Embed Size (px)
Citation preview

高血壓治療新趨勢
Name: 黃文伸Date: 97.06.27
Topics
• 高血壓之控制率
• 高血壓用藥之選擇
• Fix-Dose Combination之優勢
• 血壓藥之發展趨勢
Topics
• 高血壓之控制率
• 高血壓用藥之選擇
• Fix-Dose Combination之優勢
• 血壓藥之發展趨勢
三高 (代謝症候群)
難分難解的三角習題
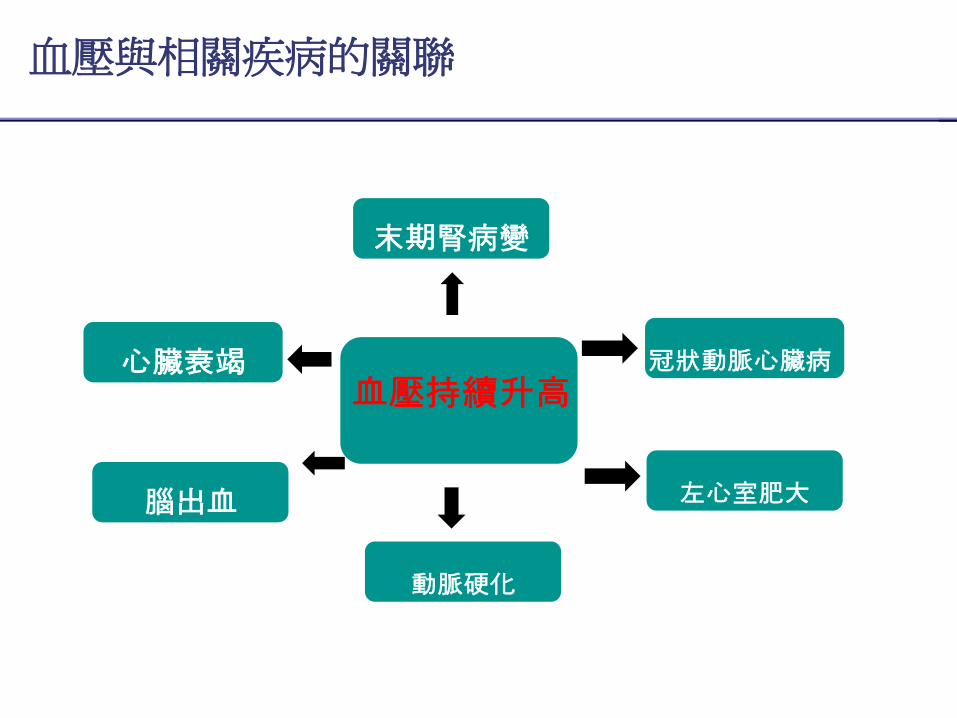
血壓與相關疾病的關聯
血壓持續升高冠狀動脈心臟病
左心室肥大
心臟衰竭
腦出血
動脈硬化
末期腎病變
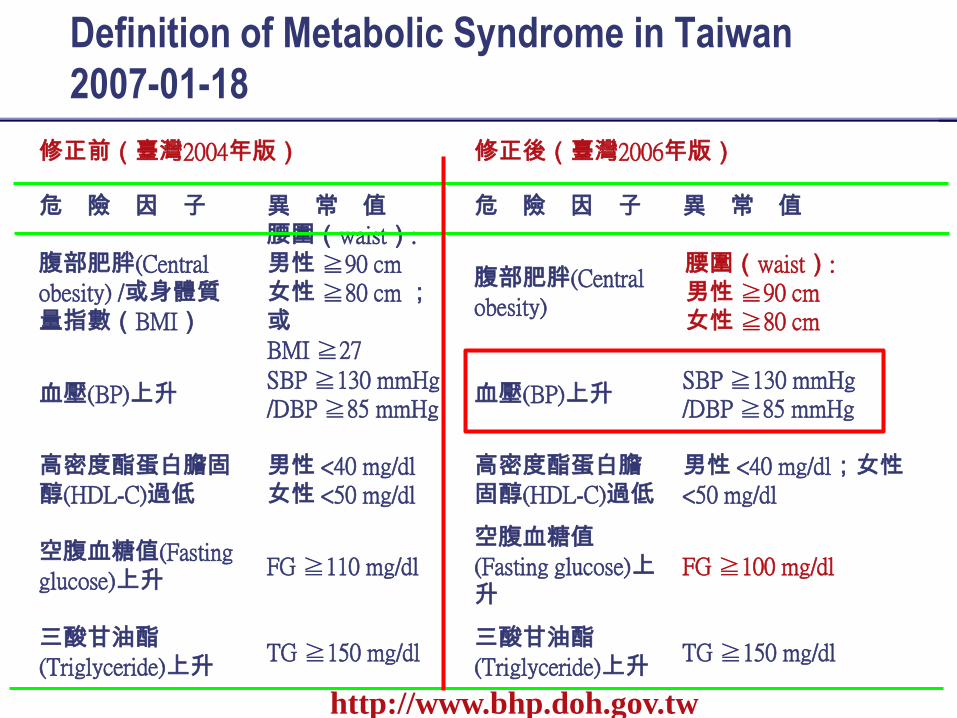
Definition of Metabolic Syndrome in Taiwan
2007-01-18
修正前(臺灣2004年版) 修正後(臺灣2006年版)
危 險 因 子 異 常 值 危 險 因 子 異 常 值
腹部肥胖(Central obesity) /或身體質
量指數(BMI)
腰圍(waist):男性 ≧90 cm 女性 ≧80 cm ;或
BMI ≧27
腹部肥胖(Central obesity)
腰圍(waist):男性 ≧90 cm女性 ≧80 cm
血壓(BP)上升SBP ≧130 mmHg /DBP ≧85 mmHg
血壓(BP)上升SBP ≧130 mmHg /DBP ≧85 mmHg
高密度酯蛋白膽固
醇(HDL-C)過低
男性 <40 mg/dl女性 <50 mg/dl
高密度酯蛋白膽
固醇(HDL-C)過低
男性 <40 mg/dl;女性
<50 mg/dl
空腹血糖值(Fasting glucose)上升
FG ≧110 mg/dl空腹血糖值
(Fasting glucose)上升
FG ≧100 mg/dl
三酸甘油酯
(Triglyceride)上升TG ≧150 mg/dl
三酸甘油酯
(Triglyceride)上升TG ≧150 mg/dl
http://www.bhp.doh.gov.tw
1177-SL-08-01
8
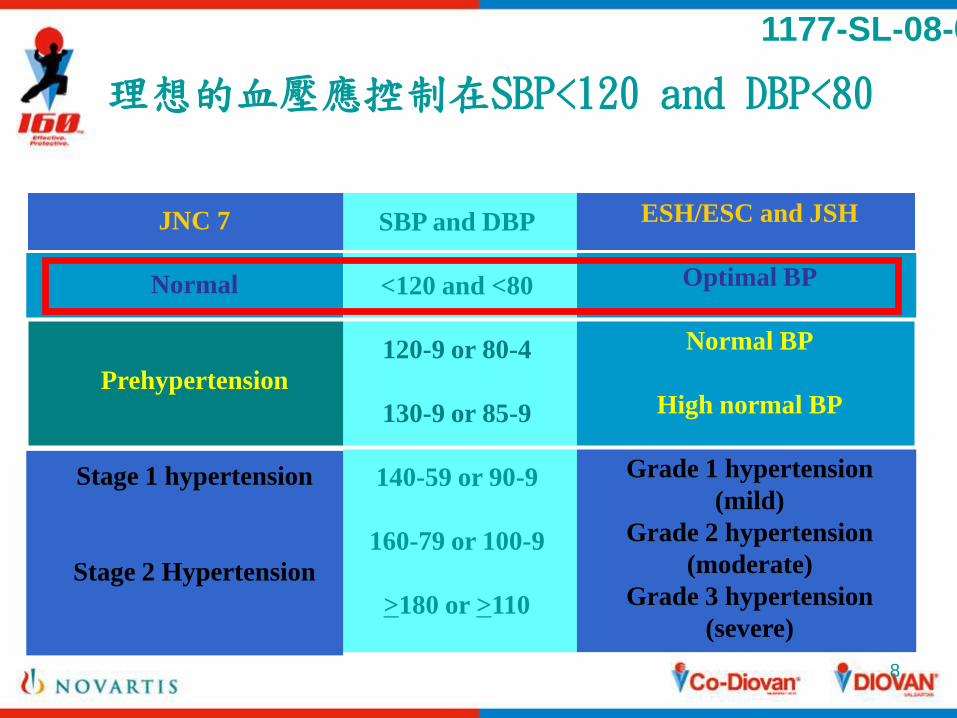
ESH/ESC and JSH
Optimal BP
Normal BP
High normal BP
Grade 1 hypertension
(mild)
Grade 2 hypertension
(moderate)
Grade 3 hypertension
(severe)
SBP and DBP
<120 and <80
120-9 or 80-4
130-9 or 85-9
140-59 or 90-9
160-79 or 100-9
>180 or >110
理想的血壓應控制在SBP<120 and DBP<80
JNC 7
Normal
Prehypertension
Stage 1 hypertension
Stage 2 Hypertension
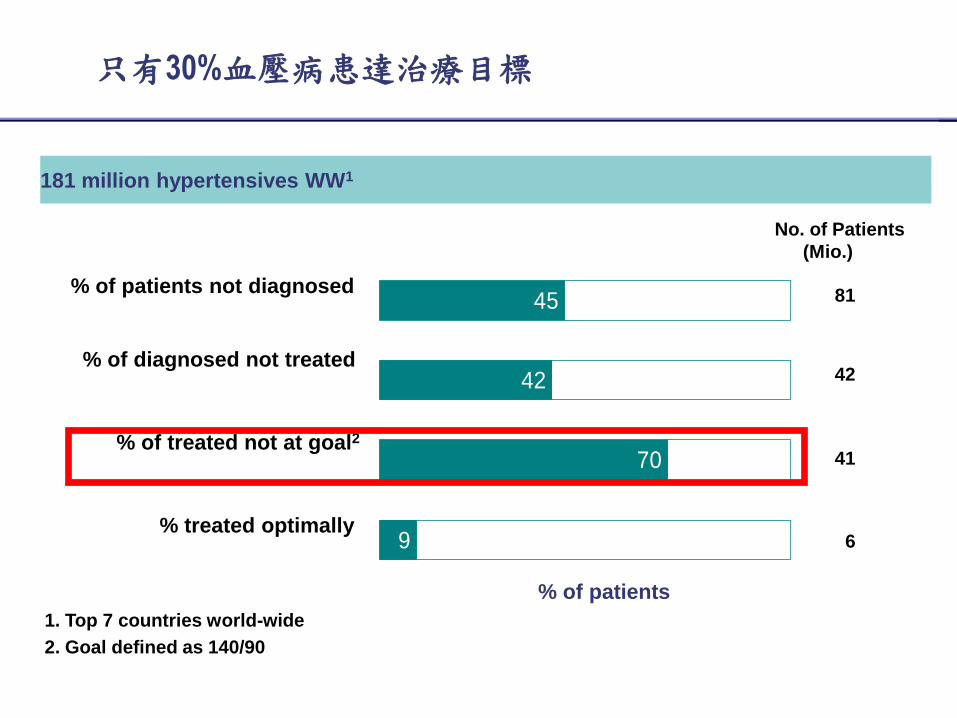
只有30%血壓病患達治療目標
1. Top 7 countries world-wide
2. Goal defined as 140/90
% of patients not diagnosed
% of patients
% of diagnosed not treated
% of treated not at goal2
% treated optimally
45
42
70
9
181 million hypertensives WW1
81
42
41
6
No. of Patients
(Mio.)
