Embed Size (px)
Citation preview

Pre Pregnancy Care – A Primary Care Approach - Overview
Dr. Sri Wahyu Taher
Pakar Perunding Perubatan Keluarga
Klinik Kesihatan Simpang Kuala
Alor Setar

FACTS
•4 out of 10 women report that their pregnancies are unplanned
•Perinatal deaths are 50% higher among babies born to adolescent mothers
•Up to 10% of pregnancies among women with untreated gonococcal infections result in perinatal death

FACTS
• Maternal under nutrition and iron-deficiency anemia account for at least 20% of maternal mortality
• In the absence of interventions, rates of HIV transmission from mother to child are between 15 and 45%

Do we need Pre Pregnancy Care Services in Primary Care Clinics?
• Healthy women getting into pregnancy
• Woman in reproductive age with medical problems conceiving
• Woman with medical risk factors conceiving
• Anticipate a positive outcome with minimal or zero complication
• Comfort / reassurance / confidence
• Plan for future pregnancy
• Comprehensive preparation - BIOPSYCHOSOCIAL

International Comparisons of
Infant Mortality Rates, 2007 (latest data as of Feb, 2013)
Rank Country Rate
1 Iceland 2.0
2 Sweden 2.5
8 Portugal 3.4
13 Austria 3.7
22 United Kingdom 4.8
24 Canada 5.1
28 United States 6.8
MODs Peristats, 2009

Global Maternal Mortality – 1990, 2005 and 2013

In 2013, 4.6 million
(74% of all under-five deaths) occurred within the first year of life.
Infant mortality rate total: 13.69 deaths/1,000 live births male: 15.82 deaths/1,000 live births
female: 11.42 deaths/1,000 live births
(2014 estimate - Malaysia)
Infant mortality is closely related to maternal mortality and morbidity

Incidence of Adverse Pregnancy Outcomes,
most recent years
Spontaneous Abortion 20% (estimated average)
Infant Mortality 6.6/1000 live births (2008)
Fetal Mortality 6.2/1000 live births plus fetal
deaths (2005)
Major Birth Defects 3.3% (2002)
Low Birth Weight 8.1% (2010)
Preterm Delivery 12.0% (2010)
Complications of Pregnancy 30.7% (CDC data, 2002)
Unintended Pregnancies 49% (2006)
Unintended Births 31% (2006)


So why is Pre Pregnancy Care Important?

NHMS 2015

11.6
15.2
17.5
7.0 7.2
8.3
4.5
8.0
9.2
4.2 4.9 4.7
0.0
2.0
4.0
6.0
8.0
10.0
12.0
14.0
16.0
18.0
20.0
NHMS III (2006) NHMS 2011 NHMS 2015
Pre
vale
nce
(%
)
Prevalence of Diabetes, ≥18 years (2006, 2011, 2015)
Total diabetes Known Undiagnosed IFG

Prevalence of Diabetes, ≥ 30 Years, NHMS (1996, 2006, 2011 and 2015)
8.3
14.9
20.8
22.5
6.5
9.5
10.7 10.6
1.8
5.4
10.1
11.9
0.0
5.0
10.0
15.0
20.0
25.0
NHMS 1996 NHMS 2006 NHMS 2011 NHMS 2015
Total Known Undiagnosed
Pre
vale
nce
(%
)

0.0 0.7
1.4
3.4 3.4
6.9
10.5
14.8
20.6
26.5
24.4
27.9
24.4
5.5 5.2
7.4 7.2
9.5 11.0 11.5
12.2 12.4 11.8
13.6
11.2 12.6
5.5 5.9
8.9
10.6
12.9
17.6
22.0
27.0
32.9
38.3 38.0 39.1
37.0
3.6 3.6 3.9 3.9 4.6
6.0 5.8 5.8 5.9 5.5 4.8 5.4 6.0
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
40.0
45.0
Pre
vale
nce
(%
)
Prevalence of Diabetes, ≥18 years, by age groups (2015)
Known Undiagnosed Total diabetes IFG

