Embed Size (px)
Citation preview
Claudio Mastroianni
Dipartimento di Sanità Pubblica e Malattie Infettive Direttore UOC Malattie Infettive, Latina
LA TBC NELL’ERA DEI BIOLOGICI
" Epidemiologia e screening“
“La vecchia nemica dell’umanità, conosciuta come tisi, la grande peste bianca, tubercolosi, o qualsivoglia altro nome, sta per essere ridotta ad un problema irrilevante per l’uomo.
Il futuro è invero brillante, e la completa eradicazione di questa malattia è ormai all’orizzonte.”
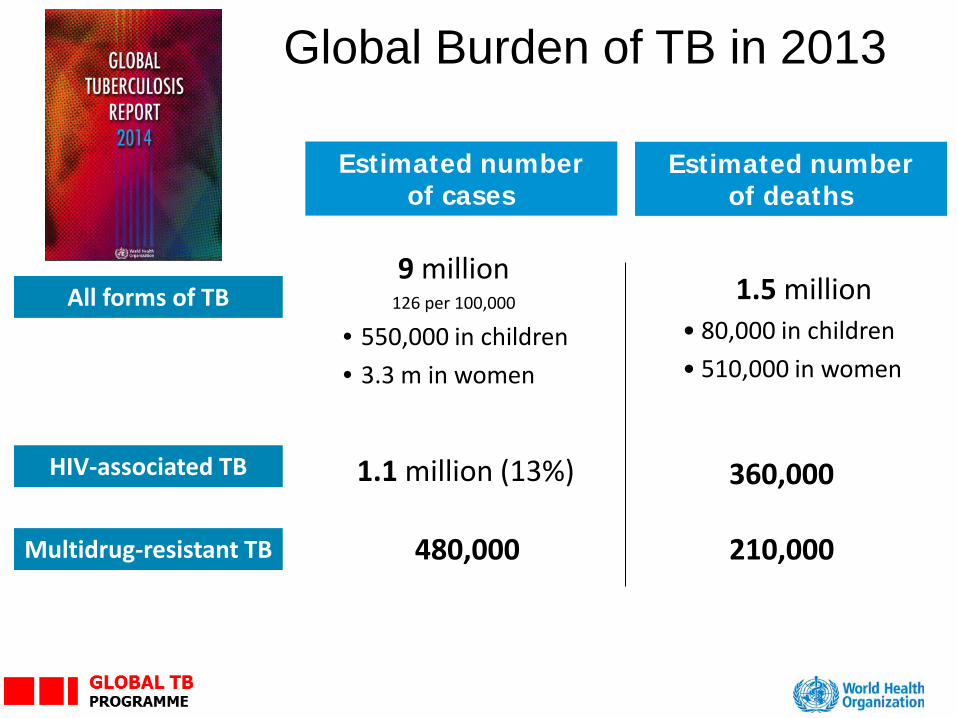
Estimated number of cases
Estimated number of deaths
1.5 million • 80,000 in children • 510,000 in women
9 million 126 per 100,000
• 550,000 in children • 3.3 m in women
480,000
All forms of TB
Multidrug-resistant TB
HIV-associated TB 1.1 million (13%) 360,000
Global Burden of TB in 2013
210,000
23/09/2015 Titolo Presentazione Pagina 4
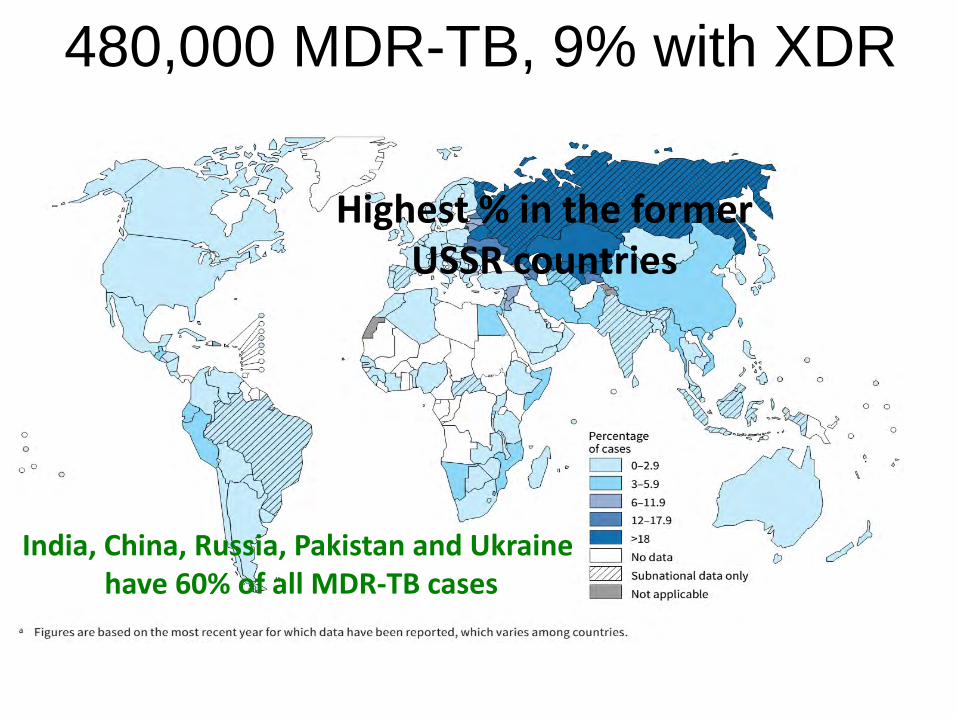
480,000 MDR-TB, 9% with XDR
India, China, Russia, Pakistan and Ukraine have 60% of all MDR-TB cases
Highest % in the former USSR countries
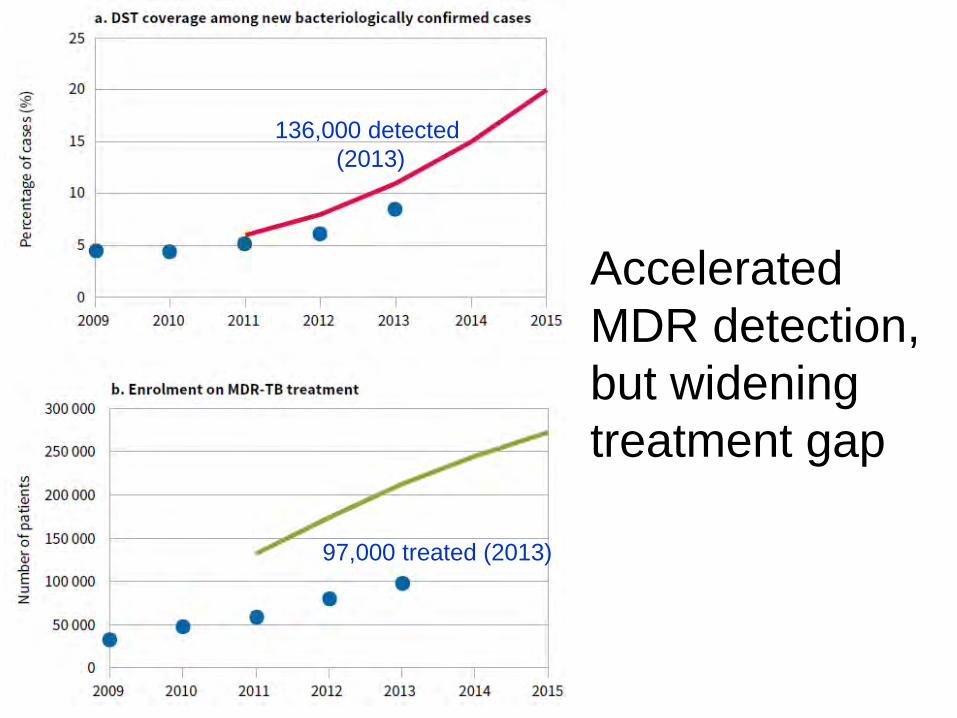
Accelerated MDR detection, but widening treatment gap
136,000 detected (2013)
97,000 treated (2013)
23/09/2015 Titolo Presentazione Pagina 8
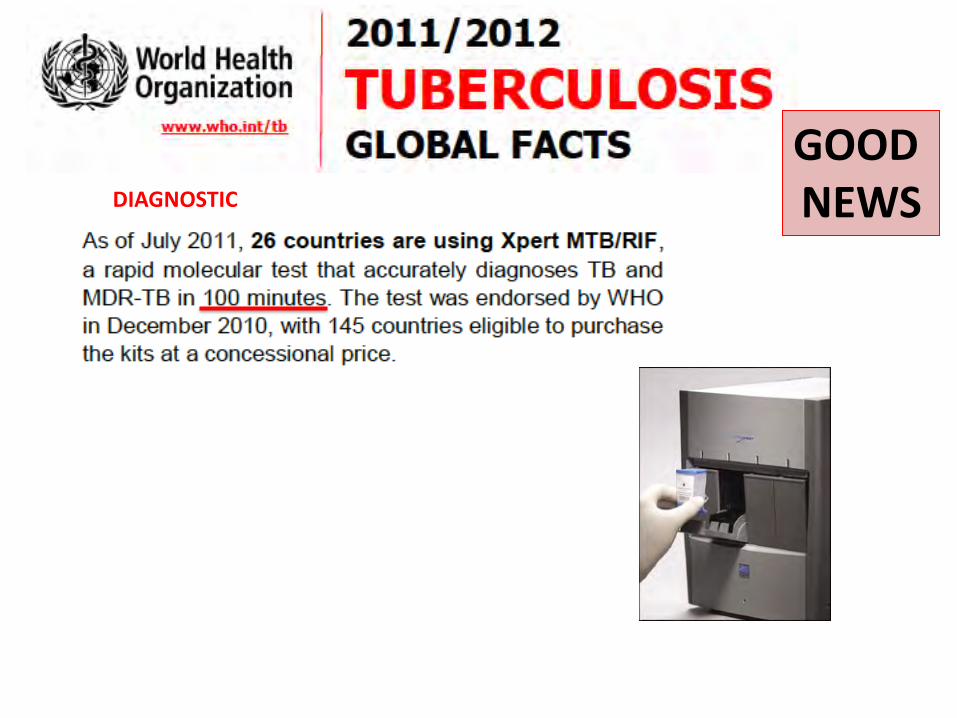