10
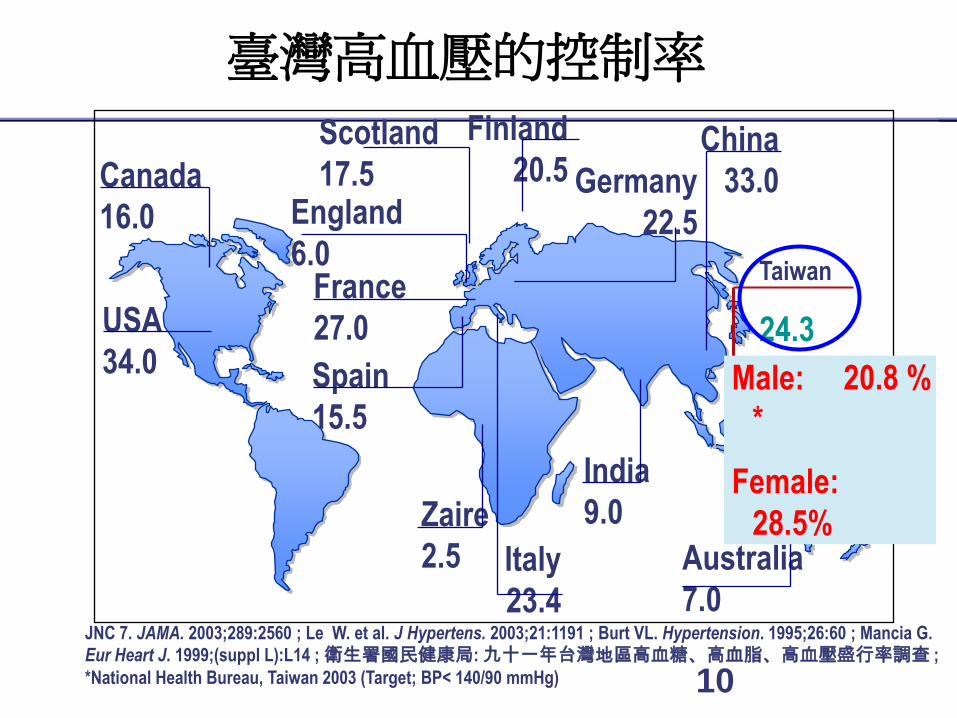
USA
34.0
Canada
16.0
Australia
7.0
Finland
20.5Scotland
17.5 Germany
22.5
Spain
15.5
France
27.0
England
6.0
India
9.0Zaire
2.5 Italy
23.4
臺灣高血壓的控制率
JNC 7. JAMA. 2003;289:2560 ; Le W. et al. J Hypertens. 2003;21:1191 ; Burt VL. Hypertension. 1995;26:60 ; Mancia G.
Eur Heart J. 1999;(suppl L):L14 ; 衛生署國民健康局: 九十一年台灣地區高血糖、高血脂、高血壓盛行率調查 ;
*National Health Bureau, Taiwan 2003 (Target; BP< 140/90 mmHg)
Taiwan
24.3
China
33.0
Male: 20.8 %
*
Female:
28.5%
11
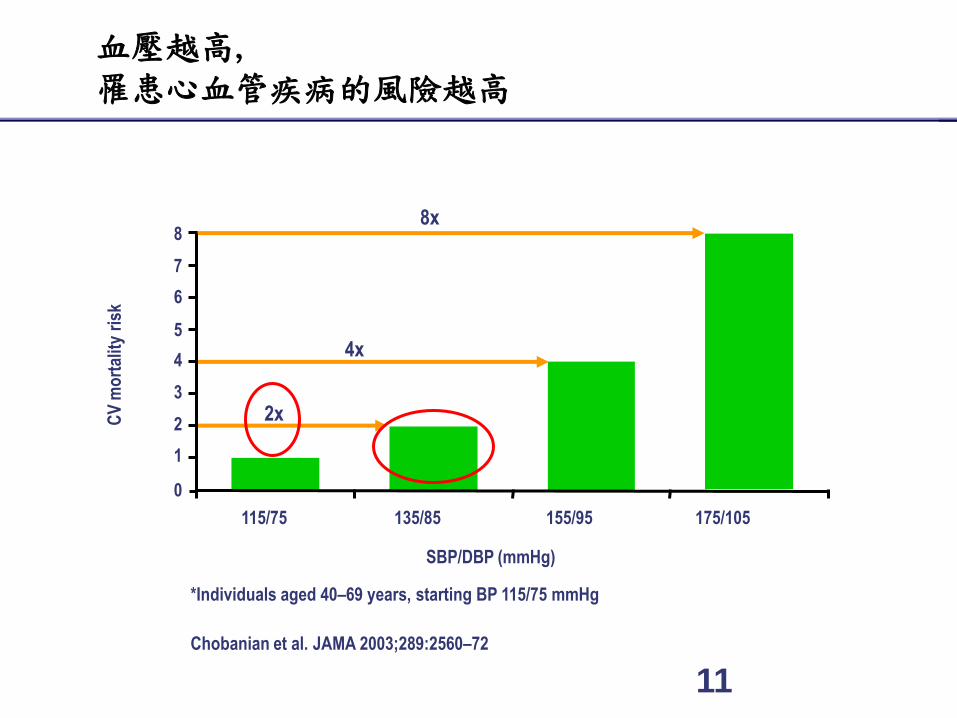
血壓越高,罹患心血管疾病的風險越高
*Individuals aged 40–69 years, starting BP 115/75 mmHg
Chobanian et al. JAMA 2003;289:2560–72
CV
mo
rtal
ity
risk
SBP/DBP (mmHg)
0
1
2
3
4
5
6
7
8
115/75 135/85 155/95 175/105
2x
4x
8x
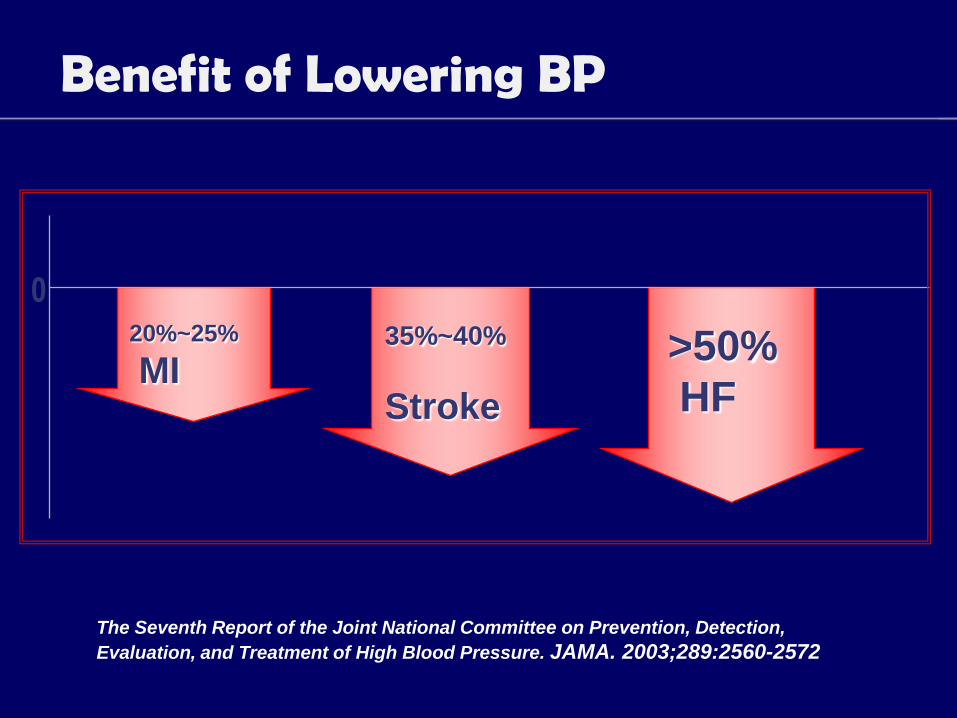
Benefit of Lowering BP
20%~25%
MI35%~40%
Stroke
>50%
HF
0
The Seventh Report of the Joint National Committee on Prevention, Detection,
Evaluation, and Treatment of High Blood Pressure. JAMA. 2003;289:2560-2572
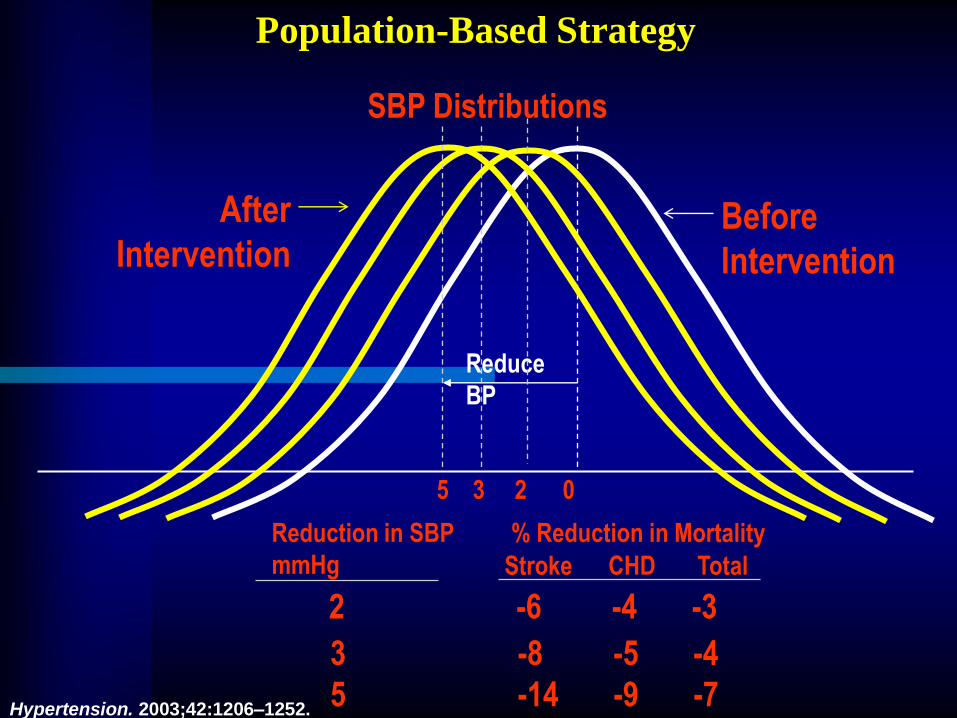
SBP Distributions
Before
Intervention
Reduction in SBP
mmHg
% Reduction in Mortality
Reduce
BP
After
Intervention
2 -6 -4 -3
3 -8 -5 -4
5 -14 -9 -7
Population-Based Strategy
Stroke CHD Total
5 3 2 0
Hypertension. 2003;42:1206–1252.
