Embed Size (px)
Citation preview
1
Multidisciplinary and Multimodal Approach
To the Pre-Operative Diagnosis
of Pancreatic Cysts
Martha Bishop Pitman, M.D.Director of Cytopathology
Massachusetts General Hospital
Professor of Pathology
Harvard Medical School
Boston, MA
Pancreatic Cysts
• 1.2% of the general population
• 7-8% of the elderly
• 10% of pancreatic neoplasms
• Benign, premalignant and malignant
• Most patients are asymptomatic
• Management conundrum
• Accurate diagnosis requires a multidisciplinary
and multimodal team approach
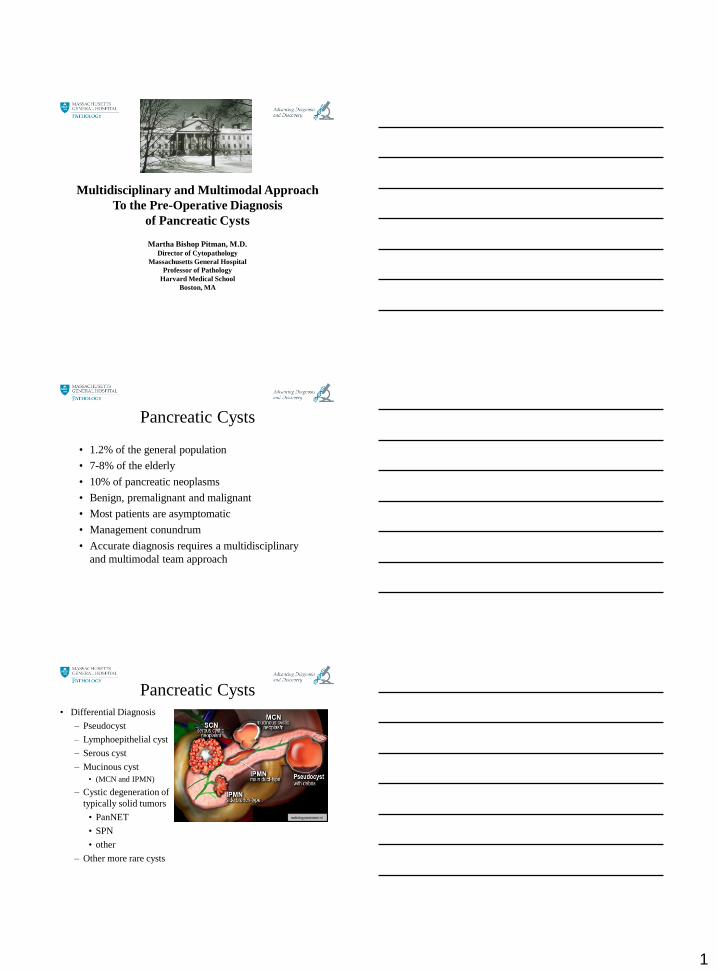
Pancreatic Cysts• Differential Diagnosis
– Pseudocyst
– Lymphoepithelial cyst
– Serous cyst
– Mucinous cyst
• (MCN and IPMN)
– Cystic degeneration of
typically solid tumors
• PanNET
• SPN
• other
– Other more rare cysts
radiologyassistant.nl
2
Management Options
• Surgical
– Distal pancreatectomy
– Middle pancreatectomy
– Pancreatoduodenectomy (Whipple)
• Medical
– Drain
– Ablate
• Observation
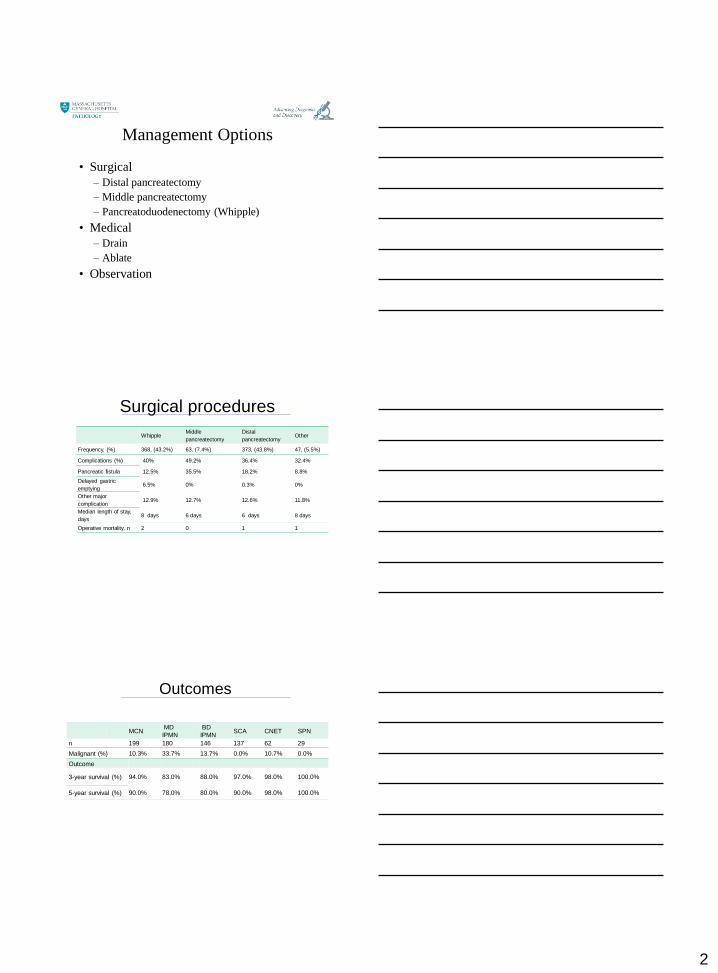
Surgical procedures
WhippleMiddle
pancreatectomy
Distal
pancreatectomyOther
Frequency, (%) 368, (43.2%) 63, (7.4%) 373, (43.8%) 47, (5.5%)
Complications (%) 40% 49.2% 36.4% 32.4%
Pancreatic fistula 12.5% 35.5% 18.2% 8.8%
Delayed gastric
emptying6.5% 0% 0.3% 0%
Other major
complication12.9% 12.7% 12.6% 11.8%
Median length of stay,
days8 days 6 days 6 days 8 days
Operative mortality, n 2 0 1 1
MCN MD
IPMN
BD
IPMN SCA CNET SPN
n 199 180 146 137 62 29
Malignant (%) 10.3% 33.7% 13.7% 0.0% 10.7% 0.0%
Outcome
3-year survival (%) 94.0% 83.0% 88.0% 97.0% 98.0% 100.0%
5-year survival (%) 90.0% 78.0% 80.0% 90.0% 98.0% 100.0%
Outcomes
3
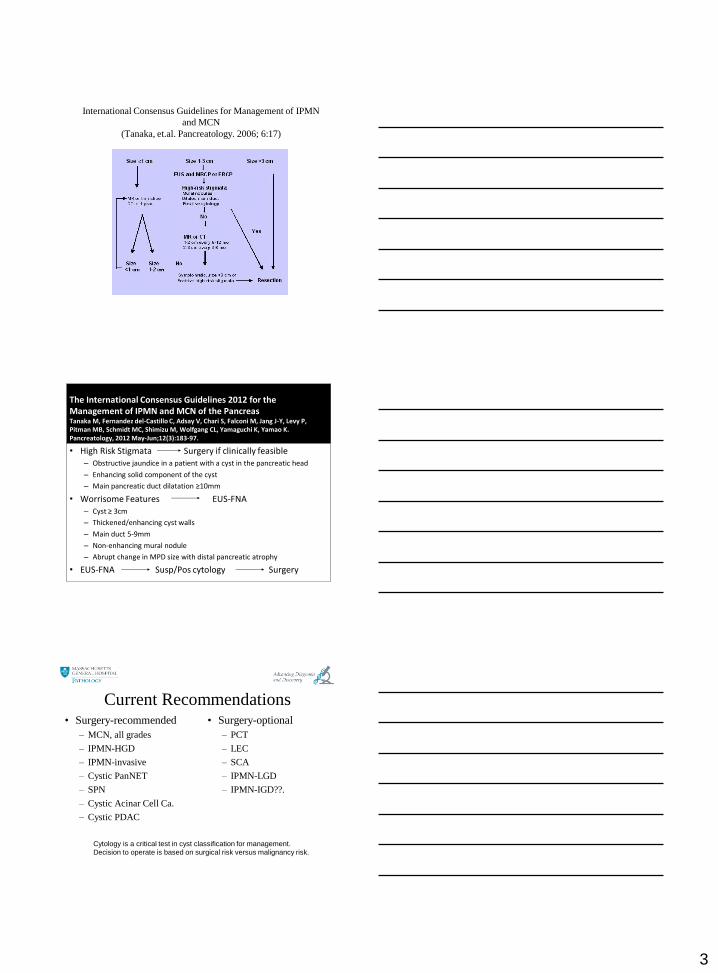
International Consensus Guidelines for Management of IPMN
and MCN
(Tanaka, et.al. Pancreatology. 2006; 6:17)
The International Consensus Guidelines 2012 for the Management of IPMN and MCN of the PancreasTanaka M, Fernandez del-Castillo C, Adsay V, Chari S, Falconi M, Jang J-Y, Levy P, Pitman MB, Schmidt MC, Shimizu M, Wolfgang CL, Yamaguchi K, Yamao K.Pancreatology, 2012 May-Jun;12(3):183-97.
• High Risk Stigmata Surgery if clinically feasible– Obstructive jaundice in a patient with a cyst in the pancreatic head
– Enhancing solid component of the cyst
– Main pancreatic duct dilatation ≥10mm
• Worrisome Features EUS-FNA– Cyst ≥ 3cm
– Thickened/enhancing cyst walls
– Main duct 5-9mm
– Non-enhancing mural nodule
– Abrupt change in MPD size with distal pancreatic atrophy
• EUS-FNA Susp/Pos cytology Surgery
Current Recommendations• Surgery-optional
– PCT
– LEC
– SCA
– IPMN-LGD
– IPMN-IGD??.
• Surgery-recommended
– MCN, all grades
– IPMN-HGD
– IPMN-invasive
– Cystic PanNET
– SPN
– Cystic Acinar Cell Ca.
– Cystic PDAC
Cytology is a critical test in cyst classification for management.
Decision to operate is based on surgical risk versus malignancy risk.
4
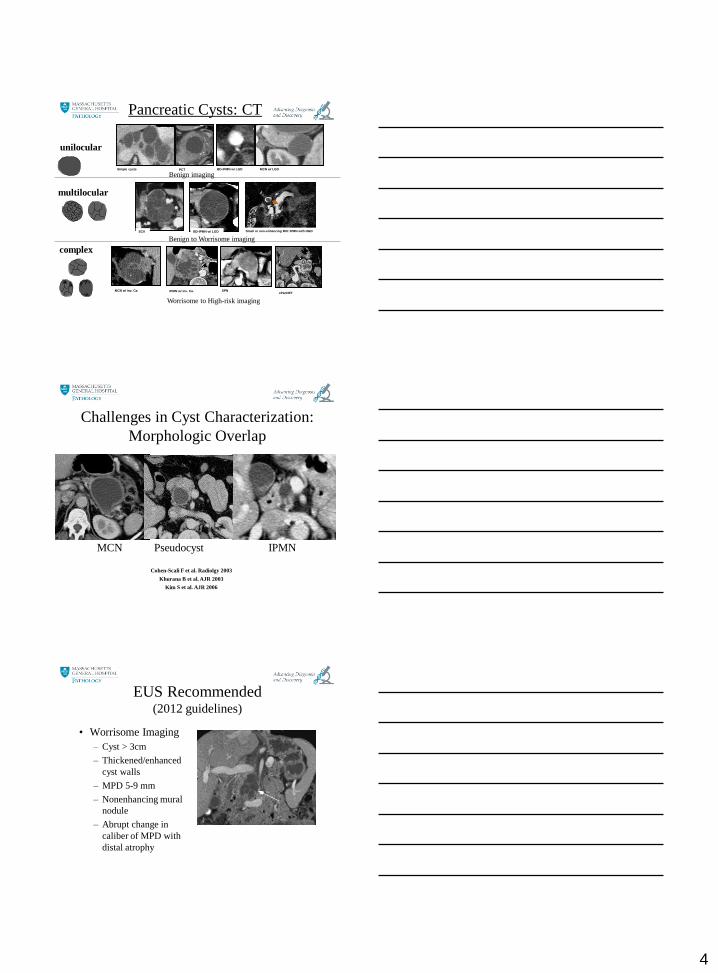
Pancreatic Cysts: CT
Benign to Worrisome imaging
Worrisome to High-risk imaging
unilocular
multilocular
complex
Benign imagingSimple cysts PCT BD-IPMN w/ LGD MCN w/ LGD
SCA BD-IPMN w/ LGD
MCN w/ inv. Ca. IPMN w/ inv. Ca.