Prevalence of Diabetes, ≥18 years, by Ethnicity (2015)
14.6
9.0 9.8
5.2
12.0
7.7 7.7
3.8
22.1
16.0
11.9
7.7
10.7
6.8 8.1
3.1
7.4
2.5
8.6
4.3
0.0
5.0
10.0
15.0
20.0
25.0
Total Diabetes Known Diabetes Undiagnosed DM IFG
Malay Chinese Indian Other Bumiputras Other
%

19.8
25.4
18.5
16.7
19.3
14.8
18.1 19.4
20.6
15.5
18.6
14.2 14.8
17.4
19.2
0.0
5.0
10.0
15.0
20.0
25.0
30.0
Pre
vale
nce
(%
)
Prevalence of Diabetes, ≥18 years, by States (2006, 2011 & 2015)
NHMS III (2006) NHMS 2011 NHMS 2015

Intendedness of conception
Interpregnancy interval
Maternal age
Exposure ART/ovulation stimulation
Spontaneous abortion
Abnormal placentation
Chronic disease control
Congenital anomalies
Timing of entry into prenatal care
Important Examples of Determinants Poor Maternal & Perinatal Outcome


In obstetrics,
many of our
outcomes or their
determinants are
present before we
ever meet our
patients

The preconception movement is based on the
realization that:
Prenatal care starts too late to prevent
many of these poor pregnancy outcomes
Women who have higher levels of health
before pregnancy have healthier
reproductive outcomes

Evidence for PPC relevance

Evidence for its relevance
• PPC was a/w improved glycaemic control in early pregnancy and significant reductions in adverse pregnancy outcome (malformation, stillbirth and neonatal death) and very prematurity (Temple et al; Diabetes Care Vol 29, 2006)
• Preconception health status plays a fundamental role in determining risk for adverse pregnancy-related outcomes - WHO

Evidence for its relevance
•High HbA1c and T2DM independently is associated with serious adverse fetal outcome (Clausen et al;Diabetes Care, 2005)
•Pregnancy outcome in T2DM are better in c/w T1DM mothers when given equal pre pregnancy care intensified medical treatment (Hillman & Herranz; Diabetes Care vol 29, Nov 2006)

Statistics – How did we do past few years?

0
5
10
15
20
25
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
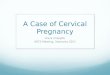
2012 2013 2014 2015 2016 2017
No. of Death 14 8 18 23 15 15
MMR Kedah 39.3 22.3 50.2 64.8 40.8 40.8
Mat
ern
al d
eath
/10
0 0
00
LB
Source of data: MMR (Kedah) from HIMS reten
Nu
mb
er o
f d
eath
Data merujuk kepada semua jenis kematian (all pregnancy related death)
MATERNAL MORTALITY RATIO KEDAH 2012 – 2017

26.7%
46.6%
26.7%
13.4%
46.6%
40.0%
0 2 4 6 8 10 12 14 16
2016
2017
2016 2017
Direct 4 7
Indirect 4 2
Fortuituos 7 6
TOTAL 15 15
KLASIFIKASI KEMATIAN IBU NEGERI KEDAH 2016 - 2017

53.30%
53.30%
46.70%
46.70%
0% 20% 40% 60% 80% 100%
2016
2017
Preventable Non Preventable
PREVENTABLE / NON PREVENTABLE BY CAUSES OF DEATH 2016 - 2017
PREVENTABILITY
PPH
PULMONAR
Y
EMBOLISM
AMNIOTIC
FLUID
EMBOLI HDP Medical Other
‘16 ‘’17 ‘16 ‘’17 ‘16 ‘17 ‘16 ‘17 ‘16 ‘17 ‘16 ‘17
Yes 1 4 0 1 0 0 0 0 4 2 3 0
No 0 - 1 1 1 1 0 0 1 4 3 2
Total 1 4 2 2 1 1 0 0 5 6 6 2