Topics
• 高血壓之控制率
• 高血壓用藥之選擇
• Fix-Dose Combination之優勢
• 血壓藥之發展趨勢
Selection of Anti-Hypertensive
Agents
Effective – lowering BP efficacy
Compelling indication
2003 WHO/ISH Guideline
2003 ESH/ESC Guideline
2003 JNC 7 Guideline
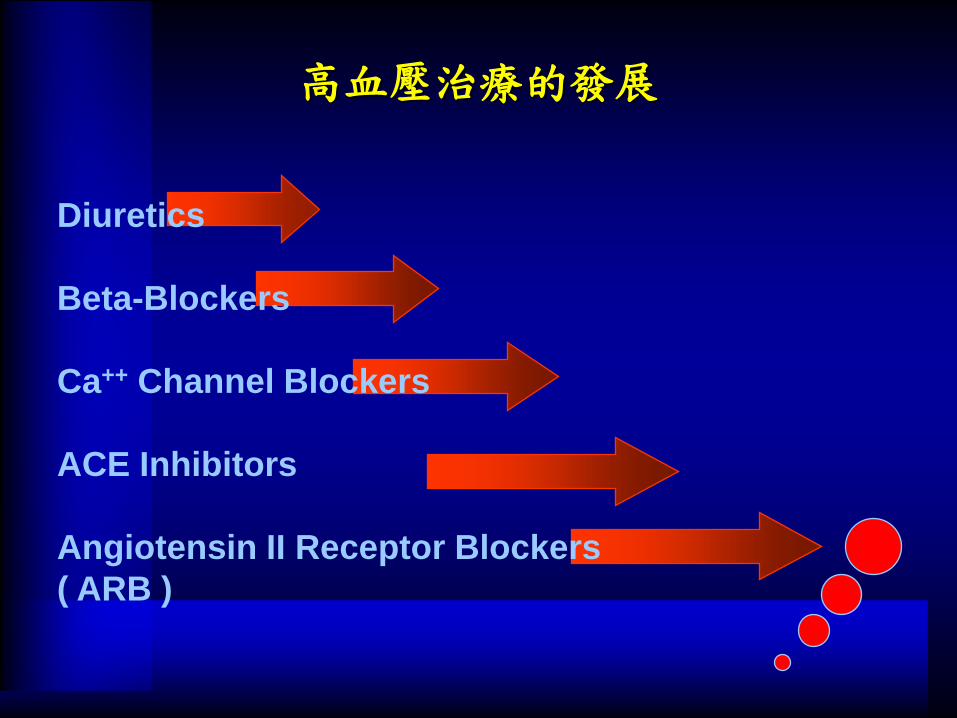
高血壓治療的發展
Diuretics
Beta-Blockers
Ca++ Channel Blockers
ACE Inhibitors
Angiotensin II Receptor Blockers
( ARB )
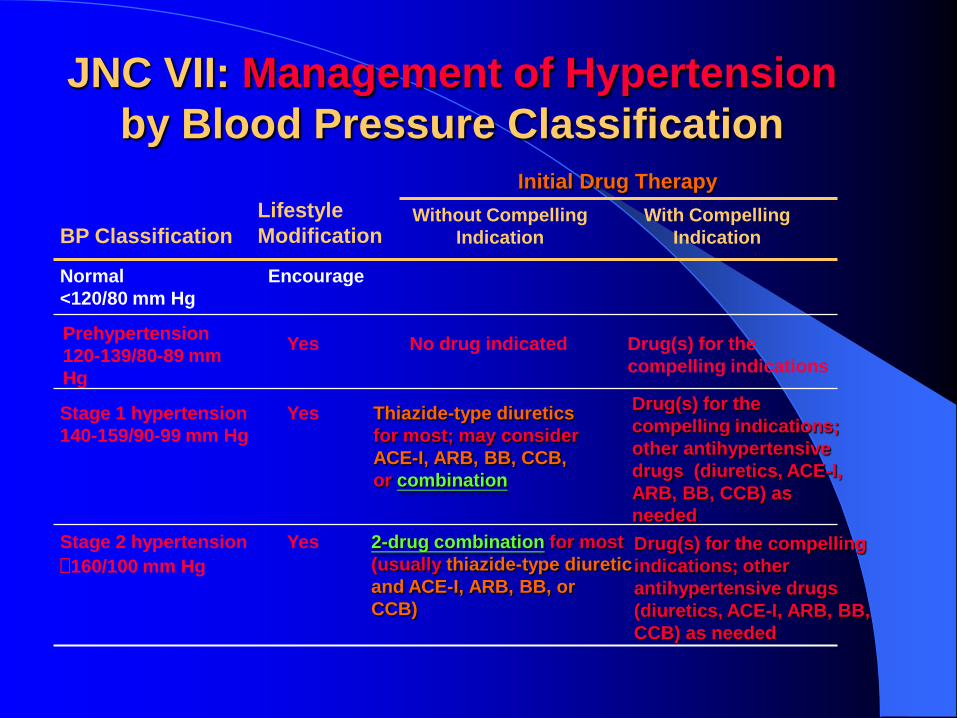
JNC VII: Management of Hypertension
by Blood Pressure Classification
Drug(s) for the compelling
indications; other
antihypertensive drugs
(diuretics, ACE-I, ARB, BB,
CCB) as needed
Drug(s) for the
compelling indications;
other antihypertensive
drugs (diuretics, ACE-I,
ARB, BB, CCB) as
needed
BP Classification
Lifestyle
Modification
Initial Drug Therapy
Without Compelling
Indication
With Compelling
Indication
Normal
<120/80 mm Hg
Prehypertension
120-139/80-89 mm
Hg
Stage 1 hypertension
140-159/90-99 mm Hg
Stage 2 hypertension
160/100 mm Hg
Encourage
Yes
Yes
Yes
No drug indicated Drug(s) for the
compelling indications
Thiazide-type diuretics
for most; may consider
ACE-I, ARB, BB, CCB,
or combination
2-drug combination for most
(usually thiazide-type diuretic
and ACE-I, ARB, BB, or
CCB)
Topics
• 高血壓之控制率
• 高血壓用藥之選擇
• Fix-Dose Combination之優勢
• 血壓藥之發展趨勢
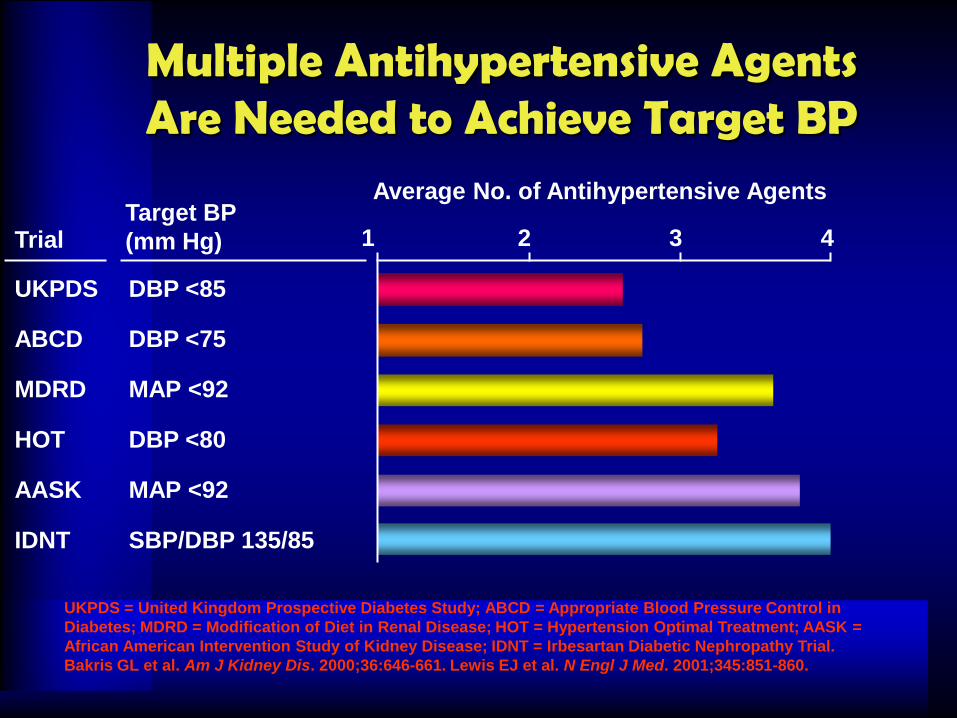
AASK MAP <92
Target BP
(mm Hg)
Average No. of Antihypertensive Agents
1
UKPDS DBP <85
ABCD DBP <75
MDRD MAP <92
HOT DBP <80
Trial 2 3 4
IDNT SBP/DBP 135/85
Multiple Antihypertensive Agents Are Needed to Achieve Target BP
UKPDS = United Kingdom Prospective Diabetes Study; ABCD = Appropriate Blood Pressure Control in
Diabetes; MDRD = Modification of Diet in Renal Disease; HOT = Hypertension Optimal Treatment; AASK =
African American Intervention Study of Kidney Disease; IDNT = Irbesartan Diabetic Nephropathy Trial.
Bakris GL et al. Am J Kidney Dis. 2000;36:646-661. Lewis EJ et al. N Engl J Med. 2001;345:851-860.