DIAGNOSTIC
GOOD NEWS
23/09/2015 Titolo Presentazione Pagina 9
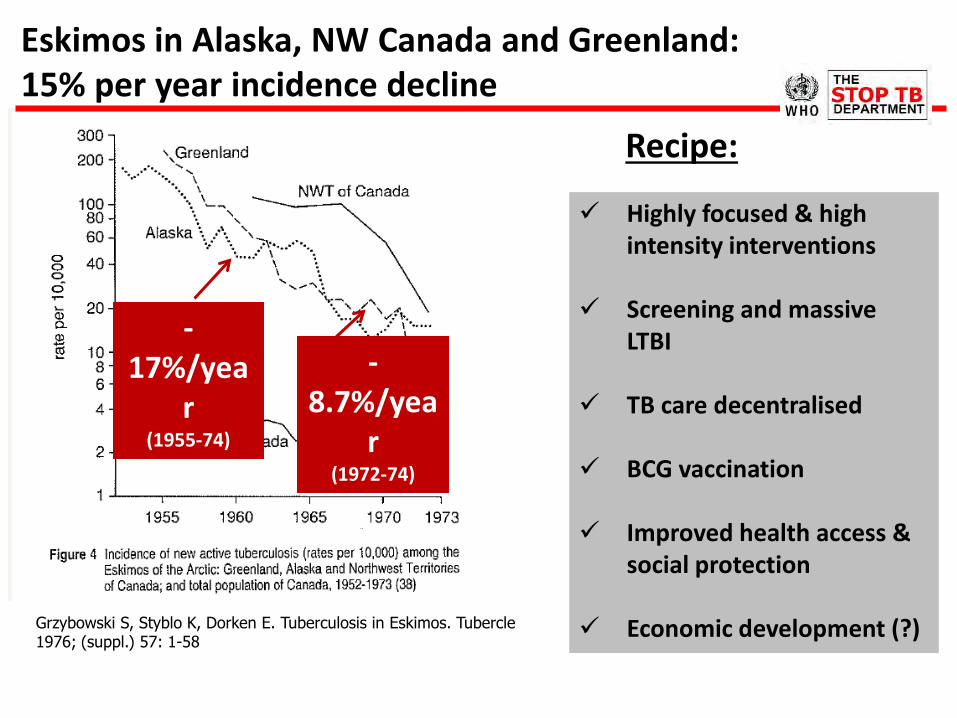
Eskimos in Alaska, NW Canada and Greenland: 15% per year incidence decline
Highly focused & high intensity interventions
Screening and massive LTBI
TB care decentralised
BCG vaccination
Improved health access &
social protection
Economic development (?)
Recipe:
-17%/yea
r (1955-74)
-8.7%/yea
r (1972-74)
Grzybowski S, Styblo K, Dorken E. Tuberculosis in Eskimos. Tubercle 1976; (suppl.) 57: 1-58

I
23/09/2015 Titolo Presentazione Pagina 11
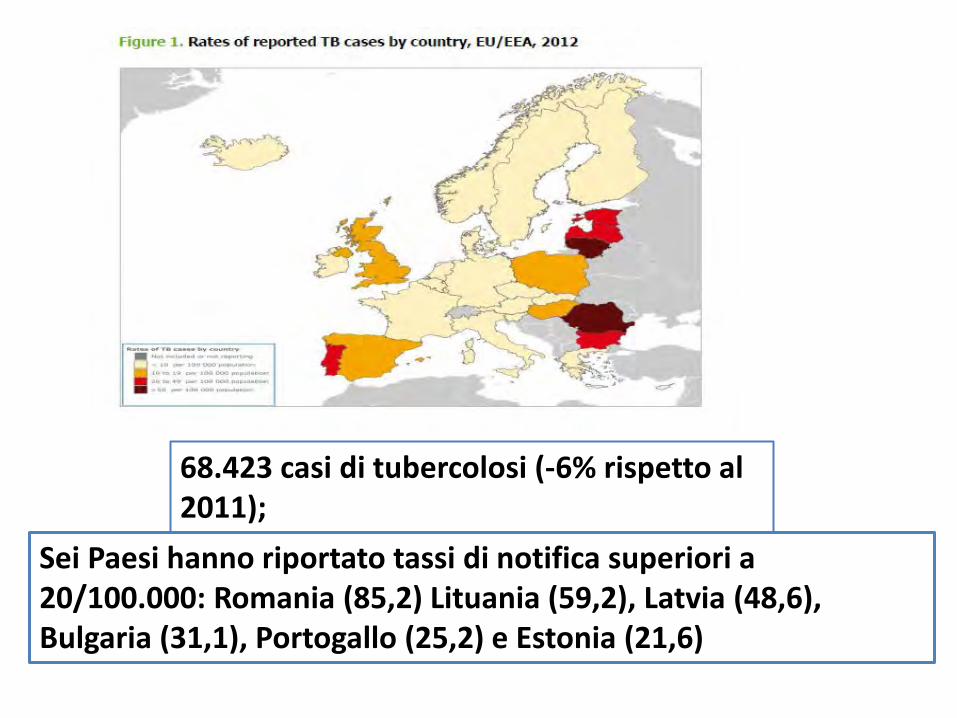
68.423 casi di tubercolosi (-6% rispetto al 2011); 13.5 casi/100.000 abitanti Sei Paesi hanno riportato tassi di notifica superiori a
20/100.000: Romania (85,2) Lituania (59,2), Latvia (48,6), Bulgaria (31,1), Portogallo (25,2) e Estonia (21,6)
13
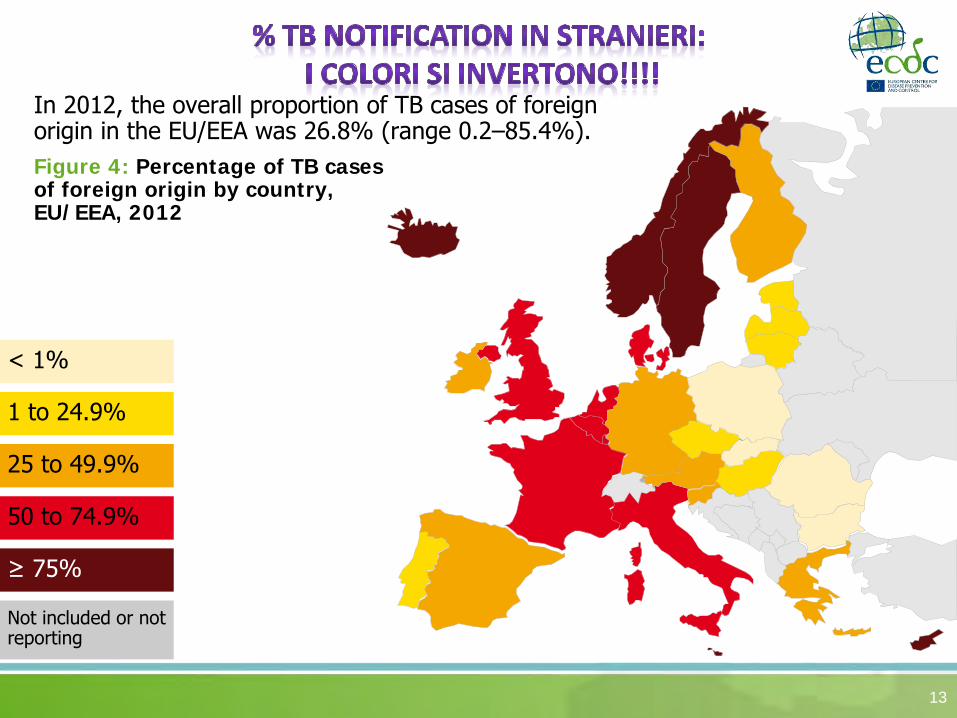
In 2012, the overall proportion of TB cases of foreign origin in the EU/EEA was 26.8% (range 0.2–85.4%). Figure 4: Percentage of TB cases of foreign origin by country, EU/EEA, 2012
25 to 49.9%
≥ 75%
1 to 24.9%
50 to 74.9%
< 1%
Not included or not reporting
Multidrug-resistant TB
14
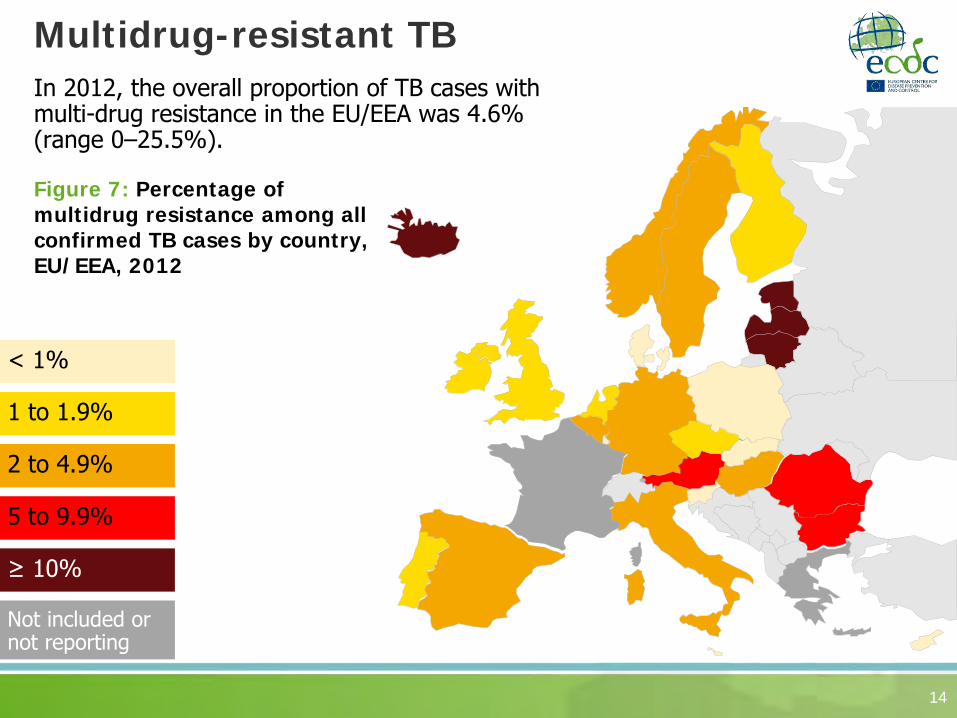