BILANGAN KEMATIAN IBU MENGIKUT DAERAH TAHUN 2015 – 2017 NEGERI KEDAH
DAERAH ESTIMATED LIVE BIRTH
NO. OF MATERNAL DEATHS (RATES PER 100 000 LB)
BALING 2885
BANDAR BHARU 803
KOTA SETAR 7084
KUALA MUDA 7887
KUBANG PASU 4269
KULIM 4853
LANGKAWI 1886
PADANG TERAP 1441
PENDANG 2229
SIK 1432
YAN 1186
NEGERI KEDAH 36784
2015 2016 2017
1 (34.6) 2 (69.3) 2 (69.3)
1 (12.4) 0 0
4 (56.4) 2 (28.2) 0
7 (88.7) 2 (25.3) 6 (76.1)
2 (46.8) 1 (23.4) 0
3 (61.8) 4 (82.4) 4 (82.4)
2 (10.6) 1 (53.0) 2 (10.6)
0 1 (69.4) 1 (69.4)
0 0 0
1 (69.8) 1 (69.8) 0
2 (16.8) 1 (84.3) 0
23 (62.5) 15 (40.7) 15 (40.7)

TAHUN JUMLAH WANITA DI SARING
JUMLAH RISIKO KESIHATAN
DIKESAN
PERATUS RISIKO KESIHATAN DIKESAN DALAM KALANGAN WANITA DISARING
2011 19349 7890 39.2
2012 25 544 8153 31.9
2013 29135 8507 29.2
2014 34925 8764 25.1
2015 39537 9193 23.3
2016 38245 11084 29.0
2017 35043 11960 34.1
PERKHIDMATAN PPC DI KLINIK KESIHATAN 2011 – 2017

PPC MENGIKUT ENTRY POINT DI KLINIK KESIHATAN 2017 NEGERI KEDAH
BALINGBANDA
RBHARU
KOTASETAR
KUALAMUDA
KUBANG PASU
KULIMLANGKA
WI
PADANG
TERAP
PENDANG
SIK YAN
KD 186 178 123 232 0 775 112 157 35 18 111
KEMKESIHATAN
0 4 0 0 0 0 0 0 0 0 16
UPL 171 131 1240 1020 474 1037 247 71 256 271 142
MCH 194 132 1219 467 610 528 521 252 382 232 416
35.2% 29.7%
47.2%
27.2%
56.3%
22.6%
59.2% 52.5% 56.8%
44.5%
60.7%
31%
29.4%
48%
59.3%
43.7%
44.3%
28.1%
14.8%
38% 52% 20.7%
0
0.9%
0
0
0
0
0
0
0 0
2.3% 33.8% 40%
4.8% 13.5%
0
33.1%
12.7%
32.7%
5.2% 3.5%
16.3
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
PER
ATU
S
Axis Title
JUMLAH 551 445 2582 1719 1084 2340 880 480 673 521 685
* Fokus utama PPC di UPL : Kuala Muda, Sik, Kota Setar (Shift from MCH ke UPL entry point)

HPT DM AnemiaBad
Obs HxThyrotoxicosis
HeartDis
Epilepsy
CTD Mental Asthma RV+ve STI Obesiti Others
2015 23.2 23.5 2.6 5.5 1.5 1.3 0.3 0.01 0.1 1.3 0.1 0.1 1 3.9
2016 24.6 30.3 2.1 18 1.4 0.9 10.3 0.1 0.3 4.7 0.1 0.03 3.5 13.7
2017 18.5 26 1.8 18.8 1.3 0.8 0.3 0.01 0.3 4.6 0.1 0.1 13.4 14
0
5
10
15
20
25
30
35
PER
ATU
S PPC BERDASARKAN FAKTOR RISIKO 2015 – 2017 NEGERI KEDAH
Peningkatan risiko kesihatan obesiti


ISU KEMATIAN IBU PERKARA ISU
Direct cause
Kematian yang boleh dicegah disebabkan oleh PPH (3) dan HDP (2) disebabkan oleh: -Lewat mengenalpasti dan merawat PPH - Kelemahan pengendalian Placenta Praevia Major di swasta - kelemahan monitoring pre eclampsia - kelemahan pengendalian hypertensive crisis di swasta
Indirect cause -Ibu hamil dengan penyakit kronik tidak mendapat kaunseling secukupnya (PPC) tentang risiko kehamilan semasa merancang untuk hamil - Gagal kenalpasti keterukan penyakit dan tidak merujuk kes
Fortuitous -Kegagalan mengesan/diagnosa penyakit pada semua peringkat jagaan