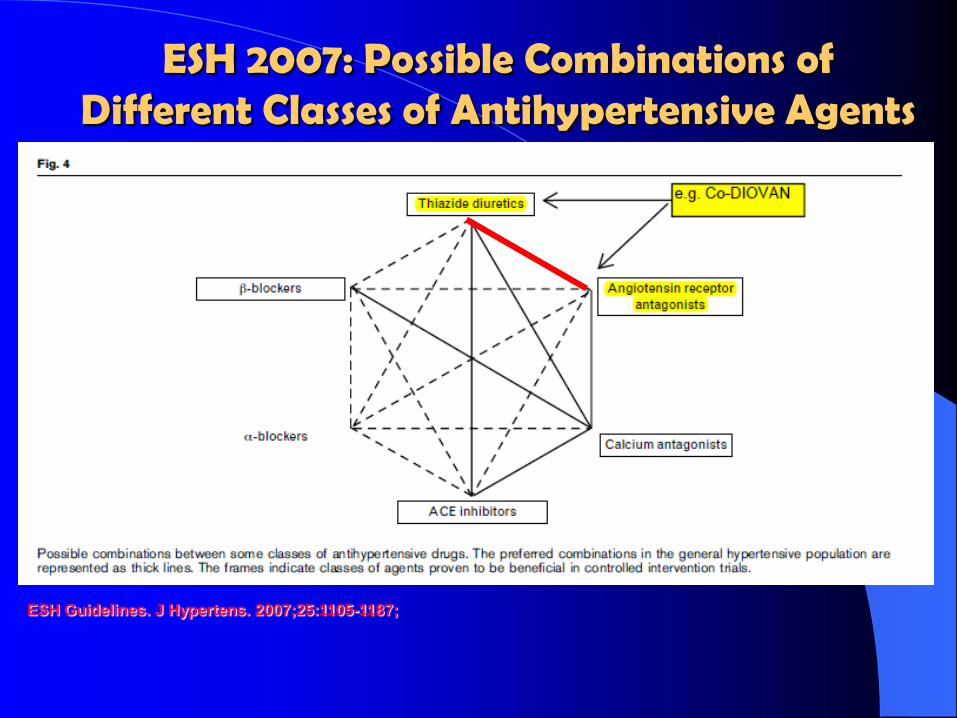
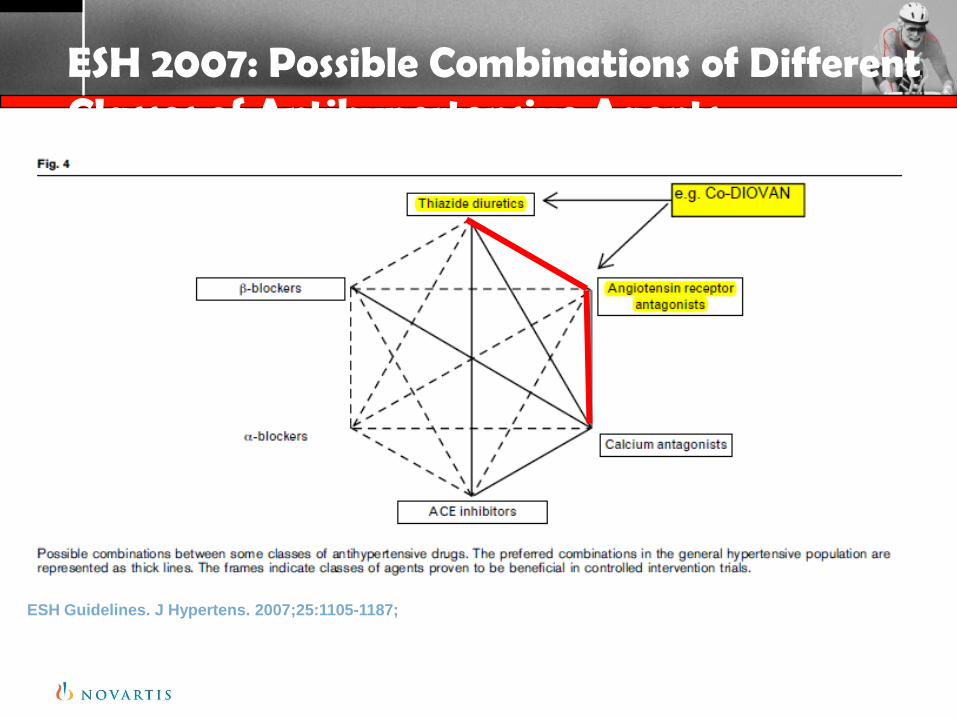
ESH 2007: Possible Combinations of Different Classes of Antihypertensive Agents
ESH Guidelines. J Hypertens. 2007;25:1105-1187;

Co-DIOVAN®
(Valsartan 80mg +12.5mg
HCTZ)
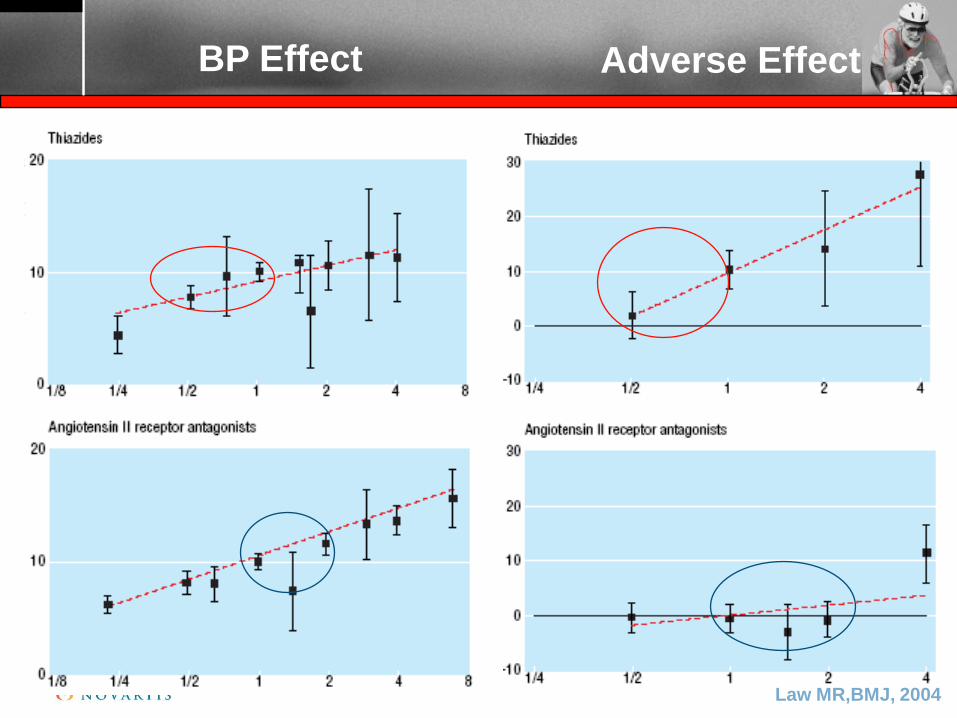
BP Effect Adverse Effect
Law MR,BMJ, 2004
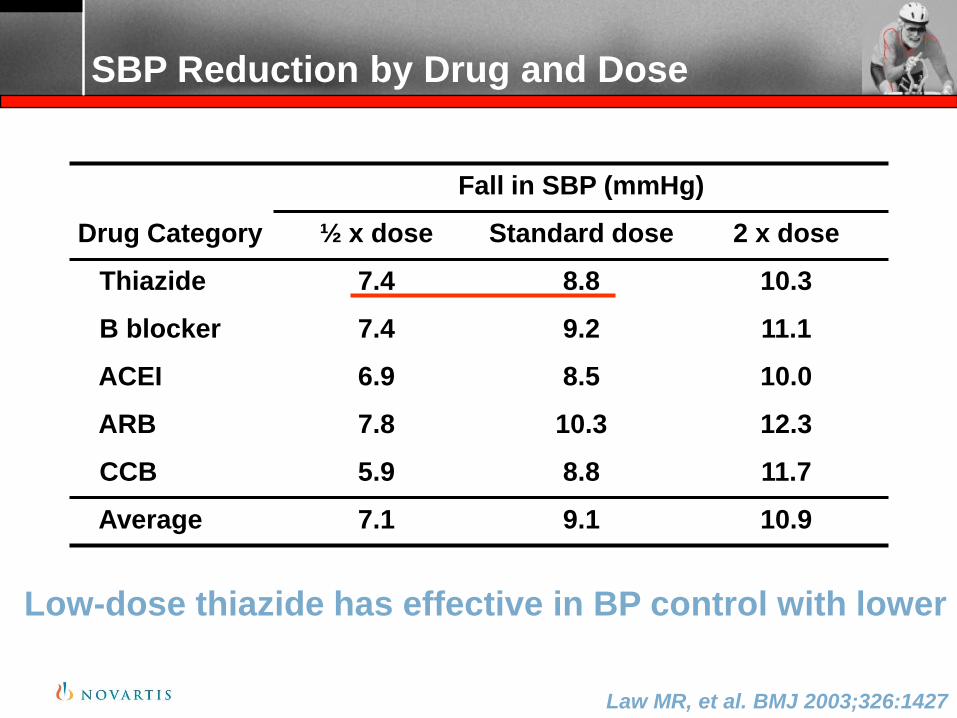
Fall in SBP (mmHg)
Drug Category ½ x dose Standard dose 2 x dose
Thiazide 7.4 8.8 10.3
B blocker 7.4 9.2 11.1
ACEI 6.9 8.5 10.0
ARB 7.8 10.3 12.3
CCB 5.9 8.8 11.7
Average 7.1 9.1 10.9
Law MR, et al. BMJ 2003;326:1427
SBP Reduction by Drug and Dose
Low-dose thiazide has effective in BP control with lower side effect
Law MR, et al. BMJ 2003;326:1427
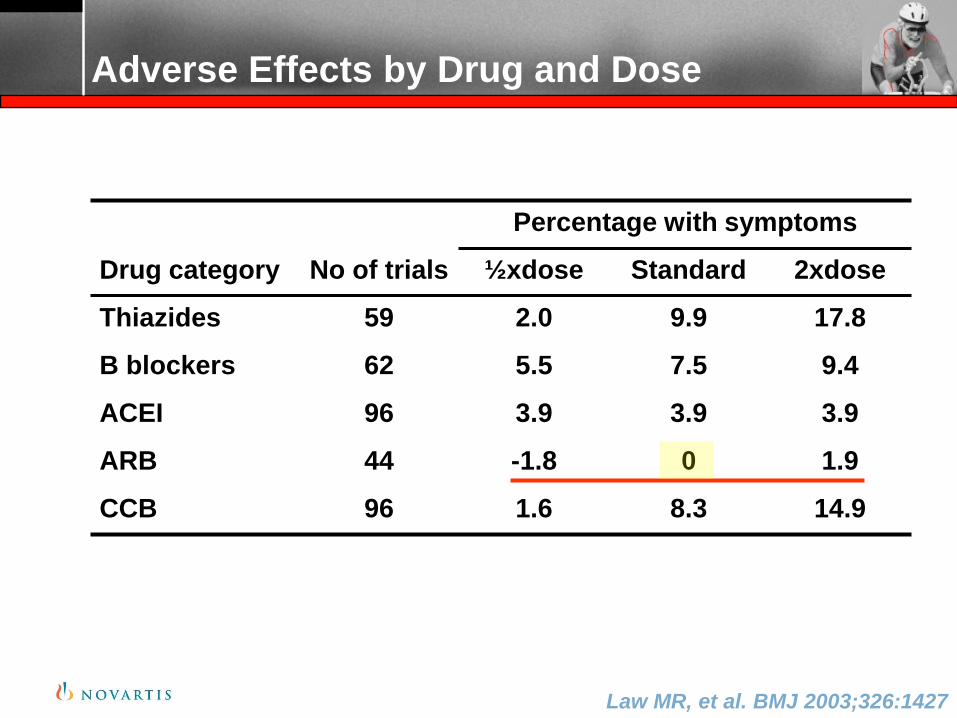
Percentage with symptoms
Drug category No of trials ½ xdose Standard 2xdose
Thiazides 59 2.0 9.9 17.8
B blockers 62 5.5 7.5 9.4
ACEI 96 3.9 3.9 3.9
ARB 44 -1.8 0 1.9
CCB 96 1.6 8.3 14.9
Adverse Effects by Drug and Dose
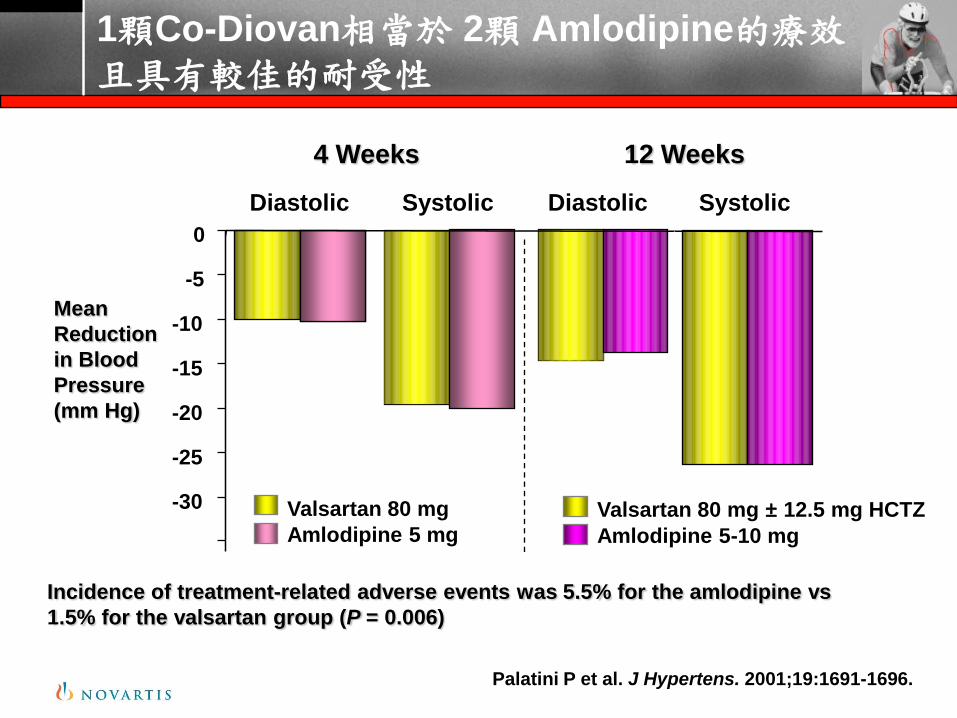
1顆Co-Diovan相當於 2顆 Amlodipine的療效且具有較佳的耐受性
Palatini P et al. J Hypertens. 2001;19:1691-1696.