In 2012, the overall proportion of TB cases with multi-drug resistance in the EU/EEA was 4.6% (range 0–25.5%). Figure 7: Percentage of multidrug resistance among all confirmed TB cases by country, EU/EEA, 2012
2 to 4.9%
≥ 10%
1 to 1.9%
5 to 9.9%
< 1%
Not included or not reporting

I
23/09/2015 Titolo Presentazione Pagina 15
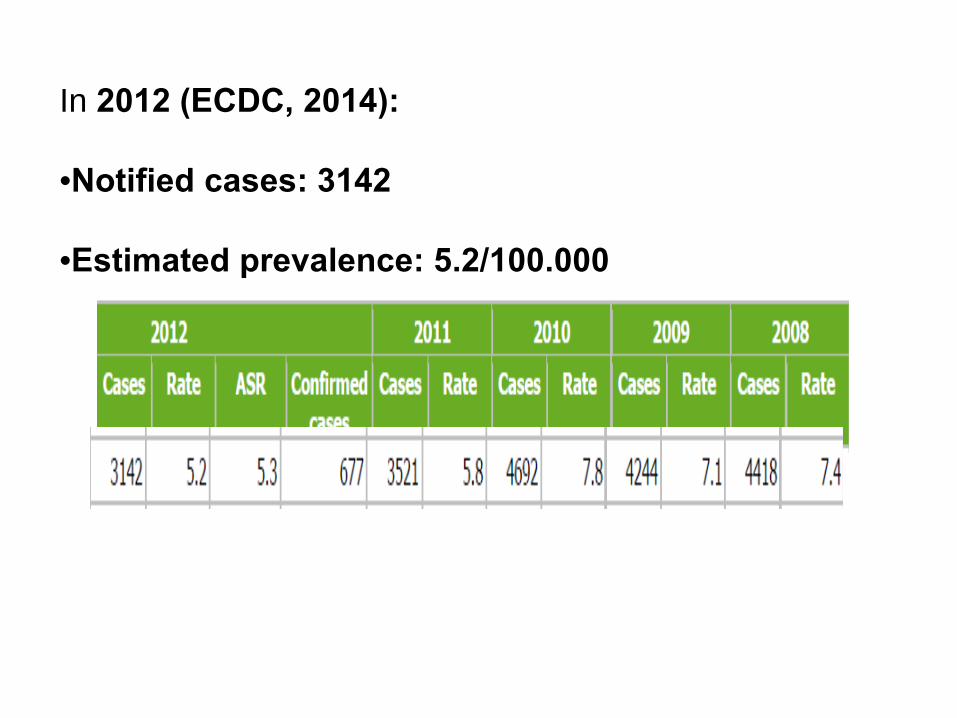
In 2012 (ECDC, 2014): •Notified cases: 3142 •Estimated prevalence: 5.2/100.000
23/09/2015 Titolo Presentazione Pagina 18
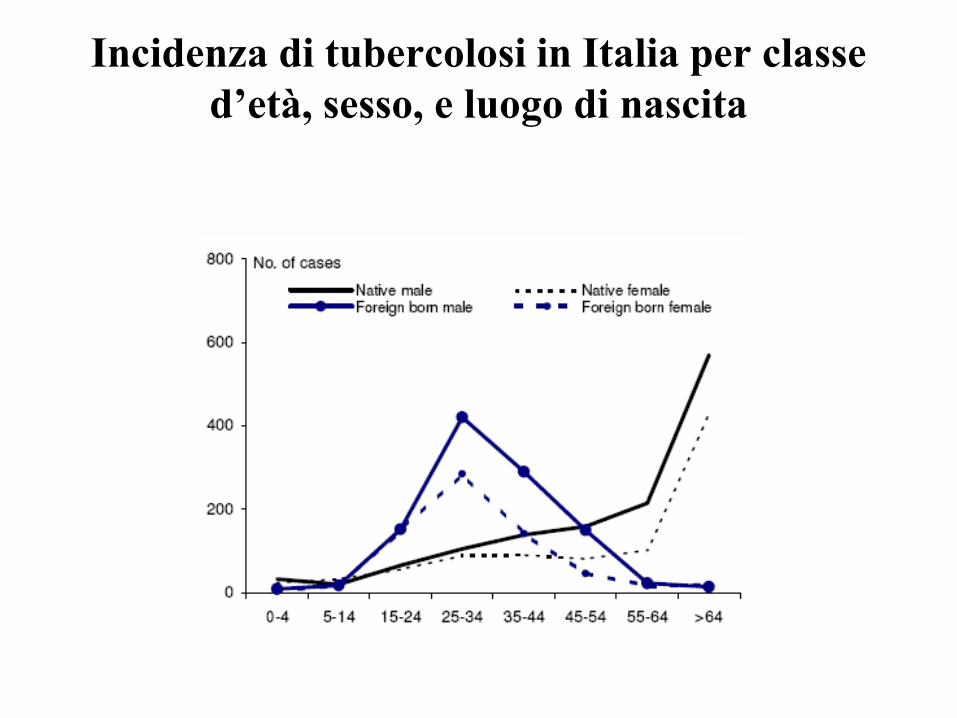
Incidenza di tubercolosi in Italia per classe d’età, sesso, e luogo di nascita
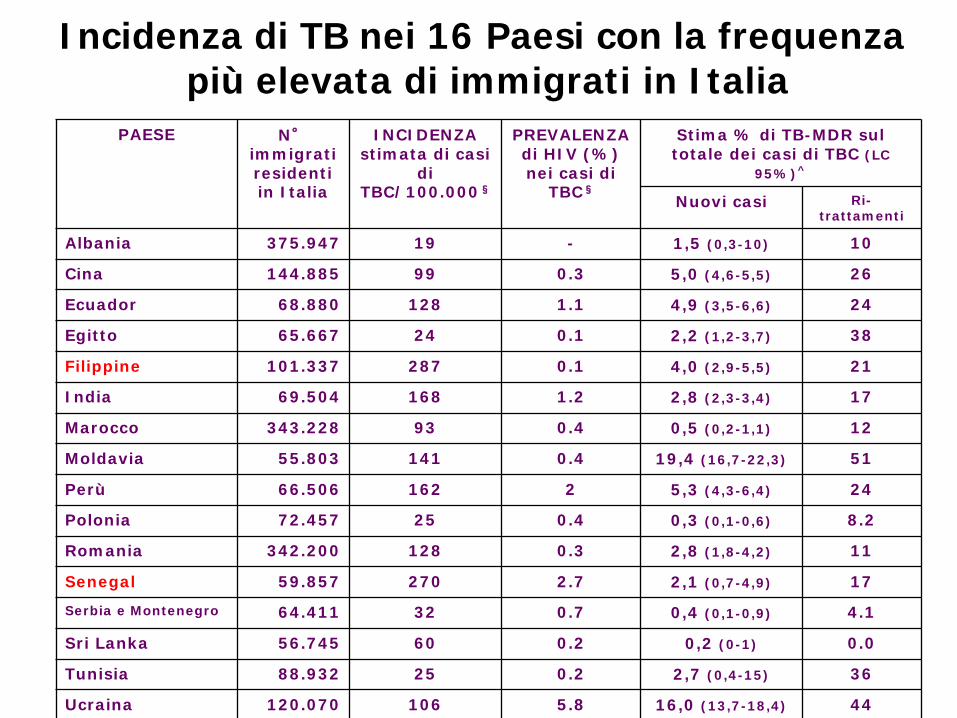
PAESE N° immigrati residenti in Italia
INCIDENZA stimata di casi
di TBC/100.000§
PREVALENZA di HIV (%) nei casi di
TBC§
Stima % di TB-MDR sul totale dei casi di TBC (LC
95%)^
Nuovi casi Ri-trattamenti
Albania 375.947 19 - 1,5 (0,3-10) 10
Cina 144.885 99 0.3 5,0 (4,6-5,5) 26
Ecuador 68.880 128 1.1 4,9 (3,5-6,6) 24
Egitto 65.667 24 0.1 2,2 (1,2-3,7) 38
Filippine 101.337 287 0.1 4,0 (2,9-5,5) 21
India 69.504 168 1.2 2,8 (2,3-3,4) 17
Marocco 343.228 93 0.4 0,5 (0,2-1,1) 12
Moldavia 55.803 141 0.4 19,4 (16,7-22,3) 51
Perù 66.506 162 2 5,3 (4,3-6,4) 24
Polonia 72.457 25 0.4 0,3 (0,1-0,6) 8.2
Romania 342.200 128 0.3 2,8 (1,8-4,2) 11
