Embed Size (px)
Citation preview

Methods
• Patients: Unresectable GBM PS 0-2, MMS≥25• Centralized radiological Review RANO criteria• Centralized pathological Review: MGMT tissue &
MGMT serum• RT planning using post neoadjuvant MRI with GD T1
and FLAIR sequences• Endpoints:
– Primary: Overall Response Rate after 2 pre-RT cycles powered to detect a 30% difference between arms (α and β errors of 0.05 and 0.20).
– Secondary:1.Toxicity2.Percentage of neurological deterioration
before RT3.Progression free survival and Overall survival4.Quality of Life differences5.MGMT Serum vs Tissue to predict results
Salvador Villà et alAbst 1015

COI
• The project was funded by the Spanish Ministery of Science and Innovation: Projects on non-commercial investigation of human medications, Instituto de Salud Carlos III (ISCIII). Project EC08/00071
• ROCHE provided support for data collection• MSD provided pre-radiotherapy temozolomide
and funds for MGMT assessment• S. Villà: advisory boards, ROCHE

103 GBM patients registered
Centralized Randomization (1:1)
51 allocated to TMZ arm 48 allocated to BEV arm
45 started TMZ
48 started BEV & TMZ
TMZ /RDT per protocol 22 (48.9%)
BEV & TMZ & RDT per protocol 32 (66.7%)
Adjuvant TMZ completed 6 c: 6.7% completed ≥3 c: 15.6%
Adjuvant TMZ completed 6 c: 10.4% completed ≥3 c: 20.8%
3 withdrawal IC2 P before inclusion1 did not meet inclusion criteria
2 GBM not confirmed1 hemorrhage on MRI1 refusal
30 received 2 c37 completed 2 c9 progression
5 toxicity1 refusal
3 progression8 toxicity
Other treatment off-protocol12
(26.7%)Palliative Care
5 (10.4%)
2 (4.4%) RDT 1 (2.1%)
8 (17.8%)
RDT&TMZ 6 (12.5%)
1 *(2.2%)
Other 4 (8.3%)*more than one treatment
Salvador Villà et al Abst 1015

BEV-related Toxicity in Neoadjuvant Phase
TMZ arm BEV arm
All grade
s
Grade 3 & 4
Grade 5
All grade
s
Grade 3 & 4
Grade 53
patients
HTA - - - 8.4 4.2 -
Hemorrhage 2.2 - - 10.4 2.1 -
CNS hemorrhage
- - - 8.4 2.1 4.2
Arterial thrombosis
2.2 2.2 - - - -
Venous thrombosis
6.6 2.4 - 4.2 4.2 -
Digestive perforation
- - - 4.2 2.1 2.1To be added 2 patients more died in arm TMZ+BEV because diarrhea and pancytopenia
Salvador Villà et al Abst 1015

Endpoint resultsEndpoint TMZ Arm BEV Arm p
Neurological deterioration before RDT
22 (48.9%) 10 (20.8%) 0.004
Patients with 2 cycles pre-RDT 30 (66%) 37 (77%) 0.18
Patients who received full pre-specified protocol (RDT&TMZ)
22 (48.9%) 32 (66.7%) 0.08
Response PR+SD RANO 11 (26.1) 28 (65.1) 0.001
PFS (m, 95% CI) 2.2 (2.1-2.5) 4.8 (3.6-6.1) HR:0.79 (0.52-1.2) p=0.28
OS (m, 95% CI) 7.7 (5.7-14.5) 10.8 (7-14.5) HR:0.71 (0.46-
1.10) p=0.12
1 year survival 29.6 % 48.9% p=0.06PFS all pts: 2.8 m (95% CI, 0.9-4.7) OS all pts: 9.1 m (95% CI, 6.8-11-3)Salvador Villà et al
Abst 1015

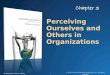
PFS and OS by MGMT status
MGMT STATUS PFS (mo) HR (95%
CI) P OS (mo) HR (95% CI) P
NOT METHYLATED
2.3 (2.0-2.5) 0.49
(0.28-0.87)
0.014.5 (2.3-6.7)
0.36 (0.19-0.67) 0.001
METHYLATED 4.7 (4.1-5.2)
12.2 (8.7-15.6)
PFSOS

Conclusions
• Addition of BEV significantly improved ORR (primary endpoint):– PR in 7.1% of p in the TMZ Arm vs 25.6% in the BEV Arm
(p=0.001)– clinical benefit (PR + SD) in 26.1% vs 65%
• Addition of BEV also improved other measures of benefit:– Less pre-radiotherapy neurological deterioration (38.9% vs.
20.8%; p=0.004)– Higher rate of completion of pre-specified protocol (58.9% vs.
66.7%; p=0.08)• No significant differences in PFS, OS and 1-y survival were
observed• Neoadjuvant with TMZ alone is not advisable• More toxicity in the BEV Arm • MGMT methylation was associated with longer PFS and
OS
Salvador Villà et al Abst 1015