4 Weeks 12 Weeks
-30
-25
-20
-15
-10
-5
0
Diastolic Systolic Diastolic Systolic
Mean
Reduction
in Blood
Pressure
(mm Hg)
Valsartan 80 mg ± 12.5 mg HCTZ
Amlodipine 5-10 mg
Valsartan 80 mg
Amlodipine 5 mg
Incidence of treatment-related adverse events was 5.5% for the amlodipine vs
1.5% for the valsartan group (P = 0.006)
ESH 2007: Possible Combinations of Different Classes of Antihypertensive Agents
ESH Guidelines. J Hypertens. 2007;25:1105-1187;
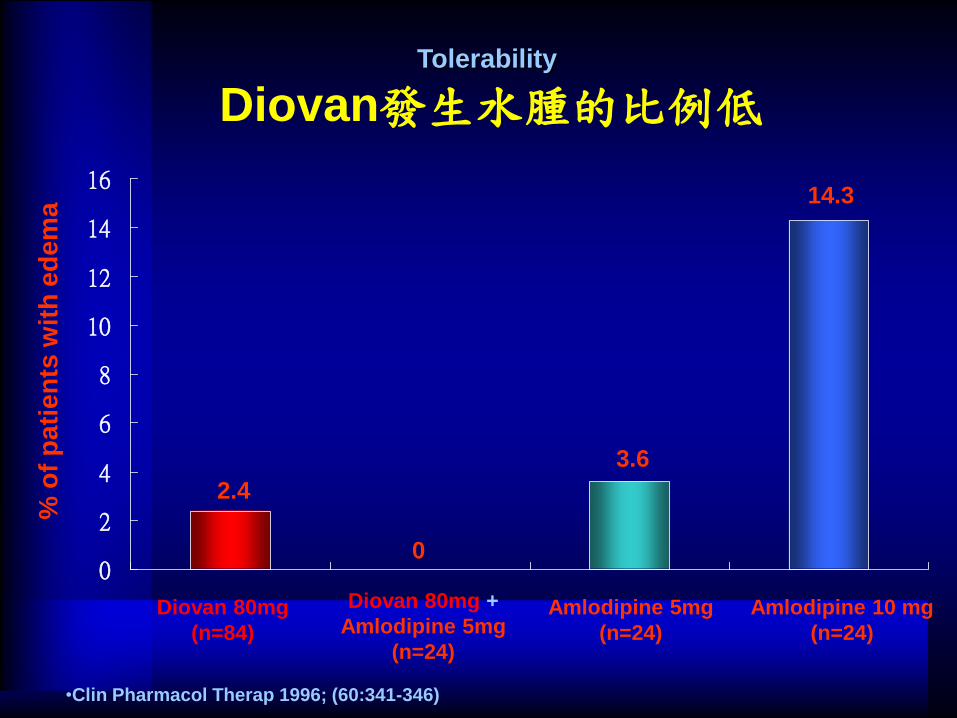
0
2
4
6
8
10
12
14
16
2.4
0
3.6
14.3
Diovan 80mg
(n=84)
Diovan 80mg +
Amlodipine 5mg
(n=24)
Amlodipine 5mg
(n=24)
Amlodipine 10 mg
(n=24)
% o
f p
ati
en
ts w
ith
ed
em
aTolerability
Diovan發生水腫的比例低
•Clin Pharmacol Therap 1996; (60:341-346)
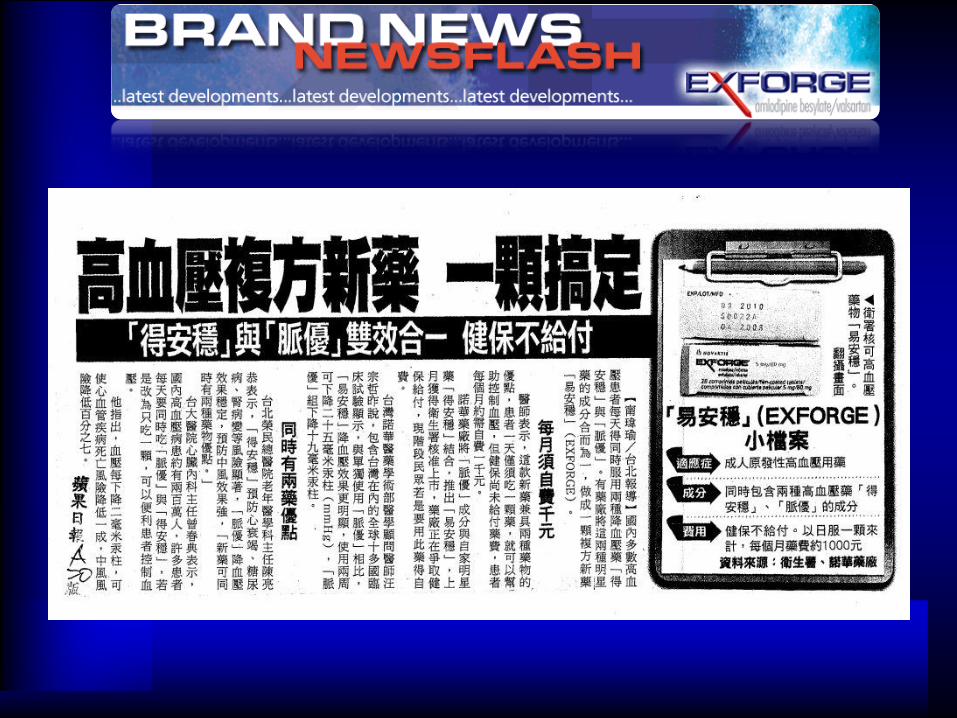
蘋果日報新聞稿
Exforge(易安穩)的正面評價報導
同時有兩藥優點-台北榮民總醫院老年醫學科主任陳亮恭表示,「得安穩」預防心衰竭、糖尿病、腎病變等風險顯著,「脈優」降血壓效果穩定,預防中風效果強,「新藥可同時有兩種藥物優點。」-台大醫院心臟內科主任曾春典表示,國內高血壓病患約有兩百萬人,許多患者每天要同時吃「脈優」與「得安穩」,若是改為只吃一顆,可以便利患者控制血壓。
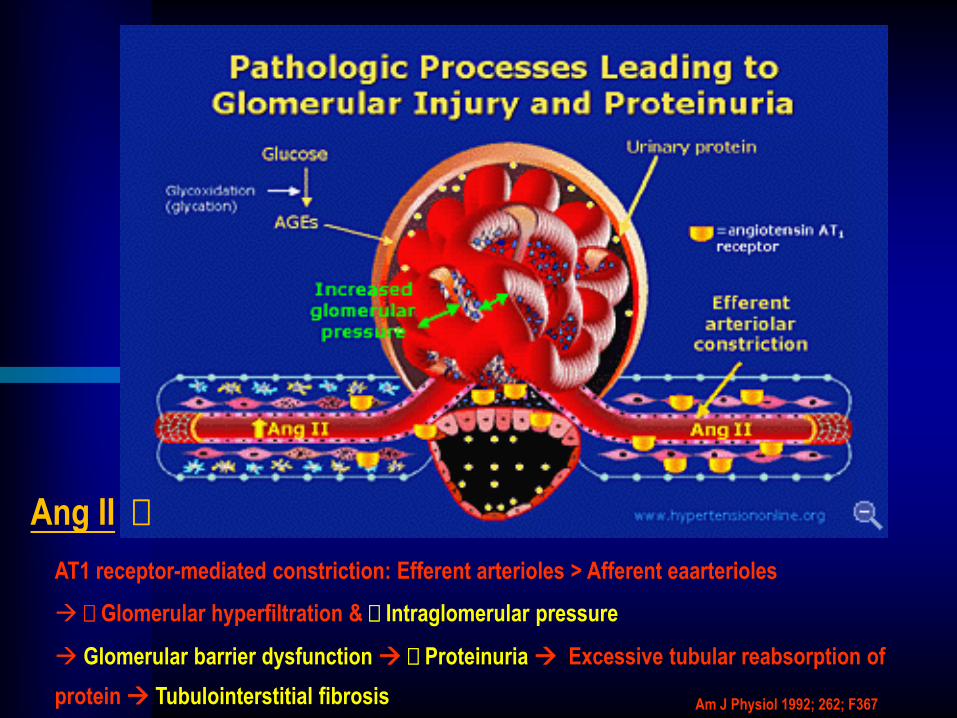
AT1 receptor-mediated constriction: Efferent arterioles > Afferent eaarterioles
Glomerular hyperfiltration & Intraglomerular pressure
Glomerular barrier dysfunction Proteinuria Excessive tubular reabsorption of
protein Tubulointerstitial fibrosis Am J Physiol 1992; 262; F367
Ang II
S
M A
R T
Microalbuminuria Reduction with Intensive
Antihypertensive Treatment by Renin-Angiotensin System-
Blocking or Calcium Channel-Blocking in Hypertensive
Patients with Type 2 Diabetes Mellitus
Shiga MicroAlbumiuria Reduction Trial (SMART) group
Atsunori Kasiwagi, MD, PhD
Professor of Endocrinology and