Senegal 59.857 270 2.7 2,1 (0,7-4,9) 17
Serbia e Montenegro 64.411 32 0.7 0,4 (0,1-0,9) 4.1
Sri Lanka 56.745 60 0.2 0,2 (0-1) 0.0
Tunisia 88.932 25 0.2 2,7 (0,4-15) 36
Ucraina 120.070 106 5.8 16,0 (13,7-18,4) 44
Incidenza di TB nei 16 Paesi con la frequenza più elevata di immigrati in Italia
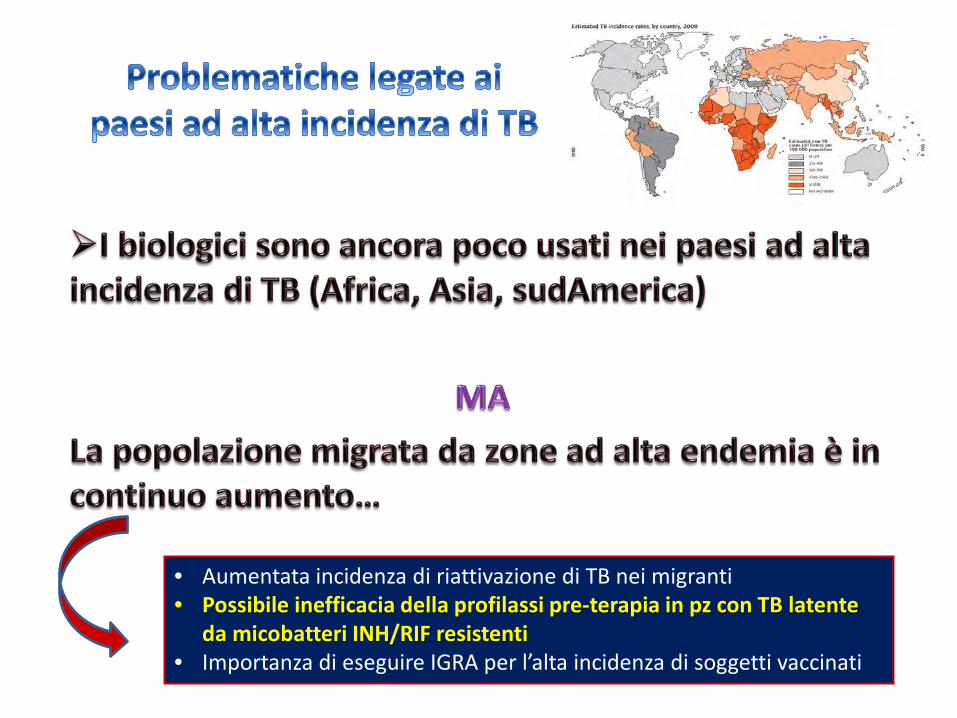
• Aumentata incidenza di riattivazione di TB nei migranti • Possibile inefficacia della profilassi pre-terapia in pz con TB latente
da micobatteri INH/RIF resistenti • Importanza di eseguire IGRA per l’alta incidenza di soggetti vaccinati
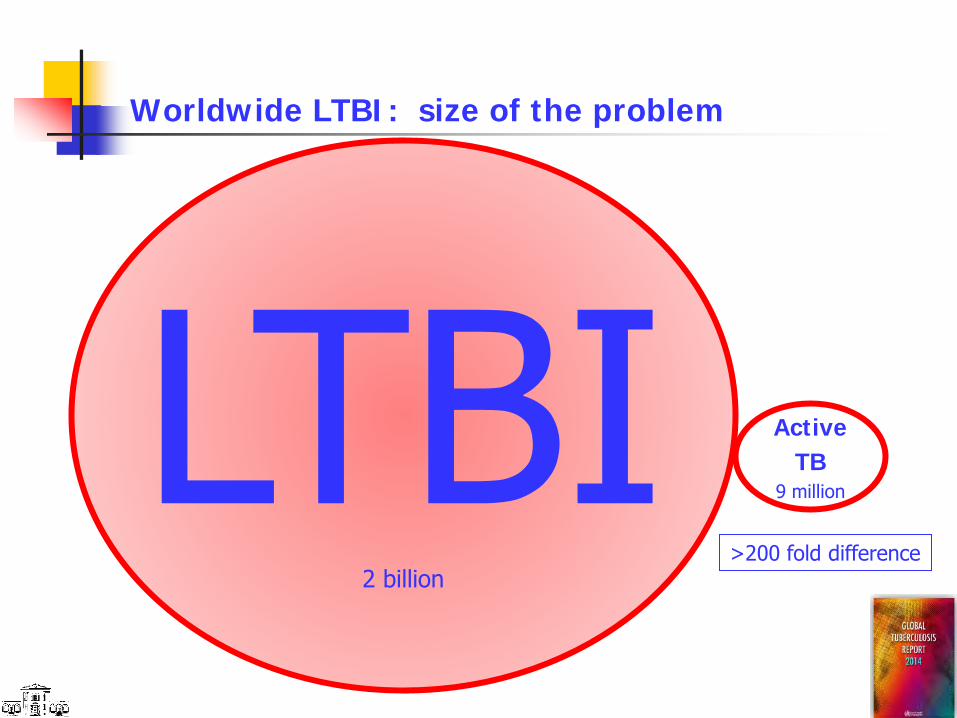
Worldwide LTBI: size of the problem
LTBI 2 billion
Active TB
9 million
>200 fold difference
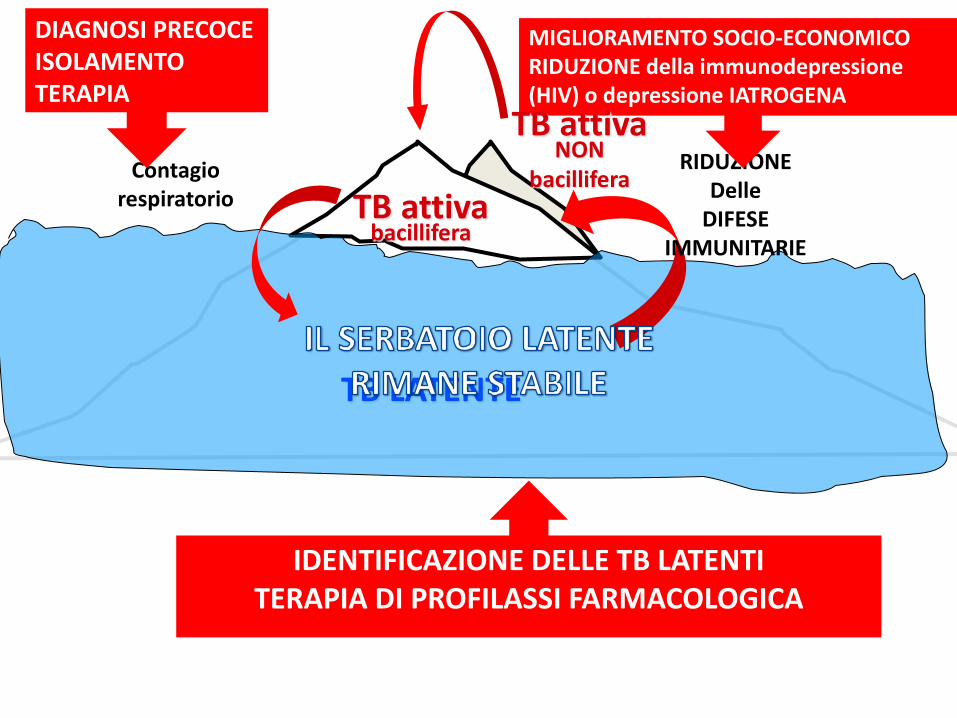
TB attiva bacillifera
TB LATENTE
Contagio respiratorio
RIDUZIONE Delle
DIFESE IMMUNITARIE
DIAGNOSI PRECOCE ISOLAMENTO TERAPIA
MIGLIORAMENTO SOCIO-ECONOMICO RIDUZIONE della immunodepressione (HIV) o depressione IATROGENA
TB attiva NON
bacillifera
IDENTIFICAZIONE DELLE TB LATENTI TERAPIA DI PROFILASSI FARMACOLOGICA
LTBI
x
From Goletti D
Persons at Risk for Developing TB Disease
• Those who have been recently infected • Those with clinical conditions that
increase their risk of progressing from LTBI to TB disease