Absolute Contraindication for Pregnancy (to be follow up/register at PPC)
High grade Pulmonary Hypertension of Any Origin (≥50% of systemic pressure)
Eisenmenger Syndrome
Severe Heart Failure (NYHA class III/IV)
Severe Left Heart Obstruction (Aortic Stenosis with average pressure gradient >50 mmHg, High grade Aortic isthmus stenosis –recurrent)
Severe Mitral Stenosis (Average pressure gradient > 10 mmHg, valve aperture area < 1cm2)
Marfan Syndrome with ectasia of the aorta ascendens(≥ 45mm)
Cyanotic Heart Disease (especiallywith oxigen saturation < 80%)

What did we do?

Health
Maintenance
Post
Reproductive
Years
Pre-pregnancy
Planning Pregnancy Postpartum
Newborn (a new life)
The Women’s Health Continuum
A set of intervention that aim to identify and modify biomedical, behavioural, and social risks to a woman’s health or pregnancy outcome through prevention and management, emphasizing those factors that must be acted on before conception or early in pregnancy to have maximal impact (CDC,2006)
Definition-PRE PREGNANCY CARE (PPC)

Process of care PPC in Health Clinics and Hospitals
Health Clinics Klinik Bandar Hospital
MCH: Family Planning Child Health services Postnatal services Women’s health
OPD: NCD Wellness services Premarital screening Thalasemia screening Adolescent services MMT/NSEP
OPD: NCD Wellness services Premarital screening Thalasemia screening Adolescent services MMT/NSEP
Specialist clinics: MOPD SOPD O&G Orthopaedic Cardiology Nephrology
Women in reproductive age of 15-55 years Women in reproductive age of 15-
55 years
Risk Factor?
Absent Present
History taking by screening format Physical Examination Laboratory investigation
Refer MO/FMS
*Referral
Follow up
Pre-pregnancy care (integrated) Counseling
Health education Family Planning Preparation for next pregnancy
PPC in O& G Hospital
History taking by screening format Physical examination Laboratory investigation
Follow up


Pre Pregnancy Care / Pre Conception Care
• To be made available to all women
• Not only to women who wishes to conceive
• But all woman in reproductive age who has the potential to conceive
• With or without partner
• Gives an opportunity for health screening and care
• Primary interventions

Examples of Primary Prevention Opportunities: Congenital Anomalies
The Opportunity: The Potential Benefit:
Prevention of neural tube defects
50-70% can be prevented if a woman
has adequate levels of folic acid
during earliest weeks of
organogenesis—before she receives
her prenatal vitamins
Birth Defects related to poor glycemic
control of mother (including sacral
agenesis, cardiac defects and neural
tube defects)
Can be reduced from ~10% to 2-3%
through glycemic control of the
woman before organogenesis

Examples of Primary Prevention Opportunities: Congenital Anomalies
The Opportunity: The Potential Benefit:
Minimize a prospective
mother’s contact with
teratogenic exposures such
as prescribed medications,
environmental exposures and
alcohol
Teratogenic substances
interfere with normal organ
development primarily during
the period of organogenesis

PPC in Kedah
• We started to do the ground work in 2010
• Guideline and general flow process 2011
• Implementation one KK one district – middle of 2011
• Implementation of all KKs – 2012
• Implementation in hospital 2013 – there was a glitch – no budget for family planning, so a bit delayed
• 2014 – PPC at hospital
• Implementation and collaboration between KK and hospital strengthened – middle of 2014
• 2015 – KK started to receive budget for Implanon NXT
• 2016 – auditing at KK
• 2016 onwards plan of action and further strengthening of the program

What did we offer?
Primary Prevention Opportunities

PPC in Kedah – Primary Care a Broader Perspective
• Target – women in reproductive age – 16 to 50 of age
• Screening for potential medical condition
• Intervention to the high risk group
• Intervention for the pre diabetes / obese
• Optimization for their medical conditions
• Stress management
• Family Planning
• Vaccination
• Psychosocial support