Metabolism Division,
Shiga University of Medical Science
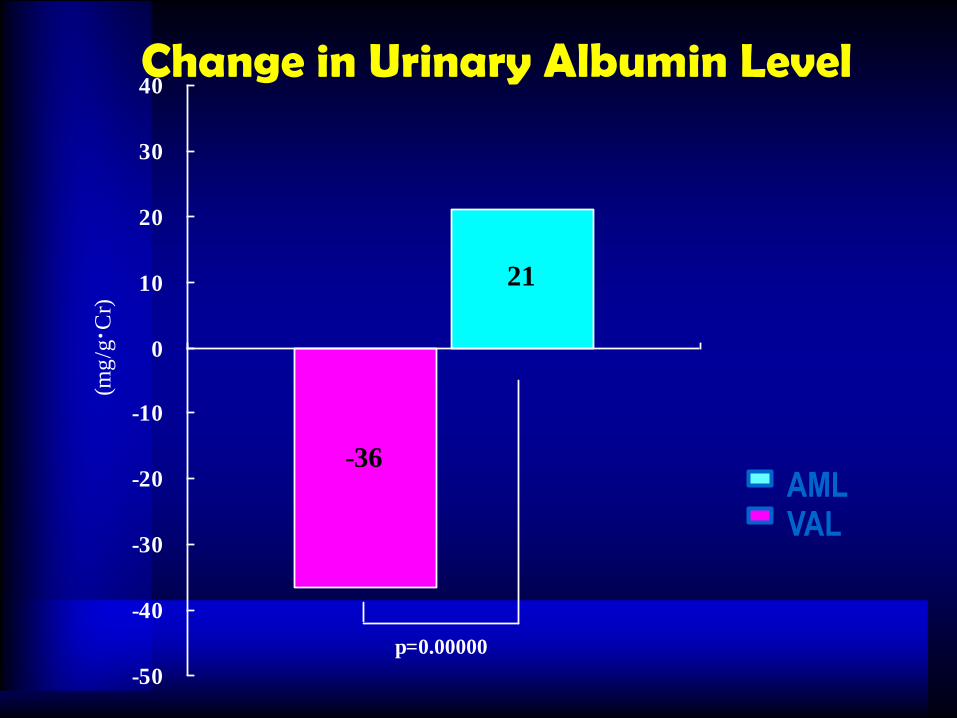
Change in Urinary Albumin Level
-36
21
-50
-40
-30
-20
-10
0
10
20
30
40(m
g/g
・ Cr)
p=0.00000
AMLVAL
Journal of Hypertension 2007, Vol 25 No 9
Albuminuria response to very
high-dose valsartan in type 2
diabetes mellitus
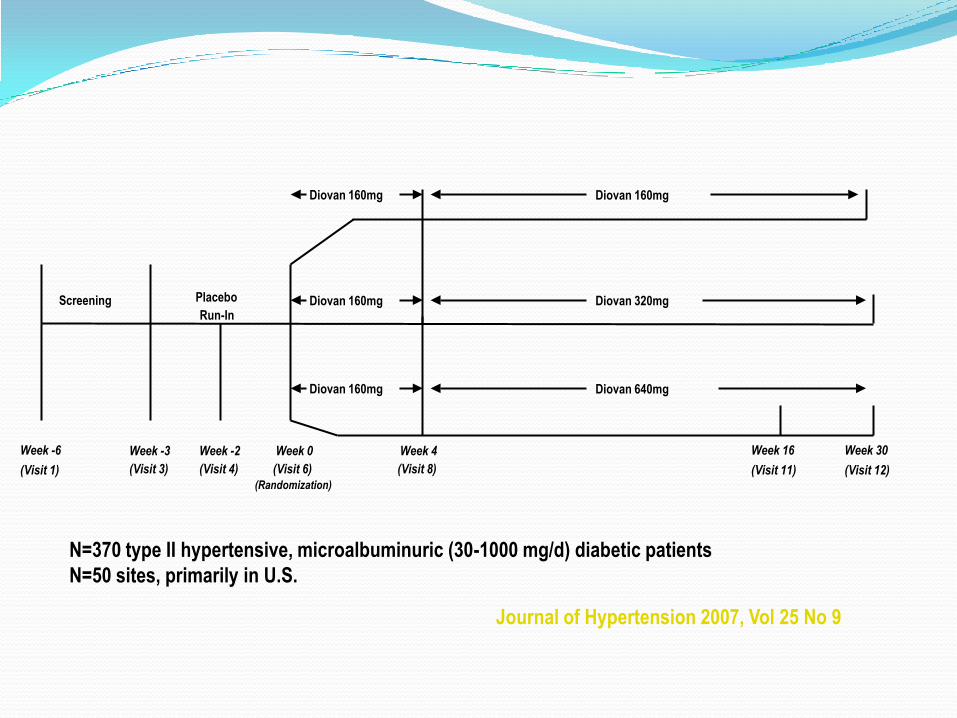
Placebo
Run-In
Diovan 160mg
Week 4
(Visit 8)
Week 0
(Visit 6)
(Randomization)
Diovan 640mg
Diovan 320mg
Diovan 160mg
Week 30
(Visit 12)
Screening
Week -3
(Visit 3)
Week -6
(Visit 1)
Week -2
(Visit 4)
Diovan 160mg
Diovan 160mg
Week 16
(Visit 11)
N=370 type II hypertensive, microalbuminuric (30-1000 mg/d) diabetic patients
N=50 sites, primarily in U.S.
Journal of Hypertension 2007, Vol 25 No 9
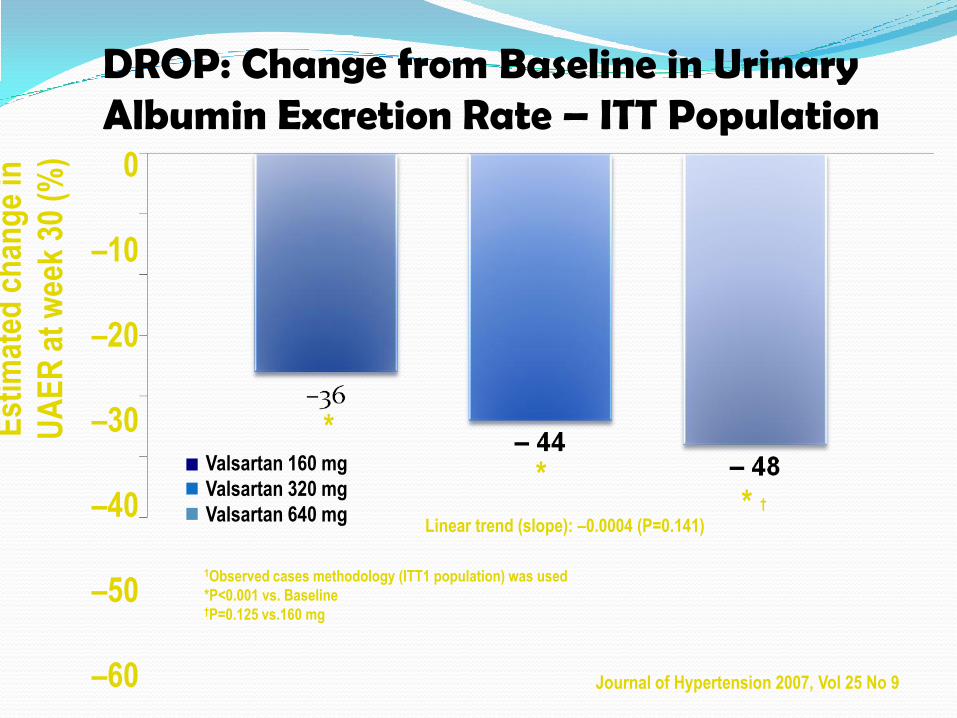
Est
imat
ed c
han
ge
in
UA
ER
at
wee
k 30
(%
)
Valsartan 160 mg
Valsartan 320 mg
Valsartan 640 mg
0
–10
–20
–30
–40
–50
–60
1Observed cases methodology (ITT1 population) was used
*P<0.001 vs. Baseline†P=0.125 vs.160 mg
*
** †
Linear trend (slope): –0.0004 (P=0.141)
DROP: Change from Baseline in Urinary Albumin Excretion Rate – ITT Population
Journal of Hypertension 2007, Vol 25 No 9
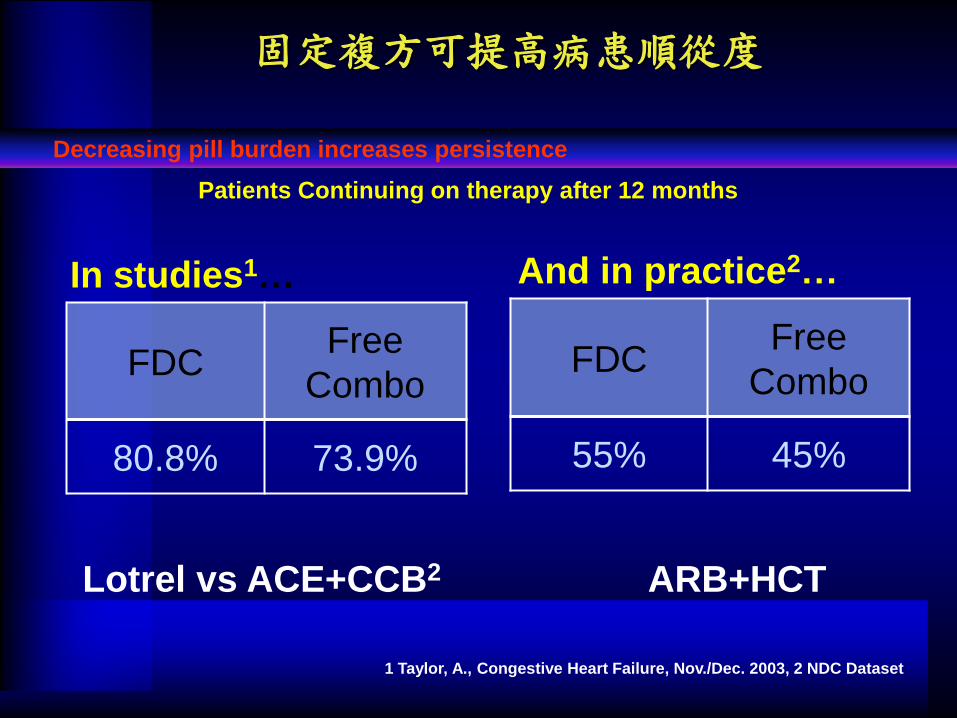
固定複方可提高病患順從度
FDCFree
Combo
80.8% 73.9%
1 Taylor, A., Congestive Heart Failure, Nov./Dec. 2003, 2 NDC Dataset
FDCFree
Combo
55% 45%
In studies1… And in practice2…
Lotrel vs ACE+CCB2 ARB+HCT
Patients Continuing on therapy after 12 months
Decreasing pill burden increases persistence
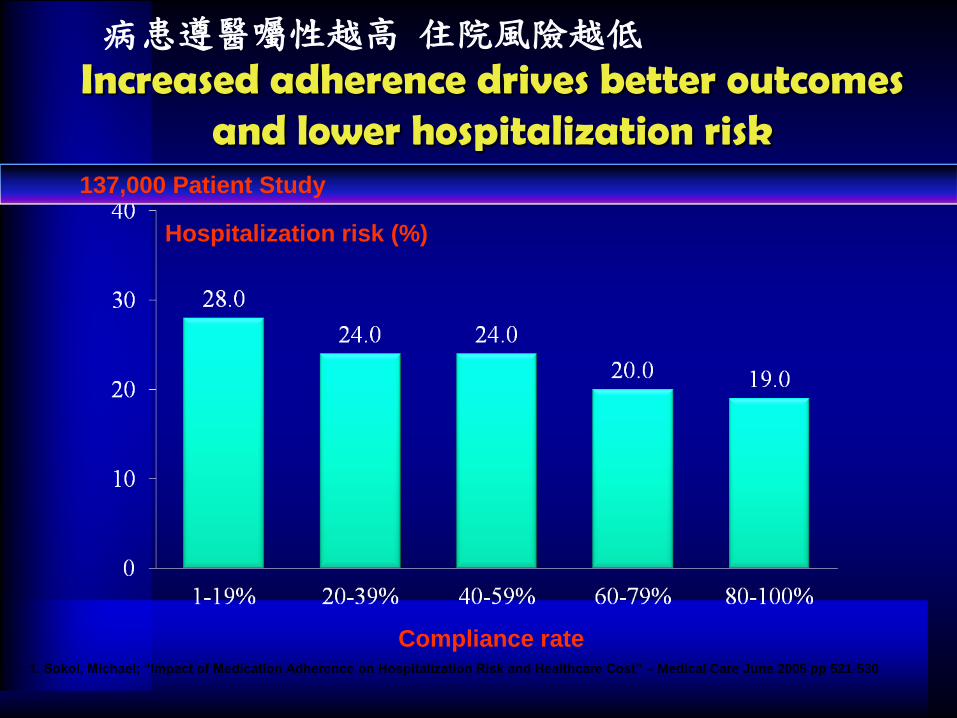