Persons at high risk for developing TB disease fall into 2 categories
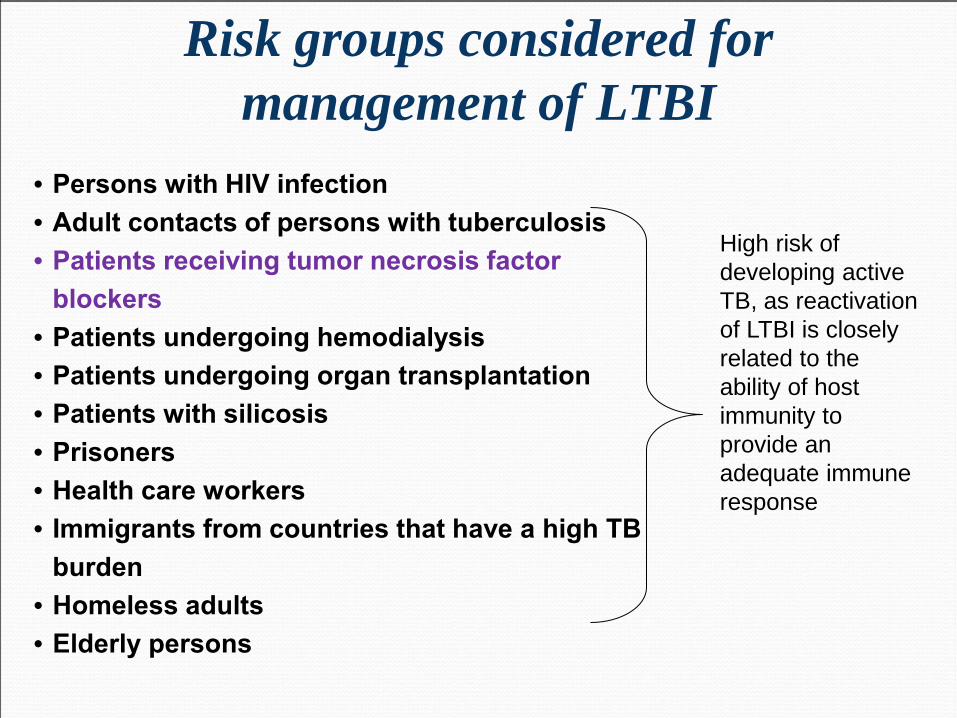
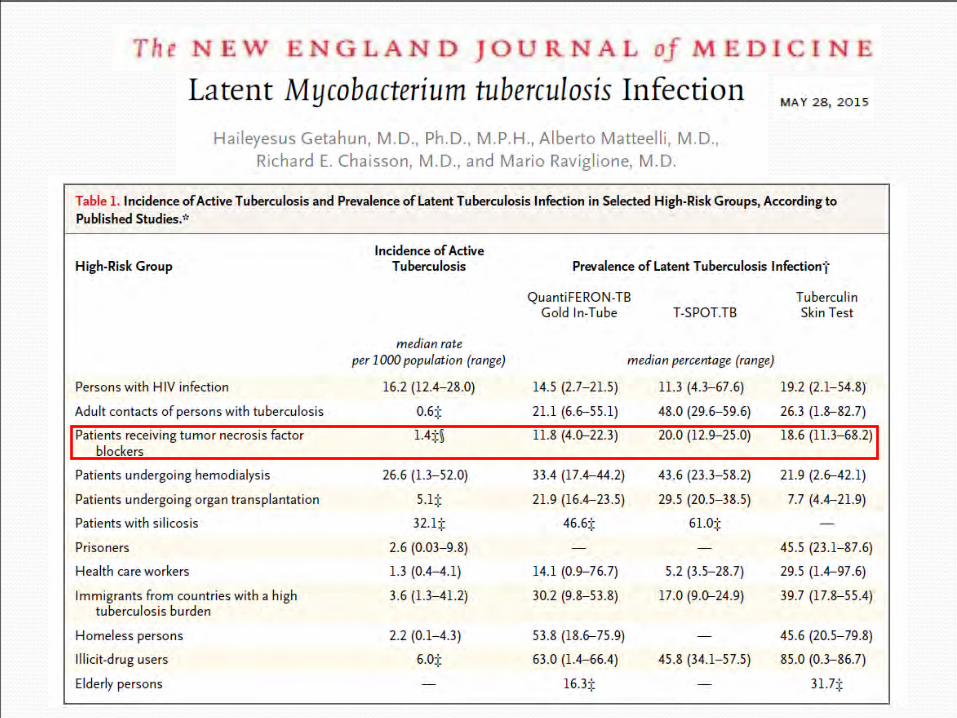
Risk groups considered for management of LTBI
• Persons with HIV infection • Adult contacts of persons with tuberculosis • Patients receiving tumor necrosis factor
blockers • Patients undergoing hemodialysis • Patients undergoing organ transplantation • Patients with silicosis • Prisoners • Health care workers • Immigrants from countries that have a high TB
burden • Homeless adults • Elderly persons
High risk of developing active TB, as reactivation of LTBI is closely related to the ability of host immunity to provide an adequate immune response
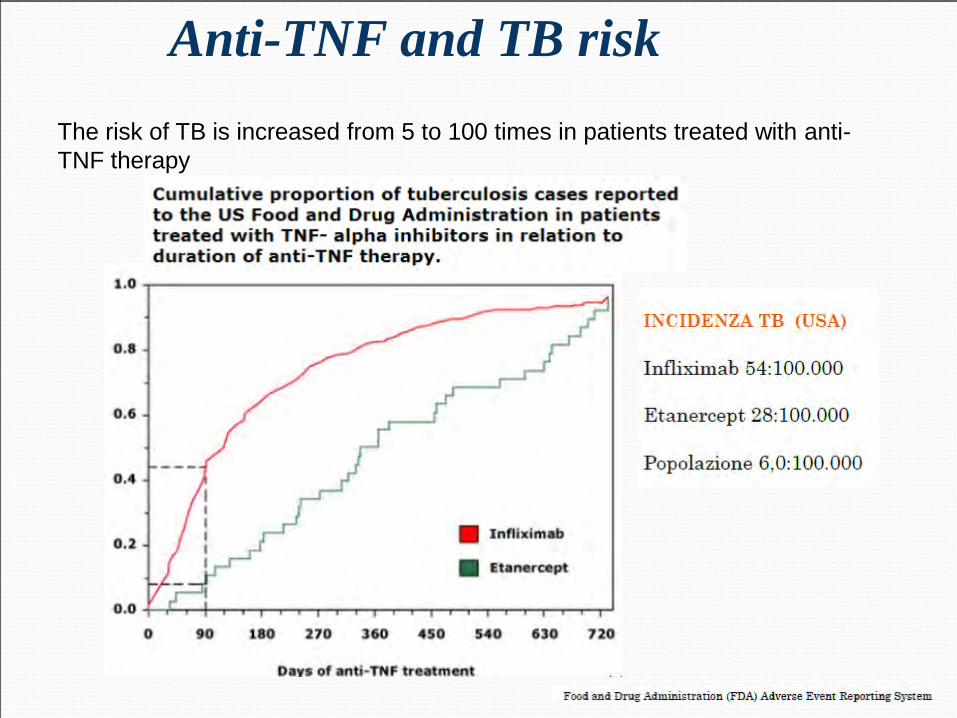
The risk of TB is increased from 5 to 100 times in patients treated with anti-TNF therapy
Anti-TNF and TB risk
Clin Microbiol Infect 2007
Screening for latent TB before starting TNF-α blocking treatment is mandatory for clinicians
Prevention efforts have partially decreased the risk of TB in this setting
However, optimal screening methods for latent TB represent an area of evolving controversy and active investigation
Risk of TB reactivation anti-TNF-α
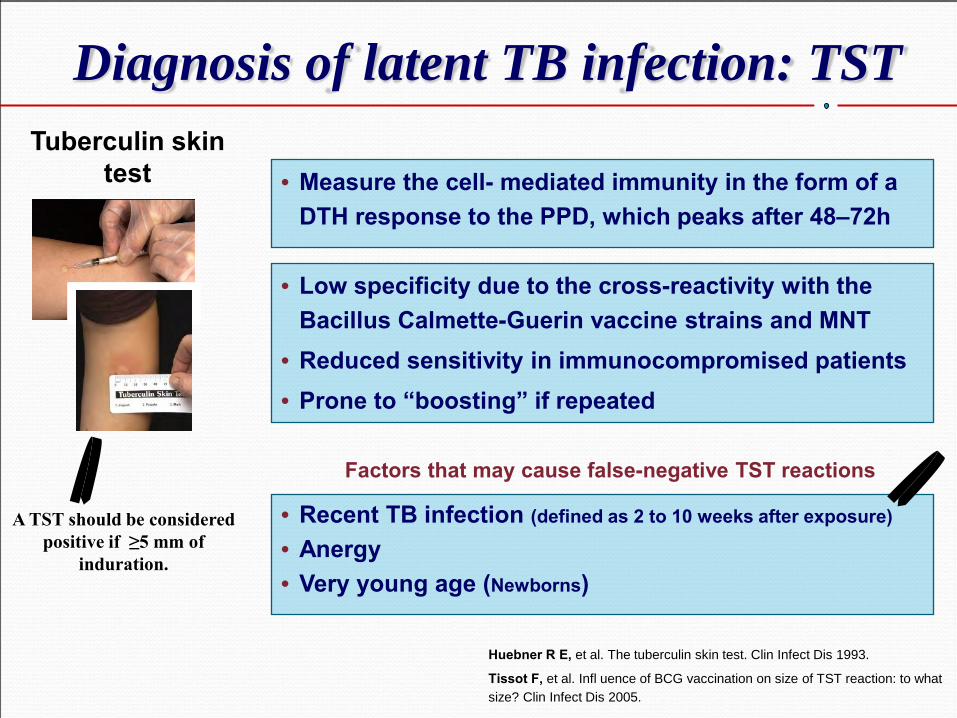