Small or non-enhancing MN: IPMN with HGD
SPNcPanNET
MCN Pseudocyst IPMN
Cohen-Scali F et al. Radiolgy 2003
Khurana B et al. AJR 2003
Kim S et al. AJR 2006
Challenges in Cyst Characterization:
Morphologic Overlap
EUS Recommended(2012 guidelines)
• Worrisome Imaging
– Cyst > 3cm
– Thickened/enhanced
cyst walls
– MPD 5-9 mm
– Nonenhancing mural
nodule
– Abrupt change in
caliber of MPD with
distal atrophy
5
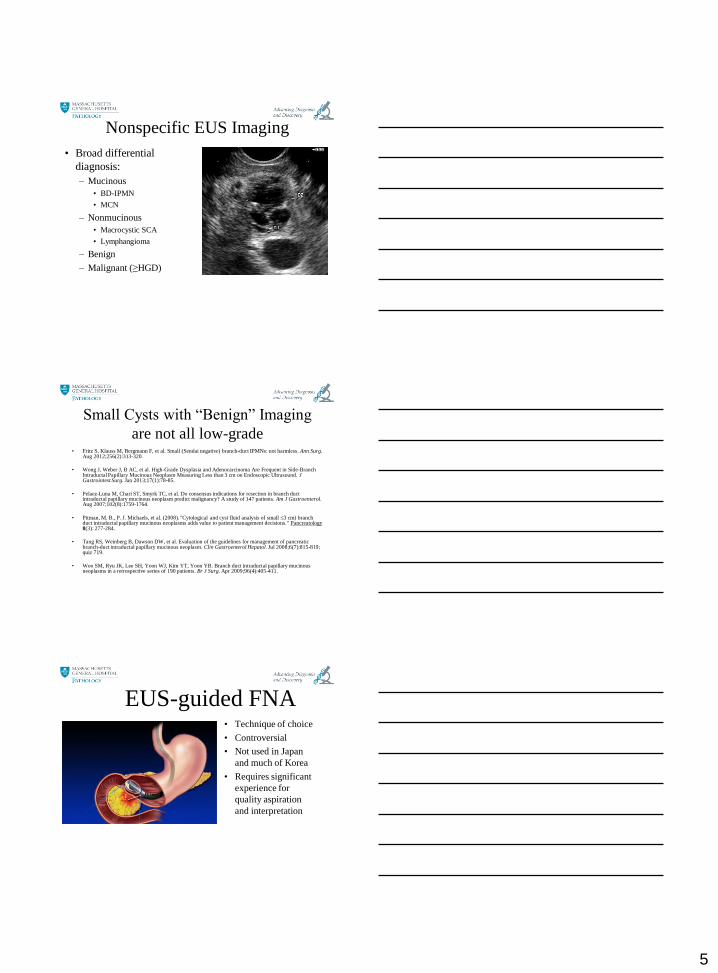
Nonspecific EUS Imaging
• Broad differential
diagnosis:
– Mucinous
• BD-IPMN
• MCN
– Nonmucinous
• Macrocystic SCA
• Lymphangioma
– Benign
– Malignant (≥HGD)
Small Cysts with “Benign” Imaging
are not all low-grade• Fritz S, Klauss M, Bergmann F, et al. Small (Sendai negative) branch-duct IPMNs: not harmless. Ann Surg.
Aug 2012;256(2):313-320.
• Wong J, Weber J, B AC, et al. High-Grade Dysplasia and Adenocarcinoma Are Frequent in Side-Branch Intraductal Papillary Mucinous Neoplasm Measuring Less than 3 cm on Endoscopic Ultrasound. J Gastrointest Surg. Jan 2013;17(1):78-85.
• Pelaez-Luna M, Chari ST, Smyrk TC, et al. Do consensus indications for resection in branch duct intraductal papillary mucinous neoplasm predict malignancy? A study of 147 patients. Am J Gastroenterol. Aug 2007;102(8):1759-1764.
• Pitman, M. B., P. J. Michaels, et al. (2008). "Cytological and cyst fluid analysis of small ≤3 cm) branch duct intraductal papillary mucinous neoplasms adds value to patient management decisions." Pancreatology8(3): 277-284.
• Tang RS, Weinberg B, Dawson DW, et al. Evaluation of the guidelines for management of pancreatic branch-duct intraductal papillary mucinous neoplasm. Clin Gastroenterol Hepatol. Jul 2008;6(7):815-819; quiz 719.
• Woo SM, Ryu JK, Lee SH, Yoon WJ, Kim YT, Yoon YB. Branch duct intraductal papillary mucinous neoplasms in a retrospective series of 190 patients. Br J Surg. Apr 2009;96(4):405-411.
EUS-guided FNA• Technique of choice
• Controversial
• Not used in Japan
and much of Korea
• Requires significant
experience for
quality aspiration
and interpretation
6
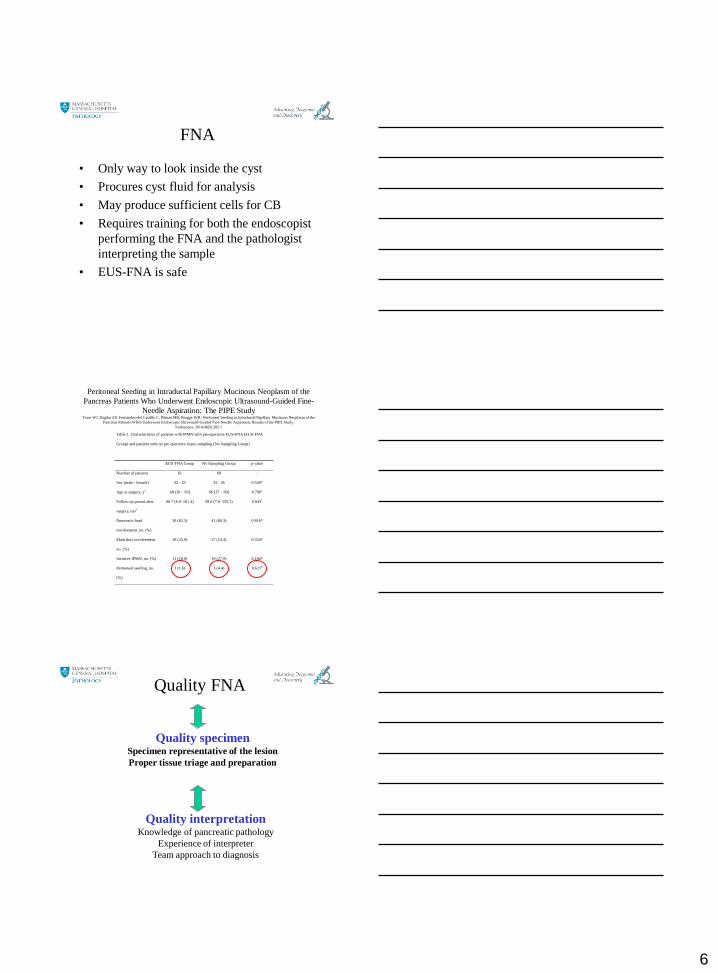
FNA
• Only way to look inside the cyst
• Procures cyst fluid for analysis
• May produce sufficient cells for CB
• Requires training for both the endoscopist
performing the FNA and the pathologist
interpreting the sample
• EUS-FNA is safe
Peritoneal Seeding in Intraductal Papillary Mucinous Neoplasm of the
Pancreas Patients Who Underwent Endoscopic Ultrasound-Guided Fine-
Needle Aspiration: The PIPE StudyYoon WJ, Dagilar ES, Fernandez-del Castillo C, Pitman MB, Brugge WR. Peritoneal Seeding in Intraductal Papillary Mucinous Neoplasm of the
Pancreas Patients WHO Underwent Endoscopic Ultrasound-Guided Fine-Needle Aspiration; Results of the PIPE Study.
Endoscopy. 2014;46(5):382-7
Table 1. Characteristics of patients with IPMN with pre-operative EUS-FNA (EUS-FNA
Group) and patients with no pre-operative tissue sampling (No Sampling Group)
EUS-FNA Group No Sampling Group p value
Number of patients 61 68 -
Sex (male : female) 32 : 29 32 : 36 0.540*
Age at surgery, y† 68 (39 – 83) 66 (37 – 89) 0.790
‡
Follow-up period after
surgery, mo†
66.7 (6.0–161.4) 58.6 (7.6–155.2) 0.843‡
Pancreatic head
involvement, no. (%)
38 (62.3) 41 (60.3) 0.816*
Main duct involvement,
no. (%)
28 (45.9) 37 (54.4) 0.334*
Invasive IPMN, no. (%) 11 (18.0) 19 (27.9) 0.184*
Peritoneal seeding, no.
(%)
1 (1.6) 3 (4.4) 0.621§
Quality FNA
Quality specimenSpecimen representative of the lesion
Proper tissue triage and preparation
Quality interpretationKnowledge of pancreatic pathology
Experience of interpreter
Team approach to diagnosis
7
HARVARDMEDICAL SCHOOL
MASSACHUSETTS GENERALPHYSICIANS ORGANIZATION
Two basic questions for Cyst analysis
1) Is the cyst mucinous or non-mucinous?
2) Is the cyst low-grade or high-grade?
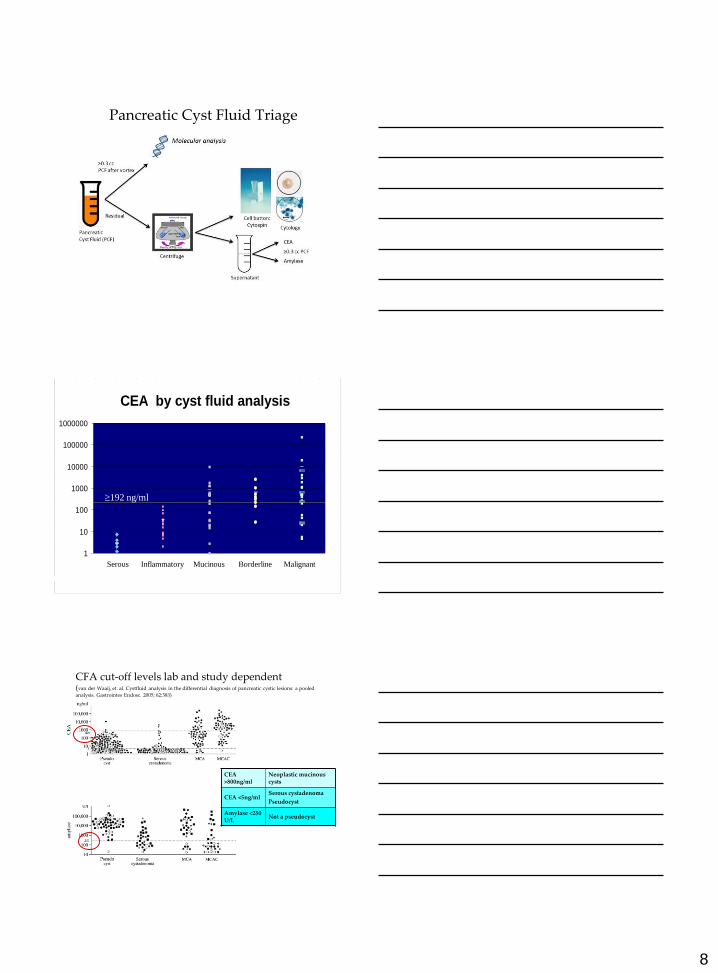
Mucinous HGA
IPMN with LGD
GI duplication
cyst
Non-neoplastic
Mucinous cyst
Cystic PanNET
Cystic Acinar
Cell carcinoma
SPN
IPMN/MCN with HGD
IPMN/MCN with
Invasive carcinoma
Cystic PDAC
IPMN with IGD
PCT
LEC
SCA
Surgery
MCN
with
LGD
HARVARDMEDICAL SCHOOL
MASSACHUSETTS GENERALPHYSICIANS ORGANIZATION
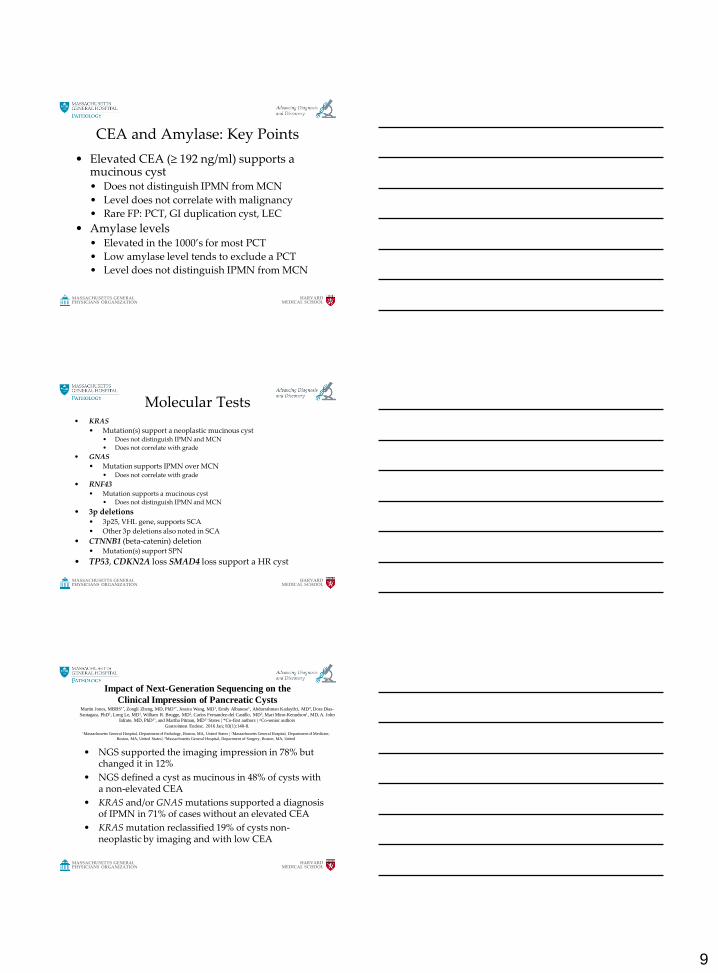
Cytological Preparations
• Cysts• Direct smears
• If fluid thick enough
• Fresh undiluted cyst fluid
• CEA; Amylase• Molecular • Cytology
• Cytospin• Cellblock
No-ROSE
8
HARVARDMEDICAL SCHOOL
MASSACHUSETTS GENERALPHYSICIANS ORGANIZATION
Pancreatic Cyst Fluid Triage
HARVARDMEDICAL SCHOOL
MASSACHUSETTS GENERALPHYSICIANS ORGANIZATION
Include Secondary Pathology
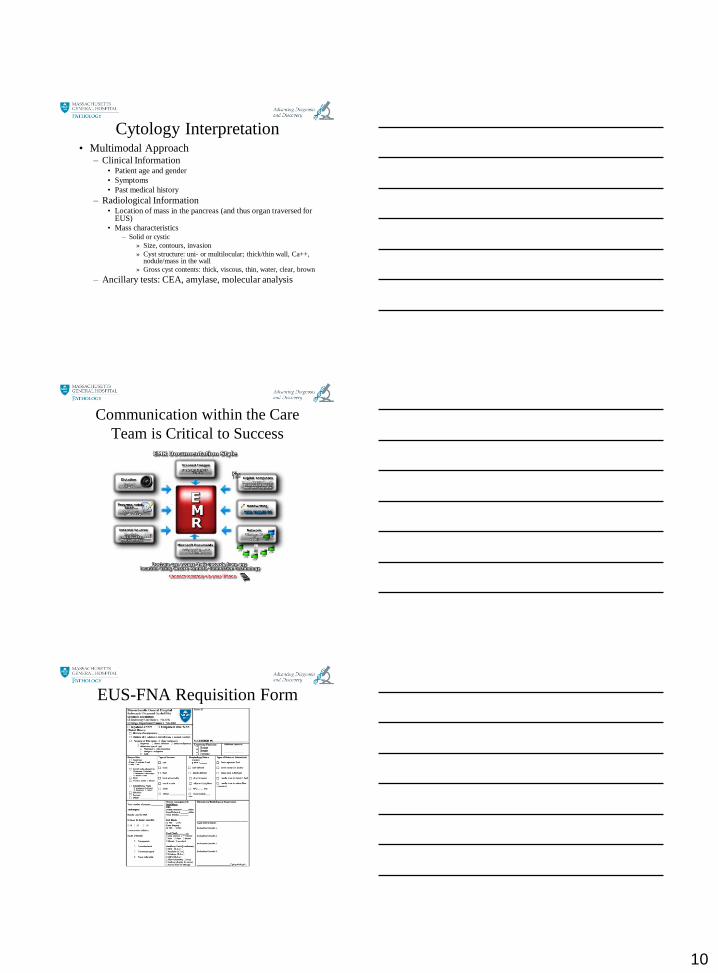
CEA by cyst fluid analysis
1
10
100
1000
10000
100000
1000000
