources within a trauma system improves survival within the system and up to 50% of
potentially survivable injuries are surgical.19,20 4. The FST is proven in rapid, modern maneuver warfare and with modifications has succeeded in providing surgical and
nonsurgical trauma care for stability and counterinsurgency operations in our current theaters.21 5. Current Army trauma system surgical and presurgical (ATLS) assets need increased modularly and flexibility to rapidly
tailor trauma care for changing conflict types within a single, complex battlefield.1,16-18,22
Presurgical Trauma Care 1. Prehospital paramedic care decreases mortality and increases trauma system efficiency.23 2. A large portion of trauma patients can be treated or temporized by EM physicians performing ATLS level LSIs.24-26 3. EM physicians are currently underutilized within the Army trauma system.24,25 4. Using EM and highly-trained ATLS physicians in the presurgical portion of the trauma system can increase system
efficiency and resource utilization.24-27 5. Certain patients always need early surgeon involvement for life-saving surgery (hypotension with penetrating neck and
torso trauma).27,28
Medical Evacuation Times 1. The golden hour was a “best guess” rule-of-thumb created 30 years ago and was not based on data.29 2. Combat trauma deaths likely occur in a bimodal distribution with the first peak of death from immediately after
wounding to 15 minutes and the second peak at 60 to 180 minutes.19,30-32 3. The time distribution of death is highly dependent on type of injury and not all injuries produce temporal-based peaks
of death (specifically severe head injury).32 4. High-level enroute care may decrease mortality despite longer evacuation times.33 5. Prehospital care in the military system is divided into ATLS facility care and surgical facility care.33,34 6. By reviewing TPtoA and TPtoS data, we can begin to describe which injuries require rapid initial ATLS care versus
surgical care.32,35,36
Medical Evacuation System 1. Advanced care (paramedic-level and above) during transport of the severely wounded improves survival.37-39 2. A template for each type of conflict with specific MEDEVAC triage criteria to determine appropriate enroute and
presurgical treatment is needed.22,34,39 3. Research is needed to determine the physiologic and anatomic parameters for appropriate enroute treatment and
triage (ATLS versus surgical).39-41
GLOSSARY ATLS - advanced trauma life support MEDEVAC - military medical evacuation DCS - damage control surgery RTS - revised trauma score EM - emergency medicine TPtoA - time from point-of-injury to the first ATLS facility FST - forward surgical team TPtoS - time from point-of-injury to first surgical facility LSIs - lifesaving interventions
Sivile traumesystem
Transforming US Army Trauma Care: An Evidence-Based Review of the Trauma Literature LTC Kyle N. Remick; LTC James A. Dickerson II; LTC Shawn C. Nessen;COL Robert M. Rush; COL Greg J. Beilman; The united states army medical department journal, july-september 2010

15.09.12 18 Helse for stridsevne
FORSVARET Forsvarets sanitet
Hva er et militært traumesystem?
15.09.12 19 Helse for stridsevne
FORSVARET Forsvarets sanitet
Militært traumesystem
• USA innførte deGe i 2004/2005
– Basert på erfaringer fra 1. Gulmrig (1992) – Erkjennelse av at sivilt traumesystem var mye bedre
• Storbritannia

15.09.12 20 Helse for stridsevne
FORSVARET Forsvarets sanitet
Joint Theater Trauma System That every military member injured in the theater of operaEons has the opEmal chance for survival and maximal potenEal for funcEonal recovery • Innført i 2005
– Right paEent – Right place – Right Eme – Right care

15.09.12 21 Helse for stridsevne
FORSVARET Forsvarets sanitet
JTTS komponenter
• prevenEon, • pre-‐hospital integraEon • educaEon • Leadership and communicaEon • Quality improvement/performance improvement • research • informaEon systems.