Tuberculin skin test
Diagnosis of latent TB infection: TST
• Low specificity due to the cross-reactivity with the Bacillus Calmette-Guerin vaccine strains and MNT
• Reduced sensitivity in immunocompromised patients • Prone to “boosting” if repeated
Huebner R E, et al. The tuberculin skin test. Clin Infect Dis 1993.
Tissot F, et al. Infl uence of BCG vaccination on size of TST reaction: to what size? Clin Infect Dis 2005.
• Measure the cell- mediated immunity in the form of a DTH response to the PPD, which peaks after 48–72h
A TST should be considered positive if ≥5 mm of
induration.
• Recent TB infection (defined as 2 to 10 weeks after exposure)
• Anergy • Very young age (Newborns)
Factors that may cause false-negative TST reactions
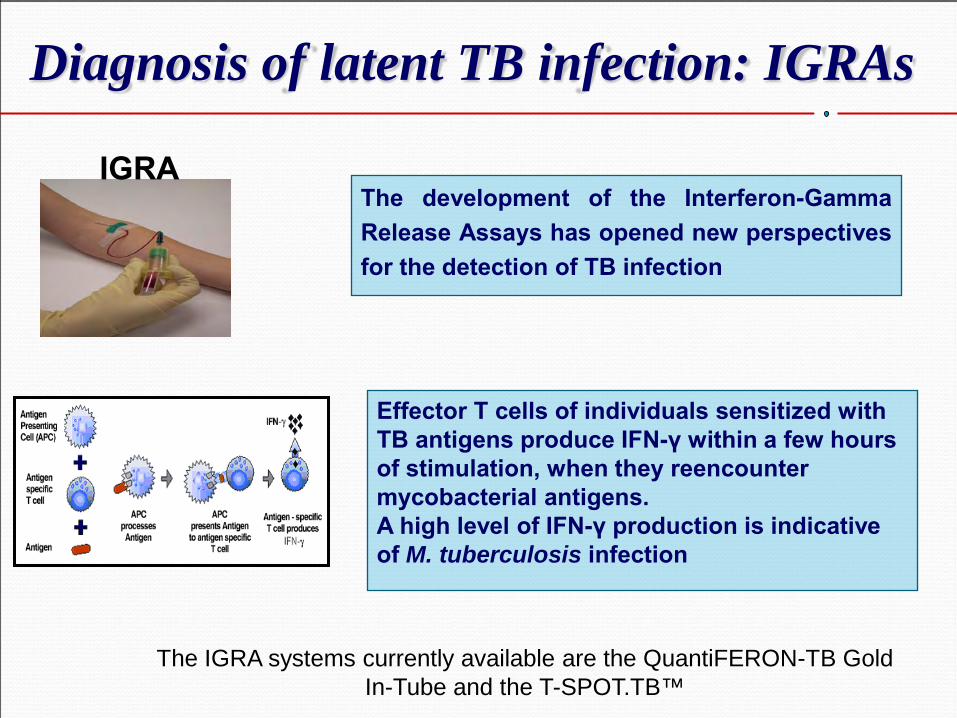
IGRA The development of the Interferon-Gamma Release Assays has opened new perspectives for the detection of TB infection
The IGRA systems currently available are the QuantiFERON-TB Gold In-Tube and the T-SPOT.TB™
Diagnosis of latent TB infection: IGRAs
Effector T cells of individuals sensitized with TB antigens produce IFN-γ within a few hours of stimulation, when they reencounter mycobacterial antigens. A high level of IFN-γ production is indicative of M. tuberculosis infection