Who are in the PPC team?
All Levels of Health Care Providers
(Multidisciplinary Team Based Approach)

Team Members
• Doctors / FMSes
• Paramedics
• Nurse Educator
• Dietician / Nutritionist
• Physical Therapist / Physiotherapist
• Occupational Therapists
• Pharmacist
• Psychologist / counselor
• O & G specialists / medical and other specialties (referral point)

• Established Diabetes Mellitus / Newly Diagnosed Diabetes Mellitus in pregnancy / GDM – IGT – Diet Control / Positive OGTT 6 weeks post partum
• In reproductive age (16 – 50)
• Men / husband / partner
• Any woman with medical conditions / risk factor
• Refer individually / together with partner
Who to refer to PPC

•Hospital with specialist
•Hospital without specialist
•Health Clinics (OPD/MCH) •GP clinics
•Private Medical Centers
•RSAT •LPPKN
Who can refer

Primary Care Perspectives
• FMS to lead the team • Integration of all discipline for one aim • Intervention programs • Can be conducted at OPD / Family Health Unit / NCD
unit • Continuity of care cycle between antenatal and PPC
Services • Multiple point of entries (child health / maternal /
BSSK / OPD / Chronic Disease Care unit / Saringan Pra Perkahwinan etc)

PPC – at tertiary / secondary level
• Receive referral cases at various point of entry
• Co-ordination and joint care with other disciplines
• Handles difficult cases that need sub specialized counseling eg. Genetic counseling etc.
• Referral back to primary care
• Able to focus on complicated cases

Flow Chart PPC in Kota Setar

Components of Pre Pregnancy Care

Components of Pre Pregnancy Care
• Risk assessment (screening)
• Health promotion (primary prevention example vaccine)
• Interventions for identified risks (intervention of medical / psychological / social risk factors)
• Optimization & intensification of various medical conditions
• Family Planning (integration with Wellness Clinic)
• Implementation and monitoring

Pre Pregnancy Care Risk Assessment (1)
• Reproductive life plan
• Reproductive history
• Medical and surgical history
• Medication use
• Infections and immunizations
• Genetic screening and family history

Pre Pregnancy Care Risk Assessment (2)
• Nutritional assessment
• Smoking & Substance abuse
• Toxins and teratogenic agents
• Psychosocial concerns
• Physical exam
• Laboratory testing

Pre Pregnancy Care Health promotion
• Family Planning
• Healthy weight and nutrition
• Healthy behaviors
• Stress resilience
• Healthy environments
• Inter-conception care

Pre Pregnancy Care - Interventions for Identified Risks & Medical Conditions
• Folic acid supplementation
• Rubella testing, vac. If necessary
• Control of pre-gestational DM
• Management of hypothyroidism, HPT etc
• Avoidance of teratogenic agents like accutane, coumadin, some anticonvulsants, alcohol, tobacco
• NCD intervention program
• Optimization & Intensification
• Referral if necessary

Pre Pregnancy Care - Implementation
• PPC should not occur only in selected in primary care clinics
• It should be implemented in all primary care clinics & hospitals
• Private and government (including collaboration) • Should be for all women in reproductive age –
opportunistic modality • Every women must have a reproductive life plan • Men should be involved • If planning for a conception – PPC should be regular • PPC should be promoted in the community –
awareness drive / campaign etc

Family Planning
• WHO Medical Eligibility Criteria
• Patient friendly
• Acceptable to patient and husband
• Availability
• Refer to O & G clinic for further assistance
• Refer to health clinics if patient can’t afford from private
• Promote universally

Male Role in Preparing for Pregnancy
Male planning to become father should:
Review family medical & genetic hx
Practice STD risk-reduction behaviors.
Avoid tobacco, alcohol, illicit/street drugs,
chemical exposure.
Assess financial status.
Be supportive of partner.
Play active role in pre-pregnancy planning.