Serous Inflammatory Mucinous Borderline Malignant
192 ng/ml
CFA cut-off levels lab and study dependent(van der Waaij, et. al. Cystfluid analysis in the differential diagnosis of pancreatic cystic lesions: a pooled
analysis. Gastrointes Endosc. 2005; 62:383)
CEA >800ng/ml
Neoplastic mucinous cysts
CEA <5ng/mlSerous cystadenoma
Pseudocyst
Amylase <250 U/L
Not a pseudocyst
9
HARVARDMEDICAL SCHOOL
MASSACHUSETTS GENERALPHYSICIANS ORGANIZATION
CEA and Amylase: Key Points
• Elevated CEA (≥ 192 ng/ml) supports a mucinous cyst• Does not distinguish IPMN from MCN
• Level does not correlate with malignancy
• Rare FP: PCT, GI duplication cyst, LEC
• Amylase levels• Elevated in the 1000’s for most PCT
• Low amylase level tends to exclude a PCT
• Level does not distinguish IPMN from MCN
HARVARDMEDICAL SCHOOL
MASSACHUSETTS GENERALPHYSICIANS ORGANIZATION
Molecular Tests • KRAS
• Mutation(s) support a neoplastic mucinous cyst• Does not distinguish IPMN and MCN
• Does not correlate with grade
• GNAS
• Mutation supports IPMN over MCN• Does not correlate with grade
• RNF43• Mutation supports a mucinous cyst
• Does not distinguish IPMN and MCN
• 3p deletions• 3p25, VHL gene, supports SCA
• Other 3p deletions also noted in SCA
• CTNNB1 (beta-catenin) deletion• Mutation(s) support SPN
• TP53, CDKN2A loss SMAD4 loss support a HR cyst
HARVARDMEDICAL SCHOOL
MASSACHUSETTS GENERALPHYSICIANS ORGANIZATION
• NGS supported the imaging impression in 78% but changed it in 12%
• NGS defined a cyst as mucinous in 48% of cysts with a non-elevated CEA
• KRAS and/or GNAS mutations supported a diagnosis of IPMN in 71% of cases without an elevated CEA
• KRAS mutation reclassified 19% of cysts non-neoplastic by imaging and with low CEA
Impact of Next-Generation Sequencing on the
Clinical Impression of Pancreatic Cysts
1Massachusetts General Hospital, Department of Pathology, Boston, MA, United States | 2Massachusetts General Hospital, Department of Medicine,
Boston, MA, United States | 3Massachusetts General Hospital, Department of Surgery, Boston, MA, United
Martin Jones, MBBS1*, Zongli Zheng, MD, PhD1*, Jessica Wang, MD1, Emily Albanese1, Abdurrahman Kadayifci, MD2, Dora Dias-
Santagata, PhD1, Long Le, MD1, William R. Brugge, MD2, Carlos Fernandez-del Castillo, MD3, Mari Mino-Kenudson1, MD, A. John
Iafrate, MD, PhD1 ,̂ and Martha Pitman, MD1 ̂States | *Co-first authors | ^Co-senior authors
Gastrointest Endosc. 2016 Jan; 83(1):140-8.
10
Cytology Interpretation• Multimodal Approach
– Clinical Information• Patient age and gender
• Symptoms
• Past medical history
– Radiological Information• Location of mass in the pancreas (and thus organ traversed for
EUS)
• Mass characteristics– Solid or cystic
» Size, contours, invasion
» Cyst structure: uni- or multilocular; thick/thin wall, Ca++, nodule/mass in the wall
» Gross cyst contents: thick, viscous, thin, water, clear, brown
– Ancillary tests: CEA, amylase, molecular analysis
Communication within the Care
Team is Critical to Success
EUS-FNA Requisition Form
11
Recommended Standardized
Reporting Terminology• Nondiagnostic
• Negative– AP, CP, AIP, LEC, PCT, Splenule
• Atypical
• Suspicious
• Neoplastic– Benign: SCA
– Other: MCN, IPMN, PanNET SPN
• Positive/Malignant– PDAC, ACC, PBL, lymphomas, metastases
Pitman MB, Centeno BA. Ali SZ, Genevay M, Stelow E, Mino-Kenudson M, Fernandez-del Castillo C, Schmidt CM, Brugge WR, and Layfield L.
Standardized Terminology and Nomenclature for Pancreatobiliary Cytology: The Papanicolaou Society of Cytopathology Guidelines for
Pancreatobiliary Cytology. Diagn Cytopathol, 2014.; 42(4):338-350
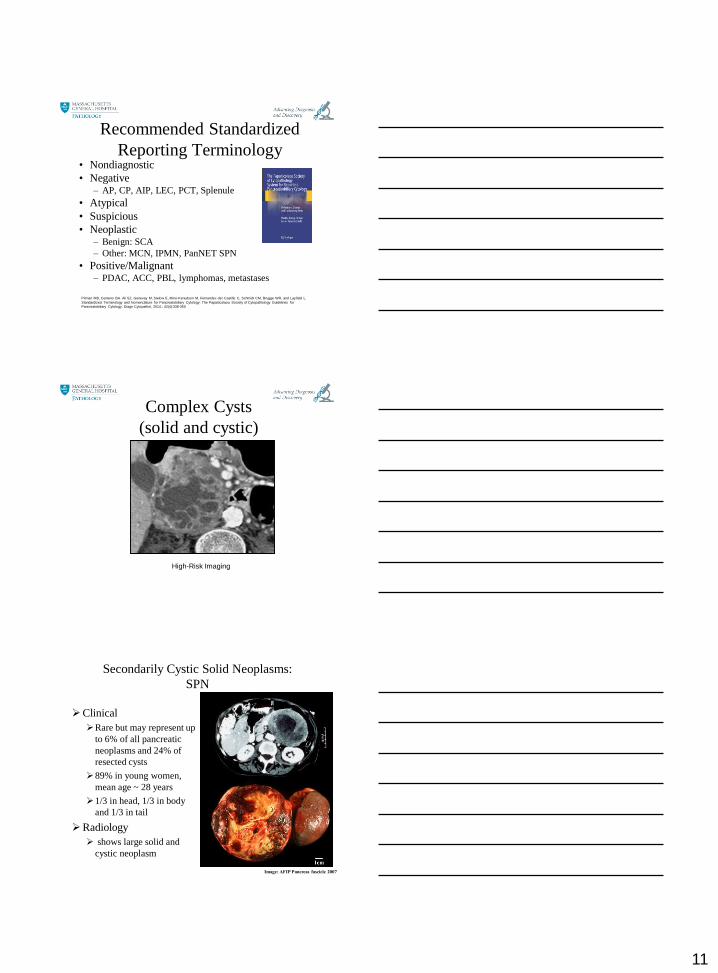
Complex Cysts
(solid and cystic)
High-Risk Imaging
Clinical
Rare but may represent up
to 6% of all pancreatic
neoplasms and 24% of
resected cysts
89% in young women,
mean age ~ 28 years
1/3 in head, 1/3 in body
and 1/3 in tail
Radiology
shows large solid and
cystic neoplasm
Image: AFIP Pancreas fascicle 2007
Secondarily Cystic Solid Neoplasms:
SPN
12
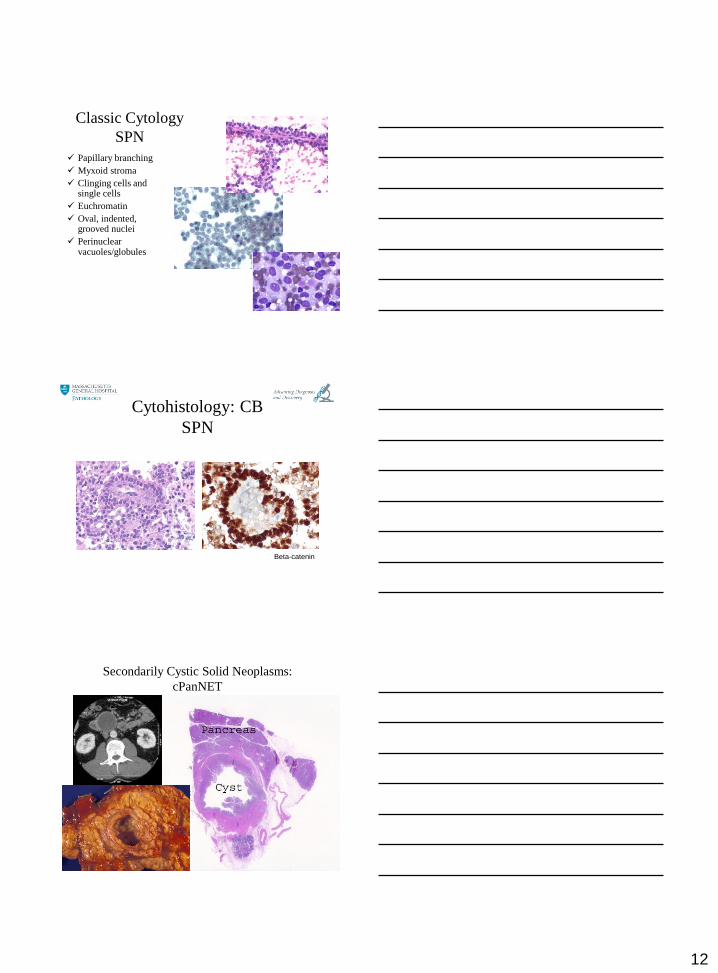
Classic Cytology
SPN
Papillary branching
Myxoid stroma
Clinging cells and single cells
Euchromatin
Oval, indented, grooved nuclei
Perinuclear vacuoles/globules
Cytohistology: CB
SPN
Beta-catenin
Secondarily Cystic Solid Neoplasms:
cPanNET
13
Cystic PanNETs
• ~10% of PanNETS
• Half are completely cystic and half are solid
and cystic
• Most are nonfunctioning
• If clinically suspected, serum chromogranin A
(CgA) levels may support the diagnosis when
elevated (sensitivity ~70%)– False positive CgA levels have been reported in patients taking proton pump
inhibitors, renal or liver failure and untreated hypertension.