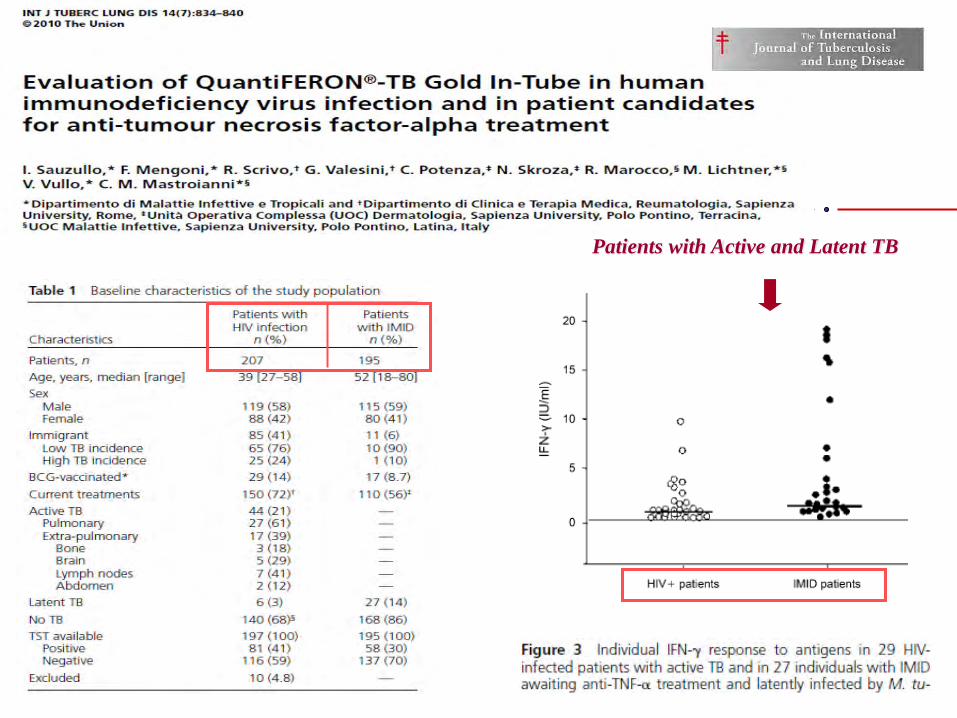
Patients with Active and Latent TB
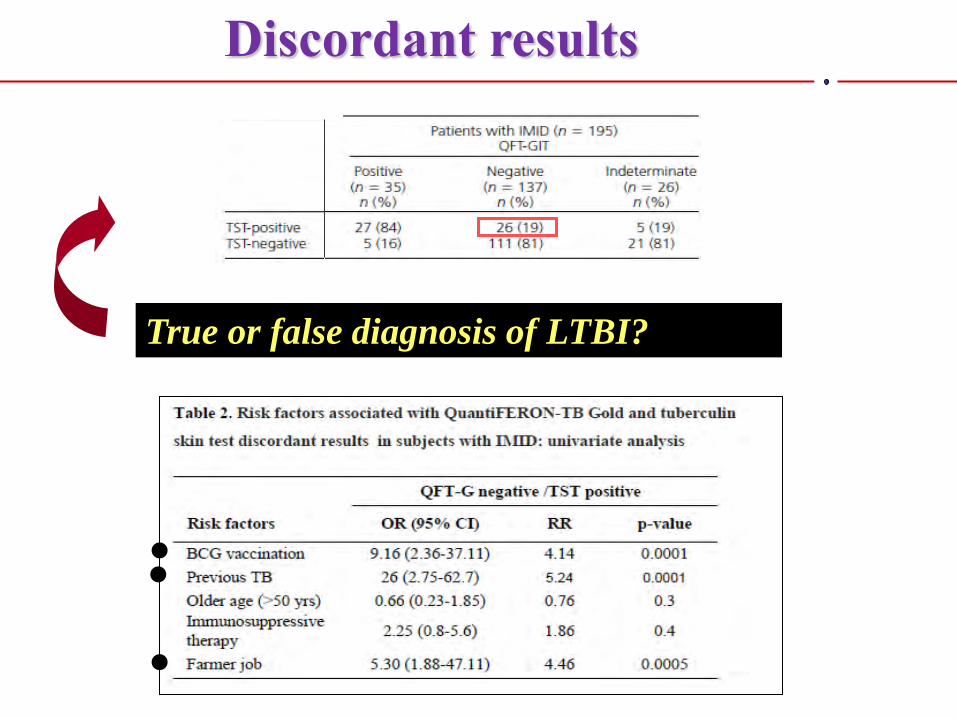
Discordant results
True or false diagnosis of LTBI?
The clinical use of repeated blood tests and the correct interpretation of individual IFN-gamma changes could be
useful in identifying possible cases of LTBI reactivation or newly acquired tuberculosis
infection during longterm anti-TNF treatment
Multi-functional analysis of CD4+ T cells could be useful for ruling out TB infection in patients classified at screening as LTBI-negative but who show IGRA fluctuations under long term TNF antagonist treatment.
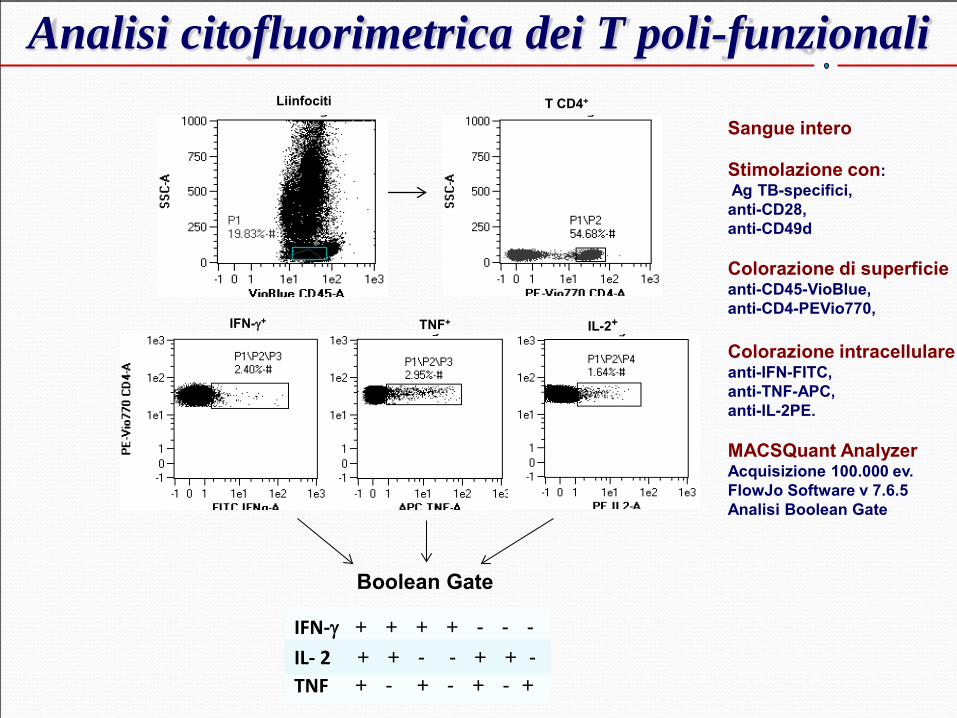
Analisi citofluorimetrica dei T poli-funzionali
Boolean Gate
IFN-γ + + + + - - -
TNF + - + - + - + IL- 2 + + - - + + -
Liinfociti T CD4+
TNF+ IL-2+ IFN-γ+
Sangue intero Stimolazione con: Ag TB-specifici, anti-CD28, anti-CD49d Colorazione di superficie anti-CD45-VioBlue, anti-CD4-PEVio770, Colorazione intracellulare anti-IFN-FITC, anti-TNF-APC, anti-IL-2PE. MACSQuant Analyzer Acquisizione 100.000 ev. FlowJo Software v 7.6.5 Analisi Boolean Gate
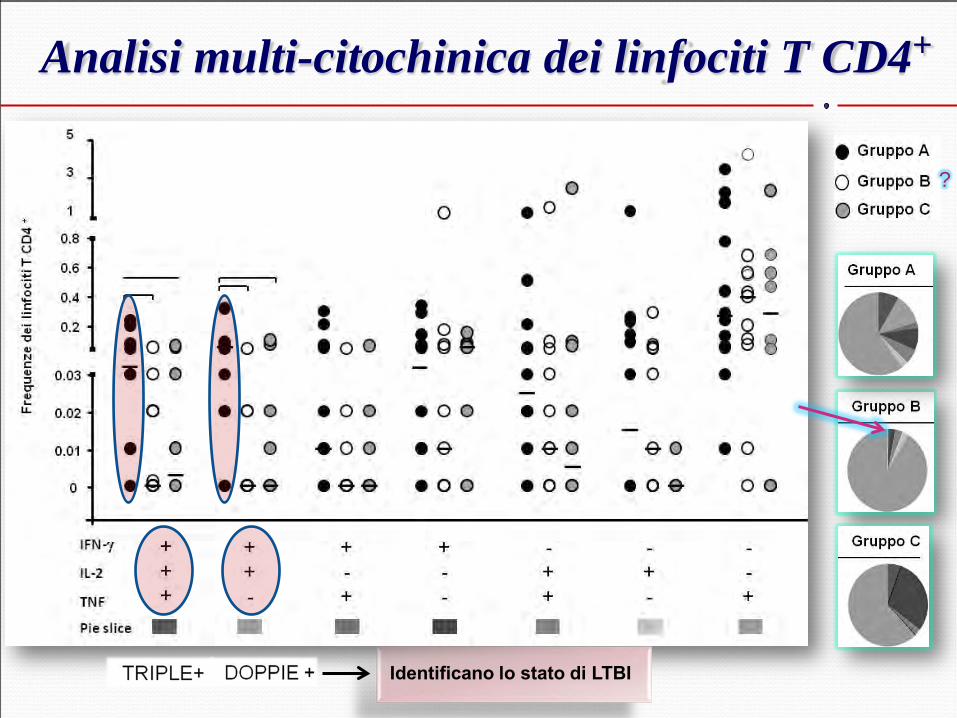
Analisi multi-citochinica dei linfociti T CD4+
Identificano lo stato di LTBI
?