PPC Check List

Flow Chart Defaulter Tracing

On going process of strengthening PPC
(audits, improvement and plan of action)

Defaulter Tracing Team
• Done in OPD / multidisciplinary referral system within KK
• FMS leader
• 2 MOs in charge / PJ / JK / JM / PPP (kanan)
• Documentation – clear & legible & complete
• Registration
• Defaulter tracing – every 2 weeks (JM) > trace card > matron audit > trace patient
• Audits – MO or FMS
• Charting and updating registration – JM / SN
• BSSK issues

Weakness points
• Missed registration
• Defaulter tracing poor
• Poor charting
• Clinical audit – MO does not fulfil component of PPC, commonly on FP, supplementation, other disease screening example anemia
• Patients were not treated to target
• No definitive counseling example – ‘not to conceive until HbA1C < 6.5%’
• Type of family planning

PPC Clinical Audit Component
• Optimization of existing Medical Illness • Screening for other medical condition (NCD, STIs) • Managing patient using team based multidisciplinary
approach (Physio, OT, PSP, Dietician, Pharmacist, Hospital Referral)
• Supplementation (example iron, folic acid) • Social (smoking, substance abuse) • Vaccination • Genetic counseling / referral • Mental health screening • Family Planning • Management of other medical conditions example
obesity, dyslipidaemia

Remedial Measures
• Activity of PPC team in line with pelan tindakan kesihatan keluarga negeri 2016 / 2017 / 2018
• Every team member has specified duty / responsibility • Example – JM – Defaulter tracing, registration, card tracing • JK – screening, registration, charting, basic counseling • FMS / PJ / MOs – audit, monitoring, meetings, planning,
strategizing • CMEs, FAQ confrontation to staffs, drills, case scenarios • Regular audits • Implementation of FDC • Meetings on pencapaian /audit every 3 months (now every 4 months)

Benefits of Pre Pregnancy Care

Giving Protection
Examples of giving protection: • Folic acid supplementation to protect against neural tube defects and
other congenital anomalies
• Examples of immunizations against infectious diseases that can impact pregnancy outcomes:
• Rubella
• Varicella
• Hepatitis B

Preconception Interventions: Give protection
•Folic Acid Supplements: Reduce the occurrence of neural tube defects by two thirds
•Rubella Sero-negativity: Rubella immunization provides protective sero-positivity and prevents the occurrence of congenital rubella syndrome
•HIV/AIDS: timely antiretroviral treatment can be administered, pregnancies can be better planned
•Hepatitis B: Vaccination is recommended for men and women who are at risk for acquiring hepatitis B virus (HBV) infection.

Managing Conditions
Examples of conditions known to be detrimental to reproductive outcomes if in poor control before conception:
•Diabetes
•Maternal PKU
•Obesity
•Hypothyroidism
•Sexually transmitted infections

Preconception Interventions: Manage conditions
•Diabetes: 3-fold increase in birth defects among infants of women with type
1 and type 2 diabetes, without management
•Hypothyroidism: Dosage of Levothyroxine should be adjusted in early
pregnancy to maintain levels needed for neurological development
•Maternal PKU: Low phenylalanine diet before conception and
throughout pregnancy prevents mental retardation in infants born to mothers
with PKU
•Obesity: Associated adverse outcomes include neural tube defects, preterm
birth, c-section, hypertensive and thromboembolic disease.
•STDs: have been strongly associated with ectopic pregnancy, infertility, and
chronic pelvic pain.

Avoiding Exposures
Examples of exposures known to be teratogenic or otherwise harmful in early pregnancy:
• Medications: • Many antiseizure medications
• Oral anticoagulants
• Accutane
• Others
• Alcohol
• Tobacco

SUBSTANCE USE
Impact of alcohol use on women’s health:
• Risk for motor vehicle and other accidents
• Risk for unintended pregnancy
• Risk for addiction
• Risk for nutritional depletions and inadequacies
Impact of alcohol use on reproductive outcomes:
• Delayed fertility
• Increased SABs
• Fetal alcohol spectrum disorders (full fetal alcohol syndrome can only occur with fetal exposure between days 17-56 of gestation)

SUBSTANCE USE
Impact of tobacco use on women’s health:
• Implicated in most of the leading causes of death for women:
• Heart disease (#1 cause of death)
• Stroke (#2)
• Lung cancer (#3)
• Lung disease (#4)
Impact of tobacco use on reproductive outcomes:
• Leading preventable cause of infant mortality and morbidity
• Preventable cause of low birth weight and prematurity
• Associated with placental abnormalities including placenta previa and placenta abruptio