– Elevated serum pancreatic polypeptide increases sensitivity to 93%
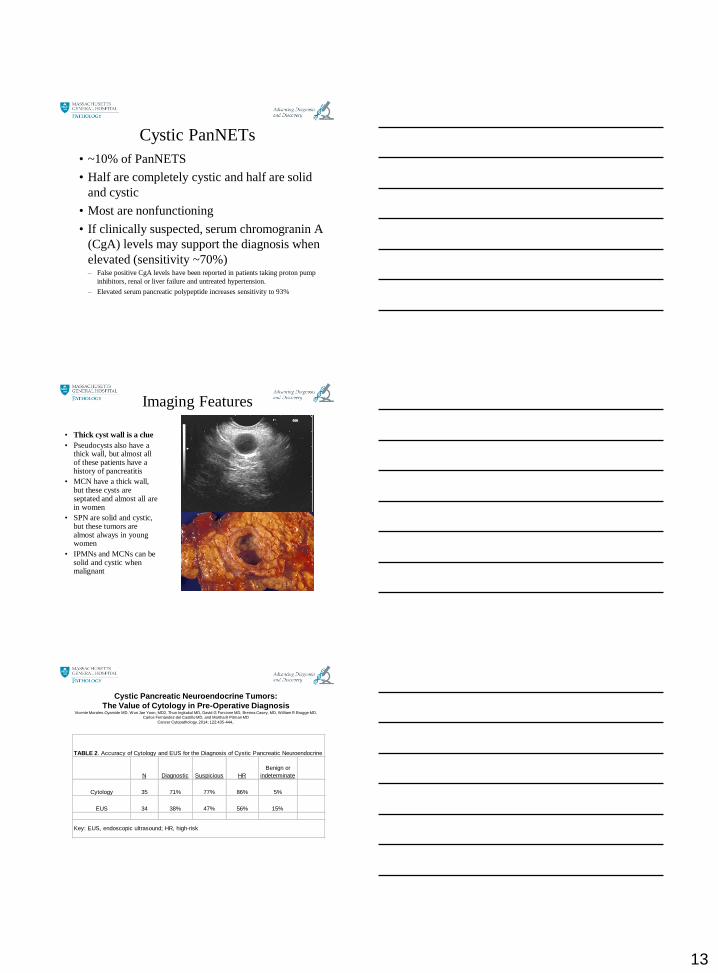
Imaging Features
• Thick cyst wall is a clue
• Pseudocysts also have a thick wall, but almost all of these patients have a history of pancreatitis
• MCN have a thick wall, but these cysts are septated and almost all are in women
• SPN are solid and cystic, but these tumors are almost always in young women
• IPMNs and MCNs can be solid and cystic when malignant
Cystic Pancreatic Neuroendocrine Tumors:
The Value of Cytology in Pre-Operative Diagnosis Vicente Morales-Oyarvide MD, Won Jae Yoon, MD2, Thun Ingkakul MD, David G Forcione MD, Brenna Casey, MD, William R Brugge MD,
Carlos Fernández-del Castillo MD, and Martha B Pitman MD
Cancer Cytopathology. 2014; 122:435-444..
N Diagnostic Suspicious HR
Benign or
indeterminate
Cytology 35 71% 77% 86% 5%
EUS 34 38% 47% 56% 15%
Key: EUS, endoscopic ultrasound; HR, high-risk
TABLE 2. Accuracy of Cytology and EUS for the Diagnosis of Cystic Pancreatic Neuroendocrine Tumors
14
Cystic pancreatic neuroendocrine tumors:
endoscopic ultrasound and fine-needle aspiration characteristics.
Yoon WJ, Daglilar ES, Pitman MB, Brugge WR.
Endoscopy. 2013;45(3):189-94.
Table 3. Comparison of CPanNet patients and mucinous cyst patients
CPanNet (n=15)* Mucinous cyst (n=15)
† P value
‡
Sex (male : female) 9 : 6 9 : 6 1.000§
Age, y, median (range) 57 (34 – 80) 57 (33 – 79) 0.950∥
Cyst diameter, mm,
median (range)
29 (16 – 70) 23 (8 – 90) 0.110∥
Wall thickness (thick :
thin)
10 : 5 2 : 13 0.003§
Septation (yes :no) 6 : 9 9 : 6 0.273§
Associated mass lesions
(yes : no)
8 : 7 4 : 11 0.136§
Cyst fluid CEA level,
ng/mL, median (range)
1.1 (0.3 – 500) 400 (2.8 – 6661) <0.001∥
Diagnostic cytology
(n, %)
11 (73.3)# 3 (20.0)
** 0.003
§
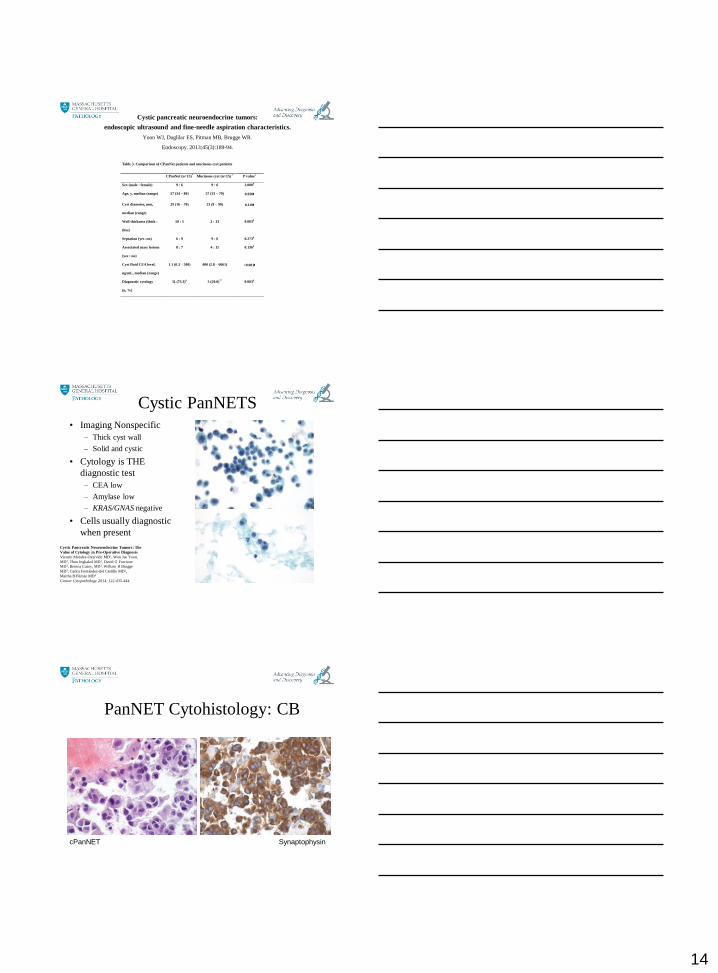
Cystic PanNETS• Imaging Nonspecific
– Thick cyst wall
– Solid and cystic
• Cytology is THE
diagnostic test
– CEA low
– Amylase low
– KRAS/GNAS negative
• Cells usually diagnostic
when present
Cystic Pancreatic Neuroendocrine Tumors: The
Value of Cytology in Pre-Operative Diagnosis
Vicente Morales-Oyarvide MD1, Won Jae Yoon,
MD2, Thun Ingkakul MD1, David G Forcione
MD3, Brenna Casey, MD3, William R Brugge
MD3, Carlos Fernández-del Castillo MD1,
Martha B Pitman MD4
Cancer Cytopathology, 2014; 122:435-444.
PanNET Cytohistology: CB
SynaptophysincPanNET
15
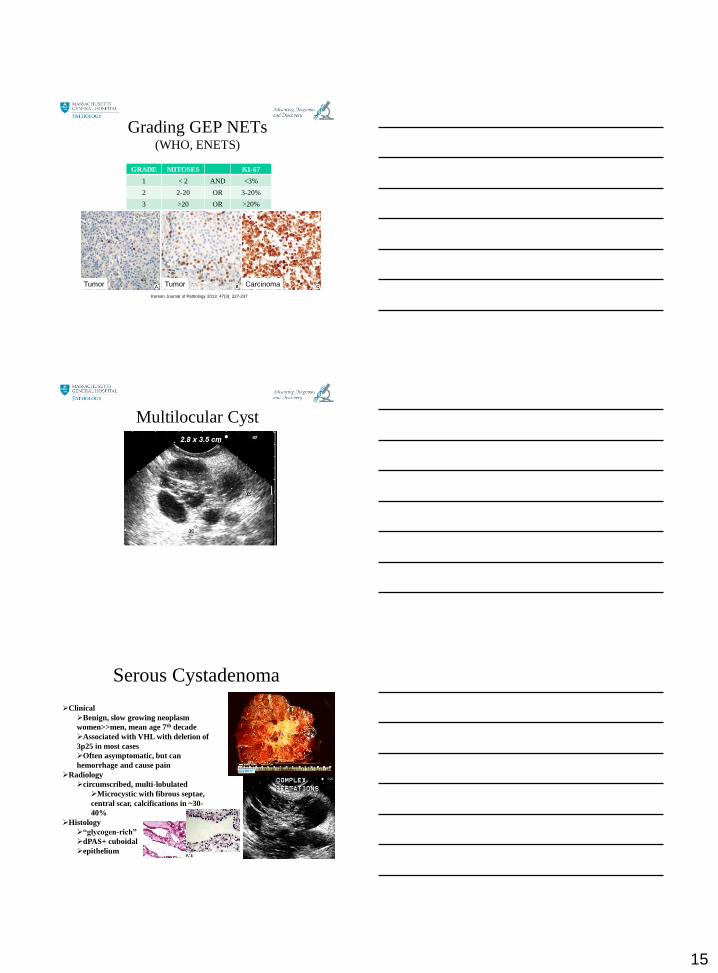
Grading GEP NETs(WHO, ENETS)
GRADE MITOSES KI-67
1 < 2 AND <3%
2 2-20 OR 3-20%
3 >20 OR >20%
Korean Journal of Pathology 2013; 47(3): 227-237
Tumor CarcinomaTumor
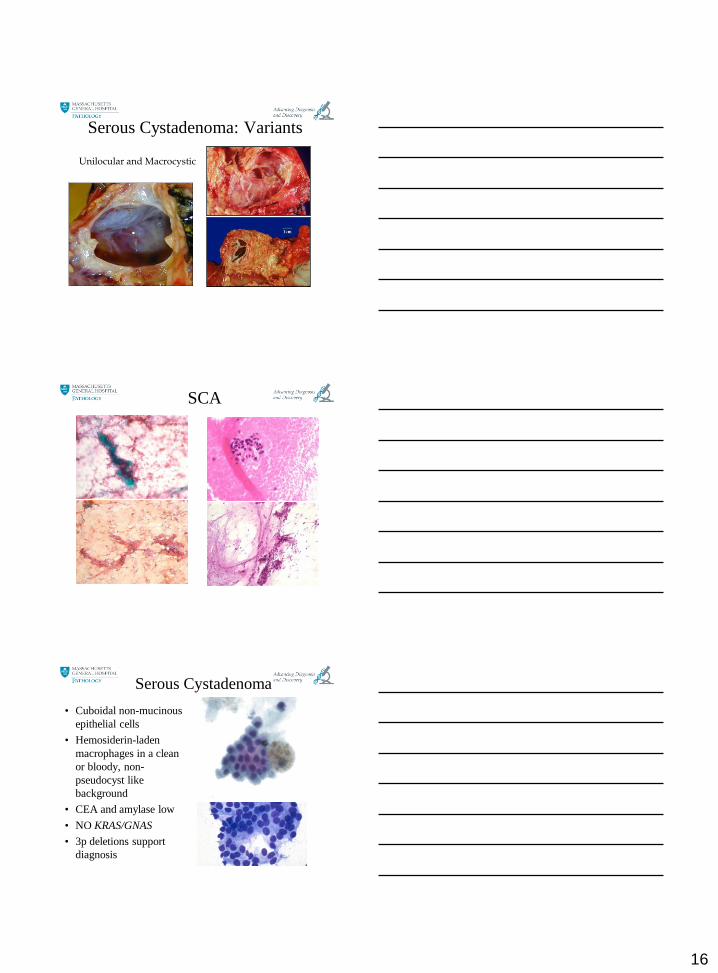
Multilocular Cyst
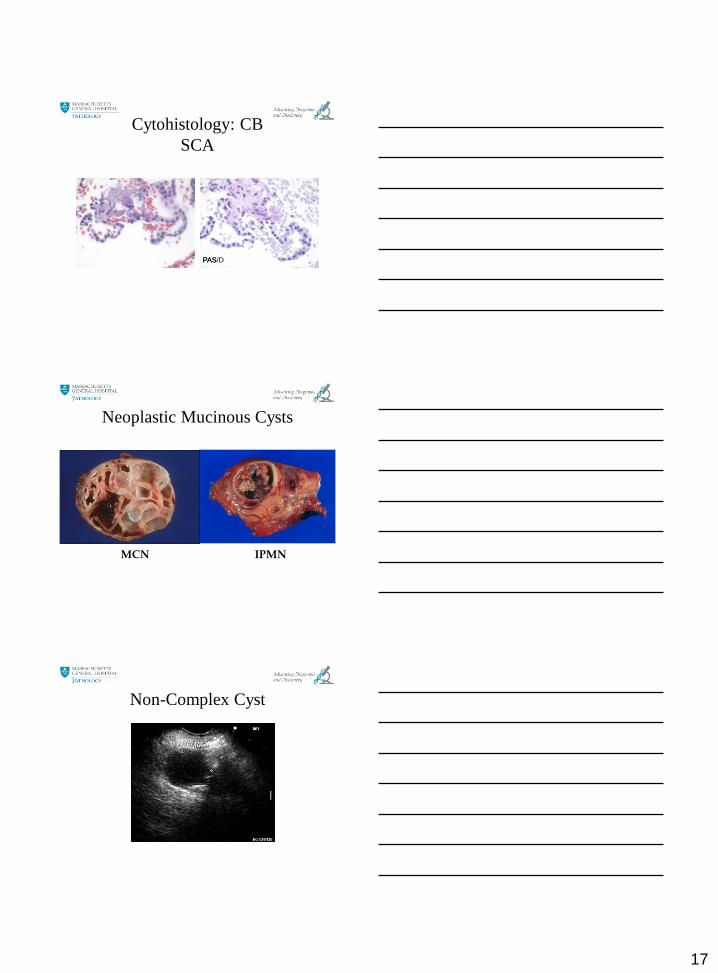
Serous Cystadenoma
Clinical
Benign, slow growing neoplasm
women>>men, mean age 7th decade
Associated with VHL with deletion of
3p25 in most cases
Often asymptomatic, but can
hemorrhage and cause pain
Radiology
circumscribed, multi-lobulated