15.09.12 22 Helse for stridsevne
FORSVARET Forsvarets sanitet
Storbritannia
when evaluating the performance of personnel andvehicle protective systems. There is close liaison withthe attending scientific adviser that allows new pat-terns of wounding and the impact of changes inweaponry to be rapidly identified.
(b) Hospital exerciseImmediately prior to deployment, the entire field hos-pital undertakes a validation exercise in a replica fieldhospital in York. This exercise (called hospital exercise;HOSPEX) can assess an individual’s performance(microsimulation techniques), a team’s performancesuch as the trauma team or operating team (meso-simulation techniques) and the hospital’s globalperformance in response to continued bursts of casual-ties (macrosimulation techniques; [56]). Anonymizedcasualty data from JTTR are used to construct thescenarios. The use of genuine and contemporarycase scenarios, played out in real time with simulatedlive casualties (former soldiers who have sufferedamputations) and in a realistic duplicate environment,generates the necessary face and content validity forthe exercise. Importantly, this inspires confidence inthose deploying for the first time and decreases theinitial shock of encountering critical combat woundedin the field hospital.
(c) Joint Theatre Trauma RegistryThe JTTR is derived from a composite of threeindependent databases:
— major trauma audit for clinical effectiveness(MACE);
— medical emergency response team (MERT); and— operational emergency department attendance
register (OpEDAR).
JTTR’s principal purpose is a quality assurance systemfor the management of major trauma from point ofwounding (POW) to rehabilitation. It is a tool to sup-port continuous detailed clinical audit. Data from allthree streams provide the full picture of all significantlyinjured casualties from time of injury, throughpre-hospital treatment and evacuation, to the careadministered at the field hospital. For UK militarycasualties, the continuing pathway of air evacuationto UK and definitive treatment in UK is also captured.The MERT database is an electronic record of patientstreated by the UK’s MERT (physician-led helicopter-borne pre-hospital team). As the MERT will deliverpatients to treatment facilities other than the UKfield hospital, their information will not appear inMACE unless they enter the UK system again laterin their course—additionally, patients with illnessrather than injury may be transported by MERT, butwill not appear on MACE. OpEDAR captures allpatients (injury and illness) attending the emergencydepartment of a UK field hospital [57]: patients canbe on MACE without appearing on OpEDAR ifthey receive their initial treatment in a non-UK fieldhospital, prior to evacuation to Birmingham.
An important part of the CG process is providingfeedback: where outcome is unexpectedly positive(the unexpected survivor), then practice is praisedand reinforced, but where practice is regarded as sub-optimal, the area for improvement is highlighted,organizational change is instituted and compliance ismonitored. Formal academic review of performanceduring a specified period of an operation is used toreview and compare patterns of activity and clinicaleffectiveness [58–61]. JTTR has also been used tosupport academic evaluation of complex organi-zational challenges such as the effectiveness oftourniquets [62], the effectiveness of battlefield
Joint Theatre Trauma Registry
deployed TNC
ADMEM TNC—role 4 —post-mortem—DMRC
deployed TNC Trg—MACE cse—ADMEM attachment—HOSPEX
critical event reporting (PJHQ, HQSG)clinical effectiveness reportsDstl: drive research requirementsforce protection requirementsJMC: drive training requirements
advice and feedbackelectronic data forms
Figure 4. The military trauma CG process.
Review. Trauma scoring and governance in the DMS R. J. Russell et al. 177
Phil. Trans. R. Soc. B (2011)
on March 2, 2011rstb.royalsocietypublishing.orgDownloaded from