Increased adherence drives better outcomes and lower hospitalization risk
1. Sokol, Michael; “Impact of Medication Adherence on Hospitalization Risk and Healthcare Cost” – Medical Care June 2005 pp 521-530
Hospitalization risk (%)
Compliance rate
137,000 Patient Study
病患遵醫囑性越高 住院風險越低
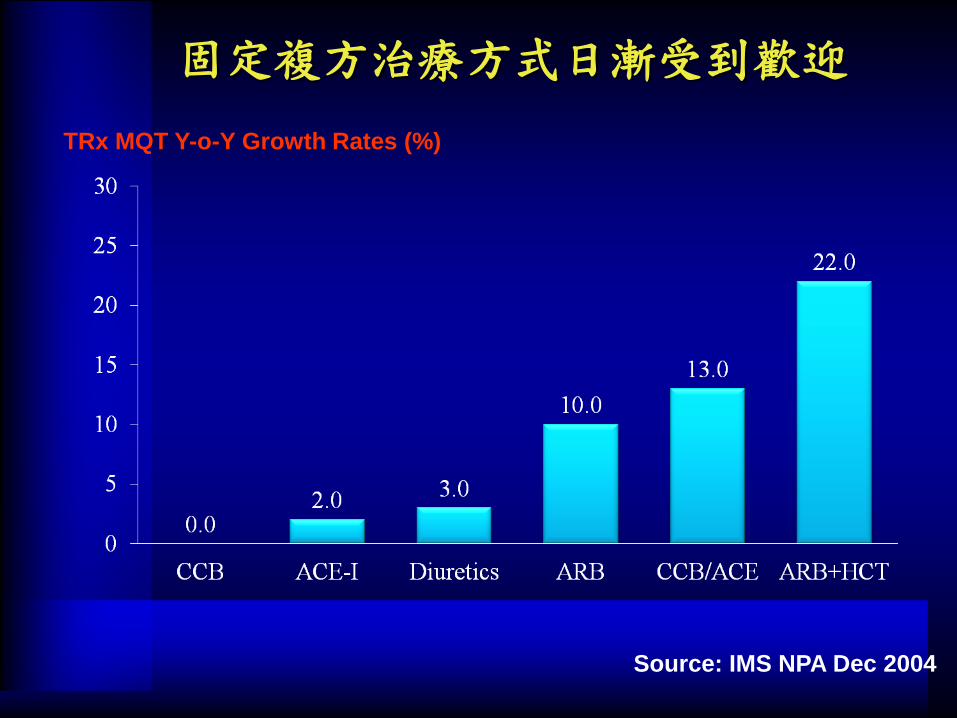
Source: IMS NPA Dec 2004
固定複方治療方式日漸受到歡迎
TRx MQT Y-o-Y Growth Rates (%)
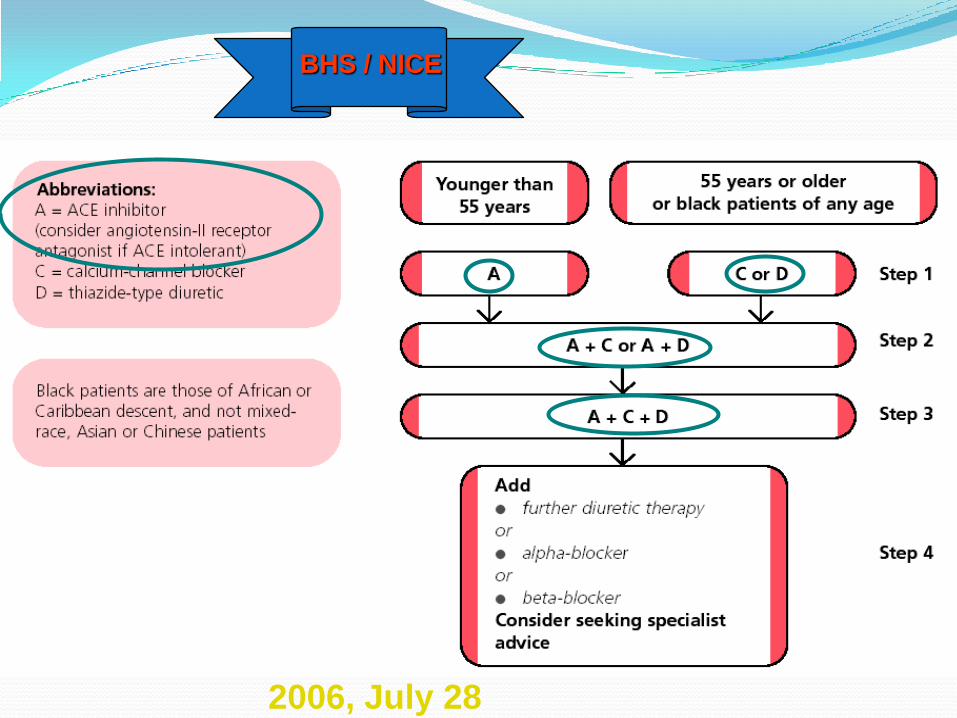
2006, July 28
BHS / NICE
Topics
• 高血壓之控制率
• 高血壓用藥之選擇
• Fix-Dose Combination之優勢
• 血壓藥之發展趨勢
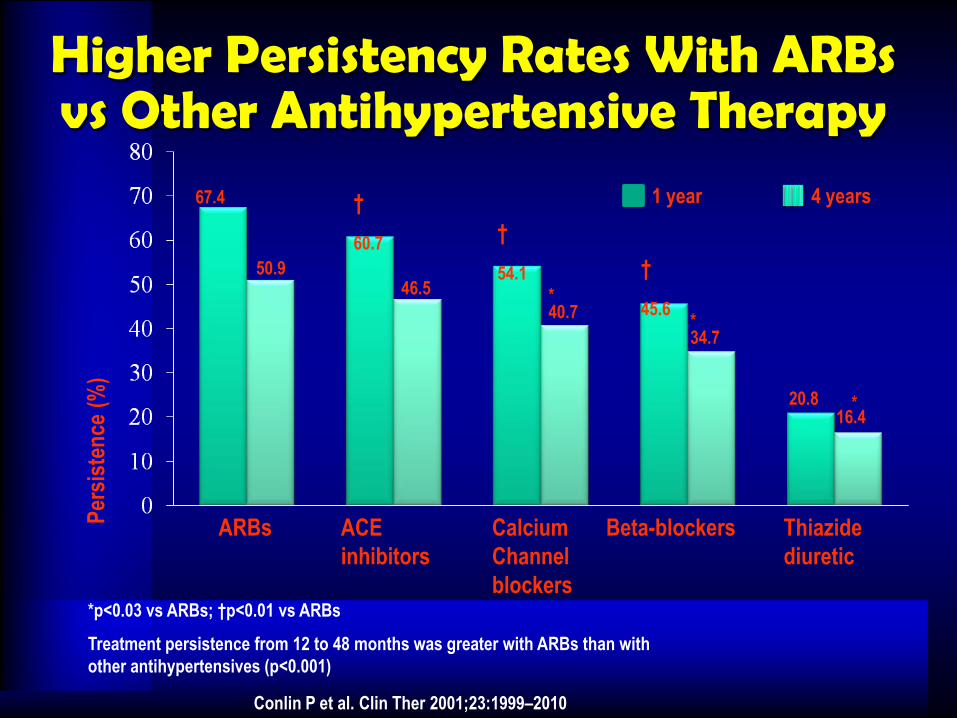
Higher Persistency Rates With ARBs vs Other Antihypertensive Therapy
67.4
Per
sist
ence
(%
)
ARBs ACE
inhibitors
Calcium
Channel
blockers
Beta-blockers Thiazide
diuretic
†
60.7
50.946.5
16.4
*34.7
*40.7
20.8
†
54.1 †
45.6
1 year 4 years
*p<0.03 vs ARBs; †p<0.01 vs ARBs
Treatment persistence from 12 to 48 months was greater with ARBs than with
other antihypertensives (p<0.001)
Conlin P et al. Clin Ther 2001;23:1999–2010
*
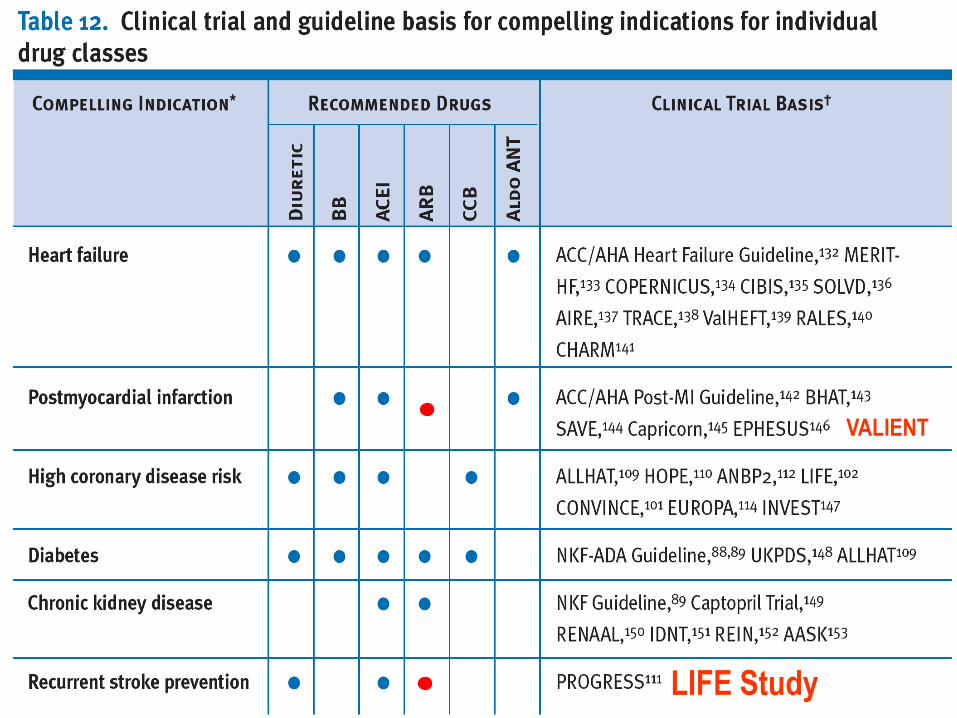
VALIENT
LIFE Study
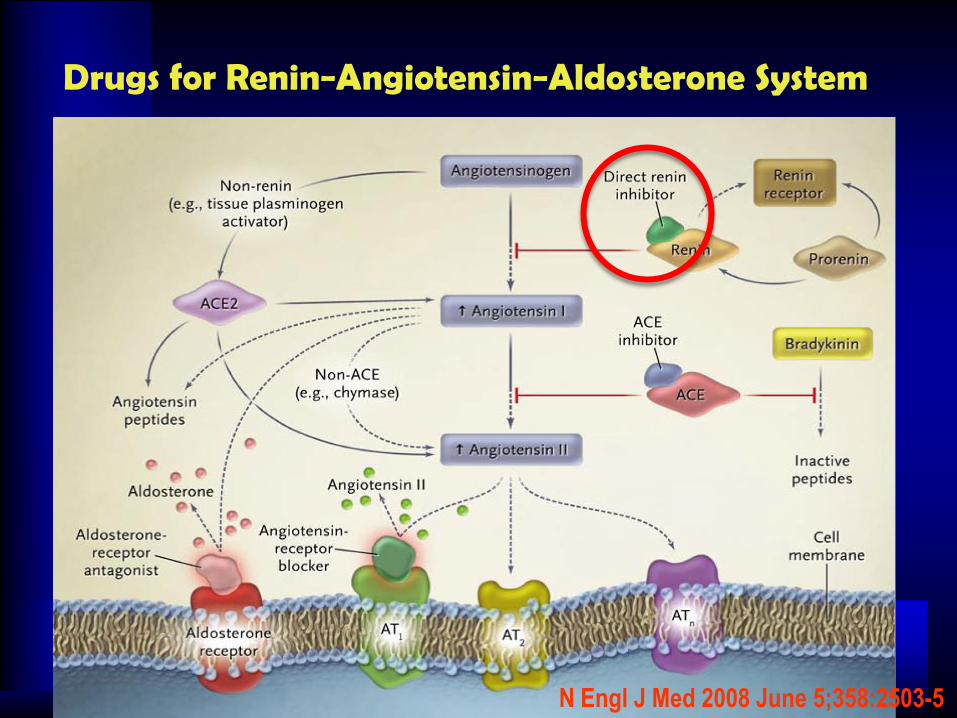
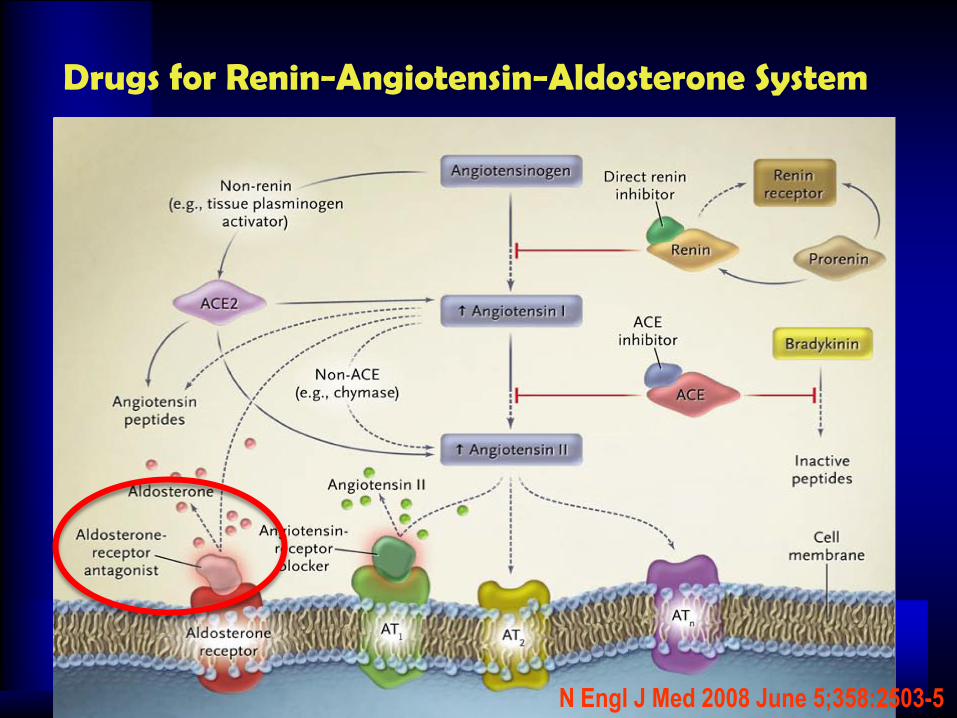
Drugs for Renin−Angiotensin−Aldosterone System
N Engl J Med 2008 June 5;358:2503-5
FDA approves aliskiren: First new antihypertensive on the market in more than 10 years
March 6, 2007
Michael O'Riordan
Basel, Switzerland - The Food and Drug Administration (FDA) has approved the blood-pressure drug aliskiren (Tekturna, Novartis), the first new antihypertensive medication to be approved in more than 10 years.