Microcystic with fibrous septae,
central scar, calcifications in ~30-
40%
Histology
“glycogen-rich”
dPAS+ cuboidal
epithelium
16
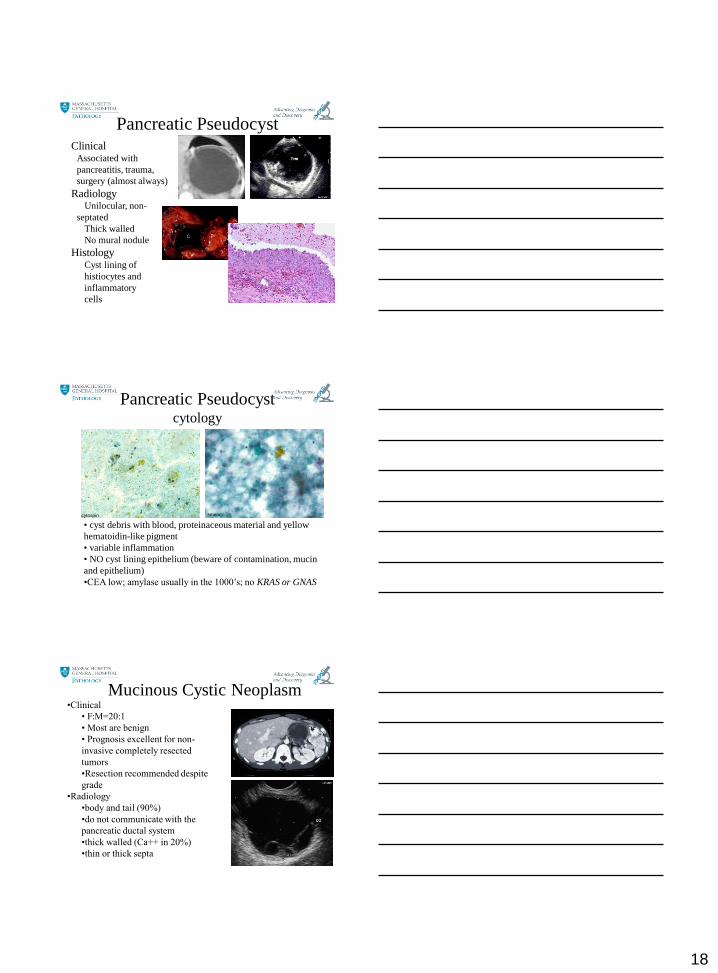
Serous Cystadenoma: Variants
Unilocular and Macrocystic
SCA
Serous Cystadenoma
• Cuboidal non-mucinous
epithelial cells
• Hemosiderin-laden
macrophages in a clean
or bloody, non-
pseudocyst like
background
• CEA and amylase low
• NO KRAS/GNAS
• 3p deletions support
diagnosis
17
Cytohistology: CB
SCA
PAS/DPAS
Neoplastic Mucinous Cysts
MCN IPMN
Non-Complex Cyst
18
Pancreatic PseudocystClinical
Associated with
pancreatitis, trauma,
surgery (almost always)
RadiologyUnilocular, non-
septated
Thick walled
No mural nodule
HistologyCyst lining of
histiocytes and
inflammatory
cells
Pancreatic Pseudocystcytology
• cyst debris with blood, proteinaceous material and yellow
hematoidin-like pigment
• variable inflammation
• NO cyst lining epithelium (beware of contamination, mucin
and epithelium)
•CEA low; amylase usually in the 1000’s; no KRAS or GNAS
cytospin smear
•Clinical
• F:M=20:1
• Most are benign
• Prognosis excellent for non-
invasive completely resected
tumors
•Resection recommended despite
grade
•Radiology
•body and tail (90%)
•do not communicate with the
pancreatic ductal system
•thick walled (Ca++ in 20%)
•thin or thick septa
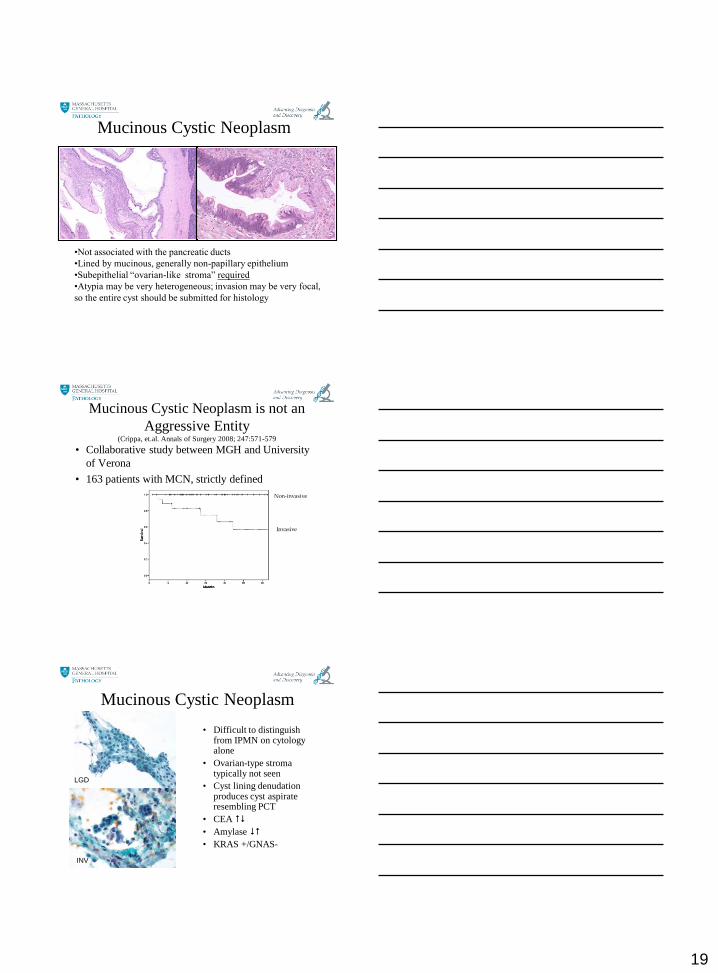
Mucinous Cystic Neoplasm
19
Mucinous Cystic Neoplasm
•Not associated with the pancreatic ducts
•Lined by mucinous, generally non-papillary epithelium
•Subepithelial “ovarian-like stroma” required
•Atypia may be very heterogeneous; invasion may be very focal,
so the entire cyst should be submitted for histology
Mucinous Cystic Neoplasm is not an
Aggressive Entity(Crippa, et.al. Annals of Surgery 2008; 247:571-579
• Collaborative study between MGH and University
of Verona
• 163 patients with MCN, strictly defined
Non-invasive
Invasive
Mucinous Cystic Neoplasm
• Difficult to distinguish from IPMN on cytology alone
• Ovarian-type stroma typically not seen
• Cyst lining denudation produces cyst aspirate resembling PCT
• CEA
• Amylase
• KRAS +/GNAS-
LGD
INV
20
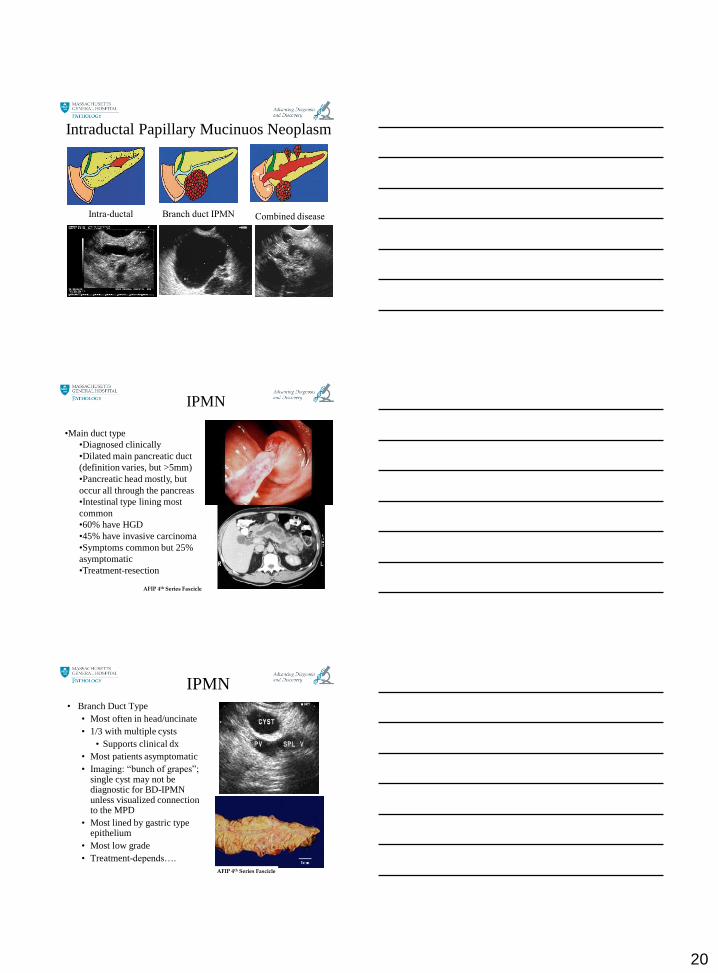
Intraductal Papillary Mucinuos Neoplasm
Intra-ductal Branch duct IPMN Combined disease
IPMN
•Main duct type
•Diagnosed clinically
•Dilated main pancreatic duct
(definition varies, but >5mm)
•Pancreatic head mostly, but
occur all through the pancreas
•Intestinal type lining most
common
•60% have HGD
•45% have invasive carcinoma
•Symptoms common but 25%
asymptomatic
•Treatment-resection
AFIP 4th Series Fascicle
IPMN• Branch Duct Type
• Most often in head/uncinate
• 1/3 with multiple cysts
• Supports clinical dx
• Most patients asymptomatic
• Imaging: “bunch of grapes”; single cyst may not be diagnostic for BD-IPMN unless visualized connection to the MPD
• Most lined by gastric type epithelium
• Most low grade
• Treatment-depends….