15.09.12 23 Helse for stridsevne
FORSVARET Forsvarets sanitet
Resultat
from the two Websites for the major categories of interest forIraq and Afghanistan.
Table 3 shows KIA, DOW, and CFR rates for threeconflicts using the most comparable numerator and denomi-nator figures for each (i.e. ground troops only and the abilityto distinguish RTD) and using the definitions referred toabove.
The case fatality rate (CFR) progressively decreasedover the conflicts WWII ! Vietnam ! Iraq and Afghanistan;p " 0.0001 between conflicts). A similar pattern was noted in%KIA (WWII ! Vietnam ! Iraq and Afghanistan; p "0.0001 between conflicts). Understandably a different patternis seen for %DOW. There was an increase in %DOW duringthe most recent conflict (Iraq and Afghanistan ! WWII !Vietnam; p " 0.004 between conflicts). Interestingly, bothDOW and KIA are higher in Afghanistan than Iraq (p "0.05).
Data were analyzed using SAS version 8.1 (SAS InstituteInc., Cary, NC). To compare among and between conflicts forthe categorical variable Live/Die Chi-square tests were used.A Bonferroni adjustment was used for multiple comparisonsand significance level is set at 0.05.
DISCUSSIONIn the present conflict, now entering its fourth year,
case fatality rates (Table 3) for combat injury amongUnited States military personnel in Afghanistan and Iraq isindeed roughly half that of Vietnam and one-third that ofWorld War II, (p " 0.01). It is not unreasonable to judgethat some of this reduction may be a result of widespreaduse of improved body armor, because chest wounds arerelatively decreased in preliminary data when comparedwith previous conflicts.20 Particularly for the reduction in%KIA, (p " 0.001), additional contributing factors mayinclude the successful transition of products from the 10year DoD research program on improved hemorrhage con-trol and increased focus on prehospital Tactical CombatCasualty Care training,22 coupled with rapid evacuation.Some degree of reciprocity between KIA and DOW ratesis expected6,21 as many of the more severly injured casu-alties who in the past would have died before reachingMTF care (KIA), now die after rapid evacuation to MTFs,changing their classification to DOW. The observed in-
crease (p " 0.01) in DOW rates would likely be higher ifnot for the improvements in surgical management utilizingdamage control techniques, improved ICU care, earlierrecognition of abdominal compartment syndrome, liberaluse of fresh whole blood and recombinant factor VIIa(rFVIIa), among other new techniques, and institution of atheater-wide trauma systems approach. Interestingly, thecalculation of DOW for Afghanistan reveals a rate of 6.7%while in Iraq it is 4.7 %, (p " 0.05), while the KIA rate is18.7 in Afghanistan and in Iraq it is 13.5% (p " 0.05).Only by using common definitions and consistent equa-tions can these comparative rates be determined. The causeof the differences between theaters is unclear. Smallernumbers overall, different application of DOW, KIA anddead on arrival definitions, wounding at altitude, muchlonger evacuation distances, different applications of bodyarmor and different injury mechanisms are all probablyimportant variables. However, these and other hypothesescannot be tested until wound severity data are compiled ina fashion that permits appropriate case-control compari-sons. Taken together, these and other changes in practiceimplemented on the current battlefield have resulted in astatistically and clinically significant decrease in the the-ater wide, four year CFR compared to previous conflicts,(p " 0.001).
In both WWII and Vietnam, of those Soldiers who died,88% were KIA and 12% DOW.4,23 Because of the significantdecrease in the KIA rate in the current war, a greater per-centage of patients are dying after reaching a MTF. In Iraqand Afghanistan of those who die, 23% are DOW and 77%KIA. Though the CFR rate has decreased, the near doublingof those patients now dying at the MTF’s emphasizes theneed to focus resources and research to aid these casualties.
Thoughtful review of KIA, DOW, and CFR rates forcombat trauma are important for optimal medical planning,training, research, and resource allocation. The need to bringcombat casualty epidemiology to a civilian standard requiresutilization of both technology and organization that are rou-tinely utilized in the United States civilian traumacommunity.24,26 Thanks to efforts by the Deputy AssistantSecretary of Defense for Health Affairs and the SurgeonsGeneral of each of the armed services, raw data appropriatefor this effort are now being collected in three separate
Table 3 Comparison of Proportional Statistics for Battle Casualties, U.S. Military Ground Troops, World War II,Vietnam, Afghanistan/Iraq
WW II8,9 Vietnam4 Total Iraq/Afghanistan1,2 Afghanistan1,2 Iraq1,2
% KIA 20.2a 20.0b 13.8c 18.7 13.5*% DOW 3.5a 3.2b 4.8c 6.7 4.7*CFR 19.1a 15.8b 9.4c 16.4 9.1*
Comparisons between WWII, Vietnam, and Total Iraq/Afghanistan, a,b,c, " 0.05.Comparison between Iraq and Afghanistan * p " 0.05.% KIA # 100 $ KIA/(WIA % RTD) & KIA; % DOW # 100 $ DOW/(WIA % RTD); CFR # 100 $ (KIA & DOW)/(WIA & KIA).
The Journal of TRAUMA! Injury, Infection, and Critical Care
400 February 2006flicts described in this study, these 3 major causes of deathcontinue to be present in Afghanistan and Iraq.26,30,31 Hol-comb et al30 identified opportunities to improve care in12 of 82 deaths (15%) among Special Operations Forces.In a review of 982 deaths, Kelly et al31 reported 24% ofdeaths as potentially survivable, with opportunity to im-prove care equally distributed between prehospital andhospital settings. Although it cannot be absolutely quan-tified as resulting from their casualty response system,an overall case fatality rate of 7.6 coupled with the elimi-nation of prehospital preventable deaths validates to anotable degree the Ranger training approach (Table 6).