The drug is the first in a new class of agents known as oral renin inhibitors and is approved for the treatment of high blood pressure as monotherapy or in combination with other antihypertensive medications. The drug is expected to be available in pharmacies this month in 150-mg and 300-mg doses.
A once-daily oral tablet, aliskiren blocks the action of renin at the top of the renin-angiotensin-system cascade. A pooled data analysis of antihypertensive treatment with the drug in more than 8000 patients, presented by Dr Matthew R Weir (University of Maryland School of Medicine, Baltimore) at the World Congress of Cardiology in Barcelona in September and previously reported by heartwire, suggested that it reduces blood pressure effectively regardless of age or gender, is well tolerated, and appears to be additive to most other antihypertensive agents, with the exception of angiotensin-receptor blockers.
In December, the FDA extended by three months its review of aliskiren following the voluntary submission of more data by Novartis. Preclinical work in rats showed some irritation of the colonic mucosa with the drug, so a decision was made to do a further study in 30 healthy volunteers. Results of this showed no changes in the mucosal lining of the colon, Novartis said.
Financial analysts have previously suggested that aliskiren may generate sales of at least $1 billion a year.
Rasilez NEJM Update
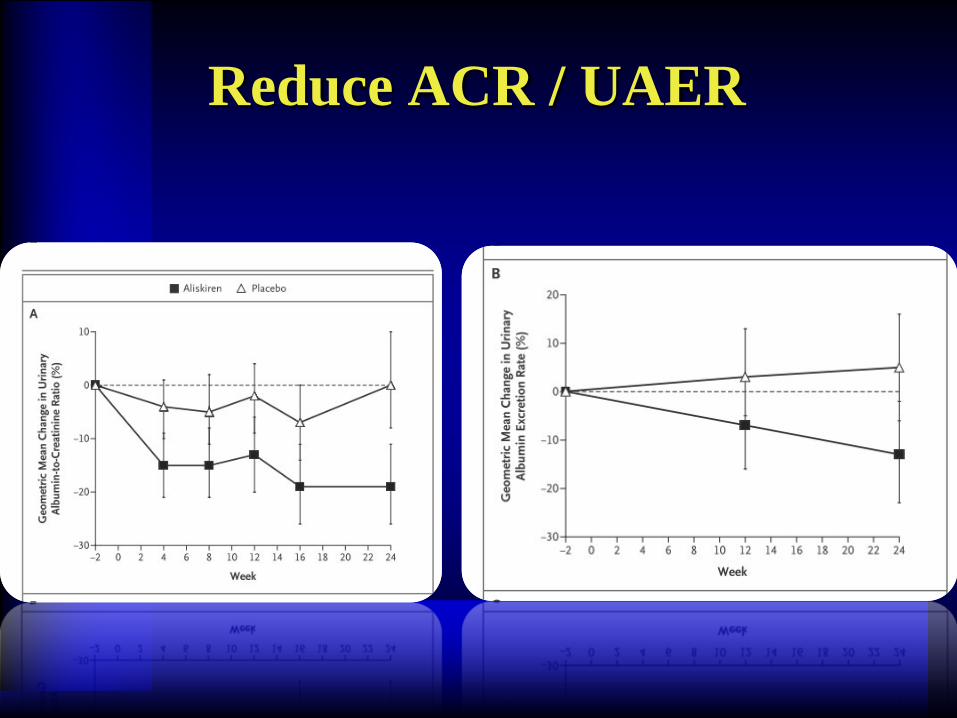
Reduce ACR / UAER
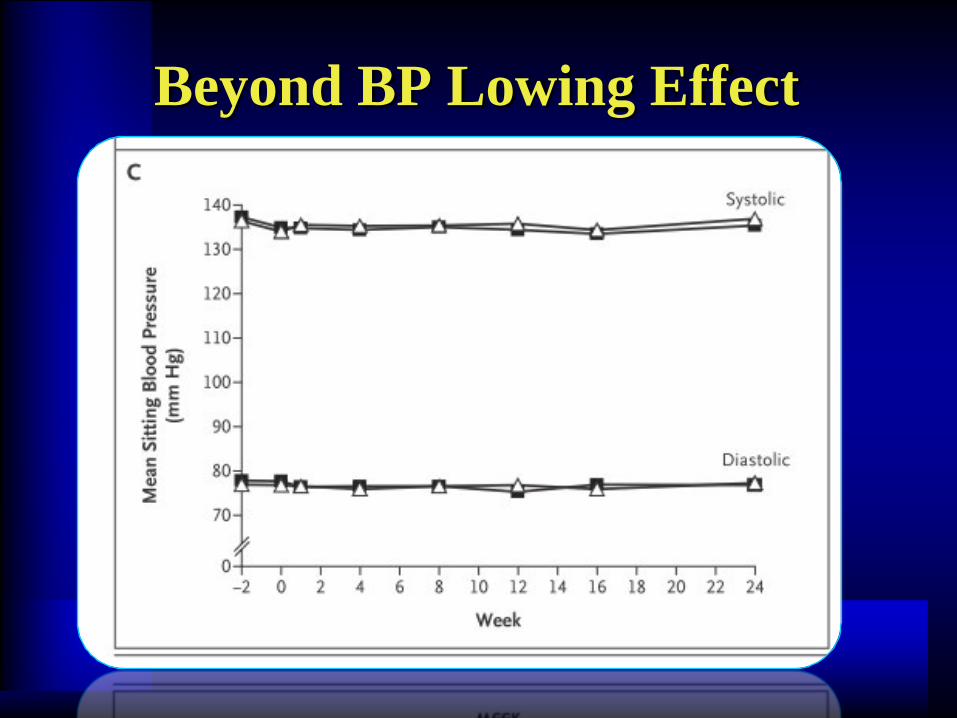
Beyond BP Lowing Effect
Drugs for Renin−Angiotensin−Aldosterone System
N Engl J Med 2008 June 5;358:2503-5