Controllable Risk Factors: Drug, Alcohol, Tobacco Use
Alcohol:. Avoid all alcohol during time attempting conception/pregnancy.
No known safe level during pregnancy. Associated with malformation, slow fetal growth, fetal death, low birth-weight, CNS abnormalities, neurologicaldefects, spontaneous abortion, abruption.
Tobacco: Associated with spontaneous abortion, ectopic pregnancy; low birth-weight, infant mortality. Can potentially decrease fertility. Vasoconstriction restricts blood flow to fetus & reduces % of oxygen & nutrients carried by blood.

Illicit or Street Drugs: May be associated with severe medical & developmental problems in newborns.
1. Marijuana, most common - tend to have babies earlier & may be smaller than term babies.
2. Cocaine: associated with miscarriage, abruption, low birth-weight, premature birth, brain damage.
3. Heroin - IV drug users - evaluate for AIDS & Hep B. In HIV + women, studies show treatment with AZT reduces transmission to baby from ~ 25% to 8%.

NUTRITIONAL STATUS: Obesity
Impact of obesity on women’s health:
• Diabetes
• Hypertension
• Cardiovascular disease
• Disabilities
Impact of maternal obesity on reproductive outcomes:
• Glucose intolerance of pregnancy
• Pregnancy induced hypertension
• Thrombophlebitis
• Infertility
• Neural tube defects
• Prematurity

NUTRITIONAL STATUS: Underweight
Impact of being underweight on women’s health:
Risk of osteoporosis in later life
Fragile health status
Impact of low pregravid weight on reproductive outcomes:
Infertility
Low birth weight
Prematurity

Supplementation
• Supplementation – (only 15.2% women in Malaysia have adequate folate from dietary intake that have adequate protections against NTD at birth) – obese women need a higher level of folate intake (0.6 mg daily)
• Folate – at least 3 months prior to pregnancy
• Calcium supplement?

Evidence-based interventions: Selected examples
• Screening for anemia • Taking a thorough family history • Family planning • Genetic counselling • Carrier screening and testing • Appropriate treatment • Providing community-based education • Community-wide or national screening
among populations at high risk • Population-wide screening
Genetic conditions
Areas addressed by the
preconception care package
Evidence-based interventions

Evidence-based interventions: Selected examples
• Keeping girls in school • Influencing cultural norms that support early marriage and
coerced sex • Creating visible, high-level support for pregnancy prevention
programmes • Educating girls and boys about sexuality, reproductive health
and contraceptive use • Building community support for preventing early pregnancy
and for contraceptive provision to adolescents • Enabling adolescents to obtain contraceptive services • Empowering girls to resist coerced sex • Engaging men and boys to critically assess norms and practices
regarding gender-based violence and coerced sex • Educating women and couples about the dangers to the baby
and mother of short birth intervals • Providing contraceptives
Too-early, unwanted and rapid successive pregnancy
Areas addressed by the preconception care package
Evidence-based interventions

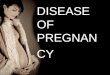
Stress Management Techniques
Relaxation & deep breathing. Planning
pregnancy can be stressful.
Stress reduction enhances chances of
conception.
Excessive stress can lead to premature birth & low
birth weight. Sleep 8-10 hr.with frequent rest periods a
day.

Conclusion

For Every Woman of Childbearing Potential, Every Time She is Seen
• Identify modifiable and non modifiable risk factors for poor health and poor pregnancy outcomes before conception
•Provide timely counseling about risks and strategies to reduce the potential impact of the risks
•Provide risk reduction strategies consistent with best practices.

“Every Woman, Every Time” is Opportunistic Care
• Takes advantage of all health care encounters to stress prevention opportunities throughout the lifespan
• Recognizes that in almost all cases preconception wellness results in good health for women, irrespective of pregnancy intentions
• Addresses conception and contraception choices at every encounter
• Involves all medical specialties—not only those directly involved in reproductive health