AFIP 4th Series Fascicle
21
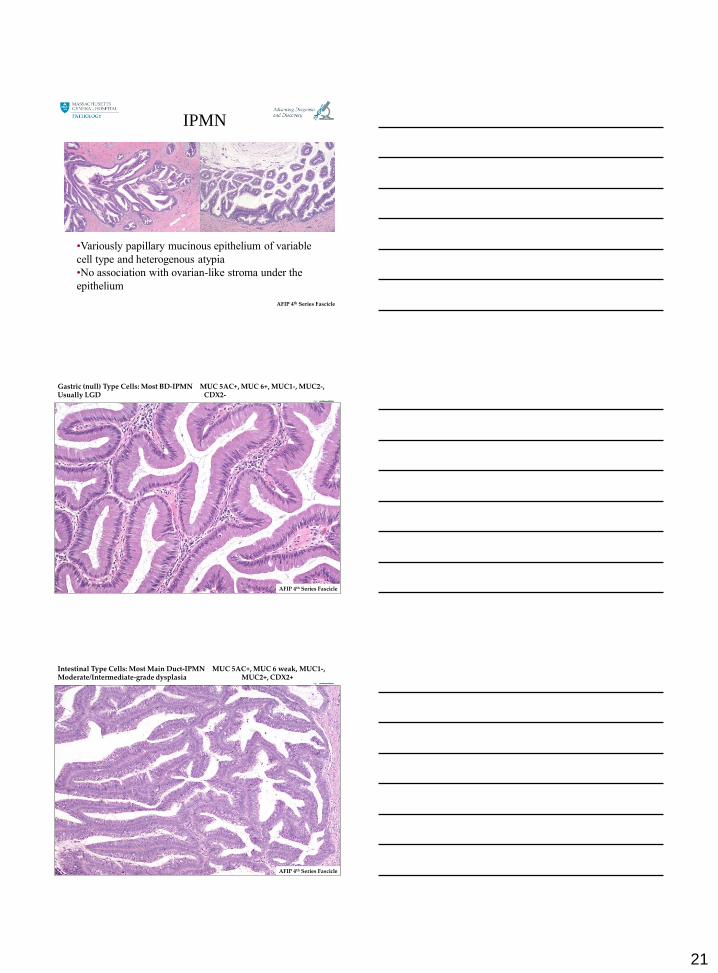
•Variously papillary mucinous epithelium of variable
cell type and heterogenous atypia
•No association with ovarian-like stroma under the
epithelium
AFIP 4th Series Fascicle
IPMN
Gastric (null) Type Cells: Most BD-IPMN MUC 5AC+, MUC 6+, MUC1-, MUC2-, Usually LGD CDX2-
AFIP 4th Series Fascicle
Intestinal Type Cells: Most Main Duct-IPMN MUC 5AC+, MUC 6 weak, MUC1-, Moderate/Intermediate-grade dysplasia MUC2+, CDX2+
AFIP 4th Series Fascicle
22
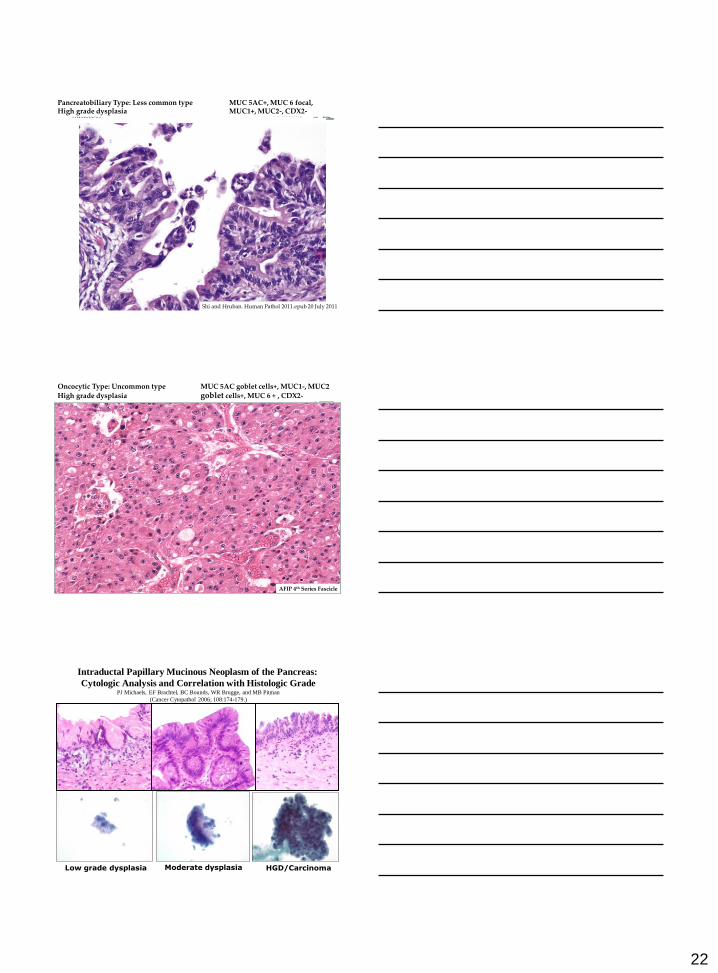
Pancreatobiliary Type: Less common type MUC 5AC+, MUC 6 focal, High grade dysplasia MUC1+, MUC2-, CDX2-
Shi and Hruban. Human Pathol 2011.epub 20 July 2011
Oncocytic Type: Uncommon type MUC 5AC goblet cells+, MUC1-, MUC2
High grade dysplasia goblet cells+, MUC 6 + , CDX2-
AFIP 4th Series Fascicle
HGD/Carcinoma
Intraductal Papillary Mucinous Neoplasm of the Pancreas:
Cytologic Analysis and Correlation with Histologic GradePJ Michaels, EF Brachtel, BC Bounds, WR Brugge, and MB Pitman
(Cancer Cytopathol 2006; 108:174-179.)
Low grade dysplasia Moderate dysplasia
23
Two basic questions for Cyst analysis
1) Is the cyst mucinous or non-mucinous?
1) Gross examination
2) CEA (best test)
3) Cytology
4) Molecular mutations
2) Is the cyst low-grade or high-grade?
1) Cytology!!
HARVARDMEDICAL SCHOOL
MASSACHUSETTS GENERALPHYSICIANS ORGANIZATION
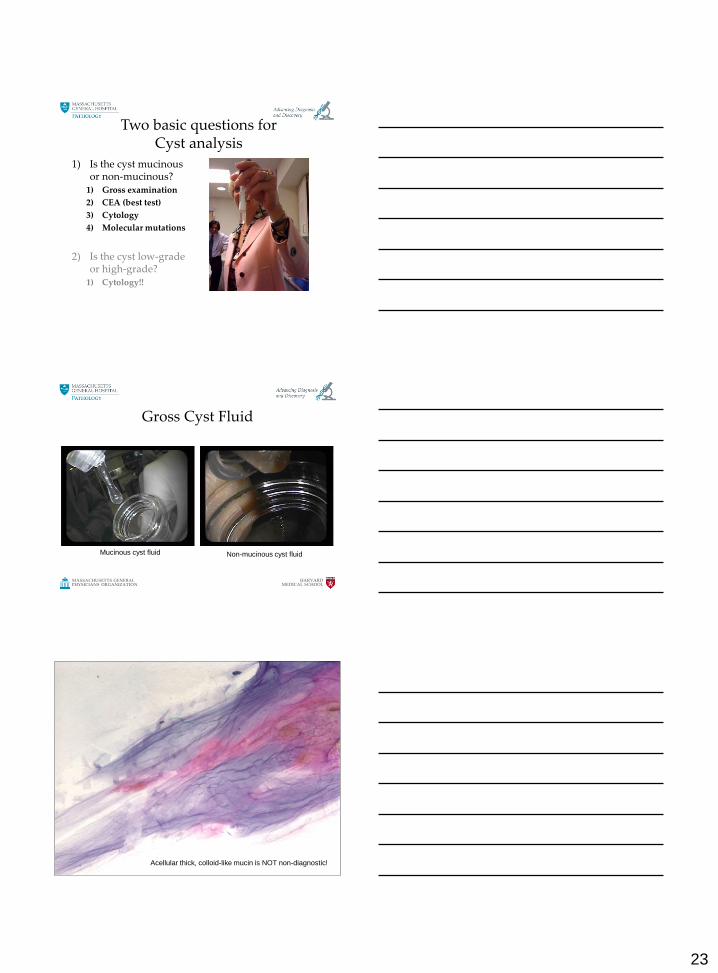
Gross Cyst Fluid
Mucinous cyst fluid Non-mucinous cyst fluid
Acellular thick, colloid-like mucin is NOT non-diagnostic!
24
HARVARDMEDICAL SCHOOL
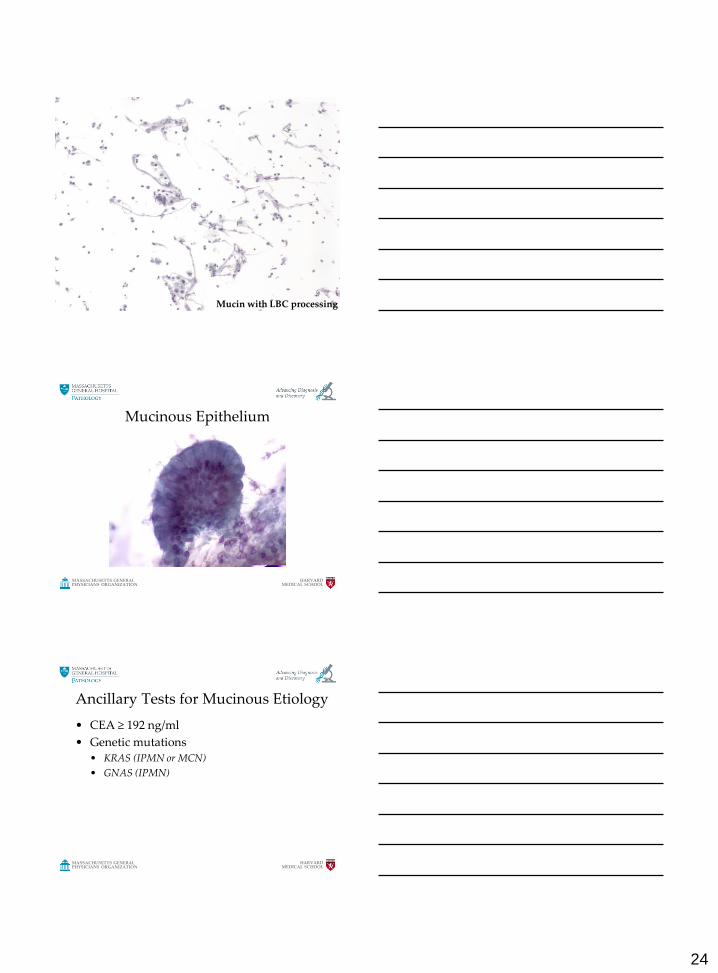
MASSACHUSETTS GENERALPHYSICIANS ORGANIZATION Mucin with LBC processing
HARVARDMEDICAL SCHOOL
MASSACHUSETTS GENERALPHYSICIANS ORGANIZATION
Mucinous Epithelium
HARVARDMEDICAL SCHOOL
MASSACHUSETTS GENERALPHYSICIANS ORGANIZATION
Ancillary Tests for Mucinous Etiology
• CEA ≥ 192 ng/ml
• Genetic mutations
• KRAS (IPMN or MCN)
• GNAS (IPMN)
25
HARVARDMEDICAL SCHOOL
MASSACHUSETTS GENERALPHYSICIANS ORGANIZATION
Two basic questions for Cyst analysis
1) Is the cyst mucinous or non-mucinous?
1) Gross examination
2) CEA (best test)
3) Cytology
2) Is the cyst low-grade or high-grade?
1) Cytology!!