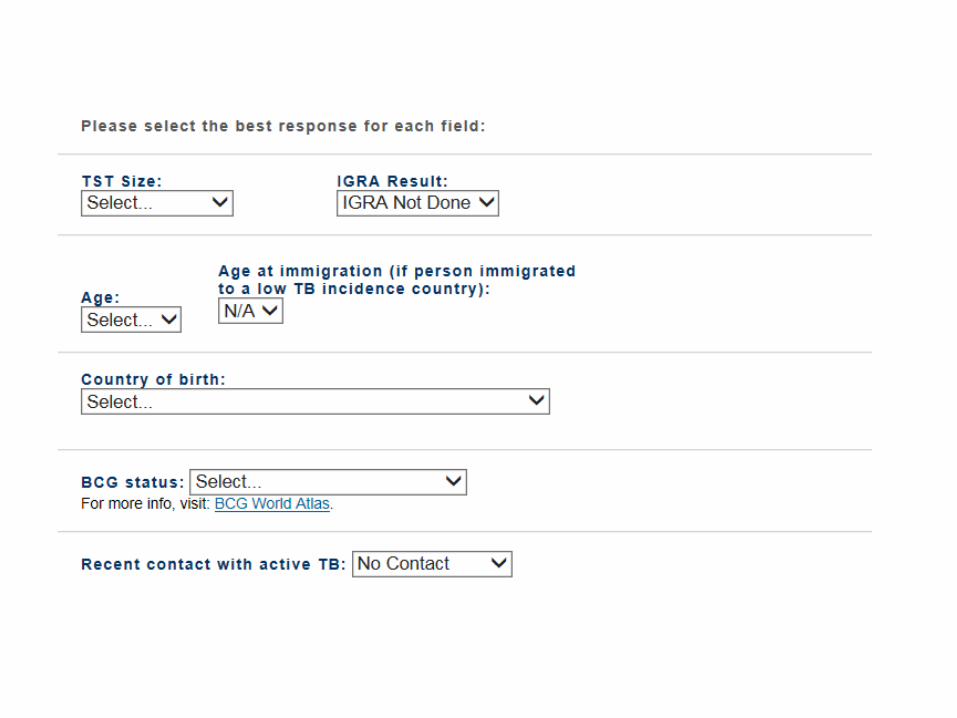
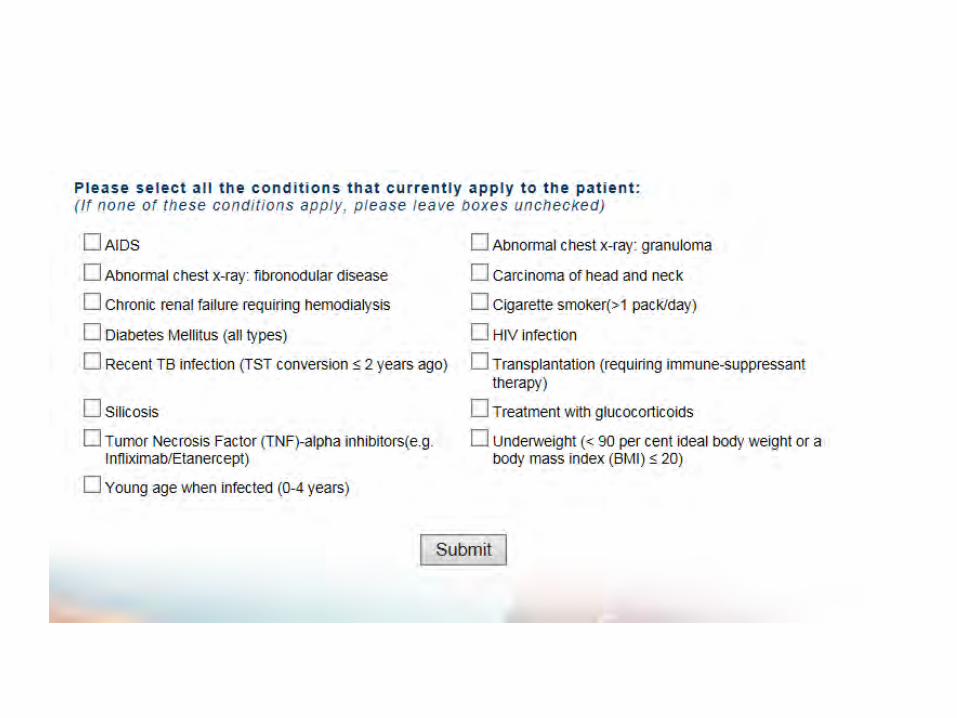
Algoritmo per TB screening nei pazienti candidati al trattamento con anti-TNF-α
(‘triple-testing’ approach”) Storia clinica, identificazione fattori di rischio per TB
(provenienza zona ad alta endemia, contatto con TB attiva, precedente diagnosi di TB latente, tossicodipendente, homeless, reclusione, Rx indicativa di pregressa TB)
Test diagnostici per LTBI (TST + IGRAs)
Rx torace (se alterazioni compatibili con TB
escludere TB attiva, es. espettorato )
Giudizio clinico Se sospetto di LTBI sulla base dello screening,
iniziare terapia con INH o altro farmaco prima dell’inizio con anti-TNF-α
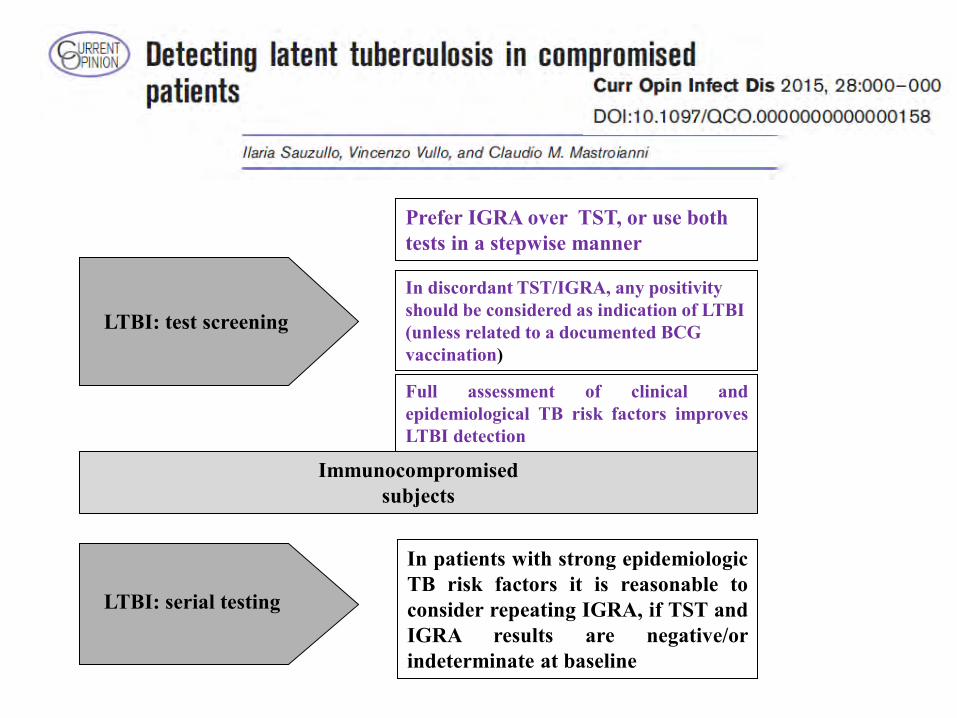
In discordant TST/IGRA, any positivity should be considered as indication of LTBI (unless related to a documented BCG vaccination)
Prefer IGRA over TST, or use both tests in a stepwise manner
In patients with strong epidemiologic TB risk factors it is reasonable to consider repeating IGRA, if TST and IGRA results are negative/or indeterminate at baseline
Immunocompromised subjects
LTBI: test screening
LTBI: serial testing
Full assessment of clinical and epidemiological TB risk factors improves LTBI detection
[www.tstin3d.com]