Training for TCCC was initiated by the Rangers in 1997and formed the basis for 2 programs of instruction, RangerFirstResponder (RFR)andCasualtyResponseTraining forRangerLeaders.12,16-18Becausecareunderfiremustbesimple,direct, and conditioned into the provider, RFR emphasizesrepetitive hands-on application of TCCC lifesaving skills
incorporated into realistic scenario-based learning. Every-one on the battlefield, not just medics, has the potential tobe a casualty or to be the first person to encounter a casu-alty; thus,RFRismandatedforallpersonnel in theregimentregardless of their role.18 This concept is best illustrated bythe fact that 26% of hemorrhage control interventions inthis study, including 42% of tourniquets, were applied bynonmedical personnel at the point of wounding, probablydecreasing the necessity for additional prehospital resus-citationandcertainlycontributing tonopreventabledeathsdue to extremity hemorrhage exsanguination.
Because the tactical commander manages all re-sources dedicated to preparing for and completing a mis-sion, it is this nonmedical leader who is ultimately re-sponsible for the prehospital casualty response system.This concept differentiates RFR and Casualty ResponseTraining for Ranger Leaders from other medical pro-grams. The goal is to educate all on the operational con-
Table 2. Comparison of Proportional Statistics for Battle Injuries in the 75th Ranger Regiment vs Total US Military Ground TroopsBetween October 1, 2001, and March 31, 2010
Statistic
75th Ranger Regiment(n=419)
US Military Ground Troops(n=43 311)
Overall OEF OIF Overall OEF OIF
RTD, %a 40b 46 36b 56 44 58KIA, %c 10.7b 12.5 9.5b 16.4 16.5 16.4DOW, %d 1.7b 2.2 1.4b 5.8 4.7 6.0CFRe 7.6 8.4 7.1 10.3 12.4 10.0
Abbreviations: CFR, case fatality rate; DOW, died of wounds; KIA, killed in action; OEF, Operation Enduring Freedom; OIF, Operation Iraqi Freedom;RTD, returned to duty in less than 72 hours.
aThe RTD percentage (RTD/wounded in action!100) defines minor wounds.26 The differences between overall and OIF values for the 2 groups werestatistically significant ("2
1=11.6, P# .001; and "21=12.8, P# .001), indicating fewer minor wounds in the Ranger populations given the same period. However, the
difference between OEF values was not statistically significant ("21=0.058, P=.81).
bStatistically significant (P# .05).cThe KIA percentage ([KIA/(KIA$wounded in action!RTD)]!100) provides a potential measure of weapon lethality, effectiveness of prehospital medical care,
and availability of tactical evacuation.26 All Ranger values appear to be lower compared with the US military ground troops. The differences between overall andOIF values for the 2 groups were statistically significant ("2
1=4.3, P=.04; and "21=4.2, P=.04). However, the difference between OEF values was not statistically
significant ("21=0.63; P=.43).
dThe DOW percentage ([DOW/(wounded in action!RTD)]!100) provides a potential measure of the precision of initial prehospital triage and care, optimizationof evacuation procedures, and application of a coordinated trauma system as well as the effectiveness of medical treatment facility care.26 Although all Rangervalues appear to be lower compared with US military ground troops, only the differences in overall and OIF values were statistically significant ("2
1=5.9, P=.02;and "2
1=4.2, P=.04). The OEF value was not statistically significant ("21=0.71, P=.40). Also of note, for US military ground troops, the DOW percentage has
remained less than 5% during the past half century; however, in this study it was found to be higher overall and in OIF.eThe CFR ([(KIA$DOW)/(KIA$wounded in action)]!100) provides a potential measure of overall battlefield lethality in a battle injury population.26 Although
all Ranger values appear to be lower compared with US military ground troops, none were found to be statistically significant ("21=2.5, P=.11; "2
1=1.9, P=.17; and"2
1=1.6, P=.21).
Table 3. Hemorrhage Control Interventions Administered by 75th Ranger Regiment Personnel by Provider Level During Care UnderFire and Tactical Field Care Phases of Tactical Combat Casualty Care Between October 1, 2001, and March 31, 2010a
Intervention
Care Provider Level, No.
Total, No.RFR Nonmedic EMT Medic Medical Officer
Pressure dressingb 33 16 136 21 206Gauze dressing 28 16 121 23 188Tourniquetc 27 10 49 3 89Hemostatic dressingd 3 1 26 7 37Total 91 43 332 54 520
Abbreviations: EMT, emergency medical technician; RFR, Ranger First Responder.aNonmedical personnel provided 26% (134/520) of all hemorrhage control interventions and 42% (37/89) of all tourniquets.bPrimarily Emergency Trauma Dressings (North American Rescue, LLC, Greer, South Carolina).cPrimarily Combat Application Tourniquets (Composite Resources, Rock Hill, South Carolina).dPrimarily HemCon bandages (HemCon Medical Technologies, Inc, Portland, Oregon) and Combat Gauze (Z-Medica Corp, Wallingford, Connecticut).
ARCH SURG/ VOL 146 (NO. 12), DEC 2011 WWW.ARCHSURG.COM1354
©2011 American Medical Association. All rights reserved. at Uniformed Services University, on December 19, 2011 www.archsurg.comDownloaded from

15.09.12 24 Helse for stridsevne
FORSVARET Forsvarets sanitet
• Damage control resusitaEon – Innføring av 1:1:1 transfusjon – Hypotensiv resusitering – Minimlal krystalloid bruk
• Redusert mortalitet massiv transfusjon • Hodeskadepasienter bedre resultat • TCCC
Resultat

15.09.12 25 Helse for stridsevne
FORSVARET Forsvarets sanitet
Hva har Norge? • Traumeregister • Overføringskriterier • Kliniske retningslinjer • Trening/opplæring • Traumemøter/M&M møter • LogisEkk
Prehospitalt
Feltsykehus
DefiniEv Behandling

15.09.12 26 Helse for stridsevne
FORSVARET Forsvarets sanitet
Konklusjon
• Traumesystem – Berger liv og funksjonsevne
• Standarden er USA og Storbritannia