HARVARDMEDICAL SCHOOL
MASSACHUSETTS GENERALPHYSICIANS ORGANIZATION
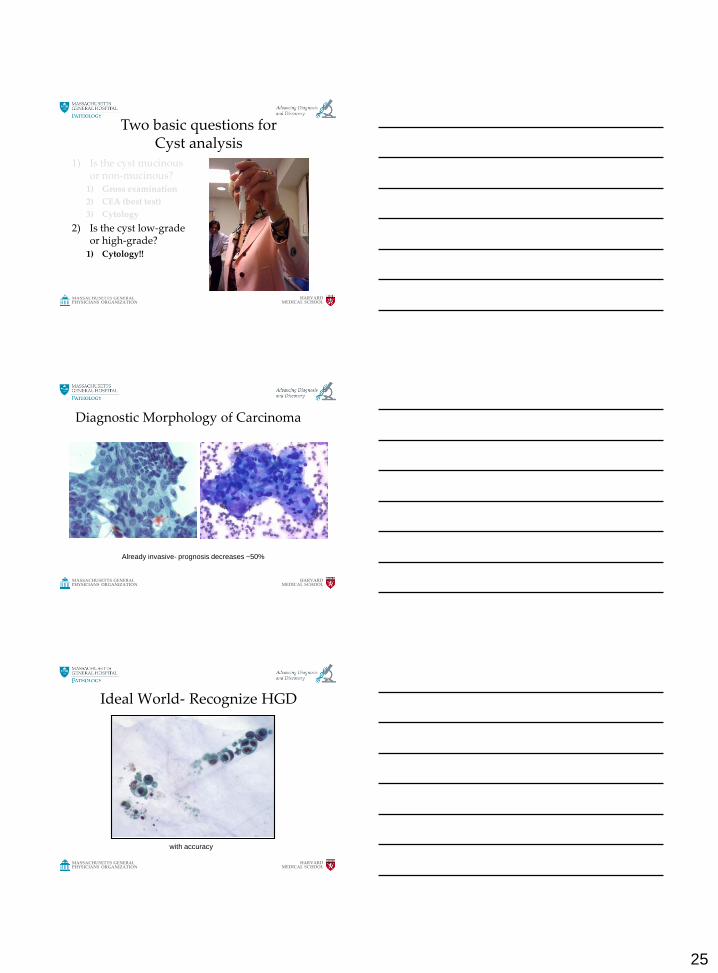
Diagnostic Morphology of Carcinoma
Already invasive- prognosis decreases ~50%
HARVARDMEDICAL SCHOOL
MASSACHUSETTS GENERALPHYSICIANS ORGANIZATION
Ideal World- Recognize HGD
with accuracy
26
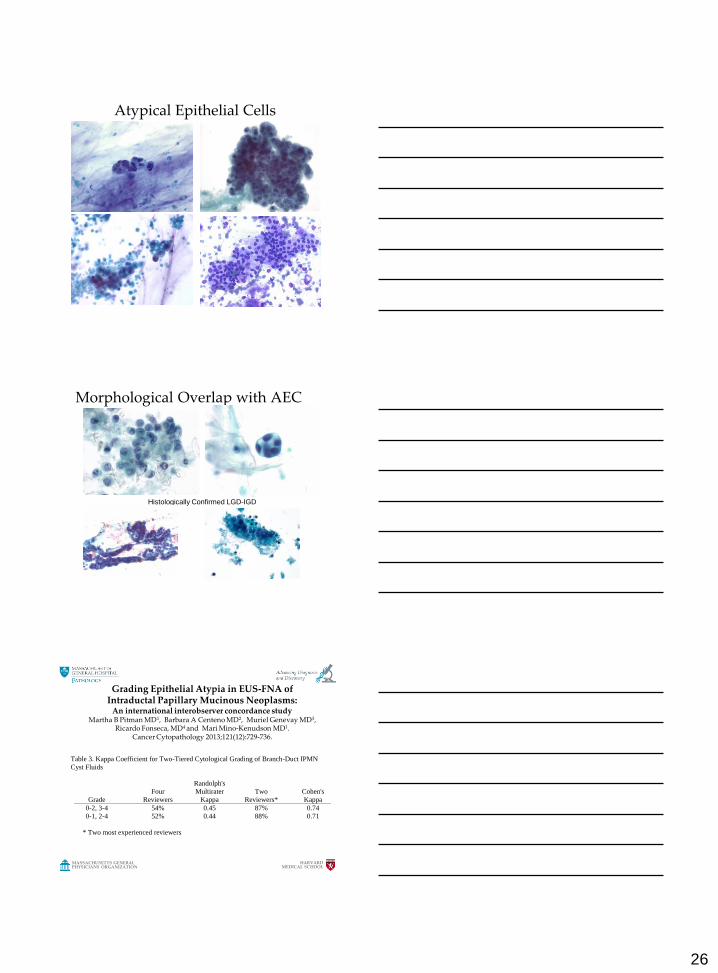
Atypical Epithelial Cells
Morphological Overlap with AEC
Histologically Confirmed LGD-IGD
HARVARDMEDICAL SCHOOL
MASSACHUSETTS GENERALPHYSICIANS ORGANIZATION
Grading Epithelial Atypia in EUS-FNA of Intraductal Papillary Mucinous Neoplasms:
An international interobserver concordance study Martha B Pitman MD1, Barbara A Centeno MD2, Muriel Genevay MD3,
Ricardo Fonseca, MD4 and Mari Mino-Kenudson MD1.Cancer Cytopathology 2013;121(12):729-736.
Table 3. Kappa Coefficient for Two-Tiered Cytological Grading of Branch-Duct IPMN
Cyst Fluids
Grade
Four
Reviewers
Randolph's
Multirater
Kappa
Two
Reviewers*
Cohen's
Kappa
0-2, 3-4 54% 0.45 87% 0.74
0-1, 2-4 52% 0.44 88% 0.71
* Two most experienced reviewers
27
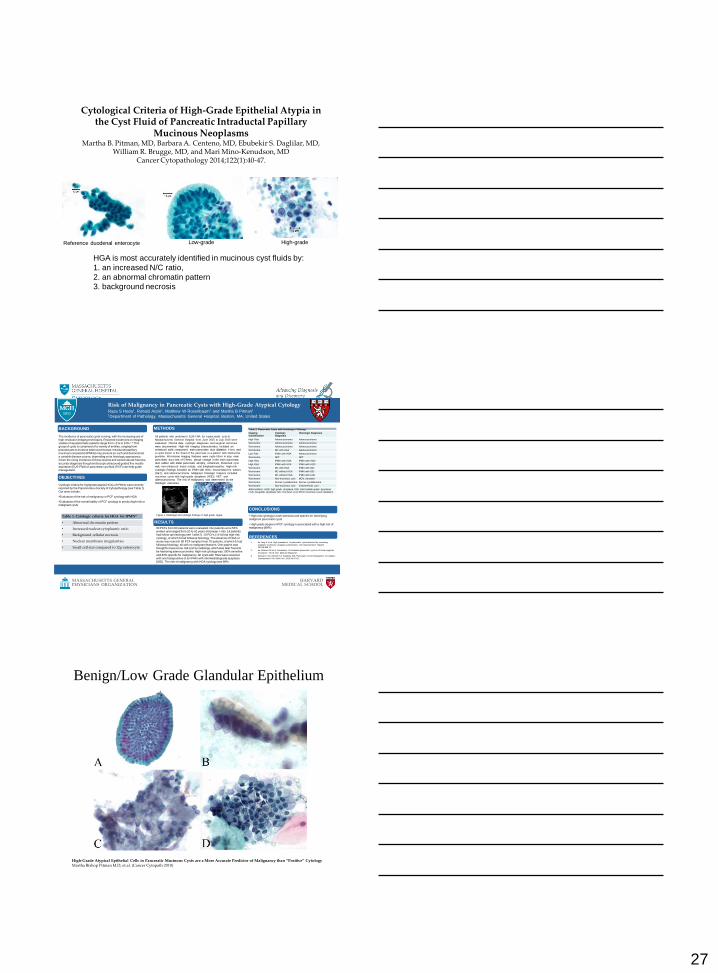
Cytological Criteria of High-Grade Epithelial Atypia in the Cyst Fluid of Pancreatic Intraductal Papillary
Mucinous NeoplasmsMartha B. Pitman, MD, Barbara A. Centeno, MD, Ebubekir S. Daglilar, MD,
William R. Brugge, MD, and Mari Mino-Kenudson, MDCancer Cytopathology 2014;122(1):40-47.
HGA is most accurately identified in mucinous cyst fluids by:
1. an increased N/C ratio,
2. an abnormal chromatin pattern
3. background necrosis
Reference duodenal enterocyte Low-grade High-grade
HARVARDMEDICAL SCHOOL
MASSACHUSETTS GENERALPHYSICIANS ORGANIZATION
Risk of Malignancy in Pancreatic Cysts with High-Grade Atypical CytologyRaza S Hoda1, Ronald Arpin1, Matthew W Rosenbaum1 and Martha B Pitman1
1Department of Pathology, Massachusetts General Hospital, Boston, MA, United States
METHODSBACKGROUND
RESULTS
1. de Jong K et al. High prevalence of pancreatic cysts detected by screening
magnetic resonance imaging examinations. Clin Gastroenterol Hepatol. 2010;8:806-11.
2. de Oliveira PB et al. Prevalence of incidental pancreatic cysts on 3 tesla magnetic
resonance. PLoS One. 2015;10:e0121317.
3. Ketwaroo GA, Mortele KJ, Sawhney MS. Pancreatic Cystic Neoplasms: An Update.
Gastroenterol Clin North Am. 2016;45:67-81.
Cytologic criteria for highgrade atypia (HGA) of IPMNs were recently reported by the Papanicolaou Society of Cytopathology (see Table 1). Our aims include:
•Evaluation of the risk of malignancy in PCF cytology with HGA
•Evaluation of the overall ability of PCF cytology to predict high-risk or malignant cysts
The incidence of pancreatic cysts is rising, with the increasing use of high-resolution imaging techniques. Reported incidences on imaging studies of asymptomatic patients range from <1% to 24%.1-3 This group of cysts is comprised of a variety of entities, ranging from pseudocysts to invasive adenocarcinomas. Intraductal papillary mucinous neoplasms (IPMNs) may present as such and demonstrate a variable disease course, depending on its histologic appearance. Given the rising incidence of these lesions and varied natural histories,
accurate diagnosis though endoscopic ultrasound guided fine needle aspiration (EUS-FNA) of pancreatic cyst fluid (PCF) can help guide management.
• High-risk cytology is both sensitive and specific for identifying malignant pancreatic cysts
• High grade atypia on PCF cytology is associated with a high risk of malignancy (89%)
OBJECTIVES
CONCLUSIONS
REFERENCES
Table 1. Cytologic criteria for HGA for IPMN4
• Abnormal chromatin pattern
• Increased nuclear:cytoplasmic ratio
• Background cellular necrosis
• Nuclear membrane irregularities
• Small cell size compared to 12µ enterocyte
All patients who underwent EUS-FNA for a pancreatic cyst at
Massachusetts General Hospital from June 2015 to July 2016 were
evaluated. Clinical data, cytologic diagnoses and surgical outcomes
were documented. High-risk imaging characteristics included an
enhanced solid component, main pancreatic duct dilatation ≥1cm, and
a cystic lesion in the head of the pancreas in a patient with obstructive
jaundice. Worrisome imaging features were cysts ≥3cm in size, main
pancreatic duct size of 5-9mm, abrupt change in the main pancreatic
duct caliber with distal pancreatic atrophy, enhanced, thickened cyst
wall, non-enhanced mural nodule, and lymphadenopathy. High-risk
cytologic findings included an IPMN with HGA, neuroendocrine tumors
(NET), and adenocarcinoma. Malignant histologic features included
mucinous cysts with high-grade dysplasia (HGD), NET, and
adenocarcinoma. The risk of malignancy was determined by the
histologic outcomes.
Table 2. Pancreatic Cysts with Histologic Followup.
Imaging Classification
Cytologic Diagnosis
Histologic Diagnosis
High Risk Adenocarcinoma Adenocarcinoma
Worrisome Adenocarcinoma Adenocarcinoma
Worrisome Adenocarcinoma Adenocarcinoma
Worrisome MC with HGA Adenocarcinoma
Low Risk IPMN with HGA Adenocarcinoma
Worrisome NET NET
High Risk IPMN with HGA IPMN with HGD
High Risk IPMN with HGA IPMN with HGD
Worrisome MC with HGA IPMN with IGD
Worrisome MC without HGA IPMN with IGD
Worrisome MC without HGA IPMN with LGD
Worrisome Non-mucinous cyst MCN, denuded
Worrisome Serous cystadenoma Serous cystadenoma
Worrisome Non-mucinous cyst Endometriotic cyst
Abbreviations: HGD, high-grade dysplasia; IGD, intermediate-grade dysplasia; LGD, low-grade dysplasia; MC, mucinous cyst; MCN, mucinous cystic neoplasm
90 PCFs from 80 patients were evaluated. Our patients were 54% women and ranged from 20 to 91 years old (mean = 66). 14 patients had follow-up histology (see Table 2). 10 PCFs (11%) had high-risk cytology, of which 9 had followup histology. The absence of HGA or worse was noted in 80 PCF samples from 70 patients, of which 5 had followup histology, all with no malignant features. One patient was thought to have a low-risk cyst by radiology, which was later found to be harboring adenocarcinoma. High-risk cytology was 100% sensitive
and 83% specific for malignancy. All cysts with HGA were resected with one falsepositive of an IPMN with intermediategrade dysplasia (IGD). The risk of malignancy with HGA cytology was 89%.
Figure 1. Radiologic and cytologic findings of high-grade atypia.
Benign/Low Grade Glandular Epithelium
High-Grade Atypical Epithelial Cells in Pancreatic Mucinous Cysts are a More Accurate Predictor of Malignancy than “Positive” CytologyMartha Bishop Pitman M.D, et.al. (Cancer Cytopath 2010)
28
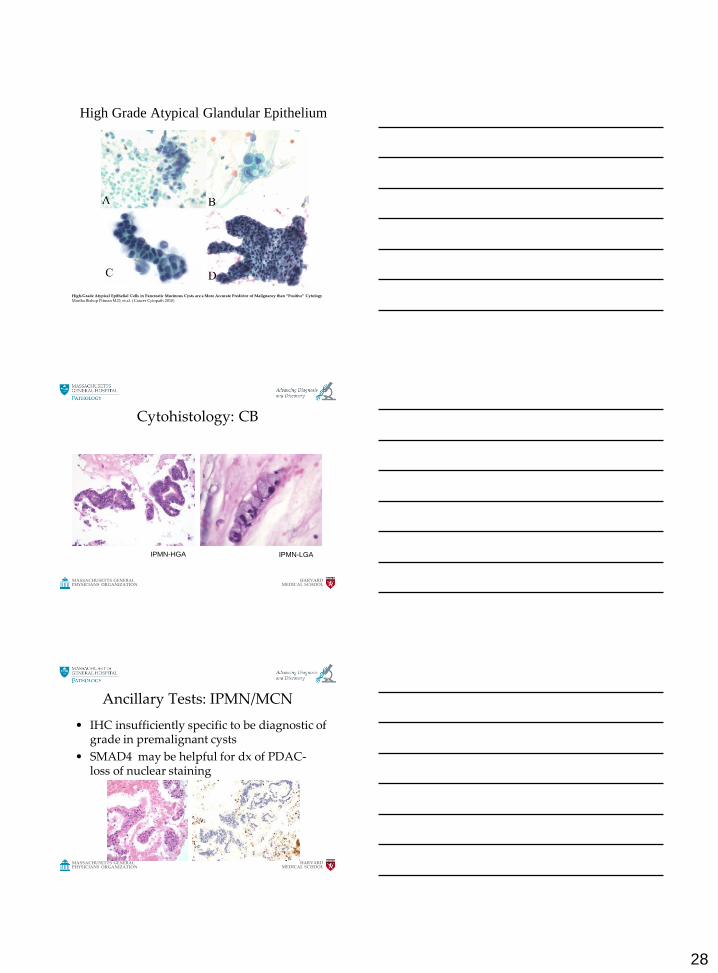
High Grade Atypical Glandular Epithelium
High-Grade Atypical Epithelial Cells in Pancreatic Mucinous Cysts are a More Accurate Predictor of Malignancy than “Positive” CytologyMartha Bishop Pitman M.D, et.al. ( Cancer Cytopath 2010)
HARVARDMEDICAL SCHOOL
MASSACHUSETTS GENERALPHYSICIANS ORGANIZATION
Cytohistology: CB
IPMN-HGA IPMN-LGA
HARVARDMEDICAL SCHOOL
MASSACHUSETTS GENERALPHYSICIANS ORGANIZATION
Ancillary Tests: IPMN/MCN
• IHC insufficiently specific to be diagnostic of grade in premalignant cysts
• SMAD4 may be helpful for dx of PDAC-loss of nuclear staining
29
HARVARDMEDICAL SCHOOL
MASSACHUSETTS GENERALPHYSICIANS ORGANIZATION
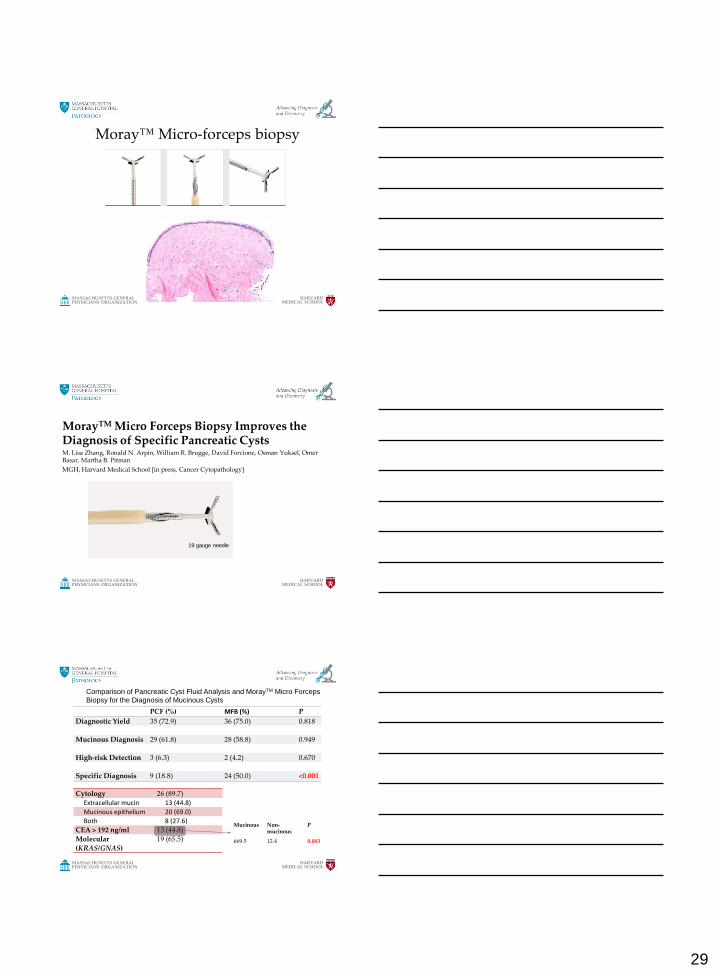
Moray™ Micro-forceps biopsy
HARVARDMEDICAL SCHOOL
MASSACHUSETTS GENERALPHYSICIANS ORGANIZATION
Platform PresentationMorayTM Micro Forceps Biopsy Improves the Diagnosis of Specific Pancreatic CystsM. Lisa Zhang, Ronald N. Arpin, William R. Brugge, David Forcione, Osman Yuksel, Omer Basar, Martha B. Pitman
MGH, Harvard Medical School [in press, Cancer Cytopathology]
19 gauge needle
HARVARDMEDICAL SCHOOL
MASSACHUSETTS GENERALPHYSICIANS ORGANIZATION
PCF (%) MFB (%) P
Diagnostic Yield 35 (72.9) 36 (75.0) 0.818
Mucinous Diagnosis 29 (61.8) 28 (58.8) 0.949
High-risk Detection 3 (6.3) 2 (4.2) 0.670
Specific Diagnosis 9 (18.8) 24 (50.0) <0.001
Cytology 26 (89.7)Extracellular mucin 13 (44.8)
Mucinous epithelium 20 (69.0)
Both 8 (27.6)
CEA > 192 ng/ml 13 (44.8)Molecular
(KRAS/GNAS)
19 (65.5)
Comparison of Pancreatic Cyst Fluid Analysis and MorayTM Micro Forceps
Biopsy for the Diagnosis of Mucinous Cysts
Mucinous Non-mucinous
P
669.5 12.4 0.003
30
HARVARDMEDICAL SCHOOL
MASSACHUSETTS GENERALPHYSICIANS ORGANIZATION
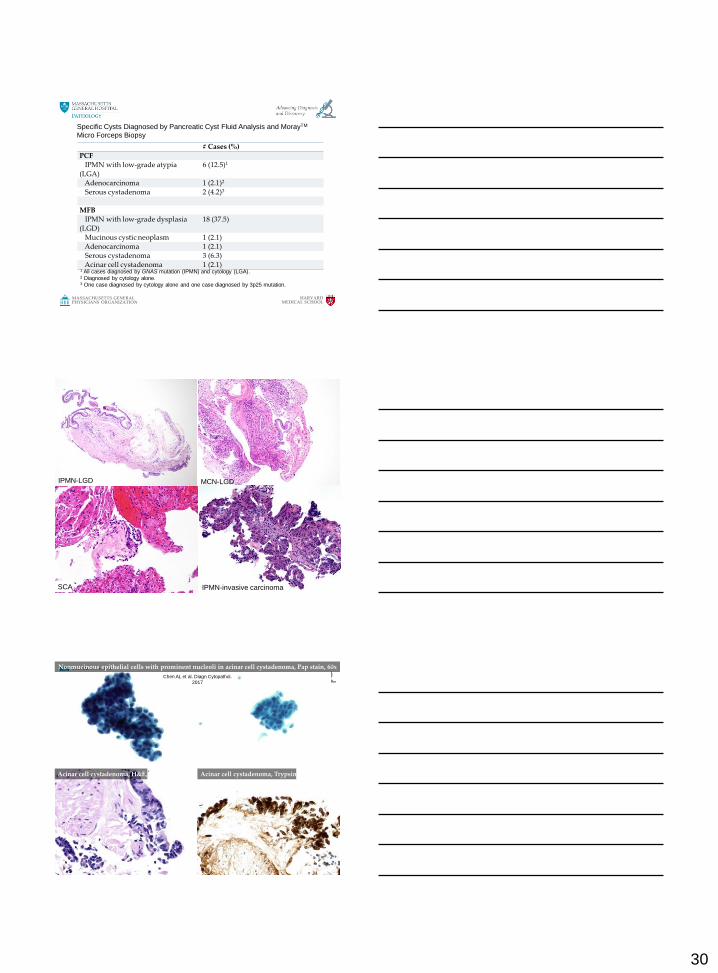
# Cases (%)PCF
IPMN with low-grade atypia
(LGA)
6 (12.5)1
Adenocarcinoma 1 (2.1)2
Serous cystadenoma 2 (4.2)3
MFBIPMN with low-grade dysplasia
(LGD)
18 (37.5)
Mucinous cystic neoplasm 1 (2.1)Adenocarcinoma 1 (2.1)Serous cystadenoma 3 (6.3)Acinar cell cystadenoma 1 (2.1)
1 All cases diagnosed by GNAS mutation (IPMN) and cytology (LGA).2 Diagnosed by cytology alone.3 One case diagnosed by cytology alone and one case diagnosed by 3p25 mutation.
Specific Cysts Diagnosed by Pancreatic Cyst Fluid Analysis and MorayTM
Micro Forceps Biopsy
HARVARDMEDICAL SCHOOL
MASSACHUSETTS GENERALPHYSICIANS ORGANIZATION
IPMN-LGD MCN-LGD
SCA IPMN-invasive carcinoma
HARVARDMEDICAL SCHOOL
MASSACHUSETTS GENERALPHYSICIANS ORGANIZATION
Nonmucinous epithelial cells with prominent nucleoli in acinar cell cystadenoma, Pap stain, 60x
Acinar cell cystadenoma, H&E, 40x Acinar cell cystadenoma, Trypsin, 40x
Chen AL et al. Diagn Cytopathol.
2017
31
HARVARDMEDICAL SCHOOL
MASSACHUSETTS GENERALPHYSICIANS ORGANIZATION
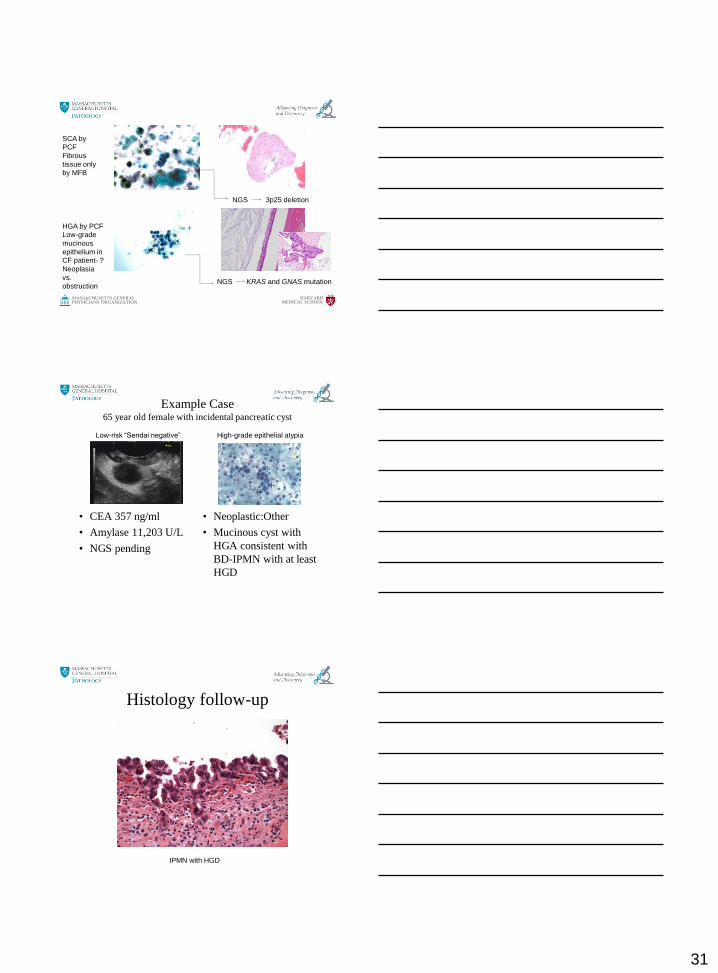
PCF Analysis and Histology discordanceSCA by
PCF
Fibrous
tissue only
by MFB
HGA by PCF
Low-grade
mucinous
epithelium in
CF patient- ?
Neoplasia
vs.
obstruction
NGS 3p25 deletion
NGS KRAS and GNAS mutation
Example Case65 year old female with incidental pancreatic cyst
• CEA 357 ng/ml
• Amylase 11,203 U/L
• NGS pending
• Neoplastic:Other
• Mucinous cyst with
HGA consistent with
BD-IPMN with at least
HGD
Low-risk “Sendai negative” High-grade epithelial atypia
Histology follow-up
IPMN with HGD
32
Acknowledgements
• Dr. Carlos Fernandez-del Castillo
• Dr. Dushyant Sahani
• Dr. Bill Brugge
• Dr. Mari Mino-Kenudson
• Dr. Ralph Hruban
• Dr. David Klimstra
• Dr. Lester Layfield